Paeds · clinical-pharmacology-and-therapeutics
Weight-based dosing, body-surface area and dose calculation
Also known as Paediatric weight-based drug dosing · mg per kilogram dosing in children · Body-surface area dosing and the Mosteller formula · Maximum adult dose cap in paediatric prescribing · Therapeutic drug monitoring and dose calculation
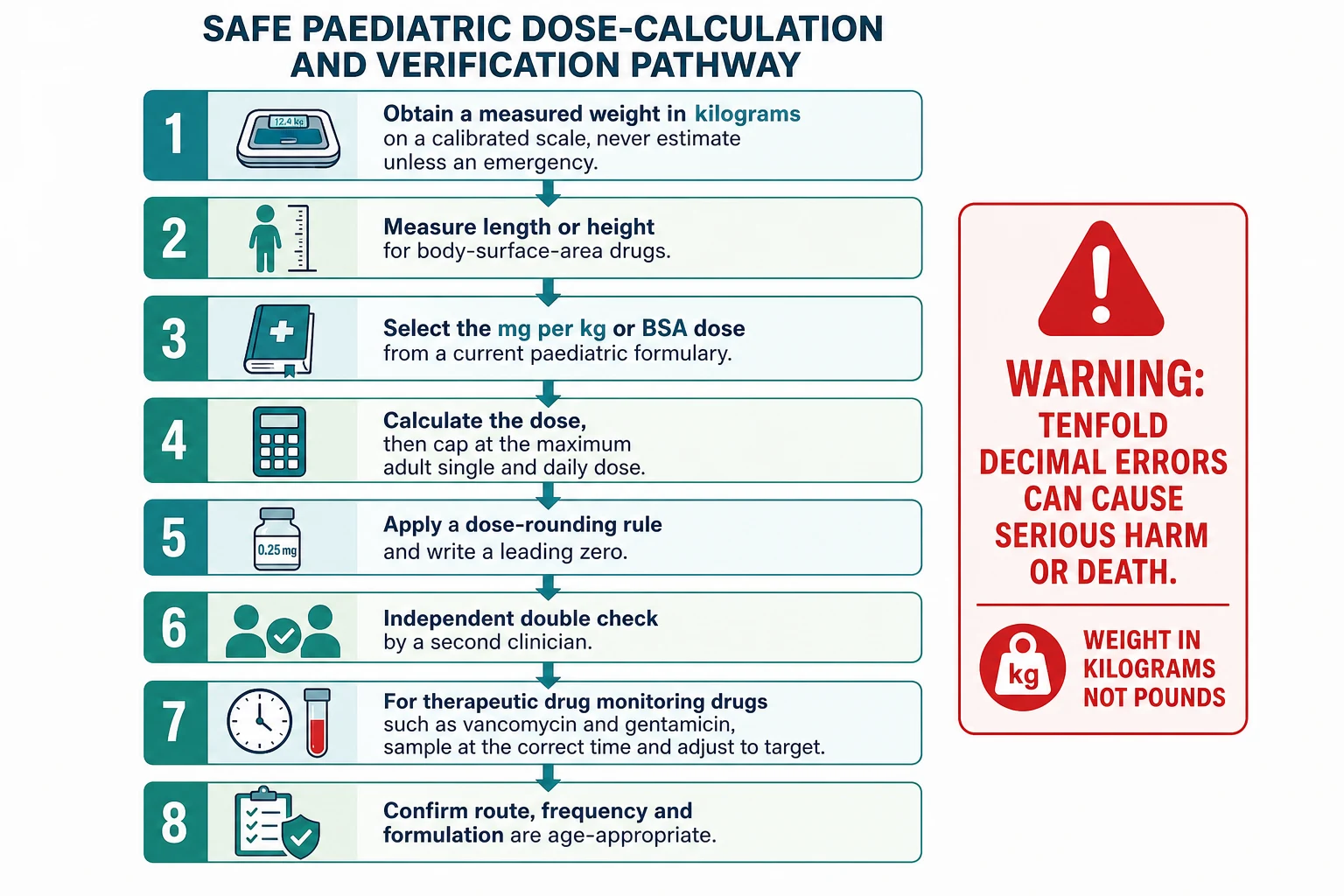
A fellowship approach to calculating a safe paediatric drug dose: weigh the child in kilograms on a calibrated scale, measure length or height for body-surface-area drugs, take the mg per kg or Mosteller body-surface-area dose from a current paediatric formulary, calculate the dose, cap it at the maximum adult single and daily dose, round sensibly, write a leading zero, and have a second clinician check it independently. For therapeutic drug monitoring drugs such as vancomycin and gentamicin, sample at the correct time and adjust to the AUC or trough target. Never estimate a weight unless it is an emergency, and never let a tenfold decimal error reach the child.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Weight-based dosing is the practice of sizing a child's medicine to the body, because an adult dose given to a small child is a poison and an infant dose given to an adolescent is a failure. The child is weighed in kilograms on a calibrated scale, the dose per kilogram is taken from a current paediatric formulary, and the two are multiplied; the result is then capped at the maximum adult dose so a large adolescent never receives more than an adult would. Body-surface-area dosing extends the same idea to drugs whose clearance tracks metabolic mass rather than weight alone, and it is calculated from the Mosteller formula at the bedside. The discipline lives in the details: the weight must be right, the units must be kilograms, the decimal point must be in the right place, and a second person must check the answer. [2] [12]
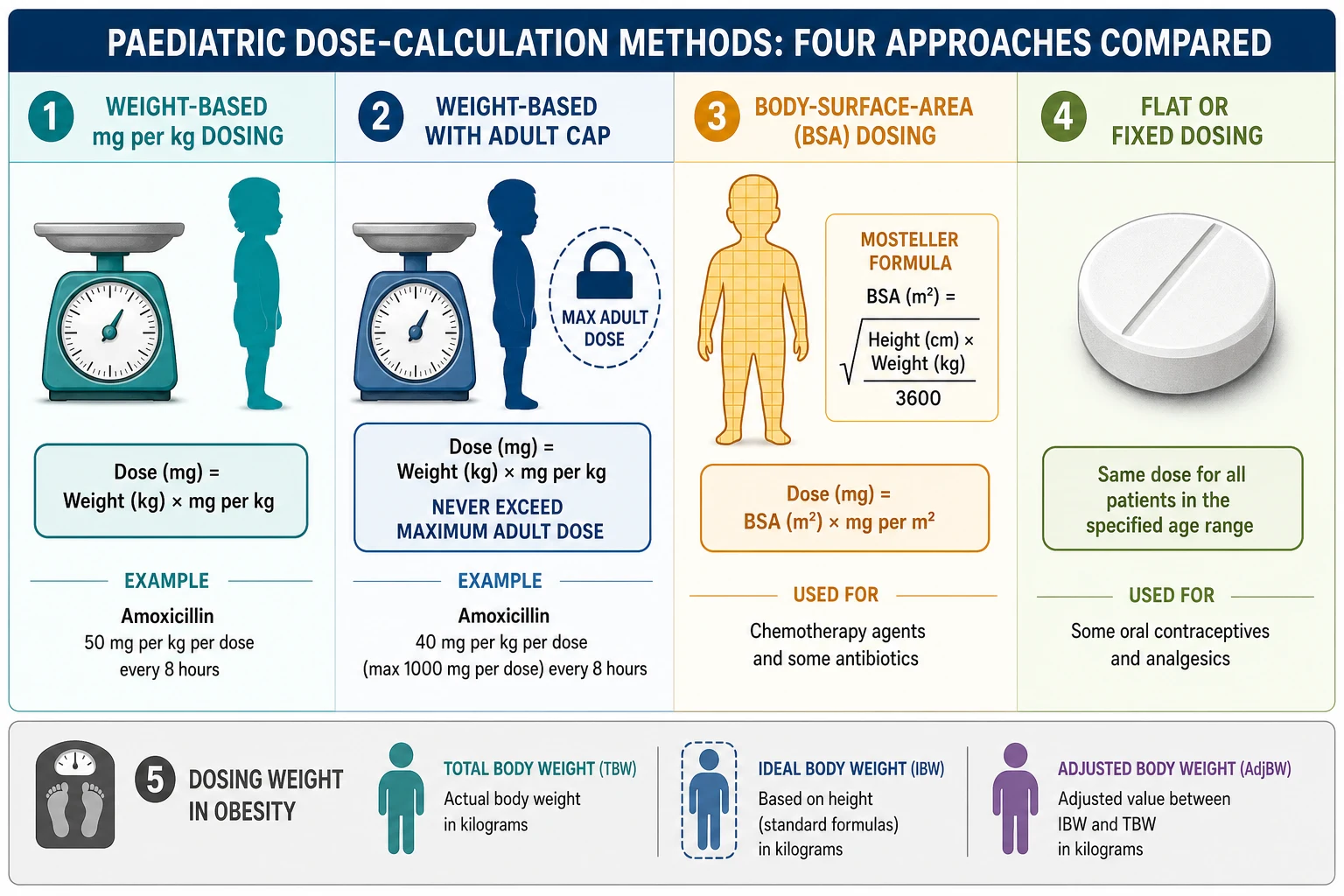
A mg per kg dose multiplies a weight in kilograms by a milligram-per-kilogram figure to give the dose for one administration, and the result is never allowed to exceed the adult maximum single dose. A body-surface-area dose multiplies a body-surface area in square metres by a milligram-per-square-metre figure, and is reserved for drugs whose distribution and clearance track metabolic body size, such as cytotoxic chemotherapy, some antivirals and some antibiotics. A flat or fixed dose gives the same amount to every patient regardless of size and is used for a small number of medicines where the therapeutic window is wide and the pharmacokinetics are forgiving. The paediatric prescriber chooses the right scalar deliberately, because using the wrong scalar for a narrow-therapeutic-index drug is a leading cause of harm. [1] [10]
The unifying principle is safety by design: a calculation that is easy to get wrong is made safer by a measured weight, a standard formula, a cap, a rounding rule, and an independent check. Children are not small adults because their body composition, their protein binding, their liver enzyme maturation and their renal clearance change with age, so a single adult dose divided by some fraction of body weight is never a safe rule. The exam answer is the workflow, not the arithmetic of one drug: weigh, measure, look up, calculate, cap, round, write, check. [2] [5]
