Paeds · clinical-pharmacology-and-therapeutics
Poisoning antidotes and toxicology pharmacology
Also known as Paediatric antidotes pharmacology · NAC acetylcysteine for paracetamol poisoning · Naloxone for opioid toxicity · Snake antivenom in children · Chelation therapy deferoxamine succimer · Toxidromes and antidote mechanisms
A fellowship approach to poisoning antidotes and toxicology pharmacology in children, covering the four mechanism classes of antidote, the toxidrome-driven bedside assessment, N-acetylcysteine for paracetamol poisoning, naloxone for opioid-induced respiratory depression, snake and other antivenoms, and chelation therapy for iron and lead. It gives weight-based doses and routes, the receptor, substrate, and binding mechanisms each antidote exploits, and the monitoring and pitfalls of reversing a toxin in a child.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A toddler who has drunk grandma's iron tablets, a teenager unconscious from an opioid, a country child bitten by a brown snake — these are the children whose survival turns on a single substance given at the right moment. An antidote is a medicine that counteracts a specific toxin by a defined pharmacological mechanism, and although few poisoned children need one, the child who does needs it without delay. The paediatric pharmacology of antidotes is therefore the science of matching a poison to its reversal agent by weight, route, mechanism, and timing, layered on the bedrock of airway, breathing, and circulation. [3] [8]
The discipline sits between the clinical toxicology topics — paracetamol poisoning, iron and salicylate poisoning, opioid and recreational drug toxicity, and envenomation — which carry the full management of each toxin, and the general prescribing topics which carry dose calculation and medication safety. This hub distils what is common across them: how antidotes work, how to dose them in a child, how to choose among them at the bedside, and how to monitor and avoid their own harms. A fellowship candidate must hold four mechanism classes, five named antidotes with their weight-based doses, and the toxidrome pattern that triggers each one. [1] [3]
The reason mechanism matters is that an antidote is not a generic antidote. Naloxone reverses an opioid because it competes for the mu-receptor; it does nothing for a benzodiazepine or an iron tablet. N-acetylcysteine works for paracetamol because it replenishes the glutathione that the toxic metabolite consumes; it does nothing for a snakebite. Deferoxamine binds iron atom-for-atom and is useless against lead, which needs succimer or EDTA. The candidate who reaches for an antidote without naming its mechanism is reaching in the dark, and in a child that darkness can be lethal. [8] [10]
From a poisoned child to the right antidote
1 · Resuscitate
Secure the airway, support breathing with bag-valve-mask if the rate or effort is inadequate, and restore circulation with fluid boluses. An antidote never precedes the ABCDE assessment.
2 · Identify the toxin
Take a focused history — what, how much, when, by what route — and examine for a toxidrome. Call the regional poison information centre early for any unknown or mixed ingestion.
3 · Match the mechanism
Decide whether the antidote must occupy a receptor, bind the toxin, restore a substrate, or supply antibody. The mechanism dictates the agent and the dose interval.
