Paeds · clinical-pharmacology-and-therapeutics
Vaccines and immunobiology
Also known as Childhood immunisation schedule · Live vaccine contraindications · Catch-up vaccination · Vaccination in immunocompromised children · Rotavirus vaccination age limits
A fellowship approach to vaccines and immunobiology in children covering the scheduled immunisation programme with on-time dosing at birth, two, four, six, twelve and eighteen months, the distinction between live attenuated vaccines (measles-mumps-rubella, varicella, rotavirus, BCG, yellow fever) and inactivated subunit, toxoid, conjugate and recombinant vaccines, the absolute contraindications to live vaccines of significant immunocompromise and pregnancy, the four-week spacing rule when two live vaccines are not given on the same day, the strict rotavirus age limits with the first dose before fifteen weeks and the course complete by twenty-four weeks, vaccination of premature infants by chronological age with full doses and no reduction, catch-up scheduling built on minimum intervals rather than restarting, and the recognition and management of adverse events following immunisation including anaphylaxis.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a six-week premature baby reaching two months of age in the neonatal unit, a four-year-old newly arrived from overseas whose immunisation record is incomplete, and a twelve-year-old on methotrexate for juvenile idiopathic arthritis whose second measles-mumps-rubella dose is overdue. Each of them needs a vaccination decision, and each tests a different part of the immunisation pathway — on-time dosing, catch-up, and the live-vaccine rule. [1] [2]
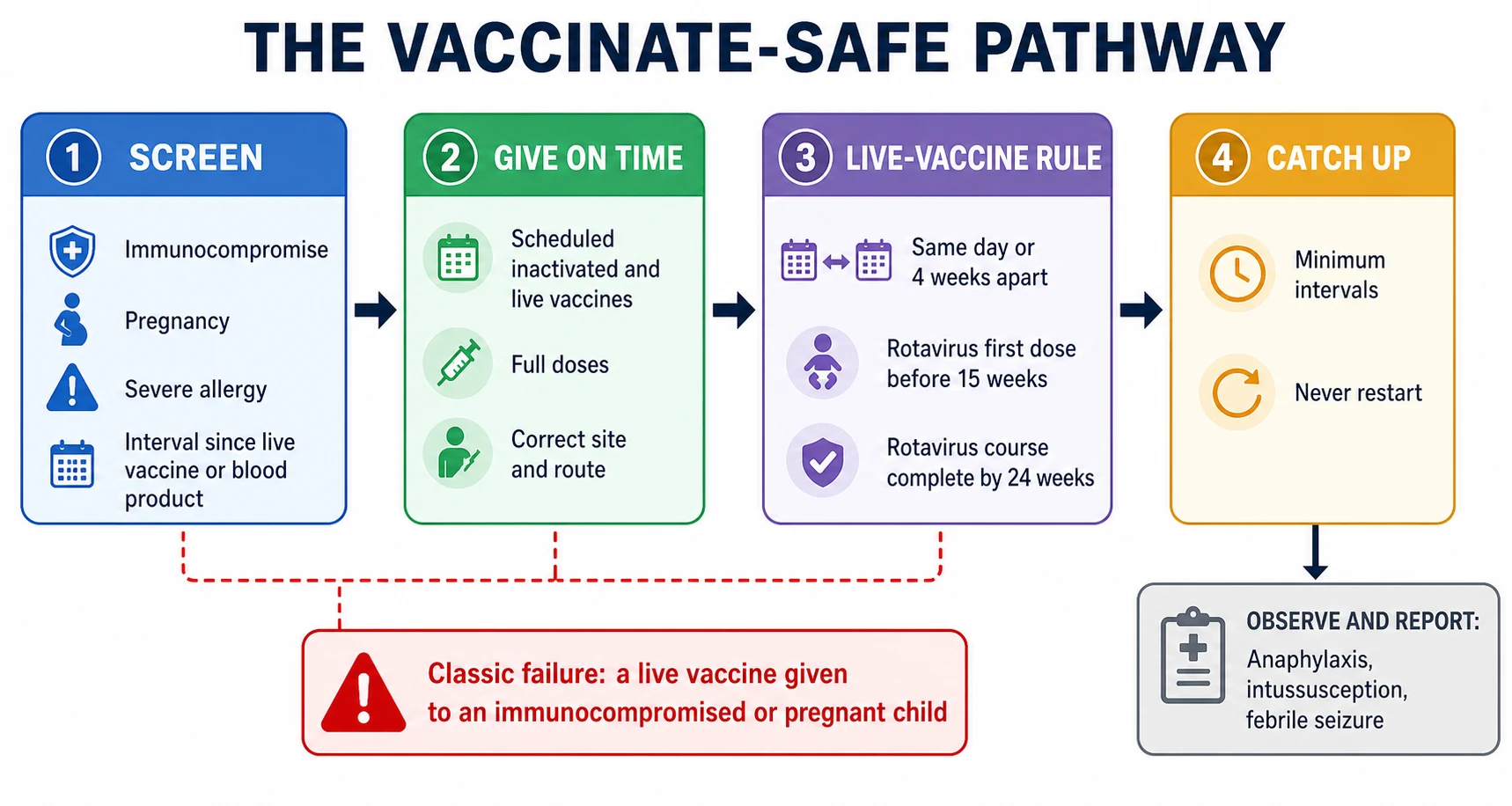
Two ideas carry the whole topic. The first is the on-time, on-schedule principle: every dose is given at the recommended age, because timely, high-coverage vaccination is what prevents outbreaks of vaccine-preventable disease and protects those who cannot be vaccinated. The second is the right-vaccine, right-child rule: before any vaccine is given you confirm there is no contraindication, check the interval since any live vaccine or blood product, and verify the child's record — and a child who is behind is caught up, never turned away. [1] [9]
From the first contact to a child safely vaccinated
1 · Confirm the child and the record
Identify the child, review the immunisation history, and confirm the vaccines due at this visit against the schedule.
