Paeds · endocrinology-diabetes-and-growth
Endocrine emergencies: integrated approach
Also known as Endocrine emergencies · Paediatric endocrine crisis · Endocrine emergency integrated approach · DKA adrenal crisis thyroid storm · Acute endocrine failure · Endocrine collapse
Fellowship guide to the integrated approach to paediatric endocrine emergencies: the shared recognition and resuscitation framework that unifies DKA, adrenal crisis, thyroid storm and the sodium-water disorders (SIADH and diabetes insipidus), the bedside triage with glucose, blood gas and electrolytes, the empiric life-saving treatments that cannot wait for confirmatory endocrine tests, and the cross-cutting pitfalls of missed cortisol, missed glucose and missed sodium.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The idea that organises this page is deceptively simple. Every endocrine emergency is the same shape of problem seen from a different angle: a hormone axis has failed, the body's compensation has run out, and the child now sits in a metabolic and haemodynamic collapse that only the missing or blocked hormone can reverse. The resuscitation is also the same shape: secure the airway, get intravenous access, check the bedside glucose and the blood gas, send the electrolytes, and then give the empiric life-saving therapy before the confirmatory endocrine test returns. What changes from emergency to emergency is only which hormone you reach for — insulin, hydrocortisone, a beta-blocker with an antithyroid drug, or hypertonic saline. [1] [5]
This page synthesises the shared approach across the four dominant paediatric endocrine emergencies, linking to the dedicated leaves for diabetic ketoacidosis and the hyperosmolar hyperglycaemic state, adrenal insufficiency and adrenal crisis, hyperthyroidism and Graves disease, and diabetes insipidus and SIADH. It does not repeat their full pathways. The integrated leaf teaches what those emergencies share: the recognition, the resuscitation, the communication, the ICU escalation and the cross-cuting pitfalls that catch the registrar who knows each disease separately but cannot see the pattern. [1] [12]
Overview & Definition
A child who arrives vomiting, dehydrated and breathless, or drowsy with a low blood pressure, or seizing with an abnormal sodium — that is the opening scene of a paediatric endocrine emergency. The condition is an acute, potentially life-threatening failure of a hormone axis, where the missing or excess hormone produces a metabolic and haemodynamic collapse, and its replacement or blockade is the immediate life-saving treatment. [1] [5]
The first thing to understand is that these emergencies do not announce themselves by name. The child does not say "I am in adrenal crisis"; the child says "I feel sick and I cannot stop vomiting", and the nurse says "the blood pressure is not coming up". The endocrine diagnosis lives in the pattern of the blood results, and the job of the clinician is to reach for the bedside glucose and the electrolytes early enough that the pattern becomes visible before the child arrests. That is the heart of the integrated approach: the endocrine emergency is a metabolic pattern hiding inside a sick child, and the bedside tests are the torch that finds it. [3] [5]
Classification
The fastest way to classify a paediatric endocrine emergency is by the axis that fails and the metabolic signature it leaves, because the signature is what you see on the bedside glucose and the first blood gas. The figure below maps the four dominant emergencies onto the triage tool that splits them within minutes. [1] [5]