4 · Give the weight-based dose
Calculate every antidote dose from the child's weight, give it by the correct route, and titrate where the drug has a narrow margin — naloxone to respiratory rate, N-acetylcysteine to the protocol.
5 · Monitor and reassess
Watch for both recurrence of toxicity and for antidote adverse effects. Many antidotes are shorter-acting than the toxin they reverse, so renarcotisation and rebound are real risks.
Classification
Antidotes sort neatly into four mechanism families, and the candidate who memorises these four families can reason out almost any toxin. Receptor antagonists displace the toxin from its receptor — naloxone at the mu-opioid receptor, flumazenil at the benzodiazepine site. Binding agents seize the toxin directly — chelators wrap a metal atom, and digoxin-specific Fab fragments bind a digoxin molecule. Substrate and metabolism restorers replenish what the toxin consumed or block the enzyme that makes it toxic — N-acetylcysteine refills glutathione, and fomepizole blocks alcohol dehydrogenase. Antibody therapy supplies immunoglobulin that neutralises venom or a biological toxin. [1] [3]
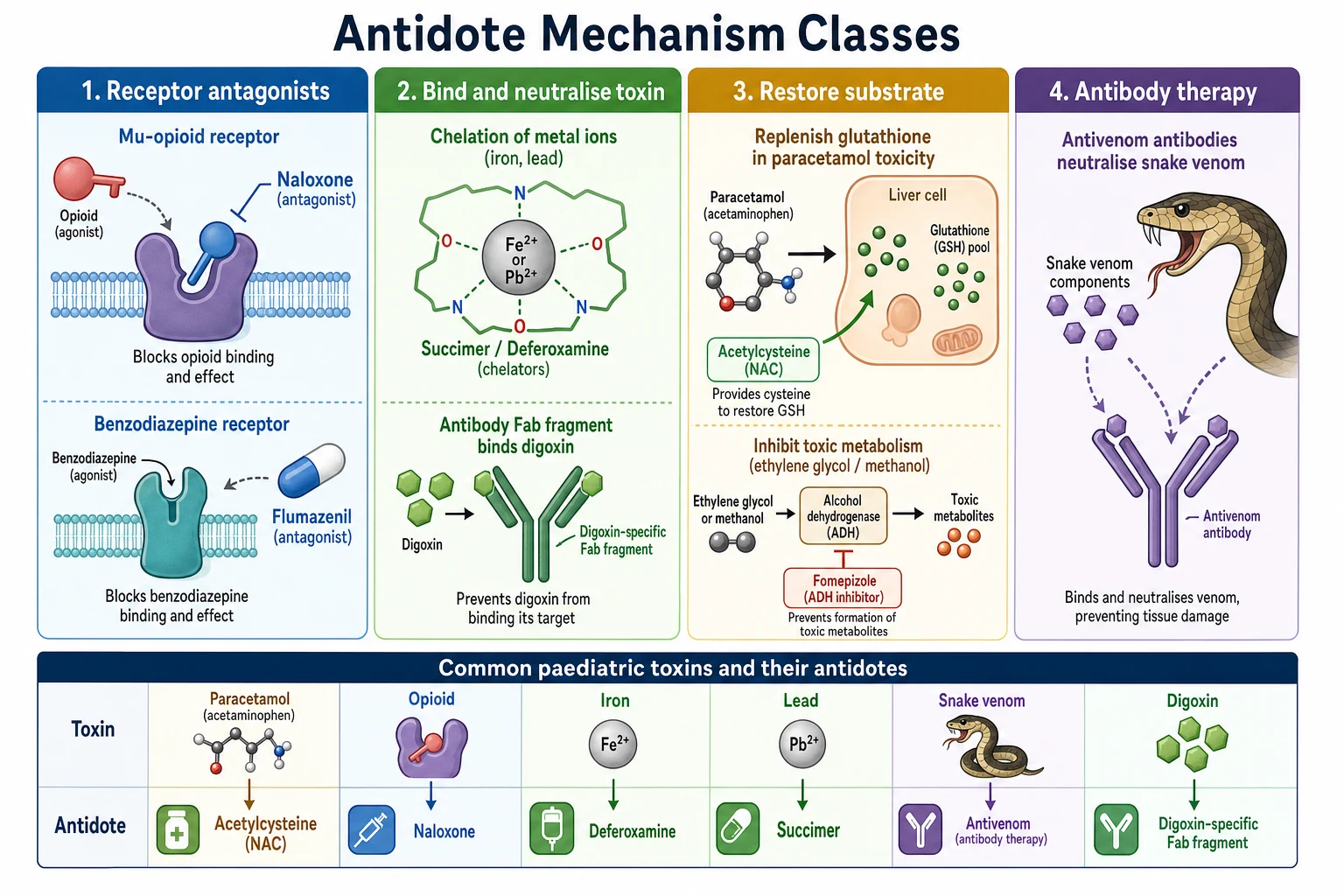
The practical teaching point is that mechanism predicts behaviour. A receptor antagonist like naloxone is fast but short, because it competes and then washes out while the opioid persists — hence renarcotisation. A binding agent like deferoxamine works for as long as it is infused and there is free metal to bind. A substrate restorer like N-acetylcysteine must be given before the toxic metabolite has done irreversible damage, which is why timing governs paracetamol antidote use. An antibody like antivenom is dosed by the amount of venom to neutralise, not by the child's weight alone. [4] [8]
| Antidote | Toxin | Mechanism class | Key paediatric point |
|---|---|---|---|
| N-acetylcysteine | Paracetamol | Substrate restorer | IV 150 then 50 then 100 mg/kg over 21 h; anaphylactoid reaction common and rate-related |
| Naloxone | Opioid | Receptor antagonist | 10 microgram/kg titrated to respiratory rate; short half-life, watch for renarcotisation |
| Snake antivenom | Snake venom | Antibody therapy | Species-specific; IV; give early for systemic envenomation; anaphylactoid risk |
| Deferoxamine | Iron | Binding agent (chelator) | IV 15 mg/kg/h; vin-rose urine; start when toxicity present |
| Succimer (DMSA) | Lead | Binding agent (chelator) | Oral for moderate lead; chelation lowers levels but the TLC trial showed no neuropsychological benefit at low-moderate exposure |
| Digoxin-specific Fab | Digoxin | Binding agent (antibody) | Dose by digoxin load or serum level; life-saving for digoxin and related cardiotoxins |
| Fomepizole | Methanol, ethylene glycol | Metabolism blocker | Blocks alcohol dehydrogenase to stop toxic acid formation; first-line over ethanol |
| Flumazenil | Benzodiazepine | Receptor antagonist | Dangerous in chronic users — can precipitate seizures; not a routine reversal agent |
[1] [6] [10] Doses are indicative weight-based ranges drawn from AMH Children's Dosing Companion, BNFc, and RCH Melbourne Clinical Practice Guidelines; always confirm against the current formulary and the poison information centre for the child's age and weight.
