Paeds · endocrinology-diabetes-and-growth
Congenital hypothyroidism
Also known as congenital hypothyroidism · neonatal hypothyroidism · cretinism (historical) · primary congenital hypothyroidism · central congenital hypothyroidism
A fellowship approach to congenital hypothyroidism: the newborn-screening-to-treatment pipeline that prevents intellectual disability, the dose and timing of levothyroxine that protects the developing brain (10 to 15 mcg per kg per day, started within the first two weeks), the primary-versus-central classification that explains which babies the TSH screen misses, and the long-term surveillance and permanence reassessment that carries the child into adult endocrine care.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A well baby is flagged on the newborn bloodspot screen at day four with a raised TSH; or a midwife notices prolonged jaundice, a large posterior fontanelle, and a sleepy, constipated two-week-old; or a premature twin returns a falsely reassuring early screen and presents at six weeks with failure to thrive. The fellowship task in each is the same: confirm, treat at full dose within two weeks, and build the surveillance net that carries the brain through its critical first thousand days. [3] [4]
The four moves — Confirm, Treat, Monitor, Reassess
Overview & Definition
Congenital hypothyroidism is the deficiency of thyroid hormone that is present at birth, whether because the gland never formed, formed in the wrong place, formed but cannot make hormone, or is not being driven by an intact pituitary axis. It is one of the commonest preventable causes of intellectual disability, and the entire machinery of newborn screening was built to detect it in the asymptomatic first weeks, before the clinical picture declares itself. [4] [9]
The historical name — cretinism — described the untreated end-state: severe intellectual disability, deafness, spasticity, and the coarse features and growth failure that gave the condition its name. That end-state is now a failure of the screening programme, not an expected outcome, because early and adequate levothyroxine restores the developmental trajectory. The disease itself has not changed, but the clinical task has shifted from rescuing a brain-damaged child to running a reliable pipeline that keeps the thyroid axis normal from the first week of life. [9] [7]
What has not changed is the biology the screening protects against. Thyroid hormone, as T3, drives myelination, synaptogenesis, and neuronal migration through the first thousand days, and the fetal and neonatal brain are wholly dependent on it. A baby whose thyroid hormone is low through that window pays a cognitive cost that is hard to recover, which is why the dose, the timing, and the adherence matter more than any other detail in the topic. [10] [1]
Classification
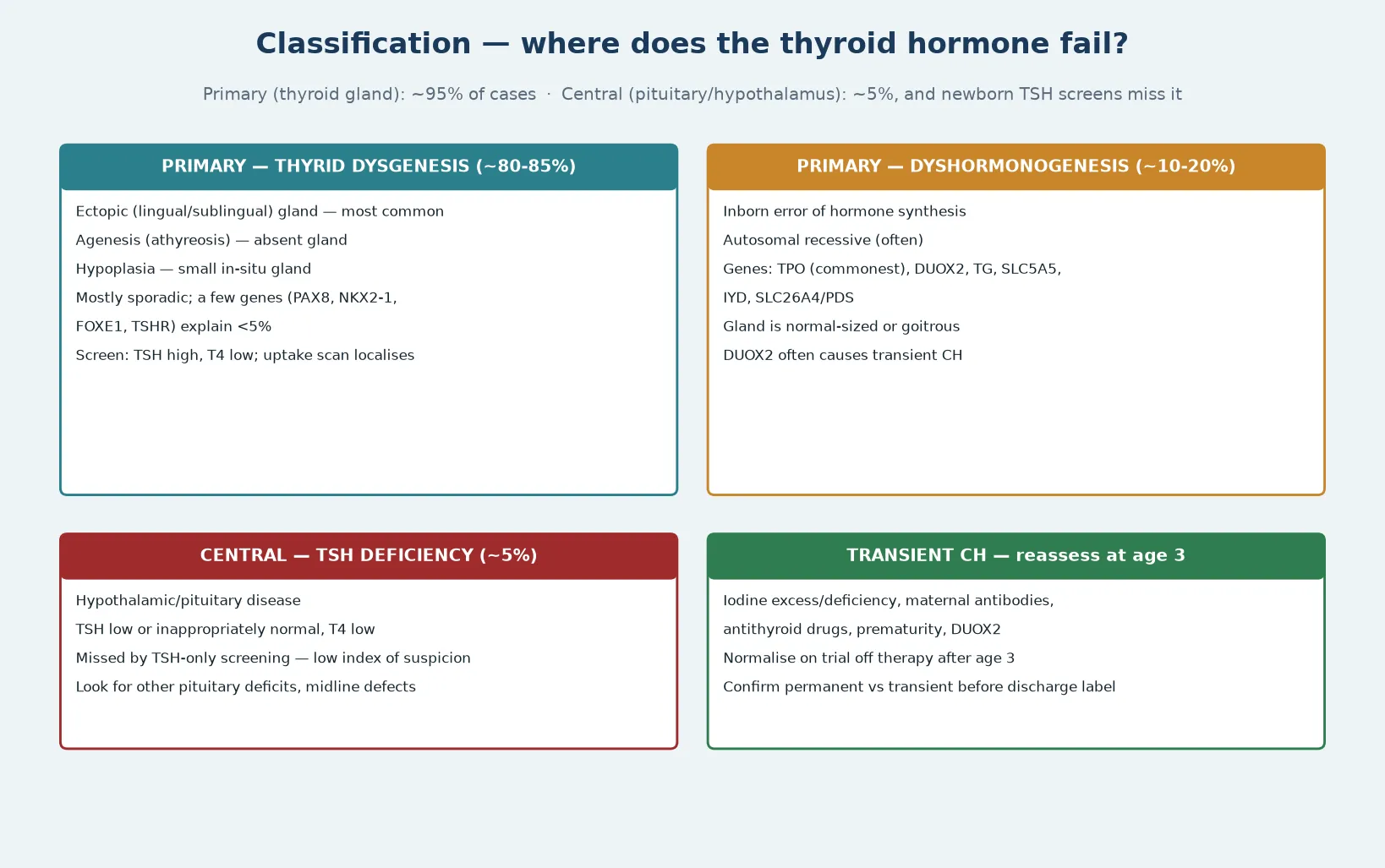
The classification that earns marks at fellowship separates primary from central disease, and within primary disease separates the structural causes from the biosynthetic ones. Primary congenital hypothyroidism — a faulty thyroid gland — accounts for about 95 per cent of cases, and it carries a high TSH because the intact pituitary drives the failing gland harder. Central congenital hypothyroidism — a faulty hypothalamus or pituitary — accounts for the remaining 5 per cent, and it carries a low or inappropriately normal TSH because the drive itself is absent. [4] [10]
Within primary disease, thyroid dysgenesis is the largest group, accounting for about 80 to 85 per cent. Dysgenesis means the gland never formed correctly: it is ectopic, sitting under the tongue or in the lingual position; athyreotic, absent altogether; or hypoplastic, present but too small. Most dysgenesis is sporadic, and identified genes such as PAX8, NKX2-1, FOXE1, and the TSH receptor explain only a small minority, which is why family recurrence is usually low. The remaining primary cases — about 10 to 20 per cent — are dyshormonogenesis, inborn errors of hormone synthesis that are usually autosomal recessive, often leave a normal-sized or goitrous gland, and are the form most likely to be transient or familial. [4] [1]
Dyshormonogenesis is where the molecular detail has grown. Thyroid peroxidase (TPO) is the commonest gene; DUOX2 and its maturation factor DUOXA2, thyroglobulin (TG), the sodium-iodide symporter SLC5A5, iodotyrosine deiodinase IYD, and pendrin SLC26A4 are the others. A distinctive teaching point is that DUOX2 mutations often cause transient congenital hypothyroidism, which is one reason a permanence reassessment at age three exists — a child labelled at birth may not need lifelong treatment. [1] [4]
A separate and important category is transient congenital hypothyroidism, in which the deficiency resolves. Causes include iodine excess from antiseptics or contrast, iodine deficiency, transplacental maternal thyroid-blocking antibodies, maternal antithyroid drugs, and prematurity. The practical rule is that the permanence of congenital hypothyroidism is not declared at birth but confirmed at age three by a supervised trial off therapy, unless the gland is ectopic or the starting dose was high, in which case the disease is almost certainly permanent. [2] [1]
