Paeds · endocrinology-diabetes-and-growth
Acquired hypothyroidism and Hashimoto thyroiditis
Also known as Hashimoto thyroiditis · Chronic lymphocytic thyroiditis · Autoimmune thyroiditis · Acquired hypothyroidism · Juvenile hypothyroidism
Acquired hypothyroidism is thyroid-hormone deficiency that develops after a period of normal thyroid function. In iodine-sufficient regions Hashimoto (chronic lymphocytic) thyroiditis is by far the commonest cause in children and adolescents: an autoimmune, antibody-mediated destruction of thyroid follicular cells that produces a goitre, a rising TSH and a falling free T4. Presentation is often subtle — growth slowdown, fatigue, constipation, weight gain and school decline — so the diagnosis rests on venous TSH with free T4 and anti-TPO antibodies. Treatment is levothyroxine, weight-based and titrated to a normal TSH; outcome is excellent once replacement begins, with catch-up growth and full cognitive preservation. The skill is recognising the insidious picture, confirming biochemically, screening the associated autoimmune syndromes (Down, Turner, type 1 diabetes, coeliac), and counselling the family on a long but reversible condition.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A ten-year-old girl is brought in because her teacher says she is tired and "not herself," her trousers have tightened, and the family notices she feels the cold. On examination there is a firm, bosselated, symmetrically enlarged thyroid. This is the textbook face of acquired hypothyroidism from Hashimoto thyroiditis — and the reason every general paediatric trainee needs to recognise, confirm and treat it confidently. [3][4]
Acquired hypothyroidism means inadequate circulating thyroid hormone arising after the newborn period, once the gland has previously functioned normally. It is a clinical–biochemical state, not a single disease: the thyroid can fail because autoimmune lymphocytes destroy it, because iodine is too scarce or too plentiful, because the gland has been removed or irradiated, or because a drug suppresses hormone synthesis. [1][6]
Hashimoto thyroiditis (chronic lymphocytic thyroiditis) is the autoimmune form and the one you will meet most often. Lymphocytes and antibodies infiltrate and gradually destroy thyroid follicular cells, so hormone output falls and the pituitary raises TSH in compensation — producing the goitre, rising TSH and falling free T4 that define the condition. First described by Hakaru Hashimoto in 1912, it is now the commonest cause of acquired hypothyroidism in iodine-sufficient children and adolescents. [8][3]
The clinical skill is threefold: catch the insidious presentation before growth and school performance erode; confirm biochemically rather than treating symptoms alone; and place the child in context — screening for type 1 diabetes, coeliac disease, Down and Turner syndrome, where Hashimoto travels in company. [9][10][12]
Classification
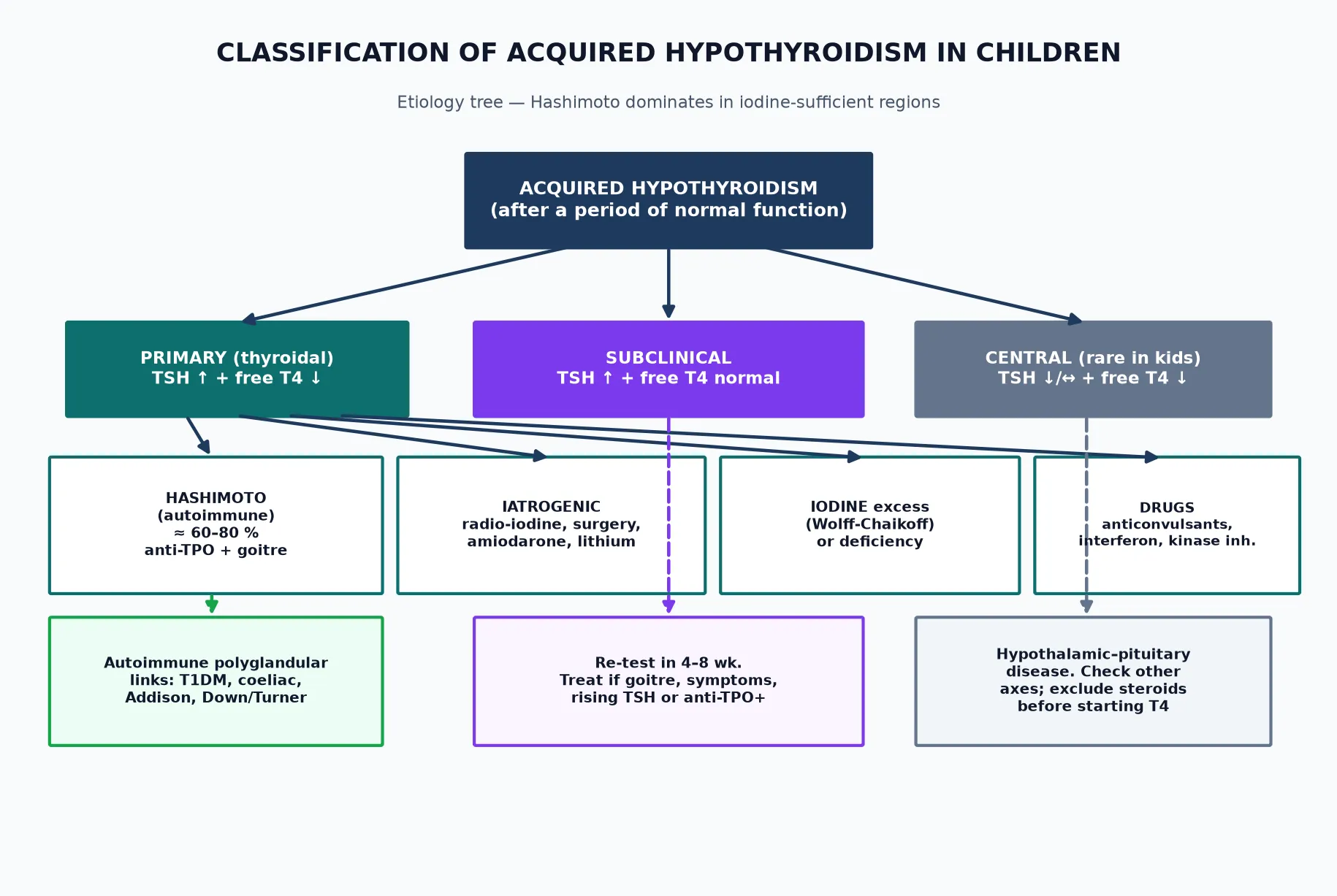
Frame acquired hypothyroidism along two axes: anatomical level (where the axis breaks) and severity (how far it has fallen). Most children you see sit in the primary, overt box — but the algorithm holds for every case. [1][6]
Overt primary hypothyroidism
- TSH raised + free T4 low
- Symptomatic — goitre, growth slowdown, fatigue
- Treat with levothyroxine immediately
- Hashimoto is the usual cause
Subclinical hypothyroidism
- TSH raised + free T4 normal
- Often asymptomatic; re-test in 4–8 weeks
- Treat if goitre, symptoms, anti-TPO+ or rising TSH
- Spontaneous normalisation is common
Central (secondary) hypothyroidism
- Low or inappropriately normal TSH + low free T4
- Hypothalamic–pituitary cause
- Exclude adrenal insufficiency before T4
- Multiple pituitary axes often involved
Autoimmune (Hashimoto)
- Anti-TPO positive in ~90%
- Goitre + lymphocytic infiltrate
- Female sex and adolescence predominate
- May remit in up to a third over years
By anatomical level. Primary disease (the thyroid itself) accounts for almost all acquired hypothyroidism in childhood and shows a raised TSH with a low free T4. Central disease — hypothalamic or pituitary in origin — is uncommon in children; its signature is a low or inappropriately normal TSH accompanying a low free T4, and it usually forms part of multiple pituitary hormone deficiency rather than standing alone. [1][4]
