Paeds · clinical-pharmacology-and-therapeutics
Off-label and unlicensed medicine use
Also known as Off-label prescribing in children · Unlicensed medicine use in paediatrics · Paediatric specials and compounding · Use of medicines outside the product licence · Paediatric evidence gap
Fellowship guide to off-label and unlicensed medicine use in children: the three prescribing categories, why paediatric prescribing is so often outside the product licence, prevalence across settings, the link with adverse drug reactions, the safe-use governance pathway (licensed alternative, evidence, formulation, documentation, consent, monitoring and reporting), and the regional regulatory frameworks that are closing the paediatric evidence gap.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A registrar on a neonatal unit is asked to start caffeine citrate for apnoea of prematurity. The box is not licensed for the baby's gestational age and the strength on the ward is a pharmacy-made solution. The registrar hesitates. This leaf owns that moment — off-label and unlicensed medicine use — and the reasoning that turns it from a worry into a defensible, child-centred decision. The broader medication-safety and pharmacovigilance theory lives on its own leaves; this page is about the licence. [1] [5]
Hold three words apart, because examiners live in the gaps between them. A licensed (sometimes called on-label) medicine is used within all the terms of its marketing authorisation — the approved age or weight band, the approved indication, route, dose and formulation. An off-label medicine is a licensed product used outside one or more of those terms: the right drug, in a child of the wrong age, or for an unapproved indication, route or dose, or in a formulation that differs from the licensed one. An unlicensed medicine has no valid marketing authorisation for that product or formulation in the country at all — a pharmacy-made "special", an imported product, something extemporaneously compounded, or an investigational product in a clinical trial. [1] [6]
The reason this distinction matters clinically is that each category carries a different governance load. A licensed medicine comes with a regulator-vetted dose range, a tested formulation, and a post-marketing safety database. The moment you step outside the licence you take personal responsibility for the dose, the evidence, the formulation quality and the monitoring — because the regulator's safety net no longer covers that exact use. The rest of this page is about discharging that responsibility well. [7] [5]
Classification
Classify along the axis the examiner expects: which term of the authorisation has been exceeded, because each carries a different evidence and risk profile. The five terms are age (or weight), indication, route, dose, and formulation. An eight-year-old given an adult-licensed antidepressant for an anxiety indication is off-label on age and indication; the same drug given by a route or at a dose not in the licence is off-label on route or dose; a tablet crushed into a suspension because no liquid exists is off-label on formulation — and may also become unlicensed if pharmacy compounds it from raw material rather than a licensed product. [1] [6]
The second axis is whether a licence exists at all. This separates off-label from unlicensed, and it is the single most common point of confusion. Off-label always starts from a product that is licensed somewhere; unlicensed means the product or formulation has no licence in the jurisdiction. The UK captures part of the unlicensed world under the "specials" route — unlicensed medicines manufactured to order under a specials licence when no licensed product meets the patient's need. Extemporaneous compounding (made up on the day, in the pharmacy, from raw ingredients) is a further subset with its own stability and quality questions. [5] [6]
