Paeds · clinical-pharmacology-and-therapeutics
Renal and hepatic dose adjustment in children
Also known as Dose adjustment in organ impairment · Renal dose reduction · Hepatic dose reduction · eGFR-based dosing in children · Therapeutic drug monitoring and dose titration
A fellowship approach to adjusting medicine doses for reduced kidney and liver function in children: bedside Schwartz eGFR, KDIGO staging, the Child-Pugh score, the high-risk nephrotoxic and hepatotoxic drugs, vancomycin and gentamicin therapeutic drug monitoring, and a stepwise prescribing algorithm from neonatal life through transition to adult care across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child walks in. You reach for a drug. The textbook dose is a dose for a child with normal kidneys and a normal liver. The moment either organ falters, that textbook dose becomes a guess — and for some drugs a dangerous one. Dose adjustment is the deliberate act of changing the dose, the interval, or both so that the same drug stays inside its therapeutic window when the clearance machinery is impaired. [5]
The reason this matters so much in children is twofold. Children are small, so a small arithmetic error is a large relative error. And children's organ function is not static: a neonate's filtration is a fraction of an adult's, a dehydrated toddler's filtration can collapse in hours, and a transplanted teenager's can swing with each tacrolimus level. A safe prescription in paediatrics is therefore never a one-off number; it is a number tied to a measured organ function and a plan to recheck it. [1]
Two organs dominate the question. The kidney clears water-soluble drugs and their metabolites, so when glomerular filtration falls, those drugs and their active metabolites accumulate. The liver clears fat-soluble drugs by metabolism (mostly the cytochrome P450 system) and by bile flow, so when hepatic blood flow, enzyme capacity, or synthetic function fall, those drugs hang around too long. Most dose-adjustment decisions you will make at the bedside are about one of these two organs, and a surprising number — the septic child in shock, the cirrhotic with an infection — are about both at once. [5] [6]
Three terms will recur, and examiners expect you to use them precisely. Dose reduction means giving less drug per dose. Interval extension means leaving more time between doses. Therapeutic drug monitoring (TDM) means measuring the drug in the blood and using the result to titrate. These are not interchangeable. Aminoglycosides are concentration-dependent killers, so for them you usually extend the interval rather than shrink the dose. Vancomycin is time-dependent, so you often adjust both. Understanding why each tool fits each drug is the difference between a memorised rule and a defensible prescription. [7]
Finally, a framing rule that will keep you safe: the loading dose usually still applies, and the maintenance dose is what falls. A loading dose depends on the volume of distribution, which often does not change much in organ failure (and may rise in fluid overload). Clearance is what falls. So load to fill the tank, then slow the refill. This single principle prevents two common errors — under-treating a sick child by withholding a needed load, and poisoning them by maintaining a normal rate. [5]
Classification
You cannot dose-adjust sensibly until you classify two things: how impaired each organ is, and how the drug behaves. Mix these axes and you will get the dose wrong in a way that looks defensible. [4]
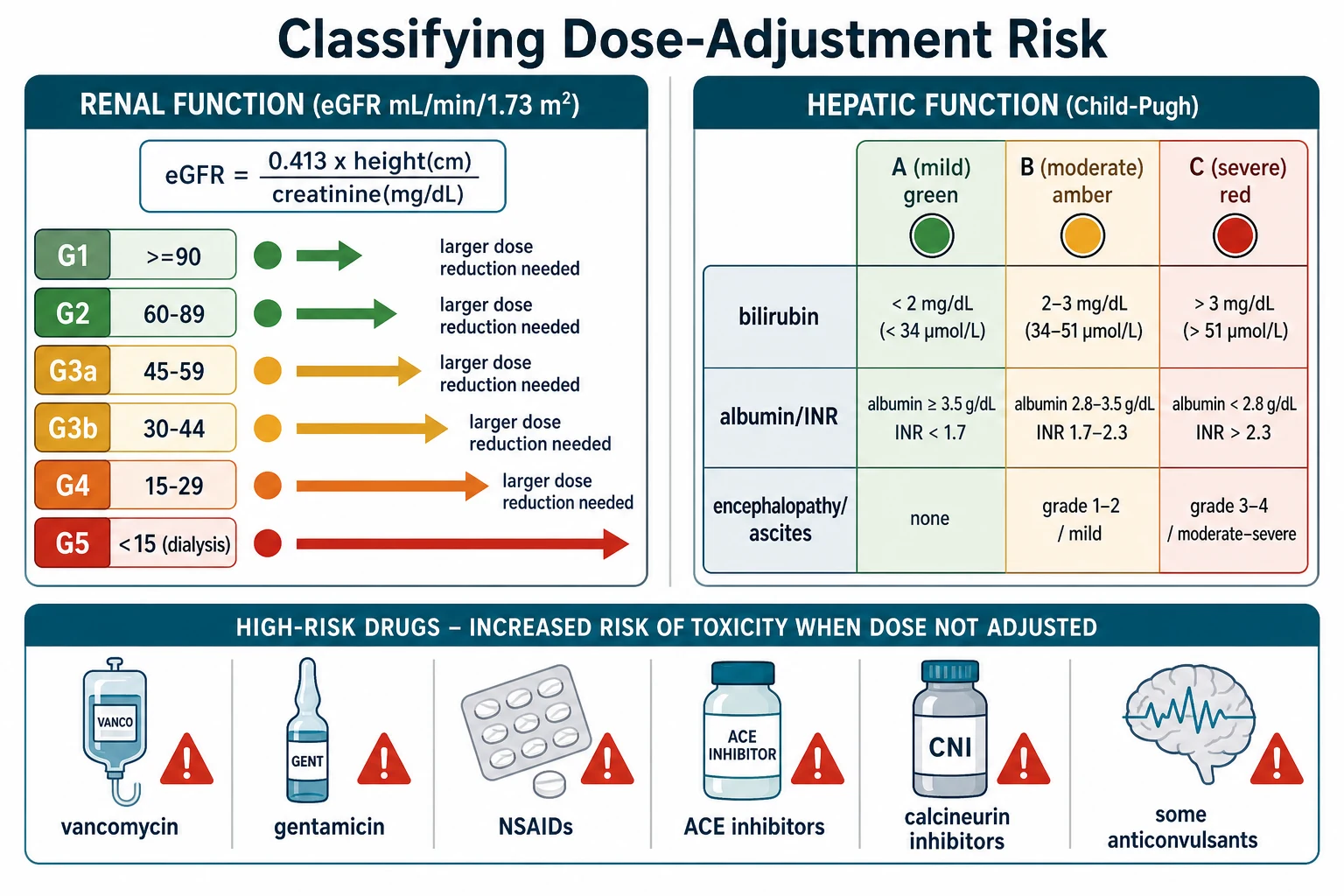
Classifying the kidney: KDIGO GFR categories. The kidney is classified by the estimated glomerular filtration rate (eGFR), and the global standard is the KDIGO category system. G1 is at least 90 mL per min per 1.73 m2 and is normal. G2 is 60 to 89 and is mildly decreased. G3a is 45 to 59, G3b is 30 to 44, G4 is 15 to 29, and G5 is under 15 — kidney failure, often but not always treated with dialysis. Most renally cleared drugs begin to need attention from category G3a, and by G4 nearly all of them do. These thresholds are not decoration; they are the bands the BNFc and most formularies use to phrase their dose-reduction advice, so learn them as numbers. [4]
Classifying the kidney at the bedside: the Schwartz equation. In a child you estimate GFR, you do not measure it routinely. The bedside Schwartz equation gives eGFR in mL per min per 1.73 m2 equal to 0.413 times the height in cm divided by the serum creatinine in mg per dL. The 0.413 constant is the one to quote; the older 0.55 (and 0.45 for infants) belonged to an era of less accurate creatinine assays and will overestimate GFR today. Height appears in the equation because creatinine is generated by muscle, and in a growing child height is the proxy for muscle mass — which is exactly why a guessed height produces a guessed dose. [1]
Classifying the kidney when creatinine lies: cystatin C and the race-free equations. Creatinine is unreliable when muscle mass is abnormal, which is common in neuromuscular disease, cachexia, amputation, or severe critical illness. Cystatin C is a muscle-independent filtration marker produced by all nucleated cells, and a cystatin-C-based or combined equation is the better cross-check when you suspect the creatinine-based estimate is fooling you. The CKiD race-free equations now use creatinine, cystatin C, or both without a race coefficient, and the Full Age Spectrum equation offers continuity across the paediatric-to-adult transition. [2] [3]