Epidemiology & Risk Factors
Poisoning is among the commonest reasons a young child presents to an emergency department, and most ingestions are exploratory and trivial. The peak age is the toddler — one to four years — who can reach and open a container but cannot read or judge danger, and whose weight means that an adult dose is a large dose per kilogram. A small number of these children become seriously unwell, and it is in that small number that an antidote becomes the difference between recovery and death. [8] [9]
The children most at risk of severe poisoning are predictable. The toddler with access to a grandparent's medicines — iron, digoxin, opioids — takes the largest single danger, because these are the agents for which an antidote is essential. The adolescent with intentional self-harm takes staggered or mixed overdoses where timing is uncertain and several toxins may be in play. The opioid-exposed or opioid-tolerant child is at risk both of overdose and of withdrawal if naloxone is given too aggressively. And the rural or remote child exposed to venom or agricultural chemicals may be hours from definitive care, so early antidote advice by phone is part of the rescue. [3] [7]
Exploratory toddler
Unintentional single ingestion
- Most ingestions are trivial and need no antidote
- Iron, digoxin, and opioids are the dangerous exceptions
- Weight-based dosing matters — an adult tablet is a large dose
- Activated charcoal if within one hour and airway is safe
Adolescent overdose
Intentional, mixed, staggered
- Timing often unknown — treat paracetamol regardless of level
- Multiple toxins possible — toxidrome may be mixed
- Mental-health assessment is part of disposition
- Higher risk of hepatotoxicity from delayed presentation
Opioid-tolerant child
Chronic opioid or substitution therapy
- Low-dose naloxone to avoid precipitating withdrawal
- May need a naloxone infusion for long-acting opioids
- Monitor for renarcotisation as naloxone wears off
- Under-treatment of pain is also a harm
Envenomated child
Rural or remote
- Time to antivenom drives outcome
- Call poison centre for species identification and dose
- Pressure-immobilisation for Australian elapids
- Anaphylactoid reaction to antivenom possible
Pathophysiology
Antidote pharmacology is the pharmacology of reversal, and each reversal works at a defined molecular site. A toxin produces harm by binding a receptor, by depleting a substrate, by disrupting an enzyme, or by damaging tissue directly, and the antidote intervenes at whichever step is reversible. Understanding the step tells you whether an antidote can work at all, how fast, and for how long. [1] [3]
Paracetamol is the paradigm of substrate depletion. At therapeutic doses paracetamol is cleared by glucuronidation and sulfation, with a small fraction metabolised by cytochrome P450 2E1 into the reactive intermediate NAPQI, which is immediately detoxified by glutathione. After an overdose the conjugation pathways saturate, more paracetamol is shunted into the P450 pathway, NAPQI accumulates, glutathione is depleted, and free NAPQI binds hepatocyte proteins and causes centrilobular necrosis. N-acetylcysteine works by replenishing glutathione and by supplying sulfhydryl groups that directly detoxify NAPQI — but only while the hepatocyte is still salvageable, which is why timing governs its use. [1] [2]
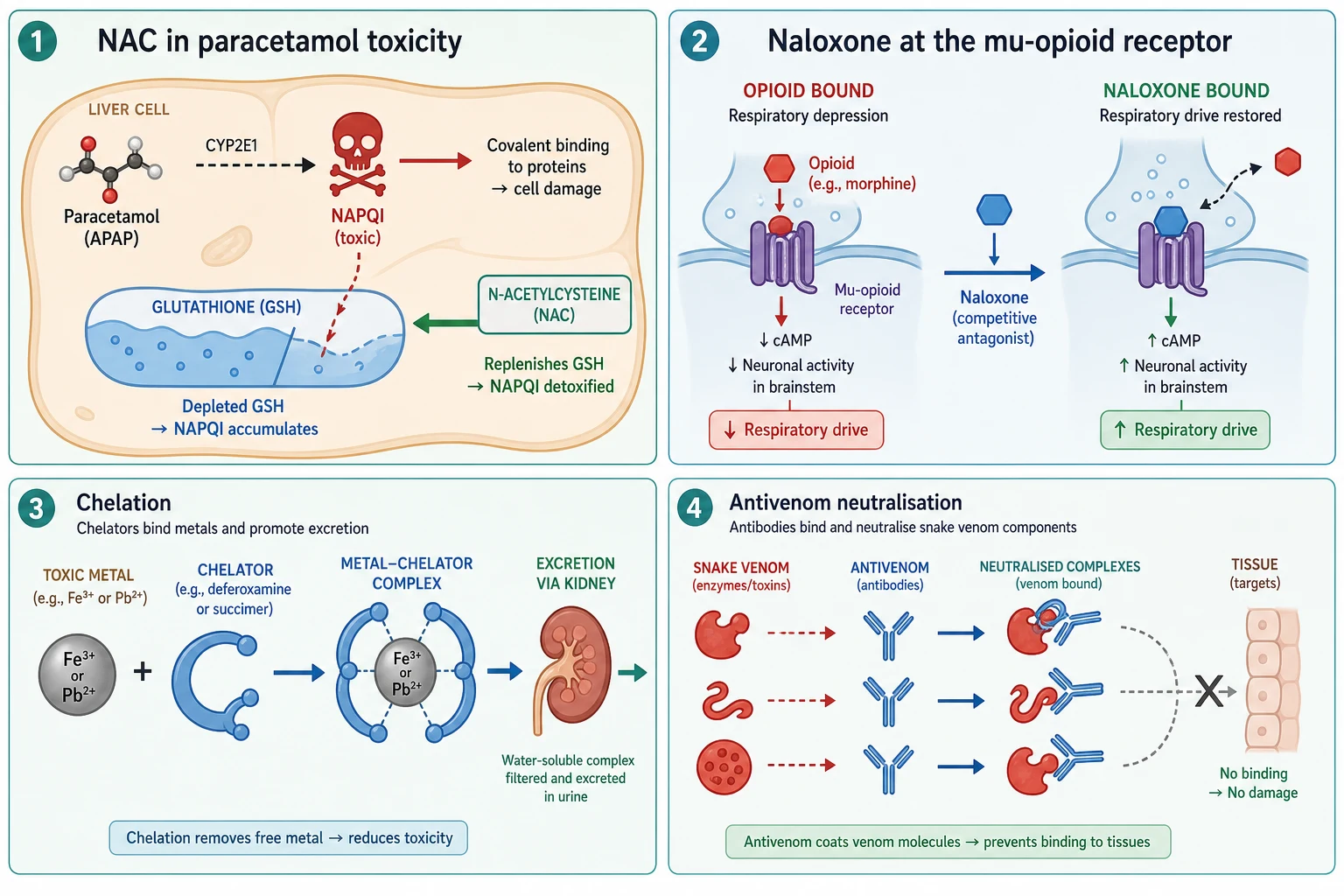
Opioids are the paradigm of receptor competition. An opioid agonises the mu-opioid receptor in the brainstem respiratory centre, reducing respiratory drive and producing the classic toxidrome of sedation, miosis, and hypoventilation. Naloxone is a competitive mu-receptor antagonist: it displaces the opioid from the receptor and restores respiratory drive within minutes. Because naloxone has a short half-life of roughly 30 to 80 minutes — shorter than most opioids — it wears off while the opioid persists, and the child can re-sedate. This pharmacokinetic mismatch is why naloxone is titrated to respiratory rate and why an infusion is sometimes needed for long-acting opioids. [3] [4]
Iron is the paradigm of direct tissue toxicity and chelation. Free iron damages mitochondria and the gastric mucosa, produces a metabolic acidosis, and in severe poisoning causes shock and hepatotoxicity. Deferoxamine binds free ferric iron atom-for-atom to form the water-soluble ferrioxamine complex, which is excreted in the urine and turns it a characteristic vin-rose colour. Chelation removes only free iron, so it must be started while iron is still circulating before it has distributed into the cell. [8] [9]
Lead poisons by binding sulfhydryl groups and disrupting enzyme function, especially in the developing nervous system, and chelation with succimer or calcium-EDTA increases lead excretion. The crucial pharmacological caveat is the Treatment of Lead-Exposed Children trial, which found that succimer lowered blood lead levels but did not improve neuropsychological outcome at low-to-moderate exposure — chelation is reserved for higher levels or symptomatic poisoning, not for every elevated level. [10] [11]
