Paeds · clinical-pharmacology-and-therapeutics
Therapeutic drug monitoring
Also known as Drug level monitoring in children · TDM in paediatrics · Therapeutic drug monitoring · Vancomycin and gentamicin monitoring · Phenytoin level monitoring
A fellowship approach to therapeutic drug monitoring in children covering why narrow-therapeutic-index drugs such as aminoglycosides, vancomycin, phenytoin, digoxin and tacrolimus are monitored, how developmental pharmacokinetics and the maturation of glomerular filtration move a level, how linear and Michaelis-Menten nonlinear kinetics differ, the vancomycin area-under-the-curve target, extended-interval aminoglycoside dosing, the phenytoin free fraction in hypoalbuminaemia, and the correct sampling times for a true trough, peak and steady-state level.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a three-year-old on a gentamicin drip for a urinary tract infection, a neonate on vancomycin for a line infection, and a ten-year-old on phenytoin for epilepsy. Each child carries a drug whose healing dose and its harmful dose sit close together. Therapeutic drug monitoring is the discipline that keeps those children in the safe gap between the two. [6] [7]
A drug earns monitoring when two things are true at once. First, the dose that achieves the effect and the dose that causes harm lie close together — a narrow therapeutic index. Second, the blood concentration predicts the effect better than the dose alone does, because between the dose written and the level reached stand absorption, distribution, metabolism, excretion, age, organ function, interactions and adherence. Aminoglycosides, vancomycin and phenytoin meet both tests; amoxicillin does not, because a wide gap separates its effective dose from any toxic dose. [6] [7]
From the first dose to a safe, on-target level
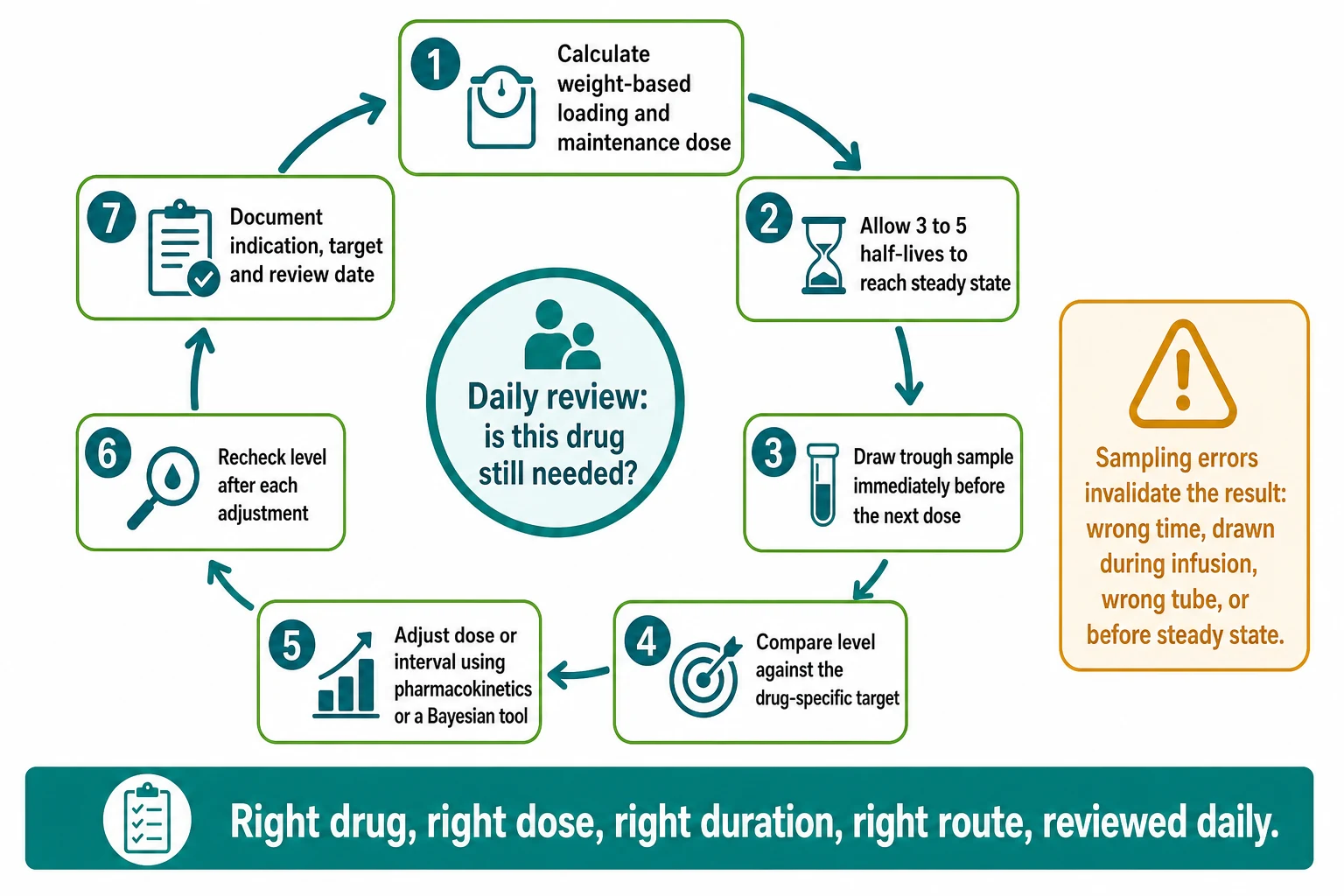
1 · Dose by weight and age
Prescribe a weight-based loading and maintenance dose, age-adjusted for developmental pharmacokinetics and organ function.