G1–G2 (≥60)
- Normal to mildly reduced
- Standard dose for most renally cleared drugs
- Still avoid nephrotoxin stacking
- Recheck if the child becomes unwell
G3a–G3b (30–59)
- Mild to moderate reduction
- Many drugs need a first dose reduction
- Monitor levels for vancomycin and aminoglycosides
- Watch for further decline
G4–G5 (<30)
- Severe reduction to kidney failure
- Almost all renally cleared drugs adjusted
- Some drugs contraindicated or replaced
- Dialysis itself removes some drugs
Classifying the liver: the Child-Pugh score. The liver has no single bedside equivalent of the Schwartz equation, so clinicians fall back on the Child-Pugh score (also called Child-Turcotte-Pugh). It adds up five variables — bilirubin, albumin, INR (or prothrombin time), ascites, and encephalopathy — each scored 1 to 3. The total sorts a child into class A (mild, 5 to 6 points), class B (moderate, 7 to 9), and class C (severe, 10 to 15). For the bilirubin band, under 34 micromol per L scores 1, 34 to 51 scores 2, and over 51 scores 3; albumin over 35 g per L scores 1, 28 to 35 scores 2, and under 28 scores 3. Child-Pugh is rough and partly subjective (ascites and encephalopathy are clinical), but it remains the most widely used bedside grade of hepatic impairment for dosing. [6]
Classifying the drug: how is it cleared? The other axis is the drug itself. Is it cleared mainly by the kidney (gentamicin, vancomycin, most beta-lactams, digoxin)? Mainly by the liver (morphine, phenytoin, diazepam, tacrolimus)? By both? Is it highly protein-bound (phenytoin, warfarin) so that a low albumin changes its free fraction? Is it a high-extraction, flow-dependent drug (morphine, labetalol, lidocaine) whose clearance collapses in shock? Or a low-extraction, capacity-dependent drug (phenytoin, theophylline) whose clearance falls as CYP enzymes fail? You will not memorise every drug, and you should not try. You will learn the high-risk ones and then look up the rest in the BNFc or your local formulary before you sign the chart. [5] [6]
Epidemiology & Risk Factors
Reduced organ function in a child is far more common than the healthy newborn on the ward suggests. The children we actually prescribe for — neonates, oncology patients, transplant recipients, cystic fibrosis, cardiac, nephrology, the critically ill — carry baseline impairment or fluctuating function as the rule, not the exception. [11]
Consider the wards you work on. Studies of non-critically ill hospitalised children show that a meaningful proportion are exposed to nephrotoxic medications, and that a substantial minority of those exposed develop acute kidney injury as a direct consequence — not in intensive care, but on ordinary medical and surgical wards. The risk is concentrated in oncology, transplant, cardiac and complex-chronic cohorts, but it reaches every service. [11]
The child at highest risk is the one with several risk factors stacked: low baseline eGFR, low albumin, rising bilirubin, high INR, sepsis, and two or more nephrotoxins at once. Each factor alone may look manageable; together they convert a standard dose into a toxic one. The clinician's job is to recognise the stack before the child pays for it. [11] [12]
Prematurity and young infancy create a physiological dose-adjustment problem even without disease. A neonate's GFR is a fraction of adult values at birth and climbs over the first weeks of life, so renally cleared drugs such as gentamicin and vancomycin need longer intervals and level-tailored dosing. Hepatic enzyme pathways and bile flow are immature, prolonging the half-life of drugs such as morphine. Albumin is lower and binding is weaker, raising free fractions. None of this is pathology; all of it is dose adjustment. [10]
Polypharmacy multiplies risk in a way that is easy to overlook in a child with medical complexity, who may be on ten or more chronic medicines. Each drug may be reasonable alone, but the combination raises the chance of a CYP interaction, additive nephrotoxicity, or a formulation problem that turns a calculated dose into the wrong delivered dose. [5]
Pathophysiology
To dose-adjust with understanding rather than by rote, you need the ADME picture: how a drug is absorbed, distributed, metabolised, and excreted, and where failing organs distort each step. [5]
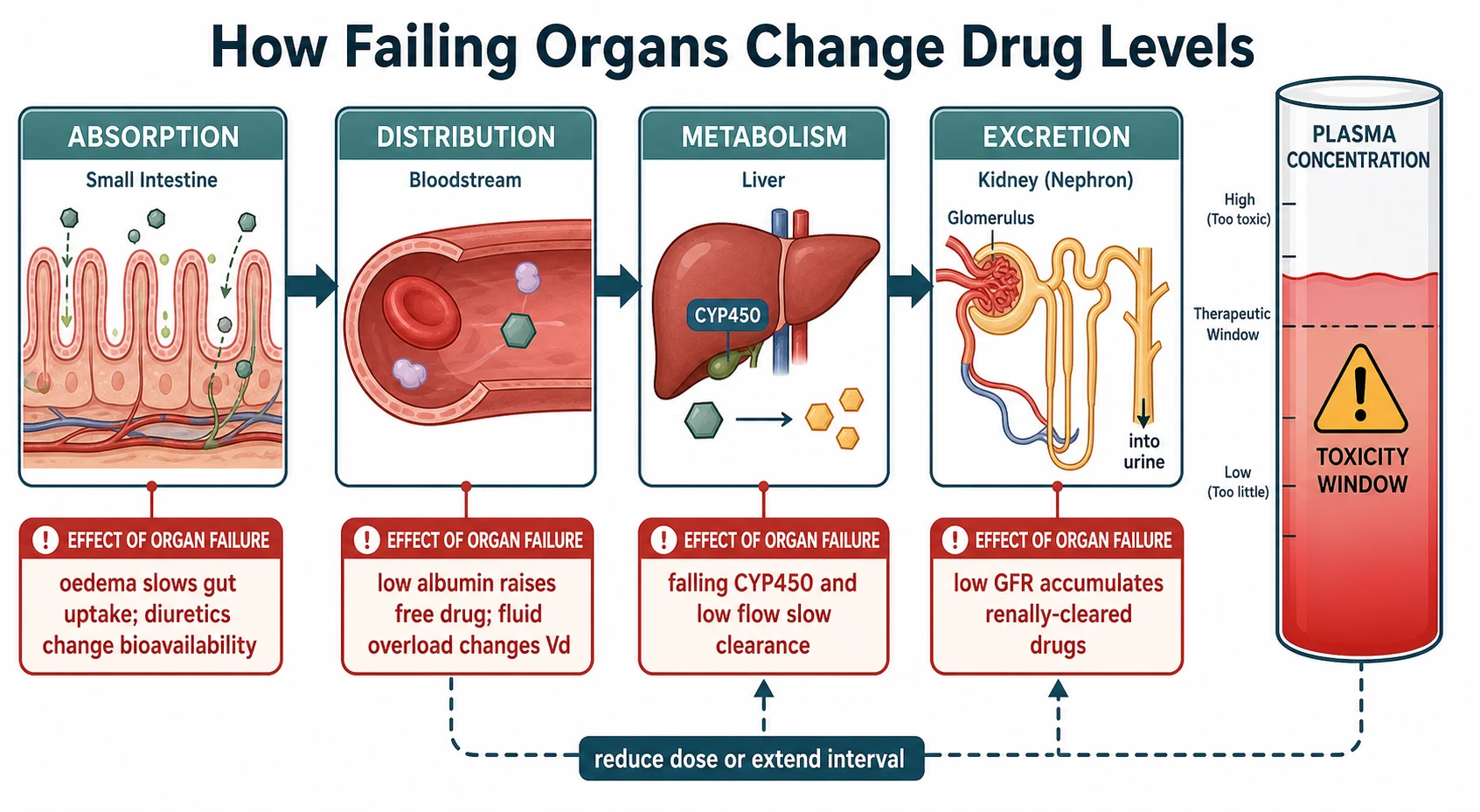
Excretion is where the kidney dominates. A drug that is cleared by the kidney leaves the body in the urine, filtered at the glomerulus and sometimes secreted or reabsorbed along the tubule. When GFR falls, less drug is removed per hour, the half-life lengthens, and repeated standard doses pile on top of each other. The child does not just have a higher number on the assay — they have more drug acting on them, which is what produces the toxicity: an aminoglycoside attacking the cochlea and the proximal tubule, vancomycin injuring the kidney, digoxin blocking conduction. The clinical problem is not the level; the level is the marker for the harm. [5]
Metabolism is where the liver dominates, in two different ways. High-extraction drugs such as morphine, metoprolol, propranolol, labetalol and lidocaine are cleared in proportion to hepatic blood flow, so anything that cuts liver flow — shock, low cardiac output, cirrhotic vascular rerouting — drops their clearance fast. Low-extraction drugs such as phenytoin, diazepam, theophylline and warfarin are cleared in proportion to enzyme capacity, so loss of functional CYP450 mass (cirrhosis, hepatitis, drug inhibition) drops their clearance. A child in shock on a morphine infusion fails on the first mechanism; a child with chronic cirrhosis on phenytoin fails on the second. [6]