By aetiology. Hashimoto thyroiditis causes roughly 60 to 80% of primary acquired hypothyroidism in iodine-replete children. The remainder is iatrogenic (radioiodine or thyroid surgery for Graves disease, hemithyroidectomy for nodules), iodine-related (deficiency, or the Wolff–Chaikoff effect from iodine excess — contrast, amiodarone, antiseptics), drug-induced (lithium, amiodarone, tyrosine-kinase inhibitors, interferon, anticonvulsants), or — rarely in childhood — infiltrative (cysts, haemochromatosis, sarcoid). [1][3]
By severity. Overt hypothyroidism (raised TSH, low free T4) is symptomatic and treated without delay. Subclinical hypothyroidism (raised TSH, normal free T4) is the grey zone: many children normalise spontaneously, so the rule is to re-test before committing to lifelong tablets, then treat when the child has a goitre, symptoms, a rising TSH or positive antibodies. [5][11]
Epidemiology & Risk Factors
Autoimmune thyroiditis is common in young people. Pooled estimates put the prevalence of elevated TSH or thyroid autoantibodies at around 1 to 2% of children and adolescents in iodine-sufficient populations, with the rate climbing steeply after puberty and in those carrying an associated autoimmune or chromosomal condition. [1][3]
Acquired hypothyroidism and Hashimoto thyroiditis — by the numbers
Sex and age. The female-to-male ratio is roughly 2:1 before puberty but widens to 4:1 or even 8:1 afterwards, mirroring the oestrogen-driven immune skew of adolescence. Peak onset falls in early-to-mid puberty, though the disease can appear at any age after the newborn period. [3][8]
Risk factors that tip the balance toward Hashimoto: [3]
| Risk factor | Why it matters |
|---|---|
| Family history of autoimmune thyroid disease | Strong heritable component (HLA-DR3/DR5, CTLA-4, PTPN22) |
| Down syndrome (trisomy 21) | Lifetime risk of hypothyroidism 15–30%; screen annually [9] |
| Turner syndrome | Autoimmune thyroiditis in ~15–30% of girls; screen annually [10] |
| Type 1 diabetes mellitus | Anti-TPO positivity ~15–30%; thyroiditis in ~5–10%; screen yearly [12] |
| Coeliac disease, vitiligo, alopecia, Addison disease | Shared autoimmune polyglandular clustering |
| Pubertal female | Oestrogen and immune maturation unmask susceptibility |
| High or low iodine intake | Both destabilise the axis and can trigger autoimmunity |
| Radiation to neck / radioiodine / thyroid surgery | Direct follicular-cell loss |
In iodine-deficient regions endemic goitre and iodine-deficiency hypothyroidism still rival autoimmune disease as the leading cause, and salt-iodisation programmes are the cornerstone of prevention. In iodine-sufficient regions — including most of ANZ, the UK, North America and Europe — Hashimoto dominates and iodine-related disease is uncommon but worth asking about after iodinated contrast or amiodarone. [1][6]
Pathophysiology
The hypothalamic–pituitary–thyroid axis is a classic negative-feedback loop. The hypothalamus releases thyrotropin-releasing hormone (TRH); TRH drives the pituitary thyrotrophs to secrete thyroid-stimulating hormone (TSH); TSH binds the TSH receptor on thyroid follicular cells and stimulates iodide uptake, organification onto thyroglobulin, coupling into T4 and T3, and release into the blood. Circulating T4 (peripherally deiodinated to the active T3) feeds back on both TRH and TSH to close the loop. When the thyroid fails, TSH climbs; when the pituitary or hypothalamus fails, TSH does not — that single fact is what lets a venous TSH and free T4 localise the lesion. [6][4]
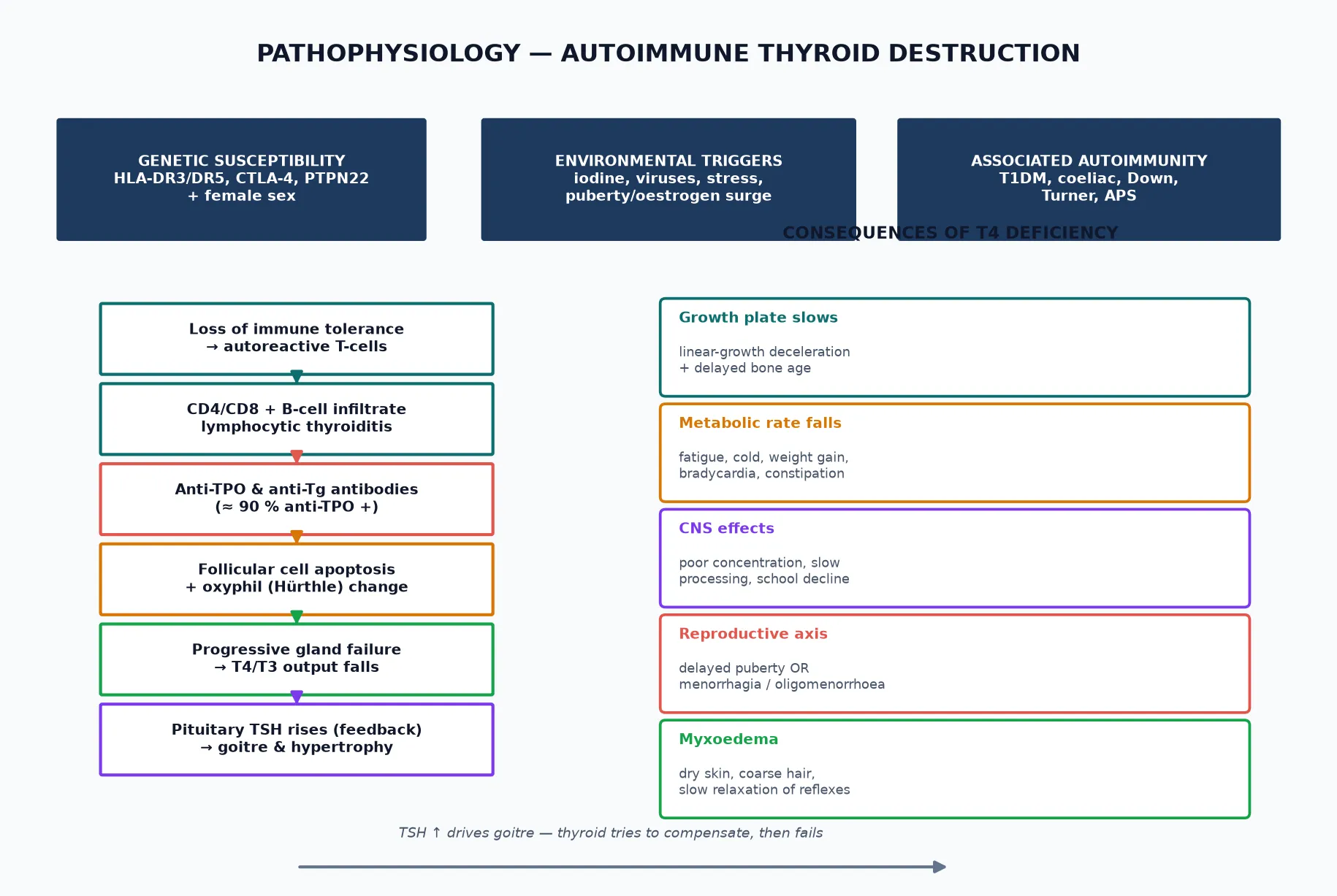
Hashimoto as an organ-specific autoimmune disease. In a susceptible child, immune tolerance to thyroid antigens breaks down. CD4+ T-helper cells activate cytotoxic CD8+ T-cells and B-cells; B-cells mature into plasma cells producing anti-thyroid peroxidase (anti-TPO) and anti-thyroglobulin (anti-Tg) antibodies. Anti-TPO is the workhorse marker — positive in about 90% of paediatric Hashimoto — and, although it is chiefly a diagnostic fingerprint, it also inhibits the TPO enzyme that organifies iodide, compounding the hormone deficit. Lymphocytes stream into the interstitium, forming germinal centres; follicular cells die by apoptosis and are replaced by Hürthle (oxyphil) cells; fibrosis follows in long-standing disease. The gland enlarges (goitre) early, then may atrophy as destruction outpaces regeneration. [8][6]
