Paeds · clinical-pharmacology-and-therapeutics
Immunosuppressive and biologic therapies
Also known as Methotrexate in juvenile idiopathic arthritis · TNF inhibitors in children · Biologic therapies in paediatrics · DMARDs in children · Pre-biologic screening in children
A fellowship approach to immunosuppressive and biologic therapies in children covering low-dose weekly methotrexate as the anchor disease-modifying antirheumatic drug in juvenile idiopathic arthritis, the tumour necrosis factor inhibitors etanercept, adalimumab and infliximab across rheumatology and inflammatory bowel disease, the interleukin-1, interleukin-6 and B-cell-depleting biologics, the pre-biologic screen for tuberculosis, hepatitis B and varicella with dual tuberculin and IGRA testing, folic acid supplementation and full-blood-count and liver-enzyme monitoring on methotrexate, and live-vaccine timing before immunosuppression begins.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a six-year-old with polyarticular juvenile idiopathic arthritis whose morning stiffness will not settle, a twelve-year-old with Crohn's disease who is losing weight despite steroids, and a child with frequent-relapse nephrotic syndrome who has become steroid-dependent. Each of them will meet an immunosuppressive or a biologic drug. Methotrexate comes first in the rheumatic diseases, and the tumour necrosis factor inhibitors follow or run alongside it. [1] [6]
Two ideas carry the whole topic. The first is the screen-treat-monitor sequence: every biologic and every conventional immunosuppressant is started only after latent tuberculosis, hepatitis B, hepatitis C, HIV and varicella have been excluded or treated, and then kept safe by structured blood-count and liver-enzyme monitoring. The second is the anchor-and-target principle: methotrexate is the anchor disease-modifying drug in juvenile idiopathic arthritis, and the biologics are precision tools that block a single named cytokine when the anchor alone is not enough. [5] [6]
From the first referral to a child safely on therapy
1 · Confirm the diagnosis
Establish the immune-mediated disease with the specialist team before starting any immunosuppressive or biologic agent.
2 · Complete the pre-start screen
Screen for latent tuberculosis (tuberculin skin test and interferon-gamma release assay), hepatitis B, hepatitis C, HIV, varicella, and baseline bloods.
3 · Give live vaccines first
Complete measles-mumps-rubella and varicella vaccination, then wait before starting the immunosuppressant.
4 · Start the anchor or the biologic
Begin methotrexate once weekly with folic acid, or the chosen biologic at a weight-based or surface-area dose, under specialist guidance.
5 · Monitor and review
Check the full blood count and liver enzymes on a structured schedule, watch for infection, review growth and adherence, and plan the duration with the team.
Classification
The immunosuppressive and biologic drugs divide naturally by the target they hit. The conventional synthetic disease-modifying drugs work broadly. Methotrexate is the archetype — a folate-pathway inhibitor given once a week at a dose far below cancer-chemotherapy levels. Azathioprine and its prodrug 6-mercaptopurine, mycophenolate mofetil, and the calcineurin inhibitors ciclosporin and tacrolimus belong here too, used across nephrology, hepatology and transplant medicine. [1] [5]
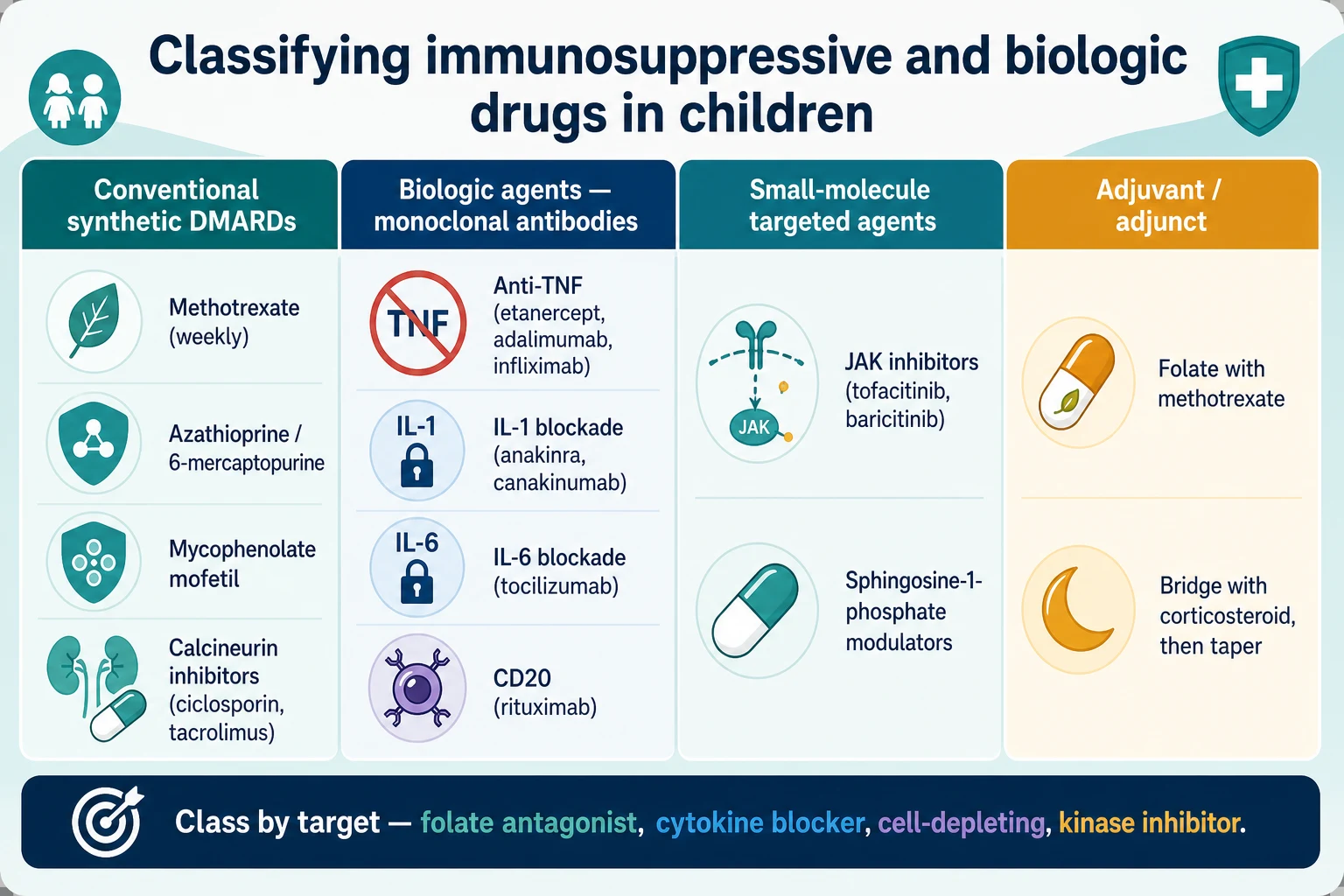
The biologic agents are monoclonal antibodies or receptor constructs that block one cytokine at a time. The tumour necrosis factor inhibitors — etanercept, adalimumab and infliximab — neutralise tumour necrosis factor alpha and dominate paediatric rheumatology and inflammatory bowel disease. The interleukin-1 blockers anakinra and canakinumab, the interleukin-6 blocker tocilizumab, and the B-cell-depleting anti-CD20 rituximab extend the toolkit into autoinflammatory syndromes, systemic juvenile idiopathic arthritis and refractory nephrotic syndrome. The small-molecule targeted agents, principally the Janus-kinase inhibitors tofacitinib and baricitinib, block intracellular signalling downstream of several cytokine receptors. [2] [6]