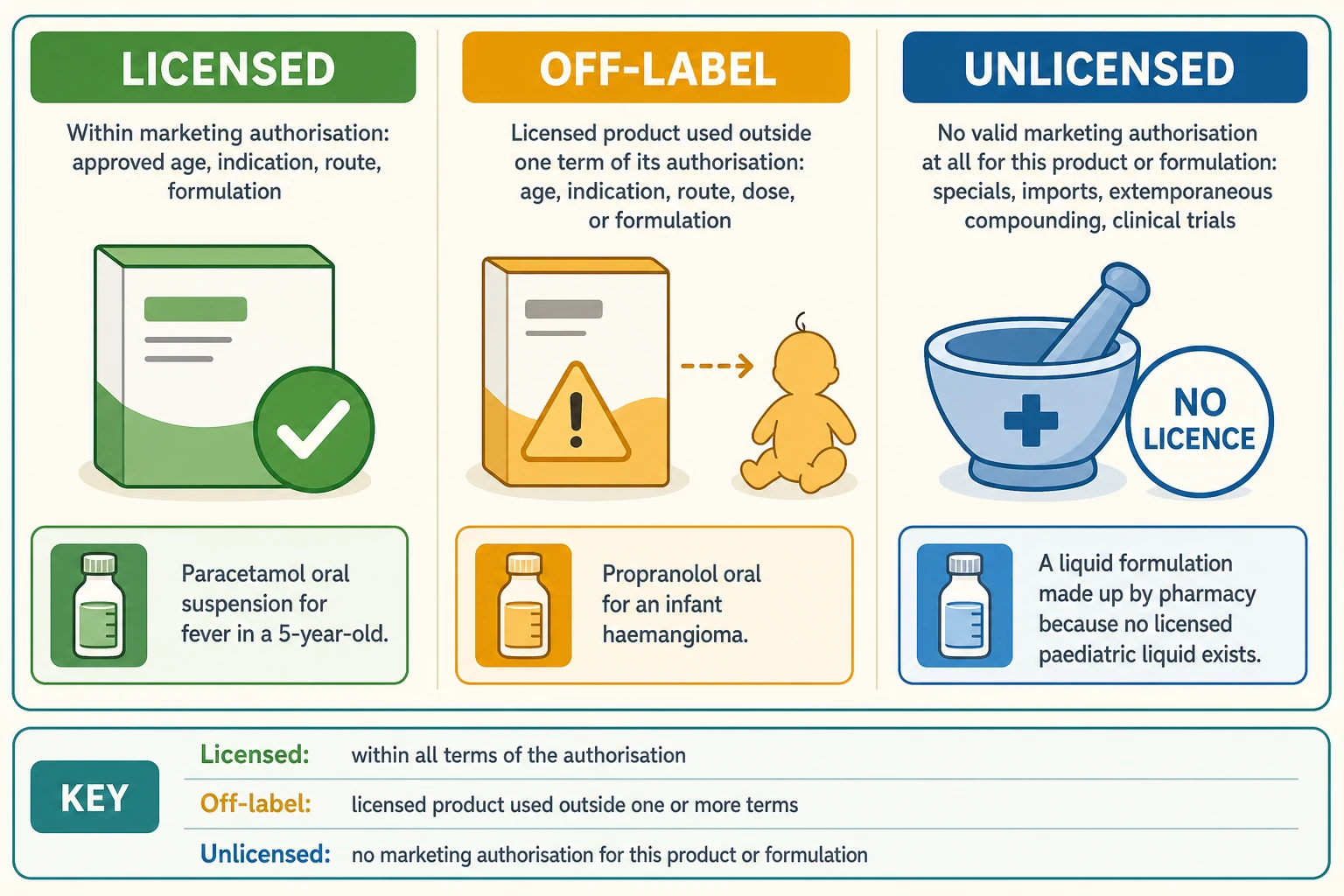
Three prescribing categories at a glance
- Within every term of the marketing authorisation
- Approved age, indication, route, dose, formulation
- Regulator-vetted dose and tested formulation
- Post-marketing safety database applies
- A licensed product used outside one or more terms
- Wrong age or weight, indication, route, dose or formulation
- Product exists and is licensed somewhere
- Prescriber carries the evidence and dose responsibility
- No valid marketing authorisation for the product or formulation
- Specials, imported products, extemporaneous compounding, trials
- Supply chain and quality questions added
- Highest governance load, often Medicines Committee approval
Epidemiology & Risk Factors
The numbers are the answer to the examiner's favourite opening question: how common is this? Conroy's 2000 BMJ survey across European paediatric wards, through the European Network for Drug Investigation in Children, was the landmark — it showed that a substantial proportion of prescriptions on ordinary children's wards were either unlicensed or off-label, and that the proportions rose sharply in the youngest children. 't Jong's 2001 survey of a Dutch children's hospital confirmed the pattern across sub-specialty care, and the 2004 European Respiratory Journal paper showed that even respiratory medicines — bread-and-butter paediatric prescribing — were frequently off-label or unlicensed. [1] [2] [3]
Kimland and Odlind's 2012 review synthesised the field: off-label use is widespread across paediatric age groups and settings, and it is structural rather than accidental. Cuzzolin's 2006 review made the same point across newborns and children in different settings. The intensive-care data are the starkest: Nir-Neuman's 2018 study found that unlicensed and off-label medication use in paediatric and neonatal intensive care units had not fallen over a decade — the children who need the most medicines are still the ones with the least licensed evidence. [6] [5] [9]
Risk concentrates wherever small bodies, narrow therapeutic windows and polypharmacy meet. Neonates and preterm infants top the table, followed by paediatric and neonatal intensive care, oncology, rare disease, and children with medical complexity. Outpatient and primary-care exposure is lower in intensity but enormous in volume — Sohn's 2016 study of US national trends documented high off-label use of atypical antipsychotics in children and adolescents, a reminder that psychotropic and respiratory drug classes drive much of community exposure. [9] [11]
Pathophysiology
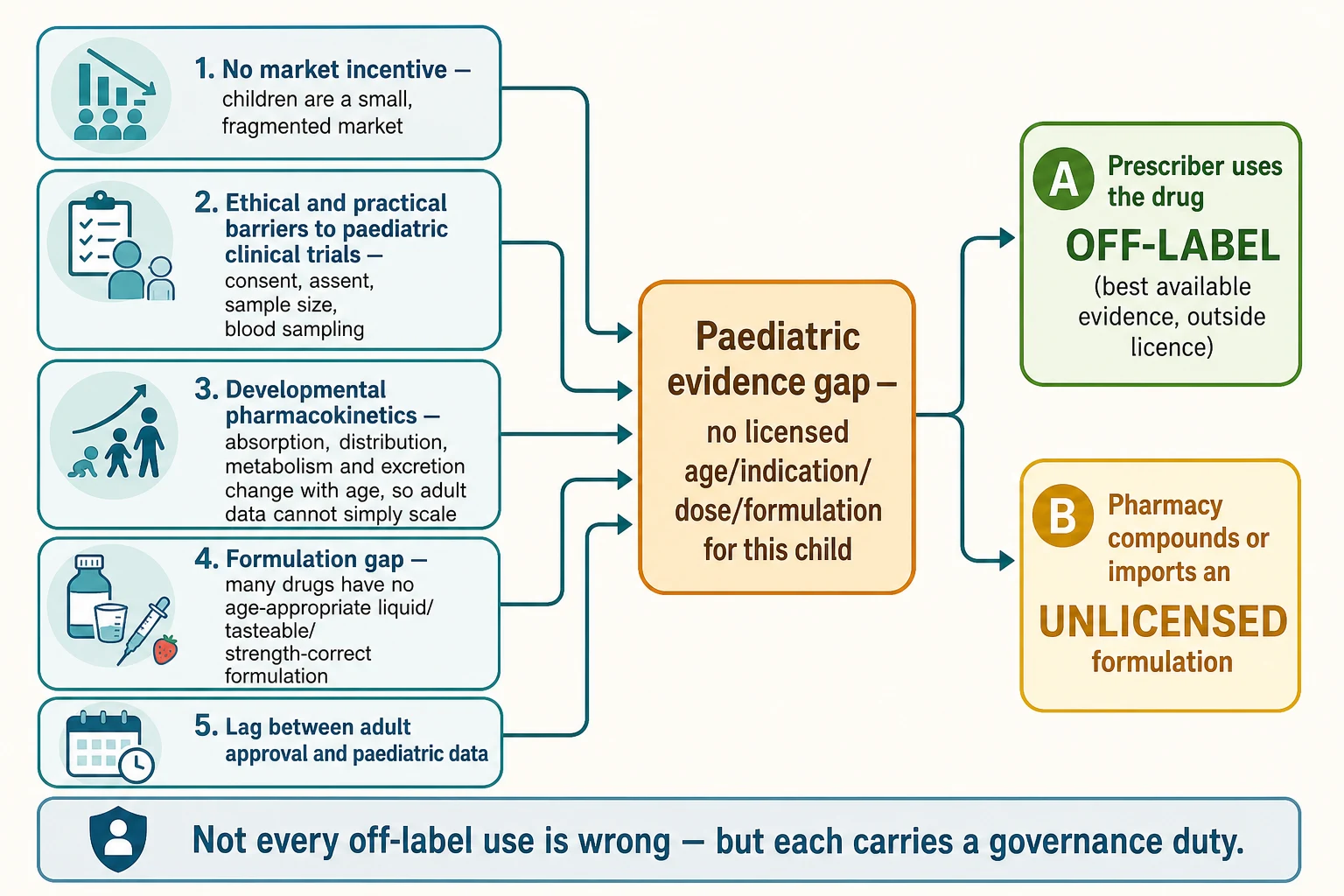
There is no single disease mechanism here — the mechanism is a system gap, and understanding it is half the viva. Five drivers push paediatric prescribing outside the licence, and they converge on one node: the paediatric evidence gap. [6] [10]
The first driver is the market: children are a small, fragmented market split across age bands, so for a manufacturer the return on a paediatric programme is low and the perceived medicolegal risk is high. The second is trial logistics: paediatric trials need consent from parents, assent from children, larger relative blood volumes per sample, and age-stratified cohorts, all of which make them slower and costlier than adult trials. The third is developmental pharmacokinetics: absorption, distribution, metabolism and excretion change with gestational and postnatal age, so an adult dose cannot simply be scaled by weight — and the studies to map those changes often do not exist. The fourth is the formulation gap: many drugs have no age-appropriate liquid, no palatable preparation, and no strength-correct paediatric form, so the child is given a crushed tablet, a split dose, or a pharmacy-made solution. The fifth is regulatory lag: medicines are approved for adults first, and the paediatric licence, if it ever comes, follows years later. [6] [10]