Classification
The single most useful classification is by the scalar that sizes the dose to the child, because the scalar decides the formula, the cap, and the pitfall. Look at the drug, look at the child, and the dosing method follows: most drugs are milligram per kilogram, the cytotoxics and some antimicrobials are milligram per square metre, a few are flat, and the obese child needs a deliberate choice of weight scalar for a narrow-therapeutic-index drug. [1] [6]
Weight-based (mg/kg)
Most paediatric drugs
- Dose = weight (kg) × mg per kg, for one administration
- Always cap at the maximum adult single dose and daily dose
- Example: paracetamol 15 mg per kg per dose, max 60 mg per kg per day, adult max 1 g per dose and 4 g per day
- Pitfall: a large adolescent exceeds the adult cap if you stop at the multiplication
Body-surface-area (mg/m²)
Chemotherapy, some antivirals, some antibiotics
- Dose = BSA (m²) × mg per m², calculated by the Mosteller formula
- BSA = √(height cm × weight kg / 3600)
- Example: chemotherapy regimens, valganciclovir, some antifungals
- Pitfall: BSA dosing can increase toxicity over weight-based dosing for some drugs, so the scalar is deliberate
Flat / fixed
Wide therapeutic window
- Same dose for every patient regardless of weight or surface area
- Used for a small number of oral medicines with forgiving pharmacokinetics
- Example: some oral contraceptives and some combination analgesic tablets
- Pitfall: still respect an age or weight minimum before using an adult formulation
Weight scalar in obesity
Narrow therapeutic index
- Total body weight for some drugs, ideal body weight for others, adjusted body weight as a middle path
- The choice depends on whether the drug distributes into fat and on its therapeutic index
- A wrong scalar causes toxicity (total weight) or failure (ideal weight)
- Pitfall: never default to total body weight for every drug in the obese child
Classification by age band frames the developmental reason the scalar matters. A preterm neonate has a higher proportion of total body water and immature liver and renal clearance, so the milligram-per-kilogram figure is lower and the interval longer for many drugs. An infant clears some drugs faster per kilogram than an adult because of a high liver mass-to-body ratio, so the milligram-per-kilogram figure may be higher and the interval shorter. A school-age child approaches adult clearance per kilogram, and an adolescent is dosed as an adult once the weight-based dose reaches the adult cap. The scalar is constant; the age band changes the number you look up. [5] [9]
Epidemiology & Risk Factors
Paediatric dosing errors are common because the calculation is a multistep process performed under time pressure by people who are not always the prescriber, and because the child's small body turns a small arithmetical mistake into a large dose per kilogram. Weight errors, decimal errors, unit errors and cap errors cluster at the points where a number passes from one person or one format to another, which is why an independent double check and a single written weight in kilograms are the two most evidence-supported defences. The child who is harmed is usually the one whose weight was estimated, written in pounds, or never capped at the adult dose. [2] [3]