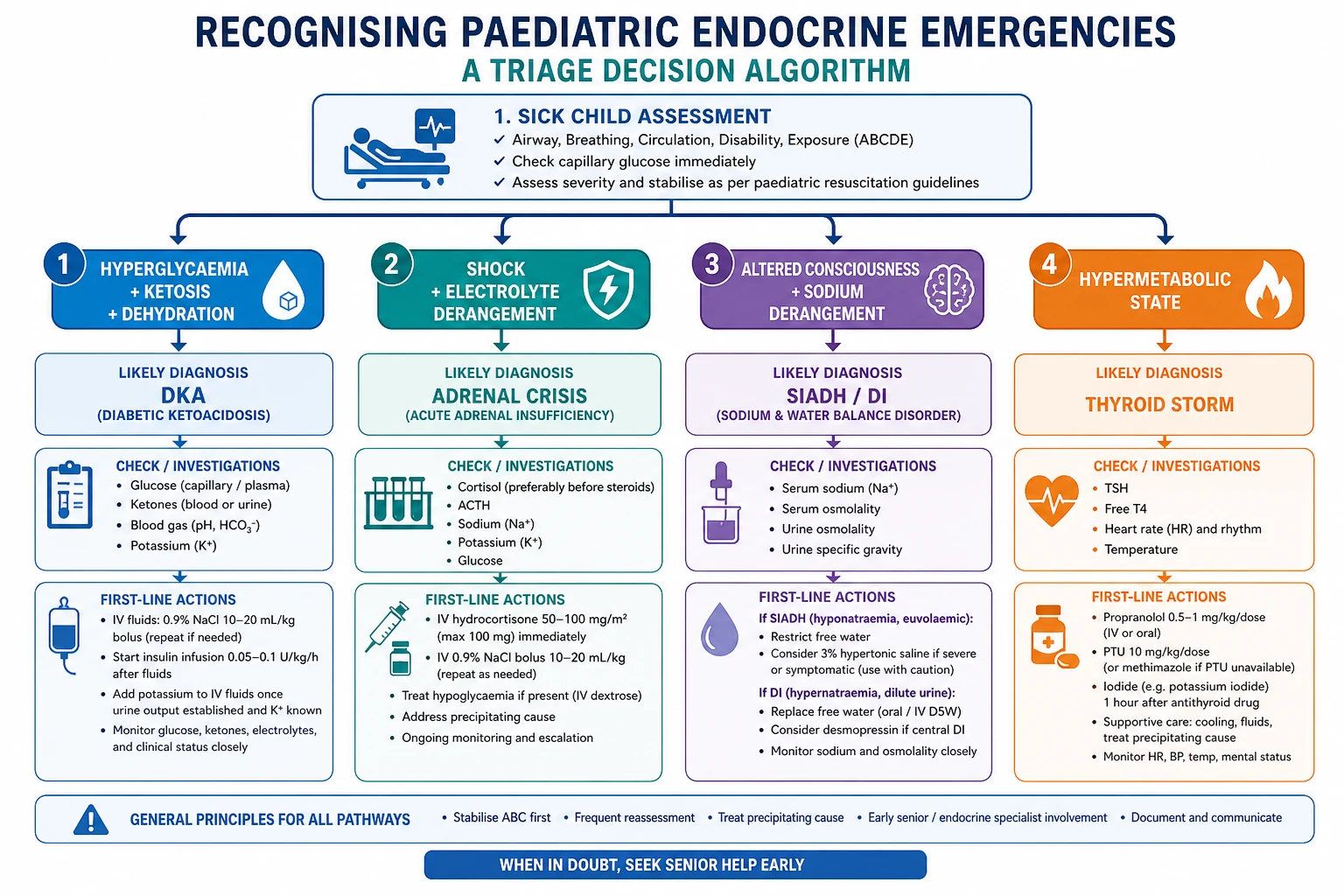
DKA
- Insulin deficiency: hyperglycaemia, ketones, metabolic acidosis
- Polyuria, weight loss, vomiting, Kussmaul breathing, dehydration
- Cerebral oedema risk: 0.5–1% of episodes, 20–40% mortality
- Treat with fluids + insulin infusion 0.05–0.1 U/kg/hr (never a bolus)
Adrenal crisis
- Cortisol deficiency: shock, hypoglycaemia, hyponatraemia ± hyperkalaemia
- Fluids unresponsive shock, vomiting, abdominal pain, collapse
- Primary loses aldosterone too (high K+); secondary keeps it (normal K+)
- Treat with IV hydrocortisone 50–100 mg (child) or 25 mg (infant) stat
Thyroid storm
- Thyroid hormone excess: hyperthermia, tachyarrhythmia, altered consciousness
- Goitre, known or undiagnosed hyperthyroidism, precipitant trigger
- Rare in children but carries significant mortality
- Block with beta-blocker + antithyroid drug + steroid + cooling
SIADH / DI
- ADH dysregulation: water balance failure and sodium derangement
- SIADH: euvolaemic, low sodium, seizure risk, often CNS trigger
- DI: hypovolaemic, high sodium, dilute urine, often post-pituitary surgery
- SIADH seizure: 3% saline 2 mL/kg; DI: rehydrate + desmopressin
The classification matters because it decides which empiric treatment you reach for in the first hour. A high glucose with a metabolic acidosis sends you down the DKA pathway — fluids and an insulin infusion. A low glucose sends you straight for intravenous dextrose. A low sodium with a high or normal potassium and a child in shock sends you to the adrenal-crisis pathway — hydrocortisone and saline. A low sodium with a normal potassium and a seizing child sends you to the SIADH pathway — hypertonic saline. A high sodium with dilute urine sends you to diabetes insipidus. The metabolic signature is the compass. [1] [5]
Epidemiology & Risk Factors
Diabetic ketoacidosis is the commonest paediatric endocrine emergency, and the reason it is so common is that the diabetes is often not yet diagnosed. Roughly 15 to 70 per cent of children present in DKA at the onset of type 1 diabetes, with the highest rates in the youngest children and in those whose polyuria, weight loss and vomiting have been attributed to a virus or to gastroenteritis for days before the metabolic collapse arrives. In established diabetes, DKA recurs with intercurrent illness, insulin omission, or pump failure, and the adolescent who stops taking insulin is the classic recurring-presentation patient. [1] [2]
The reason every candidate must know DKA inside out is cerebral oedema. It complicates roughly 0.5 to 1 per cent of paediatric DKA episodes, but when it happens it carries a mortality of 20 to 40 per cent, and it is the single leading cause of diabetes-related death in children. The children at highest risk are those under five, those with severe acidosis or a very high glucose at presentation, those with a low corrected sodium, and those who have received bicarbonate or very rapid fluid resuscitation. The modifiable risk factors — fluids, bicarbonate, insulin bolus — are the things the registrar controls, which is why the DKA fluid and insulin protocol is one of the highest-yield topics in the written paper. [3] [13]
ENDO
Treat empirically before confirmatory endocrine tests return — the test confirms but does not resuscitate
Bedside glucose, blood gas and electrolytes split the four emergencies within minutes
The leading cause of diabetes death in children: headache or altered consciousness during DKA treatment is the sign