2 · Screen for contraindications
Check for significant immunocompromise, pregnancy, a severe prior reaction, and the interval since any live vaccine or blood product.
3 · Decide live versus inactivated
Confirm whether a live vaccine is safe for this child, and apply the four-week spacing rule for two live vaccines not given on the same day.
4 · Give the vaccines on time
Administer at the correct age, site, and route, observe the child afterwards, and document each dose in the register.
5 · Catch up the gaps
Use minimum intervals to catch up any missed doses, report adverse events, and arrange the next visit.
Classification
The vaccines a child receives split by how they are made and whether they can replicate. The live attenuated vaccines contain a weakened organism that copies itself in the host and so generates a strong, durable immune response from a single encounter — but because they replicate, they are largely contraindicated in significant immunocompromise and in pregnancy. The measles-mumps-rubella vaccine, the varicella vaccine, the oral rotavirus vaccine, BCG, and yellow fever belong here. [1] [6]
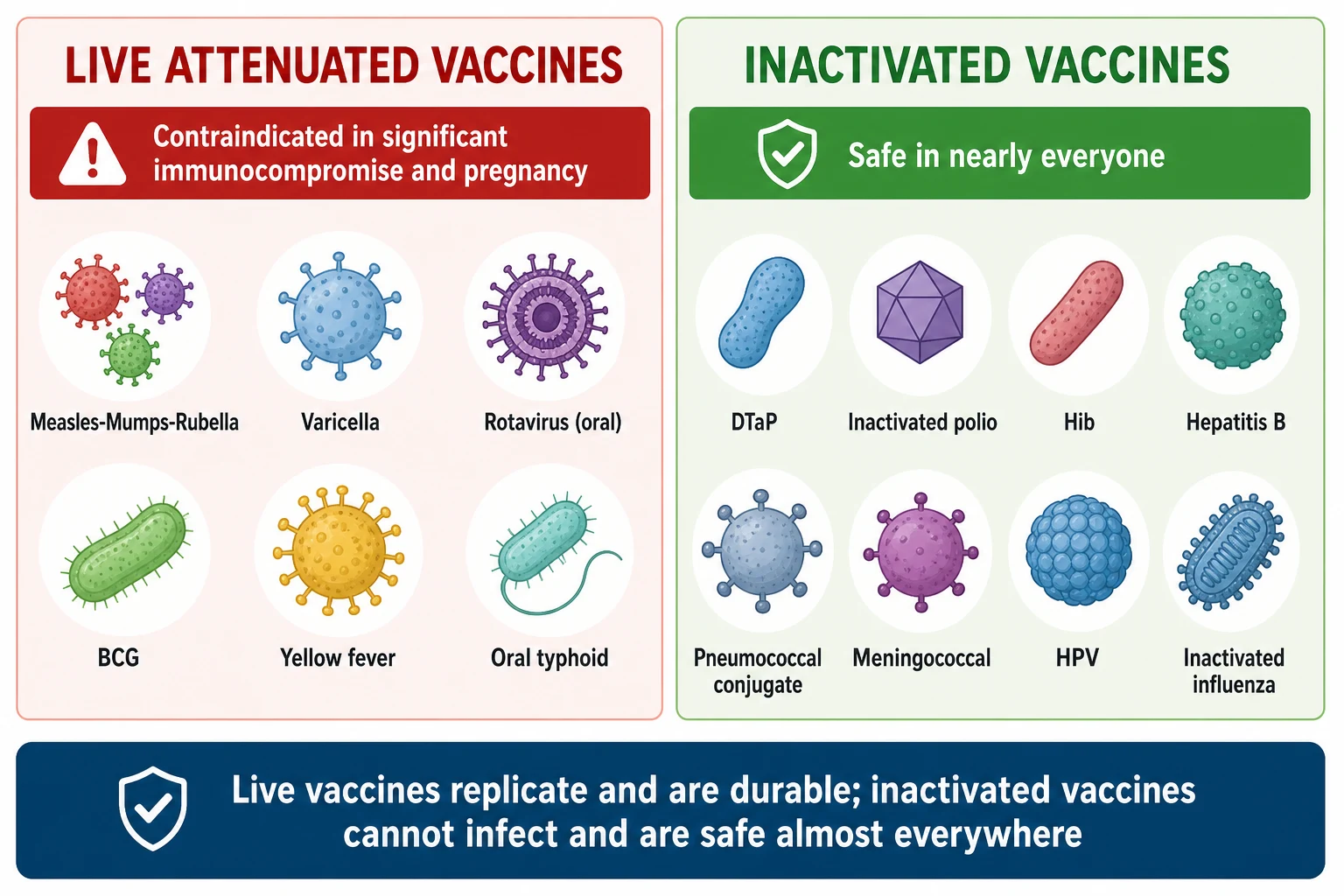
The inactivated vaccines cannot replicate and cannot cause the disease they prevent. This broad family includes the toxoid vaccines (diphtheria, tetanus), the protein subunit and recombinant vaccines (hepatitis B, human papillomavirus, COVID-19), the conjugate and polysaccharide vaccines (Haemophilus influenzae type b, pneumococcal, meningococcal), and the killed whole-organism or split-virion vaccines (inactivated polio, inactivated influenza). These are safe in immunocompromised hosts, though the immune response may be weaker and extra doses may be needed. [1] [8]
| Feature | Live attenuated vaccines | Inactivated vaccines |
|---|---|---|
| Examples | Measles-mumps-rubella, varicella, rotavirus, BCG, yellow fever | Diphtheria-tetanus-pertussis, inactivated polio, hepatitis B, pneumococcal, human papillomavirus, inactivated influenza |
| Replication in host | Yes — generates durable memory | No — cannot cause infection |
| Immunocompromised child | Largely contraindicated | Safe; response may be weaker |
| Spacing rule | Same day or at least four weeks apart | Minimum-interval catch-up applies |
| Typical number of doses | Often fewer for durable immunity | Often multiple doses and boosters |
Epidemiology & Risk Factors
High immunisation coverage is what keeps vaccine-preventable disease rare, and the bar is set by how contagious each organism is. Measles is among the most infectious agents known and needs around ninety-five per cent of the population immune to interrupt transmission, which is why even small falls in uptake allow outbreaks. The recurrence of measles in communities with low coverage is the clearest demonstration that the protection is collective, not only individual. [10]
Several factors push a child toward undervaccination and toward the harms that follow. Late or missed doses are commonest — a family moves, a visit is delayed, a record is lost — and a child who is behind is a child at risk. Premature birth once led to delayed vaccination, but the evidence supports vaccinating by chronological age with full doses. Migration and displacement leave children with incomplete or undocumented records and place them squarely in the catch-up pathway. Immunocompromise changes the live-vaccine rule entirely. And vaccine hesitancy, fed by misinformation and by genuine concern about rare adverse events, erodes the coverage on which herd immunity depends. [3] [10]
Fully vaccinated child
On-time coverage
- Receives every dose at the recommended age
- Builds individual and herd immunity
- Minimal interval checks apply
- Inactivated and live vaccines given as scheduled
Child behind on doses
Catch-up needed
- Does not restart the series
- Caught up using minimum intervals
- Live-vaccine spacing rule still applies
- Higher risk during the gap
Immunocompromised child
Live-vaccine rule