2 · Reach steady state
Wait four to five half-lives (for vancomycin, usually around the fourth dose) before interpreting a maintenance level, unless a post-load level is needed urgently.
3 · Sample at the true trough
Draw the trough immediately before the next dose, from a clean line, not during the infusion.
4 · Compare to the target
Match the level to the age-specific target: AUC for vancomycin, peak for aminoglycosides, range for anticonvulsants.
5 · Adjust and recheck
Change the dose or interval using pharmacokinetics or a Bayesian tool, then recheck after steady state is re-established.
Classification
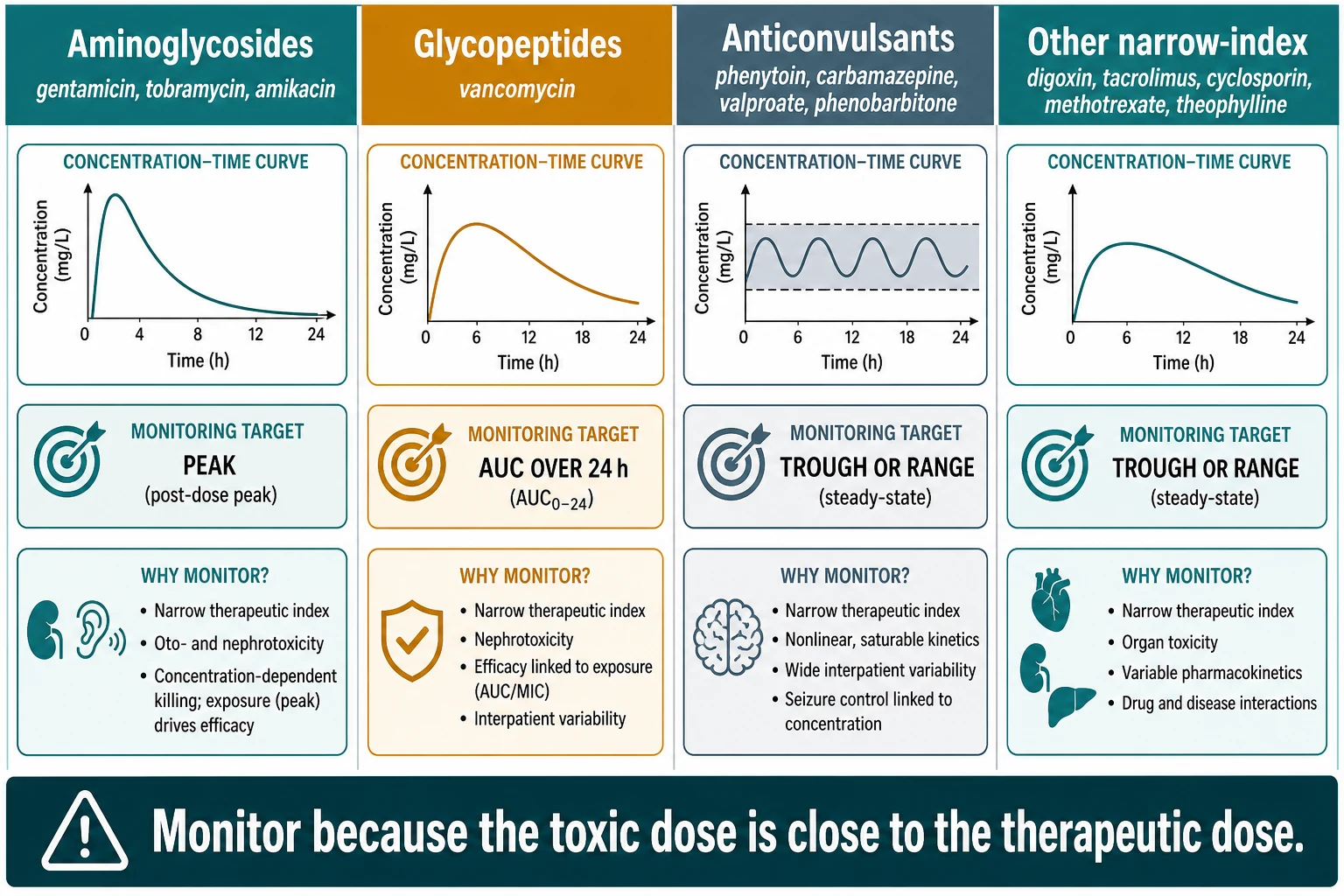
The drugs a general paediatrician monitors fall into four practical groups, and the group tells you which pharmacokinetic number to chase. Aminoglycosides such as gentamicin, tobramycin and amikacin are concentration-dependent killers: you monitor the peak, because the higher the peak above the minimum inhibitory concentration (MIC), the better the kill. Vancomycin is an area-under-the-curve drug: you monitor the total exposure over 24 hours relative to the MIC, because that exposure predicts both cure and toxicity. The anticonvulsants — phenytoin, carbamazepine, valproate and phenobarbitone — are range drugs: you keep the concentration inside a therapeutic band to prevent seizures without causing sedation or ataxia. The remaining narrow-index drugs — digoxin, tacrolimus, cyclosporin, methotrexate and theophylline — are monitored for organ protection, because their toxic effect falls on the heart, the kidney, the marrow or the brain. [1] [5]
| Drug | Why monitor | Parameter you target | Key caution |
|---|---|---|---|
| Aminoglycosides (gentamicin, tobramycin, amikacin) | Narrow index; oto- and nephrotoxicity; concentration-dependent kill | High peak; low or undetectable trough | Once-daily extended interval; individualise in neonates |
| Vancomycin | Narrow index; nephrotoxicity; AUC over MIC drives efficacy | AUC₂₄/MIC ≥ 400 for serious MRSA | Bayesian AUC monitoring preferred; trough imprecise |
| Phenytoin | Nonlinear kinetics; narrow index; free fraction shifts | Total 10–20 mg/L (free 1–2 mg/L) | Small dose change, large level change; hypoalbuminaemia |
| Carbamazepine, valproate, phenobarbitone | Range drugs; seizure control vs toxicity | Range (verify in formulary) | Free level for valproate at high dose |
| Digoxin, tacrolimus, cyclosporin, methotrexate, theophylline | Organ protection — heart, kidney, marrow, brain | Drug- and indication-specific trough | Long-term structured monitoring; interaction-rich |
Epidemiology & Risk Factors
Therapeutic drug monitoring is everyday paediatric inpatient practice. On a single general ward round you will see vancomycin and gentamicin in the child with sepsis, phenytoin or levetiracetam in the child with epilepsy, and tacrolimus in the child after transplant. The drugs are common; the discipline of sampling at the right time is what separates safe from unsafe practice. [6]
Several factors push a level out of its target window. Young age is the most powerful, because the renal and hepatic machinery that clears a drug is still maturing. Critical illness changes both the volume of distribution (more total body water in sepsis) and the clearance (augmented renal clearance in PICU). Organ impairment — a rising creatinine, liver disease, low albumin — slows clearance or raises the free fraction. Drug interactions with enzyme inducers (rifampicin, phenytoin, carbamazepine) and inhibitors (azoles, macrolides) perturb levels of co-administered drugs. And extracorporeal circuits — ECMO, continuous renal replacement therapy, and burns — redraw both the volume of distribution and the clearance, so standard dosing misleads. [2] [7]
Neonate
Immature clearance
- Low GFR and immature hepatic enzymes
- High total body water enlarges volume of distribution
- Low albumin raises free fraction
- Intervals individualised by gestational and postnatal age
Critically ill child
Augmented clearance
- PICU augmented renal clearance lowers vancomycin levels
- Sepsis and oedema change the volume of distribution
- Higher mg/kg or more frequent dosing often needed
- Close monitoring essential
Child with organ impairment
Reduced clearance
- Rising creatinine slows aminoglycoside and vancomycin clearance
- Hypoalbuminaemia raises the free fraction of phenytoin
