Paeds · endocrinology-diabetes-and-growth
Diabetic ketoacidosis
Also known as DKA · Paediatric diabetic ketoacidosis · Diabetic coma · Ketoacidosis in type 1 diabetes · New-onset diabetes with ketoacidosis
A fellowship approach to paediatric diabetic ketoacidosis: recognise the child with hyperglycaemia, ketosis and acidosis who is dehydrated and breathing deeply, diagnose on the triad of glucose over 11 millimoles per litre with venous pH below 7.3 or bicarbonate below 15 and ketonaemia, grade severity by pH and bicarbonate, and deliver the ISPAD-aligned protocol of careful rehydration over 48 hours, insulin at 0.05 to 0.1 units per kilogram per hour started an hour or two after fluids, early potassium replacement, and glucose-guided dextrose — while watching relentlessly for cerebral oedema, the complication that kills, and driving the resolution criteria of a closed anion gap before transition to subcutaneous insulin.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The single unifying idea is that DKA is dangerous twice over: once from the metabolic derangement itself, and again from the treatment, because correcting it too fast can precipitate cerebral oedema in a child whose brain has adapted to the illness. Every decision in the protocol is a compromise between fixing the acidosis and protecting the brain. [1] [3]
Overview & Definition
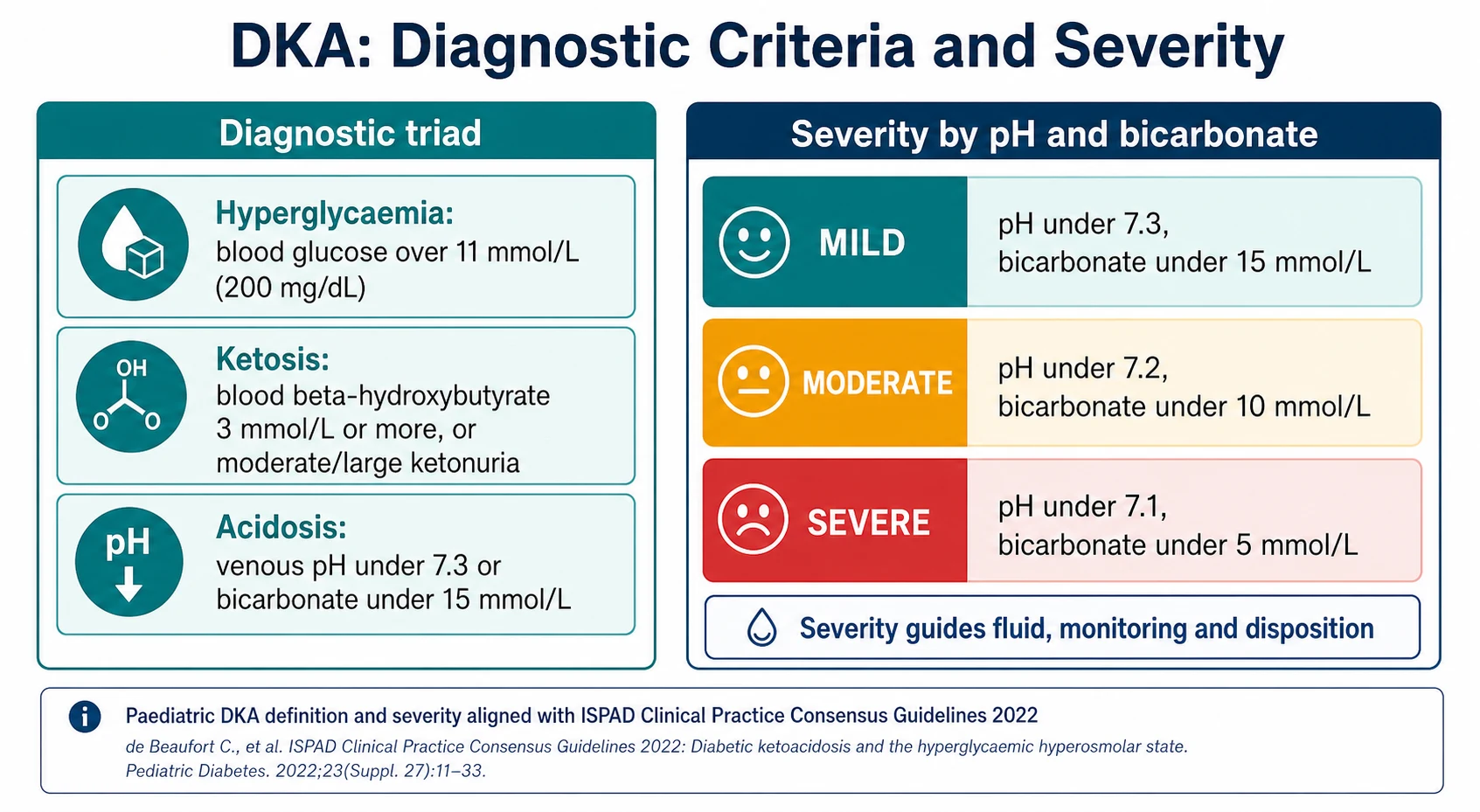
A child in diabetic ketoacidosis has run out of usable insulin, and the body has switched into a starvation-like emergency even though glucose is abundant in the blood. Without insulin the cells cannot take up glucose, so the liver pours out more and breaks down fat for fuel, generating ketoacids that overwhelm the blood's buffering capacity. The result is the diagnostic triad that defines the condition: a high glucose, ketones, and an acidosis. [1] [7]
The formal biochemical definition used by ISPAD requires all three components together. There must be hyperglycaemia, with a blood glucose above 11 millimoles per litre (200 milligrams per decilitre); there must be acidosis, with a venous pH below 7.3 or a serum bicarbonate below 15 millimoles per litre; and there must be ketosis, with a blood beta-hydroxybutyrate of 3 millimoles per litre or more, or moderate to large ketonuria. A child can be in DKA with a glucose that is only modestly raised — so-called euglycaemic DKA — which is why the acidosis and the ketones, not the glucose alone, make the diagnosis. [1] [8]
DKA matters because it is both common and lethal. It is the presenting feature in a large proportion of children with new-onset type 1 diabetes, and it recurs in children with established diabetes during illness, insulin omission, or pump failure. The great majority of children recover fully, but cerebral oedema — although rare — accounts for most of the deaths and much of the long-term neurological harm, and it is the reason the treatment protocol is so cautious. [1] [4]
