Paeds · clinical-pharmacology-and-therapeutics
Pharmacogenomics and precision therapeutics
Also known as Pharmacogenomics in children · Precision medicine and prescribing · TPMT and thiopurine testing · CYP2D6 and codeine · HLA-B and carbamazepine
A fellowship approach to pharmacogenomics and precision therapeutics in children covering how inherited gene variants change the way an individual child handles a drug, the Clinical Pharmacogenetics Implementation Consortium gene-drug pairs a general paediatrician must know, thiopurine methyltransferase and NUDT15 before azathioprine or 6-mercaptopurine, CYP2D6 and the codeine ultrarapid-metaboliser trap, HLA-B star 15 colon 02 screening before carbamazepine, HLA-B star 57 colon 01 before abacavir, CYP2C19 and clopidogrel, and how to order a genotype, read a report, and change the prescription.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a six-year-old of Han Chinese background about to start carbamazepine for epilepsy, a ten-year-old with Crohn disease about to start azathioprine, and a four-year-old sent home with codeine after adenotonsillectomy. Each child is carrying a hidden inherited variant that will turn a standard prescription into a serious adverse drug reaction. Pharmacogenomics is the discipline that finds those variants first and changes the prescription before the harm arrives. [9] [10]
Two ideas carry the whole topic. The first is the gene-drug pair: pharmacogenomics is not a genome-wide screen, it is a small set of specific genes whose variants predict a specific drug's effect to a degree strong enough to change practice. The Clinical Pharmacogenetics Implementation Consortium (CPIC) publishes the gene-drug pairs that are ready for the clinic, and the fellowship candidate must know the four that meet children most often — TPMT and NUDT15 with the thiopurines, CYP2D6 with codeine, HLA-B star 15 colon 02 with carbamazepine, and HLA-B star 57 colon 01 with abacavir. The second is the actionable result: a pharmacogenomic test only helps if the result reaches the prescriber and the prescription changes, so the discipline closes on communication, not on the laboratory. [1] [9] [10]
From a planned prescription to a precision one
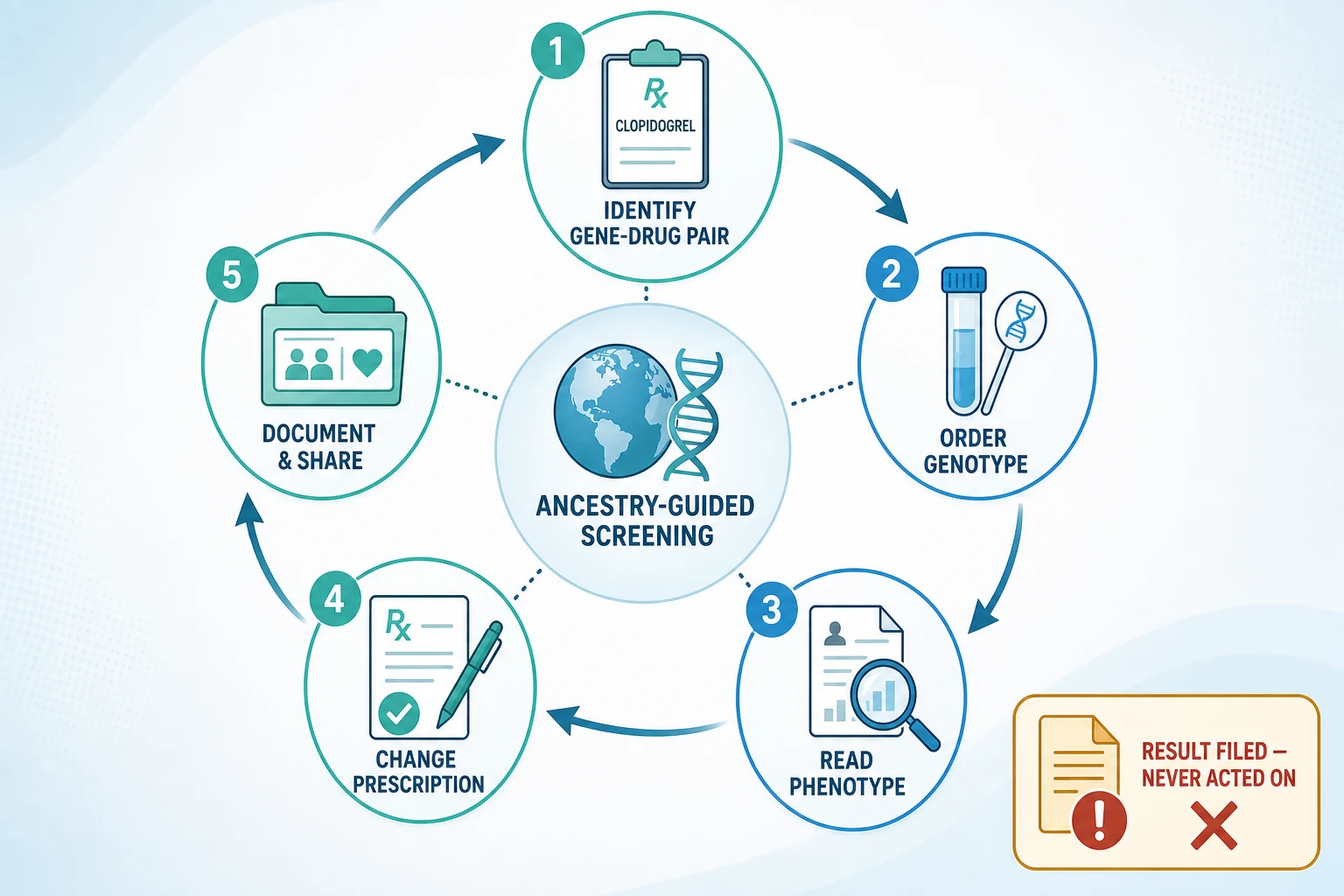
1 · Identify the gene-drug pair
Recognise the prescription that carries a CPIC-level pharmacogenomic risk — thiopurine, aromatic antiepileptic, codeine, abacavir.