- Hepatic disease slows metabolism
- Reduce dose or extend the interval
Child on interacting drugs
Inducers and inhibitors
- Enzyme inducers (rifampicin, phenytoin) lower co-drug levels
- Enzyme inhibitors (azoles, macrolides) raise them
- Check the interaction before adjusting the dose
- Recheck after starting or stopping the interacting drug
Pathophysiology
The reason therapeutic drug monitoring works is that the concentration a dose produces is not fixed — it moves with the child. Four developmental processes carry the dose into the bloodstream and out again, and each one changes with age. [7]
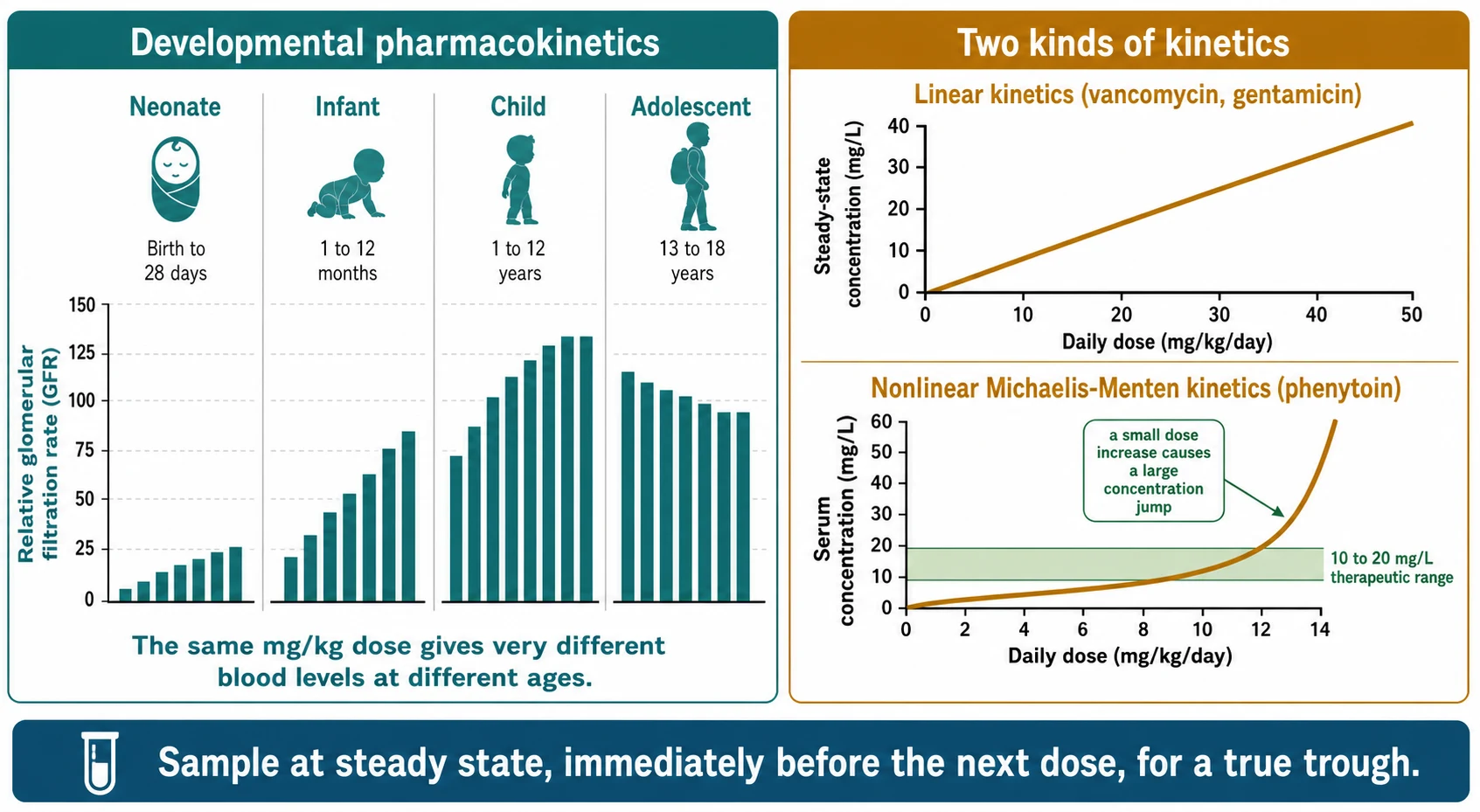
Absorption of oral drugs is variable in the neonate because gastric acidity is low and emptying is irregular, but it approaches adult patterns by infancy. Distribution changes with body composition: the neonate's high total body water and extracellular fluid enlarge the volume of distribution of water-soluble drugs such as the aminoglycosides, so the same mg/kg dose reaches a lower peak. Metabolism follows a biphasic curve — hepatic enzyme activity is slow at birth, then overshoots adult per-kilogram rates in early childhood, before settling. Elimination mirrors this pattern: glomerular filtration rate is low at birth, reaches adult values by around eight to twelve months, and exceeds adult per-kilogram values during childhood. The practical consequence is that a neonate clears many drugs slowly and a young child clears them fast, so neither age can be dosed like an adult scaled by weight. [7]
Two kinetic behaviours decide how a level responds to a dose change, and the contrast between them is the single most testable idea in this topic. Drugs with linear, first-order kinetics — vancomycin and the aminoglycosides — clear at a rate proportional to their concentration, so doubling the dose roughly doubles the steady-state level. Phenytoin is different. Its metabolism is saturable: the enzyme that clears it approaches its maximum capacity (Vmax) within the therapeutic range, governed by the Michaelis-Menten constant (Km). Below Km a dose increase raises the level proportionally; as the dose approaches Km, the clearance pathway saturates, and a small extra dose sends the level sharply upward. [8]
A second mechanism makes the total phenytoin level misleading. Phenytoin is about 90 per cent bound to albumin, so only the free 10 per cent crosses into the brain and acts. In a child with hypoalbuminaemia — nephrotic syndrome, liver disease, critical illness — the free fraction rises, and a total level that sits inside the therapeutic range can still produce toxic free-drug concentrations. A normal total level in a sick child is not reassuring on its own; request a free phenytoin level, or correct the total for albumin. [9]
Clinical Presentation
The clinical presentation of a monitoring problem is the child whose level has slipped outside its window, and you usually meet it as a change in the child rather than a change in the number. The slow-to-wake child on phenytoin, the ataxic toddler, or the child with new nystagmus is showing you a phenytoin level that has climbed above 20 mg/L. The oliguric child on gentamicin, or the child whose creatinine is creeping up on vancomycin, is showing you aminoglycoside or vancomycin accumulation. The seizing child whose phenytoin was "in range" weeks ago may have a level that has fallen because of a new enzyme-inducing drug or poor adherence. [8] [9]
Toxicity declares itself along a graded ladder that mirrors the rising concentration. With phenytoin, nystagmus appears first, often around 20 to 30 mg/L; ataxia follows around 30 mg/L; drowsiness, confusion and eventually coma appear as the level climbs higher. With aminoglycosides, the earliest injury is renal — a non-oliguric rise in creatinine that is usually reversible if the drug is stopped — and the ototoxicity is often delayed and harder to detect at the bedside. With vancomycin, the worry is nephrotoxicity, which rises with prolonged high exposure and with co-administered nephrotoxins. [6] [8]
Differential Diagnosis
When a level returns outside its target, your first job is to decide whether the level is real or whether the sample has lied. An out-of-range number has four causes, and three of them are errors you must exclude before you change the dose. [1] [10]