Why the symptoms track the failing axis. Thyroid hormone sets the basal metabolic rate and governs linear growth, gut motility, cardiac function, CNS processing and the tempo of puberty. As T4 falls, the growth plate slows first (height velocity drops, bone age lags), metabolic rate drops (fatigue, cold intolerance, weight gain, bradycardia, constipation), the brain slows (poor concentration, sluggish processing, school decline), and the reproductive axis stutters — either delayed puberty or, paradoxically, premature thelarche and menorrhagia from TRH-driven prolactin and GnRH dysregulation. Myxoedema — glycosaminoglycan accumulation in skin and soft tissue — produces the dry skin, coarse hair, puffy face and delayed-relaxation reflexes of more advanced disease. [4][6]
The goitre is compensatory, not destructive. Rising TSH drives the surviving follicular cells to hypertrophy in a bid to extract every available iodide molecule — so the gland swells. Early Hashimoto often presents with a euthyroid or even transiently hyperthyroid goitre (hashitoxicosis, from preformed hormone release as follicles rupture) before settling into hypothyroidism. This explains why a firm goitre can sit alongside normal thyroid function for months, and why the trend in TSH matters more than any single value. [3][8]
Clinical Presentation
The hallmark is insidious onset. Unlike congenital hypothyroidism, which screening catches before symptoms, acquired hypothyroidism declares itself through slow erosion of energy, growth and mood over weeks to months — easily attributed to adolescence, school stress or a virus. The earlier the recognition, the less growth and schooling is lost. [3][4]
Growth and body composition change first and most reliably. Linear growth decelerates while weight creeps up, so the child crosses centiles — height falling, weight or BMI rising. Bone age lags behind chronological age. Parents describe "shooting up then stopping," and school nurses flag a child who is no longer the tallest in the class. [4][1]
Energy, temperature and gut. Fatigue, somnolence and exercise intolerance are nearly universal. Cold intolerance, dry skin, brittle hair, coarse facial features (late), bradycardia, and constipation — sometimes severe enough to mimic functional constipation — round out the metabolic slowing. A child who sleeps through weekend mornings and wears a jumper when peers do not is worth a TSH. [4][6]
Cognition, mood and school. Slowed processing speed, poor concentration, declining grades and low mood can precede the physical signs. These are reversible with treatment, which is reassuring to emphasise — but they also mean a quiet academic decline in an adolescent girl should prompt thyroid testing before it is attributed to motivation. [4][3]
Reproductive axis. Puberty may be delayed, or — in younger children with severe longstanding disease — paradoxically early (premature thelarche, even isosexual precocity, from TRH-driven FSH/LH and prolactin). Adolescent girls may present with menorrhagia, oligomenorrhoea or amenorrhoea. Galactorrhoea with a normal-range prolactin that falls with thyroxine is a classic endocrine vignette. [1][4]
The goitre. The thyroid is typically diffusely enlarged, firm and bosselated, symmetric or slightly asymmetric, non-tender and mobile on swallowing. A rapidly enlarging, hard, fixed or tender lobe, or palpable cervical lymphadenopathy, shifts the differential toward cyst, haemorrhage or — rarely in childhood — carcinoma or lymphoma, and warrants ultrasound and fine-needle aspiration rather than a trial of thyroxine alone. [3][8]
Severe decompensation — myxoedema coma. Rare in children but life-threatening: hypothermia, bradycardia, hypoventilation, hyponatraemia, ileus and progressive drowsiness. Triggered by intercurrent illness, sedatives or cold exposure in a long-undiagnosed child. Treat in intensive care with intravenous levothyroxine and hydrocortisone (give steroids first — autoimmune hypothyroidism can coexist with adrenal insufficiency), warm gradually, and correct hyponatraemia cautiously. [4][6]
Differential Diagnosis
A firm goitre with a raised TSH is usually Hashimoto — but several mimics and companions must be actively excluded, because they change the plan. [3][4]
Simple/colloid goitre
- Diffuse smooth goitre
- TSH and free T4 normal
- Antibodies negative or low
- Observe; no thyroxine needed
Graves disease (early / hashitoxicosis)
- Goitre but hyperthyroid symptoms
- TRAb positive
- May evolve to hypothyroidism
- Distinguish by full TFTs and TRAb
Iodine-deficiency goitre
- Diffuse soft goitre
- Dietary history; endemic region
- Anti-TPO negative
- Correct iodine; TFTs normalise
Thyroid nodule / cyst / carcinoma
- Asymmetric or solitary nodule
- May have normal TFTs
- Hard, fixed or with nodes → FNA
- Ultrasound essential