2 · Order the genotype
Request TPMT and NUDT15, HLA-B star 15 colon 02, HLA-B star 57 colon 01, or CYP2D6 activity before the first dose when a result is available.
3 · Read the phenotype
Translate genotype into a metaboliser phenotype — poor, intermediate, normal, rapid, or ultrarapid — using the CPIC translation table.
4 · Change the prescription
Reduce the dose, choose an alternative drug, or avoid the drug entirely as the CPIC recommendation directs.
5 · Document and share
Record the result and the reason in the chart, flag it for future prescriptions, and tell the family in plain language.
Classification
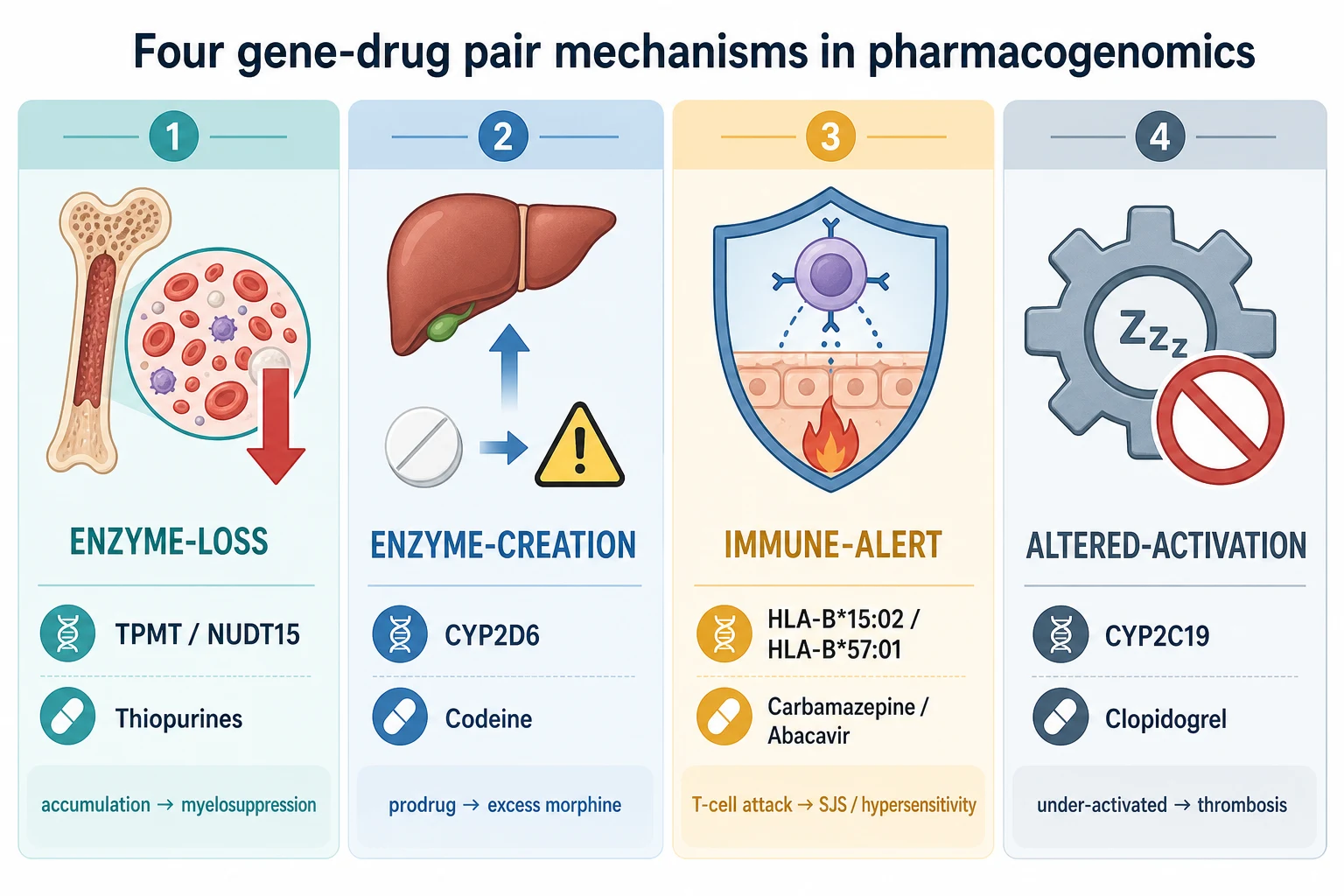
The gene-drug pairs a general paediatrician meets fall into four practical groups, and the group names the mechanism that puts the child at risk. Enzyme-loss pairs such as TPMT and NUDT15 with the thiopurines mean a child cannot clear the active drug and accumulates it to toxicity — myelosuppression. Enzyme-creation pairs such as CYP2D6 with codeine mean a child makes the active drug too fast, turning a harmless prodrug into an overdose. Immune-alert pairs such as HLA-B star 15 colon 02 with carbamazepine and HLA-B star 57 colon 01 with abacavir mean a drug-HLA complex triggers a T-cell attack on skin and viscera. Altered-activation pairs such as CYP2C19 with clopidogrel mean a prodrug is under-activated and the child is under-treated rather than poisoned. [1] [5] [9]
| Gene | Drug | Risk phenotype | Prescribing action |
|---|---|---|---|
| TPMT, NUDT15 | Azathioprine, 6-mercaptopurine, 6-thioguanine | Poor metaboliser — myelosuppression | Start at greatly reduced dose or choose alternative; never standard dose |
| CYP2D6 | Codeine, tramadol | Ultrarapid metaboliser — morphine overdose | Avoid codeine and tramadol in children under 12, and under 18 after tonsillectomy |
| HLA-B star 15 colon 02 | Carbamazepine, oxcarbazepine | Positive allele — Stevens-Johnson syndrome | Do not use carbamazepine or oxcarbazepine; choose an alternative antiepileptic |
| HLA-B star 57 colon 01 | Abacavir | Positive allele — hypersensitivity syndrome | Abacavir contraindicated; never rechallenge |
| CYP2C19 | Clopidogrel | Poor metaboliser — reduced active drug | Use an alternative antiplatelet if clinically indicated |
| G6PD | Rasburicase, dapsone, primaquine, sulphonamides | Deficient — haemolysis | Screen at-risk children before these drugs; avoid in deficiency |
Epidemiology & Risk Factors
Pharmacogenomic risk is unevenly distributed, and ancestry is the single most useful predictor at the bedside because allele frequencies differ sharply between populations. HLA-B star 15 colon 02 is carried by roughly 10 to 15 per cent of Han Chinese and people of Southeast Asian ancestry but by less than 1 per cent of Europeans, which is why carbamazepine Stevens-Johnson syndrome clusters in Asian populations and why screening is ancestry-directed. NUDT15 loss-of-function variants are common in East Asian and Hispanic children but rare in Europeans, which is why a child of Asian ancestry on a standard thiopurine dose can develop profound neutropenia that a European child on the same dose would not. [6] [8] [11]
The clinical situations that bring a pharmacogenomic decision into a general paediatric clinic are common. A new diagnosis of inflammatory bowel disease, nephrotic syndrome, autoimmune hepatitis, or juvenile dermatomyositis triggers an azathioprine or 6-mercaptopurine discussion and with it the TPMT and NUDT15 question. A new focal epilepsy in a child of Asian ancestry triggers the HLA-B star 15 colon 02 question before the first aromatic antiepileptic. A post-tonsillectomy analgesia plan triggers the codeine and CYP2D6 question. And the start of paediatric HIV care triggers the HLA-B star 57 colon 01 question before abacavir. [2] [5] [7]
Child of Asian ancestry
High-risk alleles
- HLA-B star 15 colon 02 in 10 to 15 per cent — carbamazepine SJS risk
- NUDT15 variants common — thiopurine myelosuppression risk
- Screen before carbamazepine and before thiopurines
- Ancestry guides the test, the result guides the drug
Oncology child
Thiopurine exposure
- Acute lymphoblastic leukaemia maintenance on 6-mercaptopurine
- TPMT and NUDT15 both tested before or at start
- Poor metaboliser needs a large dose reduction
- Additive toxicity when both genes are affected
Post-tonsillectomy child
Codeine trap
- CYP2D6 ultrarapid metaboliser converts codeine to excess morphine