Each emergency is one hormone failing — insulin, cortisol, thyroid hormone, or ADH — and one targeted treatment reverses it
Adrenal crisis is less common than DKA but just as lethal when missed. Roughly 5 to 10 per cent of children with chronic adrenal insufficiency have a crisis each year, with infections, gastrointestinal illness with vomiting, surgery and missed or under-dosed replacement as the recurring precipitants. The children most at risk are those with known adrenal insufficiency or congenital adrenal hyperplasia who meet a stressor without the stress dose, and those with undiagnosed autoimmune Addison disease or glucocorticoid-induced suppression who present in crisis as the first manifestation. [5]
Thyroid storm is rare in children — the paediatric systematic review found only case reports and small case series — but it carries a significant mortality and it is the reason every candidate must know the blocking regimen. The sodium-water emergencies are common on the ward but rarely become emergencies in themselves; the emergency is the symptomatic hyponatraemia that seizes, or the hypernatraemic dehydration that collapses, and both share the vulnerability of the brain to rapid sodium change. [7] [10]
Pathophysiology
Every endocrine emergency is a hormone-axis failure, and the body's compensatory response to the missing or excess hormone is what you see at the bedside. The mechanism differs for each emergency, but the shared principle — one hormone, one axis, one collapse — is the mental model that makes the integrated approach work. The figure below shows what happens to the body when each axis fails. [1] [5]
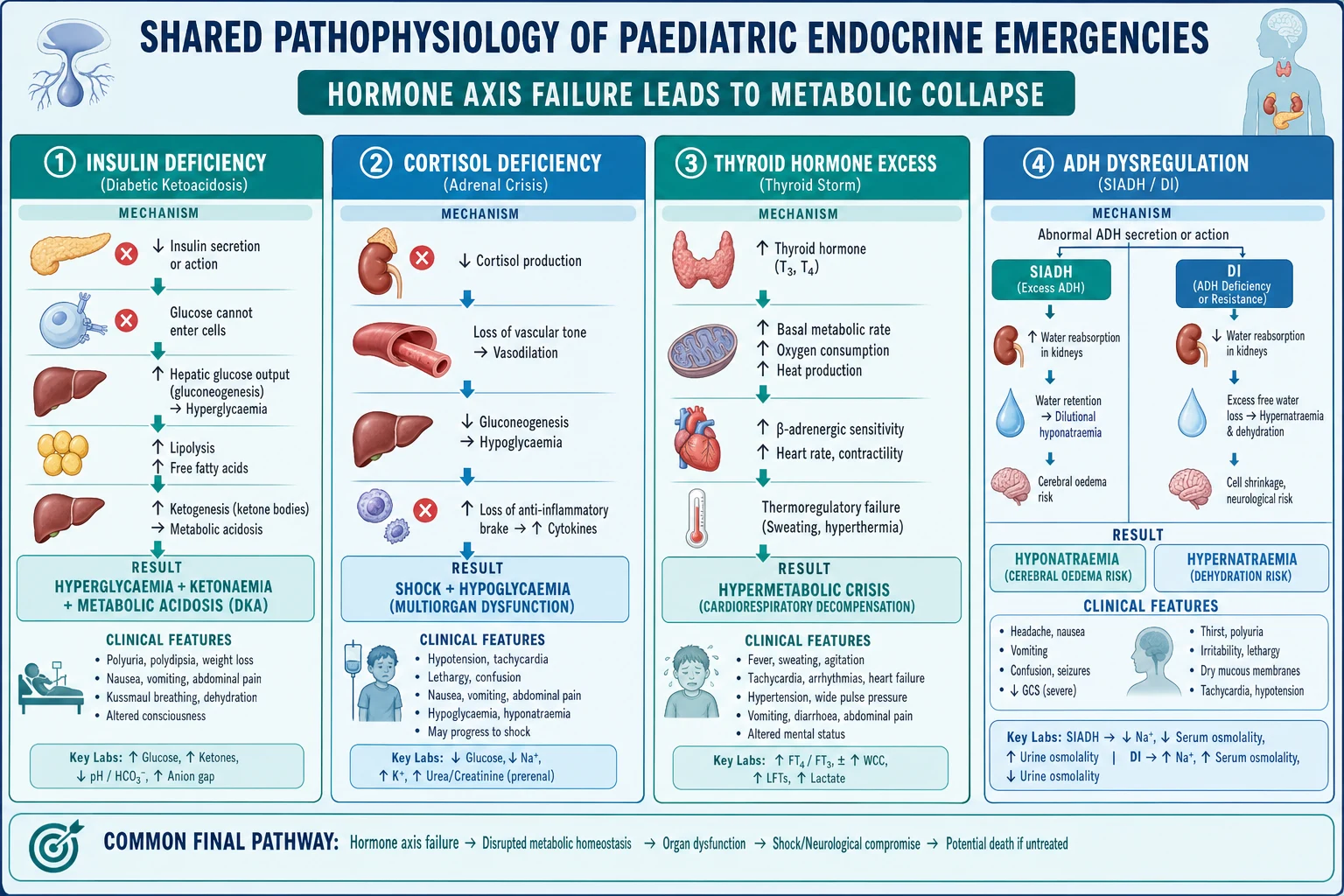
In diabetic ketoacidosis the problem is insulin deficiency. Without insulin, glucose cannot enter the cells, so it accumulates in the blood and spills into the urine, dragging water and electrolytes with it through osmotic diuresis — that is the dehydration and the electrolyte loss. The body, starved of glucose inside the cells, switches to fat breakdown, and unopposed lipolysis generates ketone bodies that drive a high-anion-gap metabolic acidosis. The counter-regulatory hormones — glucagon, cortisol, adrenaline and growth hormone — accelerate the cycle, and the deep sighing breathing (Kussmaul) is the lungs trying to blow off the acid. The whole thing spirals because the missing hormone, insulin, is the only thing that can turn it off. [1] [2]
In adrenal crisis the problem is cortisol deficiency, and what you see is what cortisol was holding together. Cortisol sensitises the blood vessels to catecholamines, so without it the vascular tone collapses and the child becomes hypotensive — that is the shock. Cortisol drives gluconeogenesis, so without it the child cannot maintain a blood glucose — that is the hypoglycaemia. And cortisol is an anti-inflammatory brake, so without it an intercurrent infection runs unchecked. In primary adrenal failure the child also loses aldosterone, so sodium is wasted and potassium retained — that is the hyperkalaemia that makes the primary crisis biochemically loud. [5] [6]
In thyroid storm the problem is the opposite of deficiency: too much thyroid hormone drives a hypermetabolic crisis. The body's thermoregulation fails (the high fever), the cardiac output decompensates (the severe tachycardia or atrial arrhythmia), and the central nervous system runs out of control (the agitation, delirium or coma). It is almost always triggered — by infection, surgery, non-adherence with antithyroid medication, or iodine load — and the trigger and the hormone excess together produce the storm. [7]