Those five drivers meet at the evidence gap — no licensed age, indication, dose or formulation for this child — and the gap resolves in one of two ways. The prescriber uses a licensed product off-label on the best available evidence, or pharmacy makes or imports an unlicensed formulation. That fork is the whole practical content of this page: it is where governance begins. [5] [7]
Clinical Presentation
Off-label and unlicensed use rarely presents as a complaint in the way sepsis or anaphylaxis does. It surfaces at four predictable moments, and recognising them is the clinical skill. [6] [5]
The first is medicines reconciliation, when you list a child's drugs and notice that several are outside their licence — the morphine infusion in a preterm baby, the propranolol for an infantile haemangioma, the liquid omeprazole made up by pharmacy. The second is the family question: a parent reads the box and asks "why doesn't this say my child's age?" That is a consent and communication trigger, not an error, and it is one of the highest-yield OSCE stems on this topic. The third is the adverse drug reaction: a child on an off-label or unlicensed medicine has a reaction, and because the post-marketing database for that exact use is thin, the reaction must be reported to build the evidence the licence lacks. The fourth is the pharmacy or Medicines Committee alert: the product needs an unlicensed-medicines approval before it can be supplied, or a specials order has to be placed. [8] [12]
A useful bedside mindset: every time you prescribe to a child, run the licence question in the background — is this drug licensed for this child's age, indication, route and dose? If the honest answer is no, the rest of this page is your operating procedure. [6] [5]
Differential Diagnosis
When you encounter a medicine used outside its licence, the diagnostic question is which kind of outside-the-licence use is this, because the governance follows the category. [6] [7]
- Off-label use versus a prescribing error. Off-label is intentional, evidence-based and governed; an error is unintentional and potentially harmful. A two-year-old given an age-appropriate, evidence-based dose of a licensed drug for an unapproved indication is off-label; the same drug given at ten times the dose is an error. The two can coexist — an error can happen on an off-label prescription — but they are not the same thing. [7]
- Off-label versus unlicensed. Ask whether the product itself is licensed somewhere. Propranolol for an infantile haemangioma is off-label (the product is licensed for hypertension in adults). A caffeine solution compounded by the neonatal pharmacy because no licensed preparation is available at that strength is unlicensed. [5]
- Off-label versus a clinical-trial (investigational) product. Routine care outside the licence is governed by your safe-use pathway; an investigational medicinal product is governed by the trial protocol, ethics approval and the research pharmacy. [7]
- Evidence-based off-label versus unsupported off-label. Is the use supported by a guideline, a systematic review or a formulary monograph, or is it a memory-based guess? The governance pathway treats these very differently. [6]
- Unlicensed specials versus extemporaneous compounding versus imported product. Each has a different supply, quality, stability and approval route — specials are made under a specials licence, extemporaneous compounding happens on the day in the pharmacy, and importation draws on another country's licensed product. [5]
Clinical & Bedside Assessment
