Paeds · clinical-pharmacology-and-therapeutics
Opioids and acute pain medicines
Also known as Opioid analgesia in children · Acute pain management in children · Morphine oxycodone fentanyl dosing · Codeine contraindication in children · Tramadol contraindication in children · WHO analgesic ladder for children
A fellowship approach to opioids and acute pain medicines in children covering the WHO two-step analgesic ladder, mu-opioid receptor pharmacology and its dose-limiting adverse effects, developmental morphine pharmacokinetics, weight-based dosing for morphine, oxycodone, fentanyl and hydromorphone, the CYP2D6 prodrug mechanism that makes codeine and tramadol contraindicated in children, multimodal opioid-sparing analgesia, patient- and nurse-controlled analgesia safety, age-appropriate pain assessment, and naloxone reversal of opioid-induced respiratory depression.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A four-year-old waking from appendicectomy, a teenager with sickle-cell crisis, a neonate before a chest drain — these are the children whose acute pain you will be asked to relieve safely. Acute pain is pain of recent onset and expected short duration, arising from a defined injury, procedure, or illness, and it is a clinical sign that demands treatment in its own right rather than a symptom to be endured. Untreated acute pain is not benign: it drives tachycardia and hypertension, splinting and atelectasis, sleeplessness, and a behavioural sensitisation that can seed chronic pain, so the goal of therapy is prompt, sustained relief with the least harm. [8] [9]
Opioids are the most powerful acute-pain medicines we have, and they earn their power from a single pharmacological fact: they agonise the mu-opioid receptor. That same receptor produces analgesia in the brain, spinal cord, and peripheral nerves, and it also produces the dose-limiting harms — respiratory depression, sedation, constipation, nausea, and pruritus — that govern every prescribing decision. A fellowship candidate must therefore hold two truths at once: opioids are effective and necessary for moderate-to-severe acute pain, and every opioid prescription is a controlled negotiation between analgesia and respiratory depression. [9]
The single most important regulatory change in modern paediatric analgesia is the removal of codeine and tramadol. Both are prodrugs: they are inactive or weak until the cytochrome P450 2D6 (CYP2D6) enzyme converts them into active opioid — codeine to morphine, tramadol to O-desmethyltramadol. Because CYP2D6 activity is inherited, an ultrarapid metaboliser turns a normal dose into a lethal one, and a series of post-tonsillectomy deaths in young children forced regulators to act. The United States Food and Drug Administration issued a boxed warning, and the United Kingdom and European regulators issued contraindications: codeine and tramadol are now contraindicated in children under 12 years, and for postoperative pain management after tonsillectomy or adenoidectomy in children under 18 years. [1] [2] [3]
From first complaint of pain to a safe monitored regimen
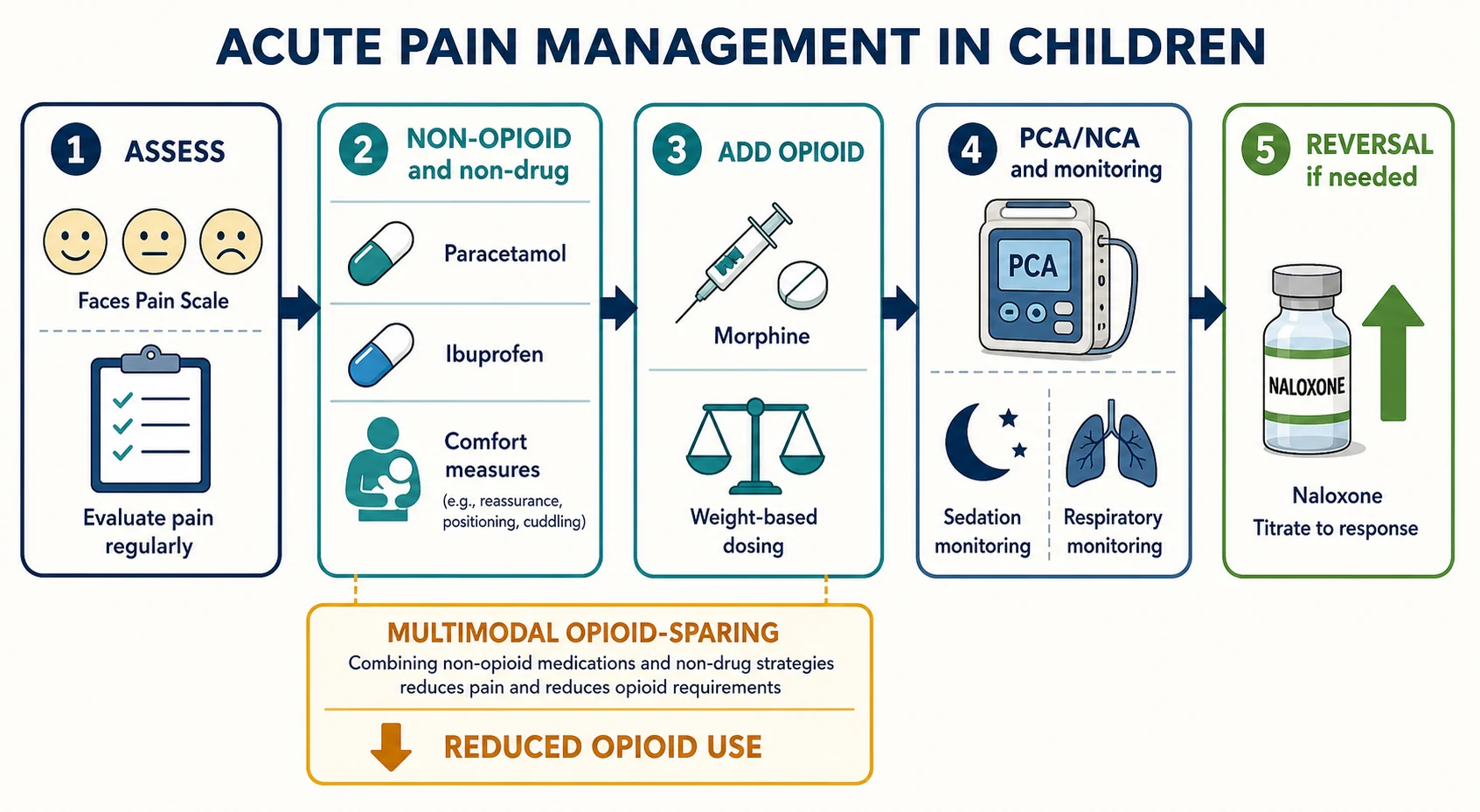
1 · Assess
Use an age-appropriate tool — FLACC for two months to seven years, the Faces Pain Scale for four to twelve years, the numeric rating scale for eight years and over — and record a score before you treat.