Snake venom is a mixture of enzymes — procoagulants, neurotoxins, myotoxins — that circulate and attack specific tissues. Antivenom is purified animal-derived antibody, either whole immunoglobulin or Fab fragments, that binds and neutralises the circulating venom so it can no longer reach its target. Because antivenom does not reverse damage already done, early administration before tissue injury is established is the principle that governs its use. [6] [7]
Clinical Presentation
A poisoned child presents with a toxidrome — a cluster of signs that points to a receptor or mechanism — and the toxidrome, more than the history, often selects the antidote. The history may be absent, inaccurate, or mixed, but the examination reveals the physiology. The candidate must know the five core toxidromes cold and the antidote each one demands. [3]
The opioid toxidrome is sedation, pin-point pupils (miosis), and reduced respiratory rate and depth, and it is the one that demands naloxone. The earliest and most reliable sign is a falling respiratory rate with rising sedation; oxygen saturation falls late and is an unreliable sentinel. The anticholinergic toxidrome is the opposite — mydriasis, dry mouth and skin, flushed face, urinary retention, tachycardia, and delirium summarised as "blind as a bat, dry as a bone, red as a beet, mad as a hatter". The cholinergic toxidrome is SLUDGE — salivation, lacrimation, urination, defecation, gastrointestinal upset, and emesis — with miosis and bronchospasm, and it demands atropine and pralidoxime for organophosphate exposure. [3]
The sympathomimetic toxidrome — mydriasis, tachycardia, hypertension, hyperthermia, and agitation — points to stimulants and needs supportive care and benzodiazepines, not an antidote. The sedative-hypnotic toxidrome — sedation, ataxia, and slurred speech — points to benzodiazepines or alcohol, and here lies a trap: flumazenil can reverse the sedation but can also precipitate seizures in a child who takes benzodiazepines chronically, so it is not a routine antidote. Specific toxins add their own signatures — metabolic acidosis and an anion gap in iron, methanol, or ethylene glycol; coagulopathy in snake envenomation; hyperkalaemia and bradycardia in digoxin toxicity. [3] [8]
Differential Diagnosis
When a child arrives with a reduced level of consciousness, the assumption of poisoning must be tested against the mimics, because giving the wrong antidote to the wrong diagnosis harms. The structured differential asks four questions: is the pupil size and the respiratory pattern consistent with a toxidrome; is there a metabolic cause such as hypoglycaemia or sepsis; is there a structural cause such as trauma or raised intracranial pressure; and does the course track a toxin or something else. [3]
| Diagnosis | Distinguishing features | Key action |
|---|---|---|
| Opioid toxicity | Miosis, slow shallow breathing, opioid exposure; responds to naloxone | Stimulate, support ventilation, give naloxone titrated to respiratory rate |
| Hypoglycaemia | Any presentation; rapid onset; confirmed by bedside glucose | Give 2 to 5 mL/kg of 10 percent glucose IV immediately |
| Sepsis or meningitis | Fever, capillary refill, rash or meningism; evolving independently of toxin | Sepsis screen, cultures, antibiotics, and fluid resuscitation |
| Raised intracranial pressure or trauma | Focal signs, abnormal pupils or posturing, history of head injury | Neuroprotection, imaging, neurosurgical assessment |
| Post-ictal state | History or witness of seizure; gradual recovery over minutes to hours | Support airway, identify and treat seizure cause, observe |
A bedside blood glucose is the single most important test in any child with a reduced level of consciousness, because hypoglycaemia mimics poisoning and is instantly reversible — never omit it. A naloxone trial functions as both treatment and diagnostic test: a child who brightens and breathes faster after naloxone confirms opioid toxicity, while a child who does not respond forces a search for another cause. Paradoxically, giving an antidote is itself part of the diagnostic process when the toxin is uncertain. [3] [4]
Clinical & Bedside Assessment
The bedside assessment of a poisoned child is the ABCDE, performed before any antidote and repeated after it. Airway patency, breathing rate and depth, circulation with pulse and capillary refill, disability with a glucose, GCS, and pupil check, and exposure to search the skin for a bite, a patch, or a source — these five steps stabilise the child and often reveal the toxin. A focused history from the family or paramedics captures what was taken, how much, when, and by what route, and a call to the regional poison information centre resolves uncertainty about dose thresholds and antidote choice. [3] [8]
