Paeds · clinical-pharmacology-and-therapeutics
Medication adherence and formulation challenges
Also known as Paediatric medication adherence · Compliance and concordance in children · Palatability and taste of children's medicines · Age-appropriate paediatric formulations · Liquid, chewable and mini-tablet formulations in children
Fellowship guide to medication adherence and formulation challenges in children: why adherence is the prescriber's job, the dimensions of non-adherence (initiation, implementation, persistence), the formulation gap and palatability science, age-appropriate formulations (liquids, chewable and dispersible tablets, mini-tablets), excipient safety in neonates, the bedside assessment of adherence barriers, the stepwise formulation-and-adherence management pathway, and the regional initiatives (STEP database, paediatric investigation plans) closing the formulation gap.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A registrar in a paediatric nephrology clinic sees a 6-year-old renal transplant recipient whose tacrolimus levels have been bouncing unpredictably for months. The dose is correct, the family understands the diagnosis, but the child spits out the bitter liquid and the half-tablets crumble. The registrar reaches for "non-adherence" as the label. This leaf owns that moment — medication adherence and formulation challenges — and reframes it from a failing of the child into a property of the prescribing that the prescriber can fix. The broader pharmacology, off-label use and pharmacovigilance theory lives on its own leaves; this page is about the swallow, the taste and the daily reality of taking medicine as a child. [1] [6]
Hold three words apart, because examiners live in the gaps between them. Adherence is the extent to which a person's medicine-taking behaviour corresponds to the agreed recommendations; it is shared, negotiated and behavioural. Compliance is the older term that implied the patient obeys the prescriber — it is now discouraged precisely because it frames the child or family as the problem. Persistence is the length of time a patient continues to take the medicine before stopping; it is a separate dimension from day-to-day implementation. The ABC taxonomy used in adult and paediatric research separates adherence into initiation (taking the first dose), implementation (taking it as prescribed over time) and discontinuation (stopping); non-adherence can sit in any one of these. [2]
The reason this framing matters clinically is that the formulation is half of adherence. A child cannot be adherent to a tablet they cannot swallow, a liquid that makes them vomit, or a regimen so complex that no family can sustain it. Nunn and Richey's 2005 British Journal of Clinical Pharmacology paper set out the paediatric formulation gap and remains the canonical reference; it is the paper to name at viva. The rest of this page is about closing that gap at the bedside. [1] [3]
Classification
Classify along the axis the examiner expects: which dimension of adherence is failing, because each carries a different intervention. Initiation non-adherence means the child never starts — the prescription is not filled, the first dose is never given, often a hidden problem in newly diagnosed chronic disease. Implementation non-adherence is the day-to-day pattern — missed doses, wrong timing, dose omissions during intercurrent illness, "drug holidays". Discontinuation (or non-persistence) means the child stops taking the medicine altogether before the agreed end — common in adolescence, after symptom resolution, or when the family loses faith in the treatment. [2] [12]
The second axis is whether the barrier sits in the formulation, the regimen, or the child and family. A formulation barrier is a medicine that is physically hard to take — too bitter, too large, the wrong strength, only available as a tablet when the child needs a liquid. A regimen barrier is a dosing schedule a family cannot sustain — four-times-daily liquids, multiple drugs, doses timed to school hours. A child-and-family barrier sits in development, neurodiversity, sensory aversion, health literacy, family stress, or beliefs about the medicine. Most real non-adherence has all three layers, and the assessment is about disentangling them. [2] [3]
Three dimensions of adherence at a glance
- Does the child ever take the first dose?