Child factors
- Small body mass magnifies any dose error into a large dose per kilogram
- An unknown or estimated weight in an emergency invites a tenfold error
- Obesity changes the right weight scalar for narrow-therapeutic-index drugs
- Neonatal and age-band differences in clearance change the look-up dose
Process factors
- Weight recorded in pounds and mistaken for kilograms multiplies the dose by 2.2
- A missing or misplaced decimal point causes a tenfold overdose or underdose
- No adult-dose cap lets a large adolescent receive more than an adult
- A therapeutic drug monitoring level drawn at the wrong time misdirects the dose
System factors
- Rural or remote settings with fewer layers of double check
- Out-of-hours prescribing with limited pharmacist review
- Complex chronic and technology-dependent children on many narrow-therapeutic-index drugs
- Care transitions where a weight is not re-measured or re-written
The tenfold error is the signature paediatric dosing failure because a misplaced decimal is invisible to the eye and lethal in the body, and because the small child tolerates neither ten times nor a tenth of a needed dose. The risk is magnified whenever a weight is written without a unit, whenever a leading zero is omitted or a trailing zero is added, and whenever a calculation is checked only by the person who made it. Obesity adds a second layer of risk, because the prescriber who defaults to total body weight for every drug gives water-soluble narrow-therapeutic-index drugs at toxic doses and lipid-soluble drugs at subtherapeutic doses. [3] [4]
Pathophysiology
The reason children are dosed by weight or by body-surface area, and not by a fraction of an adult dose, is that drug clearance tracks metabolic body size and not body weight alone. Body-surface area approximates metabolic mass across species and across age bands because it scales with basal metabolic rate, cardiac output and organ blood flow, which is why cytotoxic chemotherapy and several antimicrobials are standardised to the square metre rather than the kilogram. The Mosteller formula estimates body-surface area from the two measurements you already have at the bedside, height and weight, and it has been validated across the paediatric age range as an accurate and reproducible bedside tool. [1] [11]
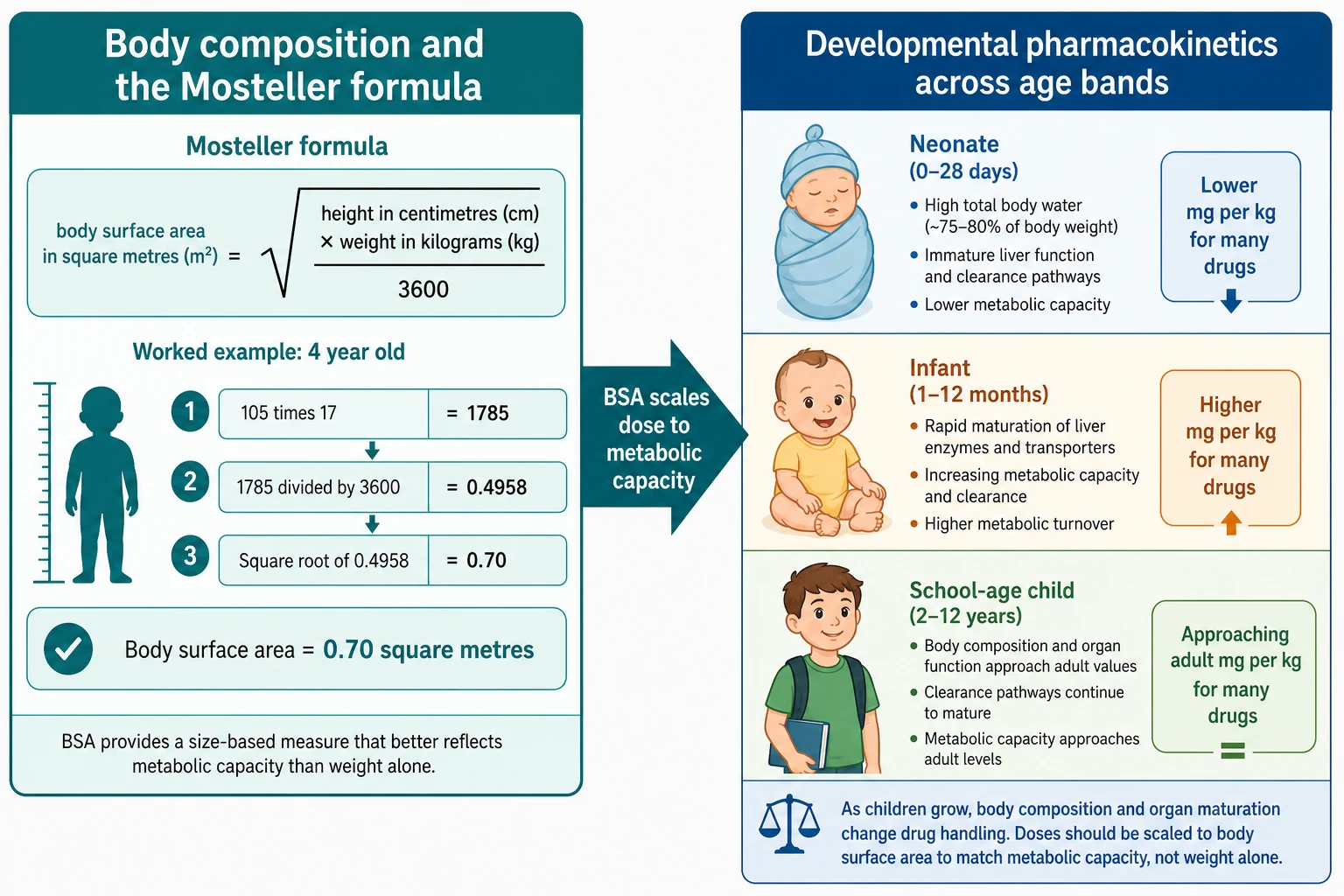
Developmental pharmacokinetics explains why the look-up number changes with age even when the scalar is the same. A preterm neonate has a larger volume of distribution for water-soluble drugs (a higher percentage of total body water), lower albumin and alpha-1-acid glycoprotein binding, immature hepatic glucuronidation and cytochrome activity, and a low glomerular filtration rate, so the milligram-per-kilogram figure is lower and the interval longer for many drugs. Over the first two years of life, liver clearance matures faster than body size, so the infant may need a higher milligram-per-kilogram figure or a shorter interval than the adult for some drugs. The prescriber does not derive these numbers; the formulary derives them, and the calculation discipline is to look them up and apply them faithfully. [5] [9]