2 · Non-opioid first
Start with non-pharmacological measures (comfort, positioning, distraction) plus scheduled paracetamol and, where appropriate, an NSAID. This is the foundation of opioid-sparing multimodal analgesia.
3 · Add a strong opioid
For moderate-to-severe pain add morphine (oral 0.2 to 0.5 milligram per kilogram every four hours, or intravenous 0.1 to 0.2 milligram per kilogram titrated). Oxycodone, fentanyl, and hydromorphone are alternatives with defined weight-based doses.
4 · Monitor
Record paired pain and sedation scores, watch the respiratory rate (the earliest sign of opioid harm), and keep naloxone at the bedside. Never run a basal opioid infusion in the opioid-naive child.
5 · Review and step down
Reassess before and after every dose, titrate to effect, prophylax constipation, and step down from intravenous to oral as pain settles before discharge.
Classification
Acute pain medicines fall into three families, and the candidate should hold all three at once: non-opioid analgesics (paracetamol and the NSAIDs, covered in depth in the analgesics-and-antipyretics topic); opioids, the focus of this topic; and adjuvant analgesics (ketamine, clonidine, dexmedetomidine, gabapentinoids, and regional local-anaesthetic blocks) that reduce opioid requirement. The opioids themselves divide into the strong opioids used for moderate-to-severe pain and the weak opioids that historically bridged the gap — a distinction that has collapsed in modern paediatrics because the weak opioids, codeine and tramadol, are now contraindicated in children. [2] [8]
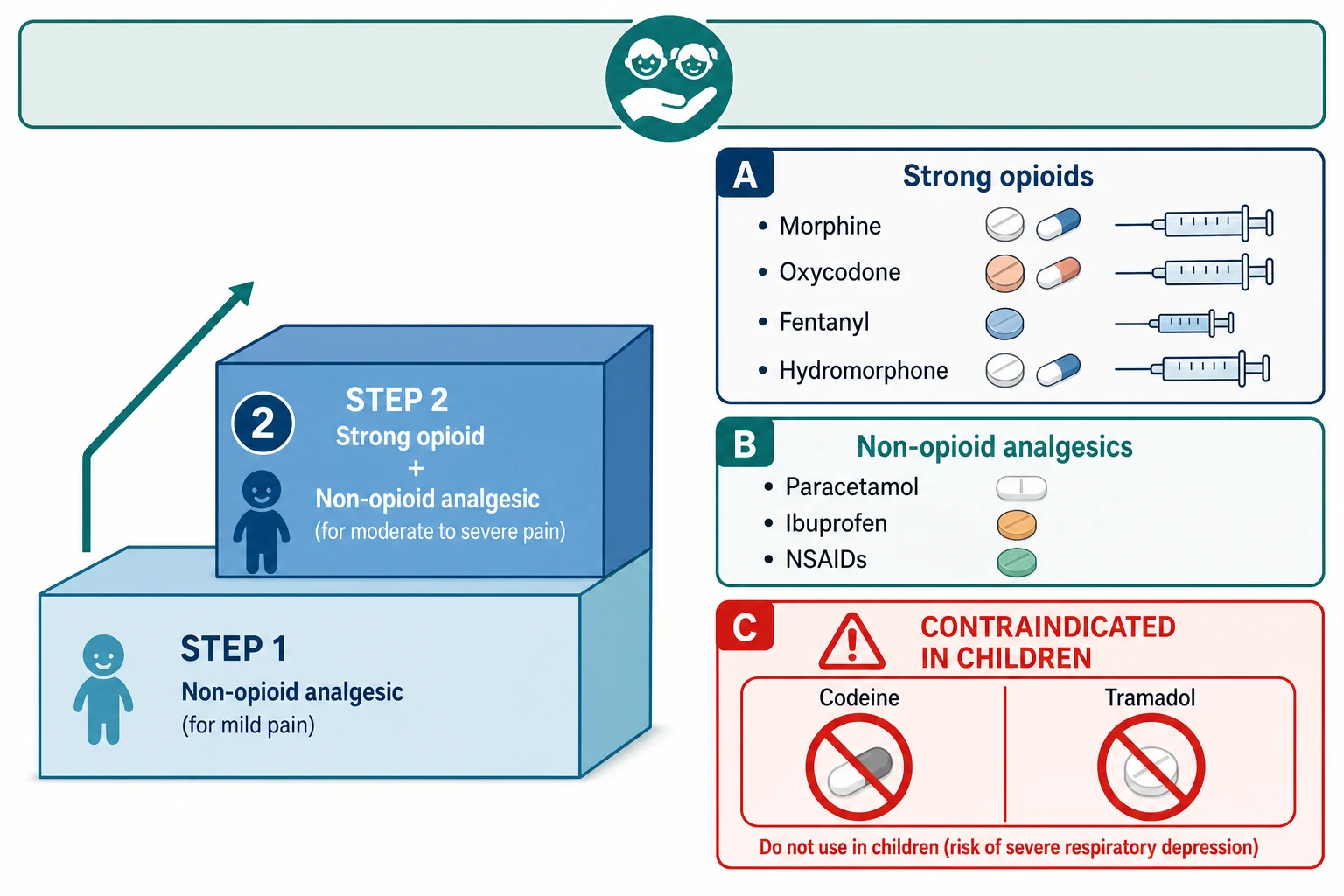
The strong opioids share a mechanism — pure mu-opioid agonism — but differ in potency, onset, route, and metabolism, and these differences drive selection at the bedside. Morphine is the prototype strong opioid and the first-line choice for moderate-to-severe acute pain: it is effective by mouth and by vein, inexpensive, and well understood. Oxycodone has high oral bioavailability and is a practical oral alternative when morphine is poorly tolerated. Fentanyl is far more potent and rapid, suited to brief procedural pain and to the patient who is haemodynamically fragile. Hydromorphone is a useful alternative in renal considerations and morphine intolerance. Methadone is reserved for complex, opioid-tolerant, or neuropathic pain because of its long and variable half-life. [6] [7]
| Opioid | Typical paediatric dose | Route and onset | Practical place |
|---|---|---|---|
| Morphine | Oral 0.2 to 0.5 mg/kg every 4 h; IV 0.1 to 0.2 mg/kg titrated; infusion 10 to 40 microgram/kg/h | Oral, IV, infusion; IV onset minutes | First-line strong opioid for moderate-to-severe acute pain |
| Oxycodone | Oral IR 0.1 to 0.2 mg/kg every 4 to 6 h (initial max 5 mg) | Oral (IR and CR); oral onset 20 to 30 min | Oral alternative when morphine not tolerated; ~1.5x oral morphine potency |
| Fentanyl | IV 1 microgram/kg; intranasal 1.5 microgram/kg | IV, intranasal; onset within minutes | Brief procedural pain; haemodynamically unstable patient |
| Hydromorphone | Oral 0.04 to 0.08 mg/kg; IV 0.015 mg/kg | Oral, IV | Morphine intolerance; favoured over morphine in renal considerations |
| Methadone | Specialist-supervised; long variable half-life | Oral, IV | Opioid-tolerant, neuropathic, or palliative pain only |
[6] [7] Doses are indicative weight-based ranges drawn from AMH Children's Dosing Companion, BNFc, and RCH Melbourne Clinical Practice Guidelines; always confirm against the current formulary for the child's age, weight, and organ function.
The two weak opioids deserve their own line because they are the commonest prescribing error an examiner will test. Codeine is a prodrug converted by CYP2D6 to morphine, and tramadol is converted by the same enzyme to the active O-desmethyltramadol. Their analgesic effect and their toxicity both depend on an enzyme whose activity is genetically determined and unpredictable in any individual child. After several deaths from respiratory depression in ultrarapid-metaboliser children following tonsillectomy, regulators concluded that the risk was not worth a benefit that paracetamol, NSAIDs, and morphine already provide better. They are now contraindicated in children. [1] [2] [3]
Epidemiology & Risk Factors
Acute pain is among the commonest reasons a child receives a medicine in hospital, and postoperative and procedural pain dominate the prescribing. Despite the regulatory action on codeine and tramadol, prescribing did not stop at once: a study of periprocedural prescribing after the United States boxed warning found that codeine and tramadol continued to be dispensed to children, underscoring why every prescriber must know the contraindication by heart rather than rely on systems to catch it. [5]
The children at greatest risk of opioid harm are not evenly distributed. An infant clears morphine more slowly than an older child, so a weight-scaled adult dose over-treats and endangers the baby. A child with upper-airway obstruction or obstructive sleep apnoea — exactly the child presenting for tonsillectomy — is already primed for desaturation and is exquisitely sensitive to opioid respiratory depression. Obesity compounds this. A child on a concurrent sedative (a benzodiazepine, an antiepileptic, an antihistamine) suffers additive central nervous system depression. The opioid-naive child given a background infusion cannot protect himself from a dose he did not ask for. [9] [6]