Distribution is where albumin and fluid matter. Many drugs circulate bound to albumin, and only the free (unbound) fraction is active. In hypoalbuminaemia — common in nephrotic syndrome, liver failure, and critical illness — the free fraction of a highly bound drug such as phenytoin rises, so a total phenytoin level that looks therapeutic can still produce toxicity. In those children, measure the free phenytoin, or interpret the total level with an albumin correction. Volume of distribution changes too: ascites, fluid overload and burns expand the volume, which changes the loading dose (more drug to fill the bigger tank) but not the maintenance rate. [5] [6]
Absorption is the least common but real contributor. Gut oedema in severe illness or nephrotic syndrome can slow or erraticise absorption; diarrhoea or rapid gut transit can reduce it; and in cirrhosis, portosystemic shunting can increase the bioavailability of drugs normally cleared on first pass. None of these is the headline mechanism, but each can explain why a carefully calculated dose behaves unexpectedly. [6]
Put together, reduced clearance raises the plasma concentration into the toxicity window, and the feedback the body cannot provide is the one the prescriber must: reduce the dose, extend the interval, or measure and titrate. The pharmacology of every dose-adjustment decision in this topic is a variation on that one loop. [5] [7]
Clinical Presentation
The child harmed by a dose that was not adjusted rarely presents with "drug toxicity" written on their forehead. They present as deterioration, and the drug is found when someone thinks to look. [11]
A child accumulating a renally cleared sedative or anticonvulsant looks sleepy, then drowsy, then hard to rouse. A child accumulating an aminoglycoside may complain of tinnitus or hearing loss (and in a pre-verbal child you see it as a failure to startle, or balance problems once mobile). A child accumulating morphine slows their breathing. A child in NSAID-related acute kidney injury stops passing urine and may show hyperkalaemia on the blood gas. A child with vancomycin-related nephrotoxicity has a creatinine that creeps up day by day. Each of these is a reason to stop, recheck the dose, and recheck organ function — not a reason to push on with the original prescription. [7] [10]
The clinical features that should trigger a dose review are the features of failing organ function itself: oliguria, new oedema, jaundice, new or worsening ascites, a rising creatinine, a falling platelet count with a climbing INR, and new encephalopathy. Any of these in a child on a high-risk drug means the prescription written yesterday may be wrong today. [11]
Transplant and oncology children have their own warning patterns. A tacrolimus-treated transplant child with a rising creatinine may have calcineurin-inhibitor nephrotoxicity, rejection, or both — and the only way to separate them is the drug level alongside the clinical picture. An oncology child on nephrotoxic chemotherapy who then receives vancomycin for a line infection is the textbook case of nephrotoxin stacking, and the AKI often arrives in the second week of that combination. [11] [12]
The presentation of infusion-related reactions deserves a word because it can be confused with anaphylaxis. Vancomycin given too fast causes rate-related histamine release — the "red man syndrome" of flushing, itch and hypotension. The treatment is to slow or stop the infusion, give an antihistamine, and restart at a lower rate; it is not usually a reason to abandon a needed drug. True anaphylaxis is rare and demands adrenaline. Telling them apart at the bedside is a high-yield exam point. [7]
Differential Diagnosis
When a child on a high-risk drug deteriorates, the first question is not "what is wrong with the drug" but "is this the drug, the disease, or both." Three distinctions carry most of the weight. [5]
Drug toxicity versus disease progression. The resolving data are the drug level, the trend of organ function, and the clinical response to a dose hold or reduction. If the vancomycin trough is high and the creatinine rises, and both settle when the dose is adjusted, you have your answer. If the child deteriorates despite a normal level and good organ function, the drug is less likely to be the culprit and you must chase the disease. [7] [8]
True fall in GFR versus a creatinine that misleads. A rising creatinine can reflect genuine kidney injury, but it can also reflect muscle breakdown (rhabdomyolysis, status epilepticus), a drug interfering with the assay, or simply lab timing. Cystatin C and the urine output trend help separate a real fall in filtration from a number that looks worse than the kidney. [2] [3]
Pre-renal rise versus intrinsic injury. A dehydrated child has a creatinine that rises because the kidney is underperfused, not because the tubule is dead. The pre-renal kidney needs fluid (and the dose may not need changing once perfusion is restored), whereas the intrinsic kidney needs both fluid support and dose reduction. Giving fluid to intrinsic AKI as if it were pre-renal, and failing to adjust the drug, is a classic compound error. [5]