The first cause to exclude is a timing error. A "trough" drawn an hour after the dose, or a level drawn during the infusion, will read falsely high; a level drawn from the line that delivered the drug will be contaminated and meaningless. The second is a steady-state error — the level was checked before four to five half-lives had passed, so it reflects the loading dose rather than the maintenance dose. The third is a conversion or transcription error — phenytoin reported in µmol/L misread as mg/L, or the wrong patient's result filed against this child. Only after you have excluded all three should you conclude that the level reflects a genuine change in the child's clearance — reduced (renal impairment, interaction, reduced albumin) or augmented (PICU, burns, cystic fibrosis). [8] [10]
Clinical & Bedside Assessment
Bedside assessment of a monitoring request means checking the request, not just the child. Five questions turn a number into a safe decision. What is the dose, the route and the interval? What time was the last dose given, and what time was the sample drawn? Has the child reached steady state? Are there reasons the clearance might have changed — renal impairment, an interaction, hypoalbuminaemia, critical illness? Does the child look toxic or under-dosed, or do they look well while the number looks wrong? A request that cannot answer these needs the dose held, the sample repeated at the correct time, and the question asked again. [1] [10]
Confirming the dose and interval sounds trivial, but it is where most monitoring failures begin. A child transferred overnight may carry a dose that was changed at the referring hospital; a vancomycin interval written as "twice daily" may be operating as once-daily because the ward has slipped a dose. Always read the drug chart, the last dose time, and the sample time together. Confirming renal function (creatinine, urine output) and albumin closes the loop on clearance and free fraction. [2] [9]
When a level is high, examine the child for the toxicity that fits the drug. For aminoglycosides, look for falling urine output and a rising creatinine, and ask about tinnitus or hearing change. For phenytoin, look for horizontal nystagmus on lateral gaze, test gait for ataxia, and assess alertness. For vancomycin, check renal function and look for an infusion reaction (histamine-mediated "red man syndrome") if the infusion was fast. [6] [8]
Investigations
The investigation in therapeutic drug monitoring is the blood level itself, taken at the correct moment and interpreted against the correct target. The true trough — drawn within the 30 to 60 minutes before the next dose — is the workhorse sample for vancomycin and the anticonvulsants, because it catches the drug at its lowest point in the cycle and tells you whether accumulation is occurring. For aminoglycosides under traditional multiple-daily dosing, a peak (drawn about 30 minutes after the end of a 30-minute infusion) and a trough are paired; under extended-interval dosing, a single random level drawn 6 to 14 hours after the dose is read against a Hartford-style nomogram to set the interval. [4] [6]
| Drug | Sample | When to draw | What it tells you |
|---|---|---|---|
| Vancomycin | Trough (or AUC pair) | Within 30–60 min before the 4th dose and before each dose | Accumulation; basis for AUC calculation |
| Aminoglycoside (extended interval) | Random post-dose | 6–14 h after the once-daily dose | Read on a Hartford-style nomogram to set the interval |
| Aminoglycoside (traditional) | Peak and trough | Peak 30 min after infusion ends; trough before next dose | Peak vs MIC; accumulation |
| Phenytoin (maintenance) | Trough (total, free if low albumin) | Just before a dose, at steady state | Range; free fraction in hypoalbuminaemia |
| Tacrolimus, digoxin | Trough | Just before a dose | Long-term organ protection |
A level drawn before steady state is reached does not represent the maintenance dose — it reflects the loading dose and the rising accumulation curve. Vancomycin reaches steady state after about four to five half-lives, which in an older child is around the fourth dose; in a neonate with a long half-life this can take much longer, so neonatal levels are often timed to a calculated rather than a fixed point. When a child is critically ill and you cannot wait for steady state, you may need a level after the loading dose to confirm that the first dose achieved adequate exposure — but you must label it as such and recheck at steady state. [3] [11]