Classification
DKA is graded by severity, and the grade drives the intensity of monitoring and the choice of where the child is nursed. Severity is defined by the depth of the acidosis rather than by the glucose, because it is the acidosis and the fluid deficit that threaten the child. A mild episode has a venous pH below 7.3 or a bicarbonate below 15 millimoles per litre; a moderate episode has a pH below 7.2 or a bicarbonate below 10; and a severe episode has a pH below 7.1 or a bicarbonate below 5. [1]
The second useful axis is the clinical context, because it shapes both the cause and the prevention. New-onset DKA announces the diagnosis of diabetes and often follows a period of undiagnosed polyuria and weight loss. Established-diabetes DKA follows insulin omission, an intercurrent illness, or a failure of an insulin pump, in which the loss of basal insulin can precipitate ketoacidosis within hours. Recognising which context you are in tells you whether the family needs a first diagnosis and full education, or a review of the sick-day rules and the reasons the child missed insulin. [1] [8]
| Severity | Venous pH | Bicarbonate (mmol/L) | Typical setting |
|---|---|---|---|
| Mild | < 7.3 | < 15 | Ward with close observation |
| Moderate | < 7.2 | < 10 | High-dependency or ward with hourly review |
| Severe | < 7.1 | < 5 | Intensive care or high-dependency, consider retrieval |
Epidemiology & Risk Factors
DKA is the commonest acute complication of type 1 diabetes in childhood and remains a frequent mode of first presentation. A substantial fraction of children are already in ketoacidosis when their diabetes is diagnosed, and the proportion is higher in younger children, in those without a family history to prompt earlier testing, and in communities with poorer access to care. In established diabetes, the recurrent-DKA pattern concentrates in a small group of high-risk adolescents. [1] [8]
The precipitants divide cleanly. At first presentation, the cause is simply undiagnosed diabetes that has progressed to insulin failure. In established disease, the common triggers are missed or reduced insulin, an intercurrent infection or other illness that raises insulin requirements, and pump failure — the child on a pump has no long-acting depot, so an occluded line or a failed site can tip them into ketoacidosis within a few hours. Psychosocial stress, eating disorders, and deliberate insulin omission drive the recurrent pattern in adolescents. [1]
[1]The risk factors that matter most in the exam are those for cerebral oedema, because that is the complication that determines outcome. The Glaser case-control study identified a lower initial partial pressure of carbon dioxide, a higher initial urea, and treatment with bicarbonate as independent risk factors, reflecting more severe dehydration and acidosis. Younger age and new-onset diabetes are consistently associated. These are the children who need the most cautious fluid and insulin regimen and the closest neurological watch. [3] [9]