Down syndrome and Turner syndrome are not mimics — they are the field. A child with trisomy 21 has a lifetime hypothyroidism risk of 15–30% and should be screened annually from infancy; girls with Turner syndrome carry a 15–30% rate of autoimmune thyroiditis and need yearly TSH and free T4 as standard surveillance. In type 1 diabetes, thyroid antibodies are found in 15–30% and overt thyroiditis in 5–10%, so annual screening is embedded in diabetes care. Missing the diagnosis in these children is the most preventable error in the whole topic. [9][10][12]
Non-thyroidal illness and drugs can transiently disturb the axis — severe illness (euthyroid-sick syndrome), high-dose glucocorticoids, dopamine, amiodarone, lithium, iodinated contrast and anticonvulsants. Repeat testing once the child is well (4–6 weeks) avoids labelling a transient abnormality as permanent disease. [6][4]
Functional constipation, fatigue, growth-delay variants and depression are the clinical traps. A child treated for months for "lazy bowels" or "adolescent tiredness" whose growth has quietly decelerated is the classic late presentation — a single TSH and free T4 resolves it. Always pair growth assessment with thyroid testing when the centiles are crossing down. [1][4]
Clinical & Bedside Assessment
The encounter has two layers: confirm the gland is enlarged and hypofunctioning, and place the child in their autoimmune and developmental context. [3][4]
Growth. Measure height, weight and BMI, plot on age- and sex-appropriate charts, and — critically — calculate height velocity and compare with the parents' mid-parental height. Crossing centiles downward for height with a rising BMI is the single most useful clinical signal. Bone age X-ray (left hand and wrist) lags behind chronological age in long-standing disease and is a useful adjunct when the diagnosis is delayed. [1][4]
Thyroid examination. Inspect the neck with the child's chin slightly lifted, ask them to swallow sips of water, then palpate from behind using both hands. Characterise the goitre: diffuse or nodular, smooth or bosselated, soft or firm, tender or non-tender, symmetric or asymmetric. Estimate size against the WHO grading (no goitre, palpable but not visible, visible at normal neck position, large). Palpate cervical and supraclavicular lymph nodes — their presence changes the differential toward malignancy or subacute thyroiditis. [3][8]
Systemic signs of hypothyroidism. Bradycardia (or its absence in an adolescent who should be bradycardic — a relative tachycardia), dry skin, cool peripheries, delayed relaxation of the ankle reflexes, proximal muscle weakness, and a hoarse voice in advanced disease. Pubertal staging (Tanner) and menarche history, since both delayed puberty and menorrhagia point to the thyroid. [4][6]
Autoimmune context. Screen actively for type 1 diabetes (polyuria, polydipsia, weight loss — check HbA1c/glucose if any doubt), coeliac disease (growth failure, gastrointestinal symptoms, iron deficiency), vitiligo, alopecia and a family history of autoimmune disease. In Down and Turner syndrome the thyroid assessment is part of the routine annual review, not a prompted test. [9][10][12]
Bedside pitfalls. A normal thyroid examination does not exclude Hashimoto — early or atrophic disease can be non-goitrous. Conversely, a goitre with normal thyroid function is simple or colloid goitre until antibodies and the trend prove otherwise. Never start thyroxine on symptoms alone — confirm biochemically first. [1][5]
Investigations
Investigation is tiered and confirmatory: venous TSH and free T4 first, antibodies next, imaging selectively, and ancillary tests for the associated conditions. [1][4]
Tier 1 — Confirm the axis (every suspected case). A venous TSH and free T4 define both the presence and the anatomical level of hypothyroidism. Raised TSH with low free T4 is overt primary disease; raised TSH with normal free T4 is subclinical disease (re-test); low or inappropriately normal TSH with low free T4 is central disease (check other pituitary axes). Capillary or point-of-care testing is not a substitute for venous confirmation before committing to treatment. [6][1]
Tier 2 — Establish the cause. Anti-TPO antibodies are positive in roughly 90% of Hashimoto and confirm an autoimmune basis; anti-thyroglobulin antibodies add little in isolation but support the picture when anti-TPO is borderline. TSH-receptor antibodies (TRAb) distinguish Hashimoto from Graves when the clinical picture is ambiguous (a hyperthyroid phase or a very vascular goitre). [8][3]