Epidemiology & Risk Factors
Congenital hypothyroidism occurs in roughly one in every two thousand to four thousand newborns, which makes it one of the commonest congenital endocrine disorders and a condition every general paediatrician will meet. The incidence is rising in screened populations, partly because of more sensitive TSH thresholds that catch milder and transient cases, and partly because of improved survival of premature and low-birth-weight infants who carry a higher background risk. [4] [2]
The strongest risk factor is the biology of thyroid development. Thyroid dysgenesis is usually sporadic and the recurrence risk in a subsequent sibling is low, but dyshormonogenesis is autosomal recessive and carries a 25 per cent sibling recurrence risk, which is why a family history of congenital hypothyroidism, goitre, or unexplained intellectual disability in a sibling shifts the pre-test probability toward a biosynthetic defect. Female infants are affected slightly more often than males in dysgenesis, and the sex ratio equalises in dyshormonogenesis. [4] [1]
Prematurity, low birth weight, twinning, and iodine status are the modifiable and confounding risk factors that shape screening practice. Premature and low-birth-weight infants have a delayed TSH rise, so an early single sample can read falsely normal and a repeat screen is mandatory. Iodine deficiency remains a cause in iodine-poor regions, while iodine excess from povidone-iodine antiseptics or contrast in the perinatal period can transiently suppress the neonatal thyroid. A fellowship answer names these factors because they explain both false-negative screens and the transient-versus-permanent question that follows every positive one. [2] [10]
Pathophysiology
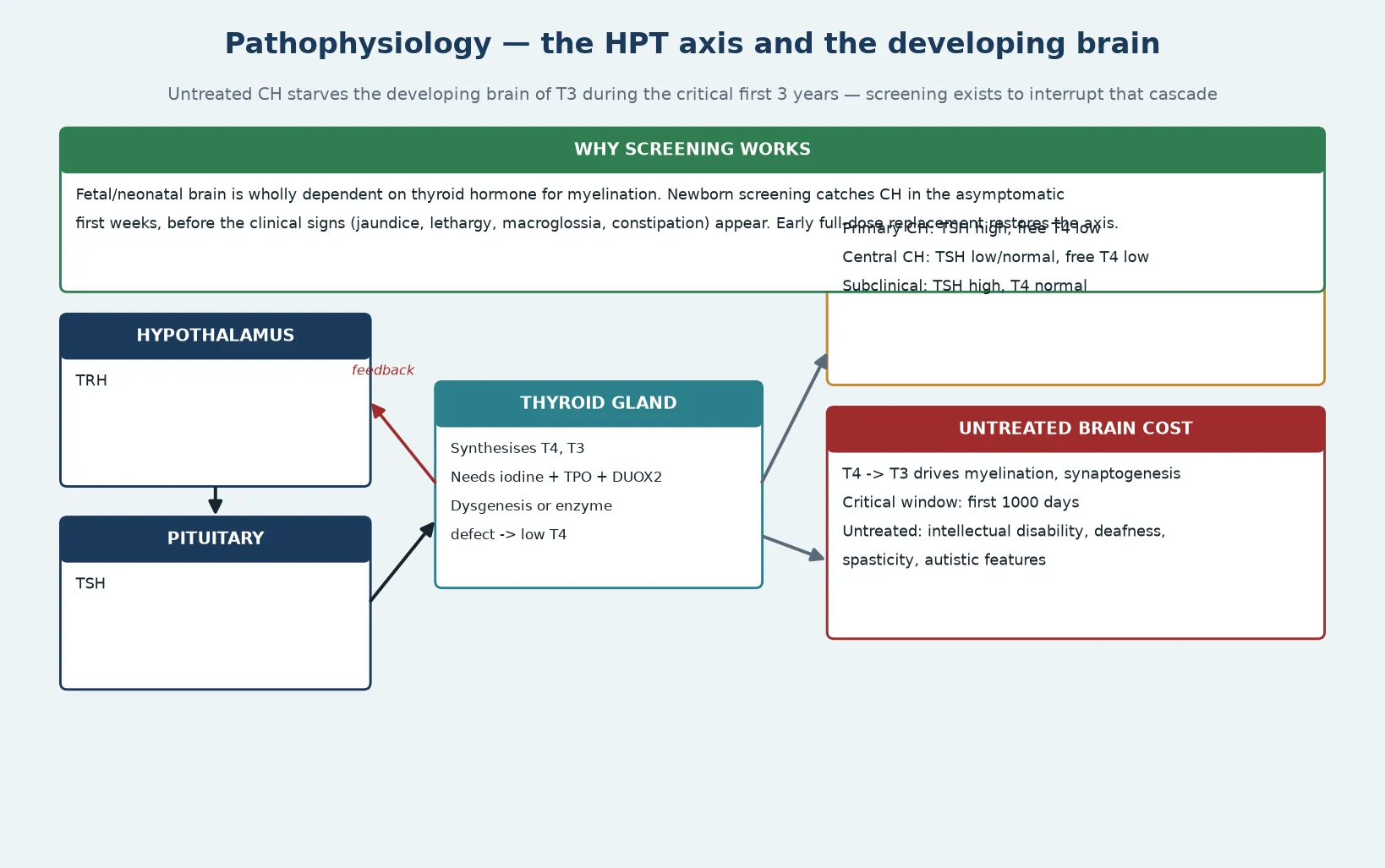
The pathophysiology has two halves: the thyroid axis and the developing brain, and a fellowship answer earns depth by connecting them. The hypothalamus releases thyrotropin-releasing hormone, which drives the pituitary to release thyroid-stimulating hormone, which drives the thyroid follicular cell to take up iodine, oxidise it with DUOX2, couple it to thyroglobulin through thyroid peroxidase, and release T4 and a smaller amount of T3. T4 is converted peripherally to the active T3, and the whole loop closes on negative feedback at both the pituitary and the hypothalamus. [10] [4]
When the gland is dysgenetic or an enzyme is missing, T4 and T3 fall, the negative feedback relaxes, and TSH rises — the biochemical signature of primary congenital hypothyroidism. When the pituitary or hypothalamus is the problem, the drive fails, T4 falls, and the TSH stays inappropriately low or normal — the signature of central disease, and the reason a TSH-only screen misses it. The classification maps directly onto the axis, and the biochemistry follows the lesion, which is why reading a thyroid function test as primary or central is the first diagnostic move. [10] [1]
The brain half is why screening exists. Thyroid hormone, acting as T3 at nuclear receptors, drives myelination, neuronal migration, synaptogenesis, and dendritic arborisation through the first thousand days, with the fetal and early neonatal brain particularly dependent on it. Untreated congenital hypothyroidism produces the historical cretinism phenotype — intellectual disability, sensorineural deafness, spasticity, and autistic features — because those developmental processes are starved of hormone at their critical window. The cost is dose-dependent and time-dependent: the longer and the deeper the hormone deficit, the larger and less recoverable the cognitive loss. [9] [7]
This is the biological justification for the treatment rules. A high initial dose of levothyroxine, started within the first two weeks, restores thyroid hormone to the developing brain at the moment it is most needed, and the monitoring targets — free T4 normal by two weeks, TSH normal by four weeks — are calibrated to that neuroprotective window. The pathophysiology is not background detail; it is the reason the dose, the timing, and the adherence are treated as resuscitation-grade priorities rather than routine endocrine management. [5] [6]
Clinical Presentation
The newborn with congenital hypothyroidism is usually asymptomatic, which is the whole point of screening — by the time the clinical signs appear, the brain has already been exposed to hormone deficiency. A fellowship answer therefore frames the presentation as a spectrum from the screen-detected well baby to the classic untreated infant, and earns depth by naming the subtle early signs that precede the full picture. [4] [3]