In the sodium-water emergencies the problem is antidiuretic hormone (ADH, also called vasopressin). In SIADH there is too much ADH, so the kidneys retain free water and the sodium is diluted — the brain swells and the child can seize. In diabetes insipidus there is too little ADH, so the kidneys lose free water and the sodium concentrates — the brain dehydrates. Both share a single vulnerability: the brain adapts to a sodium level over hours to days, and a rapid change — in either direction — is what causes the neurological injury. That is why the treatment rule for both is the same: correct slowly. [9] [10]
Clinical Presentation
The presentation of an endocrine emergency is the presentation of a sick child with a metabolic clue, and the clue is what separates the endocrine emergency from sepsis, gastroenteritis or an acute abdomen. Start with the paediatric assessment triangle: the child who looks toxic, who is tachycardic, tachypnoeic, peripherally shut down, or who has an altered conscious state, is your entry into the resuscitation room, and the bedside glucose and blood gas are your first move. [1] [3]
The DKA presentation runs from the chronic to the acute. Over days to weeks the child has polyuria, polydipsia and weight loss — the classic osmotic triad of new diabetes — and then over hours the vomiting, abdominal pain, deep sighing breathing, ketotic breath and dehydration arrive as the metabolic acidosis takes hold. In the young child the diabetes is often undiagnosed, so the story is a "virus" or "gastroenteritis" that has suddenly got worse, and the deep breathing is attributed to pneumonia. Altered consciousness is a late and dangerous sign, and it is the sign that places the child on the cerebral-oedema watch. [1] [14]
The adrenal crisis presentation is shock that does not respond to fluids, with vomiting and abdominal pain severe enough to mimic an acute abdomen, and the biochemical triad of hyponatraemia, hyperkalaemia (in primary disease) and hypoglycaemia. The child may be hyperpigmented (primary disease) or pale (secondary), and the history of recent or current glucocorticoid therapy is the single most useful clue in secondary disease. In children the hypoglycaemia is often the dominant feature and may present as seizures or reduced consciousness before the shock is obvious. [5] [6]
The thyroid storm presentation is high fever, severe tachycardia or an atrial arrhythmia, heart failure, and agitation, delirium or coma. There is usually a goitre, and there is almost always a trigger — infection, surgery, radioactive iodine, or non-adherence with antithyroid medication. The child looks hypermetabolic and toxic, and the cardiovascular instability is the immediate threat. [7]
The SIADH presentation is a child who is euvolaemic (not dehydrated, not oedematous) with a falling sodium, developing headache, nausea, then confusion, seizure or coma. The trigger is usually a central nervous system insult — meningitis, head injury, post-neurosurgery — or a respiratory infection. The diabetes insipidus presentation is the opposite: a child who is dehydrated with a high sodium, producing large volumes of dilute urine, often in the context of recent pituitary surgery or a brain insult. [9] [10]
Differential Diagnosis