The adult-dose cap follows from the same logic. As the child grows, the weight-based dose rises until, for an adolescent, the calculated dose would exceed what an adult receives; at that point the cap binds, and the dose stops at the adult maximum single dose and the adult maximum daily dose. The cap is not a courtesy, it is a safety boundary that prevents a large adolescent from receiving a supratherapeutic dose simply because the multiplication continued past the adult ceiling. For body-surface-area drugs, the same logic does not apply in the same way, which is why some body-surface-area regimens produce more toxicity than weight-based regimens and the scalar must be the one the formulary specifies. [4] [10]
Clinical Presentation
A dosing problem usually presents in one of three ways, and the candidate who names all three looks systematic. The first is the child who receives a tenfold overdose and presents with the toxicity of that drug, whether that is opioid respiratory depression, beta-blocker bradycardia or cytopenia after chemotherapy. The second is the child who receives a tenth of the needed dose and fails to respond, the fever that does not settle, the seizure that recurs, the level that never reaches target. The third is the near miss caught at the bedside before the drug is given, when a nurse or a parent reads the calculation and the decimal point is wrong. [3] [12]
The recognisable at-risk situations are the ones the exam rewards. An emergency with an unknown weight, a rural transfer with a hand-written drug chart, an obese child on a narrow-therapeutic-index infusion, a neonate on a once-daily aminoglycoside, and a complex chronic child on multiple anticonvulsants are all situations where a dosing error is more likely and an independent check is more valuable. The clinical sign of the error is the drug effect, read against the dose the child actually received, and the discipline is to question the dose whenever the clinical picture and the expected response diverge. [2] [7]
Differential Diagnosis
When a child has an unexpected drug effect, build the differential of the dose in a fixed order: is the dose ten times wrong, is the weight wrong, is the unit wrong, is the cap missing, is the formulation wrong, is the timing wrong. The first three are arithmetic; the last three are pharmaceutical. Asking them in this order finds the cause faster than reaching for a new diagnosis, because the common reason a child looks overdosed is that the child was overdosed. [2] [3]
Arithmetic causes
- Tenfold error from a missing or misplaced decimal point
- Weight written in pounds and read as kilograms (factor of 2.2)
- No adult-dose cap on a large adolescent
- Calculation checked only by the person who made it
Pharmaceutical causes
- Wrong strength or formulation (oral liquid concentrations differ between brands)
- Wrong frequency or interval from a look-up error
- A therapeutic drug monitoring level drawn at the wrong time misdirecting the dose