- Postoperative opioid respiratory depression has killed children
- Codeine and tramadol contraindicated under 12 years
- Use non-opioid multimodal analgesia instead
Child starting abacavir
Immune-alert pair
- HLA-B star 57 colon 01 predicts abacavir hypersensitivity
- Screen before the first dose — mandatory in HIV care
- Positive result means abacavir is contraindicated
- Never rechallenge after a hypersensitivity reaction
Pathophysiology
The reason pharmacogenomics works is that a gene variant changes the amount of active drug that reaches its target, or changes whether the immune system recognises the drug as foreign. Four mechanisms cover almost every gene-drug pair you will meet, and each one maps to a prescribing action. [9]
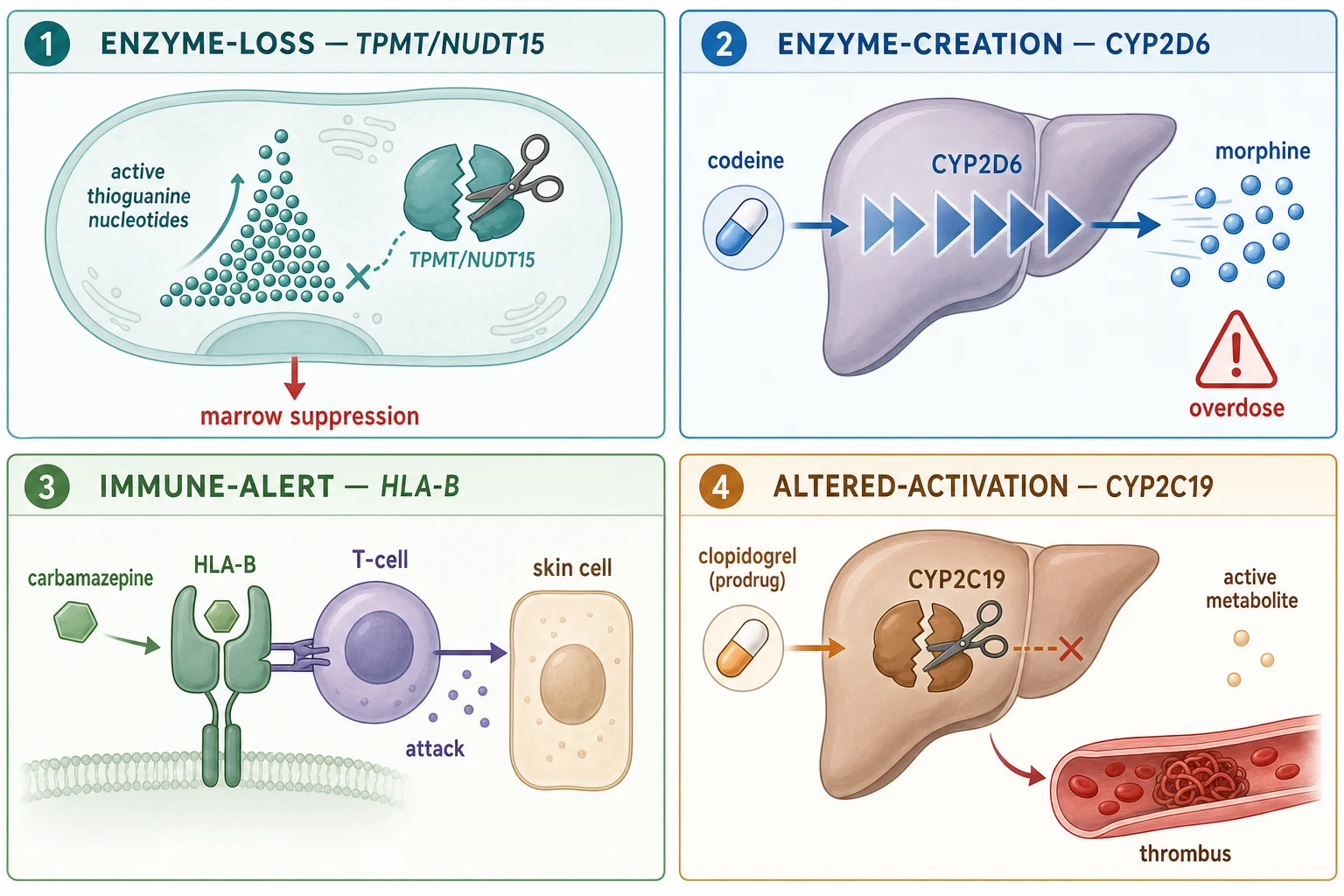
The thiopurine pathway is the archetype of enzyme-loss. Azathioprine and 6-mercaptopurine are converted inside the cell to active thioguanine nucleotides that kill proliferating lymphocytes and marrow precursors. Two enzymes clear them before they accumulate — thiopurine methyltransferase (TPMT) and NUDT15. A child who inherits two loss-of-function copies of either gene clears the drug slowly, the thioguanine nucleotides pile up, and the marrow is suppressed. A child with one loss-of-function copy clears it at an intermediate rate and needs a reduced dose. The 2018 CPIC update combines both genes, because a child can be affected through either or both, and the effects add up. [1] [11]
The codeine pathway is the archetype of enzyme-creation. Codeine itself is a weak analgesic; it must be converted by CYP2D6 into morphine to relieve pain. A CYP2D6 ultrarapid metaboliser — who inherits extra functional copies of the gene — converts codeine to morphine so fast that a therapeutic codeine dose produces a morphine overdose, with respiratory depression and death reported in tonsillectomised children. A poor metaboliser at the other extreme converts almost none and gets no analgesia. The CPIC opioid guideline maps CYP2D6, OPRM1, and COMT genotypes to the risk of opioid harm. [2] [3]
The HLA-mediated hypersensitivity pathway is the archetype of immune-alert. A drug or its metabolite binds the peptide-binding groove of a specific human-leucocyte-antigen allele, and the resulting drug-HLA-peptide complex is presented to T cells as foreign. HLA-B star 15 colon 02 presents carbamazepine and oxcarbazepine and triggers the keratinocyte apoptosis of Stevens-Johnson syndrome and toxic epidermal necrolysis, first described in Han Chinese by Chung and colleagues in 2004. HLA-B star 57 colon 01 presents abacavir and triggers a systemic hypersensitivity with fever, rash, and gastrointestinal and respiratory features that can be fatal on rechallenge. A positive result means the drug is contraindicated — not merely cautioned. [5] [6] [7]
Clinical Presentation
The clinical presentation of a pharmacogenomic adverse drug reaction is the child who has been harmed by a standard dose of a standard drug, and the pattern of harm names the mechanism. The child with severe mucositis, sepsis from neutropenia, or pancytopenia two to six weeks after starting azathioprine is showing you TPMT or NUDT15 deficiency. The toddler with blistering skin, target lesions, and mucosal erosion one to two weeks after starting carbamazepine is showing you HLA-B star 15 colon 02 positive Stevens-Johnson syndrome. The post-tonsillectomy child with bradypnoea, miosis, and unrousability on night two is showing you CYP2D6 ultrarapid codeine-to-morphine conversion. [1] [2] [6]
Each pharmacogenomic harm declares itself along a recognisable timeline. Thiopurine myelosuppression is delayed, appearing weeks into treatment as the active nucleotides accumulate and the marrow fails. Carbamazepine Stevens-Johnson syndrome appears within the first one to eight weeks of exposure, almost always early in the course. Codeine opioid toxicity appears within hours of the first or second dose, while the child still has an active prescription in the home. The abacavir hypersensitivity syndrome appears within the first six weeks and worsens with each dose, which is why rechallenge after a recognised reaction is so dangerous. [5] [7]
Differential Diagnosis
When a child on a standard drug develops an unexpected severe reaction, your first job is to decide whether the cause is pharmacogenomic, dose-related, interaction-related, or an unrelated disease. Four causes explain most out-of-character drug reactions, and only one of them is genetic. [9] [10]
