Paeds · clinical-pharmacology-and-therapeutics
Inhaled therapies and device selection
Also known as Inhaler device selection in children · Spacer and valved holding chamber use · MDI, DPI and nebuliser in paediatrics · Aerosol drug delivery in children · Age-based inhaler choice
A fellowship approach to inhaled therapies and device selection in children covering the four device families — pressurised metered-dose inhaler, dry-powder inhaler, soft-mist inhaler and nebuliser — why a valved holding chamber (spacer) transforms pressurised-inhaler delivery, how aerosol particle size, inspiratory flow and coordination decide where a drug lands, and the age-based device ladder from the masked spacer in infants and toddlers to the dry-powder inhaler in the school-age child and self-managed adolescent.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a wheezy eighteen-month-old, a five-year-old with viral wheeze, and a twelve-year-old with established asthma. All three need an inhaled bronchodilator, but what they actually need to make that drug work is three different devices. The toddler cannot time a fast aerosol cloud to a single breath and cannot draw the powder through a disk, so she needs a pressurised inhaler seated in a small spacer with a mask sealed to her face. The five-year-old can use a spacer with a mouthpiece but probably cannot yet inhale a dry powder reliably. The twelve-year-old can choose a dry-powder inhaler or a spacer, guided by her own inspiratory flow and preference. [1] [2]
Two ideas govern everything that follows. First, the dose that reaches the lung is not the dose written on the label — it is the fraction that escapes the device, survives the upper airway, and is small enough and timed well enough to deposit in the bronchi. A pressurised inhaler used without a spacer deposits most of its dose in the oropharynx, not the lung; the same drug through a spacer multiplies lung delivery several-fold. [1] Second, that fraction depends on properties of the child that change with age — tidal volume, inspiratory flow, breath-hold ability, and the seal of a mask. A device that fits a teenager will deliver almost nothing to a toddler, and a device that fits a toddler will frustrate a teenager into non-adherence. Selecting the device is therefore a clinical act, not a pharmacy default. [2] [3]
From the prescription to the lung
1 · Choose the drug
Select reliever (salbutamol) or preventer (inhaled corticosteroid) by the child's diagnosis and severity, weight-based where relevant.
2 · Match the device
Pick the device by age, inspiratory flow and coordination — spacer plus mask under four, spacer plus mouthpiece four to six, DPI from school age.
3 · Prepare the device
Prime a new spacer, shake a pressurised inhaler, load a dry-powder device, and ensure the mask seals or the mouthpiece is sealed by the lips.
4 · Deliver the breath
One actuation into the spacer followed by slow tidal breathing (younger) or slow deep breaths with a breath-hold (older); one sharp inhalation for a DPI.
5 · Check and re-teach
Rinse after an inhaled corticosteroid, count the doses, and re-check technique at every visit — technique drifts.
Classification
Walk into a respiratory clinic and you will meet four families of inhaled device, and the family names what the child must do to make it work. A pressurised metered-dose inhaler (pMDI) is the familiar small canister that fires a measured aerosol cloud at high speed the instant it is pressed. Its strength is that the dose is fixed and it needs no inspiratory effort to release; its weakness is that the cloud is so fast it hits the back of the throat unless a spacer slows it. A dry-powder inhaler (DPI) — the Turbuhaler, Accuhaler or Breezhaler — holds the drug as a powder the child must draw out with a fast, deep breath, so it needs no coordination but demands a strong inspiratory flow. A soft-mist inhaler (SMI), such as the Respimat, releases a slow, long-lasting mist from a mechanical spring. A nebuliser turns liquid drug into a fine mist driven by compressed air or oxygen, so the child simply breathes normally through a mask or mouthpiece for several minutes. [1] [2]