| Drug | Class and target | Representative paediatric use | Key caution |
|---|---|---|---|
| Methotrexate | Conventional synthetic — folate antagonist (anti-inflammatory at low weekly dose) | Anchor disease-modifying drug in juvenile idiopathic arthritis | Once weekly, never daily; folic acid; monitor FBC and LFTs |
| Etanercept | Biologic — soluble TNF receptor | Polyarticular juvenile idiopathic arthritis | TB reactivation; injection-site reactions |
| Adalimumab, infliximab | Biologic — anti-TNF monoclonal antibody | Juvenile idiopathic arthritis; Crohn disease; ulcerative colitis | Latent TB screen essential; immunogenicity may need dose escalation |
| Anakinra, canakinumab | Biologic — IL-1 blockade | Systemic juvenile idiopathic arthritis; periodic fever syndromes | Injection reactions; infection vigilance |
| Tocilizumab | Biologic — IL-6 blockade | Systemic and polyarticular juvenile idiopathic arthritis | Neutropenia; lipid and liver-enzyme monitoring |
| Rituximab | Biologic — anti-CD20 B-cell depletion | Refractory nephrotic syndrome; some vasculitides | Hypogammaglobulinaemia; infusion reactions; re-vaccination timing |
| Tofacitinib, baricitinib | Small molecule — Janus-kinase inhibitor | Selected polyarticular juvenile idiopathic arthritis | Infection; herpes zoster; lipid monitoring |
Epidemiology & Risk Factors
Juvenile idiopathic arthritis is the most common rheumatic disease of childhood, and methotrexate reaches the majority of children whose arthritis is not controlled by intra-articular steroid and non-steroidal agents. The biologic agents enter when methotrexate fails or when the disease is severe at the outset. In inflammatory bowel disease, the anti-tumour necrosis factor agents infliximab and adalimumab are now established for moderate-to-severe paediatric Crohn disease and ulcerative colitis. [6] [7]
Several factors push a child toward immunosuppressive therapy and toward its harms. A high disease-activity burden at diagnosis predicts the need for early aggressive combination treatment. Young age and small body size make dosing a surface-area calculation rather than an adult tablet. Endemic latent tuberculosis in the family or community raises the reactivation risk when a tumour necrosis factor inhibitor is started. Incomplete vaccination leaves a child exposed to measles, varicella or influenza once the immune system is dampened. And poor access to laboratory monitoring — a real problem in remote and disadvantaged settings — turns a safe drug into a dangerous one if the blood count and liver enzymes cannot be checked on schedule. [9] [10]
Child starting methotrexate
Anchor therapy
- Once-weekly low-dose folate antagonist
- Folic acid on the non-methotrexate days
- FBC and LFTs on a structured schedule
- Watch for nausea, mucositis, transaminitis
Child starting an anti-TNF
Precision biologic
- Latent TB screen with TST and IGRA before the first dose
- Hepatitis B, hepatitis C, HIV and varicella checked
- Live vaccines completed beforehand
- Vigilance for serious and atypical infection
Immunocompromised host
Compounded risk
- Highest risk of reactivating latent TB and viral hepatitis
- Live vaccines contraindicated once immunosuppressed
- Atypical infections can present without classical signs
- Needs coordinated specialist and primary care
Child in a remote setting
Access barrier
- Latent TB prevalence may be higher
- Timely laboratory monitoring is harder to arrange
- Cold-chain for biologics and travel burden matter
- A single coordinator closes the safety gap
Pathophysiology