At any prescribing moment, the bedside assessment is a short, repeatable check that turns the licence question into a decision. Weigh the child in kilograms — not an estimate, not a rounded number — because every paediatric dose is weight-based and a wrong weight silently makes every subsequent calculation wrong. Then confirm the dose against a paediatric reference (the BNFc in the UK, the Australian Medicines Handbook Children's edition, the Royal Children's Hospital Melbourne guidelines, or Neofax for neonates) rather than the adult licence. [7] [5]
Then run the four-point governance check. First, is there a licensed alternative that meets the clinical need and is locally available? If yes, prefer it. Second, what is the evidence behind the proposed off-label or unlicensed use — a guideline, a systematic review, a formulary monograph? Third, is this high-risk? Narrow therapeutic index, neonate or infant, an IV inotrope or sedative, or a compounded formulation all raise the bar. Fourth, what is the local governance status — is the product on the formulary, does it need Medicines Committee approval, is a specials order already in place? [7] [12]
The governance check at the bedside
Investigations
There is no laboratory test for "off-label status" — it is a documentation classification made against the product's licence terms. The investigations this topic asks for are reference and monitoring investigations, both of which carry more weight precisely because the licence does not. [5] [12]
For the reference side, check the local paediatric formulary and the national children's formulary for the evidence base and the recommended paediatric dose; read the summary of product characteristics or product information for the licensed terms; and confirm the local Medicines Committee unlicensed-medicines list for the approval status. For the monitoring side, therapeutic drug monitoring becomes more important, not less, when the dose is uncertain: anticonvulsants such as phenytoin, aminoglycosides such as gentamicin, and vancomycin all need levels read against the paediatric target range, and off-label or unlicensed use is a reason to monitor more closely, not to assume the standard schedule will do. [12]
Plan an adverse drug reaction reporting pathway from the outset. Because the post-marketing safety database for off-label and unlicensed paediatric use is thin, every reaction is informative. Name the scheme you would use: the Yellow Card in the UK, the Blue Card (ADRS) scheme in Australia, MedWatch in the US. Reporting is the single most concrete thing a clinician can do to close the evidence gap the regulator has not. [8] [12]
Management — Resuscitation
There is no resuscitation for the licensing category itself, but an adverse drug reaction or an overdose from an off-label or unlicensed medicine is a real resuscitation scenario, and it has one rule: treat the child first; govern the prescribing afterwards. [8] [4]
- Rescue the child — airway, breathing, circulation; give the reversal agent if one exists (for example naloxone for an opioid, flumazenil where appropriate, glucose for insulin-induced hypoglycaemia); call for senior help. [4]
- Stop the suspect medicine and any medicines that interact with it. [8]
- Escalate to the consultant, the on-call pharmacist and the unit leadership. [8]
- Preserve the product and the documentation — the bottle, the compounded solution, the pump settings, the prescription and the order trail — so the event can be analysed and reported. [12]
- Report the adverse drug reaction to the national pharmacovigilance scheme once the child is stable. [12]
Management — Definitive & Stepwise
The definitive management of off-label and unlicensed use is a governance pathway, not a drug regimen. It is the sequence you run every time the licence does not match the child, and it is the backbone of a fellowship answer. Six steps, in order. [7] [5]