TROUGH — the five things a level must have to be trustworthy
Bayesian forecasting software and population pharmacokinetic models have moved vancomycin and aminoglycoside dosing from nomograms toward individualised prediction. A Bayesian tool takes the child's age, weight, renal function and a measured level, and estimates the individual's clearance and volume of distribution so the next dose targets the desired exposure. This is now the recommended approach for vancomycin AUC monitoring, and it is especially valuable in neonates and in PICU, where standard dosing misleads. [10] [11]
Management — Resuscitation
The resuscitation moment in therapeutic drug monitoring is the child with a toxic level and clinical toxicity. The first action is to stop the exposure: withhold the next dose of vancomycin or the aminoglycoside while you check renal function, recheck the level, and assess the child. For phenytoin toxicity with nystagmus or ataxia, withhold the next dose, provide supportive care, protect the airway if the child is drowsy, and recheck the level as it falls. There is no specific reversal agent for aminoglycoside or vancomycin toxicity — management is supportive, with attention to renal perfusion and avoidance of other nephrotoxins. [6] [8]
The immediate management of suspected sampling error is not to change the dose. Repeat the level at the correct time, confirm the dose and interval, exclude an interaction, and re-assess. A single out-of-range level that contradicts a clinically well child is more often a sampling problem than a true change in clearance. [10]
Management — Definitive & Stepwise
The definitive management of a monitored drug is to use the level to individualise the dose. Vancomycin is the drug whose monitoring has changed most. The 2020 consensus guideline from the American Society of Health-system Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists moved the target from the trough to the 24-hour area under the concentration–time curve over the MIC, recommending an AUC₂₄/MIC of 400 or more for serious MRSA infection. AUC-guided dosing — usually achieved with two timed levels or with Bayesian forecasting from a single level — achieves target exposure while reducing nephrotoxicity compared with a trough-only strategy that chased a trough of 15 to 20 mg/L. [1]
Dosing and monitoring principles (verify against the current local formulary)
Aminoglycosides illustrate how the pharmacodynamic pattern drives both the dose and the monitoring. Because gentamicin, tobramycin and amikacin are concentration-dependent killers with a post-antibiotic effect, once-daily extended-interval dosing maximises the peak, exploits the post-antibiotic effect, and minimises accumulation. Meta-analyses in neonates and in older children confirm that extended-interval dosing is as effective as traditional multiple-daily dosing with no increase in nephro- or ototoxicity — though neonatal intervals are individualised by gestational and postnatal age, and children with endocarditis, severe renal impairment, or burns may need a traditional or modified regimen. [4] [5] [6]
Phenytoin requires the most careful dose adjustment of any monitored drug because of its nonlinear kinetics. The loading dose is 15 to 20 mg/kg, given slowly intravenously because rapid infusion causes arrhythmia and hypotension; the maintenance dose starts at 4 to 8 mg/kg/day. Because the metabolism saturates near the top of the therapeutic range, every maintenance dose change must be small and followed by a recheck — a 25 per cent increment near the top of the range can double the level. When the albumin is low, request a free phenytoin level or correct the total, because the free fraction — the part that crosses into the brain — rises as albumin falls. [8] [9]
Specific Subtypes & Scenarios
The neonate is the patient where developmental pharmacokinetics matters most and where monitoring intervals are most individualised. Glomerular filtration and hepatic enzyme activity are immature in the first weeks of life, so standard mg/kg doses at standard intervals designed for older children will accumulate. Neonatal vancomycin and aminoglycoside intervals are set by gestational and postnatal age, and population pharmacokinetic and Bayesian tools developed specifically for neonates (such as DosOpt) allow individualised dose prediction from a measured level. Neonatal monitoring targets the same exposure as in older children but reaches it by a slower, age-individualised path. [4] [10] [11]