The first cause to weigh is a pharmacogenomic reaction, identified by the characteristic pattern and timing — thiopurine cytopenia, aromatic-antiepileptic Stevens-Johnson syndrome in an Asian-ancestry child, codeine opioid toxicity in the postoperative period. The second is a dose or prescribing error — a child given an adult dose, a once-weekly drug given daily, or a decimal-point miscalculation. The third is a drug interaction — an enzyme inhibitor such as a macrolide or azole raising the level of a co-administered drug, or an inducer lowering it. The fourth is an unrelated diagnosis — a viral marrow suppression presenting during azathioprine therapy, or a febrile illness mimicking abacavir hypersensitivity. The pharmacogenomic result settles the question when it is positive; when it is negative, you return to dose, interaction, and disease. [9] [10]
The clopidogrel and CYP2C19 case is the mirror image, because here the child is under-treated rather than poisoned. A poor metaboliser activates too little clopidogrel and is exposed to thrombotic events that a normal metaboliser would not suffer, so the differential of a stent thrombosis on clopidogrel includes CYP2C19 loss of function alongside adherence and interaction. [4]
Clinical & Bedside Assessment
Bedside assessment of a pharmacogenomic question means asking, before the first dose, whether this child is one of the few for whom the standard prescription is dangerous. Five questions turn a routine prescription into a precision one. Which drug is planned, and does it carry a CPIC-level gene-drug pair? What is the child's ancestry, and does it raise the chance of a high-risk allele? Has a genotype been done before, and is the result in the chart? Is the family consanguineous, or is there a known familial adverse drug reaction? If I start the drug now, when will the genotype return, and can I wait? A prescription that cannot answer these when a test is available needs the test ordered first. [1] [10]
Confirming the indication and the alternative is where pharmacogenomic reasoning meets ordinary prescribing. A child who needs carbamazepine and tests HLA-B star 15 colon 02 positive still has epilepsy — the question is not whether to treat, but which drug to choose, and the answer is a non-aromatic alternative such as levetiracetam, valproate, or topiramate. A child who needs a thiopurine and tests poor metaboliser still has inflammatory bowel disease — the answer is a large dose reduction under specialist guidance, mycophenolate, or a biologic. Confirming the timing closes the loop: some results return within days and can precede the first dose, others return later and force a decision about whether to start cautiously while waiting. [5] [9]
GENE — the four paediatric pairs every registrar must name
Investigations
The investigation in pharmacogenomics is the genotype itself, ordered once and read against a CPIC translation table that converts it into a phenotype. TPMT and NUDT15 are requested together before azathioprine, 6-mercaptopurine, or 6-thioguanine, because either gene can cause thiopurine toxicity and the effects are additive. HLA-B star 15 colon 02 is requested before carbamazepine or oxcarbazepine in children of Asian ancestry, where the allele frequency justifies the screen. HLA-B star 57 colon 01 is requested before abacavir as a standard of HIV care. CYP2D6 is requested when a child unexpectedly reacts to or fails a CYP2D6-substrate drug, though the practical paediatric response to codeine is to avoid it rather than to test. [1] [5] [7]
| Drug planned | Test to order | Phenotype categories | Decision rule |
|---|---|---|---|
| Azathioprine, 6-mercaptopurine, 6-thioguanine | TPMT and NUDT15 genotype | Poor, intermediate, normal metaboliser | Poor: avoid or reduce by 90 per cent; intermediate: reduce |
| Carbamazepine, oxcarbazepine (Asian ancestry) | HLA-B star 15 colon 02 | Positive or negative | Positive: do not use; choose alternative antiepileptic |
| Abacavir | HLA-B star 57 colon 01 | Positive or negative | Positive: contraindicated; never rechallenge |
| Codeine, tramadol | CYP2D6 activity | Poor to ultrarapid | Ultrarapid: avoid; practical rule is to avoid in all under 12 |
| Clopidogrel | CYP2C19 genotype | Poor to ultrarapid | Poor metaboliser: consider alternative antiplatelet |
| Rasburicase, dapsone, primaquine | G6PD activity (enzyme assay) | Deficient or normal | Deficient: avoid oxidant drug; haemolysis risk |
