Paeds · clinical-pharmacology-and-therapeutics
Safe prescribing, administration and monitoring
Also known as Medication safety in children · Preventing paediatric medication errors · The rights of medication administration · Therapeutic drug monitoring in children · High-alert medicines and dose checking
Fellowship guide to safe prescribing, administration and monitoring of medicines in children: the medication-use process, the paediatric factors that make dosing error-prone (weight-based calculation, developmental pharmacokinetics, off-label use), where errors happen and how to stop them (the rights of administration, independent double-checks, computerised order entry with decision support, unit-based pharmacists, standard concentrations), high-alert medicines, and therapeutic drug monitoring targets for gentamicin, vancomycin and phenytoin, with ANZ, UK, US and Canada guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The rights of medication administration — every dose, every time
Overview & Definition
A four-year-old on the ward is prescribed gentamicin for a urinary infection. The dose is worked out from her weight, written on a chart, transcribed, drawn up, given over an hour, and followed by a level. Each of those steps is a chance to get it right or to harm her, and a medication error at any one of them — a misplaced decimal, a missed level, a doubled dose after transfer — can outpace the infection itself. Safe prescribing, administration and monitoring is the discipline of running a medicine through that whole chain so that the right child reliably gets the right drug, at the right dose, by the right route, at the right time, with the response checked. [1] [1]
Medication safety draws a clear line between an error and the harm it may cause. A medication error is any preventable event in the medication-use process that may cause or lead to inappropriate use, whether or not the child is injured; an adverse drug event is actual harm from a medicine, which may be preventable, ameliorable, or unavoidable. Most errors are intercepted or cause no harm, yet they mark a system whose next failure may not be benign, which is why safety practice hunts the error even when no child was hurt. [1] [7]
The paediatric difference is the whole reason this topic exists as its own subject. Adults take standard doses; children almost never do. A dose depends on weight or body-surface area, on age-dependent handling of the drug, and often on an evidence base extrapolated from adults and used off-label, so the calculation step that adults skip is the single most error-prone step in children. Layer on the narrow therapeutic windows of neonatal and critical care medicines, and a safe system is not a courtesy but a necessity. [5] [10]
Classification
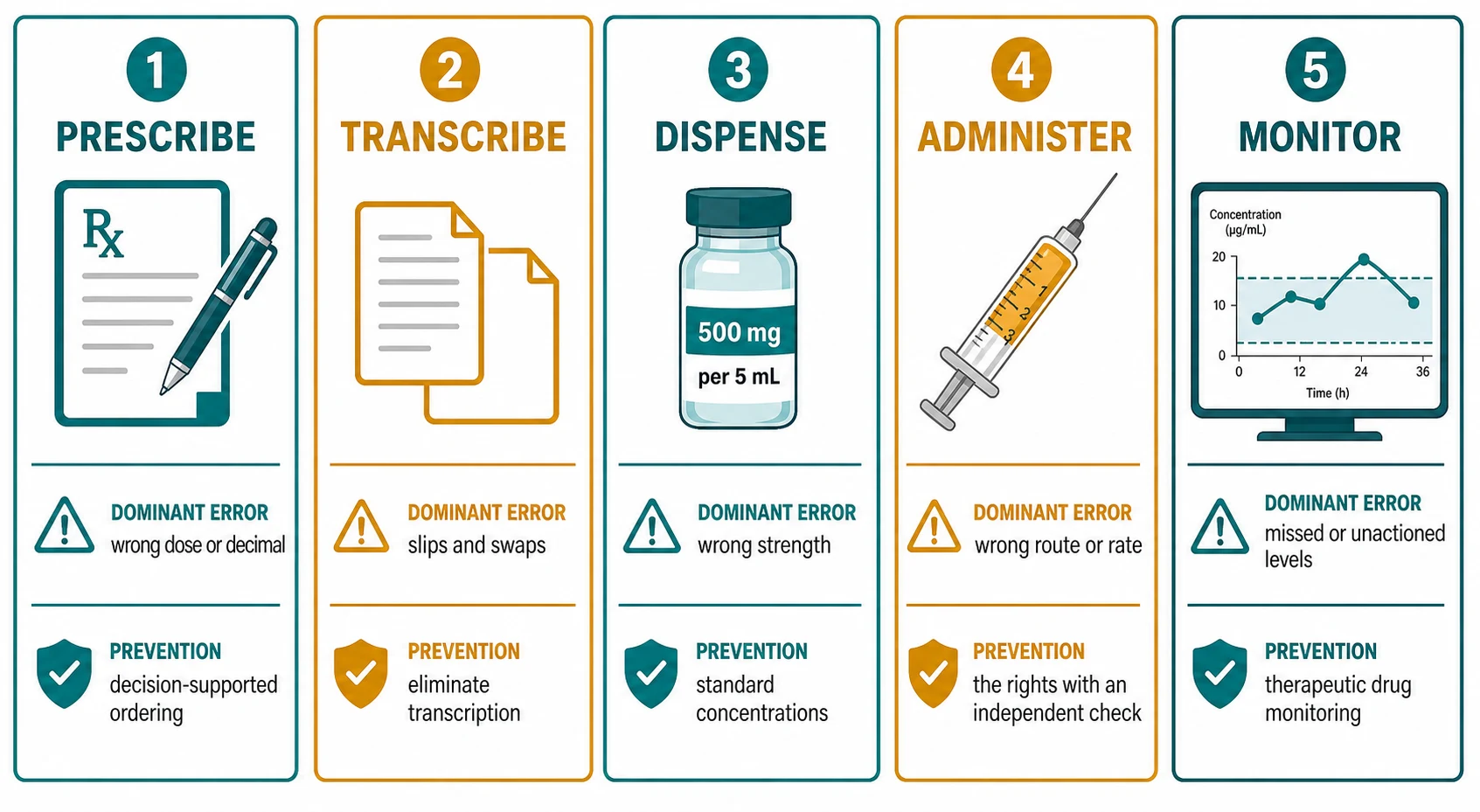
Sort medicines safety work by where in the medication-use process the failure occurs, because each stage owns different errors and different fixes. [1] [2]
Prescribing errors originate at the pen or the order entry screen — a wrong drug, a wrong dose from a miscalculation, a decimal-point slip, a look-alike name, or an un-indicated medicine. Prescribing generates more errors than any other stage, so it is also where prevention pays back most. [1] [2]