Pathophysiology
The engine of DKA is the combination of insulin deficiency and a surge of the counter-regulatory hormones — glucagon, catecholamines, cortisol, and growth hormone. Insulin is the hormone of the fed state, and its absence flips the body into the fasting programme at the very moment glucose is plentiful. The liver stops storing glucose and starts making it, from glycogen and then from new synthesis, while the muscle and fat stop taking it up. Glucose therefore rises steeply. [1] [7]
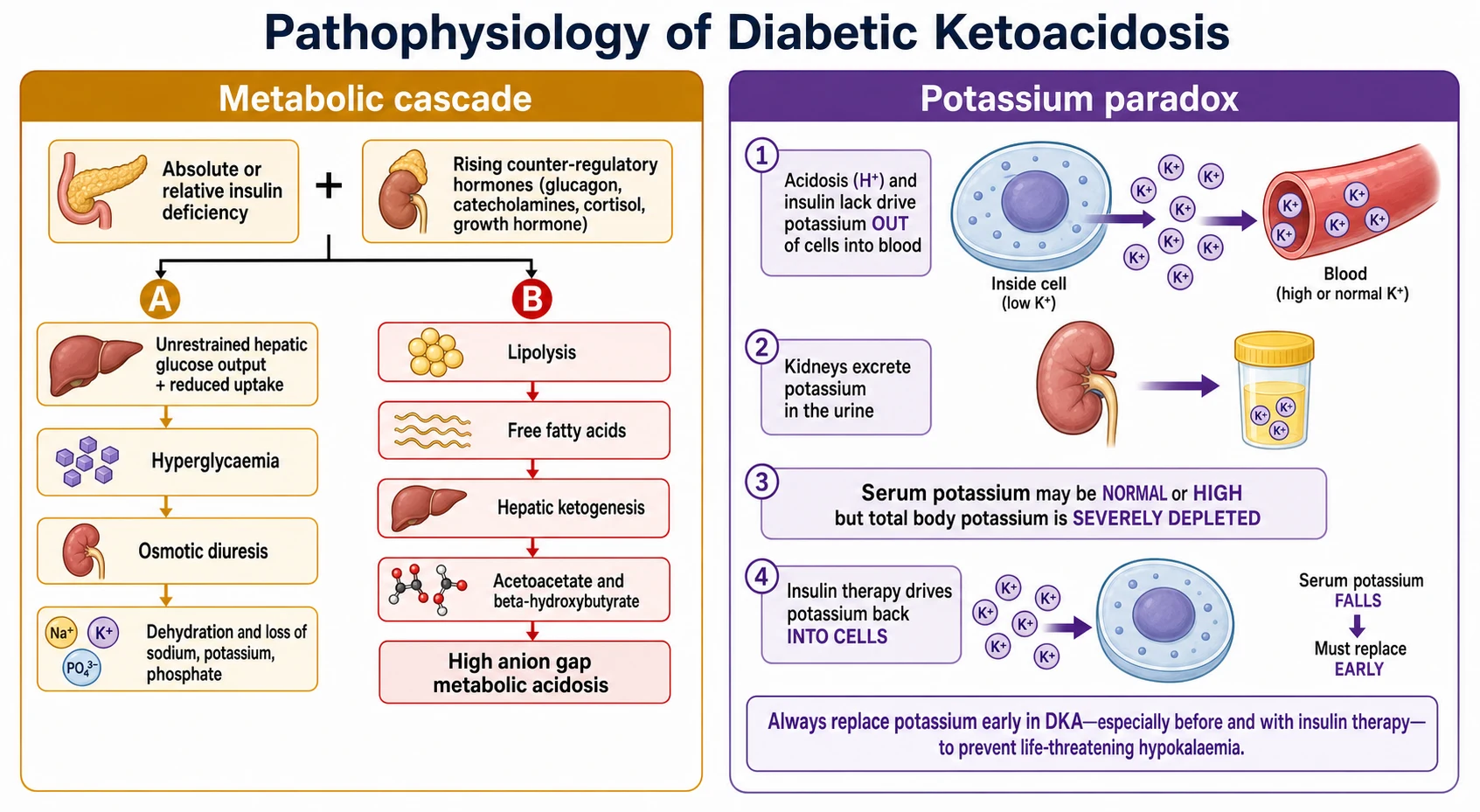
Two consequences flow from the high glucose. The first is osmotic diuresis: once glucose exceeds the renal threshold it drags water and electrolytes into the urine, producing the polyuria, the profound dehydration, and the loss of sodium, potassium, and phosphate that define the fluid picture. The second is ketogenesis: with no insulin to restrain it, fat is broken down to free fatty acids, which the liver converts to the ketoacids acetoacetate and beta-hydroxybutyrate. These acids consume bicarbonate and generate a high anion gap metabolic acidosis, and the body compensates by blowing off carbon dioxide through deep Kussmaul breathing. [1] [7]
The most examined subtlety is the potassium paradox. The acidosis and the lack of insulin both push potassium out of the cells into the blood, so the measured serum potassium at presentation is usually normal or even high — yet the total body store is severely depleted by the urinary losses. The moment insulin and fluids begin, potassium floods back into the cells and the serum level falls, sometimes dangerously. This is why potassium is replaced early and monitored hourly, and why insulin is never started in a child who is already hypokalaemic without first correcting the potassium. [1] [7]
Clinical Presentation
The classic history is days to weeks of polyuria, polydipsia, and weight loss, culminating in vomiting, abdominal pain, lethargy, and deep breathing. In a child not yet known to have diabetes, the early symptoms are easily attributed to a urinary infection, gastroenteritis, or a chest infection, and the diagnosis is often made only when the child is visibly unwell. A high index of suspicion and a single finger-prick glucose are all that is needed to avoid the missed diagnosis. [1] [7]
On examination the child is dehydrated, often more so than they appear, because the intracellular fluid is preferentially lost. The hallmark signs are Kussmaul breathing — the deep, sighing respiration that blows off carbon dioxide to compensate for the acidosis — and the sweet, fruity smell of acetone on the breath. Tachycardia, dry mucous membranes, sunken eyes, and reduced skin turgor complete the picture, and in severe cases there is drowsiness progressing to coma. [1] [7]