- Hidden in newly diagnosed chronic disease
- Prescription filled, first dose given, plan understood
- Intervention: structured start, education, first-dose follow-up
- Day-to-day dosing as prescribed
- Missed doses, wrong timing, drug holidays
- The most common form of non-adherence
- Intervention: simplify regimen, dosing aids, reminders
- Child stops the medicine before the agreed end
- Peak in adolescence and after symptom relief
- Persistence over time
- Intervention: review rationale, transition support, ongoing relationship
Epidemiology & Risk Factors
The numbers behind paediatric adherence are sobering and consistent across chronic diseases. The headline figure candidates should know is that non-adherence to long-term medicines in children and adolescents is common, frequently around half or more of patients, with the highest rates of poor adherence in adolescence, in complex regimens, and in conditions where the medicine is asymptomatic or its benefit is long-term. Dean and colleagues' 2010 systematic review in Archives of Disease in Childhood — the canonical paediatric adherence review — synthesised interventions to enhance medication adherence in children and adolescents with chronic illness, and found that no single intervention type reliably solved adherence, that effect sizes were modest, and that combined behavioural and educational approaches outperformed education alone. [2]
The pattern reproduces across disease groups. In severe mental illness, Edgcomb and colleagues' 2018 meta-analysis found similarly high non-adherence, with adolescence, stigma, complex regimens and side-effects driving the signal; the same is reported for epilepsy, asthma, sickle cell disease, HIV, transplant, and inflammatory bowel disease. The consistency is the point — non-adherence is a property of the prescribing and the developmental stage, not of any one disease, and that is why the formulation-and-adherence intervention is generic across conditions. [12]
Risk concentrates wherever development, complexity and formulation meet. The youngest children (infants and toddlers) struggle because they cannot swallow tablets and are exquisitely bitter-sensitive; school-age children struggle when regimens interrupt school; adolescents struggle with identity, autonomy, peer stigma and the shift to self-management; children with medical complexity and technology dependence struggle with polypharmacy and enteral-tube administration. A bitter or large-volume liquid, a four-times-daily schedule, and an asymptomatic disease are the structural risk triad. [2] [12]
Pathophysiology
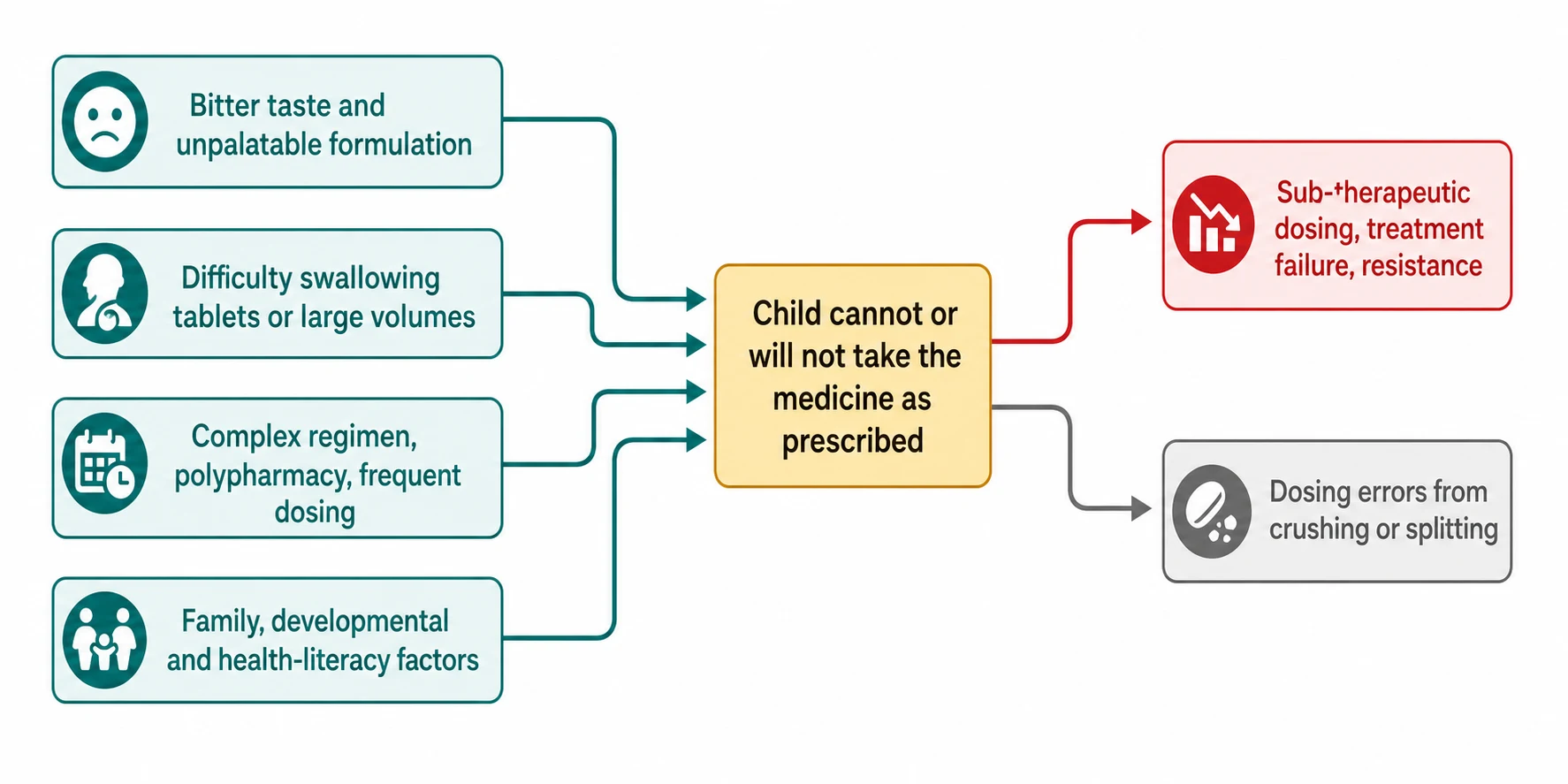
There is no single disease mechanism here — the mechanism is a mismatch between the medicine and the child, and understanding it is half the viva. Four drivers converge on a single node: the child cannot or will not take the medicine as prescribed. [1] [3]
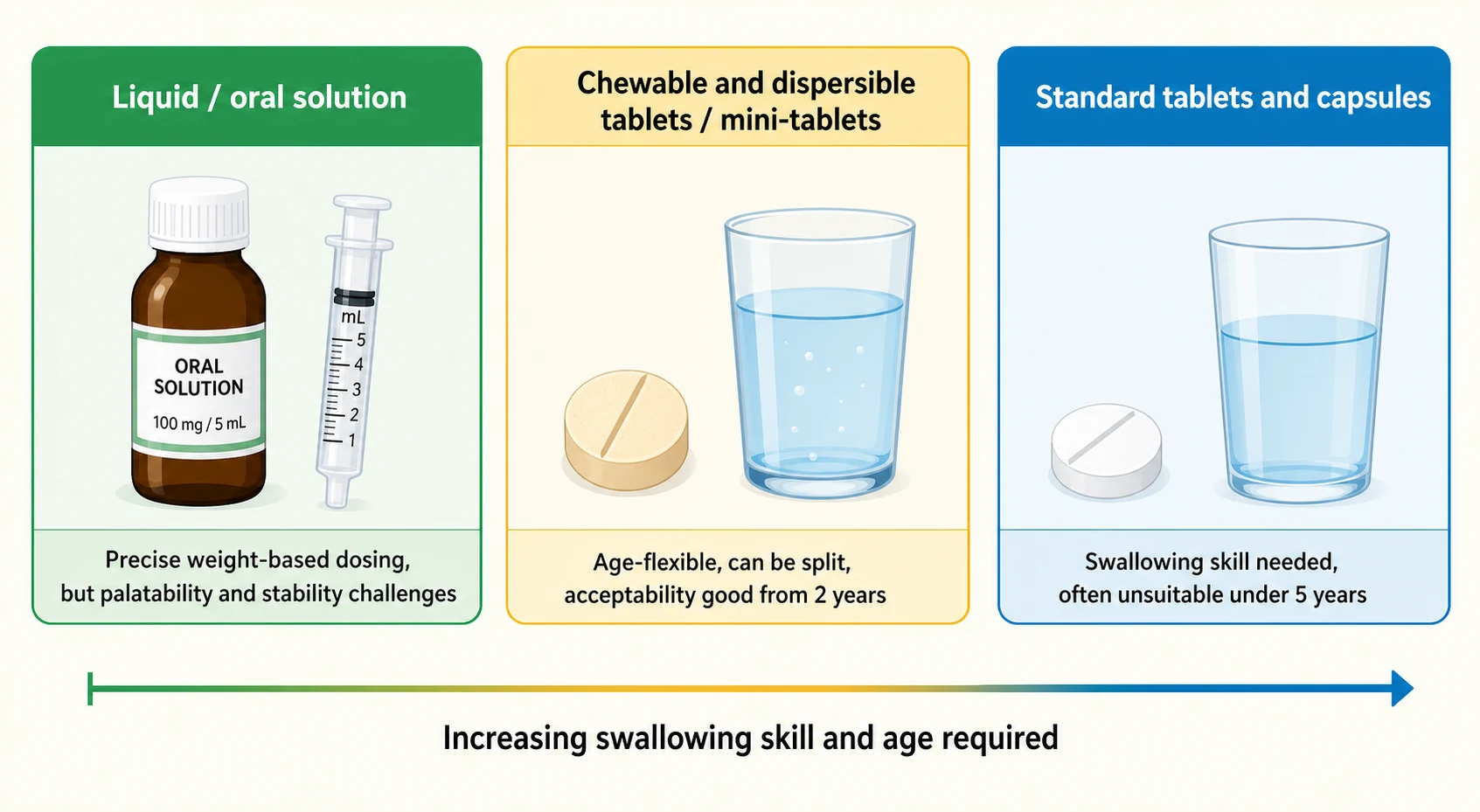
The first driver is taste and palatability. Children are not small adults in taste — they are biologically more sensitive to bitter compounds, an evolutionary protection against poisoning, and most active pharmaceutical ingredients are intensely bitter. Mennella's body of work (Clin Ther 2008 overview and 2013 review of bitter-taste basic science) set out the developmental biology: children live in a more intense sensory world, prefer sweet and salty, reject bitter, and cannot be reasoned out of a taste aversion. A liquid that an adult tolerates may be genuinely untakeable for a two-year-old. [3] [4]
The second driver is swallowing ability and developmental readiness. Safe swallowing of a standard tablet is a developmental skill that most children acquire somewhere around five to six years, but with wide variability, and mini-tablets (2 mm) are swallowable by many children from about two years. Münch and colleagues' 2023 evaluation of film-coated mini-tablets, and the cross-over work on chewable and dispersible formulations, have changed what "age-appropriate" means: the answer is no longer "always give a liquid". [9] [10]
The third driver is the regimen. Adherence falls as the number of daily doses rises — a twice-daily regimen outperforms four-times-daily, and once-daily outperforms both when it exists. Polypharmacy, timed doses during school hours, medicines that need refrigeration, and medicines that interact with food or enteral feeds all raise the implementation burden. [2]