For the liver, the parallel distinction is benign transaminitis (a laboratory abnormality that does not by itself change clearance much) versus genuine hepatic synthetic failure, signalled by a rising INR, falling albumin, and encephalopathy. The former may not require dose change; the latter demands it. The INR is the liver's "creatinine" for dosing purposes — it tracks synthetic function, which is what matters for clearance, far better than the ALT does. [6]
Finally, separate an idiosyncratic adverse drug reaction (which means stop the drug) from predictable accumulation toxicity (which means adjust the dose). They are not the same problem and they do not have the same solution. [5]
Clinical & Bedside Assessment
The dose-adjustment assessment is a bedside act, not a laboratory one. The numbers matter, but they only matter once you have examined the child and read the chart. [5]
Begin with the body. Weigh the child, and in any child under two (or unable to stand) measure length, and in any older child measure height — lying or standing, with the right technique. Without a measured height or length there is no trustworthy Schwartz eGFR, and without a trustworthy eGFR there is no defensible renal dose. This single step, often skipped, is the difference between a calculated dose and an invented one. [1]
Assess hydration and perfusion next. Feel for delayed capillary refill, cool peripheries, a sunken fontanelle, dry mucosae, and reduced skin turgor. The point is to separate a reversible pre-renal creatinine rise — which needs fluid and may not need a permanent dose change — from established intrinsic kidney injury, which needs both. A child in shock is not a child in whom to trust a single creatinine; they are a child in whom to resuscitate first and dose-adjust after. [5]
For the liver, examine for jaundice (sclera first, then skin), spider naevi, palmar erythema, ascites (shifting dullness, fluid thrill), and hepatic encephalopathy. Stage the encephalopathy, because the grade changes both the dose and the disposition: grade 1 is mild confusion or sleep-wake disturbance, grade 2 is lethargy and disorientation, grade 3 is somnolence but rousable, and grade 4 is coma. A child at grade 3 or 4 is critically ill and their hepatically cleared drugs need aggressive adjustment. [6]
Now read the medicine chart as an examination in itself. Look for the markers of dose-adjustment risk: more than one nephrotoxin at once, a weight that is days old, a verbal-only dose, a high-risk drug with no level ordered, a corrected calcium or potassium that has drifted. Each is a prompt to pause. Ask the nurse whether the child is actually tolerating and absorbing the medicine — vomiting, diarrhoea, or a blocked feeding tube can make a perfect prescription deliver nothing. [11]
And ask the family. The carer often holds the information that changes the dose — the home dose, the last time a level was checked, whether the child has missed doses, whether a new over-the-counter or complementary medicine has started. Dose adjustment fails when it is done to the chart and not with the family. [5]
Investigations
The investigations for dose adjustment are the investigations of organ function, plus the drug level where one exists. [4]
Renal function. Serum creatinine, reported on a modern enzymatic assay, is the entry point, and the bedside Schwartz equation converts it into an eGFR. In children with abnormal muscle mass, a cystatin-C-based or combined equation is more reliable. Urine output is a clinical investigation in its own right — an oliguric child has a falling effective clearance regardless of the last creatinine, because of the creatinine lag: the blood value rises only after filtration has already fallen and muscle has had time to load the blood. A single normal creatinine in a sick, oliguric child under-represents injury; trend it. [1] [2]
Hepatic function. For dosing, the panel is bilirubin (total and fractionated), albumin, INR, and transaminases, with synthetic function weighted most heavily. The INR reflects the liver's ability to make clotting factors and is the closest bedside marker of the functional hepatic mass that clears drugs; the ALT reflects injury but not necessarily clearance. A child with a normal ALT and a climbing INR has failing hepatic clearance and needs dose adjustment; a child with a high ALT and a normal INR often does not. [6]
Albumin. A low albumin changes the interpretation of highly protein-bound drugs. For phenytoin, the most commonly encountered example, the free level is the better test when albumin is low; a free phenytoin reference interval of roughly 1 to 2 mg per L is what you act on. State the albumin whenever you quote a total phenytoin. [5]
Therapeutic drug monitoring. For vancomycin, draw the level at the right time: a trough is taken just before the next dose. The 2020 international consensus moved away from trough-only monitoring for serious MRSA infection toward area-under-the-curve guided dosing, targeting an AUC of 400 to 600 mg per h per L, because trough alone both under-doses and over-doses a meaningful fraction of children. Where AUC tools (including Bayesian estimators validated in neonates and children) are available, use them; where they are not, a trough remains a pragmatic but imperfect surrogate. For gentamicin given by extended interval, the trough (taken just before the next dose) should be low or undetectable, and the interval is then tailored to the level using the local protocol. [7] [8] [9]
A dose-adjustment ladder at the bedside