- Live vaccines largely contraindicated
- Inactivated vaccines safe but may be weaker
- Household contacts should be fully vaccinated
- Specialist input on timing and serology
Migrant or displaced child
Record gaps
- Records may be incomplete or absent
- Assume non-immune and build catch-up
- Verify against the national schedule
- Interpreter and culturally safe care
Pathophysiology
Vaccines work by persuading the immune system to remember an organism it has never truly met. The goal is the same for every vaccine — generate memory B cells and memory T cells that respond faster and stronger on a real encounter — but live and inactivated vaccines reach that goal by different routes. The live attenuated vaccines replicate silently in the host, presenting the whole organism to the immune system much as a natural infection would, which is why a single dose often produces durable immunity. The inactivated vaccines present only fragments of the organism, often with an adjuvant to boost the signal, and so usually need multiple doses and boosters. [1] [9]
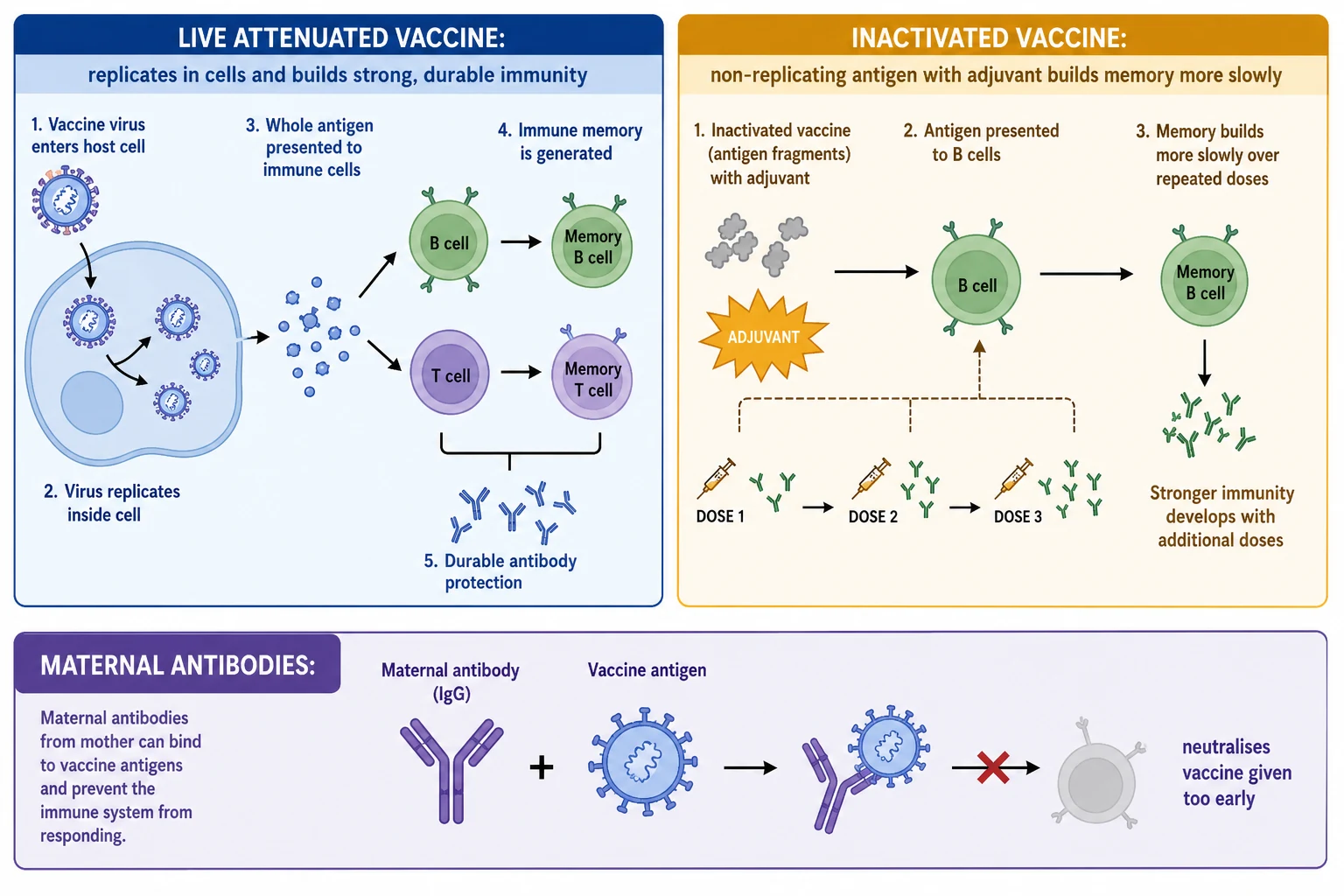
Maternal antibody is the reason the schedule is built the way it is. A young infant carries antibodies passed from the mother across the placenta and through breast milk, and these antibodies can bind a vaccine antigen and blunt the infant's own response. This is why some vaccines, particularly live vaccines such as measles-mumps-rubella, are scheduled later in the first year when maternal antibody has waned, rather than at birth when it would be neutralised. [9]
Because live attenuated vaccines replicate, two of them given close together can interfere with each other's take. The immune response mounted to the first can suppress replication of the second if they are not given on the same day, which is the biological basis of the four-week spacing rule. This interference does not occur with the oral rotavirus vaccine, which is handled separately in the gut. The same logic — that a replicating organism and a dampened immune system are a dangerous combination — is why live vaccines are contraindicated in significant immunocompromise, where they can cause uncontrolled vaccine-strain disease. [2] [11]
Clinical Presentation
You meet vaccination in three clinical settings. The first is the routine scheduled visit, where an on-time infant or child receives the vaccines due at that age and the task is to give them correctly, observe the child, and document. The second is the catch-up scenario, where a child has an incomplete record — a migrant family, a child whose parents paused vaccination, a premature infant whose doses were deferred — and the task is to build a plan with minimum intervals. The third is the child who has had a reaction or who cannot be vaccinated in the usual way, where the task is to distinguish a true contraindication from a precaution or a false belief, and to vaccinate safely. [1] [2]
Adverse events following immunisation declare themselves along recognisable lines. Common and expected reactions include fever, irritability, and redness or soreness at the injection site in the day or two after an inactivated vaccine. A measles-mumps-rubella fever or rash appears characteristically six to twelve days after the dose. The rarer, serious events include anaphylaxis within minutes of any vaccine, intussusception within a week of rotavirus vaccine, and a febrile seizure driven by post-vaccine fever. Recognising the time window is part of recognising the event. [5] [6]
Differential Diagnosis
When a family says a child "cannot be vaccinated", the first task is to separate a true contraindication from a precaution and from a false contraindication. The list of true contraindications is short: a severe allergic reaction to a previous dose or a vaccine component, and significant immunocompromise or pregnancy for live vaccines. Almost everything else families raise is a precaution or a false contraindication, and vaccinating is both safe and indicated. [1] [2]