Tier 3 — Imaging and ancillary. Thyroid ultrasound is reserved for an asymmetric, rapidly enlarging, tender, hard or nodular gland, or when cervical lymphadenopathy is present — features that raise the spectre of cyst, haemorrhage, carcinoma or lymphoma. A homogeneous, diffusely hypoechoic, hypervascular gland with a lobulated surface is the sonographic face of Hashimoto, but routine ultrasound adds little to a typical goitre and is not needed to start treatment. Scintigraphy is rarely required in children and is reserved for ambiguous congenital-versus-acquired cases. [3][1]
Tier 4 — Associated conditions and monitoring. Screen coeliac serology (tissue transglutaminase IgA with total IgA) and, where indicated, HbA1c/glucose for type 1 diabetes, a lipid profile (hypothyroidism raises cholesterol), a full blood count and ferritin (associated iron deficiency), and — in central disease — morning cortisol, IGF-1 and other pituitary axes. In girls with Turner syndrome and any child with a strong family history, the associated screen runs in parallel with the thyroid work-up. [9][10][12]
HASHIMOTO work-up
Management — Resuscitation
Acquired hypothyroidism is rarely a resuscitation problem, but three scenarios demand immediate, structured action. [4][6]
-
Myxoedema coma — the life-threatening extreme. Recognise the tetrad of hypothermia, bradycardia, hypoventilation and altered consciousness, usually with hyponatraemia and ileus, in a long-undiagnosed child. Manage in intensive care: intravenous levothyroxine with intravenous hydrocortisone given first (autoimmune hypothyroidism can coexist with adrenal insufficiency and giving T4 alone can precipitate adrenal crisis), gentle external warming, cautious fluid and sodium correction, and treatment of the precipitant (infection, sedation, cold). Mortality remains significant; this is one of the few endocrine paediatric emergencies. [6][4]
-
Severe, symptomatic overt hypothyroidism — a child with bradycardia, pericardial effusion, significant growth failure or school decline. Start full-replacement levothyroxine promptly (do not wait for antibody or imaging results), arrange paediatric endocrinology review within days, and ensure the family understands the regimen and follow-up bloods. [2][7]
-
Incidental finding of central hypothyroidism — low free T4 with low or inappropriately normal TSH. Check morning cortisol and exclude adrenal insufficiency before starting thyroxine, because T4 accelerates cortisol clearance and can unmask Addisonian crisis in combined deficiency. Image the pituitary and involve endocrinology the same day. [4][6]
For the vast majority — a stable, alert child with a goitre and raised TSH — the "resuscitation" is simply: confirm venous labs, start levothyroxine, book follow-up, and reassure the family that this is a common, fully treatable condition. [1][3]
Management — Definitive & Stepwise
Levothyroxine sodium (L-T4) is the cornerstone of treatment for every form of hypothyroidism, primary or central. It is effective, cheap, safe in pregnancy, and, for the child who takes it reliably, fully restorative. [2][7]
Drug: levothyroxine sodium. [2]
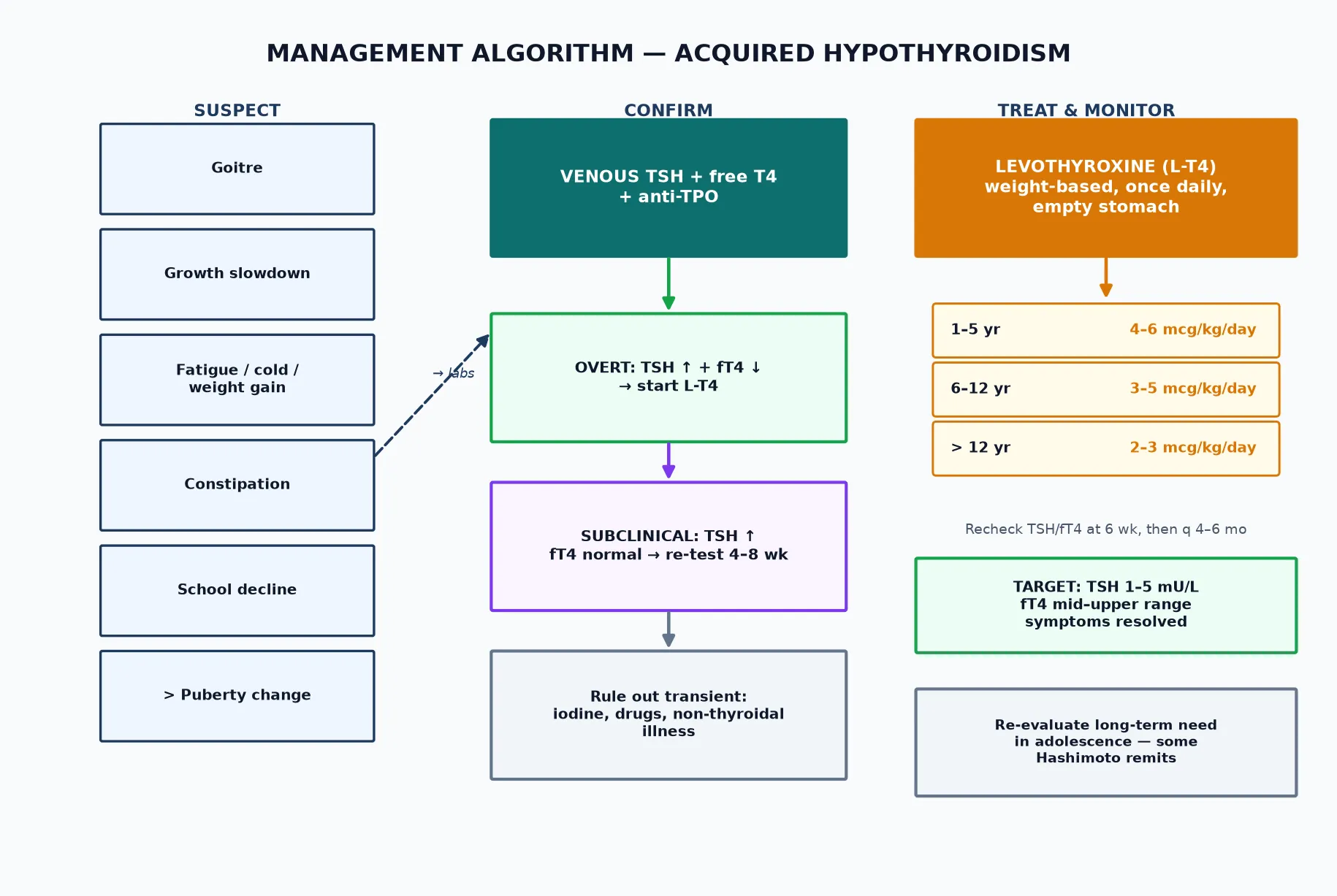
- Dose (weight-based, once daily): children 1–5 years, 4–6 mcg/kg/day; 6–12 years, 3–5 mcg/kg/day; adolescents over 12 years, 2–3 mcg/kg/day; adults and fully-grown adolescents, about 1.6 mcg/kg/day. A typical 12-year-old weighing 35 kg starts around 100 mcg/day. [2][7]
- Administration: once daily, ideally on an empty stomach 30–60 minutes before breakfast, or at bedtime three hours after the evening meal. Separate from calcium, iron, soy, proton-pump inhibitors, sucralfate, antacids and large amounts of fibre or coffee by at least four hours, all of which impair absorption. A tablet is standard; a liquid formulation is useful for infants, children with swallowing difficulty and those in whom absorption is erratic. [7][2]
- Titration and target: recheck TSH and free T4 at six weeks after any dose change, then every 4–6 months during growth and at any dose change. Aim for TSH in the normal range (roughly 1–5 mU/L), free T4 in the mid-to-upper reference range, and resolution of symptoms — the child should feel well, not merely have a normal number. [2][1]
Levothyroxine sodium (L-T4)
Adherence and the family conversation. A daily, lifelong tablet taken on an empty stomach is a real ask for a teenager. Acknowledge it, explain why timing matters (absorption varies 20–40% with food and co-medications), offer a liquid if tablets fail, link dosing to a fixed daily anchor (waking, tooth-brushing), and bring the young person — not just the parent — into the plan. Adherence is the commonest reason for a "non-responder." [2][7]