The early signs are non-specific and easily missed: prolonged jaundice — especially a mixed unconjugated and conjugated pattern from impaired hepatic glucuronidation and reduced bile flow; lethargy and poor feeding; hypotonia; a large posterior fontanelle or wide cranial sutures from delayed bone maturation; constipation; and a low, hoarse cry. Temperature instability, bradycardia, and macroglossia round out the picture. None is specific in isolation, but together they form a recognisable gestalt, and a midwife or junior clinician who flags the sleepy, jaundiced, constipated, large-fontanelle baby is often the one who accelerates the diagnosis. [3] [4]
The untreated infant develops the classic features over weeks to months: coarse facies, a large protruding tongue, dry skin and hair, an umbilical hernia, muscular pseudohypertrophy, and marked developmental delay with failure to thrive. This is the phenotype that screening was built to prevent, and in a well-run programme it should be a historical curiosity rather than a routine presentation. When it does appear, it signals a failed screen, a missed recall, or a family lost to follow-up. [4] [9]
The presentation also tracks the underlying cause. A baby with an ectopic lingual thyroid may have a palpable fullness at the base of the tongue; a baby with dyshormonogenesis may have a goitre at birth; and a baby with central disease may carry the stigmata of a pituitary or midline defect, such as hypoglycaemia, micropenis, cholestasis, or optic-nerve hypoplasia. Recognising these clues points toward central disease — the form the TSH screen misses — and triggers venous thyroid function tests rather than reassurance from a normal bloodspot. [10] [1]
Differential Diagnosis
The differential splits into three questions: what else raises the newborn TSH, what else produces a low free T4, and what else causes the clinical picture of a sleepy, jaundiced, constipated neonate. The first and most important is transient hyperthyrotrophinaemia or transient congenital hypothyroidism, in which the TSH is raised but the gland is anatomically and genetically normal and the abnormality resolves. [2] [4]
Transient congenital hypothyroidism is caused by iodine excess from povidone-iodine antiseptics or contrast media, iodine deficiency, transplacental maternal thyroid-blocking antibodies, maternal antithyroid drugs such as carbimazole or propylthiouracil, and prematurity with its delayed TSH rise. Distinguishing transient from permanent disease at birth is often impossible, which is why the permanence reassessment at age three is a universal step; treating a transient case as permanent simply means the child stays on a dose they will later prove not to need. [1] [2]
A low free T4 with a low or normal TSH raises the question of central disease and its mimics. Central congenital hypothyroidism from panhypopituitarism, septo-optic dysplasia, or a pituitary transcription-factor defect sits alongside euthyroid-sick syndrome from severe neonatal illness, in which systemic stress lowers T4 without a true thyroid disorder. Binding-protein abnormalities such as congenital thyroxine-binding globulin deficiency lower the total T4 but leave the free T4 and TSH normal, and they are a classic trap if only total T4 is measured. [10] [4]
The clinical differential of the untreated picture includes Down syndrome, which carries a higher background rate of congenital hypothyroidism and a characteristic facies; congenital adrenal hyperplasia, which shares failure to thrive but adds salt-wasting and ambiguous genitalia; and inborn errors of metabolism that present with lethargy and feeding difficulty. The discriminating move is always the thyroid function test combined with the clinical context, because the treatment of confirmed congenital hypothyroidism does not wait for the differential to close. [4] [3]
| Feature | Permanent CH (dysgenesis) | Transient CH | Central CH |
|---|---|---|---|
| TSH | High | High | Low / normal |
| Free T4 | Low | Low or borderline | Low |
| Gland on scan | Ectopic or absent | Normal in situ | Normal in situ |
| Recurrence risk | Low (sporadic) | Variable | Depends on cause |
| Long-term levothyroxine | Lifelong | Often stops at age 3 | Lifelong |
Clinical & Bedside Assessment
The recognition move is simple and runs off the screening result: an abnormal bloodspot TSH earns venous thyroid function tests, and a baby with clinical signs earns them regardless of the screen. The bedside skill is to treat the abnormal result as time-critical, to confirm with venous TSH and free T4, and to start treatment the same day rather than waiting for the recall appointment. A delayed confirmation is the commonest break in the pipeline. [1] [3]
The history gathers the discriminators that shape the diagnosis and the counselling. Ask about the bloodspot result and the day it was taken, because an early sample in a premature infant may be falsely normal. Ask about maternal thyroid disease and medications, because antithyroid drugs and blocking antibodies cause transient disease. Ask about a family history of congenital hypothyroidism, goitre, or unexplained intellectual disability, because a sibling affected raises the probability of a recessive dyshormonogenesis. Ask about perinatal iodine exposure, because povidone-iodine antiseptics and contrast suppress the neonatal thyroid. [2] [4]