A mild intercurrent illness, a low-grade fever, a runny nose, or a current antibiotic course are not contraindications — these are the false contraindications that most often delay vaccination in error. A family history of allergy or seizures, prematurity, and stable neurological conditions are likewise not reasons to defer. A precaution is a reason to weigh the decision, such as a moderate or severe acute illness, where vaccination is usually deferred until the child recovers rather than withheld. The safeguard in every case is to keep the list of true contraindications short, vaccinate at the next opportunity, and record the decision and its rationale. [1] [3]
Clinical & Bedside Assessment
Bedside assessment before vaccination means confirming the right child, the right vaccines, and the absence of a contraindication in a few minutes. Identify the child and the parent or guardian, and confirm consent. Review the immunisation record to confirm which vaccines are due and whether any are overdue. Ask specifically about immunocompromise — is the child on chemotherapy, high-dose corticosteroids, a biologic, or carrying a transplant or a known immunodeficiency — and, for an adolescent girl, about the possibility of pregnancy, because a live vaccine is contraindicated in pregnancy. [1] [2]
Then turn to the timing questions that catch the unwary. Ask whether the child has received a live vaccine or a blood product in the relevant interval, because a recent injectable live vaccine sets the four-week rule for the next one, and a recent blood product or immunoglobulin can blunt a live vaccine for months. Ask whether the child has ever had a severe reaction to a vaccine, and about severe allergies. Confirm the rotavirus age limits if an infant is being vaccinated, because breaching them is a recognised error. [2] [11]
Adherence and access are clinical signs worth asking about directly. A child whose doses are spread out may simply live far from a clinic, or the family may hold a concern that was never addressed. Ask about previous reactions, about cultural or religious considerations, and about what the family has heard about vaccines. A short, respectful conversation addresses most hesitancy and closes most access gaps. [10]
Investigations
Investigations are rarely needed before routine vaccination. The prevaccination assessment is clinical, built on the history and the record rather than on blood tests. Serology has a defined but limited role — confirming immunity when the record is uncertain, checking response after vaccination in a child who may mount a weak response, and guiding the plan for an immunocompromised child whose live-vaccine eligibility turns on immune function. [2] [8]
| Test | When it helps | What it tells you | Caveat |
|---|---|---|---|
| Varicella or hepatitis B serology | Record uncertain or high-risk exposure | Whether the child is already immune | Do not delay routine inactivated vaccines waiting for results |
| Immunoglobulin levels and lymphocyte subsets | Suspected immunodeficiency before a live vaccine | Whether a live vaccine is safe | Specialist immunology input on interpretation |
| Vaccine response serology | After vaccination in immunocompromised or transplant patients | Whether protection was achieved | May guide extra doses; specialist led |
| Pregnancy test | Adolescent girl before a live vaccine | Whether a live vaccine is contraindicated | A negative result clears the live vaccine |
The on-treatment monitoring for vaccination is the schedule itself. Each dose given is recorded in the register with the date, the vaccine, the batch, the site, and the route, so that the record stays accurate and the next visit is planned. Reporting adverse events following immunisation is part of the pathway, not an afterthought — passive surveillance depends on clinicians documenting the reactions they see. [1] [5]
VACCINATE — the prevaccination screen
Management — Resuscitation