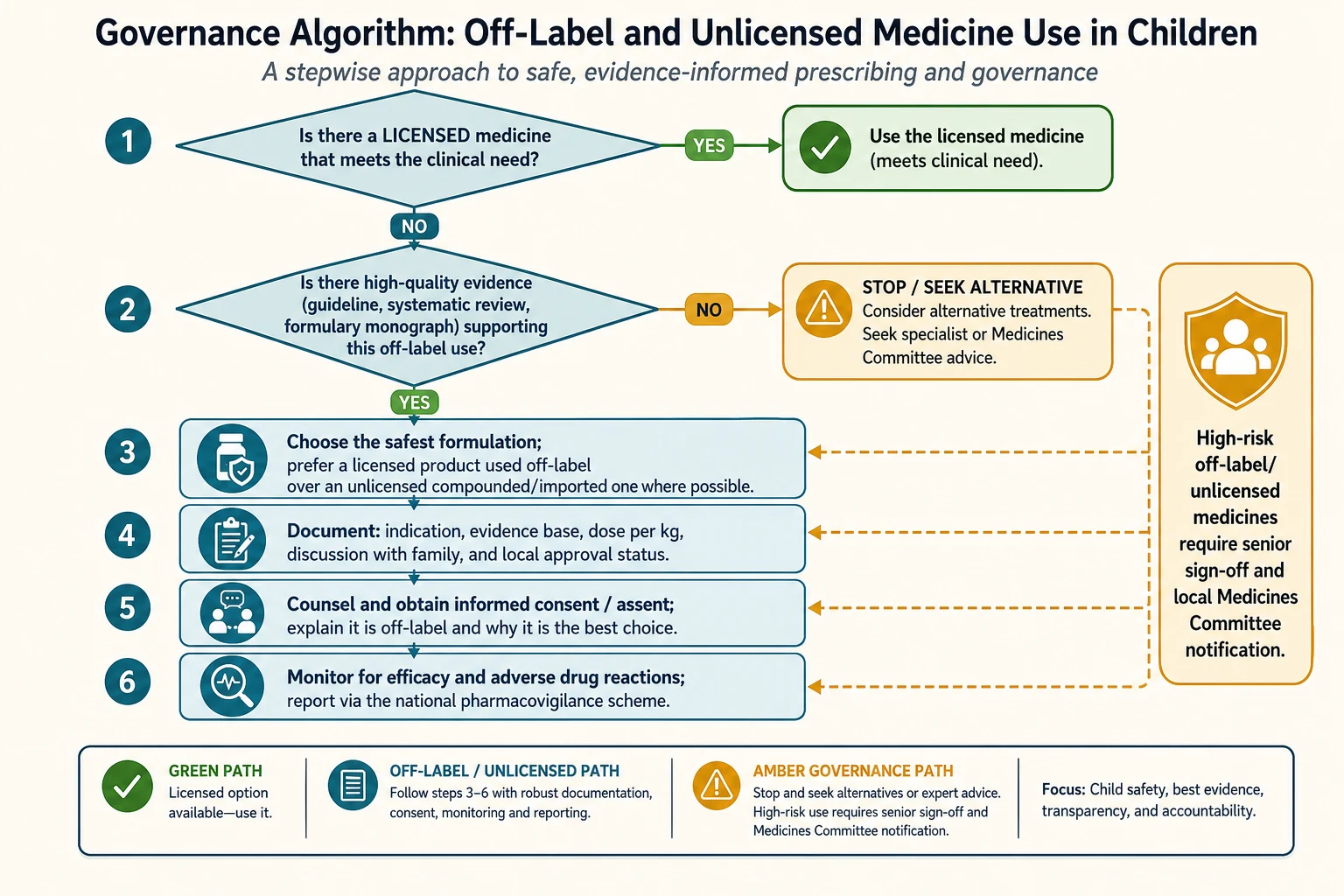
Step 1 — Is there a licensed medicine that meets the clinical need? If a licensed alternative exists and is locally available, use it. This is the single most important step, because licences change and formularies are updated; a drug that was off-label last year may now have a paediatric licence. Always check. [7]
Step 2 — Is there high-quality evidence supporting the off-label use? Look for a guideline, a systematic review, or a formulary monograph. If the evidence is thin, do not prescribe on memory — seek an alternative, or take specialist or Medicines Committee advice. An unsupported off-label prescription is the weakest category and the hardest to defend. [6] [7]
Step 3 — Choose the safest formulation. Prefer a licensed product used off-label over an unlicensed compounded or imported product where possible, because the licensed product carries a tested formulation and a quality-assured supply chain. When compounding or importation is unavoidable, confirm the stability and the strength with the pharmacy. [5]
Step 4 — Document. Record the indication, the evidence base, the weight-based dose, the discussion with the family, and the local approval status. Documentation is what converts an exposed prescriber into a defensible one; without it, you carry the accountability alone. [7]
Step 5 — Counsel and obtain consent (and assent). Tell the child and family, in plain language, that the medicine is being used outside its licence, and explain why it is the best choice for this child. For a competent child or young person, obtain assent as well as parental consent. This is both an ethical duty and a frequent OSCE station. [7]
Step 6 — Monitor and report. Watch for efficacy and adverse drug reactions, and report every reaction through the national pharmacovigilance scheme. Monitoring and reporting are how the paediatric evidence gap slowly closes. [8] [12]
High-risk off-label and unlicensed use
Identify the high-risk features: narrow therapeutic index, neonate or infant, IV inotrope or sedative, or a compounded or imported formulation
Obtain senior sign-off before the first dose
Notify the local Medicines Committee and follow the unlicensed-medicines policy
Confirm stability, strength and supply with the pharmacy
Intensify monitoring and pre-plan the pharmacovigilance report
Specific Subtypes & Scenarios
Different settings concentrate off-label and unlicensed use differently, and examiners test the contrast. [9] [3]
Neonatal and NICU use carries the highest prevalence and the narrowest margin. Preterm infants metabolise and clear drugs unpredictably, dilution maths dominates the prescribing moment, and many formulations are pharmacy-made because no licensed neonatal preparation exists at the required strength. Indomethacin, caffeine, and a range of cardiac and sedative infusions sit in this category. The safe-use pathway is identical, but the stakes — and therefore the monitoring — are higher. [9] [5]
Paediatric and neonatal intensive care shares the NICU load and adds polypharmacy, inotropes and prolonged infusions. Nir-Neuman's finding that this load did not fall over a decade is the headline statistic to quote. [9]
Respiratory medicines are a high-volume off-label class across all ages — 't Jong's 2004 European Respiratory Journal paper documented it specifically, and it includes inhaled and oral bronchodilators, steroids and montelukast-type agents prescribed outside age or indication bands. [3]
Psychotropic medicines drive large outpatient exposure. Sohn's 2016 US national-trends study showed high off-label use of atypical antipsychotics in children and adolescents, where the consent and metabolic-monitoring duties are explicit and the evidence base is often thin. [11]