Examination is focused and quick, because treatment should not wait. Look for the early signs — prolonged jaundice, lethargy, hypotonia, a large posterior fontanelle, macroglossia, an umbilical hernia — and examine for a goitre, which points to dyshormonogenesis, or a lingual mass, which points to an ectopic gland. In a baby with central features — hypoglycaemia, micropenis, cholestasis, midline or optic defects — examine the pituitary axes, because central disease carries coexistent hormone deficits. Growth, feeding, and the developmental trajectory function as vital signs here. [3] [10]
The first visit also assesses the family's capacity to sustain daily levothyroxine and frequent monitoring, because adherence is the single biggest determinant of long-term outcome. A family that cannot give a consistent daily dose, cannot attend monitoring, or cannot afford or access the tablets will see abnormal thyroid function tests that look like a treatment failure. Map the practical context — transport, health literacy, interpreter needs, and a reliable supply of the correct tablet strength — and identify a named coordinator early. [1] [4]
Investigations
The venous thyroid function test is the single confirmatory investigation, and it is treated as urgent. Measure TSH and free T4 — and in suspected central disease, free T4 is the lead value because the TSH is misleadingly low. The pattern is diagnostic: a high TSH with a low free T4 confirms primary congenital hypothyroidism; a low or inappropriately normal TSH with a low free T4 confirms central disease; and a high TSH with a normal free T4 defines subclinical or compensated disease. [1] [4]
Thyroid imaging — a radionuclide uptake scan with technetium-99m or iodine-123, and an ultrasound — localises the gland and distinguishes dysgenesis from dyshormonogenesis, but it is optional at the point of diagnosis and must never delay treatment. An ectopic gland, an absent gland, or a normal in-situ gland each point toward a cause and inform the permanence question, but the levothyroxine dose is the same regardless of the imaging result. Imaging is most useful when it is logistically feasible and when the result will change the long-term plan. [2] [1]
Additional investigations are tailored to the suspected cause. A low free T4 with central features triggers a full pituitary axis panel — cortisol, growth hormone, prolactin, and sex hormones — and a magnetic resonance imaging of the pituitary and hypothalamus, because central congenital hypothyroidism coexists with other hormone deficits that need separate management. Thyroid antibodies and maternal thyroid function are checked when transient disease from maternal blocking antibodies or antithyroid drugs is suspected. Genetic testing for dyshormonogenesis is increasingly available and informs counselling, particularly when a goitre is present or a sibling is affected. [10] [4]
A practical point that earns marks: the newborn bloodspot programme and the venous confirmation are complementary, not redundant. The bloodspot is a screening test optimised for sensitivity and carries false positives and false negatives; the venous test is the diagnostic confirmation. A baby who is clinically well with a minimally raised bloodspot TSH still needs the venous test, and a baby who is clinically unwell with a normal bloodspot still needs it if central disease is in the differential. [3] [9]
Management — Resuscitation
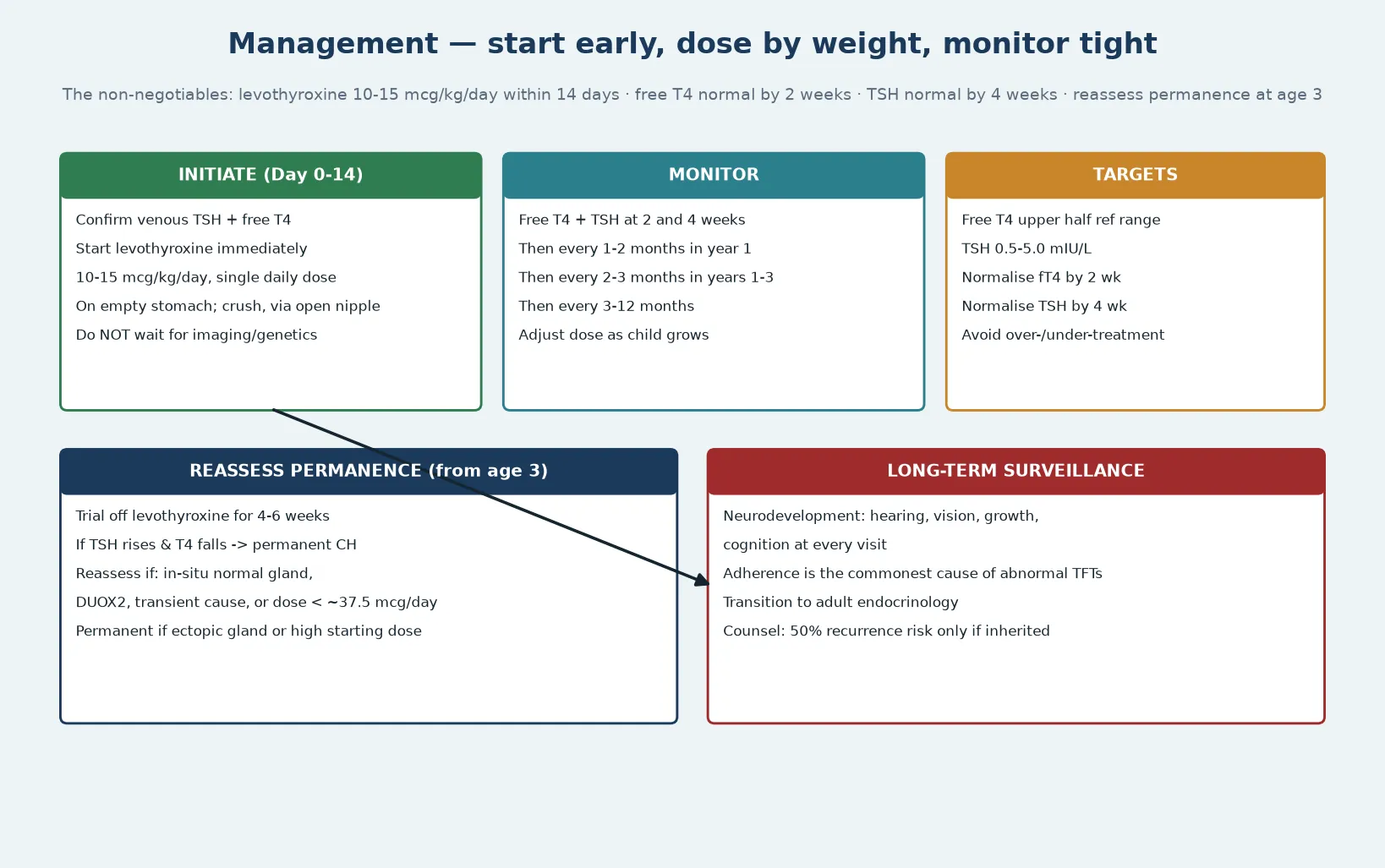
Resuscitation in congenital hypothyroidism means interrupting the hormone deficiency at the brain's critical window, and the treatment is both simple and time-critical: levothyroxine at a full dose, started as soon as the venous diagnosis is made and ideally within the first two weeks of life. There is no role for a cautious escalating dose, because a low starting dose is the commonest preventable cause of residual neurodevelopmental deficit. [5] [6]
The starting dose is levothyroxine at 10 to 15 mcg per kg per day, given as a single daily oral dose on an empty stomach. The tablet is crushed and given via an open nipple with a small volume of milk or water, never mixed into a full feed where adherence to the dose becomes unreliable. The systematic-review evidence supports a high initial dose for neurodevelopmental protection, and the 2021 ENDO-ERN consensus and the 2014 European Society for Paediatric Endocrinology guidelines both endorse the 10 to 15 mcg per kg per day range. [5] [1]
The immediate monitoring targets are explicit and are treated as resuscitation endpoints. The free T4 should normalise within two weeks and the TSH within four weeks of starting treatment, and venous thyroid function tests are checked at two and four weeks to confirm. A persistently high TSH on a correct dose does not mean the dose is wrong — it most often means non-adherence or malabsorption, and the response is to re-counsel the family on administration, not to escalate the dose endlessly. [2] [3]