The valved holding chamber — the spacer — deserves its own place in this picture because it is not a separate device so much as a transformer that changes what a pMDI can do. It is a tube or chamber with a one-way valve at the mouthpiece end: the aerosol cloud is fired into the chamber, the valve holds it suspended, and the child draws it in over several slow breaths without having to coordinate the press with the breath. A small-volume chamber (around 150 to 250 mL) suits the small tidal volume of an infant; a mask clips onto the front for the child who cannot seal the mouthpiece. Without a spacer, a pMDI in a young child deposits largely in the oropharynx and delivers little to the lung. [1] [8]
| Device | What releases the drug | What the child must do | Best fit |
|---|---|---|---|
| pMDI alone | Pressing the canister fires a fast aerosol cloud | Coordinate the press with a slow, deep breath in and a breath-hold | Almost no young child can — avoid without a spacer |
| pMDI plus spacer (valved holding chamber) | Same fast cloud, fired into the chamber | Breathe slowly through the chamber — tidal breaths for the young, slow deep breaths for the older child | First-line for infants and preschool children; all ages |
| Dry-powder inhaler (DPI) | The child's own fast breath draws the powder out | One sharp, deep inhalation, then a breath-hold | School-age child who can generate the inspiratory flow |
| Soft-mist inhaler (SMI) | A spring releases a slow, long-lasting mist | Slow, deep breath in coordinated with the trigger | Older children and adolescents; less used in young children |
| Nebuliser | Compressed air or oxygen turns liquid drug to mist | Breathe normally through a mask or mouthpiece for several minutes | The child who cannot use a spacer, or severe acute asthma needing oxygen |
Epidemiology & Risk Factors
Inhaled drugs are among the most prescribed medicines in all of paediatrics. Salbutamol, inhaled corticosteroids and their combinations appear in the management of asthma, viral wheeze, bronchiolitis, cystic fibrosis and chronic lung disease of prematurity, so almost every general paediatrician supervises a child using one every single day. The drug is common; the discipline of matching the device to the child and re-checking the technique is what separates good control from repeated emergency visits. [3]
The reasons an inhaled drug fails are usually found in the device and the breath, not the molecule. Wrong device for age is the cardinal error — a dry-powder inhaler handed to a four-year-old, or a pressurised inhaler given to a toddler without a spacer or mask. Poor coordination defeats the unaided pMDI, because the child presses at the wrong moment or holds the mouthpiece away from the open mouth. Mask leak in the infant wastes the dose, since the aerosol escapes around the seal rather than entering the airway. A static or unprimed plastic spacer attracts the drug to its walls before the child can inhale it. Technique drift erodes good control over months, because no device skill is permanent without rehearsal. And the wrong reliever route in acute severe asthma — withholding oxygen while waiting for a nebuliser, or using a nebuliser when a spacer would work — delays the dose that matters most. [1] [2]
Infant or toddler
Under four years
- Needs a spacer with a tightly-fitting mask
- Tidal breathing over several breaths delivers the dose
- A dry-powder inhaler will not work — too little flow
- Mask leak is the commonest reason a dose is wasted
Preschool child
Four to six years
- Spacer with a mouthpiece once a reliable seal is possible
- Slow deep breaths with a short breath-hold
- Dry-powder inhaler usually still too demanding
- Coordination with a bare pMDI still unreliable
School-age child
Six years and over