Transcription errors appear when a medicine is re-written or re-entered, such as a transfer between wards, a paper-to-electronic move, or a verbal telephone order. Each hand-off is a chance to drop a digit or swap a drug, which is why minimising transcription and reconciling at every transition are core defences. [3]
Dispensing and preparation errors happen in pharmacy or at the bedside — a wrong strength selected, a tablet split badly, an infusion compounded at the wrong concentration. Standard concentrations and ready-to-administer products shrink this category sharply. [8]
Administration errors are failures at the bedside itself — the wrong rate on an infusion pump, a route error, a missed or extra dose, or a high-alert drug given without a check. These are the errors most likely to reach the child, so the rights of administration and an independent double-check sit here. [1] [1]
Monitoring errors are the silent failures — a gentamicin or vancomycin level never taken, a result not acted on, a drug continued when renal function has fallen, or a clinic not reviewing adherence. Monitoring closes the loop, and its absence converts an otherwise safe prescription into harm. [9] [11]
Epidemiology & Risk Factors
Medication errors and adverse drug events are more frequent in children than in adults, and they cluster where the calculations are hardest. In Kaushal's landmark cohort of two paediatric hospitals, roughly 6 in every 100 medication orders contained an error, and the highest error rates were in the paediatric and neonatal intensive care units, where weights are smallest, doses most precise, and infusions most common. [1]
Adverse drug events are likewise common. A systematic review and meta-analysis of prospective studies estimated the incidence of adverse drug reactions in paediatric inpatients at around 9.5 per cent — roughly one in ten hospitalised children — with higher rates in neonatal and intensive care settings and a substantial proportion judged preventable. [7]
A large share of what is prescribed to children was never licensed or tested for them. Across European paediatric wards, a high proportion of prescriptions were unlicensed or off-label, and the figure was highest in neonatal units, where the evidence base is thinnest and dosing is extrapolated most aggressively. Off-label use is not inherently wrong, but it raises the baseline risk and the burden of checking. [5] [10]
Why children carry more medication risk
The risk factors an examiner expects you to name are the ones that multiply the chance of a calculation or administration failure: very low weight or prematurity, intensive care, high number of medicines and infusions, narrow-therapeutic-index drugs, changes in renal or hepatic function, and transitions of care where a list is re-written. Each is a flag to slow down and add a check rather than to hurry. [6] [8]
Pathophysiology
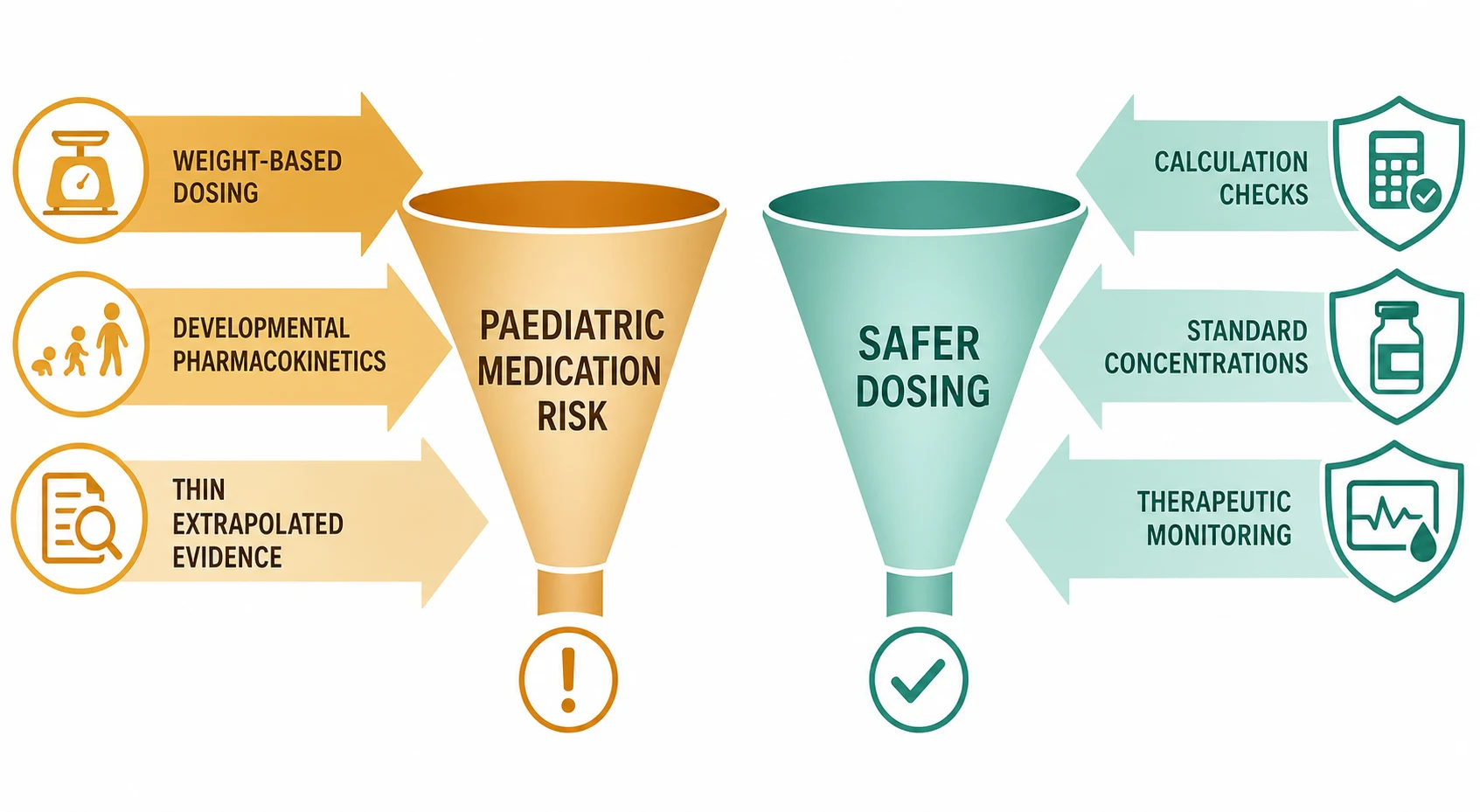
Three forces converge to make a child's prescription uniquely error-prone, and naming them is half the defence. [5] [10]