Subclinical hypothyroidism — the reasoned pause. A raised TSH with a normal free T4 is common and often transient. The evidence-based move is to re-test in 4–8 weeks before treating: up to a third of children normalise spontaneously, especially those with mildly raised TSH and negative antibodies. Treat when the child has a goitre, symptoms, a steadily rising TSH, or anti-TPO positivity — features that predict progression to overt disease. A TSH persistently above 10 mU/L with a normal free T4 is usually treated even if asymptomatic. [5][11]
Re-evaluation and the possibility of remission. Hashimoto in children is not always permanent. Studies following treated children show that a meaningful minority — up to a third in some series — achieve remission if L-T4 is weaned in late adolescence, particularly those who were biochemically mild and antibody-positive at diagnosis. Plan a supervised trial of dose reduction in stable older adolescents rather than declaring the tablet lifelong at the first visit. [1][11]
Referral. General paediatrics can confidently diagnose and initiate treatment. Refer to paediatric endocrinology for central hypothyroidism, a nodular or asymmetric gland needing imaging, associated complex autoimmune disease, refractory or unstable biochemical control, or when a supervised withdrawal trial is being planned. [3][2]
Specific Subtypes & Scenarios
-
Euthyroid/goitrous Hashimoto (autoimmune thyroiditis, normal TFTs). Positive anti-TPO with a goitre but normal TSH and free T4. Monitor TSH annually; treat only if the axis decompensates. Reassure the family that a goitre alone is not hypothyroidism. [8][3]
-
Hashitoxicosis (the transient hyperthyroid phase). Preformed hormone leaks as follicles rupture early in the autoimmune attack, producing weeks of palpitations, tremor and weight loss with a suppressed TSH — then the child tips into hypothyroidism. Distinguish from Graves by TRAb (positive in Graves, negative in hashitoxicosis) and a low radioactive-iodine uptake (though uptake is rarely tested in children). Treat symptomatically with a beta-blocker; antithyroid drugs are ineffective (no new hormone synthesis) and inappropriate. [3][4]
-
Subclinical hypothyroidism. Raised TSH, normal free T4. Re-test in 4–8 weeks; treat if goitre, symptoms, rising TSH or anti-TPO+. Up to a third normalise spontaneously. [5][11]
-
Iodine-induced (Wolff–Chaikoff). After iodinated contrast, amiodarone, or excess antiseptic iodine — particularly in an infant or a child with an underlying thyroid lesion. Usually transient; withdraw the source and re-test. [6][4]
-
Post-treatment hypothyroidism (Graves, thyroid cancer, post-surgery). Expected and managed identically with weight-based L-T4; in thyroid cancer the TSH target may be suppressed, dictated by oncology. [3][2]
-
Central (secondary) hypothyroidism. Low free T4 with low or inappropriately normal TSH from hypothalamic–pituitary disease. Always exclude adrenal insufficiency before starting T4 (give hydrocortisone first), and investigate the pituitary with imaging and the other axes. [4][6]
A typical Hashimoto course through childhood
Complications & Pitfalls
Untreated disease. Growth failure and delayed bone age, impaired school performance and mood, pubertal disturbance, constipation and, at the extreme, myxoedema coma. The good news is that all of these are preventable or reversible with timely levothyroxine — which is why prompt recognition matters so much. [1][4]
Overtreatment. Sustained TSH suppression produces hyperthyroid effects — tachycardia, anxiety, tremor, poor sleep, weight loss and, importantly, accelerated bone maturation that can compromise final adult height. Avoid driving the TSH below the reference range; a transiently low TSH during catch-up is acceptable, a chronically suppressed one is not. [2][7]
Undertreatment. Persistent fatigue, growth under-shoot and school under-performance, usually from missed doses or absorption-reducing interactions (iron, calcium, soy, PPIs taken together). Check adherence before raising the dose — a high TSH on a seemingly adequate regimen almost always means the tablet is not getting in. [2][7]
Classic pitfalls:
- Treating symptoms without venous confirmation. Fatigue, constipation and weight gain are nonspecific; always confirm TSH and free T4 first.