The toxidrome examination is its own skill. Record the respiratory rate and depth, the pupil size and reactivity, the skin — dry, sweaty, or flushed — the bowel sounds, the bladder for retention, and the temperature. Paired with the heart rate and blood pressure, these signs cluster into a toxidrome that selects the antidote. In the opioid-toxic child, the decisive trigger for naloxone is a slow or shallow respiratory effort with reduced arousability, not a falling oxygen saturation. [3] [4]
For envenomation, the bite site and the evolving systemic signs drive assessment. Look for coagulopathy — bleeding from the bite or gums, an abnormal clotting profile — neurotoxicity — descending paralysis, ptosis, ophthalmoplegia — myotoxicity — muscle pain and a rising creatine kinase — and haemodynamic instability. Australian elapid envenomation may be delayed, so a child who looks well immediately after a bite is observed and re-tested, not discharged. [6] [7]
Investigations
Antidote use is governed by a combination of history, toxidrome, and targeted assays, not by a blanket panel. The investigations that change antidote decisions are few, and the candidate should know exactly which test selects which antidote. A bedside blood glucose is universal. A paracetamol level at four hours or more selects N-acetylcysteine against the treatment line. A serum iron level at three to five hours selects deferoxamine. A digoxin level and a serum potassium guide Fab dosing. A venom detection kit, where available, identifies the snake species and the antivenom. [1] [8]
The paracetamol treatment nomogram — the Rumack-Matthew line — is the single most important investigation tool in paediatric toxicology. A serum paracetamol concentration measured at four hours or later is plotted against time since ingestion; a level at or above the treatment line triggers N-acetylcysteine. The nomogram cannot be used for staggered or repeated ingestion, for sustained-release preparations before levels are available, or when the time of ingestion is unknown — in all these cases the default is to treat. [1] [2]
For iron, a serum iron above roughly 90 micromol per litre at three to five hours, or any symptomatic child with metabolic acidosis or shock, indicates significant toxicity and the need for deferoxamine. For lead, a whole blood lead level guides chelation thresholds — levels above about 45 microgram per decilitre generally warrant chelation consideration, with higher levels and encephalopathy requiring parenteral therapy. Coagulation, full blood count, electrolytes, and liver and renal function are added to follow organ injury, but they monitor rather than select the antidote. [8] [10]
Management — Resuscitation
The first move in any poisoned child is resuscitation, and an antidote is layered onto resuscitation, never substituted for it. Open and protect the airway, support breathing with bag-valve-mask ventilation if the rate or effort is inadequate, establish intravenous access, and restore the circulation with a fluid bolus of 10 mL per kilogram of isotonic saline. A bedside glucose is checked and hypoglycaemia corrected, because hypoglycaemia is common, mimics toxicity, and is instantly reversible. [3]
The resuscitation antidote is naloxone for the opioid-toxic child with inadequate breathing. The principle is to restore respiratory effort, not to render the child fully awake. Give naloxone 10 microgram per kilogram intravenously — about 100 microgram for a 10-kilogram child — repeated every two to three minutes until the respiratory rate and effort recover. If intravenous access is delayed, intramuscular or intranasal naloxone is rapidly absorbed and is a valid alternative. In an opioid-tolerant child, start lower to avoid precipitating acute withdrawal. [3] [4]
Naloxone for opioid-induced respiratory depression in a child
Dose
10 microgram per kilogram per dose, repeated every 2 to 3 minutes until respiratory effort is restored; up to a maximum single dose of about 2 mg in an adolescent
Decontamination runs alongside resuscitation when the airway is safe. Activated charcoal binds many drugs in the gut and is most effective within one hour of ingestion; it is contraindicated when the airway is unprotected, for corrosives, and for metals and hydrocarbons it does not bind. Whole-bowel irrigation, rarely used, has a role for iron, sustained-release, or packet ingestions. The candidate should state that decontamination supports antidote use but does not replace it. [8]
Management — Definitive & Stepwise
Definitive management is the stepwise selection of the antidote matched to the confirmed toxin, dosed by weight and given by the correct route, with monitoring layered throughout. The ladder runs from supportive care, through decontamination, to a specific antidote, and then to disposition. The candidate who climbs this ladder deliberately, naming the toxin, the mechanism, and the weight-based dose at each step, demonstrates safe antidote pharmacology. [1] [3]
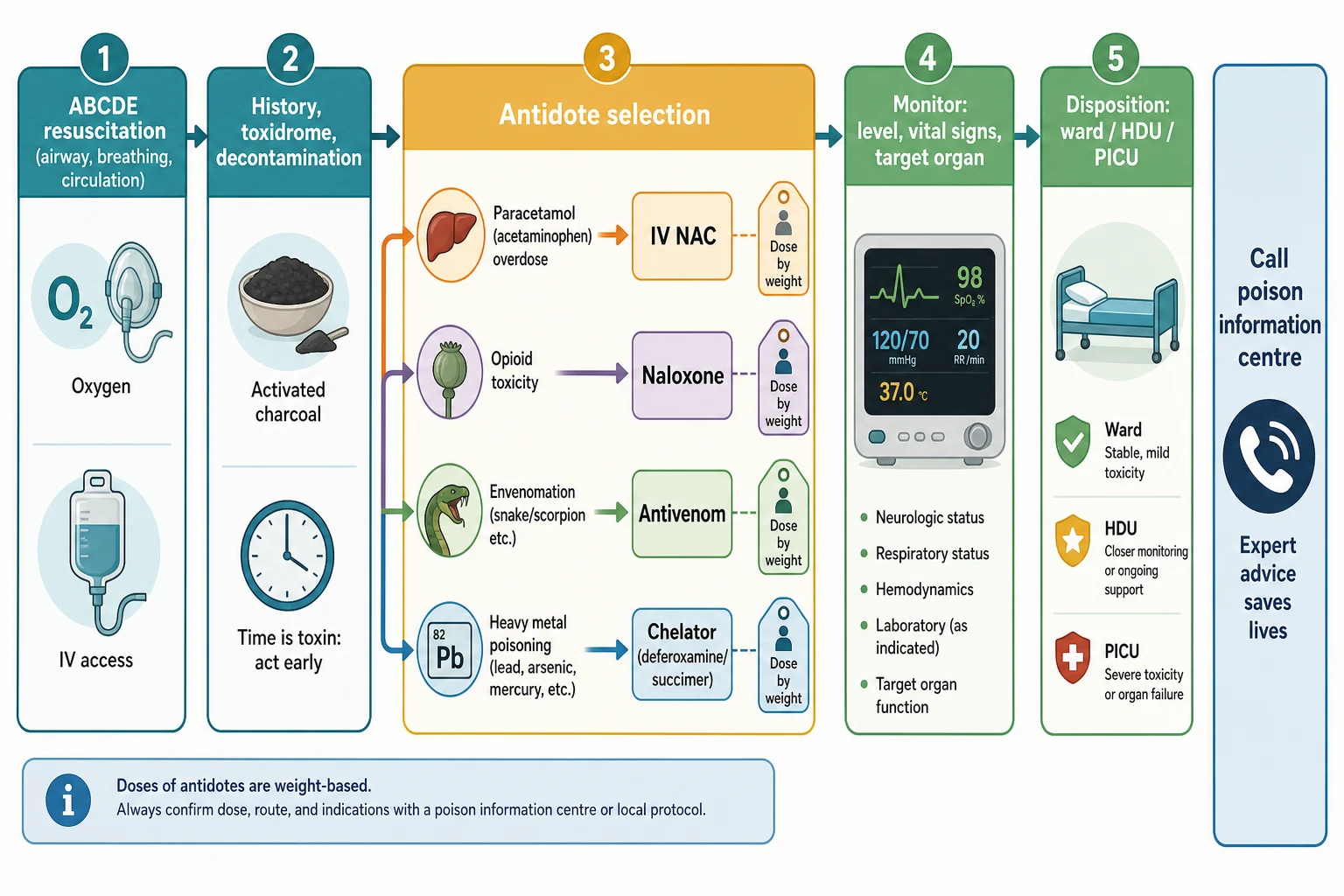