The critically ill child in PICU often has augmented renal clearance — a state of high glomerular filtration driven by inflammation, fever, vasopressors and high cardiac output — that clears vancomycin and aminoglycosides faster than standard dosing assumes. A child who should be over-exposed on a standard dose turns out to be under-exposed, and the level comes back low. The response is not to assume non-adherence (the drug is intravenous) but to raise the dose, shorten the interval, or use Bayesian AUC dosing to hit the target. A population pharmacokinetic analysis of vancomycin in infants, children and adolescents with augmented renal clearance confirms that standard regimens frequently fail to reach the AUC₂₄/MIC of 400, and that individualised dosing is needed. [2]
The monitoring timeline for a child on intravenous vancomycin
The child on long-term anticonvulsants needs monitoring at diagnosis, after each dose change, and whenever seizures break through, toxicity is suspected, or an interacting drug is added. For phenytoin, the nonlinear kinetics mean that dose changes must be small and rechecked; for valproate, a free level may be useful at high doses because the free fraction rises as the concentration climbs. The child on tacrolimus after transplant or digoxin for cardiac failure needs long-term, structured trough monitoring coordinated with the transplant or cardiology team, because these drugs interact with a long list of co-administered agents and their levels drift with changing organ function. [9]
Complications & Pitfalls
The complications of monitored drugs are the harms that monitoring exists to prevent: aminoglycoside nephrotoxicity and ototoxicity, vancomycin nephrotoxicity (worse with prolonged high exposure and co-administered nephrotoxins), phenytoin ataxia, drowsiness and cerebellar injury, digoxin arrhythmia, and methotrexate mucositis and myelosuppression. When monitoring is done well, most of these are avoidable or reversible. Aminoglycoside nephrotoxicity is usually non-oliguric and recovers over days to weeks once the drug is stopped; ototoxicity can be delayed and is harder to reverse. [4] [6]
Four pitfalls undermine monitoring at the bedside. The first is the sampling error: the level is drawn at the wrong time, during the infusion, or from the infusing line, and the number that returns is treated as if it were trustworthy. The second is the steady-state error: a level checked too early is interpreted as if it reflected the maintenance dose. The third is the conversion error: phenytoin reported in µmol/L is misread as mg/L, or a value intended for one patient is applied to another. The fourth, and the most dangerous, is treating the number instead of the child — adjusting a dose because the level is a hair outside range, without asking whether the child is seizing or ataxic. [8] [10]
Principle
- Match the dose to the concentration of a narrow-therapeutic-index drug
- Concentration predicts effect better than dose alone
- Sample at the right time, in the right child
Targets
- Vancomycin AUC₂₄/MIC ≥400 for serious MRSA
- Aminoglycoside high peak, low trough (once daily)
- Phenytoin total 10–20 mg/L, free 1–2 mg/L
- Range for carbamazepine, valproate, phenobarbitone
Sampling
- True trough within 30–60 min before the dose
- Steady state after four to five half-lives
- Not during infusion, not from the line
- Aminoglycoside random 6–14 h on a nomogram
Kinetics
- Linear: dose doubles, level roughly doubles (vancomycin, gentamicin)
- Nonlinear Michaelis-Menten: phenytoin, small change near top, large level jump
- Free fraction rises in hypoalbuminaemia
Adjust
- Pharmacokinetic or Bayesian tool
- Small phenytoin increments
- Recheck after steady state
- Document target and review date
Pitfalls
- Wrong sample time
- Before steady state
- Unit conversion error
- Treating the number, not the child
“Right target (peak, AUC, range) → right sample (true trough, steady state, clean line) → right interpretation (exclude timing, steady-state, conversion errors) → right adjustment (small, rechecked, documented) → treat the child, not the number.”