- Missing the associated conditions. Diagnosing Hashimoto but forgetting coeliac serology, HbA1c and (in at-risk syndromes) annual surveillance leaves diabetes, coeliac and Addison undetected. [9][12]
- Over-investigating a typical goitre. Antibodies and TFTs suffice; reserve ultrasound for the asymmetric, nodular, tender or hard gland.
- Starting T4 in central hypothyroidism without checking cortisol first — risks unmasking adrenal crisis.
- Declaring the disease "lifelong" at the first visit — a meaningful minority of children remit; build in a future re-evaluation.
- Forgetting pregnancy planning — adolescent girls need to know that L-T4 requirements rise 25–30% in early pregnancy, and that untreated maternal hypothyroidism harms the fetus. [2][7]
The thyroid nodule trap. A solitary, hard, fixed or rapidly growing nodule, or a gland with palpable cervical nodes, is not Hashimoto — it is thyroid cancer or lymphoma until proven otherwise by ultrasound and fine-needle aspiration. Cancer is rare in childhood but, when it occurs, is often more aggressive; low threshold for imaging is appropriate. [3][8]
Prognosis & Disposition
With prompt, adequate levothyroxine, the outlook is excellent. Catch-up growth resumes within months, bone age recovers, energy and cognition normalise, and final adult height and intellectual outcome are preserved. The cognitive deficits seen in untreated congenital hypothyroidism do not apply here — the brain is past its critical thyroid-dependent window — so a school-age child started on thyroxine can expect full cognitive recovery, and families should be told this explicitly. [1][3]
Outcome tracks:
- Duration and severity of untreated disease — the longer and deeper the deficit, the more growth and schooling is lost before recovery.
- Adherence — the single biggest determinant of long-term control; a missed tablet today is a missed growth percentile next year.
- Associated conditions — comorbid type 1 diabetes, coeliac disease or adrenal insufficiency shape prognosis more than the thyroid itself.
- Monitoring quality — consistent 4–6-monthly review catches drift before symptoms do. [2][4]
Disposition. Most children are managed in shared primary-secondary care with paediatric endocrinology input: general paediatrics initiates and titrates, endocrinology supports complex or central cases, and the primary care medical home holds the annual review (TSH, free T4, growth, and the associated-condition screen). Adolescents transition to adult endocrinology with a structured handover — carrying the diagnosis, the regimen, the monitoring plan and the knowledge that pregnancy will raise their dose. [3][2]
Special Populations
-
Down syndrome. Lifetime hypothyroidism risk 15–30%, often silent and frequently autoimmune. Annual TSH and free T4 from infancy; check at any new growth, behavioural or energy concern. The thyroid is part of the routine health surveillance, not an afterthought. [9]
-
Turner syndrome. Autoimmune thyroiditis in 15–30% of girls, often from mid-childhood. Annual TSH, free T4 and anti-TPO as standard surveillance alongside cardiac, renal and growth-hormone monitoring. [10]
-
Type 1 diabetes mellitus. Anti-TPO positivity in 15–30% and overt thyroiditis in 5–10%. Annual TSH and free T4 (some guidelines screen from diagnosis and then yearly) — hypothyroidism destabilises glycaemia and growth, so catching it early protects both. [12]
-
Coeliac disease and autoimmune clustering. Screen coeliac serology at diagnosis and periodically; vitiligo, alopecia areata, pernicious anaemia and Addison disease all travel with Hashimoto through shared HLA susceptibility. [8][6]
-
Pregnant and pregnancy-planning adolescents. L-T4 needs rise 25–30% in early pregnancy; untreated maternal hypothyroidism carries fetal and obstetric risk. Counsel early, pre-conception where possible, and monitor TSH each trimester. [2][7]
-
Indigenous, migrant and refugee families. Apply culturally safe, interpreter-supported care; ask about iodine intake (deficient or excess) and endemic-region exposure, and recognise that screening access may be limited, so opportunistic testing at any contact is justified. [1][6]
-
Children with disability and neurodiversity. Communication, examination and adherence all need adaptation; behavioural change may be the only sign of thyroid dysfunction. A liquid L-T4 formulation and a consistent daily anchor support adherence. [4]
Evidence, Guidelines & Regional Differences
The American Thyroid Association (ATA) treatment-of-hypothyroidism guidelines (Jonklaas et al., 2014) remain the foundational reference for levothyroxine dosing, titration and targets, and are cited across paediatric and adult practice; the ESPE and AAP endorse age-appropriate application of these principles in children. [7][3]
The Rodriguez et al. (2022) review in Trends in Endocrinology and Metabolism synthesises contemporary paediatric levothyroid dosing across infancy, childhood and adolescence, including liquid formulations and monitoring strategy. Bhattacharyya (2023) provides a current Indian perspective on acquired hypothyroidism in children, relevant to iodine-variable regions. The Chaker et al. (2022) Nature Reviews Disease Primers gives the modern pathophysiological and epidemiological synthesis of hypothyroidism across all ages. [2][1][6]
For subclinical hypothyroidism in children, the Salerno et al. (2020) European Journal of Endocrinology review and the Gallizzi et al. (2018) Italian Journal of Pediatrics discussion set out the re-test-before-treat strategy and the predictors of progression (goitre, symptoms, rising TSH, anti-TPO positivity), reflecting broad ESPE alignment. [5][11]
The Caturegli et al. (2014) review codifies the clinical and diagnostic criteria for Hashimoto thyroiditis, anchoring the anti-TPO-centred diagnostic approach. Hanley et al. (2016) in JAMA Pediatrics and Diaz (2014) in Pediatrics in Review are the high-yield general paediatric reviews of thyroid disorders in children. [8][3][4]
RACP and Royal Children's Hospital Melbourne guidance frame acquired hypothyroidism as a general-paediatrics diagnosis with endocrinology support; thyroid function testing is widely accessible through primary care and the annual review for children with Down syndrome, Turner syndrome and type 1 diabetes is embedded in standard care. Iodine sufficiency is the norm in most of Australia and New Zealand, so Hashimoto dominates. [1]
NICE guidance on thyroid disease (NG145) supports primary-care initiation of levothyroxine for overt hypothyroidism with TFT monitoring at 6 weeks then 4–6 monthly; the RCPCH Progress+ curriculum embeds thyroid disorders in the Endocrinology and Diabetes syllabus. UK-WHO growth charts anchor the growth assessment that so often first flags the disease. [5][11]
The ATA guidelines and ABP/AAP content outline drive practice; screening of at-risk groups (Down, Turner, type 1 diabetes) is standard. In Canada, the RCPSC EPAs and provincial pathways align, with primary-care initiation and endocrinology referral for complex or central cases. [7][3]
Controversies.