The fourth driver is excipient safety, which is its own physiology in the youngest children. Neonates and young infants handle excipients differently from adults because of immature hepatic metabolism and renal clearance, and several excipients tolerated in older children are unsafe in neonates — benzyl alcohol, propylene glycol and ethanol are the classical offenders. Allegaert's 2013 papers on tailored neonatal formulations, and the STEP (Safety and Toxicity of Excipients for Paediatrics) database launched by Salunke and colleagues in 2013, are the named frameworks that have begun to systematise excipient safety in paediatric formulations. The principle for the prescriber: in a neonate, check the excipients before you choose the formulation. [5] [6]
Clinical Presentation
Non-adherence rarely presents as a complaint in the way a cough or a fever does. It surfaces at four predictable moments, and recognising them is the clinical skill. [2]
The first is the uncontrolled chronic disease. A child whose asthma, epilepsy, sickle cell disease, transplant rejection risk, HIV or inflammatory bowel disease is flaring despite a "correct" prescription is a child in whom adherence must be openly assessed before the regimen is escalated — escalating a non-adherent child simply layers toxicity on top of under-treatment. The second is the erratic drug level: a tacrolimus, phenytoin or antiretroviral level that swings without a change in dose is a near-pathognomonic sign of intermittent dosing, and chasing the level with dose changes is a common and harmful error. The third is the family voice: a parent who reports that the child spits out the medicine, vomits after the dose, refuses at school, or whose behaviour deteriorates around medicine-time is telling you the formulation is the barrier. The fourth is the routine clinic visit, where the single best question — how does your child actually take this medicine? — surfaces non-adherence that no other assessment will. [2] [12]
A useful bedside mindset: at every chronic-disease review, run the adherence question in the background, and treat erratic disease control or erratic levels as adherence-until-proven-otherwise rather than as a pharmacology puzzle. [2]
Differential Diagnosis
When a child's disease is uncontrolled or a drug level is erratic, the diagnostic question is which kind of non-adherence or formulation problem is this, because the intervention follows the cause. [2]
- Adherence failure versus true pharmacotherapy failure. Adherence must be assessed before the regimen is escalated; a non-adherent child mislabelled as a treatment failure will accumulate escalating toxicity without benefit. The first move is always to ask openly. [2]
- Formulation barrier versus regimen barrier versus family barrier. Is the child unable to take the formulation (palatability, swallowing, volume), unable to sustain the regimen (frequency, complexity, school), or is the barrier in the family system (beliefs, health literacy, stress)? [3]
- Bitter-taste rejection versus swallowing difficulty. A young child may vomit a bitter liquid (taste) or refuse a tablet (swallowing); the formulations that solve each differ — taste-masked liquid or chewable for the first, mini-tablet or dispersible for the second. [3] [9]
- Excipient intolerance versus active-drug adverse effect. A neonate on a benzyl-alcohol-containing formulation may be reacting to the excipient, not the drug; a child on a sorbitol-containing liquid may have osmotic diarrhoea from the excipient. [5] [6]
- True non-adherence versus "white-coat adherence". Refill records and self-report can both over-state adherence around the clinic visit; the most reliable signal is an objective marker — drug level, disease biomarker, or electronic monitoring. [2]
Clinical & Bedside Assessment
At any chronic-disease visit, the bedside assessment is a short, repeatable check that turns the adherence question into a formulation-and-regimen decision. Weigh the child in kilograms — every paediatric dose is weight-based, and growth changes the dose over time, so a "stable" dose quietly becomes sub-therapeutic as the child grows. Then ask the single best question: how does your child actually take this medicine? Do not ask do they take it? — that invites a socially desirable "yes". [2]