The differential of a paediatric endocrine emergency is the differential of the sick child — sepsis, gastroenteritis, an acute abdomen, a metabolic disorder, a seizure — and sepsis sits at the top of every list because it coexists with and mimics every endocrine emergency. The discriminating tool is not the clinical picture alone but the metabolic pattern on the bedside tests, and the key habit is to cover sepsis regardless while you work up the endocrine cause. [1] [5]
The triage logic runs like this. A high glucose with a high-anion-gap metabolic acidosis and ketones is DKA until proven otherwise, but a septic child can also be hyperglycaemic, so the ketones and the gas close the gap. A low glucose with a sick child is hypoglycaemia — reach for the dextrose and then look for the cause (insulin, oral hypoglycaemic, adrenal insufficiency, sepsis, inborn error). A low sodium with a normal or high potassium and shock is adrenal crisis — give hydrocortisone empirically. A low sodium with a normal potassium and a seizing child is SIADH or cerebral salt wasting — give hypertonic saline for the seizure and then sort the two. A high sodium with dilute urine is diabetes insipidus. [9] [10]
The cerebral-oedema differential in DKA is short and urgent. Any child in DKA who develops a headache, behavioural change, incontinence, a falling heart rate with a rising blood pressure (Cushing response), a pupillary change or a falling Glasgow Coma Scale has cerebral oedema until proven otherwise. Do not wait for a CT scan to treat — give mannitol or hypertonic saline, reduce the fluid rate, and intubate if the airway or consciousness is threatened. The natural history and radiographic findings (Muir 2004) showed that the earliest signs are subtle and that delay is the preventable cause of death. [14] [13]
The SIADH differential is between syndrome of inappropriate antidiuretic hormone and cerebral salt wasting, because the treatment differs. SIADH is euvolaemic or slightly hypervolaemic with a normal or high urine sodium; cerebral salt wasting is hypovolaemic with a high urine sodium and features of dehydration. SIADH is treated with fluid restriction; cerebral salt wasting is treated with saline and sometimes fludrocortisone. The practical point is that both present with hyponatraemia, and the seizure is treated the same way (hypertonic saline), but the maintenance differs. [10]
Clinical & Bedside Assessment
The bedside assessment of a suspected endocrine emergency runs on two tracks at once: judge how sick the child is now, and gather the clues that localise the failing axis. Start with the airway, breathing and circulation, because every endocrine emergency can become a shock state. Capillary refill, heart rate, blood pressure and conscious level, with a bedside glucose, tell you whether you are resuscitating or investigating first. [1] [3]
The focused examination looks for the endocrine clues that point to the specific axis. Look at the skin for hyperpigmentation (palmar creases, gum margins, old scars in primary adrenal insufficiency), vitiligo (autoimmune clustering), and acanthosis nigricans (insulin resistance). Look at the neck for a goitre (hyperthyroidism). Look at the growth chart — weight loss in new diabetes, faltering growth in chronic adrenal insufficiency, and the acceleration of precocious puberty. Ask the insulin history in the diabetic child (omission, pump failure, intercurrent illness) and the steroid history in the suspected secondary adrenal child (oral, inhaled, nasal, topical, and when it was stopped). [5] [6]