Interpreting a level against the target is the point of measuring it. A high level demands a dose reduction or interval extension and a search for accumulating renal or hepatic impairment; a low level demands an increase and a search for non-adherence, malabsorption, or an interaction accelerating clearance. A level is never just a number to file; it always forces an action. [7] [8]
Management — Resuscitation
When a child on an adjusted drug presents in crisis, the crisis is managed first and the dose arithmetic second. Airway, breathing, and circulation come before any pharmacokinetic reasoning. [7]
For life-threatening drug toxicity — a child seizing from accumulating phenytoin, apnoeic from accumulating morphine, or reacting to a rapid vancomycin infusion — the sequence is: support the airway and breathing, stop the offending drug, give supportive care, and use an antidote where one exists. Naloxone reverses opioid respiratory depression; it does not correct the underlying accumulation, so you may need an infusion and continued observation. For an infusion reaction, slow or stop the infusion, give an antihistamine, and restart at a lower rate. [7]
For NSAID-related acute kidney injury with hyperkalaemia, the resuscitation priority is cardiac stabilisation and potassium control: intravenous calcium for ECG changes, insulin with dextrose, salbutamol, and stopping the NSAID, with cautious fluids only if the child is genuinely volume-depleted. Giving a fluid bolus reflexively to a volume-overloaded child with NSAID-related AKI worsens them. [11]
When organ function is changing hour by hour — septic shock, hepatorenal physiology, a child on escalating inotropes — the prescribing rule is: hold, reduce, monitor, or substitute. Many drugs can be held for hours without harm while you resuscitate. For drugs you cannot hold (a life-saving antibiotic, an anticonvulsant in status), reduce the maintenance rate and monitor, or substitute a safer agent. In multi-organ failure, reach for the clinical pharmacist and the toxicologist before you write; the interaction between falling clearance, rising volume of distribution, renal replacement therapy, and extracorporeal circuits is genuinely specialist work. [5]
Dialysis and haemofiltration change the picture because they remove some drugs directly. Gentamicin is dialysable; vancomycin is partly removed and often needs supplementation after haemodialysis; digoxin is poorly removed because it is highly tissue-bound. The nephrology and pharmacy teams hold the dosing tables for renal replacement therapy, and you should always confirm the dose with them rather than extrapolate from an eGFR-based table. [5]
The resuscitation phase ends when the child is physiologically stable and you have a current, trustworthy set of organ-function numbers. Only then does the deliberate dose-adjustment algorithm below begin. [11]
Management — Definitive & Stepwise
Once the child is stable, dose adjustment follows a reproducible algorithm. Run it the same way every time and you will not miss a step. [5]
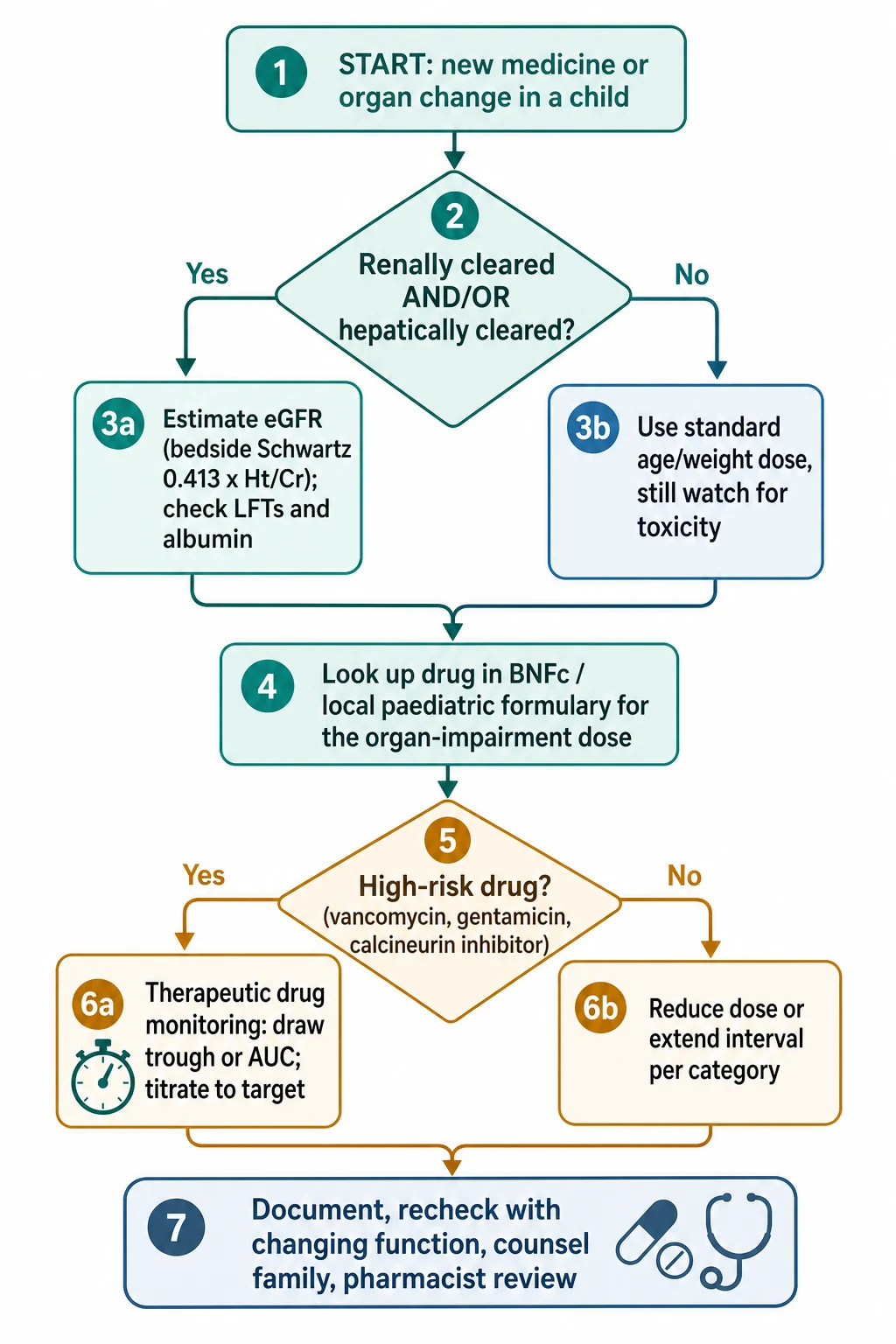
Step 1 — Identify the drug and how it is cleared. Is it renally cleared, hepatically cleared, or both? Is it highly protein-bound? High or low extraction? This tells you which organ matters most and which traps apply. [5]
Step 2 — Estimate organ function with measured data. Measure height, take the serum creatinine on a modern assay, and calculate the bedside Schwartz eGFR. Check the bilirubin, albumin and INR and grade the liver with Child-Pugh. Record the urine output. Do not proceed without a measured height. [1] [6]
Step 3 — Look up the drug-specific recommendation. Open the BNFc, the RCH Melbourne guideline, or your local paediatric formulary, and read the operative dose for that eGFR band or Child-Pugh class. This is the step that defeats memory. Never quote a remembered paediatric drug dose as definitive; always state the source you are using. [5] [10]
Step 4 — Decide dose versus interval. For concentration-dependent killers such as the aminoglycosides, extend the interval rather than shrink the dose, so the peak stays high enough to kill. For time-dependent drugs such as vancomycin and the beta-lactams, keep the time above the minimum inhibitory concentration in mind, which often means keeping the dose but extending the interval, or both. For hepatically cleared drugs in Child-Pugh B or C, the usual starting strategy is to reduce the maintenance dose by around half and titrate to response and level. [5] [7]
Step 5 — Monitor. Order the drug level for every high-risk drug, drawn at the right time. For vancomycin, use AUC-guided dosing where available. For gentamicin, use the level to set the next interval. Recheck organ function on a schedule that matches how fast it is changing. [7] [9]
Step 6 — Document, counsel, hand over. Write the reason the dose is not standard on the chart and in the notes ("dose reduced for eGFR 35 mL per min per 1.73 m2 per BNFc"). Explain the change to the family in language they can repeat back. Flag the adjusted dose at handover, and ask the pharmacist to review. A dose that is adjusted but not documented is a dose the next clinician will "correct" back to standard. [11]
[4]Vancomycin (high-risk, TDM-required)
Gentamicin (high-risk, TDM-required)
A worked renal example anchors the algorithm. A 6-year-old, 115 cm tall, has a serum creatinine of 1.4 mg per dL on a modern assay, needs a renally cleared antibiotic, and is on no other nephrotoxin. The bedside Schwartz gives eGFR equal to 0.413 times 115 divided by 1.4, which is about 34 mL per min per 1.73 m2 — KDIGO G3b. You look up the drug in the BNFc, find the G3b recommendation, reduce the maintenance dose or extend the interval accordingly, order a level if the drug is high-risk, and document the calculation. If the child then becomes oliguric, you do not trust the eGFR of 34 anymore — you recheck and re-adjust. [1] [4] [5]