- Can use a dry-powder inhaler if inspiratory flow is adequate
- Spacer plus pMDI remains effective and often preferred
- Can learn a breath-hold and a dose counter
- Choice guided by flow, coordination and preference
Adolescent
Twelve years and over
- Any device is physically possible
- Adherence and discretion often drive the choice
- Once-daily dry-powder preventer may suit the forgetful teenager
- Technique and inhaler-device counselling still essential
Pathophysiology
The reason device choice matters so much in a child is the physics of an aerosol, which is governed by particle size and by how the child breathes. For a drug to reach the small airways the particles must be small — an aerodynamic diameter of roughly one to five micrometres is the respirable range. Larger particles, and the fast-moving droplets of a bare pMDI, strike the oropharynx and are swallowed; smaller particles float out in the exhaled breath. The whole art of delivery is to turn a dose into respirable particles and then to place them inside the child at the speed and depth the child can manage. [1] [8]
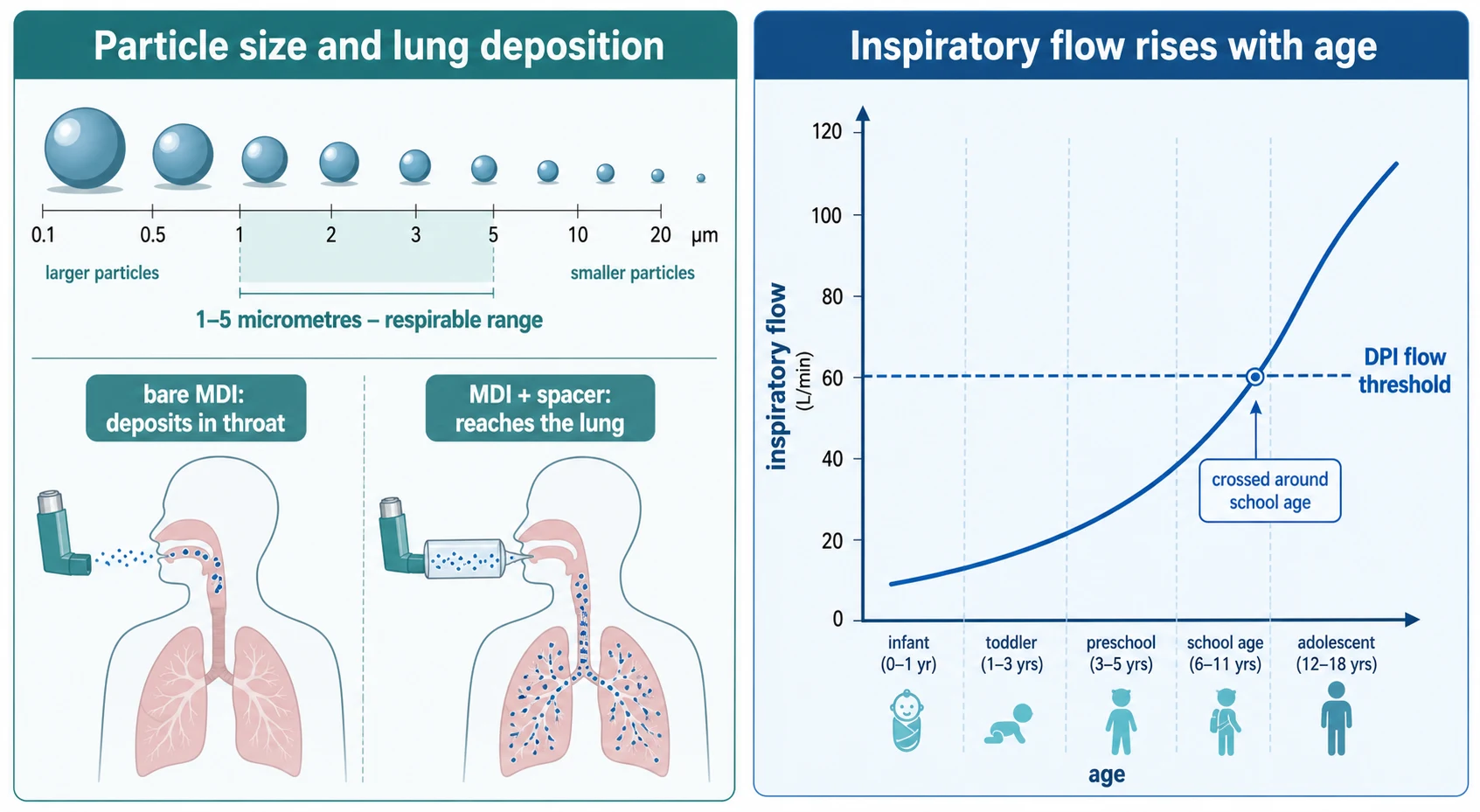
A pressurised inhaler releases its dose in less than a tenth of a second at high velocity, which is why the unaided pMDI deposits most of its drug in the mouth and throat. The spacer intercepts that fast cloud and gives it space to slow, the large droplets to evaporate and settle, so that by the time the child breathes in the particles are small and slow and lung deposition rises several-fold. A dry-powder inhaler works the opposite way: the powder sits inert in the device until the child's own fast breath shears the agglomerate apart into respirable particles. The faster and deeper the breath, the better the de-aggregation and the further the powder travels — which is exactly why a DPI is brilliant for a ten-year-old and useless for a three-year-old. [1] [8]
Two age-related mechanics complete the picture. The infant breathes tidally with a small volume, so the dose must be suspended in a spacer and cleared over several breaths, often through a mask — and a mask works only if it seals, because any leak lets the aerosol escape before it is inhaled. The school-age child can breathe deep and hold, so the same spacer delivers more per breath, and a dry-powder inhaler becomes a real option once the inspiratory flow clears the threshold the device demands. Bronchodilators and corticosteroids share this delivery physics, which is why a poorly controlled asthmatic often improves more from a device and technique fix than from a dose increase. [3] [10]
Clinical Presentation
The child whose inhaled therapy is failing does not usually say so. Instead the device problem announces itself through the disease: a wheezy child who returns to the emergency department despite a regular preventer, an asthmatic whose symptom scores creep up over a term, or an infant whose viral wheeze barely improves after salbutamol that may never have reached the lung. The device and the technique are an active part of the differential whenever an inhaled drug "isn't working." [3]
At the bedside you are looking for the mechanical signs that delivery has failed. Watch the child take a dose. Is the mask pressed firmly to the face, or is it floating loose with aerosol streaming from the gap? Does the spacer valve click with each breath, telling you the child is actually moving air through it? For a dry-powder inhaler, is the breath sharp and deep, or a shallow sip that leaves the powder in the device? Is the canister shaken, is the spacer primed and static-free, and does the older child hold the breath after inhalation? Each of these is a place where a full dose is quietly reduced to a fraction. [1] [8]
Differential Diagnosis