These drugs calm inflammation by interrupting it at two different points. Methotrexate works inside the immune cell, and the biologics work on the cytokine signal between cells. Understanding the split tells you why methotrexate is a broad anchor and why the biologics are precision tools. [1] [6]
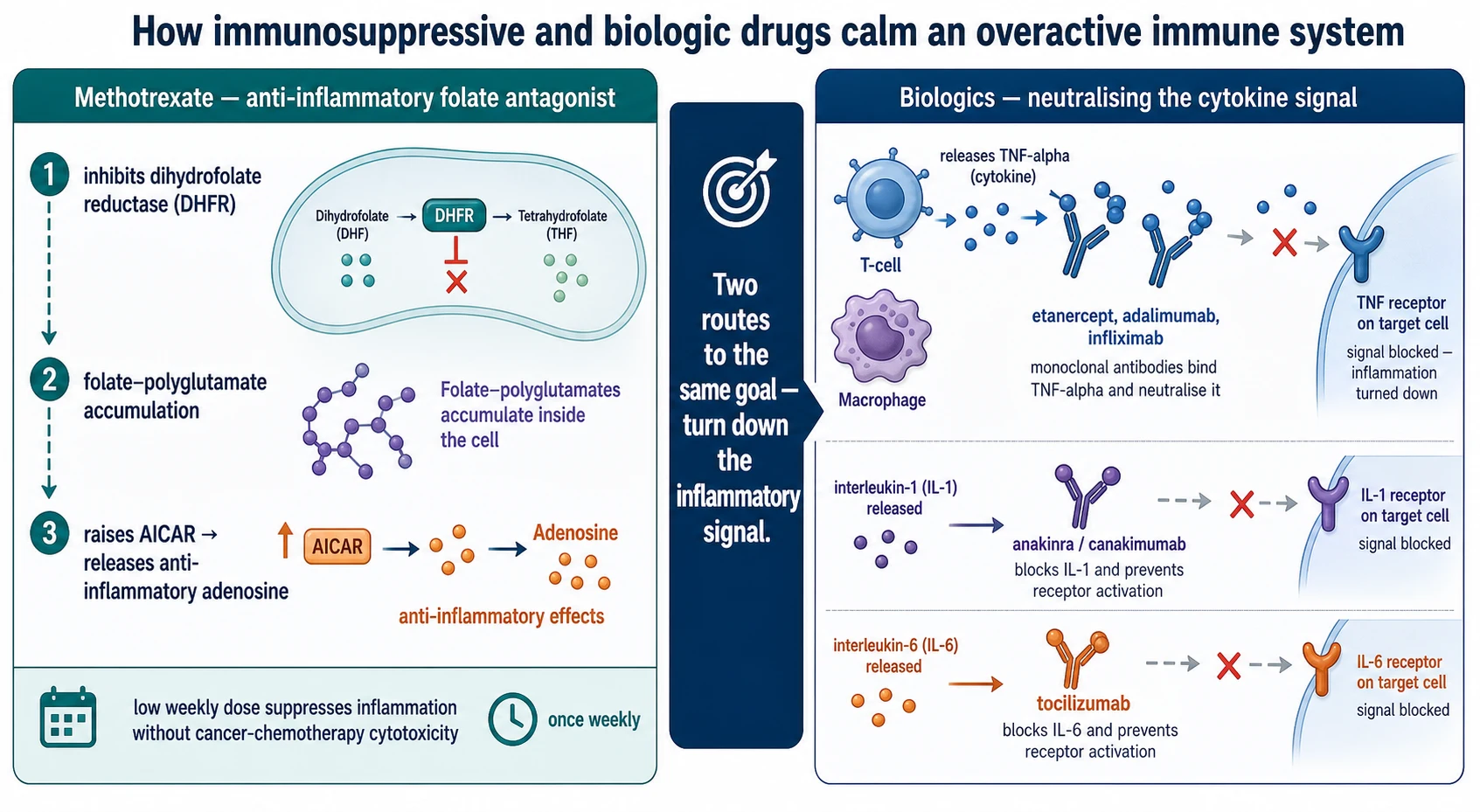
Methotrexate at the low once-weekly doses used in rheumatology does not kill cells the way high-dose chemotherapy does. It inhibits dihydrofolate reductase and leads to accumulation of methotrexate polyglutamates inside the cell, which suppress folate-dependent pathways and raise the level of adenosine, a mediator that powerfully dampens inflammation. This is why a small weekly dose quiets the immune system without the bone-marrow suppression seen at cytotoxic doses — and why folic acid is given alongside it on the non-methotrexate days to protect normal cells without abolishing the anti-inflammatory effect. [5]
The tumour necrosis factor inhibitors act one step out, in the conversation between cells. Macrophages and T cells release tumour necrosis factor alpha, which binds receptors on inflamed tissue and drives the redness, swelling and tissue damage of juvenile idiopathic arthritis and Crohn disease. Etanercept is a soluble receptor that mops the cytokine up; adalimumab and infliximab are monoclonal antibodies that bind tumour necrosis factor directly. The same logic extends to the interleukin-1 and interleukin-6 blockers, which intercept the cytokines driving systemic juvenile idiopathic arthritis and the autoinflammatory syndromes. [2] [3]
Because the tumour necrosis factor inhibitors take the brake off latent intracellular infection, the patient whose tuberculosis was dormant can develop disseminated disease once the cytokine is blocked. This single mechanism is why the pre-biologic tuberculosis screen is non-negotiable: latent infection must be found and treated with chemoprophylaxis before the first dose of an anti-tumour necrosis factor agent. [9] [10]
Clinical Presentation
You meet these drugs in three clinical settings. The first is the outpatient clinic, where a child with juvenile idiopathic arthritis is started on methotrexate after intra-articular steroid and non-steroidal agents have not controlled the synovitis. The second is the gastroenterology or rheumatology service, where a biologic is added because methotrexate or corticosteroid has failed or the disease is severe. The third is the acute presentation — a febrile child on a biologic, or a methotrexate patient with new mouth ulceration and a sore throat — where the question is whether the immunosuppression has caused harm. [6] [8]
Toxicity declares itself along recognisable lines. On methotrexate, transaminitis and neutropenia are the laboratory warnings, while nausea, mucositis and oral ulceration are the clinical ones. On the tumour necrosis factor inhibitors, the dominant worry is infection — including reactivated tuberculosis that can present atypically or disseminated, and serious bacterial infection. Infusion reactions occur with intravenous infliximab, and injection-site reactions with the subcutaneous agents. Rare but recognised effects of anti-tumour necrosis factor therapy include drug-induced lupus and demyelinating events, which demand stopping the drug and specialist review. [7] [10]
Differential Diagnosis
When a child on immunosuppressive therapy becomes unwell, the first question is whether the symptom is the disease, the drug, or an infection unmasked by the drug. A fever in a child on a tumour necrosis factor inhibitor is infection until proven otherwise, and the infection may be atypical: tuberculosis that is disseminated rather than pulmonary, a viral illness that runs an unusual course, or a bacterial sepsis that lacks the usual inflammatory signs. [10]