Previously well child
Short procedure, opioid-naive
- Standard weight-based morphine dosing
- Lowest baseline opioid-harm risk
- Single cautious dose often sufficient
- Step down to oral and non-opioid early
Infant under six months
Slow morphine clearance
- Reduced and less frequent weight-based doses
- Mandatory oximetry and sedation scoring
- Longer dosing interval, avoid basal infusion
- Avoid codeine and tramadol in breastfeeding mother
OSA or obesity
Airway-sensitive
- Heightened opioid sensitivity and desaturation risk
- Prefer non-opioid and regional strategies
- Continuous oximetry and monitored bed
- Avoid basal opioid infusion; bolus with lockout
Opioid-tolerant
Sickle-cell, oncology, chronic pain
- Continue baseline opioid plus breakthrough doses
- Higher total requirement; consider ketamine
- Avoid under-treatment and withdrawal
- Plan wean with pain or palliative team
The single strongest driver of codeine and tramadol toxicity is CYP2D6 ultrarapid metabolism, which is inherited and population-dependent, occurring in roughly 1 to 10 per cent of people depending on ethnicity. Because you cannot identify an ultrarapid metaboliser at the bedside, the contraindication applies to every child — the one predictable way to prevent the unpredictable lethal reaction is not to prescribe the drug. [3] [4]
Pathophysiology
Acute pain begins at a nociceptor, a free nerve ending that transduces a noxious stimulus into an electrical signal. That signal travels along thin myelinated A-delta fibres (fast, sharp, well-localised pain) and slow unmyelinated C fibres (dull, aching, poorly localised pain) into the dorsal horn of the spinal cord, crosses, and ascends to the thalamus and somatosensory cortex. A descending inhibitory pathway from the brain can close a "gate" in the dorsal horn and dampen the signal — the neurological basis for why comfort, distraction, and reassurance are genuine analgesia and not mere kindness. [9]
Opioids act on this system by agonising the mu-opioid receptor, a G-protein-coupled receptor found in the brain, the spinal dorsal horn, and the peripheral terminals of nociceptors. Agonism at these receptors both inhibits the ascending pain signal and amplifies descending inhibition, producing analgesia. The same receptor, however, is expressed in the respiratory centres of the medulla, in the gastrointestinal tract, in the Edinger-Westphal nucleus of the eye, in the chemoreceptor trigger zone, and in mast cells — which is why one drug simultaneously relieves pain and causes respiratory depression, constipation, miosis, nausea, and pruritus. The adverse-effect profile of an opioid is not a side-effect; it is the same receptor acting at different sites. [9]
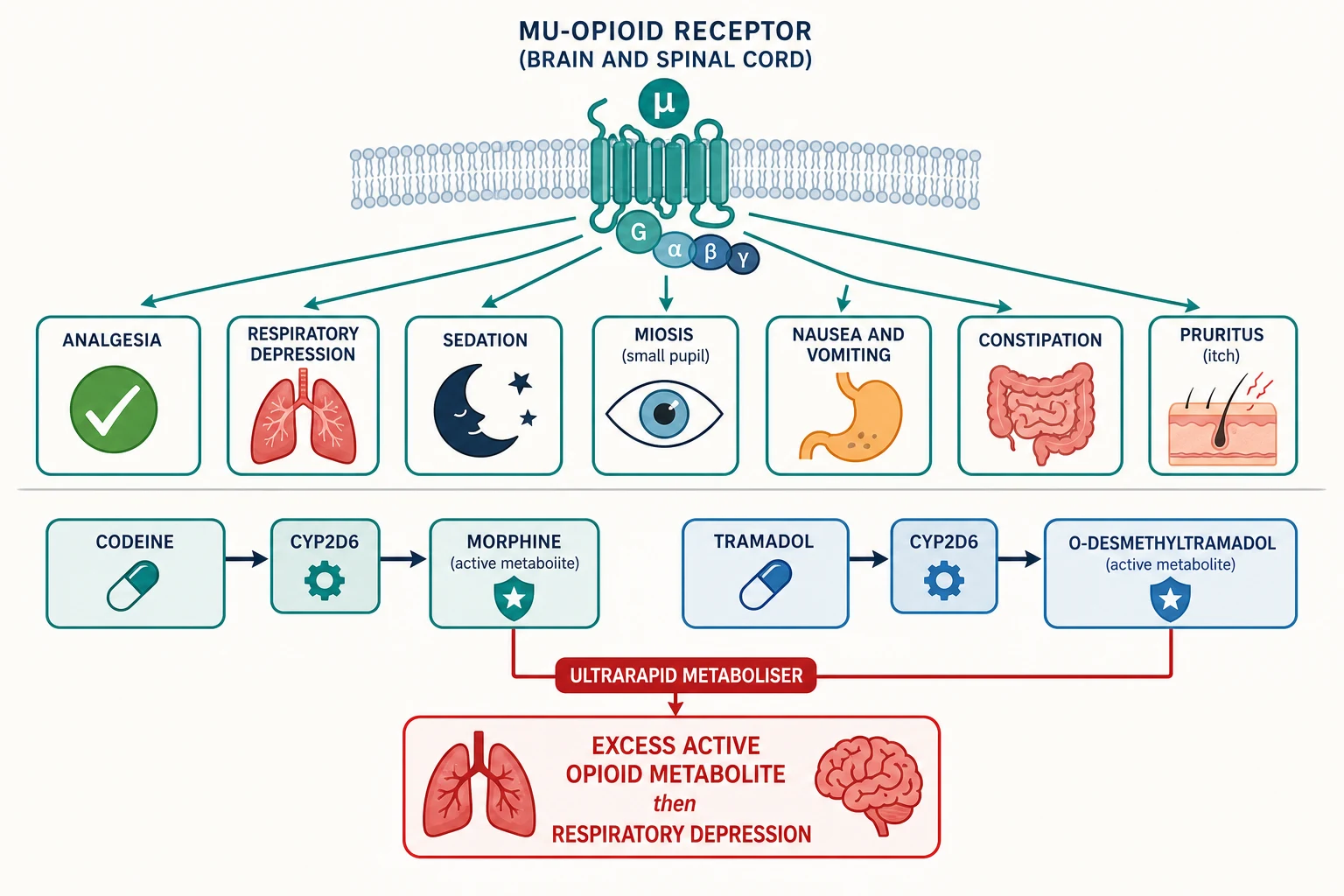
The pharmacogenetic story of codeine and tramadol is the heart of their contraindication. Codeine by itself is a weak analgesic; roughly 5 to 10 per cent of a dose is O-demethylated by CYP2D6 into morphine, and it is the morphine that does the work. Tramadol has some intrinsic monoaminergic activity, but its principal opioid analgesia comes from CYP2D6 conversion to O-desmethyltramadol, a much more potent mu-agonist than the parent drug. In a child who is a CYP2D6 ultrarapid metaboliser, these conversions run fast and far, generating opioid concentrations that suppress the medullary respiratory centre and can kill — the documented mechanism of the post-tonsillectomy deaths. At the other extreme, a poor metaboliser converts almost nothing and gets no analgesia from codeine at all, which is why the drug was always pharmacologically unreliable even before it was dangerous. [3] [4]
Developmental pharmacokinetics add a second layer that the candidate must defend. Morphine is cleared by glucuronidation (to morphine-3-glucuronide and the active morphine-6-glucuronide), and the glucuronidation enzymes are immature at birth. The landmark study of morphine clearance in postoperative infants during intravenous infusion showed that clearance rises steeply with postnatal age: a neonate clears morphine slowly and accumulates it, an infant clears it faster but still less efficiently than a school-age child, and clearance reaches and then exceeds adult values per kilogram in early childhood. The practical consequence is that the neonate and young infant need a lower dose at a longer interval and mandatory monitoring, whereas the toddler and school-age child handle weight-based morphine more briskly. A neonate is never a small adult when the drug is an opioid. [6]
Clinical Presentation
Acute pain in a pre-verbal child does not announce itself with a number. The infant or toddler in pain cries, draws up the legs, becomes rigid or withdrawn, refuses to move, and shows the behavioural and physiological signs captured in a structured tool. Vital signs — tachycardia, a raised respiratory rate, hypertension — are supportive but unreliable: a terrified but pain-free child tachycardias, and a deeply sedated child in surgical pain may have normal vital signs. Self-report is the gold standard whenever the child can give it; structured behavioural observation is the substitute when they cannot. [8]