A pharmacogenomic genotype is usually a once-in-a-lifetime test, because the germline variant does not change. That is both its strength and its weakness — a single result can guide every future prescription, but it must be recorded in a place the next prescriber can find, flagged on the chart, and shared with the family as part of their personal medicines record. Pre-emptive panels that genotype a dozen genes once and file the result for future use have been shown in the PREPARE trial to reduce clinically relevant adverse drug reactions by about 30 per cent, which is why panel testing is expanding in specialist paediatric services. [9] [10]
Management — Resuscitation
The resuscitation moment in pharmacogenomics is the child who has already been harmed by a gene-drug mismatch and arrives acutely unwell. The first action is to stop the offending drug: withhold the next azathioprine dose in the neutropenic child, stop carbamazepine immediately in the child with Stevens-Johnson syndrome, stop codeine and give naloxone for opioid respiratory depression, and stop abacavir at the first sign of hypersensitivity. Supportive care follows — broad-spectrum antibiotics for neutropenic sepsis, fluid and wound care and ophthalmology for Stevens-Johnson syndrome, airway and breathing support for opioid depression. [1] [5] [6]
The immediate management of carbamazepine Stevens-Johnson syndrome is a dermatology and critical-care emergency, not a medication-adjustment task. Stop the drug, admit for fluid, electrolyte, wound, and ocular care, and arrange specialist transfer if the body-surface area involved is large. The immediate management of thiopurine myelosuppression is to stop the drug, manage neutropenic sepsis with broad-spectrum antibiotics, and support with transfusion as needed; the marrow usually recovers as the active nucleotides clear over days to weeks. [6] [11]
Management — Definitive & Stepwise
The definitive management of a pharmacogenomic result is to change the prescription before harm, using the CPIC recommendation for that gene-drug pair. For the thiopurines, a TPMT or NUDT15 poor metaboliser should not receive a standard starting dose — the 2018 CPIC update recommends starting at a greatly reduced dose, typically around 10 per cent of standard, or choosing an alternative immunosuppressant, with full blood-count monitoring from the outset. Intermediate metabolisers start at a reduced dose. A normal metaboliser uses the standard dose. Both genes are tested, because their effects add up, and a 2024 multiethnic study in children with acute lymphoblastic leukaemia confirmed that combined TPMT and NUDT15 deficiency produces the most severe thiopurine toxicity. [1] [8] [11]
Prescribing actions by gene-drug pair (verify against the current CPIC guideline and local formulary)
For codeine and tramadol, the safest paediatric rule does not wait for a genotype. Because the CYP2D6 ultrarapid phenotype cannot be inferred from the bedside, and because postoperative codeine has killed children, codeine and tramadol are avoided in all children under twelve years, in all breastfeeding mothers, and in all children under eighteen after tonsillectomy or adenoidectomy. The CPIC opioid guideline sets the pharmacogenomic detail; the practical prescribing rule is to use non-opioid multimodal analgesia, with a non-codeine opioid reserved for breakthrough pain in the right setting. [2] [3]
For carbamazepine and oxcarbazepine, a child who is HLA-B star 15 colon 02 positive should not receive either drug, because the risk of Stevens-Johnson syndrome is high and the alternatives are effective. A child who is negative is not fully protected — HLA-B star 15 colon 02 accounts for most but not all cases — but the screen has reduced the incidence of carbamazepine Stevens-Johnson syndrome in screened Asian populations. For abacavir, a child who is HLA-B star 57 colon 01 positive must never receive the drug, and a child who has had a clinically recognised abacavir hypersensitivity reaction must never be rechallenged, because rechallenge can be fatal regardless of genotype. [5] [7]
Specific Subtypes & Scenarios