A rising alanine aminotransferase on methotrexate raises the differential of drug-induced hepatotoxicity against the liver involvement of the underlying disease, and the falling neutrophil count raises methotrexate myelosuppression against a viral marrow effect. New mouth ulceration is methotrexate mucositis until excluded. A child on a calcineurin inhibitor who becomes hypertensive or tremulous has drug toxicity to consider alongside disease flare. The safeguard in every case is to check the relevant bloods, hold the suspect drug while you assess, and involve the specialist team early. [5] [8]
Clinical & Bedside Assessment
Bedside assessment of a child on these therapies means assessing the disease control and the drug safety at the same visit. For juvenile idiopathic arthritis, examine the joints for active synovitis, ask about morning stiffness and function, and check growth — failure to thrive signals uncontrolled disease or drug intolerance. For inflammatory bowel disease, weigh the child, review stool frequency and abdominal pain, and ask about growth velocity. [6] [8]
Then turn to the drug. For methotrexate, ask about nausea, mouth soreness and appetite, and confirm the child is taking folic acid on the non-methotrexate days; many children tolerate the subcutaneous route better once the dose rises above about 12 to 15 mg/m². For any biologic, ask about fever, cough, weight loss and night sweats — the screen for tuberculosis reactivation — and about any rash or reaction at the injection or infusion site. Confirm the immunisation status, because live vaccines must not be given once the child is immunosuppressed. [5] [11]
Adherence is a clinical sign worth asking about directly. Methotrexate is weekly, and families miss doses; biologics are injected or infused on schedules that slip. A child whose disease "suddenly stops responding" may simply have stopped taking the drug. Ask about school absence, needle fear, nausea around the methotrexate day, and who gives the injection at home. [4] [6]
Investigations
The investigations divide into the pre-start screen and the on-treatment monitoring panel. The pre-start screen is the same for every biologic and for methotrexate at the higher end of dosing, and it exists to find the infections that immunosuppression will reactivate. Latent tuberculosis is sought with both a tuberculin skin test and an interferon-gamma release assay, because each method misses cases the other catches and the dual approach raises sensitivity. A chest X-ray is added when either test is positive or when the child carries tuberculosis risk. Hepatitis B serology includes surface antigen, core antibody and surface antibody; hepatitis C and HIV are screened; and varicella history is confirmed with serology when uncertain. [9] [10]
| Test | When | What it tells you | Action if abnormal |
|---|---|---|---|
| Tuberculin skin test AND interferon-gamma release assay | Before any biologic; before methotrexate at higher dosing | Latent tuberculosis — dual testing raises sensitivity | Treat latent TB with chemoprophylaxis before the first biologic dose |
| Chest X-ray | If TB test positive or TB risk present | Occult active or old tuberculosis | Specialist review; exclude active disease before immunosuppression |
| Hepatitis B (HBsAg, anti-HBc, anti-HBs) | Before any biologic or immunosuppressant | Chronic, resolved or susceptible hepatitis B | Vaccinate the susceptible; refer the chronic; prophylaxis may be needed on biologic |
| Hepatitis C and HIV | Before any biologic | Co-infection that changes the safety profile | Specialist input before starting immunosuppression |
| Varicella serology | Before any biologic | Immunity to varicella-zoster | Vaccinate the non-immune before immunosuppression begins |
| FBC, LFTs, creatinine | Baseline, then every 4–12 weeks on methotrexate | Bone-marrow and liver safety | Hold or reduce methotrexate; recheck; specialist advice |