Then run the four-point formulation check. First, can the child take the formulation they have been given? A tablet for a four-year-old, a bitter liquid for a toddler, a large volume for a child with reflux, are all formulation barriers. Second, is there an age-appropriate alternative? A chewable, dispersible, mini-tablet or taste-masked liquid may exist where none did a year ago; formularies change. Third, can the regimen be simplified? A once- or twice-daily long-acting preparation often outperforms a four-times-daily immediate-release one. Fourth, what is the family's experience? Beliefs about the medicine, side-effects, taste, school logistics, and the child's developmental stage all shape implementation. [2] [3]
The formulation check at the bedside
Investigations
There is no laboratory test for "non-adherence" — it is a clinical and behavioural classification made by open questioning, ideally triangulated with an objective marker. The investigations this topic asks for are objective adherence markers, formulation checks, and drug-level interpretation, and each carries more weight when adherence is uncertain. [2]
For objective markers, therapeutic drug monitoring is the most powerful: a tacrolimus, phenytoin, carbamazepine, valproate, or antiretroviral level that is unexpectedly low or erratic in a child on a stable dose is a strong signal of non-adherence, and chasing the level with dose escalation is the classic error. Disease biomarkers — HIV viral load, HbA1c in diabetes, inflammatory markers in inflammatory bowel disease, blood pressure in hypertension — carry the same logic. Electronic monitoring devices (smart inhalers, smart bottles) are the most accurate research-grade tool and are increasingly used clinically; pharmacy refill records are a useful proxy when available. Each method has limits, so triangulate. [2]
For the formulation check, the prescriber's investigation is to ask the pharmacist three questions: is there a licensed paediatric liquid, a chewable or dispersible tablet, or a mini-tablet at a strength that allows weight-based dosing? what are the excipients, and are they safe for this child's age (especially in neonates)? and what is the stability of any extemporaneously compounded or split preparation? The STEP database is the named reference for excipient safety. [5] [6]
Management — Resuscitation
There is no resuscitation for adherence itself, but there is one acute adherence-related scenario where resuscitation thinking applies: the child who presents in crisis because of non-adherence to a life-saving medicine — status epilepticus from missed anticonvulsants, diabetic ketoacidosis from missed insulin, acute chest syndrome from missed sickle-cell prophylaxis, or acute graft rejection from missed immunosuppression. The rule is the same as elsewhere: treat the acute crisis first; assess and fix the adherence afterwards. [2]
- Resuscitate the child — airway, breathing, circulation; treat the acute complication with standard protocols (status epilepticus, diabetic ketoacidosis, acute chest syndrome, acute rejection) and call for senior help. [2]
- Do not blame the child or family in the acute moment. The crisis is a medical emergency; the adherence conversation belongs in the recovery or outpatient phase, run openly and without judgement. [2]
- Avoid the trap of escalating the chronic dose after a non-adherence-driven crisis. Doubling the anticonvulsant or insulin dose after a crisis driven by missed doses produces toxicity once the child (briefly) becomes adherent — re-establish adherence first, then re-titrate. [2]
Management — Definitive & Stepwise
The definitive management of adherence is a formulation-and-adherence pathway, not a single prescription. It is the sequence you run at every chronic-disease visit, and it is the backbone of a fellowship answer. Six steps, in order. [2] [1]

Step 1 — Assess current adherence, openly and without blame. Ask how does your child actually take this medicine? — not do they take it? Triangulate with an objective marker (drug level, disease biomarker, refill record) where possible. The goal is a shared, accurate picture, not a confession. [2]