In central congenital hypothyroidism, levothyroxine is still the treatment, but two resuscitation-grade rules apply. First, hydrocortisone replacement must precede or accompany levothyroxine if adrenal insufficiency coexists, because starting levothyroxine first accelerates cortisol clearance and can precipitate an adrenal crisis. Second, the dose is titrated to the free T4 rather than the TSH, because the TSH is unreliable in central disease. These two rules — cortisol first, free T4-led dosing — are the central-disease traps that cost marks and harm babies. [10] [4]
Management — Definitive & Stepwise
Definitive management is dose-for-growth surveillance that runs from the neonatal period into adult endocrine care, and it is the core of fellowship-level competence. The levothyroxine dose is adjusted to weight and to the thyroid function targets as the child grows, and the monitoring frequency steps down with age while never lapsing. The schedule is staged, and each stage carries a specific check that prevents a specific harm. [1] [2]
In the first year, thyroid function is checked every one to two months, because growth is rapid and the dose is easily outgrown. In the second and third years, monitoring moves to every two to three months, and from age three the interval extends to every three to twelve months. At every visit, the child is weighed, the dose per kilogram is recalculated, and the free T4 and TSH are checked, because the commonest cause of an abnormal test is a dose that has not kept up with growth. [3] [4]
The permanence reassessment at age three is a universal and structured step, not an afterthought. The child is admitted or closely supervised for a trial off levothyroxine for four to six weeks, and the thyroid function is rechecked: a rising TSH with a falling T4 confirms permanent congenital hypothyroidism and treatment resumes; a stable normal result confirms transient disease and treatment stops. The trial is unnecessary if the gland is ectopic or absent or if the starting dose was high, because those features already declare the disease permanent. [2] [1]
The targets are explicit and worth saying aloud. The free T4 is kept in the upper half of the age-appropriate reference range, and the TSH is kept between 0.5 and 5.0 mIU per litre. Over-treatment — a persistently suppressed TSH — risks iatrogenic hyperthyroidism and its effects on growth, behaviour, and bone, while under-treatment risks recurrent hypothyroidism. The fine adjustment between these is what the dose-for-growth surveillance exists to achieve. [1] [3]
Specific Subtypes & Scenarios
Central congenital hypothyroidism is the subtype that most often defeats a screening programme, and it deserves its own management pathway. The TSH is low or inappropriately normal, so the diagnosis rests on a low free T4 with a pituitary or midline context, and the work-up is a full pituitary axis assessment rather than a thyroid-only panel. Hydrocortisone precedes levothyroxine when adrenal insufficiency coexists, the dose is titrated to free T4, and the child is managed jointly with endocrinology and neurosurgery when a structural pituitary lesion is present. [10] [4]
DUOX2-related congenital hypothyroidism is a distinct dyshormonogenesis scenario that a fellowship answer should name. DUOX2 mutations produce a dual-oxidase deficiency that impairs thyroid hormone synthesis, and they are a recognised cause of transient congenital hypothyroidism, so a child with a DUOX2 mutation and an in-situ gland is a strong candidate for the age-three permanence reassessment rather than an assumption of lifelong treatment. Recognising the genotype prevents the error of lifelong over-treatment of a transient condition. [1] [4]
The premature and low-birth-weight infant is a scenario shaped by physiology. The TSH surge is blunted and delayed in prematurity, so an early single bloodspot can read falsely normal, and a repeat screen at two to four weeks or at discharge — whichever is later — is mandatory. Premature infants also carry a higher background rate of transient and non-thyroidal illness, which complicates interpretation, so the venous confirmation is read in the clinical context rather than in isolation. [2] [10]
The infant of a mother with thyroid disease is a scenario defined by the maternal context. Transplacental maternal thyroid-stimulating or blocking antibodies, and maternal antithyroid drugs such as carbimazole and propylthiouracil, each produce transient neonatal thyroid dysfunction. The neonate is monitored with venous thyroid function tests, treated transiently if needed, and the abnormality usually resolves over weeks to months as the antibody or drug clears. Recognising the maternal cause prevents the error of labelling a transient neonatal condition as permanent. [2] [4]
Why the permanence reassessment exists — and when to skip it
The permanence reassessment at age three exists because a substantial minority of babies labelled with congenital hypothyroidism at birth have transient disease — from iodine, maternal antibodies, prematurity, or DUOX2 — and will not need lifelong levothyroxine. The trial off therapy for four to six weeks, with recheck of TSH and free T4, separates permanent from transient. The reassessment can be skipped when the disease is almost certainly permanent: an ectopic or absent gland on imaging, or a starting levothyroxine dose that is high because the hormone deficiency was severe. Naming this step shows the candidate understands that the label at birth is provisional. [2] [1]