When an inhaled drug seems not to work, the device is only one of several suspects, and the examiner expects you to separate them. The framework is to ask whether the failure is in the delivery (wrong device, poor technique, mask leak, static spacer), the adherence (the dose is rarely or never given), the diagnosis (the wheeze is not asthma — think airway malacia, foreign body, or protracted bacterial bronchitis), or the severity (the disease genuinely needs a higher step of treatment). Each points to a different action, and conflating them is the commonest reason a child is over-treated with a device that was never the problem. [2] [3]
A short list of the mimics is worth holding. Tracheomalacia and bronchomalacia cause a wheeze that is fixed and does not respond to bronchodilators, so escalating inhaled therapy worsens nothing but helps nothing either. An inhaled foreign body gives monophonic wheeze unresponsive to salbutamol and needs imaging and removal, not more puffs. Protracted bacterial bronchitis produces a wet cough that settles with antibiotics rather than preventers. Viral-induced wheeze in the preschool child responds variably to bronchodilators and is not steroid-responsive asthma. Running through these before escalating a preventer protects the child from a rising dose of a drug that cannot reach the disease. [3] [10]
Clinical & Bedside Assessment
Assessing an inhaled therapy is a practical skill, done by watching the child take the dose. Ask the family to bring every device to the visit — the preventer, the reliever, the spacer, and any old inhalers in the cupboard — because what you find in the bag is the truth, and what the family describes is often a kinder version of it. [1]
For the spacer and mask, check four things. First, the seal: the mask should sit flat against the face with no gap, and you should see the valve move with each breath. Second, the breathing pattern: a young child clears the chamber with around six slow tidal breaths per actuation, an older child with one to two slow deep breaths and a short breath-hold. Third, the actuation: the canister is shaken, one puff is fired into the chamber with the mask already in place, and the next puff waits until the first is cleared. Fourth, the spacer itself: a plastic chamber should be primed before first use and washed in detergent without rinsing or wiping, to suppress the static charge that otherwise steals the dose. [1] [8]
For the dry-powder inhaler, check the inspiratory effort and the loading. The child should exhale fully away from the device, then take one sharp, deep inhalation that you can hear, and hold the breath. A breath that is weak or exhaled into the mouthpiece ruins the dose and clogs the device. Confirm the dose counter and the loading mechanism, since a DPI that is not primed or loaded delivers nothing. For every device, confirm the child rinses the mouth after an inhaled corticosteroid to prevent oral candidiasis, and knows the difference between the reliever and the preventer. [2] [11]
The four things to check at every visit — SEAL
Investigations
Inhaled therapy has no blood test — its "investigation" is the technique check, the dose counter, and the clinical response. The single most informative manoeuvre is a standardised inhaler-technique assessment repeated at every visit, because technique decays and a child grows out of one device and into another. Use a placebo inhaler or the child's own device, watch a full dose, and correct errors on the spot. [1] [2]
The dose counter on a DPI or a metered-dose inhaler is the second check, and it answers two questions: is the device empty, and is it being used at all? A preventer canister that still reads full months after prescription is a confession of non-adherence; one that runs out too fast may mean over-use of the reliever mistaken for the preventer. Where a spacer is used, check that it is the right volume for the child — a small-volume chamber for the infant's small tidal volume, a larger chamber for the older child — and that it is in good condition, valve intact and static suppressed. [3] [4]