A worked hepatic example anchors the other axis. A 10-year-old with biliary atresia and a Kasai has bilirubin 60 micromol per L, albumin 26 g per L, INR 2.0, moderate ascites, and grade 1 encephalopathy — Child-Pugh class C. You treat every hepatically cleared drug as substantially impaired: reduce the maintenance dose by around half for drugs the BNFc flags, prefer renally cleared alternatives where they exist, avoid sedatives unless essential, and watch for cumulative effects. [6] [5]
Specific Subtypes & Scenarios
The algorithm is constant; the scenarios stress different parts of it. Walk through the high-yield ones the way an examiner will. [5]
The neonate on gentamicin for suspected sepsis. Neonatal GFR is low and rising, so the gentamicin interval is longer than in older children and is set by the postmenstrual age and the level. You dose by weight and age band, draw a level before the second or third dose depending on the unit protocol, and tailor the next interval to that level. A rising creatinine in the first days of life may be expected maternal clearance rather than injury — but a level that is climbing demands an interval extension regardless of the cause, because the drug will accumulate either way. [10]
The child with CKD on an anticonvulsant. A child at CKD stage G3b on phenytoin carries two traps: the eGFR-based dose reduction, and the hypoalbuminaemia that makes the total phenytoin level misleading. Send a free phenytoin whenever the albumin is low, adjust to the free target, and watch for drug interactions — phenytoin is a potent CYP inducer that can lower the levels of concurrent medicines. [4] [5]
The transplant child on tacrolimus with a rising creatinine. Here the drug is both the treatment and a likely cause of the problem. Calcineurin inhibitors constrict the afferent arteriole and cause functional then structural nephrotoxicity. Check the tacrolimus trough, look for interacting drugs (azoles, macrolides, grapefruit all raise it), and work with the transplant team to separate toxicity from rejection — which may require a biopsy rather than guesswork. [5] [11]
The child with nephrotic syndrome on an ACE inhibitor during a relapse. An ACE inhibitor dilates the efferent arteriole and lowers intraglomerular pressure; in a relapsing, oedematous, hypoalbuminaemic child who may also be intravascularly depleted, that can precipitate acute kidney injury. The safe move during a heavy relapse is often to hold the ACE inhibitor, restore intravascular volume, and restart once the child is stable. [5]
The child with cirrhosis, ascites, and an infection. This is the both-organs scenario. Cirrhosis with ascites is usually Child-Pugh C, the infection may drive hepatorenal physiology, and every diuretic, antibiotic, and sedative is in play. Reduce hepatically cleared drugs, prefer renally cleared antibiotics guided by the (falling) eGFR, avoid NSAIDs entirely, and reassess daily. [6]
The adolescent with cystic fibrosis on repeated aminoglycoside courses. Cumulative aminoglycoside exposure threatens both hearing and kidney function over years. Track the cumulative dose, perform periodic audiometry, and use the lowest effective course with level-tailored intervals each time. The dose-adjustment question here is longitudinal, not per-admission. [10]
The oncology child on nephrotoxic chemotherapy with vancomycin. This is nephrotoxin stacking, and it is the scenario the NINJA (Nephrotoxic Injury Negated by Just-in-Time Action) programme was built to prevent. Where possible, avoid the combination; where you cannot, monitor closely, consider alternative analgesia to NSAIDs, and involve pharmacy early. [11] [12]
Complications & Pitfalls
The complications of failing to dose-adjust are the toxicities themselves: nephrotoxicity, ototoxicity, neurotoxicity, hepatotoxicity, prolonged sedation, and the downstream harm of a prolonged admission or an avoided drug. The pitfalls are the cognitive errors that get you there. [11]
The first pitfall is the wrong Schwartz constant. Quoting 0.55 with a modern enzymatic assay overestimates the eGFR, falsely reassures you, and leaves a child over-dosed. The bedside constant is 0.413; quote it and use it. [1]
The second is the guessed height. A height you have estimated rather than measured produces an eGFR you have estimated rather than calculated. In a child whose dose depends on it, measure. [1]
The third is inverting a threshold. Dose reduction usually becomes important from KDIGO G3a (under 60), not from G1. A child at G4 is not "nearly normal"; they are severely impaired and almost every renally cleared drug needs adjustment. Getting the direction of the threshold wrong is a classic fail. [4]
The fourth is nephrotoxin stacking. Two nephrotoxic drugs together (an NSAID with an aminoglycoside; vancomycin with piperacillin-tazobactam) cause disproportionate harm through additive mechanisms. Avoid the combination where you can; monitor hard where you cannot. [11] [12]
The fifth is the unseen interaction. A CYP inhibitor started overnight — an azole antifungal, a macrolide, amiodarone — can raise a calcineurin-inhibitor or statin level dramatically and convert an adjusted, safe dose into a toxic one. Re-read the medicine list whenever you add a drug, not just when you prescribe. [5]