- A weight estimated and never replaced by a measured value
Patient causes
- Wrong weight scalar in obesity for a narrow-therapeutic-index drug
- Renal or hepatic impairment that lowers clearance and raises the level
- A drug interaction that inhibits or induces clearance
- Age-band clearance differences not reflected in the chosen dose
The discriminator that separates an arithmetic cause from a pharmaceutical one is the calculation itself. Re-weigh the child, re-do the arithmetic from the formulary dose, and compare the answer with what was prescribed: a tenfold discrepancy is a decimal error, a 2.2-fold discrepancy is a pound-versus-kilogram error, and a dose above the adult maximum is a missing cap. If the arithmetic is correct, the cause is pharmaceutical or patient-related, and the level or the formulation is the next thing to check. [2] [6]
Clinical & Bedside Assessment
The bedside assessment for dosing is the measurement of the weight and the height, performed deliberately and recorded once in kilograms and in centimetres. Weigh the child on a calibrated scale without shoes and without heavy clothing, and for an infant use a tray scale; if the child cannot stand, measure length lying down and mark the chart as a length rather than a height. The single written weight in kilograms is the foundation of every dose that follows, and an estimated weight is a placeholder to be replaced the moment a scale is available. [2] [11]
The focused history that frames the dose is brief and operational: the child's age (for the age band and the look-up dose), any renal or hepatic disease (for clearance), the other medicines (for interactions), and the intended route and formulation (for what can actually be given). The synthesis you speak at the bedside is a single sentence: the weight, the drug, the formulary dose, the calculated dose, the cap, and the plan to check it. Speaking the calculation out loud, as a handover, is itself a check because the second listener hears an error the writer missed. [2] [7]
Investigations
The investigations that support dosing are few and targeted, and they matter most for the narrow-therapeutic-index drugs whose level guides the next dose. For vancomycin, the consensus target is an area-under-the-curve over twenty-four hours of 400 to 600 mg·h/L, measured by a Bayesian or a trough-based approach, with the trough drawn just before a dose once steady state is reached. For gentamicin, extended-interval dosing is monitored against a target area-under-the-curve and a low trough, while traditional dosing is monitored against a peak and a trough drawn at defined times after the dose. The discipline is to record the dose time on the tube, so the laboratory can interpret the number. [7] [8]
Other investigations are dictated by the drug and the child. Renal function (urea, creatinine, estimated glomerular filtration rate) guides the dose of renally cleared drugs; liver function guides hepatically cleared drugs; a full blood count guides cytotoxic dosing; and a weight and a height guide every dose. The point for the exam is that the dose is not a single act but a cycle: dose, measure the level or the effect, adjust, and dose again, with the calculation re-checked at each step. [7] [9]