Step 2 — Identify the barrier. Is the barrier in the formulation (palatability, swallowing, volume, strength), the regimen (frequency, complexity, school hours), or the child and family (development, neurodiversity, sensory aversion, beliefs, health literacy, family stress)? Most real non-adherence has more than one layer; name them all. [2] [3]
Step 3 — Match the formulation to the child. This is where the modern formulation science earns its place. For infants and toddlers, prefer a palatable, taste-masked liquid, a dispersible tablet, or increasingly a mini-tablet (2 mm) which many young children can swallow from about two years — Münch and colleagues' 2023 mini-tablet work is the named evidence. For preschool and young school-age children, chewable and dispersible tablets are often the best bridge — Palmeirim's 2020 chewable-mebendazole trial and Perez's 2021 chewable-mebendazole acceptability study in 2-to-4-year-olds are the named examples. For older school-age children and adolescents, a standard tablet or capsule is usually fine once swallowing is reliable, and a long-acting once-daily form often beats a short-acting three-times-daily one. Choose the formulation the child can actually take, not the one the prescriber finds easiest to write. [7] [9] [10]
Step 4 — Simplify the regimen and support memory. Prefer once- or twice-daily over four-times-daily where an equivalent long-acting option exists; reduce the number of medicines where possible; align doses with daily routines (mealtimes, tooth-brushing); provide dosing aids (oral syringes, pill boxes, calendars) and consider reminders (alarms, apps). Haslund-Krog's 2022 prednisolone cross-over study is a clean example of how the formulation alone — without changing the drug — measurably improves acceptability in children. [8]
Step 5 — Counsel the child and family. Teach tablet-swallowing technique (there are validated behavioural protocols), offer taste-masking strategies (chilling the liquid, following with a preferred drink, using a coated formulation), explain the rationale in plain language, and invite questions. For an older child or adolescent, the conversation is with them, not just the parent — autonomy over medicine-taking predicts adherence. [2] [9]
Step 6 — Review and reinforce. Adherence is not a one-off fix; re-assess it at every visit, adjust the formulation as the child grows, and treat the chronic-disease relationship as the long-term substrate of adherence. [2]
High-risk medicines: extra steps
Identify the high-risk feature: narrow therapeutic index, transplant immunosuppressant, anticonvulsant, antiretroviral, or adolescent on self-management
Triangulate adherence with an objective marker at every visit — drug level, disease biomarker, refill record
Involve the pharmacist for formulation choice, excipient check and extemporaneous-compounding stability
Pre-plan transitions (ward to home, paediatric to adult) with explicit adherence handover
Offer behavioural support early; do not wait for a crisis to escalate to specialist adherence services
Specific Subtypes & Scenarios
Different settings and diseases concentrate adherence problems differently, and examiners test the contrast. [2]
Neonates and young infants carry the formulation problem in its purest form. The excipient-safety question dominates — benzyl alcohol, propylene glycol and ethanol in adult or older-child formulations can cause real harm in a neonate — and Allegaert's 2013 papers and the STEP database are the named responses. Dilution maths, extemporaneous compounding, and enteral-tube administration all raise the implementation burden, and the formulation choice is a pharmacist conversation, not a registrar reflex. [5] [6]
Toddlers and preschool children are the palatability and swallowing frontier. They cannot take standard tablets, they are biologically bitter-sensitive, and they often refuse large-volume or foul-tasting liquids. The modern answer is a taste-masked liquid, a dispersible tablet, or a mini-tablet — the chewable-mebendazole and mini-tablet evidence has shifted the default away from "always a liquid". [3] [9]