The presentation the candidate must never miss is opioid-induced respiratory depression. The earliest sign is a reduction in the depth and then the rate of breathing, accompanied by increasing sedation and small (pin-point) pupils. Oxygen saturation is a late and unreliable sentinel, because desaturation falls only after substantial respiratory depression has developed — by the time the child is cyanosed, the harm is advanced. Arousability and respiratory rate are the bedside sentinels: a child who is hard to rouse and breathing slowly after an opioid is opioid-toxic until proved otherwise. [9]
The commoner adverse effects present in characteristic ways. Nausea and vomiting appear within hours and can derail oral recovery. Constipation is near-universal and does not improve with time, because tolerance to the gastrointestinal effect does not develop. Pruritus and urinary retention are distressing but reversible. Sedation is the warning that precedes respiratory depression, which is why a rising sedation score demands dose reduction before apnoea. [9]
Inadequately treated acute pain presents in its own way — splinting, shallow breathing, atelectasis, immobility, tachycardia, hypertension, sleeplessness, and behavioural distress — and it prolongs admission and seeds persistent post-surgical pain. The candidate is therefore balancing two harms: opioid harm from over-treatment and the physiological and psychological harm of under-treatment. The resolution is not less analgesia but better analgesia — scheduled, multimodal, monitored, and titrated. [8] [12]
Differential Diagnosis
When a child deteriorates after an opioid, opioid-induced respiratory depression is high on the list but it is not the only explanation, and a structured differential prevents the dangerous assumption. The four questions that convert a vague "drowsy" into a diagnosis are: timing relative to the last opioid dose, the concurrent sedative or anaesthetic still on board, the child's opioid-naive or tolerant status, and the pupil and respiratory pattern. Opioid toxicity peaks as the drug peaks; residual anaesthetic fades over hours; airway obstruction is positional and noisy; sepsis and raised intracranial pressure each carry their own trajectory. [9]
| Diagnosis | Distinguishing features | Key action |
|---|---|---|
| Opioid-induced respiratory depression | Onset tracks opioid peak; small pupils; reduced depth then rate of breathing; responds to naloxone | Stimulate, support ventilation, titrate naloxone to respiratory rate |
| Residual anaesthetic or sedative | Temporally related to theatre or last sedative dose; pupils variable; clears with time | Supportive airway care; allow metabolism; review sedatives |
| Upper-airway obstruction | Noisy or obstructed breathing; positional; tragal tug or recession; normal pupils | Airway opening manoeuvres; positional change; assess for OSA |
| Hypoxaemia or hypercapnia from another cause | Pneumonia, atelectasis, splinting; consistent with chest findings | Oxygen, treat cause; chest examination and imaging |
| Sepsis or raised intracranial pressure | Fever, capillary refill, or neurological signs; evolving independently of opioid | Sepsis screen and cultures; neurological assessment and imaging |
Postoperative nausea and vomiting carries its own differential: opioid effect, anaesthetic agent, vestibular stimulation, ileus, and, rarely, raised intracranial pressure. The temporal relationship to the opioid dose, the presence of vertigo, and the abdominal examination distinguish them and guide the choice of antiemetic versus opioid dose reduction. Postoperative agitation or delirium similarly splits into pain (child is consolable and settles with analgesia), hypoxia, opioid dysphoria, anticholinergic effect, and emergence — and the first move is always to assess and treat pain and to check an oxygen saturation. [9]
Clinical & Bedside Assessment
The assessment of acute pain begins with the age-appropriate pain score, recorded before and after every intervention. The candidate should know three tools cold. FLACC (Face, Legs, Activity, Cry, Consolability) scores each domain from zero to two for a total of ten and is validated from two months to seven years, with a revised r-FLACC version for children with cognitive impairment. The Faces Pain Scale shows a row of neutral-to-distressed faces and is used from about four to twelve years. The numeric rating scale (zero to ten) is used from about eight years and over, whenever the child can use a number. Whenever a child can self-report, self-report wins; behavioural tools are the substitute, not the equal. [8]