The on-treatment monitoring for methotrexate is a full blood count and liver enzymes and creatinine, checked at baseline, soon after starting, and then roughly every four to twelve weeks depending on stability. The same bloods apply to the calcineurin inhibitors, with added attention to blood pressure and, for tacrolimus, drug levels. For the biologics, the monitoring is largely clinical — infection surveillance, growth, and injection or infusion reactions — with bloods guided by the specific agent, such as neutrophil and lipid monitoring on tocilizumab. [8] [11]
SCREAM — the pre-biologic screen you cannot skip
Management — Resuscitation
The resuscitation moment in this topic is the febrile immunosuppressed child. A child on a tumour necrosis factor inhibitor with a fever may have an ordinary viral illness, but they may equally have bacteraemia or reactivated tuberculosis that presents without the usual localising signs. The immediate actions are to assess for sepsis using the standard paediatric pathway, take cultures, begin empirical antibiotics early when sepsis is suspected, and hold the next biologic dose while you investigate. [10]
For suspected methotrexate toxicity — neutropenia, severe mucositis, or transaminitis with symptoms — hold the drug, check the full blood count and liver enzymes, give supportive care, and seek specialist advice; folinic acid (not folic acid) rescue is used for methotrexate overdose under specialist guidance. For an infusion reaction to infliximab, slow or stop the infusion, treat the reaction, and reconsider the rate and premedication for future doses with the team. [7] [8]
Management — Definitive & Stepwise

Methotrexate is the anchor disease-modifying drug in juvenile idiopathic arthritis, established by the placebo-controlled trial of Giannini and colleagues. It is given once weekly by mouth or subcutaneous injection at a dose of about 10 to 15 mg/m², with folic acid on the non-methotrexate days to reduce mucosal and hepatic toxicity. The MARAJIA expert consensus sets out the dosing, route-switch, monitoring and adverse-effect management that paediatric rheumatology services follow, including the move to subcutaneous dosing when the oral dose rises above about 12 to 15 mg/m² or when nausea is limiting. [1] [5]
Dosing and monitoring principles (verify against the current local formulary)
The tumour necrosis factor inhibitors are the biologics you will prescribe most often. Etanercept, the first biologic licensed for juvenile idiopathic arthritis, was shown to be effective in the trial of Lovell and colleagues, given subcutaneously at about 0.4 mg/kg twice weekly. Adalimumab, added with or without methotrexate, gave better control with methotrexate on board in the trial of Lovell and colleagues, at a dose of about 24 mg/m² every other week. In Crohn disease, infliximab at about 5 mg/kg at weeks 0, 2 and 6 and then every 8 weeks — the REACH regimen of Hyams and colleagues — is the standard induction and maintenance, with adalimumab as an alternative anti-tumour necrosis factor option with long-term paediatric safety data. [2] [3] [7] [8]
Vaccination is part of definitive management, not an afterthought. The EULAR and PRES recommendations for paediatric patients with autoimmune inflammatory rheumatic disease make the principle explicit: complete the live vaccines — measles-mumps-rubella and varicella — before immunosuppression begins, then wait the recommended interval, because live vaccines are contraindicated once the child is on biologic therapy. Inactivated vaccines, including annual influenza, can be given on treatment, though the immune response may be blunted. [11]
Specific Subtypes & Scenarios
The child with polyarticular juvenile idiopathic arthritis is the archetype. After intra-articular corticosteroid and a trial of non-steroidal agents, methotrexate is started once weekly with folic acid, and the joints, growth and bloods are reviewed at structured intervals. When methotrexate alone does not control the disease, a tumour necrosis factor inhibitor is added; etanercept and adalimumab are the commonest choices, and adalimumab works better with concomitant methotrexate. [1] [3]