Weight-based and body-surface-area dosing means every prescription is an arithmetic act. The clinician must weigh the child, convert, calculate a per-kilogram dose, cap it at adult maxima where relevant, and choose the right units, and any one of those steps can fail. Body-surface area, used for chemotherapy and many cytotoxic and immunosuppressant regimens, is calculated from the Mosteller formula — the square root of height in centimetres times weight in kilograms divided by 3600 — and a single dropped digit propagates as a ten-fold error. [1] [5]
Developmental pharmacokinetics mean the right dose for a neonate is not the right dose for a school-age child. Water content is high and albumin binding low in early life, hepatic metabolism matures over the first months, and renal clearance rises then falls across childhood, so a dose that is correct one week may be toxic or ineffective the next as organ function changes. This developmental variation is why monitoring, not just prescribing, carries so much weight in paediatrics. [9]
A thin and extrapolated evidence base leaves prescribers to estimate where data are absent. Many medicines lack paediatric pharmacokinetic studies or licensed formulations, so clinicians dilute adult products, use off-label doses, and compound bespoke concentrations, each of which adds a calculation and a chance to err. The consequence is the same as the cause: more calculation steps, more monitoring burden, more risk. [5] [10]
Clinical Presentation
Medication errors rarely announce themselves; they are detected, not presented, and the way you find them shapes how you prevent them. [1] [6]
A near miss caught at the bedside. A nurse drawing up an infusion notices the rate on the pump differs from the prescription, or a pharmacist flags a ten-fold dose before it leaves the pharmacy. Near misses are the system working; the duty is to report them so the weakness that allowed the slip is fixed before the next one is not caught. [6] [8]
An unexpected clinical deterioration. A child becomes apnoeic after an opioid, hypoglycaemic after insulin, bradycardic on a beta-blocker, or nephrotoxic after several days of an aminoglycoside. When a child deviates from their expected course, a medicine is always on the differential, and the first question is what was given, when, and at what dose. [7]
An abnormal therapeutic level. A gentamicin trough drawn before the next dose is supratherapeutic, a vancomycin area-under-the-curve estimate is outside its target window, or a phenytoin level is subtherapeutic and the child is still seizing. The level is the presentation of a monitoring or prescribing problem, and it demands action, not just documentation. [9] [11]
A double or omitted dose after transfer. The ward team and the retrieval team have both given the regular anticonvulsant, or neither has, because the medicine list was not reconciled. Transitions of care are where reconciliation failures surface, and a careful drug history at each handover is how they are found. [3]
Differential Diagnosis
When a child deteriorates or a level is abnormal, distinguish the mechanism before you act, because the fix differs for each. [6] [7]
| You see | Most likely mechanism | Distinguishing feature | Trap |
|---|---|---|---|
| Apnoea after an opioid | Opioid toxicity from dose, rate or accumulation | Pinpoint pupils, reverses with naloxone | Treating as central apnoea of prematurity |