The oncology child on maintenance 6-mercaptopurine for acute lymphoblastic leukaemia is the patient where thiopurine pharmacogenomics is most life-critical, because the drug is given daily for years at a dose that balances leukaemia control against marrow toxicity. Yang and colleagues showed that an inherited NUDT15 variant is a determinant of mercaptopurine intolerance in children, and Maillard and colleagues confirmed in 2024 that TPMT and NUDT15 effects are additive across multiethnic populations, so a child affected at both genes is at the highest risk of all. Testing is now standard before or at the start of maintenance, and the dose is individualised to the genotype as well as to the white-cell count. [8] [11]
The precision-prescribing timeline for a child starting azathioprine for Crohn disease
The child of Asian ancestry starting an aromatic antiepileptic is the patient where HLA pharmacogenomics is most life-critical. The HLA-B star 15 colon 02 screen before carbamazepine, oxcarbazepine, and the structurally related aromatic anticonvulsants is now standard in populations where the allele is common, and a positive result shifts the choice to a non-aromatic alternative. The child starting abacavir in paediatric HIV care is screened for HLA-B star 57 colon 01 as a routine standard, because abacavir hypersensitivity is severe and the screen is highly predictive. The child on clopidogrel after a cardiac or neurovascular stent is the patient where CYP2C19 loss of function shifts the choice of antiplatelet, though the practical decision is usually made with the cardiology or neurology team. [4] [5] [7]
Complications & Pitfalls
The complications of untreated pharmacogenomic risk are the severe adverse drug reactions the discipline exists to prevent — thiopurine myelosuppression with neutropenic sepsis, carbamazepine and oxcarbazepine Stevens-Johnson syndrome and toxic epidermal necrolysis, codeine and tramadol opioid respiratory depression, and abacavir hypersensitivity with the danger of rechallenge. When pharmacogenomic testing is done and acted on, most of these are preventable. Stevens-Johnson syndrome carries a real mortality, and neutropenic sepsis from thiopurine myelosuppression has killed children who should have been tested first. [1] [6] [11]
Four pitfalls undermine pharmacogenomics at the bedside. The first is the untested start — the thiopurine or carbamazepine begun without a genotype when a result was available. The second is the result not acted on — the positive report filed in the chart while the original prescription carries on, which is the most common and most dangerous failure of all. The third is the ancestry-blind screen — failing to test a child of Asian ancestry for HLA-B star 15 colon 02 before carbamazepine, or a child of Asian or Hispanic ancestry for NUDT15 before a thiopurine, because the allele frequency that justifies the screen was not considered. The fourth is the misread phenotype — confusing poor with ultrarapid, or assuming a negative HLA result gives total protection when it only accounts for most cases. [5] [9] [10]
Principle
- Use inherited gene variants to choose a drug and dose before the first dose
- Act on gene-drug pairs with a CPIC-level evidence base
- Mechanism names the danger — loss, creation, immune-alert, altered-activation
Pairs
- TPMT and NUDT15 with thiopurines — myelosuppression
- CYP2D6 with codeine and tramadol — opioid overdose
- HLA-B star 15 colon 02 with carbamazepine and oxcarbazepine — SJS
- HLA-B star 57 colon 01 with abacavir — hypersensitivity
- CYP2C19 with clopidogrel — under-activation
Actions
- Thiopurine poor metaboliser: avoid standard dose or start at about 10 per cent
- Codeine and tramadol avoided under 12 years, under 18 after tonsillectomy
- HLA-B star 15 colon 02 positive: do not use carbamazepine or oxcarbazepine
- HLA-B star 57 colon 01 positive: abacavir contraindicated, never rechallenge
Ancestry
- HLA-B star 15 colon 02 in 10 to 15 per cent of Han Chinese
- NUDT15 loss-of-function common in East Asian and Hispanic children
- Ancestry guides the test, the result guides the drug
Process
- Order the genotype before the first dose when a pair is in play
- Read the phenotype, change the prescription, document the reason
- Flag the chart and share with the family
- Result filed and never acted on is the classic failure
Pitfalls
- Untested start
- Positive result not acted on
- Ancestry-blind screen
- Misread phenotype — poor versus ultrarapid, negative does not mean total protection
“Identify the gene-drug pair → order the genotype → read the phenotype → change the prescription → document and share — and never let a positive result sit in the chart while the original prescription carries on.”