School-age children struggle most when the regimen collides with school — a midday dose, a medicine needing refrigeration, or one given by a non-trained adult — and simplifying toward before-school and bedtime dosing, or providing a school-approved administration plan, is often the highest-yield move. [2]
Adolescents carry the highest non-adherence prevalence across diseases. Identity, autonomy, peer stigma, side-effects, mental health, and the shift to self-management all conspire; structured transition, an honest conversation about the medicine, long-acting formulations (including long-acting injectables where they exist), and a non-judgemental clinician relationship are the interventions with the best evidence. [12]
Chronic complex disease and transplant bring polypharmacy, narrow therapeutic indices, and lifelong treatment; here adherence is the single biggest determinant of graft survival, viral suppression, or seizure freedom, and objective monitoring plus a specialist pharmacist are standard. [2]
Acute antimicrobial courses are their own adherence problem: short courses of bitter liquids for otitis media, pharyngitis or urinary infection are commonly stopped early once the child feels better. Saito's 2023 review of paediatric oral antimicrobial formulations in Japan is a named example of how formulation choice (taste-masked, once-daily, shorter course) directly improves completion. [11]
Enteral tube administration has its own formulation sub-specialty: not every tablet can be crushed, not every capsule can be opened, and some drugs interact with enteral feeds (phenytoin is the classic). Confirm crushability, bioavailability, and feed interactions with the pharmacist before modifying a formulation for a tube. [1]
Complications & Pitfalls
The complications of adherence failure are mostly clinical consequences of under-treatment and system failures in how we prescribe, and they are where candidates lose marks. [2]
The first pitfall is blaming the child or family. Non-adherence is a property of the prescribing, the formulation and the system, not a moral failing of the family. Asking "why aren't you giving the medicine?" in a tone of judgement closes the conversation and is both a clinical and an exam failure. The second is escalating the dose of a non-adherent child. Doubling an anticonvulsant, insulin, or immunosuppressant after a crisis driven by missed doses produces toxicity once adherence briefly returns; the rule is to re-establish adherence first, then re-titrate. [2]
The third is assuming the formulation is age-appropriate. A tablet for a four-year-old, a bitter liquid for a toddler, or a benzyl-alcohol-containing liquid for a neonate are all formulation failures the prescriber owns. The fourth is crushing tablets or opening capsules without checking. Bioavailability, stability, and feed interactions all change when a formulation is modified; phenytoin and enteral feeds, enteric-coated and modified-release drugs, and cytotoxic handling are the classic traps. [1] [6]
The fifth is ignoring excipient safety in neonates. Benzyl alcohol (gasping syndrome), propylene glycol (hyperosmolality, neurological toxicity), ethanol, and high sorbitol (osmotic diarrhoea) are all well-described paediatric excipient toxicities; the STEP database exists precisely because this is a real and recurring harm. [5] [6]
The sixth is relying on self-report or refill records alone. Both over-estimate adherence, especially around clinic visits ("white-coat adherence"); triangulate with an objective marker — drug level, disease biomarker, electronic monitoring. The seventh is treating adherence as a one-off fix. Adherence drifts with growth, developmental stage, and family circumstances; review it at every chronic-disease visit. [2]
Prognosis & Disposition
For the child, the prognosis is that of the underlying disease and the degree to which the medicine is actually taken — a well-chosen, well-tolerated, simply-regulated medicine taken reliably produces disease control; a "correct" prescription that is not taken produces treatment failure. What adherence changes is the long-term substrate of disease control: graft survival in transplant, viral suppression in HIV, seizure freedom in epilepsy, remission in inflammatory bowel disease, and transplant-free survival in many chronic diseases all track adherence more closely than they track the dose. [2]