The sixth is the unmonitored high-risk drug. Prescribing vancomycin or an aminoglycoside without ordering a level is a system failure as much as a clinical one. Build the level into the initial order set. [7] [9]
The seventh is over-caution — withholding a needed drug through fear of toxicity. Dose adjustment is not dose avoidance. A child with septic shock still needs the antibiotic; the job is to give it safely, not to defer it. [5]
Prognosis & Disposition
The outlook for a child with a dose-adjustment problem is the outlook for the underlying organ injury, modified by how promptly the dose was corrected. Drug-related kidney injury from a single, promptly stopped nephrotoxin often recovers fully; injury from a sustained, stacked combination may leave chronic kidney disease. The threshold for higher-acuity care is lower when the child is oliguric, hyperkalaemic, encephalopathic, has a rising INR, or has reacted to an infusion. [11]
Baseline organ function changes the prognosis of an additional insult. A child with pre-existing CKD who receives a nephrotoxic antibiotic has less renal reserve to absorb the hit, which is precisely why dose adjustment matters more for them, not less. A child with chronic liver disease has less hepatic reserve for any new insult. [4] [6]
Disposition after an adjusted-dose admission should include explicit follow-up surveillance: a creatinine trend after a nephrotoxic course, LFTs after a hepatotoxic one, a drug level to confirm the adjusted dose is on target, and — for aminoglycosides — audiometry after significant cumulative exposure. The discharge summary should state the dose adjustment and its reason, so the medical home and the next team carry it forward. [10] [11]
For safe discharge on an adjusted dose, the carer must be able to demonstrate the dose back to you, the supply must be sufficient to the next review, and the safety-net must be explicit: what to watch for, when to return, and who to call. A correctly adjusted dose delivered wrongly at home undoes the entire inpatient effort. [5]
Special Populations
Neonates and premature infants. Immature GFR and hepatic enzymes, a higher total body water, and lower albumin binding make every dose a dose-adjustment problem. Renally cleared drugs need longer intervals and level-tailored dosing; hepatically cleared drugs need longer dosing intervals or lower rates. The neonatal formulary (NeoFax, local unit protocols) is the operative reference, and weight and postmenstrual age, not eGFR equations tuned for older children, drive the arithmetic. [10]
Children with medical complexity and technology dependence. Polypharmacy, feeding tubes that change bioavailability, unreliable weights, and multiple prescribers make this group the highest-yield for a systematic pharmacist-led medication review. Each drug is reasonable alone; the combination is where harm hides. [5]
Children with cancer and transplant recipients. Cumulative nephrotoxic exposure, conditioning-regimen organ injury, and the constant presence of calcineurin inhibitors demand proactive adjustment and active surveillance rather than reactive dose changes. [11] [12]
Children with neuromuscular disease, cachexia, or amputation. Creatinine under-represents reduced function because muscle mass is low, and body surface area is hard to estimate. Reach for cystatin C, and interpret any creatinine-based eGFR with suspicion. [2]
Indigenous, remote, and rural children. Distance from pharmacy and pathology changes the plan: a drug needing close level monitoring may be impractical far from a laboratory, and a safer, less-monitor-intensive alternative may be better. Build the monitoring into the retrieval and follow-up plan. [10]
Migrant, refugee, and asylum-seeking families. Language discordance and unfamiliar formulations risk a correctly calculated dose being given wrongly at home. Use a professional interpreter, confirm the family can demonstrate the dose, and check whether a familiar formulation is available locally. [5]
Adolescents at transition to adult care. The paediatric Schwartz equation cannot simply follow the patient into adult care — adult equations behave differently above the transition threshold, and a paediatric weight-based dose can under-shoot or overshoot an adult one. Reconcile the equation, cap the weight at adult doses where appropriate, and confirm continuity with the adult team before transfer. The Full Age Spectrum equation exists precisely to smooth this handover. [3]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric dose adjustment is a mix of global staging systems, consensus guidelines, pharmacological reviews, and regional paediatric formularies. Knowing which to reach for, and which overrides which, is part of the answer. [4]
The KDIGO 2012 guideline remains the global frame for classifying chronic kidney disease and framing drug-dosing categories by GFR. Its categories are reproduced in every major formulary, which is why the 90-60-45-30-15 thresholds appear so consistently. The guideline leaves the drug-specific dosing to regional formularies, so KDIGO stages the kidney; the BNFc doses the drug. [4] [4]
The BNF for Children is the primary paediatric formulary for the UK and much of the Commonwealth, carrying explicit renal and hepatic dose-reduction bands by drug. NICE NG203 (2021) governs the investigation and management of CKD in the UK and underpins referral thresholds. [5] [4]