| Rising creatinine on an aminoglycoside | Nephrotoxicity from accumulation | Supratherapeutic trough, missed level | Attributing to dehydration alone |
| Hypoglycaemia on an infusion | Insulin error or wrong rate | Low glucose, high insulin C-peptide suppressed | Calling it sepsis without checking the pump |
| Ongoing seizures on phenytoin | Subtherapeutic level | Level below target, missed or vomited doses | Loading again without checking the level |
| Two doses given overnight | Reconciliation failure at transfer | Duplicated drug on two charts | Noting it but not reporting it |
True toxicity versus a look-alike error. A child may be genuinely sensitive to a correct dose, or harmed because the wrong drug was selected from a look-alike pair — for instance hydralazine and hydroxyzine, or dopamine and dobutamine. Inspecting the original order and the dispensed product separates an adverse drug reaction from a dispensing error. [8] [6]
Medication effect versus disease progression. Sedation in a withdrawing or septic child can be disease, or it can be benzodiazepine or opioid accumulation. The discipline is to hold the medicine and reassess rather than to assume, because attributing drug effect to disease — and vice versa — is a recurring error in paediatric inpatient care. [7]
Clinical & Bedside Assessment
The bedside assessment of a prescription is a deliberate, staged check, not a glance at the chart, and it is the layer that stops errors that prescribing and dispensing missed. [1] [1]
Confirm the weight with a current, measured value. A dose calculated against an estimated or stale weight inherits whatever error is in that number, so weigh the child and document the date of the weight, then re-calculate the dose from a current reference such as the local paediatric formulary or BNF for Children. Never calculate from a parent's estimate when a scale is available. [5]
Run the rights of administration at the point of giving. Confirm the right patient with two identifiers, the right drug against the original order, the right dose re-calculated independently, the right route, the right time and frequency, and the right reason documented. For infusions add the right rate and the right concentration. [1]
Apply an independent double-check to high-alert medicines. Insulin, opioids, concentrated electrolytes such as potassium and hypertonic saline, anticoagulants, and chemotherapy should be checked by a second person who independently re-calculates the dose and verifies the pump settings, not merely glances at the label. Independence is the point: two people reaching the same answer from scratch. [6] [6]
Reconcile the medicines at every transition. On admission, build the list from the family, the general practitioner, and the dispensing pharmacy; at each internal transfer and at discharge, compare what the child was taking with what they are now prescribed, and resolve every discrepancy explicitly. Reconciliation is the single most reliable defence against doubled and omitted doses. [3]
Investigations
The investigations of medication safety are the levels, the audit tools, and the review of the order itself — each answers a different question about whether the dose is right and whether it is working. [9] [11]