The opioid-toxicity bedside assessment is its own skill. Record the respiratory rate and depth, the sedation score (for example a four-point scale from alert and artrousable through to unresponsive), the pupil size, the oxygen saturation, and the heart rate. The decisive trigger for naloxone is a child who is hard to rouse with a slow or shallow respiratory effort after an opioid — do not wait for a falling oxygen saturation, which is a late sign. The pain-and-sedation pair recorded together is the single most useful monitoring habit in acute-pain practice: a rising sedation score on a stable opioid infusion demands dose reduction before apnoea occurs. [9] [10]
Investigations
Acute-pain management is governed far more by scores than by laboratory tests. The pain score and the sedation score are the primary monitoring investigations for any opioid regimen, and they should be recorded at a frequency that matches the intensity of therapy — hourly for an infusion, before and after each bolus, and on every ward round. Opioid blood-level monitoring is rarely used in routine acute pain; it has a small role for methadone and for complex PICU morphine infusions where level-guided dosing is needed. [9]
Physiological monitoring is added in proportion to risk. For a child on a basal or continuous opioid infusion, for an opioid-naive infant, for a child with OSA or obesity, and whenever an opioid is combined with a benzodiazepine, add continuous pulse oximetry, hourly respiratory rate and sedation scoring, and, in high-risk settings, capnography. Baseline renal and hepatic function and an accurate weight should be checked before selecting the opioid, dose, and interval in a child with organ impairment, because morphine and its active metabolite morphine-6-glucuronide accumulate in renal failure and oxycodone clearance falls in hepatic impairment. [9]
A trial of naloxone functions as both a treatment and a diagnostic test: a child with suspected opioid-induced respiratory depression who brightens and breathes faster after a weight-based naloxone dose has confirmed the diagnosis, while a child who does not respond forces a search for another cause. The dose is small and titrated so that respiratory drive is restored without precipitating acute withdrawal. [11]
Management — Resuscitation
The immediate management of opioid-induced respiratory depression is a sequence every candidate must recite: stimulate the child, open and support the airway, provide bag-valve-mask ventilation if breathing is inadequate, and give naloxone titrated to the respiratory rate rather than to full consciousness. The principle of titration is essential: the goal is to restore adequate breathing, not to render the child acutely awake and in severe pain, because a large naloxone dose precipitates acute opioid withdrawal, uncontrolled pain, agitation, and in rare cases pulmonary oedema. [9] [11]
Naloxone for opioid-induced respiratory depression in a child
Dose
10 microgram per kilogram per dose, repeated every 2 to 3 minutes until respiratory effort is restored; up to a maximum single dose of about 2 mg in an adolescent
The rescue dose for breakthrough severe acute pain is intravenous morphine 0.1 to 0.2 milligram per kilogram titrated in increments to effect, given slowly with the child observed — this is how you bring a child in severe sickle-cell or postoperative pain under control safely and rapidly, reassessing after each increment. After any respiratory-depression event, stop the offending opioid, switch the child to a monitored bed, arrange continuous oximetry and hourly sedation scoring, keep naloxone at the bedside, and review the regimen with the acute-pain service before any further opioid is given. [6] [9]
Management — Definitive & Stepwise
Definitive acute-pain management is a ladder climbed deliberately, with each rung justified by the pain score and stepped down as the child improves. Assess with the age-appropriate tool. Begin with non-pharmacological measures (comfort, positioning, distraction, sucrose in the infant) plus scheduled paracetamol and, where appropriate, an NSAID — this non-opioid foundation is the basis of opioid-sparing multimodal analgesia and should be in place for every child with significant pain. Add a strong opioid for moderate-to-severe pain, titrated to effect. Bring in regional and adjuvant strategies to reduce opioid requirement. Review before and after every dose and step down to oral as pain settles. [8] [12]
Morphine (first-line strong opioid for moderate-to-severe acute pain)
Dose
Oral 0.2 to 0.5 mg/kg every 4 h; IV bolus 0.1 to 0.2 mg/kg titrated slowly in increments; continuous infusion 10 to 40 microgram/kg/h (lower and less frequent in the neonate and young infant)
The principle of multimodal opioid-sparing analgesia is that combining agents with different mechanisms — paracetamol, an NSAID, a regional local-anaesthetic block, and an opioid — produces better pain control at a lower opioid dose, and therefore fewer opioid adverse effects. The 2025 JAMA Pediatrics network meta-analysis of pharmacologic management of acute pain in children found that combination therapy outperformed single agents, and the opioid-sparing multimodal protocol after selective dorsal rhizotomy reduced opioid use without compromising analgesia. The candidate should present multimodal analgesia as the standard, not an add-on: give paracetamol and an NSAID on a schedule, use a regional block where feasible, and let the opioid be the titrated top-up rather than the sole agent. [8] [12]