The child with systemic juvenile idiopathic arthritis follows a different path. The interleukin-1 and interleukin-6 blockers are central here because the disease is cytokine-driven, and methotrexate is less reliably effective. Canakinumab and tocilizumab have transformed a disease once dominated by systemic corticosteroids, at the cost of careful infection surveillance and, for tocilizumab, neutrophil and lipid monitoring. [6]
The first year of a child on weekly methotrexate for juvenile idiopathic arthritis
The child with paediatric Crohn disease who is steroid-dependent or has complicated disease meets infliximab or adalimumab. The REACH regimen of infliximab at about 5 mg/kg is the standard induction and maintenance, and the long-term paediatric data on adalimumab support its use where an anti-tumour necrosis factor agent is needed. Concomitant immunomodulation reduces immunogenicity and antibody formation, which is why methotrexate or an antimetabolite sometimes runs alongside. The child with frequent-relapse or steroid-dependent nephrotic syndrome may meet rituximab, a B-cell-depleting biologic, when calcineurin inhibitors and antimetabolites have failed. [7] [8]
Complications & Pitfalls
The complications of these drugs are the harms that screening and monitoring exist to prevent. Methotrexate causes transaminitis, neutropenia, mucositis and nausea; the tumour necrosis factor inhibitors cause infection — including reactivated tuberculosis that can be disseminated — and infusion or injection reactions; the calcineurin inhibitors cause nephrotoxicity, hypertension and tremor. Most of these are avoidable or reversible when the screen and the monitoring are done well. [5] [10]
Four pitfalls recur at the bedside. The first is the missed pre-biologic screen: a tumour necrosis factor inhibitor started without latent tuberculosis testing, and the child develops disseminated disease. The second is the weekly-versus-daily methotrexate error: the drug written as a daily dose, causing cytotoxic bone-marrow suppression. The third is the live vaccine on treatment: a measles-mumps-rubella or varicella vaccine given to a child already on a biologic, risking uncontrolled vaccine-strain infection. The fourth is the unmonitored prescription: methotrexate continued for months without a full blood count or liver enzymes, until neutropenia or hepatitis declare themselves. [9] [11]
Principle
- Screen before you treat, monitor while you treat
- Methotrexate is the anchor; biologics are precision tools
- Class by target: folate antagonist, cytokine blocker, cell-depleting, kinase inhibitor
Methotrexate
- Once weekly, about 10 to 15 mg/m²
- Folic acid on non-methotrexate days
- Subcutaneous if dose above ~12 to 15 mg/m² or nausea
- FBC and LFTs every 4 to 12 weeks; never daily
TNF inhibitors
- Etanercept, adalimumab, infliximab
- Latent TB screen (TST + IGRA) before first dose
- Infliximab 5 mg/kg weeks 0, 2, 6 then every 8 weeks for Crohn
- Watch for infection and infusion reactions
Pre-start screen
- Tuberculosis: TST AND IGRA
- Hepatitis B, hepatitis C, HIV
- Varicella immunity; vaccinate if non-immune
- Baseline FBC, LFTs, renal, pregnancy test
Vaccination
- Live vaccines BEFORE immunosuppression
- No live vaccines on biologic therapy
- Annual inactivated influenza on treatment
Pitfalls
- Skipped pre-biologic screen
- Methotrexate written daily
- Live vaccine on treatment
- Unmonitored long-term methotrexate
“Screen (TB, hepatitis, varicella, bloods) → treat (methotrexate weekly with folate, or the chosen biologic at a weight-based dose) → monitor (FBC, LFTs, infection, growth) → never start without the screen, never give methotrexate daily, never give live vaccines on treatment.”