Therapeutic drug monitoring targets narrow-therapeutic-index drugs whose effect cannot be judged clinically and whose clearance varies across childhood. For gentamicin given by extended-interval dosing, the pre-dose trough is taken before the second or third dose and should be less than 1 mg per litre to avoid accumulation; for traditional multiple-daily dosing, a peak of 5 to 10 mg per litre and a trough below 2 mg per litre are the conventional targets. [9]
For vancomycin in serious methicillin-resistant staphylococcal infection, the 2020 consensus guideline shifts monitoring from trough toward the area under the curve over 24 hours relative to the minimum inhibitory concentration, targeting an AUC to MIC ratio of 400 to 600, with the upper bound set to limit nephrotoxicity; where trough-only monitoring remains in use, a trough of 10 to 15 mg per litre (15 to 20 mg per litre for deep or severe infection) approximates the target. [11]
Therapeutic drug monitoring targets you must know
Renal and hepatic function must be reviewed before and during therapy with renally cleared or hepatotoxic drugs, because a dose correct at baseline becomes toxic as function changes — gentamicin and vancomycin accumulate as creatinine rises, and a falling clearance is the signal to re-dose or to check a level. [9] [11]
Medication-safety audit tools, such as trigger tools that scan for naloxone use, sudden stops, or abnormal levels, quantify harm that voluntary reporting misses, and the act of reviewing a sample of orders against the standard reveals prescribing patterns that no individual complaint will surface. Audit closes the loop between a single error and a system change. [8]
Management — Resuscitation
When a medication error or overdose is discovered, the first task is to stop the harm, not to investigate it — resuscitation comes before root-cause analysis. [1] [6]
Stop the exposure and assess the airway, breathing and circulation. Stop the infusion or withhold the suspect medicine immediately, support the airway and breathing, and establish vascular access and monitoring. The child who is apnoeic after an opioid needs ventilation and naloxone, the child who is hypoglycaemic after insulin needs glucose, and the child in shock from a vasodilator needs fluid and vasopressors. [1]
Give the antidote where one exists. Opioid toxicity reverses with naloxone, benzodiazepine overdose with flumazenil in selected cases, paracetamol overdose with acetylcysteine, beta-blocker toxicity with glucagon, and significant anticoagulant reversal with the specific agent. Knowing which medicine has which antidote is the resuscitation question, and it is answered from the drug history and the order. [1] [6]
Decontaminate and escalate as the toxin demands. Activated charcoal is considered within an hour of an oral ingestion that binds it, and discussion with a poisons centre guides the rest — the paediatric dose, the threshold for further measures, and the level of observation needed. Escalate to a higher level of care early when the toxidrome can progress, such as sustained-release ingestion or a delayed-toxicity medicine. [1]
Immediate response when an error is discovered
Stop the exposure