For ongoing moderate-to-severe pain, patient-controlled analgesia (PCA) and, in the child too young to operate a button, nurse-controlled analgesia (NCA) are the delivery systems of choice. A safe paediatric PCA uses a weight-based bolus (morphine around 20 microgram per kilogram), a lockout of ten to twenty minutes, and no background (basal) infusion in the opioid-naive child, because a background infusion multiplies the risk of respiratory depression in a patient who cannot protect themselves from a dose they did not request. Exclusive ordering, a dedicated line, paired sedation and oxygen monitoring, and a clear naloxone plan are the safety scaffolding. The PRISMA review of PCA safety in paediatrics confirmed that PCA is effective and acceptable when these safeguards are in place, and that respiratory depression clusters when they are not. [10]
The predictable adverse effects are preventable, and preventing them is part of the prescription, not an afterthought. Constipation is near-universal and tolerance does not develop, so prescribe a prophylactic stimulant laxative (with or without a stool softener) with every regular opioid from the first dose. Nausea and vomiting respond to a regular antiemetic and, if persistent, to opioid dose reduction or switch. Pruritus may respond to an antihistamine or to a low-dose naloxone infusion. Sedation is the warning sign: a rising sedation score is an instruction to reduce or hold the opioid before respiratory depression supervenes. [9]
Specific Subtypes & Scenarios
Post-tonsillectomy pain is the scenario that ended codeine and tramadol in children, and it remains the highest-yield vignette. The child presenting for adenotonsillectomy often has obstructive sleep apnoea and is therefore opioid-sensitive; the historic reliance on codeine killed ultrarapid-metaboliser children; and the correct modern regimen is scheduled paracetamol and ibuprofen with oral morphine or oxycodone as rescue, given with clear family safety-netting about over-sedation and airway obstruction. Confirm at the prescription that codeine and tramadol are absent. [1] [2]
Acute sickle-cell pain is severe, recurrent, and individual. The analgesic ladder applies, but severe pain demands rapid opioid — intravenous morphine titrated to effect — alongside hydration and oxygen as indicated, with reassessment at short intervals and individualised dosing, because these children are often opioid-tolerant. Codeine must not be used because of CYP2D6 variability, which makes its effect unpredictable exactly when reliable analgesia is essential. [2]
Procedural pain is brief but intense and is often under-treated. Intranasal fentanyl (around 1.5 microgram per kilogram) provides rapid analgesia for a child without intravenous access, and intravenous fentanyl or morphine with monitoring suits short painful events; nitrous oxide and non-pharmacological measures are adjuncts. The principle is that procedural pain is real pain and deserves the same weight-based, monitored approach. [9]
The neonate and young infant need special care. Morphine clearance is reduced, so use a lower dose at a longer interval with mandatory oximetry and sedation scoring, and avoid background infusions in the opioid-naive. Crucially, codeine and tramadol are contraindicated in breastfeeding mothers who may be ultrarapid metabolisers, because active opioid reaches the infant through breast milk — a regulatory point the examiner rewards. [6]
The opioid-tolerant child (sickle-cell, oncology, chronic pain) is the scenario where under-treatment is the commonest error. Continue the baseline opioid, add breakthrough doses at an appropriate fraction of the total daily dose, consider an infusion or ketamine for severe acute pain, and plan the wean with the pain or palliative team to avoid both under-treatment and withdrawal. [9] [12]
Complications & Pitfalls
The gravest complications are the ones the contraindication was designed to prevent: death from respiratory depression after codeine or tramadol in a CYP2D6 ultrarapid-metaboliser child following tonsillectomy. These were real children, and their deaths are the reason no candidate should ever prescribe either drug to a child. Prescribing persisted after the warnings, which is why the contraindication must be carried in the prescriber's head, not only in the decision-support software. [1] [5]
Opioid-induced respiratory depression is the central harm of the strong opioids, and the candidate must know its earliest sign — reduced depth and then rate of breathing with rising sedation, before any fall in oxygen saturation — and the multiplying effect of a concurrent benzodiazepine. A basal (background) opioid infusion in an opioid-naive child is a classic iatrogenic pitfall, because the child receives opioid they did not request and cannot protect themselves from; bolus-with-lockout is the safe default. [9] [10]