The resuscitation moment in this topic is the child who collapses shortly after a vaccine. Anaphylaxis is rare but it is the event you must be ready for, and it declares itself within minutes of the injection — rapid onset of airway, breathing, or circulation compromise, often with skin changes. The immediate actions are to call for help, stop the vaccination process, position the child flat with legs raised, and give intramuscular adrenaline into the anterolateral thigh at the weight-appropriate dose, repeating as needed. Oxygen, fluid, and airway support follow, and the child is observed and admitted. [1]
For intussusception after rotavirus vaccine, the rare risk declares itself within a week of the dose with intermittent abdominal pain, vomiting, and the eventual passage of redcurrant-jelly stool. The response is the standard paediatric pathway — fluid resuscitation, imaging, and surgical or pneumatic reduction under specialist care — with the vaccination link documented and reported. For a febrile seizure driven by post-vaccine fever, the child is managed along the seizure and fever pathway, the vaccination is recorded, and the family is reassured that future vaccination should continue with antipyretic advice rather than being withheld. [5] [6]
Management — Definitive & Stepwise
The scheduled programme is the spine of definitive management. Each child receives doses on time at the recommended ages from the neonatal period through adolescence, because on-time dosing is what delivers both individual protection and herd immunity. The general paediatrician's role is to give the right vaccine at the right age, document it, and ensure no child falls behind. [1]
Vaccination principles to verify against the current national immunisation handbook
The live-vaccine rules are where most prescribing errors occur, and they deserve to be stated plainly. Two injectable live vaccines given on different days must sit at least four weeks apart, or the second dose does not count. A live vaccine is contraindicated in significant immunocompromise — primary immunodeficiency, HIV with severe immunosuppression, malignancy on chemotherapy, high-dose corticosteroids, recent transplant, or biologic immunosuppression — and in pregnancy, because a replicating vaccine organism can harm the fetus or the immunocompromised host. The oral rotavirus vaccine is held to its own strict limits: the first dose before fifteen weeks of age and the whole course complete by twenty-four weeks, reflecting the small intussusception risk that rises with age. [2] [5]
Catch-up is built on a simple, reassuring principle: a child who has fallen behind does not restart the series. Every dose already given counts, and the gaps are filled using the minimum intervals between doses — commonly four weeks. The minimum age for the first dose of each vaccine is respected, and the live-vaccine spacing rule applies throughout. A clear, written catch-up plan closes the gap and protects the child during the interval. [1] [8]
Specific Subtypes & Scenarios
The premature infant is the patient where the old instinct to defer meets the evidence to vaccinate on time. Premature babies are vaccinated according to their chronological age, not a corrected age, with the same full doses and no dose reduction, because their immune response is adequate and their risk of vaccine-preventable disease is if anything higher. The hexavalent vaccine is immunogenic and safe in preterm infants, and rotavirus vaccine can be given in the hospital setting where the infant is still an inpatient at the scheduled age. A baby of a hepatitis B surface antigen-positive mother receives the hepatitis B vaccine and hepatitis B immunoglobulin within twelve hours of birth, regardless of gestation. [3] [4]
The first year of a child moving through the immunisation schedule