For paracetamol poisoning, N-acetylcysteine is the definitive antidote and it is both highly effective and safe. The intravenous regimen is 150 mg per kilogram over one hour, then 50 mg per kilogram over four hours, then 100 mg per kilogram over sixteen hours — a 21-hour total course. It is started when the paracetamol level is on or above the treatment line, when ingestion is staggered or timed-unknown, or when there is any evidence of hepatotoxicity, because late N-acetylcysteine still improves outcome. The commonest adverse effect is an anaphylactoid reaction — rash, flushing, bronchospasm — which is rate-related and usually resolves on slowing the infusion; it is not a true IgE allergy and rarely demands stopping the drug. [1] [2]
N-acetylcysteine (NAC) for paracetamol poisoning
Dose
150 mg/kg over 1 h, then 50 mg/kg over 4 h, then 100 mg/kg over 16 h (21-hour IV course)
For iron poisoning, deferoxamine is the chelator and it is given intravenously at 15 mg per kilogram per hour once significant toxicity is established — a symptomatic child, metabolic acidosis, shock, or a serum iron in the toxic range. The infusion is continued until the child is stable, the acidosis resolves, and the urine clears from its vin-rose tint. Hypotension can complicate rapid infusion, so the rate is titrated to the blood pressure. [8] [9]
For lead poisoning, chelation depends on severity. Succimer (DMSA) is given orally for moderate poisoning, while calcium-disodium EDTA is given intravenously for severe poisoning, with dimercaprol (BAL) added intramuscularly for lead encephalopathy. The candidate must hold the TLC trial finding alongside the dose — chelation lowers the blood lead level but does not improve neuropsychological outcome at low-to-moderate exposure, so it is reserved for higher levels and symptomatic disease. [10] [11]
For envenomation, antivenom is given intravenously and is species-specific. The dose is determined by the clinical severity and the venom type, guided by a venom-detection kit or regional expert advice, and it is given early for systemic envenomation — coagulopathy, neurotoxicity, myotoxicity, or haemodynamic compromise. Antivenom can cause an acute anaphylactoid reaction, so it is given where resuscitation facilities are available, with adrenaline drawn up. Pre-medication is controversial and not routine. [6] [7] [12]
Specific Subtypes & Scenarios
Paracetamol is the antidote topic the examiner tests most often. A staggered or timed-unknown ingestion defaults to treatment, because the nomogram cannot be applied and the cost of missing hepatotoxicity is high. Sustained-release paracetamol demands two levels and prolonged observation, because absorption is delayed and a late-rising level can appear. Any child with a falling trend but early presentation is plotted at four hours; a child presenting late with hepatotoxicity still receives N-acetylcysteine, because it improves outcome even after injury is established. [1] [2]
Opioid toxicity in the recreational or accidental setting is the scenario where naloxone titration is the skill. An adolescent with an illicit opioid overdose may have taken a long-acting or potent synthetic, so a single naloxone dose is insufficient — repeat to respiratory recovery, then observe for renarcotisation and consider an infusion. Intranasal naloxone is the community and pre-hospital bridge when intravenous access is not yet available, and the pharmacokinetic study in children confirmed its rapid systemic uptake. [3] [4] [5]
Snake envenomation is regionally weighted and high-yield in Australia, where elapids — brown, tiger, taipan, death adder — dominate. Pressure-immobilisation bandaging is the first-aid standard, the bite is not washed so a venom-detection swab can be taken, and antivenom is given intravenously for systemic signs. The prospective study of factors affecting outcome in envenomated children showed that time to antivenom and the severity at presentation drive prognosis, and the red-bellied black snake trial informed how aggressively antivenom is used for a common but milder species. [6] [7]
Iron and lead close the chelation scenarios. A toddler who has taken adult iron tablets presents with vomiting, then an apparent quiescent phase, then shock and acidosis — the candidate must not be reassured by the quiescent phase and must measure the serum iron and start deferoxamine when toxicity is present. A child with lead exposure from old paint or occupational take-home dust presents with abdominal pain, lethargy, or encephalopathy at high levels, and chelation is graded to severity with the TLC trial caveat in mind. [8] [9] [11]
Complications & Pitfalls
The gravest antidote errors are the ones that mistake a reversal agent for a safe one. Flumazenil given to a child who takes benzodiazepines chronically can precipitate refractory seizures, and for that reason it is not a routine reversal agent — the candidate who reaches for it for any sedated child has chosen the wrong antidote. A large naloxone bolus in an opioid-tolerant child precipitates acute withdrawal, severe pain, and agitation, and occasionally pulmonary oedema, which is why titration to respiratory rate is the rule. [3] [4]