Management — Resuscitation
The resuscitation phase applies when a dosing error has reached the child and produced a toxic effect, and the first actions are the standard airway, breathing, circulation structure plus the specific antidote or supportive therapy for the drug involved. Stop the offending drug immediately, protect the airway, support breathing and circulation, check a bedside glucose, and treat the toxidrome with the targeted antidote the strip and the picture demand. The dosing-specific action is the dose audit: re-weigh, re-calculate, identify whether the error was a decimal, a unit, a missing cap or a wrong weight scalar, and correct the chart so the error cannot repeat with the next dose. [3] [12]
The resuscitation principle for a tenfold overdose is that the drug must be measured in the body, not inferred from the chart, because the chart may be where the error lives. Draw a drug level where one exists, treat the physiology you find, and escalate to senior help, intensive care and retrieval early when the toxic effect is haemodynamic or neurological. Once the child is safe, the error is reported through the local incident system so the calculation weakness is fixed, not just survived. [3] [12]
Management — Definitive & Stepwise
The definitive management of paediatric dosing is the calculation workflow itself, applied every time and checked every time. The eight steps run from a measured weight to an independent check, and the discipline is to perform them in order, because skipping a step is how the tenfold error reaches the child. [2] [3]
Measure the weight
Weigh the child in kilograms on a calibrated scale; never estimate unless it is an emergency, and replace an estimate with a measured weight the moment a scale is available.
Measure length or height
For body-surface-area drugs, measure length in an infant or height in an older child in centimetres, and calculate body-surface area by the Mosteller formula.
Look up the dose
Take the mg per kg or mg per m² dose, the frequency and the maximum from a current paediatric formulary such as the BNFc, the AMH Children's Dosing Companion or the Royal Children's Hospital Melbourne guidelines.
Calculate and cap
Multiply the weight (or body-surface area) by the formulary figure, then cap the result at the maximum adult single dose and the maximum adult daily dose.
Round and write
Round to a dose that can be measured with the available formulation, write a leading zero (0.5 mg, never .5 mg), and never add a trailing zero (5 mg, never 5.0 mg).
Independent double check
Have a second clinician independently recalculate the dose, the cap and the units before the drug is given; this is the single strongest defence against a tenfold error.
Monitor and adjust
For therapeutic drug monitoring drugs, draw the level at the correct time relative to the dose and adjust to the AUC or trough target, re-checking the calculation at each adjustment.
Confirm formulation and route
Confirm the route, frequency and formulation are age-appropriate, and that the concentration of an oral liquid is the one the calculation assumed.