Complications & Pitfalls
The harm in congenital hypothyroidism comes most often from a break in the pipeline — a delayed or under-dosed start, a missed recall, or a family lost to follow-up — and the fellowship answer names these breaks as the cardinal pitfalls. Once treatment is started at the right dose and time, the residual neurodevelopmental risk is small but real, and the surveillance plan exists to keep it that way. [7] [9]
The acute complications are the consequences of untreated hormone deficiency presenting through a failed screen. Severe intellectual disability, sensorineural deafness, spasticity, and growth failure are the end-state that screening prevents, and their appearance in a screened population signals a programme failure — a false-negative screen, a missed recall, or non-adherence. The pitfall common to all is treating the presenting complication without recognising and correcting the underlying thyroid deficiency. [9] [4]
The long-term complications run through childhood and adolescence and are the substance of surveillance. Subtle neurodevelopmental deficits — in memory, attention, and motor coordination — persist even in well-treated children, and they are the reason formal developmental and educational follow-up is built into the plan. Over-treatment with a suppressed TSH risks behaviour change, sleep disturbance, and effects on growth and bone, while under-treatment risks recurrent cognitive effects. Each is a consequence of imperfect dose adjustment that the surveillance is designed to catch. [7] [8]
Management pitfalls share a common root: breaking the pipeline. Starting at a low dose to be cautious, delaying treatment while waiting for imaging or genetics, failing to re-dose for growth, escalating the dose for a high TSH caused by non-adherence rather than deficiency, and forgetting to reassess permanence at age three are each preventable errors. In central disease, starting levothyroxine before hydrocortisone in an adrenal-insufficient child is the trap that precipitates crisis. The safeguard is the structured pipeline and the documented surveillance plan. [5] [10]
Prognosis & Disposition
The prognosis of treated congenital hypothyroidism is excellent, and a child who is detected early, treated at a full dose within two weeks, and maintained on dose-for-growth surveillance has cognitive and motor outcomes close to the normal population. The single biggest predictor of outcome is the timing and adequacy of the initial treatment, because the developing brain's sensitivity to thyroid hormone is greatest in the first weeks and months. [7] [9]
The residual risk is small but measurable. Well-treated cohorts show subtle deficits relative to controls in memory, attention, and motor coordination, and these are larger in children whose disease was severe at diagnosis or whose treatment started later or at a lower dose. The fellowship answer frames prognosis in these honest terms — near-normal but not identical to unaffected peers — and builds developmental and educational surveillance into the plan to catch and support the children who need it. [8] [7]
The general paediatrician owns the coordination, and the disposition is shared, structured care. Endocrinology drives the thyroid axis and the dose adjustment, the newborn-screening programme owns the recall and the initial confirmation, audiology and ophthalmology screen for the hearing and vision comorbidity, and education and developmental services support the child through school. A named coordinator prevents the fragmentation that is the enemy of a monitoring-based plan, and referral to a specialist paediatric endocrine service at diagnosis measurably improves outcomes. [1] [4]
Recurrence-risk counselling closes the prognostic picture. Thyroid dysgenesis is usually sporadic and the recurrence risk in a subsequent sibling is low, but dyshormonogenesis is autosomal recessive and carries a 25 per cent recurrence risk, so a confirmed molecular diagnosis refines the counselling. In central disease the recurrence risk depends on the underlying cause. The counselling addresses not only the next pregnancy but the family's understanding that the child will, in almost all cases, live a full and typical life on a single daily tablet. [2] [4]
Special Populations
Congenital hypothyroidism interacts with the child's social, cultural, and developmental context, and the same treatment plan behaves differently across populations — access, adherence, and late presentation each shape the outcome. A plan that is clinically correct but unattainable for a family is no plan at all, because adherence to a daily tablet and attendance at frequent monitoring are the determinants of outcome. [1] [4]