In ANZ, the Royal Children's Hospital Melbourne Clinical Practice Guidelines and Paediatric Injectable Guidelines carry the operative gentamicin (extended-interval) and vancomycin protocols that clinicians actually use at the bedside. [10]
In the US, the 2020 ASHP-IDSA-PIDS-SIDP vancomycin consensus shifted practice toward AUC-guided dosing, and validated paediatric and neonatal Bayesian tools now support individualised vancomycin therapy. FDA labelling carries explicit renal and hepatic adjustment guidance for individual drugs. [7] [9]
The Child-Pugh score remains the most widely used bedside hepatic-impairment grade despite known limits: it is partly subjective, it does not separate the contributions of each variable, and it was not derived in children. Drug-specific hepatic advice in the BNFc often bypasses the score and gives a direct recommendation. Newer measures (MELD-based estimates, Child-Pugh alternatives) are debated but have not displaced the score at the paediatric bedside. [6]
The NINJA programme and its paediatric derivatives are the strongest systems-level evidence that active nephrotoxin surveillance reduces acute kidney injury in hospitalised children, and they shape how dose-adjustment risk is managed at the ward level rather than only at the prescription level. [12]
The race-free eGFR debate has reached paediatrics: the CKiD race-free equations now estimate GFR from creatinine, cystatin C, or both without a race coefficient, and the Full Age Spectrum equation provides continuity across transition. The bedside Schwartz constant (0.413) is unaffected by this debate and remains the practical entry point. [2] [3]
When ANZ, UK, US, and Canadian sources disagree on a specific drug's renal dose, the resolution at the bedside is to follow your local formulary and document it, not to synthesise a compromise from memory. [5] [10]
Exam Pearls
- Quote the bedside Schwartz as 0.413 times height in cm divided by serum creatinine in mg per dL, indexed to 1.73 m2. The 0.55 constant is obsolete for modern assays; quoting it is a known fail. [1]
- Know the KDIGO thresholds as numbers: G1 at least 90, G2 60 to 89, G3a 45 to 59, G3b 30 to 44, G4 15 to 29, G5 under 15. Renal dose reduction usually matters from G3a. [4]
- Child-Pugh is five variables (bilirubin, albumin, INR, ascites, encephalopathy) summed into A, B, C. The INR tracks hepatic synthetic function better than the ALT. [6]
- The loading dose still applies; the maintenance dose falls. This single principle resolves most "do I load?" questions in organ impairment. [5]
- Vancomycin moved to AUC-guided dosing (400 to 600 mg per h per L) in 2020; a trough drawn just before the dose is the pragmatic surrogate where AUC tools are absent. [7]
- Gentamicin is extended-interval; the trough should be low or undetectable; the interval is tailored to the level. Aminoglycosides are concentration-dependent, so extend the interval rather than shrink the dose. [10]
- Hypoalbuminaemia raises the free fraction of phenytoin; send a free level when the albumin is low, and report the albumin with the total. [5]
- Never stack nephrotoxins without a compelling reason and monitoring; NSAID plus aminoglycoside, and vancomycin plus piperacillin-tazobactam, are the classic offenders. [11] [12]
- A trough is taken just before the next dose; getting the timing wrong invalidates the level and the dose decision that follows. [7]
- Always name the formulary you are quoting (BNFc, RCH Melbourne) when you give a drug-specific number, and never present a remembered paediatric dose as definitive. [5] [10]
References
- [1]Schwartz GJ New equations to estimate GFR in children with CKD J Am Soc Nephrol, 2009.PMID 19158356
- [2]Ng DK Self-reported Race, Serum Creatinine, Cystatin C, and GFR in Children and Young Adults With Pediatric Kidney Diseases: A Report From the Chronic Kidney Disease in Children (CKiD) Study Am J Kidney Dis, 2022.PMID 34974031
- [3]Pottel H Development and Validation of a Modified Full Age Spectrum Creatinine-Based Equation to Estimate Glomerular Filtration Rate Ann Intern Med, 2021.PMID 34280339
- [4]Stevens PE Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline Ann Intern Med, 2013.PMID 23732715
- [5]Verbeeck RK Pharmacokinetics and dosage adjustment in patients with renal dysfunction Eur J Clin Pharmacol, 2009.PMID 19543887
- [6]Verbeeck RK Effect of hepatic insufficiency on pharmacokinetics and drug dosing Pharm World Sci, 1998.PMID 9820880
- [7]Rybak MJ Therapeutic monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus infections: A revised consensus guideline and review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists Am J Health Syst Pharm, 2020.PMID 32191793
- [8]Zhang T Revised therapeutic window for vancomycin in pediatric patients: evidence from a retrospective therapeutic drug monitoring study BMC Pharmacol Toxicol, 2025.PMID 41254740
- [9]Han J Implementation of Vancomycin Therapeutic Monitoring Guidelines: Focus on Bayesian Estimation Tools in Neonatal and Pediatric Patients Ther Drug Monit, 2022.PMID 34145165
- [10]Soeorg H Pharmacokinetics of Gentamicin Components C1, C1a, and C2/C2a/C2b and Subsequent Decline in Glomerular Filtration Rate in Neonates AAPS J, 2022.PMID 35760955
- [11]Holsteen PE Nephrotoxic Exposures and Acute Kidney Injury in Noncritically Ill Children Stratified by Service Hosp Pediatr, 2022.PMID 36102129
- [12]Gavigan HW Blood transfusion rates in Baby NINJA (Nephrotoxic Injury Negated by Just-in-Time Action)-a single-center experience Pediatr Nephrol, 2021.PMID 33479823