The immunocompromised child is the patient where the live-vaccine rule changes everything. Live vaccines are largely contraindicated, because a replicating organism can cause uncontrolled vaccine-strain disease in a host who cannot contain it; inactivated vaccines are safe but may mount a weaker response, so serology and extra doses may guide the plan. Household contacts should be fully vaccinated to build a ring of protection, with the live-vaccine timing respected. BCG in an HIV-exposed infant is a nuanced decision — the evidence on delayed BCG in HIV-exposed babies illustrates how the timing of even a single live vaccine is weighed against the local tuberculosis risk. [2] [7]
The solid organ transplant candidate and recipient follows a defined sequence. Live vaccines are completed before transplantation while the child is still immunocompetent, and inactivated vaccines are timed around immunosuppression with serological confirmation of response afterwards, because protection achieved before transplant may persist and protection after transplant is harder to build. The American Society of Transplantation guidelines codify this sequence. The migrant or displaced child with an incomplete record is assumed non-immune and caught up with minimum intervals; the infant exposed to a biologic immunosuppressant such as a tumour necrosis factor inhibitor in utero should not receive the live rotavirus vaccine until drug clearance is confirmed, because the circulating biologic can allow vaccine-strain replication. [8] [12]
Complications & Pitfalls
The complications of vaccination are the adverse events that observation and reporting exist to capture. Common, expected reactions — fever, irritability, injection-site soreness — are self-limiting and need only reassurance and antipyretics. The rarer, serious events are few but recognisable: anaphylaxis within minutes, intussusception within a week of rotavirus vaccine, and febrile seizures driven by post-vaccine fever. Each has a characteristic time window that aids recognition. [5] [6]
Four pitfalls recur at the bedside. The first is the missed contraindication: a live vaccine given to an immunocompromised or pregnant child, with vaccine-strain disease the consequence. The second is the live-vaccine spacing error: two injectable live vaccines given a week apart and the second counted as valid when it is not. The third is the rotavirus age breach: the first dose given at or after fifteen weeks, or the course completed after twenty-four weeks. The fourth is the false contraindication: a child with a mild cold or a low-grade fever sent home unvaccinated, when vaccination was both safe and indicated. [2] [11]
Principle
- On time, on schedule — timely high coverage delivers herd immunity
- Screen every child before the needle
- Catch up, never restart
Two families
- Live attenuated — replicate, durable, contraindicated in immunocompromise and pregnancy
- Inactivated — cannot infect, safe almost everywhere, may need more doses
Live-vaccine rules
- Two injectable live vaccines: same day or at least four weeks apart
- Otherwise the second dose does not count — repeat it
- Rotavirus first dose before fifteen weeks; complete by twenty-four weeks
Special children
- Premature: chronological age, full doses, no reduction
- Immunocompromised: live vaccines contraindicated; vaccinate household contacts
- Transplant: complete live vaccines before transplantation
Contraindications
- Severe allergy to a prior dose or component
- Significant immunocompromise and pregnancy for live vaccines
- Mild illness, fever, antibiotics, prematurity are NOT contraindications
Adverse events
- Anaphylaxis within minutes — intramuscular adrenaline into the anterolateral thigh
- Intussusception within a week of rotavirus
- Febrile seizure with post-vaccine fever; continue future vaccines
“Screen (immunocompromise, pregnancy, severe allergy, timing) → give on time (right vaccine, right age, full dose, same-day-or-four-weeks for live vaccines, rotavirus within its age limits) → catch up any gap with minimum intervals, never restart → observe and report adverse events.”