Two presentations catch the unwary. The abdominal pain and vomiting of DKA can convincingly mimic a surgical abdomen or gastroenteritis, and the temptation to operate or to treat with anti-emetics alone must be resisted until the acidosis is corrected, after which the pain usually settles. In the young child, the presentation is more nonspecific — poor feeding, lethargy, and rapid breathing that may be mistaken for pneumonia or bronchiolitis — so the threshold to check a glucose in any unwell, dehydrated infant must be low. [1] [8]
Differential Diagnosis
The first question is whether the acidosis is really ketoacidosis. A high anion gap metabolic acidosis in a child has a short differential — lactic acidosis from sepsis or shock, inborn errors of metabolism, salicylate or other toxic ingestions, and uraemia — and the combination of hyperglycaemia with ketonaemia rapidly points to DKA. A blood ketone measurement resolves the question at the bedside, and a glucose distinguishes DKA from the starvation ketosis of a fasting, vomiting child, whose glucose is normal or low. [1] [7]
The second question is whether the hyperglycaemia is DKA or the hyperosmolar hyperglycaemic state, a distinct emergency with very high glucose and osmolality but minimal ketosis and acidosis, which is managed differently and is not the subject of this page. In practice the two can overlap, and a child with features of both needs the fluid caution of the hyperosmolar state combined with the insulin approach of DKA. The presence of significant ketoacidosis is what defines the child as being in DKA. [1]
The third question, once DKA is confirmed, is what precipitated it. Search for infection, ask specifically about insulin omission and pump problems, and in the adolescent consider psychosocial stress and disordered eating. Finding and treating the precipitant is part of the management and, in recurrent DKA, is often more important than the acute biochemistry. [1] [8]
Clinical & Bedside Assessment
The assessment runs in parallel with the start of treatment, because a child in moderate or severe DKA is a time-critical emergency. Begin with the airway, breathing, and circulation, weigh or estimate the weight, and assess the degree of dehydration and the conscious level using the Glasgow Coma Scale. A depressed conscious level at presentation is itself a warning sign and mandates the closest monitoring, because it may herald cerebral involvement. [1] [7]
Quantifying the dehydration guides the fluid plan, but clinical estimates are imprecise and tend to overestimate the deficit, which is dangerous because over-generous fluids are linked to cerebral oedema. The pragmatic approach recommended by ISPAD is to assume a moderate deficit of around 5 to 7 per cent in moderate to severe DKA rather than to chase a precise clinical percentage, and to correct it evenly over 48 hours. Weigh the child, document the neurological baseline, and set up hourly observations from the outset. [1] [2]