At discharge and at every transition, make the formulation and adherence plan explicit. Confirm the community supply (a palatable or chewable alternative may take longer to source), write down the dosing schedule aligned to daily routines, provide dosing aids, and tell the family who to contact and when the next review is. For a child on a narrow-therapeutic-index medicine, plan the objective monitoring schedule and the adherence review into the follow-up. [2]
The longer-term prognosis for the field is that adherence and formulation outcomes will improve as the formulation gap closes — more paediatric liquids, chewables, dispersibles and mini-tablets; safer excipients; longer-acting once-daily options; and better behavioural and digital adherence support. Each well-designed paediatric formulation study (the chewable-mebendazole and mini-tablet trials are the named examples) moves that closure forward by one evidence point. [7] [9]
Special Populations
Neonates and preterm infants sit at the intersection of excipient safety, dilution maths, and the formulation gap. Excipient safety is the first question — check the formulation against the STEP database before prescribing, and prefer formulations free of benzyl alcohol, ethanol and high propylene glycol in neonates. [5] [6]
Children with medical complexity and technology dependence carry polypharmacy and enteral-tube administration; each formulation change needs a crushability, bioavailability and feed-interaction check, and adherence review is part of every encounter. [1]
Children with disability and neurodiversity often have sensory aversions to taste and texture that make standard formulations impossible; a behaviour-informed, taste-masked, low-volume or mini-tablet approach, often with specialist pharmacy and allied-health input, is the right response. [3]
Adolescents carry the highest non-adherence prevalence; structured transition, long-acting formulations, an honest conversation, and a non-judgemental relationship are the evidence-based interventions. [12]
Indigenous, migrant and refugee families may face language, health-literacy, cultural and access barriers; interpreter-mediated explanation of the medicine and its rationale, culturally safe communication, and attention to supply and cost (a palatable formulation that is unaffordable is functionally unavailable) are essential. [2]
Children in out-of-home care and youth justice have consent-authority and continuity-of-care complexities — adherence plans must be explicit about who gives the medicine, who holds the supply, and how information flows across placements. [2]
Children in rural and remote settings meet the supply end of the formulation gap most acutely — a palatable or chewable alternative may take days to arrive, and locally compounded substitutes carry their own stability questions. Plan early and confirm supply. [1]
Evidence, Guidelines & Regional Differences
The regional and regulatory story is about closing the paediatric formulation gap from the top down, with the prescriber and pharmacist doing the bedside work in the meantime. Each region has its own engine, and naming the right one is part of the fellowship answer. [1] [5]
In Australia and Aotearoa New Zealand, the Therapeutic Goods Administration (TGA) regulates medicines, and the Australian Medicines Handbook (AMH) Children's edition and the Royal Children's Hospital Melbourne guidelines are the practical paediatric formulation references. The PBS may constrain which formulation is subsidised, which is a separate (funding) question from which is licensed. Adverse drug reactions, including excipient-related harms, are reported through the Blue Card / Adverse Drug Reaction Reporting scheme. [1]
The STEP (Safety and Toxicity of Excipients for Paediatrics) database, launched by Salunke and colleagues in 2013, is the named cross-regional initiative systematising excipient safety in paediatric formulations; it is the reference to name when asked how excipient safety is being addressed globally. Across all regions the principle is identical: choose the formulation the child can actually take, check the excipients in the youngest children, and report excipient-related harm. [5]