Stop the infusion or withhold the suspect medicine; do not wait to confirm before acting if the child is unwell.
A-B-C and support
Assess and support airway, breathing and circulation; ventilate and gain access; attach monitoring.
Give the antidote
Naloxone for opioid, glucose for insulin-induced hypoglycaemia, acetylcysteine for paracetamol — matched to the agent.
Escalate and observe
Call the poisons centre, escalate to PICU for potentially progressive toxicity, and observe for the agent's full window of effect.
Management — Definitive & Stepwise
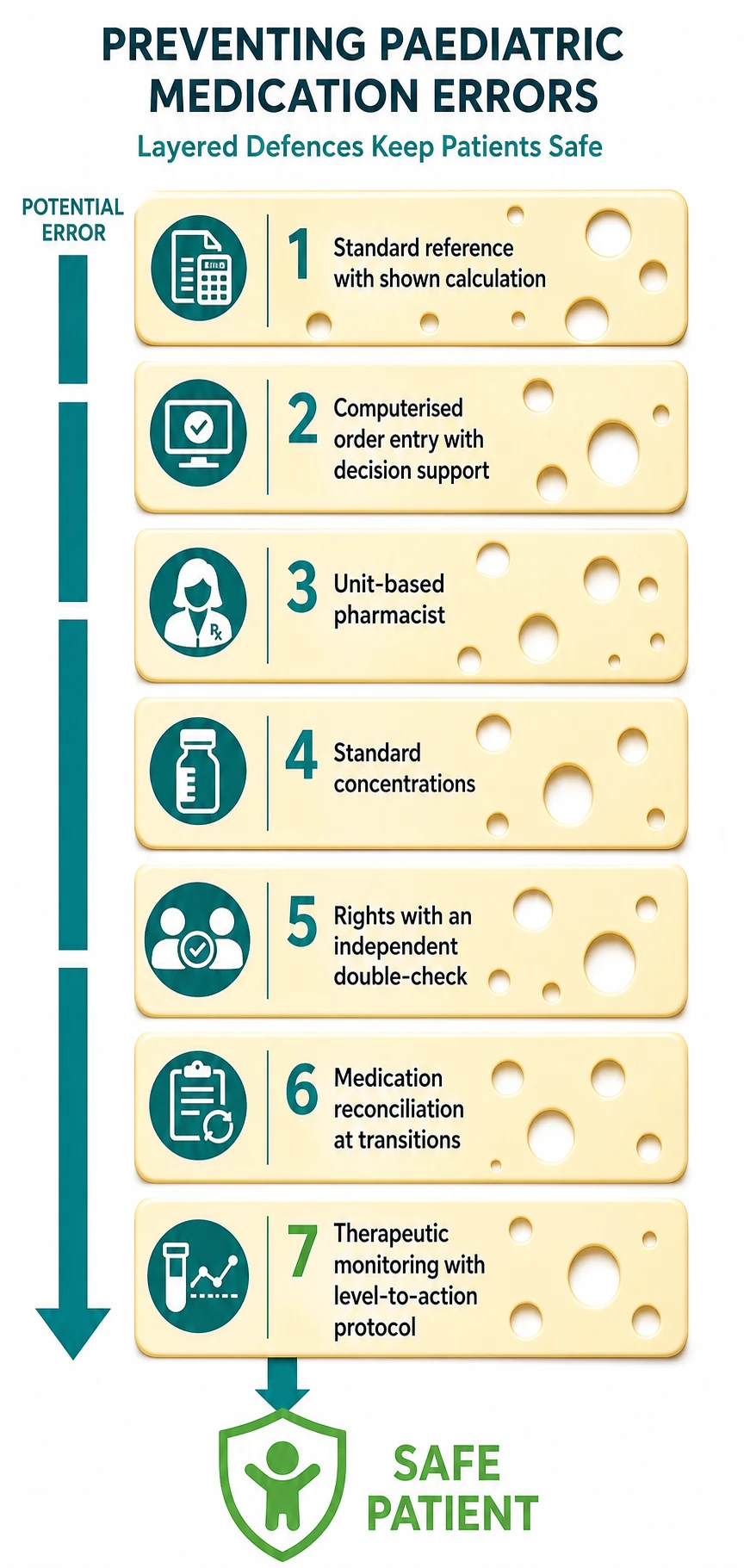
After the immediate danger has passed, definitive safety is a layered system — the Swiss-cheese model — where each layer catches what the previous missed, and where the high-yield fixes are the ones evidence has repeatedly shown to reduce error rates. [2] [8]
Prescribe from a standard reference with weight-based calculation shown. Use the local paediatric formulary or BNF for Children, state the weight and the per-kilogram calculation in the order, avoid error-prone abbreviations, and write units in full. Showing the arithmetic lets the next checker verify it, and standard references cap the variation that breeds error. [5]
Use computerised physician order entry with clinical decision support. CPOE with weight-based dosing checks, allergy and interaction alerts, and standard concentration sets intercept prescribing errors before they reach pharmacy, and modelling attributes a large share of preventable harm to its absence. Decision support is most valuable when it is specific and not noisy. [2] [3]
Embed unit-based clinical pharmacists. Pharmacists on the ward intercept serious errors at the prescribing stage, far more than order review from a central pharmacy, because they see the patient and the prescription together. This is one of the most consistently effective interventions in paediatric medication safety. [4] [8]
Standardise concentrations and use ready-to-administer products. A single standard concentration for each common infusion, and premixed or ready-to-administer products where they exist, remove the compounding step where dilution errors and ten-fold concentration slips occur. [8] [6]
Apply the rights and an independent check at administration, and monitor the response. The rights of administration are the bedside defence, an independent double-check is reserved for high-alert medicines, and therapeutic drug monitoring closes the loop for narrow-index drugs. The Cochrane review of interventions in hospitalised children found that bundled, system-level changes reduce error rates, though reducing actual harm remains harder to prove. [8]
Maaskant et al., Cochrane — interventions for reducing medication errors in children in hospital
Cochrane Database of Systematic Reviews, 2015
Systematic review of randomised and controlled studies of medication-safety interventions in hospitalised children
Key finding
System-level interventions — pharmacist involvement, standardisation, and medication reconciliation — reduced medication error rates; evidence that they reduced actual patient harm was weaker and less consistent.
Practice change
Bundle medication-safety interventions rather than relying on any single fix, and measure both error rates and patient harm separately.