Indigenous children in Australia and Aotearoa New Zealand may face later presentation through reduced access to screening recall and specialist services, particularly in remote communities, and the consequences of a missed or late diagnosis fall hardest where access is poorest. Telehealth and outreach extend the surveillance net into communities that a clinic-based model would miss, and a low threshold to repeat thyroid function tests in an unwell or failing-to-thrive infant is the safeguard against a false-negative or lost screen. [9] [3]
Migrant, refugee, and asylum-seeking families may arrive with incomplete medical records, an uncertain screening history, and no documented bloodspot result, and the diagnosis may not have been made in the country of origin. A careful reconstruction of the history, confirmation of the thyroid axis by venous tests, and an interpreter-mediated explanation of the treatment and monitoring plan are the foundations, and the written schedule is provided in the family's language. [4] [2]
Socioeconomic disadvantage shapes adherence and monitoring feasibility, because the limiting step is often a reliable tablet supply, transport to appointments, and the parental time to give a daily dose, rather than the medicine itself. Structuring the surveillance around a single coordinated visit, linking the family to a support organisation and to appointment and transport support, and using telehealth to reduce travel all improve engagement. The school-age child with subtle learning deficits is a population in their own right, and targeted educational support is the intervention that protects the developmental trajectory. [7] [8]
Evidence, Guidelines & Regional Differences
The evidence base rests on the 2020 to 2021 ENDO-European Reference Network consensus guidelines update, endorsed by the European Society for Pediatric Endocrinology and the European Society for Endocrinology, which is the most current operational reference and frames the screening, the diagnosis, the levothyroxine dose, the monitoring targets, and the permanence reassessment. The 2014 European Society for Paediatric Endocrinology consensus guidelines provide the prior international standard, and the American Academy of Pediatrics 2006 update of newborn screening and therapy remains the foundation for North American and many antipodean programmes. [1] [2] [3]
The dose and the neurodevelopmental evidence are what distinguishes a mature answer from a checklist. The Hrytsiuk 2002 systematic review established that a high initial levothyroxine dose improves cognitive outcome, and the Albert 2013 data confirmed neurodevelopmental and body-composition outcomes with high-dose initial replacement and close monitoring. The Kempers 2006 and 2007 Dutch cohorts defined the long-term intellectual and motor outcomes of screen-detected and treated young adults, anchoring the honest framing of subtle residual deficits. The Grosse 2011 health-economics analysis quantified the intellectual disability prevented through screening, which is the population-level justification for the programme. [5] [6] [7] [8] [9]
Where the evidence is weak, a fellowship answer says so honestly. The optimal TSH screening threshold — which determines how many mild and transient cases are detected — varies between programmes and is a live source of controversy. The long-term cognitive outcomes of the milder cases detected by ever-lower thresholds are genuinely uncertain, and the role of genetic testing and the management of the transient DUOX2 cases are areas of evolving practice. Naming the uncertainty is a mark of intellectual honesty that examiners reward. [1] [2]
In Australia and Aotearoa New Zealand, congenital hypothyroidism is detected through the universal newborn bloodspot screening programme, with a TSH-based assay on the day-two-to-five sample and a recall threshold set nationally. Care follows the international consensus guidelines, with paediatric endocrinology in the major centres and shared care with general paediatrics and primary care across rural and remote regions. The levothyroxine dose of 10 to 15 mcg per kg per day, the two-and-four-week monitoring, and the age-three permanence reassessment are the operational standards, and telehealth extends specialist surveillance into communities that distance would otherwise exclude. Access to paediatric endocrinology, recall follow-up, and developmental support is uneven across rural and remote communities, which intensifies the need for early, structured engagement. [1] [3]
Exam Pearls
A fellowship candidate answering on congenital hypothyroidism should land five anchor points and avoid three classic traps. The anchors are the framework examiners listen for; the traps are where easy marks are lost. [1] [3]
Anchor one: run the pipeline. Screen at day two to five, confirm with venous TSH and free T4, and start levothyroxine within two weeks. The pipeline is the topic, and a break anywhere along it is a preventable failure. [2]
Anchor two: dose high and early. Levothyroxine 10 to 15 mcg per kg per day, started within the first two weeks, protects the developing brain. A cautious low starting dose is the commonest preventable cause of residual neurodevelopmental deficit. [5] [6]