Prognosis & Disposition
The prognosis of a pharmacogenomic adverse drug reaction depends on whether the offending drug was stopped early and whether supportive care was prompt. Thiopurine myelosuppression usually recovers over days to weeks once the drug is withheld, but neutropenic sepsis during the nadir is the life-threatening event that determines outcome. Carbamazepine Stevens-Johnson syndrome carries a mortality that rises with body-surface-area involvement and continues to affect skin, eye, and visceral recovery for months. Codeine opioid respiratory depression is rapidly reversible with naloxone if recognised, and fatal if not. Abacavir hypersensitivity resolves on withdrawal but is fatal on rechallenge. [6] [7]
Disposition is intertwined with whether the child has been harmed or is being protected prospectively. A child who has developed thiopurine neutropenia needs admission for neutropenic-sepsis management and a re-plan of immunosuppression under specialist guidance. A child who has developed Stevens-Johnson syndrome needs dermatology and critical-care admission and a permanent change of antiepileptic. A child who is being started prospectively with a known genotype needs outpatient follow-up that documents the result, the chosen alternative, and the plan for future prescriptions, because the genotype will be relevant for life. [9] [10]
The long-term disposition question is whether the child should carry a pharmacogenomic result in their personal medicines record and whether a broader panel is justified. Pre-emptive panel testing — genotyping a dozen genes once and filing the result for future prescriptions — has been shown to reduce clinically relevant adverse drug reactions by about 30 per cent in the PREPARE trial, and is increasingly available in specialist paediatric services. [10]
Special Populations
The oncology child on maintenance thiopurine is the patient where the dose, the genotype, and the white-cell count are managed together for years. Both TPMT and NUDT15 are tested, the starting dose is individualised to the genotype, and the maintenance dose is titrated to the white-cell count as well as to leukaemia control. A 2024 multiethnic study confirmed that the two genes act additively, so a child affected at both is at the highest risk. The child of Asian or Hispanic ancestry is the patient where NUDT15 screening is most important before any thiopurine, because loss-of-function variants are common and a standard dose causes profound neutropenia. [8] [11]
The child of Asian ancestry starting an aromatic antiepileptic is the patient where HLA-B star 15 colon 02 screening is most important, because the allele is common and Stevens-Johnson syndrome is severe. The child starting abacavir in paediatric HIV care is screened for HLA-B star 57 colon 01 as a routine standard, and a positive result shifts the regimen. The child in a remote or disadvantaged setting may not have rapid access to a genotype, and the safe response is to choose a drug that does not require a pharmacogenomic screen where one is available, while arranging the test for the prescriptions that do. [5] [7] [10]
Australia and Aotearoa New Zealand: the Royal Children's Hospital Melbourne clinical practice guidelines and the CPIC gene-drug pair recommendations set the framework, with state and institutional laboratories operationalising TPMT, NUDT15, and HLA testing. For Aboriginal and Torres Strait Islander and Māori children, and for children of Pacific and Southeast Asian ancestry, the relevant allele frequencies differ from European populations and the screen must be guided by ancestry rather than by a default European reference. Communication of a pharmacogenomic result to a family whose first language is not English needs an interpreter and a written plain-language summary, because the result is permanent and will be relevant for future prescriptions. [1] [5]
Global and low-resource settings: where a genotype is not rapidly available, the safe response is to choose a drug that does not require a pharmacogenomic screen where one exists, and to apply the practical rules that do not need a result — avoid codeine and tramadol in young children, reduce the thiopurine starting dose cautiously with close full-blood-count monitoring, and screen for G6PD deficiency before oxidant drugs. The CPIC gene-drug pair framework holds globally; the capacity to test is what differs. [9] [10]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric pharmacogenomics rests on three lines of work. The first is the mechanistic and association studies that linked a gene variant to a drug outcome — Chung and colleagues in 2004 identifying HLA-B star 15 colon 02 as the marker for carbamazepine Stevens-Johnson syndrome, Mallal and colleagues in 2002 linking HLA-B star 57 colon 01 to abacavir hypersensitivity, and Yang and colleagues in 2015 showing NUDT15 as a determinant of mercaptopurine intolerance in children. These established the biology that the prescribing rules now act on. [6] [7] [8]
The second is the implementation guidelines published by the Clinical Pharmacogenetics Implementation Consortium, which translate a genotype into a phenotype and a prescribing action for each gene-drug pair. The 2018 thiopurine update combined TPMT and NUDT15 into one recommendation; the CYP2D6 codeine and opioid guidelines underpin the age-based avoidance; the HLA carbamazepine and oxcarbazepine update guides the aromatic-antiepileptic screen; the 2022 clopidogrel update refines the CYP2C19 action. Relling and Evans set the wider framework for pharmacogenomics in the clinic in 2015. [1] [2] [4] [5] [9]
The third is the implementation-outcome evidence that acting on pharmacogenomic results reduces harm. The PREPARE trial published in 2023 randomised clinics to a pre-emptive twelve-gene panel versus usual care and showed about a 30 per cent reduction in clinically relevant adverse drug reactions, which is the strongest evidence yet that pre-emptive testing changes outcomes and not just decisions. The 2024 multiethnic TPMT and NUDT15 study extended the thiopurine evidence to children across populations. [10] [11]
The evidence is weaker where ancestry-specific allele frequencies, paediatric pharmacokinetics, and paediatric outcome data are sparse — many gene-drug pairs were characterised in adults and extrapolated to children, and the prescribing rules for a child may differ from those for an adult because of developmental pharmacokinetics. Where the evidence is weaker, state the action, cite the CPIC guideline and the formulary, and communicate the uncertainty to the family rather than implying a certainty the data do not support. [9] [10]
Board and assessment distinctions
RACP current PREP curriculum candidates must apply safe prescribing and medication-safety principles within the acute-illness and pharmacology learning objectives, and pharmacogenomics is an emerging feature of the renewed first-year curriculum from 2027. RCPCH Progress+ embeds safe prescribing and the use of pharmacogenomic information as a patient-safety outcome. The ABP General Pediatrics Content Outline covers pharmacology and medication management, including precision prescribing. [9]
| Board or format | What the candidate must demonstrate |
|---|---|
| RACP DWE | Name the gene-drug pairs, recognise the risk phenotype, and choose the prescribing action |
| RACP DCE long case | Build a precision-prescribing plan for a child starting a thiopurine, an aromatic antiepileptic, or abacavir |
| MRCPCH clinical | Explain a pharmacogenomic result and the change of prescription to a family in plain language |
| ABP | Apply pharmacology-domain knowledge to identify, test, and act on a gene-drug pair |
| RCPSC structured oral | Defend a TPMT and NUDT15-guided thiopurine plan or an HLA-guided antiepileptic choice across ancestries |
Exam Pearls
Viva: why is codeine contraindicated in children under twelve, and after tonsillectomy under eighteen?