The most important part of the bedside assessment is what happens next, over the following hours. A structured monitoring chart tracks the hourly vital signs, the neurological status, the fluid balance, and the biochemistry, so that a rising blood pressure with a falling heart rate, a headache, or a drop in conscious level is caught the moment it appears. Cerebral oedema is a clinical diagnosis made at the bedside, not on a scan, and the child who is watched closely is the child who survives it. [1] [9]
Investigations
The diagnosis is confirmed with a small, focused set of tests. A blood glucose and a blood beta-hydroxybutyrate or urine ketone establish two arms of the triad, and a venous blood gas gives the pH and bicarbonate for the third and for grading severity. A venous gas is sufficient — an arterial sample adds nothing and hurts the child. Urea, electrolytes, and creatinine establish the potassium, the sodium, and the degree of prerenal impairment, and the corrected sodium helps track the osmolar changes during treatment. [1] [7]
Beyond the diagnostic set, the investigations serve two purposes: monitoring and finding the cause. Monitoring means hourly bedside glucose and beta-hydroxybutyrate, and electrolytes and a blood gas every one to two hours initially, so that the potassium and the pace of correction are tracked in real time. The search for a precipitant means a careful clinical assessment for infection, with cultures and other tests directed by the history rather than sent reflexively, and a low threshold for a source that is driving the ketoacidosis. [1] [8]
Reading the numbers as they change
The blood glucose falls first and fastest, but it is the closing of the anion gap and the clearance of beta-hydroxybutyrate that signal true resolution, not the glucose alone. Bedside ketone monitoring lets you watch the acidosis resolve directly and is more responsive than the venous gas. A persistently high anion gap despite a normalising glucose means insufficient insulin or an unresolved precipitant, not a reason to stop insulin — instead, add dextrose to the fluids and keep the insulin running to switch off ketogenesis. Beware the hyperchloraemic acidosis of large-volume saline, which lowers the bicarbonate without any ongoing ketosis and does not need more insulin. [1] [7]
Management — Resuscitation
Resuscitation in DKA is deliberately restrained, because the same fluids that save a shocked child can harm the brain if given too fast. The child who is genuinely shocked — with poor peripheral perfusion, prolonged capillary refill, and hypotension — receives a cautious bolus of 10 millilitres per kilogram of isotonic saline, repeated only if shock persists, and reassessed after each. The great majority of children in DKA are dehydrated but not shocked, and they do not need a fluid bolus at all; they need the steady rehydration of the maintenance-plus-deficit regimen. [1] [2]