Prognosis & Disposition
The prognosis for the diseases these drugs treat has improved markedly. Methotrexate brings many children with juvenile idiopathic arthritis into inactive disease, and the tumour necrosis factor inhibitors and interleukin blockers rescue those who do not respond. In Crohn disease, anti-tumour necrosis factor therapy induces and maintains remission and restores growth in children who were failing on corticosteroid alone. [1] [7]
Disposition is shared between the general paediatrician and the specialist service. The specialist starts and adjusts the immunosuppressant or biologic; the general paediatrician and primary care hold the monitoring schedule, the immunisation record, and the front door when the child becomes febrile. A child on a biologic who becomes unwell needs clear advice about when to seek urgent review, and the team needs a plan for holding the next dose during intercurrent illness. [8] [11]
The duration of therapy is a specialist decision that depends on the disease and the depth of remission. For methotrexate in juvenile idiopathic arthritis, the randomised withdrawal trial of Foell and colleagues showed that stopping at twelve months of remission reduced the relapse rate compared with stopping at six months — a finding that frames the shared decision about how long to continue. [4]
Special Populations
The young child on these drugs is the patient where weight and surface-area dosing, needle fear, and taste intolerance matter most. Methotrexate liquid tastes bitter, and many children tolerate the subcutaneous route better; folic acid reduces the mucosal and hepatic toll. Needle fear limits biologic adherence, and nurse-led injection education and support are part of safe prescribing. [5] [6]
The adolescent is the patient where adherence, transition and reproductive risk converge. A young person who self-administers may miss doses; the transfer to adult care is a moment to lose the patient; and for the girls of childbearing potential on methotrexate, teratogenicity demands reliable contraception and pregnancy planning. The transition should be structured, with a named coordinator and a clear handover that includes the diagnosis, the drug regimen, the monitoring schedule, and the reproductive risks. [4] [11]
Australia and Aotearoa New Zealand: the Royal Children's Hospital Melbourne clinical guidelines and the Australian Medicines Handbook Children's Dosing Companion are the primary references for methotrexate and biologic dosing and monitoring, with paediatric rheumatology and gastroenterology networks coordinating care. For Aboriginal and Torres Strait Islander and Māori children, the higher background prevalence of latent tuberculosis makes the dual tuberculin and interferon-gamma release assay screen and the cold-chain logistics for biologics in remote settings especially important, and a single coordinator with cultural support closes the gap. [9] [10]
Global and low-resource settings: where access to biologics, interferon-gamma release assay testing and reliable laboratory monitoring is limited, methotrexate remains the practical anchor, and the tuberculosis screen relies on tuberculin testing and clinical risk assessment. The principle — right drug, right screen, right monitoring — holds; the discipline of documenting the screen, the dose, the interval and the review date substitutes for the biologic when the biologic is unavailable. [5] [10]
Evidence, Guidelines & Regional Differences
The evidence for methotrexate in juvenile idiopathic arthritis rests on the placebo-controlled trial of Giannini and colleagues, which established the low once-weekly dose as effective in resistant disease, and on the MARAJIA expert consensus, which codified the dosing, route-switch, monitoring and adverse-effect management that paediatric rheumatology now follows. The methotrexate withdrawal trial of Foell and colleagues added the duration question, showing that twelve months of remission before withdrawal reduced relapse compared with six months. [1] [4] [5]
The tumour necrosis factor inhibitor evidence is built on the pivotal trials: etanercept in polyarticular juvenile idiopathic arthritis (Lovell and colleagues), adalimumab with and without methotrexate (Lovell and colleagues), and infliximab in paediatric Crohn disease through the REACH study (Hyams and colleagues), with long-term adalimumab safety data in Crohn disease from Faubion and colleagues. The Nature Reviews summary of treatment for non-systemic juvenile idiopathic arthritis (Shenoi and colleagues) integrates methotrexate and the biologics into current practice. [2] [3] [6] [7] [8]
The screening and vaccination evidence is anchored by the dual tuberculin and interferon-gamma release assay study before tumour necrosis factor initiation in Spanish children (Calzada-Hernández and colleagues), the review of tuberculosis and tumour necrosis factor inhibitors in children (Parigi and colleagues), and the EULAR and PRES vaccination recommendations for paediatric patients with autoimmune inflammatory rheumatic disease (Jansen and colleagues). The dual-screen message is consistent: each tuberculosis test alone misses cases, so the two are used together. [9] [10] [11]
The evidence is weaker where it rests on consensus rather than trial — the exact methotrexate monitoring interval, the threshold for switching route, and the management of immunogenicity to infliximab are practice-derived. Where the evidence is weaker, state the principle, cite the consensus source, and communicate the uncertainty to the family rather than implying a precision the data do not support. [5] [8]
Board and assessment distinctions
RACP current PREP curriculum candidates must apply safe prescribing and pre-treatment screening for immunosuppressive and biologic therapy within the medication-safety and acute-illness learning objectives; first-year trainees from 2027 encounter it under quality-and-safety goals. RCPCH Progress+ embeds safe prescribing and monitoring of these medicines as a core patient-safety outcome. The ABP General Pediatrics Content Outline covers pharmacology and medication management, including immunosuppressant and biologic safety. [5]
| Board or format | What the candidate must demonstrate |
|---|---|
| RACP DWE | Identify the correct methotrexate schedule, the pre-biologic screen, or the live-vaccine rule in a clinical vignette |
| RACP DCE long case | Build a screen-treat-monitor plan for a child with juvenile idiopathic arthritis or Crohn disease starting a biologic |
| MRCPCH clinical | Counsel a family on starting methotrexate: the weekly dose, the folic acid, the monitoring, and the infection precautions |
| ABP | Apply pharmacology-domain knowledge to select, dose, screen for and monitor an immunosuppressant or biologic |
| RCPSC structured oral | Defend the pre-biologic tuberculosis and viral screen and the monitoring plan across age groups |
Exam Pearls
Viva: why is methotrexate given once weekly in juvenile idiopathic arthritis?