Objective measures of response close the loop. In the school-age child, peak flow or spirometry before and after a bronchodilator confirms that the drug, correctly delivered, is reaching the airway; a child whose lung function does not move after a witnessed, well-delivered dose has a problem of diagnosis or severity, not of device. In the younger child, the response is clinical — respiratory rate, work of breathing, and auscultation after a reliever dose. [10]
Management — Resuscitation
In acute severe asthma the device decision is time-critical, and the principle is simple: give the reliever by the route that works fastest while you supply oxygen. Salbutamol by pMDI and spacer delivers the drug at least as effectively as a nebuliser for most acute attacks in children, with fewer side-effects such as tremor and tachycardia and a shorter emergency department stay. The Cochrane review of holding chambers versus nebulisers for beta-agonist treatment of acute asthma found equivalence or advantage for the spacer across children, and randomised trials in severe exacerbations have shown inhaler-and-spacer delivery to be superior to the nebuliser. [5] [6]
In the child who can cooperate, give salbutamol by pMDI through a spacer, one actuation at a time followed by the breaths, repeated over the first hour per the local acute-asthma guideline. Add ipratropium bromide for severe exacerbations. Reserve the oxygen-driven nebuliser for the child who is hypoxic, exhausted, or unable to coordinate the spacer. The schematic doses are age-stratified and must be verified against the current Australian Asthma Handbook, RCH or BNFc protocol before use — the principle to defend at viva is the route and the oxygen, not the exact puff count. [5] [6]
Management — Definitive & Stepwise
Definitive device management is an age-based ladder, taught and re-taught at every visit. The ladder exists because no single device fits a child across the whole of childhood, and stepping the child up the ladder as they grow is as important as stepping the drug. [1] [3]
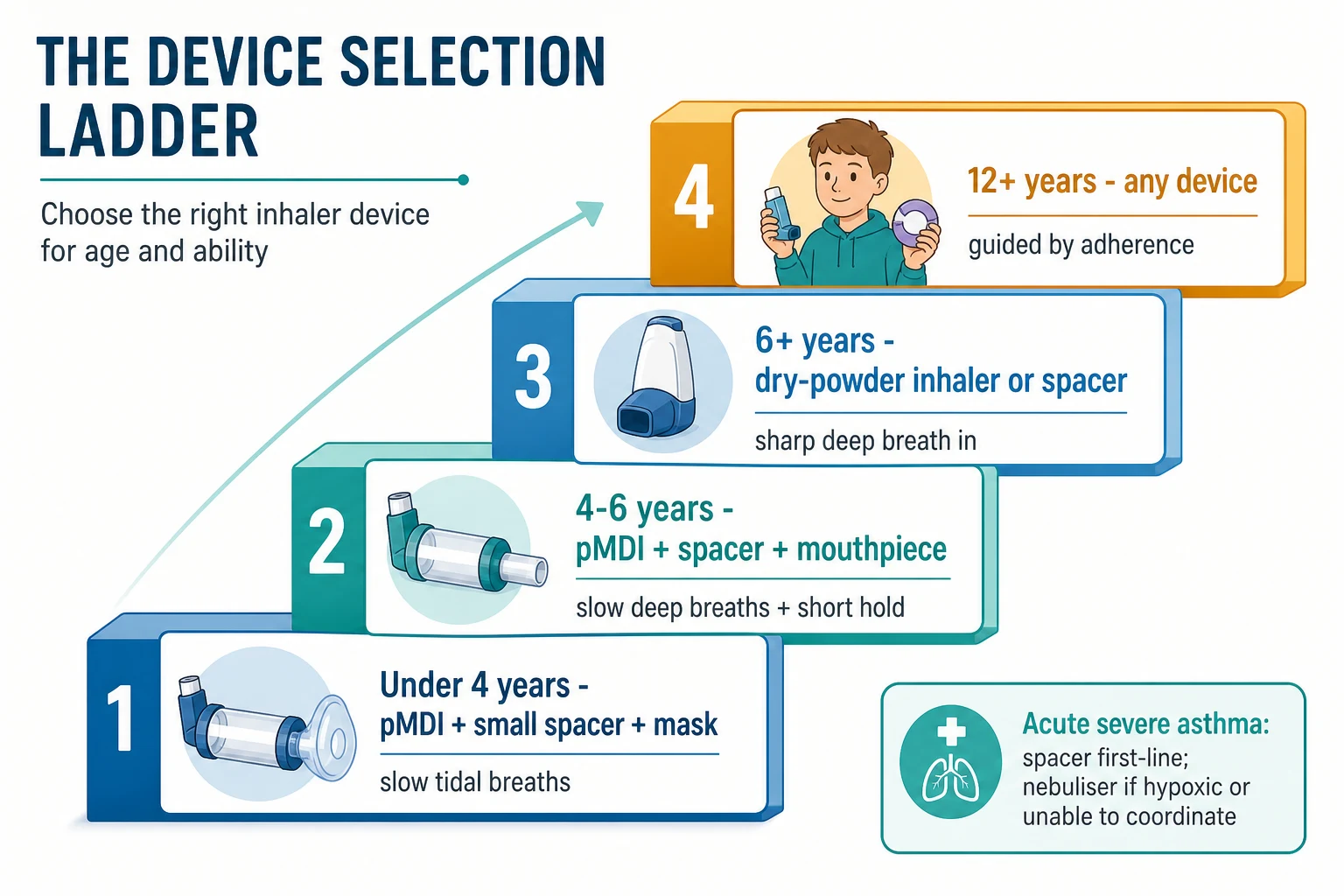
The infant and toddler under about four years uses a pressurised inhaler seated in a small-volume valved holding chamber with a tightly-fitting face mask. The dose is fired into the chamber and the child breathes tidally over several breaths; the mask is held firmly until the dose is cleared. The mask-to-mouthpiece transition happens around four to five years once the child can reliably seal the mouthpiece. A dry-powder inhaler is not suitable, because the child cannot generate the inspiratory flow. [8] [9]
The preschool child, about four to six years, moves to a spacer with a mouthpiece, taking slow deep breaths with a short breath-hold. A dry-powder inhaler remains unreliable in most of this group. The school-age child, from about six years, can use a dry-powder inhaler if the inspiratory flow is adequate, or continue a spacer plus pMDI; the systematic review of dry-powder inhaler use in primary-school-aged children confirms that technique and flow, more than age alone, decide suitability. The adolescent, twelve years and over, can use any device, and the choice is increasingly driven by adherence — a once-daily dry-powder preventer may suit the teenager who forgets, while discretion and portability shape the reliever choice. [2] [4]
| Age band | First-line device | Breath action | Rationale and caution |
|---|---|---|---|
| Under 4 years | pMDI plus small-volume spacer plus tightly-fitting mask | Slow tidal breaths, around six per actuation, mask sealed to the face | Infant tidal volume is small and coordination absent; mask leak wastes the dose |
| 4 to 6 years | pMDI plus spacer with mouthpiece | One to two slow deep breaths with a short breath-hold per actuation | Mouthpiece once a reliable seal is possible; DPI usually still too demanding |
| 6 years and over | Dry-powder inhaler, or continued pMDI plus spacer | One sharp, deep inhalation then a breath-hold for a DPI | Guided by inspiratory flow and technique, not age alone |