The ongoing care after the first calculation is the loop, not a single act. For a therapeutic drug monitoring drug, the level feeds back into the next dose; for a long-term medicine, the weight is re-measured at every visit and the dose is re-calculated as the child grows; and for a child on many drugs, each new medicine is checked against the cap, the interaction and the cumulative daily dose. The discharge handover is the last step in the loop, because the parent who takes the medicine home must receive a dose written clearly, in the right unit, with a device that measures it. [9] [12]
Specific Subtypes & Scenarios
Several scenarios change the scalar, the number or the workflow, and the exam rewards the candidate who handles each one explicitly rather than applying a single rule. The obese child, the neonate, the burned child, the child on chemotherapy and the emergency with an unknown weight each demand a deliberate choice, because the default rule is the one most likely to fail in exactly these situations. [4] [11]
The chemotherapy scenario is the purest body-surface-area problem, because cytotoxic doses are standardised to the square metre and a wrong body-surface area translates directly into a wrong cytotoxic dose. Calculate the body-surface area from the Mosteller formula, take the milligram-per-square-metre figure from the protocol, and have the calculation checked by the oncology pharmacist before the drug is compounded. The valganciclovir example shows why the scalar matters beyond chemotherapy: body-surface-area dosing of valganciclovir produced more toxicity than weight-based dosing in paediatric transplant recipients, which is the empirical reason the scalar is chosen deliberately and not by habit. [1] [10]
Complications & Pitfalls
The preventable complications of paediatric dosing are the harms of the error itself, and they are prevented by the workflow rather than by vigilance alone. The classic preventable errors are the tenfold decimal error, the pound-versus-kilogram unit error, the missing adult-dose cap, the wrong weight scalar in obesity, and the therapeutic drug monitoring level drawn at the wrong time. Each is corrected by a specific defence: a leading zero, a single written unit, an explicit cap check, a deliberate scalar choice, and a dose time written on the tube. [3] [4]
Arithmetic pitfalls
- Tenfold error from a missing leading zero or an added trailing zero
- Weight in pounds read as kilograms (factor of 2.2)
- No adult-dose cap on a large adolescent
- Calculation checked only by the person who made it
Pharmaceutical pitfalls
- Different oral liquid concentrations between brands
- A level drawn at the wrong time misdirecting the dose
- A weight estimated and never replaced by a measured value
- A formulation too concentrated or too dilute to measure the rounded dose
Harm from the error
- Toxicity of the overdose: respiratory depression, bradycardia, cytopenia
- Failure of the underdose: persistent fever, recurrent seizure, missed level
- Loss of trust after a near miss reaches the family
- Incident-report burden and clinician second-victim harm
The harm that follows a correct calculation comes from the dose-rounding step and the formulation choice. Rounding up to a measurable dose can push a narrow-therapeutic-index drug toward toxicity, and a formulation that is too concentrated for a small volume cannot be measured accurately by a parent at home. The defences are to round to a dose that the available device can measure, to provide an oral dosing syringe rather than a spoon, and to teach the family the dose in millilitres of the specific concentration dispensed. The discharge conversation is the last calculation, because the parent who misunderstands the unit gives the wrong dose at home. [12]
Prognosis & Disposition
Most paediatric dosing errors are caught before they reach the child, because the independent double check and the pharmacist review are designed to find them; the errors that reach the child are the ones that bypassed both, and their outcome depends on the drug, the magnitude of the error and the speed of correction. A tenfold overdose of a cardiovascular or central nervous system drug can be rapidly fatal in a small child, while a tenfold underdose usually declares itself as a failure to respond. The disposition follows the drug effect: intensive care for haemodynamic or neurological toxicity, observation for the half-life of the drug, and a return to the ward once the level or the physiology is safe. [3] [7]
The prognosis of the calculation system, as distinct from the child, is improved by the defences that make the next error less likely: a single written weight in kilograms, a standard formula, an explicit cap, a leading-zero rule, an independent check, and a dose time on every level tube. The discharge disposition is a written dose in the right unit with the right device, taught to the family and checked back by teach-back, because the home is where the last calculation is performed. The child who leaves hospital with a clearly written dose and a dosing syringe is the child least likely to return with an error. [2] [12]
Special Populations
The obese child is the population in which the weight scalar is most often wrong, because the prescriber who defaults to total body weight gives water-soluble narrow-therapeutic-index drugs at toxic doses. The deliberate choice is between total body weight for drugs that distribute into fat, ideal body weight for water-soluble narrow-therapeutic-index drugs, and adjusted body weight as a middle path, and the choice is guided by the drug's volume of distribution, its therapeutic index and the available evidence. The information for many drugs is limited, which is itself the reason to choose the scalar deliberately and to monitor the level where one exists. [4] [5] [6]
Total body weight
- Used for drugs that distribute into fat
- Risks toxicity for water-soluble narrow-therapeutic-index drugs
- Suitable for most drugs with a wide therapeutic window