The pharmacokinetic mismatch of a short-acting antidote and a long-acting toxin is a recurring pitfall. Naloxone wears off before most opioids, so a child who recovers can re-sedate — observation for renarcotisation and a naloxone infusion for long-acting opioids are the safeguards. Deferoxamine removes only free iron, so starting it late, after the metal has distributed, achieves little. Antivenom does not reverse tissue injury already inflicted, so a child given antivenom late still accrues the damage of the envenomation. [4] [6] [9]
The adverse effects of the antidotes themselves must be anticipated. N-acetylcysteine causes an anaphylactoid reaction that is rate-related and managed by slowing the infusion, not by abandoning the course. Antivenom causes anaphylactoid and serum-sickness reactions, so resuscitation readiness and observation are part of giving it. Deferoxamine at high dose for long periods has been associated with pulmonary and renal toxicity and with Yersinia infection, so it is stopped once the child is stable. [1] [8]
Prognosis & Disposition
The prognosis of a poisoned child given the right antidote at the right time is generally excellent, because most antidotes are highly effective when given before irreversible injury. A child with paracetamol poisoning given N-acetylcysteine on the treatment line recovers without sequelae; a child who presents late with established hepatotoxicity has a worse prognosis but still benefits from N-acetylcysteine and liver-unit support. A child with opioid toxicity given naloxone recovers immediately, provided renarcotisation is anticipated. [1] [3]
Disposition follows the toxin and the antidote. A child who has received naloxone for an opioid overdose is observed for at least several hours because of renarcotisation, and longer for long-acting opioids. A child on an N-acetylcysteine infusion completes the 21-hour course on a monitored ward. A child given antivenom is observed in a monitored setting for recurrence and for serum sickness. A child given deferoxamine is admitted until the acidosis resolves and the iron burden is controlled. [4] [6] [8]
A clear disposition plan names the toxin, the antidote course, the monitoring interval, the expected adverse effects, and the safety-netting advice to the family. In every intentional overdose, a mental-health assessment is part of disposition, and in every accidental toddler ingestion, a home-safety review and poison-prevention counselling close the loop. [3]
Special Populations
The infant and toddler are the population in whom weight-based dosing is most error-prone, because an adult dose is a large dose per kilogram and a small error in weight becomes a large error in dose. Calculate every antidote from a measured weight, use length-based tape estimation when weight is unknown, and double-check the calculation. The infant's immature metabolism also alters some antidotes, though N-acetylcysteine and naloxone are used across the age range with weight-based doses. [3] [8]
The rural and remote child with envenomation or agricultural-chemical exposure may be hours from definitive care, so early telephone advice from the poison information centre and correct first aid — pressure-immobilisation for Australian elapids — are part of the rescue. Retrieval services coordinate antivenom delivery and chelation, and the candidate should name the regional pathway. [6] [7]
The technology-dependent or chronically medicated child carries specific antidote traps. A child on long-term benzodiazepines for epilepsy must not receive flumazenil. A child on long-term opioids or substitution therapy needs low-dose naloxone to avoid withdrawal. A child with chronic lead exposure from a shunted or environmental source needs a coordinated chelation and environmental-abatement plan, because chelation alone does not prevent re-exposure. [3] [10] [11]
For migrant, refugee, and low-health-literacy families, discharge communication about poisoning prevention and antidote follow-up is hardest and most important. Use an interpreter, plain language, and a written plan, and counsel explicitly on safe storage of medicines and the early signs that should prompt a return. Poisoning recurrence is preventable, and prevention is part of the antidote topic. [3] [8]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric antidotes is a mix of consensus guidelines, randomised trials, and pharmacokinetic studies. The 2023 North American consensus statement on acetaminophen poisoning consolidated the thresholds and the N-acetylcysteine regimen, and the Cochrane review of interventions for paracetamol overdose synthesised the randomised evidence, supporting intravenous N-acetylcysteine as effective and relatively safe. The New England Journal of Medicine review of opioid analgesic overdose established naloxone as the standard reversal, and the paediatric intranasal naloxone pharmacokinetic study confirmed the rapid uptake that justifies the intranasal route when access is difficult. [1] [2] [3] [4]