The cardinal rules of the first hour are two. Do not start insulin until fluid resuscitation has begun, because insulin given into a hypovolaemic, hypokalaemic child causes a dangerous drop in glucose and potassium and a sudden osmotic shift. And never give an insulin bolus — the infusion runs at a fixed low rate. These two rules, together with the cautious fluid approach, are the safety core of the whole protocol and are the points most rewarded in an exam. [1] [6]
[1] [6]The PECARN FLUID trial settled a long-running anxiety about fluids. In a large randomised trial, neither the rate of fluid administration nor the sodium content of the fluid meaningfully affected neurological outcome, and there was no signal that faster rehydration caused more brain injury within the ranges tested. This reassures clinicians that a sensible, moderate fluid regimen is safe, while the historical caution about avoiding grossly excessive fluids and over-rapid osmolar change still stands. [2]
Management — Definitive & Stepwise
The fluid plan is the backbone. After any resuscitation bolus, calculate the maintenance requirement and add the estimated deficit, then give the total evenly over 48 hours using an isotonic fluid such as 0.9 per cent saline with added potassium. Spreading the deficit over two days rather than one is the deliberately slow approach that avoids rapid osmolar shifts. As the glucose falls, the fluid is changed to include dextrose so that the insulin can keep running to clear the ketones without causing hypoglycaemia. [1] [2]
Insulin is the treatment that actually reverses the ketoacidosis, and its job is to switch off ketogenesis, not merely to lower the glucose. It runs as a fixed continuous infusion of 0.05 to 0.1 units per kilogram per hour, begun an hour or two after fluids, and it is not stopped when the glucose falls — instead dextrose is added to the fluids to allow the insulin to continue until the acidosis has cleared. A randomised trial found that a lower rate of 0.05 units per kilogram per hour was as effective as the standard 0.1 for resolving acidosis while causing fewer episodes of hypoglycaemia and hypokalaemia, supporting the lower end of the range in many children. [6] [1]
The ISPAD DKA protocol — the stepwise sequence
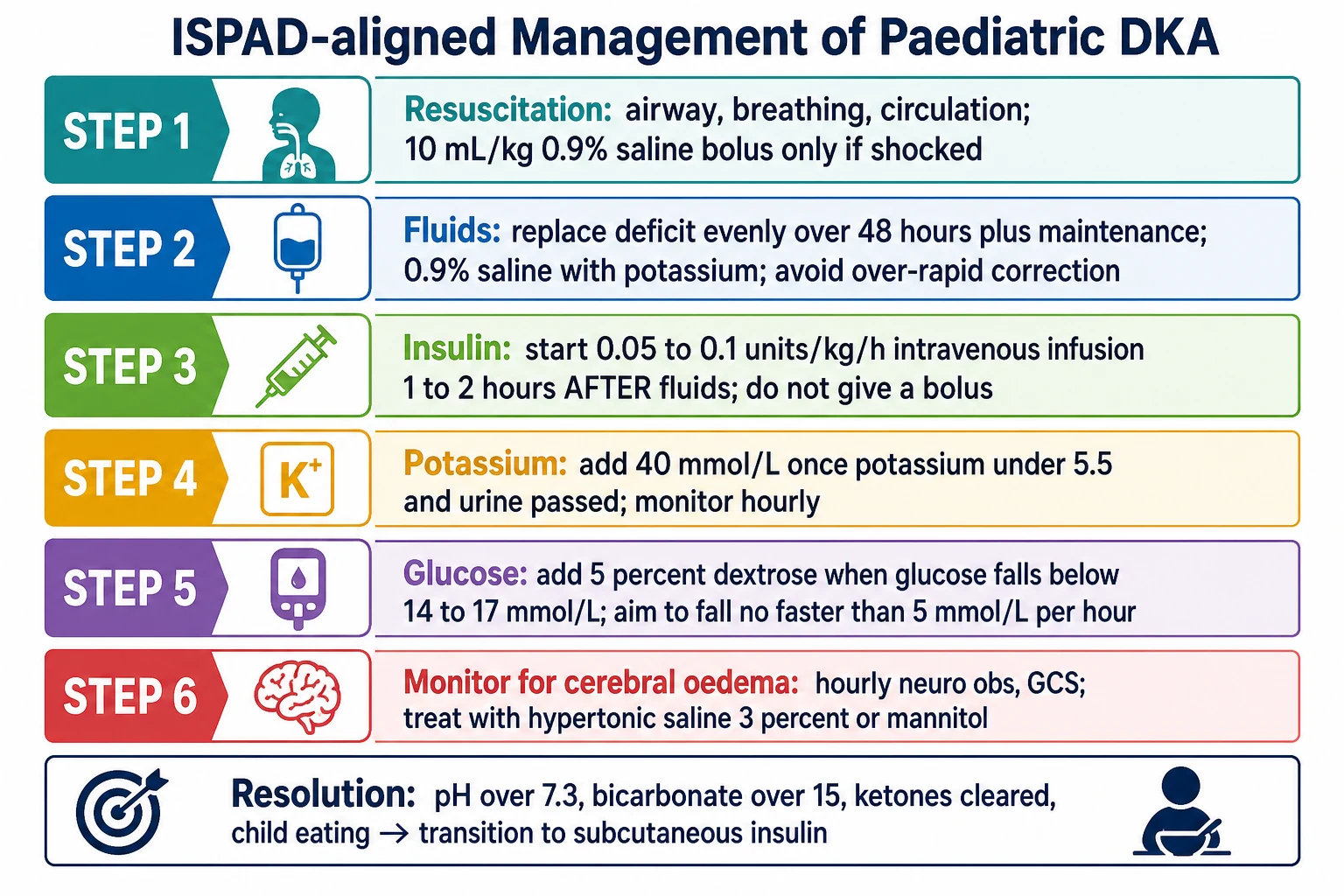
Resuscitate: ABC, and a 10 mL/kg isotonic saline bolus only if shocked; most children need no bolus.
Fluids: give maintenance plus the estimated deficit evenly over 48 hours with isotonic saline.
Potassium: add 40 mmol/L once potassium is below 5.5 mmol/L and the child has passed urine.
Insulin: start 0.05–0.1 units/kg/h by infusion 1–2 hours after fluids; never a bolus.
Glucose: add 5% dextrose once glucose falls below 14–17 mmol/L, keeping insulin running.
Monitor: hourly neuro obs and glucose, and gases and electrolytes every 1–2 hours; watch for cerebral oedema.