| 12 years and over | Any device — DPI, SMI, pMDI plus spacer | Device-specific, with attention to adherence | Choice driven by adherence, discretion and preference; technique still re-taught |
| Acute severe asthma | pMDI plus spacer for most; oxygen-driven nebuliser if hypoxic or unable to coordinate | Tidal breathing through spacer or mask | Spacer at least as effective as nebuliser with fewer side-effects; never withhold oxygen |
Two teaching rules run alongside the ladder. Teach, demonstrate, and have the child return the demonstration at every visit — written instructions alone do not change technique. And manage the corticosteroid safely: after an inhaled corticosteroid the child rinses and spits to prevent oral candidiasis and hoarseness, and the long-term safety of adding a long-acting beta-agonist to an inhaled corticosteroid in children is established only when the corticosteroid is continued alongside it. [2] [11]
Specific Subtypes & Scenarios
The infant with viral wheeze is the commonest scenario, and the trap is to give salbutamol by a device that cannot deliver it. A pressurised inhaler through a small-volume spacer with a mask, the mask held firmly through the crying, delivers far more drug than a loose mask or a bare inhaler. Where the infant will not tolerate the mask awake, aerosol delivery to a sleeping infant is feasible, though it is a specialist manoeuvre rather than a routine. [8] [9]
The child with severe acute asthma in the emergency department is the scenario where the spacer-versus-nebuliser evidence is most useful. For most children, salbutamol and ipratropium by inhaler and spacer match or exceed the nebuliser, with fewer systemic side-effects; oxygen-driven nebulisation is reserved for the hypoxic or exhausted child who cannot take the spacer. The reliever should be repeated over the first hour and the response judged clinically and, where possible, by oximetry and spirometry. [5] [6]
The technology-dependent child — the infant with chronic lung disease on home oxygen, or the child with neuromuscular weakness — may need a nebuliser or a spacer adapted to a tracheostomy or a ventilator circuit, in partnership with the respiratory team. The child in a remote setting depends even more on a spacer, because a pressurised inhaler and a plastic chamber are cheap, portable, and need neither power nor oxygen to work, which makes them the practical first choice where retrieval is hours away. [3] [8]
The adolescent in transition is the subtype where device choice becomes a conversation about adherence and independence. A dry-powder preventer taken once daily may rescue a teenager whose spacer sits unused, and the device handover to adult care is the moment to re-teach technique rather than assume it. [4] [11]
Complications & Pitfalls
The complications of inhaled therapy divide into those of the drug and those of the device. The drug side-effects are well known and mostly local: oral candidiasis and hoarseness from an inhaled corticosteroid, prevented by rinsing and spitting and by using a spacer; tremor, tachycardia and hypokalaemia from high-dose salbutamol, more frequent with nebulised than spacer-delivered reliever in acute attacks. The systemic safety of inhaled corticosteroids at standard doses in children is good, with small and reversible effects on growth that do not compromise final adult height. [10] [11]
The device pitfalls are where the examiner lives. A mask that does not seal is the commonest reason a spacer dose fails in an infant, because the aerosol escapes around the mask instead of entering the airway. A static or unprimed plastic spacer attracts the drug to its walls; prime a new spacer with several wasted actuations and wash it in detergent without rinsing or wiping to suppress static, or use a metal chamber that carries no charge. A dry-powder inhaler given to a child who cannot generate the flow delivers almost nothing, and a DPI breathed into rather than out of clogs the mechanism. Technique drift erodes good control over months and is the reason a technique check belongs at every visit. And treating the number of puffs rather than the delivery — escalating a preventer when the real problem is a loose mask — is the classic error of confusing dose with exposure. [1] [3]