Oncology and rare disease are almost entirely protocol-driven off-label or unlicensed use, because licensed paediatric options rarely exist; here the protocol, the trial network and the specialist multi-disciplinary team carry the governance. [7]
Extemporaneous compounding and specials arise whenever no licensed paediatric formulation exists — a liquid made from a crushed tablet, an omeprazole suspension, a caffeine solution. Each carries stability, bioavailability and dosing-accuracy questions, and the governance pathway treats them as unlicensed. [5]
Primary care and outpatient prescribing is where the largest number of children are exposed, even if each exposure is lower-acuity; respiratory, psychotropic and off-label analgesic or anti-reflux prescribing dominate community volume. [11]
Complications & Pitfalls
The complications of off-label and unlicensed use are mostly system and governance failures rather than pharmacological ones, and they are where candidates lose marks. [8] [4]
The first pitfall is assuming off-label means wrong or unsafe. Off-label use is frequently the evidence-based standard of care; conflating it with error is a conceptual mistake and a viva trap. The mirror pitfall is treating it as risk-free — it carries more ADR risk and a thinner safety database, and Bellis's 2013 nested case-control study linked off-label and unlicensed medicines to a higher rate of adverse drug reactions in hospitalised children, with Neubert's 2004 study reaching the same conclusion about the impact on ADRs. [8] [4]
The second is confusing off-label with unlicensed. The supply chain, the quality questions and the governance route differ, and examiners deliberately probe the boundary. The third is skipping consent: families are often not told a medicine is off-label, and when a meaningful risk exists that is both an ethical and a medicolegal failure. The fourth is poor documentation — without a recorded indication, evidence base and family discussion, the prescriber is exposed. The fifth is compounding and importation risk: stability, bioavailability and dosing errors rise with extemporaneous and imported products. The sixth is failing to report adverse drug reactions, especially for off-label and unlicensed products where the safety database is thinnest. The seventh is not re-checking whether a licensed alternative now exists — licences and formularies change, and an unlicensed medicine that was necessary two years ago may now have a licensed paediatric form. [7] [12]
Prognosis & Disposition
For the child, the prognosis is that of the underlying condition and the medicine's efficacy and safety, not the licensing category itself — a well-chosen, well-monitored off-label medicine is not inherently more dangerous than a licensed one. What the category changes is the governance and monitoring burden you carry, and the disposition planning that follows from it. [7] [9]
At discharge, make the off-label or unlicensed status explicit in the plan. Confirm the community or outpatient supply (a specials order takes longer than an off-the-shelf licensed product), write down the monitoring schedule and the pharmacovigilance pathway, and tell the family who to contact. For a child on multiple off-label or unlicensed medicines — common in complex chronic disease — a medication-reconciliation and governance review at every transition is the safety net. [12]
The longer-term prognosis for the field is that off-label and unlicensed use will remain a large share of paediatric prescribing until the evidence and formulation gaps close, and that closure depends on the paediatric investigation plans, paediatric trials and paediatric formulation programmes described in the next section. Each ADR you report moves that closure forward by one data point. [10] [12]
Special Populations