Potassium replacement follows the physiology set out above. Once the serum potassium is below 5.5 millimoles per litre and the child has passed urine, potassium is added to the fluids at 40 millimoles per litre, and it is monitored hourly because insulin will drive it down. Glucose is managed by adding 5 per cent dextrose to the fluid once the blood glucose falls below roughly 14 to 17 millimoles per litre, and by aiming for a controlled fall in glucose of no more than about 5 millimoles per litre per hour, so that the osmolality does not drop abruptly. [1] [7]
Bicarbonate is almost never given, because it does not speed recovery, worsens intracellular acidosis and hypokalaemia, and was identified as an independent risk factor for cerebral oedema. It is reserved for the rare child with life-threatening hyperkalaemia or profound acidosis compromising cardiac function, and even then only with specialist input. The resolution of DKA is defined biochemically, and only when the acidosis has cleared is the child ready to move off the intravenous protocol. [3] [1]
Specific Subtypes & Scenarios
New-onset DKA is the commonest scenario in the exam and combines an acute emergency with a life-changing diagnosis. The acute management is identical to any DKA, but the aftercare is different: the family needs a full diagnosis of type 1 diabetes, structured education in insulin, glucose monitoring, and sick-day rules, and psychological support for a diagnosis they did not see coming. The transition from the intravenous protocol to subcutaneous insulin is the bridge into their new life with diabetes. [1] [8]
The child on an insulin pump is a distinct scenario, because the pump delivers only rapid-acting insulin and provides no long-acting depot. A pump failure — an occluded cannula, a failed site, or an empty reservoir — removes all insulin within a couple of hours and can precipitate DKA quickly, sometimes with a glucose that is only modestly raised. The teaching point is that unexplained ketosis in a pump user is a pump failure until proven otherwise, and the response is to give insulin by pen or syringe and revert to injections while the problem is sorted. [1]
Euglycaemic DKA — ketoacidosis with a near-normal glucose — is the trap that catches clinicians who anchor on the glucose. It occurs in the child who has kept up some carbohydrate or partial insulin, in pregnancy, and with newer glucose-lowering agents in older adolescents. The lesson is that the diagnosis rests on the ketones and the acidosis, and the treatment still requires insulin, delivered alongside dextrose from the outset because the glucose is already low. Recurrent DKA in an adolescent is a red flag for insulin omission, mental health difficulty, or an eating disorder, and it demands a psychosocial response rather than only a biochemical one. [1] [8]
Complications & Pitfalls
Cerebral oedema is the complication that dominates the topic, because it is the leading cause of death and disability in paediatric DKA. It typically appears four to twelve hours into treatment, often just as the biochemistry is improving, and it presents with headache, a falling conscious level, irritability, incontinence, and the Cushing signs of a rising blood pressure with a falling heart rate. It is a clinical diagnosis, treated immediately with hypertonic saline or mannitol, a reduced fluid rate, and head elevation, and it must not wait for imaging. The Marcin analysis showed that outcome depends heavily on how promptly it is recognised and treated. [3] [9]
[1] [9]The other complications are largely iatrogenic and preventable. Hypokalaemia from insulin without adequate potassium replacement can cause arrhythmia, and hypoglycaemia from failing to add dextrose as the glucose falls interrupts the insulin that is clearing the ketones. Hyperchloraemic acidosis from large-volume saline lowers the bicarbonate and can be mistaken for persisting ketoacidosis, leading to unnecessary insulin. Aspiration in the drowsy vomiting child, and venous thrombosis associated with central lines and dehydration, complete the list of avoidable harms. [1] [7]
The pitfalls to name explicitly are the errors that recur in real practice: giving an insulin bolus, starting insulin before fluids, over-estimating the deficit and giving too much fluid too fast, stopping insulin when the glucose falls instead of adding dextrose, and forgetting that a normal potassium hides a large deficit. Each of these is a direct cause of harm, and avoiding them is what the protocol is designed to do. [1] [6]
Prognosis & Disposition
For the great majority of children, the prognosis of an episode of DKA is excellent: the acidosis resolves within a day or so of starting treatment, and the child recovers fully. The mortality of paediatric DKA is low overall, but it is dominated by cerebral oedema, which carries a substantial risk of death or permanent neurological disability when it occurs. The outlook of an individual episode therefore turns almost entirely on whether cerebral oedema develops and how quickly it is treated. [1] [4]
The disposition depends on severity and on the resources available. A child in severe DKA, a very young child, or any child with a depressed conscious level or signs of cerebral involvement belongs in an intensive care or high-dependency setting, and in a rural or remote hospital this means early discussion with a retrieval service. Milder episodes can be managed on a ward with a strict monitoring protocol and staff experienced in DKA. The transition to subcutaneous insulin, once the child has met the resolution criteria and can eat, is the step down from the emergency phase. [1] [8]
There is also a longer-term prognostic thread. The cognitive follow-up from the FLUID trial cohort found that a single episode of DKA, and repeated episodes, are associated with subtle reductions in cognitive function in children, especially in those with new-onset disease, underlining that DKA is not entirely benign even when the child appears to recover fully. This adds weight to prevention — earlier diagnosis, good sick-day management, and avoiding recurrent episodes — as part of the long-term care of the child with diabetes. [10] [1]