Prognosis & Disposition
When the device is right and the technique is taught and re-taught, the prognosis of inhaled therapy in children is excellent. Spacer-delivered salbutamol shortens the emergency stay and reduces side-effects in acute asthma, and a correctly matched preventer device restores control in the child whose asthma seemed refractory. The disposition turns on the technique check: a child discharged with a spacer and a taught technique, with a written action plan and a review booked, does far better than one sent out with a canister and an assumption. [5] [3]
The device is also where the long-term relationship with the disease is built. A child who learns, at the right age, that an inhaler is not a single object but a ladder they climb as they grow, comes to asthma self-management already understanding the principle of matching the tool to the body. Re-teaching the technique at every visit, stepping the device as the child grows, and reviewing the choice at adolescence and at transition to adult care, is what keeps an inhaled drug working across the whole of childhood. [2] [4]
Special Populations
The Indigenous child and the child in a remote community is the population for whom the spacer matters most. A pressurised inhaler and a valved holding chamber are inexpensive, need no power, and travel well, so they are the practical backbone of both acute and preventer therapy where oxygen cylinders and nebuliser compressors are scarce and retrieval is distant. Coordinating spacer supply through the primary-care medical home and the school, in partnership with Aboriginal health workers, is part of closing the gap in asthma outcomes. [3]
The child with disability or neurodiversity may struggle with the coordination of any device that demands a timed or forceful breath, and benefits from a spacer that allows tidal breathing, a mask adapted to the face, or a nebuliser where cooperation is limited. The technology-dependent child on home oxygen or a ventilator needs the respiratory team to adapt the delivery to the circuit, whether by a spacer adapted to a tracheostomy or nebulised drug in the ventilator line. And the child from a family with limited health literacy or for whom English is an additional language needs the technique demonstrated, not merely described, with the teach-back method confirming the family can reproduce the dose. [8] [9]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric inhaled device selection is strong on the questions that matter most. The Cochrane review of holding chambers versus nebulisers for beta-agonist treatment of acute asthma established that a spacer is at least as effective as a nebuliser for most children, with fewer side-effects, and randomised trials in severe exacerbations have shown the inhaler-and-spacer route to be superior. [5] [6] The Aerosol Drug Management Improvement Team (ADMIT) series on inhaler selection in children, and the matching-the-device review by van Aalderen and colleagues, set out the age-based ladder, while a recent systematic review has examined dry-powder inhaler use in primary-school-aged children and confirmed that technique and inspiratory flow, more than age alone, decide suitability. [2] [3] [4]
The regional differences are in how the guidance is organised, not in the underlying physics. The Australian Asthma Handbook and the Royal Children's Hospital Melbourne guideline are the primary references in Australasia and set the age-stratified reliever doses and the spacer-first stance. In the United Kingdom the BNF for Children and the BTS/SIGN asthma guideline give equivalent device advice and dosing. The Global Initiative for Asthma (GINA) strategy frames device choice within the overall stepwise controller strategy and is the global reference. The aerosol-physics consensus from the American College of Chest Physicians and the American College of Asthma, Allergy, and Immunology underpins the device-selection reasoning across regions. [1] [2]