The balance of harms runs in both directions. Under-treatment causes splinting, atelectasis, poor sleep, and behavioural sensitisation to future pain, just as over-treatment causes opioid harm. The resolution is not less analgesia but better analgesia — scheduled, multimodal, monitored, and titrated — so that the child is comfortable and breathing. Finally, naloxone itself harms if over-administered: a large bolus precipitates acute withdrawal, severe uncontrolled pain, agitation, and occasionally pulmonary oedema, so the rule is titration to respiratory rate, never to full consciousness. [11]
Prognosis & Disposition
The prognosis of an episode of acute pain depends less on the opioid chosen than on the discipline of prompt assessment, weight-based dosing, and scheduled review. A child managed on a structured multimodal regimen with paired monitoring recovers comfortably and steps down to oral analgesia within days; a child managed ad hoc with intermittent boluses and no review suffers either pain or opioid harm, and stays longer. [8]
Disposition follows the intensity of the regimen. Moderate pain controlled on oral opioid is managed on the ward. A child on a continuous opioid infusion, an opioid-naive infant, or a child with OSA or obesity on an opioid belongs in a monitored bed (HDU or PICU) with continuous oximetry and hourly sedation scoring. Step down from intravenous to oral when pain is controlled on low intravenous doses, and discharge only when the child is comfortable on oral analgesia with a clear plan. [9] [10]
Discharge safety-netting is part of the prescription. Give the family a written plan with the drug, dose, interval, and duration; counsel them on the signs of over-sedation and slow breathing and the instruction to seek help; confirm that codeine and tramadol will not be substituted by another prescriber or pharmacist; and arrange a review of pain control and adverse effects within a defined interval. A clear return precaution closes the loop. [1] [2]
Special Populations
The neonate and young infant are the population where developmental pharmacokinetics change everything. Immature glucuronidation slows morphine clearance, so use a lower weight-based dose at a longer interval, monitor with continuous oximetry, and avoid background infusions in the opioid-naive. The breastfeeding mother who is a CYP2D6 ultrarapid metaboliser can pass lethal opioid to her infant through milk, so codeine and tramadol are contraindicated in breastfeeding — a point the examiner tests. [6]
The child with upper-airway obstruction, obstructive sleep apnoea, or obesity is opioid-sensitive and primed to desaturate. Prefer non-opioid and regional strategies, use the smallest effective opioid dose, avoid background infusions, and monitor in a monitored bed. This is exactly the post-tonsillectomy child whose deaths drove the codeine contraindication. [1] [9]
Organ failure reshapes the choice. In hepatic impairment, reduce or avoid morphine and oxycodone and favour shorter-acting fentanyl with careful titration, because clearance falls and accumulation causes prolonged depression. In renal impairment, morphine and oxycodone active metabolites (morphine-6-glucuronide and oxymorphone) accumulate, so favour fentanyl, which has no active renally-cleared metabolites, and titrate cautiously. [6] [7]
The child with developmental disability who cannot self-report is at particular risk of both under-treatment and over-treatment. Use the r-FLACC behavioural tool, gather carer input on the child's usual pain behaviours, and maintain a low threshold for a carefully monitored opioid trial rather than assuming agitation is behavioural. [8]
For migrant, refugee, and low-health-literacy families, discharge communication about opioid safety is hardest and most important. Use plain language, an interpreter, a written and pictorial plan, and explicit counselling on recognising over-sedation and slow breathing, because overdose recognition and help-seeking depend on the family understanding the warning signs. [1] [9]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric acute-pain pharmacology has matured. The 2025 JAMA Pediatrics systematic review and network meta-analysis of pharmacologic management of acute pain in children compared single and combination regimens and supported combination (multimodal) therapy over single agents — providing the evidence that multimodal opioid-sparing analgesia should be the standard, not an option. The case-series review of opioid-induced respiratory depression in paediatrics documented the patterns and precipitants of the harm that monitoring and contraindications are designed to prevent, and the PRISMA review of PCA safety and efficacy established both the effectiveness of PCA and the clustering of respiratory depression when safeguards fail. [8] [9] [10]
The pharmacokinetic foundation is equally important. The morphine-clearance study in postoperative infants established the age-dependence of morphine handling that underpins infant dosing, and the population pharmacokinetic study of oxycodone from premature neonates to adults characterised oxycodone disposition across the age range, supporting its weight-based use. The intranasal naloxone pharmacokinetic study in children demonstrated rapid systemic uptake, justifying the intranasal route when intravenous access is unavailable. [6] [7] [11]