Special Populations
The very young child is the highest-risk group. Infants and toddlers present nonspecifically, are harder to assess for dehydration and conscious level, and carry the greatest risk of cerebral oedema, so they need the most cautious fluid regimen and the closest neurological monitoring. New-onset diabetes is over-represented in this group because the diagnosis is easily missed, and the threshold to check a glucose in any unwell, dehydrated infant with rapid breathing must be low. [1] [3]
The adolescent with recurrent DKA is a different challenge that is more psychosocial than biochemical. Repeated episodes usually reflect insulin omission driven by mental health difficulty, family stress, disordered eating, or the burden of living with a demanding chronic disease, and treating the acute episode without addressing the cause simply sets up the next admission. The response is a multidisciplinary one, involving diabetes education, psychology, and social support, and it should be built into the discharge plan of every recurrent presentation. [1] [8]
Access and equity shape outcomes in identifiable groups. Children in rural and remote areas, and in Aboriginal, Torres Strait Islander, Māori and Pacific communities, and in families facing socioeconomic disadvantage or who are migrants, refugees or asylum seekers, present later and more often in severe DKA because of barriers to recognition and care. The response is culturally safe education, interpreter support, strengthened primary-care awareness, and clear pathways to specialist and retrieval services, so that the child reaches treatment before the acidosis becomes severe. [1]
Evidence, Guidelines & Regional Differences
The ISPAD Clinical Practice Consensus Guidelines are the global reference for paediatric DKA, and the 2022 edition, updating the 2018 version, sets the diagnostic criteria, the severity grading, the fluid and insulin regimen, and the cerebral-oedema guidance that this page follows. The earlier ESPE/LWPES consensus established much of the framework that these guidelines refined. Together they provide a consistent, evidence-based approach that is used across Australia, New Zealand, the United Kingdom, Europe, and North America. [1] [7] [8]
The evidence base has two landmark contributions. The Glaser case-control study defined the risk factors for cerebral oedema and the association with bicarbonate therapy, shaping decades of cautious practice, and the Marcin analysis linked outcome to the speed of recognition and treatment. The PECARN FLUID trial then tested the central fear directly and found that fluid rate and sodium content did not affect neurological outcome within the ranges studied, reassuring clinicians that a sensible fluid regimen is safe and shifting some of the historical anxiety. [3] [2] [9]
[1]The residual controversies are narrow. The optimal insulin rate has moved toward the lower end of the range for many children on the strength of the Nallasamy trial, the precise fluid regimen is now known to matter less than once feared thanks to PECARN, and the role of newer glucose-lowering agents in euglycaemic DKA is an emerging issue in older adolescents. The guideline message is stable and consistent: diagnose the triad, correct it slowly, protect the potassium, and watch the brain. [6] [2] [1]
Exam Pearls
The safety core of the DKA protocol — never forget these
The fellowship candidate who states the triad, grades the severity, delivers the fluids-before-insulin sequence with the correct insulin rate and the potassium logic, and — above all — recognises and treats cerebral oedema at the bedside without waiting for imaging has the full mark. The deeper candidate adds the prevention thread: earlier recognition of new-onset diabetes, sick-day education, and a psychosocial response to recurrent DKA, framed by the knowledge that even a well-treated episode carries a small cognitive cost. [1] [10]
References
- [1]Glaser N, Fritsch M, Priyambada L, et al. ISPAD clinical practice consensus guidelines 2022: Diabetic ketoacidosis and hyperglycemic hyperosmolar state Pediatr Diabetes, 2022.PMID 36250645
- [2]Kuppermann N, Ghetti S, Schunk JE, et al. Clinical Trial of Fluid Infusion Rates for Pediatric Diabetic Ketoacidosis N Engl J Med, 2018.PMID 29897851
- [3]Glaser N, Barnett P, McCaslin I, et al. Risk factors for cerebral edema in children with diabetic ketoacidosis. The Pediatric Emergency Medicine Collaborative Research Committee of the American Academy of Pediatrics N Engl J Med, 2001.PMID 11172153
- [4]Edge JA, Hawkins MM, Winter DL, et al. The risk and outcome of cerebral oedema developing during diabetic ketoacidosis Arch Dis Child, 2001.PMID 11420189
- [5]Muir AB, Quisling RG, Yang MC, et al. Cerebral edema in childhood diabetic ketoacidosis: natural history, radiographic findings, and early identification Diabetes Care, 2004.PMID 15220225
- [6]Nallasamy K, Jayashree M, Singhi S, et al. Low-dose vs standard-dose insulin in pediatric diabetic ketoacidosis: a randomized clinical trial JAMA Pediatr, 2014.PMID 25264948
- [7]Dunger DB, Sperling MA, Acerini CL, et al. ESPE/LWPES consensus statement on diabetic ketoacidosis in children and adolescents Arch Dis Child, 2004.PMID 14736641
- [8]Wolfsdorf JI, Glaser N, Agus M, et al. ISPAD Clinical Practice Consensus Guidelines 2018: Diabetic ketoacidosis and the hyperglycemic hyperosmolar state Pediatr Diabetes, 2018.PMID 29900641
- [9]Marcin JP, Glaser N, Barnett P, et al. Factors associated with adverse outcomes in children with diabetic ketoacidosis-related cerebral edema J Pediatr, 2002.PMID 12461495
- [10]Ghetti S, Kuppermann N, Rewers A, et al. Cognitive Function Following Diabetic Ketoacidosis in Children With New-Onset or Previously Diagnosed Type 1 Diabetes Diabetes Care, 2020.PMID 32962981