[1] [3]The controversies are narrow but real. The exact age at which a child can move from a mask to a mouthpiece, or from a spacer to a dry-powder inhaler, is a clinical judgement of the individual child's flow and coordination rather than a fixed birthday. The role of the nebuliser in acute asthma has narrowed as the spacer evidence has grown, but it persists for the hypoxic or uncooperative child and for high-flow oxygen-driven delivery. These are decisions for the bedside, verified against the current local guideline. [5] [4]
Exam Pearls
Hold the device ladder as a single sentence and you hold the topic. Under four, a spacer with a mask; four to six, a spacer with a mouthpiece; from school age, a dry-powder inhaler or a continued spacer; in adolescence, any device matched to flow and adherence. A spacer is not an accessory — it is the device that makes a pressurised inhaler work in a child, by slowing and suspending the cloud so that respirable particles reach the lung. [1] [3]
Defend the three highest-yield facts at viva. First, salbutamol by pMDI and spacer is at least as effective as the nebuliser for most acute asthma in children, with fewer side-effects and a shorter emergency stay; reserve the oxygen-driven nebuliser for the hypoxic or uncooperative child. [5] [6] Second, a dry-powder inhaler needs a fast, deep breath, so it belongs to the school-age child who can generate the inspiratory flow, never the toddler. [2] [4] Third, the commonest reason an inhaled corticosteroid "fails" is not the dose but the delivery — a loose mask, an unprimed or static spacer, or technique that has drifted — so check the technique before you escalate the drug. [1] [3]
References
- [1]Dolovich, MB; Ahrens, RC; Hess, DR Device selection and outcomes of aerosol therapy: Evidence-based guidelines: American College of Chest Physicians/American College of Asthma, Allergy, and Immunology. Chest, 2005.PMID 15654001
- [2]Pedersen, S; Dubus, JC; Crompton, GK The ADMIT series--issues in inhalation therapy. 5) Inhaler selection in children with asthma. Primary Care Respiratory Journal, 2010.PMID 20640390
- [3]van Aalderen, WM; Garcia-Marcos, L; Gappa, M How to match the optimal currently available inhaler device to an individual child with asthma or recurrent wheeze. NPJ Primary Care Respiratory Medicine, 2015.PMID 25568979
- [4]Kuek, SL; Wong, NX; Dalziel, S Dry-powder inhaler use in primary school-aged children with asthma: a systematic review. ERJ Open Research, 2024.PMID 39655170
- [5]Cates, CJ; Welsh, EJ; Rowe, BH Holding chambers (spacers) versus nebulisers for beta-agonist treatment of acute asthma. Cochrane Database of Systematic Reviews, 2013.PMID 24037768
- [6]Iramain, R; Castro-Rodriguez, JA; Jara, A Salbutamol and ipratropium by inhaler is superior to nebulizer in children with severe acute asthma exacerbation: Randomized clinical trial. Pediatric Pulmonology, 2019.PMID 30672140
- [7]Sugiura, K; Hagiwara, Y; Nomura, O Procaterol via nebulizer versus metered-dose inhaler with a spacer for acute asthma exacerbation in children. Pediatrics International, 2025.PMID 40365987
- [8]Amirav, I; Newhouse, MT Aerosol therapy in infants and toddlers: past, present and future. Expert Review of Respiratory Medicine, 2008.PMID 20477295
- [9]Amirav, I; Newhouse, MT; Luder, A Feasibility of aerosol drug delivery to sleeping infants: a prospective observational study. BMJ Open, 2014.PMID 24670428
- [10]Williams, DM; Rubin, BK Clinical Pharmacology of Bronchodilator Medications. Respiratory Care, 2018.PMID 29794201
- [11]Stempel, DA; Szefler, SJ; Pedersen, S Safety of Adding Salmeterol to Fluticasone Propionate in Children with Asthma. New England Journal of Medicine, 2016.PMID 27579634