Codeine is a weak analgesic that must be converted by CYP2D6 into morphine to work. A child who is a CYP2D6 ultrarapid metaboliser — inheriting extra functional copies of the gene — converts a therapeutic codeine dose into a morphine overdose, and postoperative codeine has caused fatal respiratory depression in tonsillectomised children. Because you cannot tell at the bedside who is an ultrarapid metaboliser, the safe rule is to avoid codeine and tramadol in all children under twelve years, in breastfeeding mothers, and in all children under eighteen after tonsillectomy or adenoidectomy, and to use non-opioid multimodal analgesia instead. The CPIC opioid guideline sets the pharmacogenomic detail, but the practical rule does not wait for a genotype. [2] [3]
Structured oral: a child of Han Chinese ancestry needs carbamazepine for epilepsy
Before the first dose, screen for HLA-B star 15 colon 02, because the allele is carried by roughly 10 to 15 per cent of Han Chinese and is strongly associated with carbamazepine Stevens-Johnson syndrome, as Chung and colleagues first described in 2004. If the result is positive, do not use carbamazepine or oxcarbazepine — choose a non-aromatic alternative such as levetiracetam, valproate, or topiramate, because the child still has epilepsy and still needs treatment. If the result is negative, carbamazepine can be used with the usual monitoring, but remember that HLA-B star 15 colon 02 accounts for most but not all cases of carbamazepine Stevens-Johnson syndrome. The CPIC 2017 update guides the action; the screen has reduced the incidence of carbamazepine Stevens-Johnson syndrome in screened Asian populations. [5] [6]
References
- [1]Relling MV, Schwab M, Whirl-Carrillo M Clinical Pharmacogenetics Implementation Consortium Guideline for Thiopurine Dosing Based on TPMT and NUDT15 Genotypes: 2018 Update. Clinical pharmacology and therapeutics, 2019.PMID 30447069
- [2]Crews KR, Gaedigk A, Dunnenberger HM Clinical Pharmacogenetics Implementation Consortium guidelines for cytochrome P450 2D6 genotype and codeine therapy: 2014 update. Clinical pharmacology and therapeutics, 2014.PMID 24458010
- [3]Crews KR, Monte AA, Huddart R Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2D6, OPRM1, and COMT Genotypes and Select Opioid Therapy. Clinical pharmacology and therapeutics, 2021.PMID 33387367
- [4]Lee CR, Luzum JA, Sangkuhl K Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2C19 Genotype and Clopidogrel Therapy: 2022 Update. Clinical pharmacology and therapeutics, 2022.PMID 35034351
- [5]Phillips EJ, Sukasem C, Whirl-Carrillo M Clinical Pharmacogenetics Implementation Consortium Guideline for HLA Genotype and Use of Carbamazepine and Oxcarbazepine: 2017 Update. Clinical pharmacology and therapeutics, 2018.PMID 29392710
- [6]Chung WH, Hung SI, Hong HS Medical genetics: a marker for Stevens-Johnson syndrome. Nature, 2004.PMID 15057820
- [7]Mallal S, Nolan D, Witt C Association between presence of HLA-B*5701, HLA-DR7, and HLA-DQ3 and hypersensitivity to HIV-1 reverse-transcriptase inhibitor abacavir. Lancet (London, England), 2002.PMID 11888582
- [8]Yang JJ, Landier W, Yang W Inherited NUDT15 variant is a genetic determinant of mercaptopurine intolerance in children with acute lymphoblastic leukemia. Journal of clinical oncology, 2015.PMID 25624441
- [9]Relling MV, Evans WE Pharmacogenomics in the clinic. Nature, 2015.PMID 26469045
- [10]Swen JJ, van der Wouden CH, Manson LE A 12-gene pharmacogenetic panel to prevent adverse drug reactions: an open-label, multicentre, controlled, cluster-randomised crossover implementation study. Lancet (London, England), 2023.PMID 36739136
- [11]Maillard M, Nishii R, Yang W Additive effects of TPMT and NUDT15 on thiopurine toxicity in children with acute lymphoblastic leukemia across multiethnic populations. Journal of the National Cancer Institute, 2024.PMID 38230823