Rogan (TLC) trial — succimer chelation in lead-exposed children (NEJM 2001)
Randomised, double-blind, placebo-controlled trial of succimer versus placebo in children with blood lead levels of 20 to 44 microgram per decilitre, with neuropsychological follow-up
Key finding
Succimer lowered blood lead levels but did not improve cognitive or neuropsychological outcomes at three years of follow-up
The envenomation evidence is regionally strong. The prospective study of factors affecting outcome in children with snake envenomation defined the prognostic drivers, the randomised trial of red-bellied black snake antivenom informed dosing for a common Australian species, and the Fab-antivenom study in crotaline envenomation in children advanced purified-fragment antivenom therapy. The iron-poisoning and chelation reviews anchored deferoxamine and succimer dosing. [6] [7] [8] [12]
Regional guidance converges on the same mechanism classes and the same core antidotes, with local formulary variation in exact weight-based ranges. ANZ guidance (AMH Children's Dosing Companion, RCH Melbourne Clinical Practice Guidelines, and the National Poisons Information network) and UK guidance (BNFc, Toxbase, and the National Poisons Information Service) align on the N-acetylcysteine 21-hour regimen and on naloxone titration. US guidance (the Dart consensus and AAPCC) carries the same thresholds. Envenomation guidance is the most region-specific, because the snake species and the antivenom differ by continent — the candidate should name the regional pathway they are quoting. [1] [4] [6]
Exam Pearls
ANTIDOTE
The four mechanism classes are the single highest-yield framework. Receptor antagonists (naloxone, flumazenil) displace the toxin; binding agents (chelators, digoxin Fab) seize it; substrate restorers (N-acetylcysteine, fomepizole) replenish what it consumed; antibody therapy (antivenom) neutralises venom. Naming the mechanism lets you reason out the agent when the toxin is uncertain. [1] [3]
N-acetylcysteine is 150 mg/kg over one hour, then 50 mg/kg over four hours, then 100 mg/kg over sixteen hours, started on the treatment line or for staggered, timed-unknown, sustained-release, or hepatotoxic presentations. Naloxone is 10 microgram per kilogram intravenously, repeated every two to three minutes, titrated to respiratory rate — never to full consciousness — with a short half-life that demands observation for renarcotisation. Deferoxamine is 15 mg per kilogram per hour for iron toxicity once it is established. Antivenom is species-specific and given early for systemic envenomation. [4] [8] [6]
References
- [1]Dart, Richard C; Mullins, Michael E; Matoushek, Tomas; et al Management of Acetaminophen Poisoning in the US and Canada: A Consensus Statement JAMA Network Open, 2023.PMID 37552484
- [2]Chiew, Angela L; Gluud, Christian; Brok, Joergen; Buckley, Nicholas A Interventions for paracetamol (acetaminophen) overdose Cochrane Database of Systematic Reviews, 2018.PMID 29473717
- [3]Boyer, Edward W Management of opioid analgesic overdose New England Journal of Medicine, 2012.PMID 22784117
- [4]Malmros Olsson, Elisabet; Lonnqvist, Per-Arne; Stiller, Cari O; et al Rapid systemic uptake of naloxone after intranasal administration in children Paediatric Anaesthesia, 2021.PMID 33687794
- [5]Hadland, Scott E; Agarwal, Rishi; Raman, Srinivas N; et al Opioid prescribing for acute pain management in children and adolescents in outpatient settings: clinical practice guideline Pediatrics, 2024.PMID 39344439
- [6]Isbister, Geoffrey K; Jenkins, Sarah; Downes, Margaret A; et al Randomised controlled trial and prospective cohort investigating antivenom for red-bellied black snake envenomation Clinical Toxicology, 2024.PMID 38913734
- [7]Sankar, Jhuma; Nabeel, Raees; Sankar, Mari Jeeva; et al Factors affecting outcome in children with snake envenomation: a prospective observational study Archives of Disease in Childhood, 2013.PMID 23716133
- [8]Fine, Jerri S Iron poisoning Current Problems in Pediatrics, 2000.PMID 10742921
- [9]McGuigan, Margaret A Acute iron poisoning Pediatric Annals, 1996.PMID 8775917
- [10]Bradberry, Sally; Vale, Allister Dimercaptosuccinic acid (succimer; DMSA) in inorganic lead poisoning Clinical Toxicology, 2009.PMID 19663612
- [11]Rogan, Walter J; Dietrich, Kim N; Ware, John H; et al Effect of chelation therapy with succimer on neuropsychological development in children exposed to lead New England Journal of Medicine, 2001.PMID 11346806
- [12]Lasoff, David R; Ruha, Anne-Michelle; Curry, Steven C; et al New Fab 2 antivenom for the treatment of crotaline envenomation in children American Journal of Emergency Medicine, 2016.PMID 27567423