Neonates and preterm infants sit at the top of every prevalence table. Developmental pharmacokinetics — immature hepatic metabolism and renal clearance — narrow the therapeutic window, weight-based dosing and dilution maths dominate, and the formulation gap forces compounding. The safe-use pathway is the same; the monitoring is tighter. [9] [5]
Children with medical complexity and technology dependence carry polypharmacy and repeated off-label or unlicensed exposure across many systems; medication reconciliation and governance review at every encounter are essential. [7]
Adolescents face off-label psychotropic and reproductive-medicine prescribing, and the consent question shifts toward the mature-minor framework — a competent young person may assent or consent themselves, and the off-label status must be part of that conversation. [11]
Children in rural and remote settings meet the supply-chain end of the formulation gap most acutely — a specials order may take days to arrive, and locally compounded alternatives carry their own stability questions. Plan early and confirm supply. [5]
Indigenous, migrant and refugee families may need interpreter-mediated consent for off-label or unlicensed use; the off-label explanation must be culturally safe and understandable, and the documentation should record the use of an interpreter. [7]
Children in out-of-home care and youth justice carry consent-authority complexities — who can consent to an off-label prescription depends on the guardianship arrangement, and the governance pathway must be explicit about the decision-maker. [7]
Evidence, Guidelines & Regional Differences
The regional story is one of regulatory frameworks trying to close the evidence gap from the top down, with mixed success. Each jurisdiction has its own engine, and naming the right one for the region you are examined in is part of the answer. [10] [7]
The European Union Paediatric Regulation (in force from 2007) is the most studied top-down intervention. It requires companies to produce a Paediatric Investigation Plan (PIP) describing the studies and formulations needed to support paediatric use, and it created rewards for generating paediatric data. Lindell-Osuagwu's 2014 before-and-after study in Finland asked the obvious question — did it reduce off-label and unlicensed use? — and found that, while the Regulation increased the volume of paediatric data, it had not yet translated into a clear fall in off-label and unlicensed prescribing at the ward level. That is the nuance examiners reward: the Regulation generates data, but the data take time to reach the bedside. [10]
In Australia and Aotearoa New Zealand, the Therapeutic Goods Administration (TGA) regulates medicines; off-label use is legal and is at the prescriber's responsibility, with the Australian Medicines Handbook (AMH) Children's edition and the Royal Children's Hospital Melbourne guidelines as the practical paediatric references. The PBS may constrain what is subsidised, which is a separate (funding) question from what is licensed. ADRs are reported through the Blue Card / Adverse Drug Reaction Reporting scheme. [7]
In Canada, Health Canada regulates medicines and faces the same paediatric formulation gap; many provinces rely on paediatric references such as the Hospital for Sick Children formulary. Across all regions the principle is identical: off-label and unlicensed use is governed by the prescriber's evidence, documentation, consent and monitoring duties, and by the local Medicines Committee. [5]
The controversy in the field is whether these frameworks have delivered enough, fast enough. They have unquestionably increased the volume of paediatric data and the number of paediatric label changes, but they have not eliminated off-label use, especially in neonates, intensive care and rare disease. The connect4children (c4c) pan-European network — Aurich's 2022 white paper sets out its pharmacovigilance methodology — is one attempt to build the infrastructure that turns scattered paediatric data into usable evidence. The honest fellowship answer is that the frameworks are necessary but not sufficient, and that bedside reporting and local governance still do the heavy lifting. [10] [12]