Prognosis & Disposition
The prognosis of a monitored drug depends on whether the right exposure is reached and maintained. For vancomycin, achieving an AUC₂₄/MIC of 400 or more for serious MRSA infection improves the chance of cure; for the aminoglycosides, an adequate peak relative to the MIC predicts bacterial eradication. The harms that monitoring prevents — nephrotoxicity, ototoxicity, ataxia, arrhythmia — are usually avoidable or reversible when the level is kept inside the window and the child is reviewed daily. [1] [4]
Disposition is intertwined with the level and the route. A child on intravenous vancomycin whose levels are in target, who is clinically improving, and who can tolerate an oral stepdown can move toward discharge once the antibiotic course is shortened or switched. A child who remains toxic, whose levels cannot be controlled, or who needs prolonged parenteral therapy may need continued inpatient or outpatient parenteral management with structured monitoring. The monitoring burden itself shapes disposition: a child in a remote setting who needs repeated timed troughs may need transfer or a coordinated local plan with a reliable laboratory. [6]
Aminoglycoside nephrotoxicity, when it occurs, usually recovers over days to weeks once the drug is stopped; persistent renal dysfunction warrants nephrology review. Ototoxicity can be delayed, so a child who has had a prolonged aminoglycoside course should have hearing surveillance after recovery. [4] [6]
Special Populations
The neonate needs age-individualised dosing and monitoring as a core safety measure, not a refinement. Low glomerular filtration and immature hepatic enzymes slow clearance; high total body water enlarges the volume of distribution for water-soluble drugs; and low albumin raises the free fraction of highly bound drugs. Neonatal vancomycin and aminoglycoside intervals are set by gestational and postnatal age, and Bayesian tools developed for neonates allow individualised prediction. The neonate is the patient at highest risk of both under- and over-exposure, and monitoring is the safeguard that keeps the dose on target. [4] [10] [11]
The critically ill child with augmented renal clearance in PICU frequently underachieves the vancomycin target on standard dosing; the response is to raise the dose, shorten the interval, or use Bayesian AUC dosing. The child with cystic fibrosis has both altered volume of distribution and enhanced clearance of aminoglycosides, so higher mg/kg doses and closer monitoring are needed for an acute exacerbation. The immunocompromised child on tacrolimus and the cardiac child on digoxin need long-term, structured trough monitoring coordinated with their specialist teams, because their levels drift with changing organ function and with the many drugs they take. [2] [9]
Australia and Aotearoa New Zealand: the Royal Children's Hospital Melbourne Therapeutic Drug Monitoring guideline and Therapeutic Guidelines (eTG) are the primary references for vancomycin and aminoglycoside dosing, target ranges and sampling times, with state and institutional formularies operationalising them. For Aboriginal and Torres Strait Islander and Māori children, repeated blood sampling carries a real burden, particularly for families travelling from remote settings, and a coordinated plan with trusted venous access and clear communication to the family reduces both sampling failures and the distress of repeated needles. [1]
Global and low-resource settings: where rapid turnaround of levels is not available, weight-based, age-adjusted dosing using the WHO and national formularies remains the foundation, with monitoring reserved for prolonged therapy, renal impairment, or toxicity. The principle — right drug, right dose, right duration, reviewed daily — holds even where a level cannot be measured; the discipline of documenting the dose, the interval and the review date substitutes for the number when the number is unavailable. [7]
Evidence, Guidelines & Regional Differences
The evidence base for therapeutic drug monitoring in children has matured along two lines. The first is the vancomycin AUC shift: the 2020 consensus guideline from ASHP, IDSA, PIDS and SIDP recommended AUC₂₄/MIC of 400 or more for serious MRSA infection and AUC-guided monitoring over trough-only strategies, because AUC predicts efficacy while reducing nephrotoxicity. Population pharmacokinetic work has shown that critically ill children with augmented renal clearance frequently fail to reach that target on standard dosing, and Bayesian and model-informed precision-dosing tools have been developed for both children and neonates. [1] [2] [10] [11]
The second is the aminoglycoside extended-interval evidence. Meta-analyses in neonates (Nestaas and colleagues) and in older children (Contopoulos-Ioannidis and colleagues) confirm that once-daily extended-interval dosing is as effective as traditional multiple-daily dosing with no increase in nephro- or ototoxicity, which is why it has become the default in most paediatric services — with neonatal intervals individualised by gestational and postnatal age. The phenytoin nonlinear-kinetics principle is long established in clinical pharmacology, and the effect of hypoalbuminaemia on the free fraction of antiepileptic drugs has been characterised in clinical-setting studies. [4] [5] [8] [9]
The evidence is weaker where target ranges rest on tradition rather than trials — the carbamazepine, valproate and phenobarbitone ranges are consensus-derived, and phenytoin target ranges predate modern pharmacokinetic methods. Where the evidence is weak, state the target, cite the formulary, and communicate the uncertainty rather than implying a precision the data do not support. [8] [9]
Board and assessment distinctions
RACP current PREP curriculum candidates must apply safe prescribing, weight-based dosing and therapeutic drug monitoring within the acute-illness and medication-safety learning objectives; first-year trainees from 2027 encounter it under quality-and-safety goals. RCPCH Progress+ embeds safe prescribing and monitoring as a core patient-safety outcome. The ABP General Pediatrics Content Outline covers pharmacology and medication management as a distinct domain. [1]
| Board or format | What the candidate must demonstrate |
|---|---|
| RACP DWE | Interpret a concentration–time scenario: choose the sampling time, identify the kinetic principle, or read an out-of-range level |
| RACP DCE long case | Build a monitoring and dose-adjustment plan for a complex child on vancomycin, an aminoglycoside, or phenytoin |
| MRCPCH clinical | Explain the monitoring plan to a family and demonstrate safe prescribing reasoning |
| ABP | Apply pharmacology-domain knowledge to select, dose, monitor and adjust a narrow-index drug |
| RCPSC structured oral | Defend a vancomycin AUC or phenytoin nonlinear-kinetics monitoring plan across age groups |
Exam Pearls
Viva: why do we monitor vancomycin by AUC instead of trough?