Prognosis & Disposition
The prognosis for a child who is vaccinated on time is excellent — protection against a long list of once-common diseases, with a small and well-characterised burden of adverse events. Where coverage is high, vaccine-preventable disease becomes rare and the whole community is protected, including those who cannot be vaccinated. Where coverage falls, the same diseases return, and the measles outbreaks in under-vaccinated communities are the recurring reminder. [10]
Disposition is shared between the general paediatrician, primary care, and the public-health system. The clinician gives the vaccine, documents it in the register, reports adverse events, and ensures the next visit is planned. A child with a reaction is observed and, for anaphylaxis or intussusception, admitted and managed along the standard pathway. A child who is behind is enrolled in a catch-up plan with a clear, written schedule. [1] [5]
The duration of protection varies by vaccine. Some live vaccines confer long-lasting immunity from a small number of doses; many inactivated vaccines need boosters across childhood and adolescence to maintain protection. The schedule is built to deliver that protection across the life course, and the general paediatrician holds the continuity that keeps a child up to date from infancy to the transition to adult care. [6] [8]
Special Populations
The premature infant is the patient where full, on-time, chronological-age dosing matters most. Smaller and earlier babies have a higher risk of vaccine-preventable disease and an immune response that is adequate for routine vaccination, so deferring is the wrong instinct and vaccinating on time with full doses is the right one. [3] [4]
The immunocompromised child and the transplant candidate are the patients where the live-vaccine rule is absolute and the inactivated schedule is intensified. Live vaccines are withheld while the child is significantly immunosuppressed, and completed before transplantation whenever possible; inactivated vaccines are timed around treatment and confirmed with serology. [2] [8]
Australia and Aotearoa New Zealand: the Australian Immunisation Handbook of the Australian Technical Advisory Group on Immunisation and the Aotearoa New Zealand immunisation schedule are the primary references, with enhanced schedules for Aboriginal and Torres Strait Islander and Māori children that include additional doses for diseases such as hepatitis B and pneumococcal disease. For children in remote settings, cold-chain integrity, recall and reminder systems, and a single coordinator with cultural support close the access gap that drives undervaccination. [1] [7]
Global and low-resource settings: where access, cold-chain, and record-keeping are harder, the same principles hold — give every vaccine on time, catch up gaps with minimum intervals, respect the live-vaccine contraindications and spacing, and hold rotavirus to its age limits. The discipline of documenting each dose, batch, and date substitutes for technology when technology is unavailable, and a strong primary-care recall system is the single most effective tool against undervaccination. [1] [10]
Evidence, Guidelines & Regional Differences
The evidence for routine childhood vaccination rests on decades of randomised trials, surveillance, and the near-elimination of vaccine-preventable disease in high-coverage populations. The general-practice review of childhood immunisation (Wiley) integrates the schedule, the contraindications, and the catch-up principles into a single framework. The advances in vaccinating immunocompromised children (Miller and colleagues) set out which vaccines are safe and when, and the guidelines for solid organ transplant candidates and recipients (Danziger-Isakov and colleagues) codify the sequence around transplantation. [1] [2] [8]
The evidence for special groups is anchored by the safety and immunogenicity of the hexavalent vaccine in preterm infants (Omeñaca and colleagues), the systematic review of in-hospital rotavirus vaccination in premature and medically ill infants (Kerth and colleagues), and the pharmacokinetic validation of anti-tumour-necrosis-factor clearance in infants exposed in pregnancy (Wieringa and colleagues), which underpins the rotavirus caution in biologic-exposed babies. The four-week spacing question for two live vaccines is addressed by the observational study of yellow fever and measles vaccines (Michel and colleagues). [3] [4] [11] [12]
The adverse-event evidence includes the review of intussusception risk after rotavirus vaccination (Koch and colleagues), the live attenuated varicella vaccine review covering both varicella and zoster prevention (Gershon and colleagues), the delayed BCG study in HIV-exposed infants (Tchakoute and colleagues), the maternal-antibody review of interference with early vaccination (Niewiesk), and the analysis of measles outbreaks and vaccine exemptions that frames herd immunity and hesitancy (Quinn and colleagues). [5] [6] [7] [9] [10]
The evidence is weaker where it rests on regional handbook consensus rather than single trials — the exact age bands, the precise blood-product intervals, and the enhanced-schedule doses for indigenous children are handbook-defined. Where the evidence is consensus-derived, state the principle, cite the handbook, and communicate the schedule as one to verify against the current national reference. [1] [5]
Board and assessment distinctions
RACP current PREP curriculum candidates must deliver the immunisation programme, manage catch-up, and recognise adverse events within the medication-safety and acute-illness learning objectives; first-year trainees from 2027 encounter it under quality-and-safety goals. RCPCH Progress+ embeds immunisation delivery and catch-up as a core health-promotion and patient-safety outcome. The ABP General Pediatrics Content Outline tests immunisation under health maintenance.