Specific Subtypes & Scenarios
High-alert medicines and a handful of clinical settings account for a disproportionate share of serious harm, and each deserves its own routine. [6] [6]
Insulin is one of the most dangerous medicines on a paediatric ward, because the unit is small and a decimal or a units-versus-millilitre slip becomes a ten-fold or hundred-fold error. Prescribe in units, use standard concentrations, have a second person check every insulin infusion, and verify the pump rate against the prescription. [6]
Opioids cause apnoea and sedation, especially in the opioid-naive, the very young, and those on other depressants. Dose by weight, prescribe the lowest effective regimen, and keep naloxone accessible; the use of naloxone is itself a trigger that should prompt review and reporting. [6] [1]
Concentrated electrolytes — potassium chloride, hypertonic saline, and magnesium — are fatal in rapid bolus and must never be on the ward floor as a stock concentrate. Store them centrally, dilute to standard concentrations in pharmacy, and require an independent check and a dedicated line for administration. [6]
Anticoagulants and chemotherapy have narrow indices and serious consequences for error, and both demand independent double-checks, weight-based or body-surface-area calculation shown in the order, and careful reconciliation at transitions. For chemotherapy, the body-surface area calculation from the Mosteller formula must be verified independently. [5]
The neonate and the critically ill child combine the highest error rates with the smallest weight margin. Extended-interval gentamicin is standard in many units and is effective when monitored, but clearance varies widely in critical illness, so the trough must be taken and acted on rather than assumed. [9]
Gentamicin (extended-interval, paediatric)
Aminoglycoside — Gram-negative cover
Dose
Weight-based once-daily per local formulary; trough less than 1 mg/L
Complications & Pitfalls
The classic paediatric medication errors are few and recurring, and an examiner expects you to name each one with its mechanism and its fix. [6] [2]
Ten-fold dosing errors are the signature paediatric mistake, almost always from a misplaced decimal point, a trailing zero, or a unit confusion, and they cluster in weight-based and infusion calculations and in high-alert drugs such as opioids, insulin and anticoagulants. Over five years of surveillance at one paediatric hospital, tenfold errors reached the patient in a substantial proportion and caused harm in some — which is why decimal discipline and an independent check are non-negotiable. [6]
Decimal-point and zero errors are prevented by two simple rules: never write a trailing zero after a whole number (write 5, not 5.0), and always place a zero before a decimal less than one (write 0.5, not .5). These two habits alone remove the commonest source of ten-fold error. [2] [5]
Look-alike, sound-alike drug names and dangerous abbreviations cause selection and transcription errors — hydralazine with hydroxyzine, dopamine with dobutamine, or the ambiguous U or IU for units. Tall-man lettering, full unit names, and avoiding non-standard abbreviations are the countermeasures. [6]
Missed or mis-handled therapeutic levels convert a correct prescription into harm. A gentamicin trough not taken, a vancomycin area-under-the-curve estimate not acted on, or a phenytoin level that drifts out of range without dose adjustment are all monitoring failures, and each is preventable by a protocol that ties the level to an action. [9] [11]
Prognosis & Disposition
Most medication errors cause no harm, but the ones that do are serious, and the prognosis depends less on the error itself than on how quickly it is recognised and reversed. [1] [7]
A child who has received a significant overdose, or who is symptomatic, is observed or admitted for the full window of the agent's toxicity — which may be many hours for sustained-release or delayed-toxicity medicines — and escalated to a higher level of care if the toxidrome can progress. A child who received a ten-fold error caught before any dose, or a minor dose deviation with no effect, may need only observation and a clear explanation to the family. [1]
The disposition extends beyond the child to the system. Every error and near miss is reported through the local incident system, reviewed for root cause, and fed back to the team as a change — a standard concentration, a CPOE rule, a double-check protocol — so that the same weakness cannot produce the same harm twice. Open disclosure to the family is part of the disposition, not an afterthought to it. [8] [1]
A safety-net is only real if it is spoken. The family leaves knowing what to watch for, who to call, and when to return, and the record documents the error, the disclosure, the actions taken, and the plan for follow-up of any level or effect. [1]
Special Populations
Each high-risk group adds a layer to the standard routine, and recognising the group is the trigger to add the extra check. [5] [9]
Neonates, especially preterm infants, carry the highest medication risk: the smallest weights, the most variable clearance, the most off-label use, and the most dilute, bespoke concentrations. Doses are calculated from a current, measured weight and often from gestational age, and levels are checked more frequently because clearance changes week to week. [9] [5]
Children with medical complexity and technology dependence take many medicines, often through enteral tubes or central lines, and move between home, ward, and intensive care. The burden of reconciliation is highest here, and a shared, current medication list carried with the child is one of the most practical defences. [3]