Vancomycin efficacy for serious MRSA infection depends on total 24-hour exposure relative to the MIC — the AUC₂₄/MIC — not on a single point level. A trough of 15 to 20 mg/L was used as a proxy because it roughly correlated with an AUC of 400 or more, but the correlation is imprecise: some children reach the AUC target at a lower trough, and chasing a high trough overexposes others and increases nephrotoxicity. The 2020 consensus guideline moved the target to AUC₂₄/MIC of 400 or more, measured by two timed levels or estimated by Bayesian forecasting from a single level, because AUC monitoring achieves target exposure while reducing nephrotoxicity. [1]
Structured oral: a child on phenytoin has a total level of 28 mg/L with nystagmus
First, recognise the toxicity: a total phenytoin above 20 mg/L with horizontal nystagmus is consistent with early phenytoin toxicity, and ataxia and drowsiness follow as the level rises. Withhold the next dose, provide supportive care, protect the airway if the child is drowsy, and recheck the level as it falls. Second, recognise the mechanism: phenytoin follows saturable Michaelis-Menten kinetics, so a small dose increment near the top of the therapeutic range can produce a large level rise. Third, account for protein binding: if the albumin is low, the total level understates the free (active) fraction, so request a free phenytoin level. When you restart, lower the maintenance dose in a small step and recheck. [8] [9]
References
- [1]Rybak, Michael J; Le, Jennifer; Lodise, Thomas P Therapeutic Monitoring of Vancomycin for Serious Methicillin-resistant Staphylococcus aureus Infections: A Revised Consensus Guideline and Review by the American Society of Health-system Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 2020.PMID 32658968
- [2]He, Chen-Yu; Ye, Pei-Pei; Liu, Bo Population Pharmacokinetics and Dosing Optimization of Vancomycin in Infants, Children, and Adolescents with Augmented Renal Clearance. Antimicrobial agents and chemotherapy, 2021.PMID 34339268
- [3]Camaione, L; Elliott, K; Mitchell-Van Steele, A Vancomycin dosing in children and young adults: back to the drawing board. Pharmacotherapy, 2013.PMID 24019205
- [4]Nestaas, Erik; Bangstad, Hans-Jacob; Sandvik, Leiv Aminoglycoside extended interval dosing in neonates is safe and effective: a meta-analysis. Archives of disease in childhood Fetal and neonatal edition, 2005.PMID 15857879
- [5]Contopoulos-Ioannidis, Despina G; Giotis, Nikolaos D; Baliatsa, Dimitra V Extended-interval aminoglycoside administration for children: a meta-analysis. Pediatrics, 2004.PMID 15231982
- [6]Jenh, Anna M; Tamma, Pranita D; Milstone, Aaron M Extended-interval aminoglycoside dosing in pediatrics. The Pediatric infectious disease journal, 2011.PMID 21407038
- [7]Kearns, Gregory L; Abdel-Rahman, Susan M; Alander, Scott W Developmental pharmacology--drug disposition, action, and therapy in infants and children. The New England journal of medicine, 2003.PMID 13679531
- [8]Ludden, Thomas M Nonlinear pharmacokinetics: clinical Implications. Clinical pharmacokinetics, 1991.PMID 2044328
- [9]Patsalos, Philip N; Zugman, Maria; Lake, Charlotte Serum protein binding of 25 antiepileptic drugs in a routine clinical setting: A comparison of free non-protein-bound concentrations. Epilepsia, 2017.PMID 28542801
- [10]Tasa, Tuuli; Metsvaht, Tuuli; Kalamees, Raivo DosOpt: A Tool for Personalized Bayesian Dose Adjustment of Vancomycin in Neonates. Therapeutic drug monitoring, 2017.PMID 29084032
- [11]Dao, Kant; Guidi, Monia; Andre, Perrine Optimisation of vancomycin exposure in neonates based on the best level of evidence. Pharmacological research, 2020.PMID 31108184