- Treatment of mild subclinical hypothyroidism — the re-test-before-treat consensus is firm, but the TSH threshold for asymptomatic treatment (7 versus 10 mU/L) and the weight given to anti-TPO positivity vary between centres.
- Liquid versus tablet levothyroxine — liquid aids adherence in young children and those with absorption issues but costs more and has storage considerations; tablets remain first-line for most.
- Withdrawal trials in adolescence — increasingly supported by remission data, but not yet universal practice; a supervised taper with TSH monitoring is the safe approach.
- Routine ultrasound in Hashimoto — not recommended for the typical goitre; reserved for the asymmetric, nodular or hard gland. [5][11][2]
Exam Pearls
The HASHIMOTO picture — present like a consultant
- The commonest cause of acquired hypothyroidism in iodine-sufficient children is Hashimoto thyroiditis. [1][8]
- TSH raised + free T4 low = primary; TSH low/normal + free T4 low = central — check cortisol before T4. [4]
- Anti-TPO is positive in ~90% of Hashimoto; it is the diagnostic fingerprint. [8]
- Levothyroxine is weight-based: 4–6 mcg/kg/day (1–5 yr), 3–5 mcg/kg/day (6–12 yr), 2–3 mcg/kg/day (>12). [2][7]
- Give on an empty stomach, separate from iron, calcium, soy, PPIs by 4 h. [7]
- Recheck TSH/free T4 at 6 weeks, then q 4–6 months; target TSH 1–5 mU/L. [2]
- Subclinical hypothyroidism — re-test in 4–8 weeks before treating; treat if goitre, symptoms, rising TSH or anti-TPO+. [5][11]
- Down, Turner, T1DM, coeliac — annual thyroid surveillance is mandatory. [9][10][12]
- Myxoedema coma: IV levothyroxine + IV hydrocortisone first, then warm and correct sodium slowly. [6]
- A nodular, hard, fixed or node-bearing gland is cancer until proven otherwise — ultrasound + FNA. [3]
- A minority of children with Hashimoto remit — plan a supervised withdrawal trial in stable older adolescents. [1][11]
High-yield anchors
References
- [1]Bhattacharyya SS Acquired Hypothyroidism in Children. Indian Journal of Pediatrics, 2023.PMID 37256446
- [2]Rodriguez L, Keller L, Bin S, Khalfi A, Nguyen DT, Pantalone L, Benavides VC, Sun MH, Antenor F, Leblebici N, Cancio S, Galhardo J, Yuen T, New MI, Wang Y, Lekarev O, Gong C, Kohn B Treatment of hypothyroidism in infants, children and adolescents. Trends in Endocrinology and Metabolism, 2022.PMID 35537910
- [3]Hanley P, Lord K, Bauer AJ Thyroid Disorders in Children and Adolescents: A Review. JAMA Pediatrics, 2016.PMID 27571216
- [4]Diaz A, Lipman Diaz E Hypothyroidism. Pediatrics in Review, 2014.PMID 25086165
- [5]Salerno M, Capalbo D, Gianfrancesco F, Gaspari AL, Gallizzi R, De Filippo G, Malloy MJ, Wasniewska M Management of endocrine disease: Subclinical hypothyroidism in children. European Journal of Endocrinology, 2020.PMID 32580145
- [6]Chaker L, Razvi S, Baretic M, Bischoff-Ferrari HA, Bremner AP, de Vries EM, Ee Gan E, de Groot J, Hynes A, Kharb S, Khandale S, Lanfranco F, Loh TP, Mitchell AL, Morio Y, Nygaard B, Sahebkar A, Soh SB, Sun J, Trimboli P, Vila L, Tingi E, Wiersinga WM, Peeters RP Hypothyroidism. Nature Reviews Disease Primers, 2022.PMID 35589725
- [7]Jonklaas J, Bianco AC, Bauer AJ, Burman KD, Cappola AR, Celi FS, Cooper DS, Kim BW, Peeters RP, Rosenthal MS, Sawka AM Guidelines for the treatment of hypothyroidism: prepared by the american thyroid association task force on thyroid hormone replacement. Thyroid, 2014.PMID 25266247
- [8]Caturegli P, De Remigis A, Rose NR Hashimoto thyroiditis: clinical and diagnostic criteria. Autoimmunity Reviews, 2014.PMID 24434360
- [9]Whooten R, Schmitt J, Schwartz A Endocrine manifestations of Down syndrome. Current Opinion in Endocrinology, Diabetes and Obesity, 2018.PMID 29135488
- [10]De Sanctis V, Bellanti F, Bufano G, Cavalli L, Ciccone S, Costa F, Dell'Acqua A, Di Maio S, Dolce N, Forni GL, Giuditta M, Iossa M, Lucco G, Neri S, Ricchi A, Rigolon R, Saraco P, Schettini F, Soliman AT, Stroppiano M, Valli MB, Vincenzo G, Yassin MA Autoimmune diseases in Turner syndrome: an overview. Acta Bio-Medica, 2019.PMID 31580326
- [11]Gallizzi R, Wasniewska M, Crisafulli G, De Luca F Subclinical hypothyroidism in children: is it always subclinical? Italian Journal of Pediatrics, 2018.PMID 29454373
- [12]Ridha MF, Jabur MH, Al-Samarrai AF Thyroid auto immune antibodies in children with Type-I Diabetes mellitus in relation to diabetes control. Pakistan Journal of Medical Sciences, 2019.PMID 31372126