Children with renal or hepatic impairment need doses adjusted to function and then monitored as that function changes, because a correct dose at baseline becomes toxic as clearance falls. This links directly to the renal and hepatic dose-adjustment topic, and the dose and the level are reviewed together. [9] [11]
Aboriginal and Torres Strait Islander, Maori, and other Indigenous children, and children in out-of-home care or socioeconomic disadvantage, may move between carers and services, so the medication list and the adherence story are checked rather than assumed, and barriers to obtaining and giving medicines are addressed practically rather than judged. A strengths-based, culturally safe approach to the drug history is part of safe prescribing. [1]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric medication safety has matured from landmark incidence studies to systematic reviews of interventions, but the core lessons are stable across regions. [1] [8]
Kaushal's 2001 JAMA study established that medication errors and adverse drug events are more frequent in children than in adults and concentrate in intensive care; Fortescue and colleagues then modelled which strategies would prevent the most harm and ranked computerised order entry with decision support and unit-based pharmacists highest; Wang and the later Kaushal pharmacist study confirmed that ward-based pharmacists intercept serious errors. [1] [2] [3] [4]
Doherty's five-year review of tenfold errors named the recurring culprits — weight-based and infusion calculations, high-alert drugs, decimal and unit slips — and the Cochrane review of hospital interventions concluded that bundled, system-level changes reduce error rates even where reducing measured harm remains harder to demonstrate. [6] [8]
In Australasia, the Royal Children's Hospital Melbourne guidelines and the Australian donut-hole standards underpin practice, with the AMH Children's Dosing Companion as the standard local reference for doses, and mandatory open-disclosure and incident-reporting expectations. High-alert medicines carry standard ward-storage and double-check requirements. [1]
Exam Pearls
Mnemonic — the five stages of the medication-use process: Prescribe, tranScribe, disPense, Administer, Monitor — remember "P-S-P-A-M", and that prescribing and administration own the most errors while monitoring owns the silent ones. [1] [8]
Frequently misremembered facts, correctly stated. The gentamicin extended-interval target is a trough below 1 mg per litre, not the peak; the vancomycin target is now area-under-the-curve based, not a fixed trough; an effective double-check is independent re-calculation, not agreement with the first number; and adverse drug reactions are common (about 9.5 per cent of inpatients) even when no error occurred. [9] [11] [7]
The viva trap. Asked "how would you prevent medication errors in your unit," do not list one intervention. Give the layered answer — standard reference and shown calculation at prescribing, CPOE with decision support, unit-based pharmacists, standard concentrations, the rights with an independent check for high-alert drugs, reconciliation at transitions, and monitoring with level-to-action protocols — and name audit and reporting as the system that learns from the errors that still occur. [2] [8]
References
- [1]Kaushal R, Bates DW, Landrigan C, McKenna KJ, Clapp MD, Federico F Medication errors and adverse drug events in pediatric inpatients. JAMA, 2001.PMID 11311101
- [2]Fortescue EB, Kaushal R, Landrigan CP, McKenna KJ, Clapp MD, Federico F Prioritizing strategies for preventing medication errors and adverse drug events in pediatric inpatients. Pediatrics, 2003.PMID 12671103
- [3]Wang JK, Herzog NS, Kaushal R, Park C, Mochizuki C, Weingarten SR Prevention of pediatric medication errors by hospital pharmacists and the potential benefit of computerized physician order entry. Pediatrics, 2007.PMID 17200262
- [4]Kaushal R, Bates DW, Abramson EL, Soukup JR, Goldmann DA Unit-based clinical pharmacists' prevention of serious medication errors in pediatric inpatients. American journal of health-system pharmacy : AJHP, 2008.PMID 18574016
- [5]Conroy S, Choonara I, Impicciatore P, Mohn A, Arnell H, Rane A Survey of unlicensed and off label drug use in paediatric wards in European countries. European Network for Drug Investigation in Children. BMJ, 2000.PMID 10625257
- [6]Doherty C, Mc Donnell C Tenfold medication errors: 5 years' experience at a university-affiliated pediatric hospital. Pediatrics, 2012.PMID 22473367
- [7]Impicciatore P, Choonara I, Clarkson A, Provasi D, Pandolfini C, Bonati M Incidence of adverse drug reactions in paediatric in/out-patients: a systematic review and meta-analysis of prospective studies. British journal of clinical pharmacology, 2001.PMID 11453893
- [8]Maaskant JM, Vermeulen H, Apampa B, Fernando B, Ghaleb MA, Neubert A Interventions for reducing medication errors in children in hospital. Cochrane Database of Systematic Reviews, 2015.PMID 25756542
- [9]Lopez SA, Mulla H, Durward A, Tibby SM Extended-interval gentamicin: population pharmacokinetics in pediatric critical illness. Pediatric critical care medicine, 2010.PMID 19770786
- [10]Kimland E, Odlind V Off-label drug use in pediatric patients. Clinical pharmacology and therapeutics, 2012.PMID 22472984
- [11]Rybak MJ, Le J, Lodise T, Levine D, Bradley J, Liu C Executive Summary: Therapeutic Monitoring of Vancomycin for Serious Methicillin-Resistant Staphylococcus aureus Infections: A Revised Consensus Guideline and Review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Journal of the Pediatric Infectious Diseases Society, 2020.PMID 32659787