FDA boxed warning and MHRA/EMA contraindication — codeine and tramadol in children
Regulatory safety review following post-marketing case reports of paediatric opioid deaths
Key finding
Codeine contraindicated in children under 12 years and for post-tonsillectomy or adenoidectomy pain in children under 18 years; tramadol contraindicated under 12 years and after tonsillectomy or adenoidectomy under 18 years, because CYP2D6 ultrarapid metabolism generates lethal active opioid
Regional guidance converges on the contraindication and on morphine first-line, with local formulary variation in exact weight-based ranges. ANZ guidance (AMH Children's Dosing Companion, RCH Melbourne Clinical Practice Guidelines, and the ANZCA acute-pain framework) and UK guidance (BNFc, NICE, and the Association of Paediatric Anaesthetists) both prohibit codeine and tramadol in children and endorse multimodal morphine-based analgesia. US guidance (FDA safety communications, AAP, and ASA) carries the boxed warning. WHO persists with a two-step ladder for children that places strong opioid (morphine) directly at the second step, with no weak-opioid step. The candidate should name the formulary they are quoting. [2] [8]
Exam Pearls
OPIOID
The contraindication is the single highest-yield fact in this topic. Codeine is contraindicated in children under 12 years and for postoperative pain after tonsillectomy or adenoidectomy in children under 18 years, because CYP2D6 ultrarapid metabolisers convert it to excess morphine and die of respiratory depression. Tramadol is contraindicated in children under 12 years and after tonsillectomy or adenoidectomy under 18 years by the same prodrug mechanism, converting to O-desmethyltramadol. [1] [2] [3]
Morphine is the first-line strong opioid: oral 0.2 to 0.5 milligram per kilogram every four hours, intravenous 0.1 to 0.2 milligram per kilogram titrated in increments, infusion 10 to 40 microgram per kilogram per hour. Reduced respiratory rate is the earliest sign of opioid-induced respiratory depression; oxygen saturation falls late — never wait for cyanosis. Naloxone is 10 microgram per kilogram intravenous or intramuscular, repeated every two to three minutes to a maximum, titrated to restore respiratory rate rather than full consciousness to avoid acute withdrawal; its half-life is short, so watch for renarcotisation. [6] [11]
Constipation is near-universal and tolerance does not develop — prescribe a prophylactic stimulant laxative with every regular opioid. Avoid a basal (background) opioid infusion in the opioid-naive child on PCA — it multiplies respiratory-depression risk; bolus-with-lockout is the safe default. The WHO ladder for children is two steps — Step 1 non-opioid plus adjuvant, Step 2 strong opioid (morphine) plus non-opioid plus adjuvant — with no weak-opioid step in modern paediatric practice. And the breastfeeding mother who is a CYP2D6 ultrarapid metaboliser can pass lethal opioid to her infant through milk, so codeine and tramadol are contraindicated in breastfeeding. [2] [10]
References
- [1]Racoosin, Judith A; Roberson, David W; Pacanowski, Mark A; et al New evidence about an old drug — risk with codeine after adenotonsillectomy New England Journal of Medicine, 2013.PMID 23614474
- [2]Tobias, Joseph D; Green, Thomas P; Coté, Charles J; et al Codeine: Time to Say No Pediatrics, 2016.PMID 27647717
- [3]Pratt, Victoria M; Scott, Stuart A; Pirmohamed, Munir; et al Tramadol Therapy and CYP2D6 Genotype Clinical Pharmacology and Therapeutics, 2012.PMID 28520365
- [4]Dean, Laura; Kane, Mary Codeine Therapy and CYP2D6 Genotype Medical Genetics Summaries, 2012.PMID 28520350
- [5]Kohler, Jean E; Cartmill, Ryan S; Kalbfell, Elizabeth; et al Continued Prescribing of Periprocedural Codeine and Tramadol to Children after a Black Box Warning Journal of Surgical Research, 2020.PMID 32693330
- [6]Lynn, Anne; Nespeca, Mary K; Bratton, Sunkyung L; et al Clearance of morphine in postoperative infants during intravenous infusion: the influence of age and surgery Anesthesia and Analgesia, 1998.PMID 9585276
- [7]Morse, James D; Sundermann, Mikael; Hannam, John A; et al Population pharmacokinetics of oxycodone: Premature neonates to adults Paediatric Anaesthesia, 2021.PMID 34469607
- [8]Olejnik, Lukas; Lima, Joao P; Sadeghirad, Behnam; et al Pharmacologic Management of Acute Pain in Children: A Systematic Review and Network Meta-Analysis JAMA Pediatrics, 2025.PMID 39899301
- [9]Niesters, Monique; Overdyk, Frank; Smith, Thornton; et al Opioid-induced respiratory depression in paediatrics: a review of case reports British Journal of Anaesthesia, 2013.PMID 23248093
- [10]Sharp, Debra; Jaffrani, Aliasgar A PRISMA Systematic Review on the Safety and Efficacy of Patient-Controlled Analgesia (PCA) in Pediatrics Journal of Pediatric Nursing, 2021.PMID 34139608
- [11]Malmros Olsson, Elisabet; Lonnqvist, Per-Arne; Stiller, Cari O; et al Rapid systemic uptake of naloxone after intranasal administration in children Paediatric Anaesthesia, 2021.PMID 33687794
- [12]Shao, Brian; Tariq, Azeem A; Goldstein, Hediary E; et al Opioid-Sparing Multimodal Analgesia After Selective Dorsal Rhizotomy Hospital Pediatrics, 2020.PMID 31862854