The controversy in the field is whether the regulatory frameworks have delivered enough age-appropriate formulations fast enough. They have unquestionably increased the volume of paediatric formulation development, but they have not eliminated the formulation gap, especially in neonates, in neglected tropical and infectious diseases, and in low-resource settings where the mebendazole chewable work was done precisely because the existing tablet was unsuitable for young children. The honest fellowship answer is that the frameworks are necessary but not sufficient, and that bedside formulation choice and adherence support still do the heavy lifting. [7] [9]
Exam Pearls
- Adherence is shared and behavioural; compliance is the older, discouraged term that implied the patient obeys. Say adherence. [2]
- Adherence has three dimensions — initiation, implementation, persistence. Non-adherence can sit in any one. [2]
- The single best question at any clinic visit is how does your child actually take this medicine? — asked openly and without blame. [2]
- The formulation gap (Nunn 2005) is the structural reason children cannot take many of the medicines prescribed to them; name the paper at viva. [1]
- Children are biologically more bitter-sensitive than adults (Mennella 2008, 2013); a liquid an adult tolerates may be genuinely untakeable for a toddler. [3] [4]
- Mini-tablets (2 mm) are swallowable by many children from about two years; the answer is no longer "always give a liquid" (Münch 2023). [9]
- Chewable and dispersible tablets outperform standard tablets in preschool and young school-age children (Palmeirim 2020; Perez 2021). [7] [10]
- Excipient safety is its own physiology in neonates — benzyl alcohol, propylene glycol and ethanol are the classical offenders; the STEP database (Salunke 2013) is the named reference. [5] [6]
- An erratic drug level in a child on a stable dose is adherence-until-proven-otherwise — do not chase it with dose escalation. [2]
- The stepwise pathway: assess openly, identify the barrier, match the formulation, simplify the regimen, counsel, review and reinforce. [2]
- High-risk medicines (transplant immunosuppressants, anticonvulsants, antiretrovirals) need objective adherence monitoring and specialist pharmacist input at every visit. [2]
- In adolescents, structured transition and long-acting formulations are the best-evidenced adherence interventions (Edgcomb 2018). [12]
References
- [1]Nunn T Formulation of medicines for children. Br J Clin Pharmacol, 2005.PMID 15948931
- [2]Dean AJ A systematic review of interventions to enhance medication adherence in children and adolescents with chronic illness. Arch Dis Child, 2010.PMID 20522463
- [3]Mennella JA Optimizing oral medications for children. Clin Ther, 2008.PMID 19108800
- [4]Mennella JA The bad taste of medicines: overview of basic research on bitter taste. Clin Ther, 2013.PMID 23886820
- [5]Salunke S The STEP (Safety and Toxicity of Excipients for Paediatrics) database: part 2 - the pilot version. Int J Pharm, 2013.PMID 24070789
- [6]Allegaert K Neonates need tailored drug formulations. World J Clin Pediatr, 2013.PMID 25254168
- [7]Palmeirim MS Efficacy, safety and acceptability of a new chewable formulation versus the solid tablet of mebendazole against hookworm infections in children: a randomised controlled trial. EClinicalMedicine, 2020.PMID 33150325
- [8]Haslund-Krog SS Acceptability of Prednisolone in an Open-Label Randomised Cross-Over Study-Focus on Formulation in Children. Children (Basel), 2022.PMID 36010126
- [9]Munch J Evaluating the Acceptability, Swallowability, and Palatability of Film-Coated Mini-Tablet Formulation in Young Children. Pharmaceutics, 2023.PMID 37376177
- [10]Perez F Acceptability of Mebendazole Chewable Tablet in Children Aged 2 to 4 Years in Peru. Pharmaceutics, 2021.PMID 35056923
- [11]Saito J Drug Formulation for Pediatric Oral Antimicrobial Agents in Japan: Current Status, Prospects, and Challenges. Pediatr Infect Dis J, 2023.PMID 37343212
- [12]Edgcomb JB Medication Adherence Among Children and Adolescents with Severe Mental Illness: A Systematic Review and Meta-Analysis. J Child Adolesc Psychopharmacol, 2018.PMID 30040434