Exam Pearls
- Off-label = licensed product used outside a term of its licence; unlicensed = no licence for that product or formulation. Keep them apart — examiners probe the boundary deliberately. [1] [6]
- Off-label and unlicensed use is legal, common and often evidence-based. It is a prescribing category, not an error. [7]
- Prevalence peaks in neonates and intensive care and has not fallen over a decade (Nir-Neuman 2018); psychotropics and respiratory drugs are the high-volume classes (Sohn 2016; 't Jong 2004). [9] [11]
- The safe-use sequence is the backbone answer: licensed alternative? evidence? safest formulation? document? counsel and consent? monitor and report. [7]
- Always weigh the child in kilograms and dose against a paediatric reference (BNFc, AMH Children's, RCH Melbourne, Neofax), not the adult licence. [5]
- Off-label and unlicensed medicines carry more adverse drug reactions (Bellis 2013; Neubert 2004) — report every reaction through the national scheme (Yellow Card UK, Blue Card/ADRS Australia, MedWatch US). [8] [4]
- High-risk off-label or unlicensed use (narrow therapeutic index, neonate, IV, compounded) needs senior sign-off and Medicines Committee notification. [12]
- The EU Paediatric Regulation (2007) and PIPs, and the US BPCA/PREA under FDASIA, are the regulatory engines closing the evidence gap — but they have not yet eliminated off-label use. [10]
- When counselling families, name that the medicine is off-label, explain why it is the best choice, and document the discussion — a frequent communication-station stem. [7]
References
- [1]Conroy S Survey of unlicensed and off label drug use in paediatric wards in European countries. European Network for Drug Investigation in Children. BMJ, 2000.PMID 10625257
- [2]'t Jong GW A survey of the use of off-label and unlicensed drugs in a Dutch children's hospital. Pediatrics, 2001.PMID 11694685
- [3]'t Jong GW Unlicensed and off-label prescription of respiratory drugs to children. Eur Respir J, 2004.PMID 14979509
- [4]Neubert A The impact of unlicensed and off-label drug use on adverse drug reactions in paediatric patients. Drug Saf, 2004.PMID 15471510
- [5]Cuzzolin L Off-label and unlicensed prescribing for newborns and children in different settings: a review of the literature and a consideration about drug safety. Expert Opin Drug Saf, 2006.PMID 16907660
- [6]Kimland E Off-label drug use in pediatric patients. Clin Pharmacol Ther, 2012.PMID 22472984
- [7]Frattarelli DA Off-label use of drugs in children. Pediatrics, 2014.PMID 24567009
- [8]Bellis JR Adverse drug reactions and off-label and unlicensed medicines in children: a nested case-control study of inpatients in a pediatric hospital. BMC Med, 2013.PMID 24229060
- [9]Nir-Neuman H Unlicensed and Off-Label Medication Use in Pediatric and Neonatal Intensive Care Units: No Change Over a Decade. Adv Ther, 2018.PMID 29949042
- [10]Lindell-Osuagwu L Prescribing for off-label use and unauthorized medicines in three paediatric wards in Finland, the status before and after the European Union Paediatric Regulation. J Clin Pharm Ther, 2014.PMID 24329556
- [11]Sohn M National trends in off-label use of atypical antipsychotics in children and adolescents in the United States. Medicine (Baltimore), 2016.PMID 27281081
- [12]Aurich B c4c: Paediatric pharmacovigilance: Methodological considerations in research and development of medicines for children - A c4c expert group white paper. Br J Clin Pharmacol, 2022.PMID 34699077