- The default that must be questioned for every narrow-therapeutic-index drug
Ideal body weight
- Used for water-soluble narrow-therapeutic-index drugs
- Risks underdosing for drugs that distribute into fat
- Requires a height-based ideal-weight estimate
- Common for some anaesthetic and critical-care drugs
Adjusted body weight
- A middle path between total and ideal
- Often calculated as ideal plus 0.4 of the excess
- Used for drugs with partial distribution into fat
- A deliberate compromise for a few narrow-therapeutic-index drugs
The neonate, the child with renal or hepatic impairment, and the complex chronic child on multiple medicines are the other populations where the standard calculation must be adjusted. The neonate needs age-band doses and intervals from a neonatal formulary; the child with impaired clearance needs the dose reduced by the level of impairment and guided by the level; and the complex chronic child needs every new medicine checked against the cap, the interaction and the cumulative daily dose. The principle is constant: the scalar is the same, the number changes with the child, and the check is never optional. [7] [9]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric dose calculation is a mix of validated formulae, consensus guidelines for therapeutic drug monitoring, and observational studies of error, and the candidate who cites the right source for the right claim looks authoritative. The Mosteller formula has been validated across the paediatric age range as an accurate bedside estimate of body-surface area. The vancomycin consensus guideline moved the target from a trough range to an area-under-the-curve of 400 to 600 mg·h/L for serious methicillin-resistant Staphylococcus aureus infection. The observational evidence on weight errors, tenfold errors and obesity-related errors frames the workflow defences. [1] [8]
[7] [12]The controversies are narrow but real. Body-surface-area dosing is not always safer than weight-based dosing, as the valganciclovir example shows, and the choice of scalar for some drugs remains an evidence gap. The weight-based versus body-surface-area fluid prediction in burns differs between formulae, which is why the local burns protocol is followed and the result is checked against urine output. The unifying lesson is that the calculation is grounded in a current source, applied to the measured child, and checked by a second person, and that no formula replaces the discipline of looking up the dose. [10] [11]
Exam Pearls
The Mosteller formula is the single most testable fact: body-surface area in square metres equals the square root of height in centimetres multiplied by weight in kilograms divided by 3600, and a worked example with clean numbers is worth rehearsing. The adult-dose cap is the second most testable principle: calculate by weight, then cap at the maximum adult single dose and daily dose, because the multiplication must not run past the adult ceiling. The leading-zero and no-trailing-zero rules are the third, and they are the arithmetic defence against the tenfold error that defines unsafe paediatric prescribing. [1] [3]
The one-line answer for the viva is the workflow, not a drug: weigh the child in kilograms, measure length or height for body-surface-area drugs, look up the dose in a current formulary, calculate and cap at the adult maximum, round and write a leading zero, check independently, and for therapeutic drug monitoring drugs sample at the correct time and adjust to target. The candidate who recites that sequence, and who can work a Mosteller calculation on a napkin, has the topic. [2] [7]
References
- [1]El Edelbi, R; Lindemalm, S; Eksborg, S Estimation of body surface area in various childhood ages--validation of the Mosteller formula Acta Paediatrica, 2012.PMID 22211780
- [2]Hirata, K M; Kang, A H; Ramirez, G V Pediatric Weight Errors and Resultant Medication Dosing Errors in the Emergency Department Pediatric Emergency Care, 2019.PMID 28976456
- [3]Lesar, T S Tenfold medication dose prescribing errors Annals of Pharmacotherapy, 2002.PMID 12452740
- [4]Procaccini, D; Kim, J M; Lobner, K Medication Errors in Overweight and Obese Pediatric Patients: A Narrative Review Joint Commission Journal on Quality and Patient Safety, 2022.PMID 35045950
- [5]Kendrick, J G; Carr, R R; Ensom, M H Pediatric Obesity: Pharmacokinetics and Implications for Drug Dosing Clinical Therapeutics, 2015.PMID 26361823
- [6]Kyler, K E; Wagner, J; Hosey-Cojocari, C Drug Dose Selection in Pediatric Obesity: Available Information for the Most Commonly Prescribed Drugs to Children Paediatric Drugs, 2019.PMID 31432433
- [7]McNeil, J C; Kaplan, S L Vancomycin Therapeutic Drug Monitoring in Children: New Recommendations, Similar Challenges Journal of Pediatric Pharmacology and Therapeutics, 2020.PMID 32839650
- [8]Rybak, M J; Le, J; Lodise, T P Therapeutic Monitoring of Vancomycin for Serious Methicillin-resistant Staphylococcus aureus Infections: A Revised Consensus Guideline and Review by the American Society of Health-system Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists Clinical Infectious Diseases, 2020.PMID 32658968
- [9]Hodiamont, C J; van den Broek, A K; de Vroom, S L Clinical Pharmacokinetics of Gentamicin in Various Patient Populations and Consequences for Optimal Dosing for Gram-Negative Infections: An Updated Review Clinical Pharmacokinetics, 2022.PMID 35754071
- [10]Demirhan, S; Munoz, F M; Valencia Deray, K G Body surface area compared to body weight dosing of valganciclovir is associated with increased toxicity in pediatric solid organ transplantation recipients American Journal of Transplantation, 2023.PMID 37499799
- [11]Stevens, J V; Prieto, N S; Ridelman, E Weight-based vs body surface area-based fluid resuscitation predictions in pediatric burn patients Burns, 2023.PMID 35351355
- [12]Carroll, A R; Johnson, J A; Stassun, J C Health Literacy-Informed Communication to Reduce Discharge Medication Errors in Hospitalized Children: A Randomized Clinical Trial JAMA Network Open, 2024.PMID 38227315