Low-dose methotrexate works as an anti-inflammatory at once-weekly dosing through folate-pathway inhibition and the accumulation of anti-inflammatory adenosine, not by the cytotoxic killing that high daily doses achieve in cancer chemotherapy. The once-weekly schedule delivers enough intracellular methotrexate polyglutamate to suppress inflammation while sparing the bone marrow, and folic acid given on the non-methotrexate days reduces mucosal and hepatic toxicity without abolishing the benefit. Giving the same weekly dose daily is a dangerous error: it causes severe marrow suppression and mucositis. State the weekly schedule, the folic acid, and the dose of about 10 to 15 mg/m², and name the monitoring of the full blood count and liver enzymes. [1] [5]
Structured oral: a child is about to start an anti-TNF agent — what is your pre-start screen?
Before the first dose of a tumour necrosis factor inhibitor the child must be screened for the infections that immunosuppression can reactivate. Latent tuberculosis is sought with both a tuberculin skin test and an interferon-gamma release assay, because each method alone misses cases and the dual approach raises sensitivity; a chest X-ray is added when either test is positive or when tuberculosis risk is present, and any latent tuberculosis is treated with chemoprophylaxis before the biologic begins. Hepatitis B is screened with surface antigen, core antibody and surface antibody; hepatitis C and HIV are checked; and varicella immunity is confirmed, vaccinating the non-immune before immunosuppression starts. Live vaccines — measles-mumps-rubella and varicella — are completed before the biologic, because they are contraindicated on treatment. Baseline full blood count, liver enzymes, renal function and a pregnancy test in the relevant adolescent complete the screen. [9] [10] [11]
References
- [1]Giannini EH; Brewer EJ; Kuzmina N Methotrexate in resistant juvenile rheumatoid arthritis. Results of the U.S.A.-U.S.S.R. double-blind, placebo-controlled trial. The Pediatric Rheumatology Collaborative Study Group and The Cooperative Children's Study Group The New England journal of medicine, 1992.PMID 1549149
- [2]Lovell DJ; Giannini EH; Reiff A Etanercept in children with polyarticular juvenile rheumatoid arthritis. Pediatric Rheumatology Collaborative Study Group The New England journal of medicine, 2000.PMID 10717011
- [3]Lovell DJ; Ruperto N; Goodman S Adalimumab with or without methotrexate in juvenile rheumatoid arthritis The New England journal of medicine, 2008.PMID 18716298
- [4]Foell D; Wulffraat N; Wedderburn LR Methotrexate withdrawal at 6 vs 12 months in juvenile idiopathic arthritis in remission: a randomized clinical trial JAMA, 2010.PMID 20371785
- [5]Ferrara G; Mastrangelo G; Barone P Methotrexate in juvenile idiopathic arthritis: advice and recommendations from the MARAJIA expert consensus meeting Pediatric rheumatology online journal, 2018.PMID 29996864
- [6]Shenoi S; Horneff G; Aggarwal A Treatment of non-systemic juvenile idiopathic arthritis Nature reviews. Rheumatology, 2024.PMID 38321298
- [7]Hyams J; Crandall W; Kugathasan S Induction and maintenance infliximab therapy for the treatment of moderate-to-severe Crohn's disease in children Gastroenterology, 2007.PMID 17324398
- [8]Faubion WA; Dubinsky M; Ruemmele FM Long-term Efficacy and Safety of Adalimumab in Pediatric Patients with Crohn's Disease Inflammatory bowel diseases, 2017.PMID 28129288
- [9]Calzada-Hernández J; Anton J; Martín de Carpi J Dual latent tuberculosis screening with tuberculin skin tests and QuantiFERON-TB assays before TNF-α inhibitor initiation in children in Spain European journal of pediatrics, 2023.PMID 36335186
- [10]Parigi S; Licari A; Manti S Tuberculosis and TNF-α inhibitors in children: how to manage a fine balance Acta bio-medica : Atenei Parmensis, 2020.PMID 33004779
- [11]Jansen MHA; Rondaan C; Legger GE EULAR/PRES recommendations for vaccination of paediatric patients with autoimmune inflammatory rheumatic diseases: update 2021 Annals of the rheumatic diseases, 2023.PMID 35725297