Anchor three: know the targets. Free T4 normal within two weeks, TSH normal within four weeks, then dose-for-growth surveillance through infancy. The free T4 sits in the upper half of the range and the TSH between 0.5 and 5.0 mIU per litre. [1]
Anchor four: separate primary from central. Primary disease carries a high TSH and the screen detects it; central disease carries a low or normal TSH and the screen misses it. Any low free T4 with a pituitary or midline context needs venous tests, and in central disease give hydrocortisone before levothyroxine. [10] [4]
Anchor five: reassess permanence at age three. A supervised trial off therapy for four to six weeks separates permanent from transient disease, unless the gland is ectopic or the starting dose was high. The label at birth is provisional. [2]
The three traps to avoid are starting at a low cautious dose, waiting for imaging or genetics before treating, and escalating the dose for a high TSH caused by non-adherence rather than deficiency. Thyroid dysgenesis accounts for 80 to 85 per cent of primary cases, TPO is the commonest dyshormonogenesis gene, the starting dose is 10 to 15 mcg per kg per day, and a normal bloodspot does not exclude central disease — the high-yield facts a candidate holds. Avoid the traps and land the anchors, and the rest of the answer falls into place. [1] [4]
References
- [1]van Trotsenburg P, Stoupa A, Léger J, Rohrer T, Peters C, Colmenares A, Pohlenz J, Tylek-Lemańska D, Kühnen P, Keco A, Antonozzi I, Rapaport R, Liptáková Kśonžková L, Djordjevic M, Zdraveska N, Garré A, Cassio A, Grulichová K, Krstevska M, Markovic T, Jazbec J, Guran T, Kairamkonda V, De Marco G, Dartevelle P, Sarafi V, Serra S, Chiesa A, Morselli-Labate AM, Cappa M, Rabbiosi S, Gastaldi R, Weetman AP, Persani L, Szinnai G, Polak M, Peters C, Czernichow P, Deladoëy J, Castanet M, Bona G, Bellone J, Krude H, Park SM, Kyng NP, Skraba Z, Pertl Z, Di Iorgi N, Maghnie M, Radetti G, Tato L, Sala E, Mainardi B, Zucchinetti P, Crinò A, Di Cintio E, Delvecchio M, Di Sarno AM, Albarel F, Salerno MC, Cardinale F, Sposito M, Franzese A, Iughetti L, Maglio M, Moia S, Pozzobon G, Zampolli C, Bozzola E, Radetti G, Wassner AJ, Cappa M. Congenital Hypothyroidism: A 2020-2021 Consensus Guidelines Update-An ENDO-European Reference Network Initiative Endorsed by the European Society for Pediatric Endocrinology and the European Society for Endocrinology. Thyroid, 2021.PMID 33272083
- [2]Léger J, Olivieri A, Donaldson M, Torresani T, Krude H, van Vliet G, Polak M, Görtner G, Espe Pegliafiche S, Bitoun P, Ritzen EM, Torres Borrego J, Sack J, Pohlenz J, Sassolas G, Mullis PE, Bona G, Karlsson F, Hertel NT, Battelino T, Antonozzi I, Nordenström A, Jaruratanasirikul S, Chiesa A, Stoppioni V, Vigone MC, Castanet M, Karis J, Sippel J, Kooman JP, Gruters A, Arrigo T, Grulichova K, Tylek-Lemanska D, Ciesielski K, Donaldson M, Toft Sorensen J, Zimmermann MB, Delange F, Pohlenz J, Szinnai G, Langham S, Dandona P, Paterson W, Donaldson MD, Jackson I. European Society for Paediatric Endocrinology consensus guidelines on screening, diagnosis, and management of congenital hypothyroidism. J Clin Endocrinol Metab, 2014.PMID 24446653
- [3]American Academy of Pediatrics, Rose SR, Section on Endocrinology and Committee on Genetics, American Thyroid Association, Lawson Wilkins Pediatric Endocrine Society. Update of newborn screening and therapy for congenital hypothyroidism. Pediatrics, 2006.PMID 16740880
- [4]Rastogi MV, LaFranchi SH. Congenital hypothyroidism. Orphanet J Rare Dis, 2010.PMID 20537182
- [5]Hrytsiuk I, Gilbert R, Logan S, Pindoria S, Brook CG. Starting dose of levothyroxine for the treatment of congenital hypothyroidism: a systematic review. Arch Pediatr Adolesc Med, 2002.PMID 11980555
- [6]Albert BB, Cutfield WS, Webster D, Carll J, Derraik JG, Jefferies C, Gunn AJ, Hofman PL. Neurodevelopmental and body composition outcomes in children with congenital hypothyroidism treated with high-dose initial replacement and close monitoring. J Clin Endocrinol Metab, 2013.PMID 23861458
- [7]Kempers MJ, van der Sluijs Veer L, Nijhuis-van der Sanden RW, Kooistra L, Wiedijk BM, Faber I, Last BF, de Vijlder JJ, Grootenhuis MA, Vulsma T. Intellectual and motor development of young adults with congenital hypothyroidism diagnosed by neonatal screening. J Clin Endocrinol Metab, 2006.PMID 16303842
- [8]Kempers MJ, van der Sluijs Veer L, Nijhuis-van der Sanden RW, Lanting CI, Kooistra L, Wiedijk BM, Faber I, Last BF, de Vijlder JJ, Grootenhuis MA, Vulsma T. Neonatal screening for congenital hypothyroidism in the Netherlands: cognitive and motor outcome at 10 years of age. J Clin Endocrinol Metab, 2007.PMID 17164300
- [9]Grosse SD, Van Vliet G. Prevention of intellectual disability through screening for congenital hypothyroidism: how much and at what level? Arch Dis Child, 2011.PMID 21242230
- [10]Raymond J, LaFranchi SH. Fetal and neonatal thyroid function: review and summary of significant new findings. Curr Opin Endocrinol Diabetes Obes, 2010.PMID 19901830