[1] [2]| Board or format | What the candidate must demonstrate |
|---|---|
| RACP DWE | Identify the live-vaccine contraindication, the four-week spacing rule, or the rotavirus age limit in a clinical vignette |
| RACP DCE long case | Build a catch-up plan for a child with an incomplete immunisation record, applying minimum intervals and the live-vaccine rules |
| MRCPCH clinical | Counsel a family on the safety of vaccinating a premature infant or a child with a mild illness, and address vaccine hesitancy |
| ABP | Apply the schedule, contraindications, and catch-up principles under the health-maintenance domain |
| RCPSC structured oral | Defend the live-vaccine rules in immunocompromise and pregnancy, and the management of anaphylaxis after a vaccine |
Exam Pearls
Viva: why must two live vaccines be given on the same day or four weeks apart?
A live attenuated vaccine replicates in the host, and the immune response mounted to the first vaccine can interfere with the replication and take of a second live vaccine given soon afterwards. Giving them on the same day avoids this interference because both replicate from the start; giving them at least four weeks apart allows the first response to settle before the second begins. If they are given less than four weeks apart, the second dose may not take and does not count, so it must be repeated. The oral rotavirus vaccine is an exception because it replicates in the gut and does not interfere with injectable live vaccines. [11]
Structured oral: a two-month premature baby is in the neonatal unit — when and how do you vaccinate?
A premature infant is vaccinated according to chronological age, not a corrected age, with the same full doses and no reduction, because the immune response is adequate and the risk of vaccine-preventable disease is high. The scheduled vaccines due at two months are given at two months chronological age, and the oral rotavirus vaccine can be given in the hospital setting where the infant is still an inpatient, with infection-control measures to protect other vulnerable babies. A baby of a hepatitis B surface antigen-positive mother receives the hepatitis B vaccine and hepatitis B immunoglobulin within twelve hours of birth regardless of gestation. [3] [4]
References
- [1]Wiley CC Immunizations: vaccinations in general Pediatrics in review, 2015.PMID 26034255
- [2]Miller K; Leake K; Sharma T Advances in vaccinating immunocompromised children Current opinion in pediatrics, 2020.PMID 31790029
- [3]Omeñaca F; Vázquez L; Garcia-Corbeira P; Mesaros N; et al Immunization of preterm infants with GSK's hexavalent combined diphtheria-tetanus-acellular pertussis-hepatitis B-inactivated poliovirus-Haemophilus influenzae type b conjugate vaccine: a review of safety and immunogenicity Vaccine, 2018.PMID 29336924
- [4]Kerth JL; Kurz C; Obitz J; Vogel T; et al In-hospital rotavirus vaccination in premature and medically ill infants: a systematic review of uptake and safety Molecular and cellular pediatrics, 2026.PMID 42118471
- [5]Koch J; Harder T; von Kries R; Wichmann O Risk of intussusception after rotavirus vaccination Deutsches Arzteblatt international, 2017.PMID 28468712
- [6]Gershon AA; Gershon MD; Shapiro ED Live attenuated varicella vaccine: prevention of varicella and of zoster The Journal of infectious diseases, 2021.PMID 34590140
- [7]Tchakoute CT; Hesseling AC; Kidzeru EB; Gamieldien H; et al Delaying BCG vaccination until 8 weeks of age results in robust BCG-specific T-cell responses in HIV-exposed infants The Journal of infectious diseases, 2015.PMID 25108027
- [8]Danziger-Isakov L; Kumar D; AST ID Community of Practice Vaccination of solid organ transplant candidates and recipients: guidelines from the American society of transplantation infectious diseases community of practice Clinical transplantation, 2019.PMID 31002409
- [9]Niewiesk S Maternal antibodies: clinical significance, mechanism of interference with immune responses, and possible vaccination strategies Frontiers in immunology, 2014.PMID 25278941
- [10]Quinn SC; Jamison AM; Freimuth VS Measles outbreaks and public attitudes towards vaccine exemptions: some cautions and strategies for addressing vaccine hesitancy Human vaccines and immunotherapeutics, 2020.PMID 31403354
- [11]Michel R; Berger F; Ravelonarivo J; Dussart P; et al Observational study on immune response to yellow fever and measles vaccines in 9 to 15-month old children. Is it necessary to wait 4 weeks between two live attenuated vaccines? Vaccine, 2015.PMID 25843268
- [12]Wieringa JW; Kruizinga MD; Driessen GJA; van der Woude CJ; et al Validation of the pharmacokinetic model for anti-TNFα clearance in infants exposed to anti-TNFα during pregnancy Journal of crohn's and colitis, 2024.PMID 37823516