In DKA the serial Glasgow Coma Scale and neurological observation are mandatory, because the first sign of cerebral oedema is a change in mental status — a headache, irritability, drowsiness — not a full neurological presentation. Check the Glasgow Coma Scale hourly, watch for the Cushing response (bradycardia with hypertension), and examine the pupils. A child whose corrected sodium is falling or whose mental status is changing is on the cerebral-oedema pathway and needs immediate intervention. [11] [14]
The synthesis is the most important skill. The problem representation — "a four-year-old with two weeks of polyuria, polydipsia and weight loss, now vomiting with deep sighing breathing, a glucose of 28 and a pH of 7.1" — is DKA. "A ten-year-old boy who stopped his oral steroid six weeks ago, now drowsy and hypoglycaemic with a normal potassium" is secondary adrenal crisis. "A fourteen-year-old girl with a goitre, a fever of 39.5, a heart rate of 160 and agitation" is thyroid storm. Name the pattern, then act on it. [1] [7]
Investigations
The first-hour investigation bundle for any suspected endocrine emergency is the same: bedside glucose, a venous blood gas (for pH, bicarbonate, base excess, and a rapid sodium and potassium), urea and electrolytes, and — depending on the pattern — ketones (beta-hydroxybutyrate), cortisol, ACTH, TSH, free T4, plasma and urine osmolality, urine sodium, and a septic screen. Draw the confirmatory endocrine tests before the empiric dose if you can, because one cortisol and one ACTH measured in the acute moment often settle the diagnosis, but never delay treatment to wait for them. [1] [6]
Interpret the DKA panel against the ISPAD diagnostic criteria: a blood glucose above 11 mmol per litre, a venous pH below 7.3 or a bicarbonate below 15 mmol per litre, and beta-hydroxybutyrate above 3 mmol per litre (or moderate ketonuria). The severity is graded by the pH and the bicarbonate: mild (pH 7.2 to 7.3), moderate (pH 7.1 to 7.2) and severe (pH below 7.1). The corrected sodium is tracked with every gas, and a falling corrected sodium is the cerebral-oedema red flag. [1] [11]
Interpret the adrenal panel against the primary-versus-secondary split. A cortisol drawn in the acute stress of a sick child that is low, with a high ACTH, confirms primary adrenal insufficiency; a low cortisol with a low or inappropriately normal ACTH confirms secondary disease. A random stress cortisol above 500 nanomoles per litre in a sick child effectively excludes adrenal insufficiency, so the test is as much about ruling out as ruling in. The 250-microgram cosyntropin stimulation test is the confirmatory standard for primary disease, done once the child is stable. [5] [6]
Interpret the sodium-water panel against the osmolality. In SIADH the plasma osmolality is low (below 275 mOsm per kg), the urine osmolality is inappropriately concentrated (above 100 mOsm per kg), and the urine sodium is above 40 mmol per litre, all in a euvolaemic child. In diabetes insipidus the plasma osmolality is high, the urine osmolality is inappropriately dilute (below 300 mOsm per kg), and the urine sodium is low. The two share a brain vulnerability, but the treatment is opposite. [9] [10]
Management — Resuscitation
The shared resuscitation principle for every paediatric endocrine emergency is the same: ABCDE, intravenous access, bedside glucose, blood gas and electrolytes, then treat the empiric life-saving therapy before the confirmatory endocrine tests return. The figure below maps the integrated algorithm and the empiric treatment for each emergency. [1] [5]
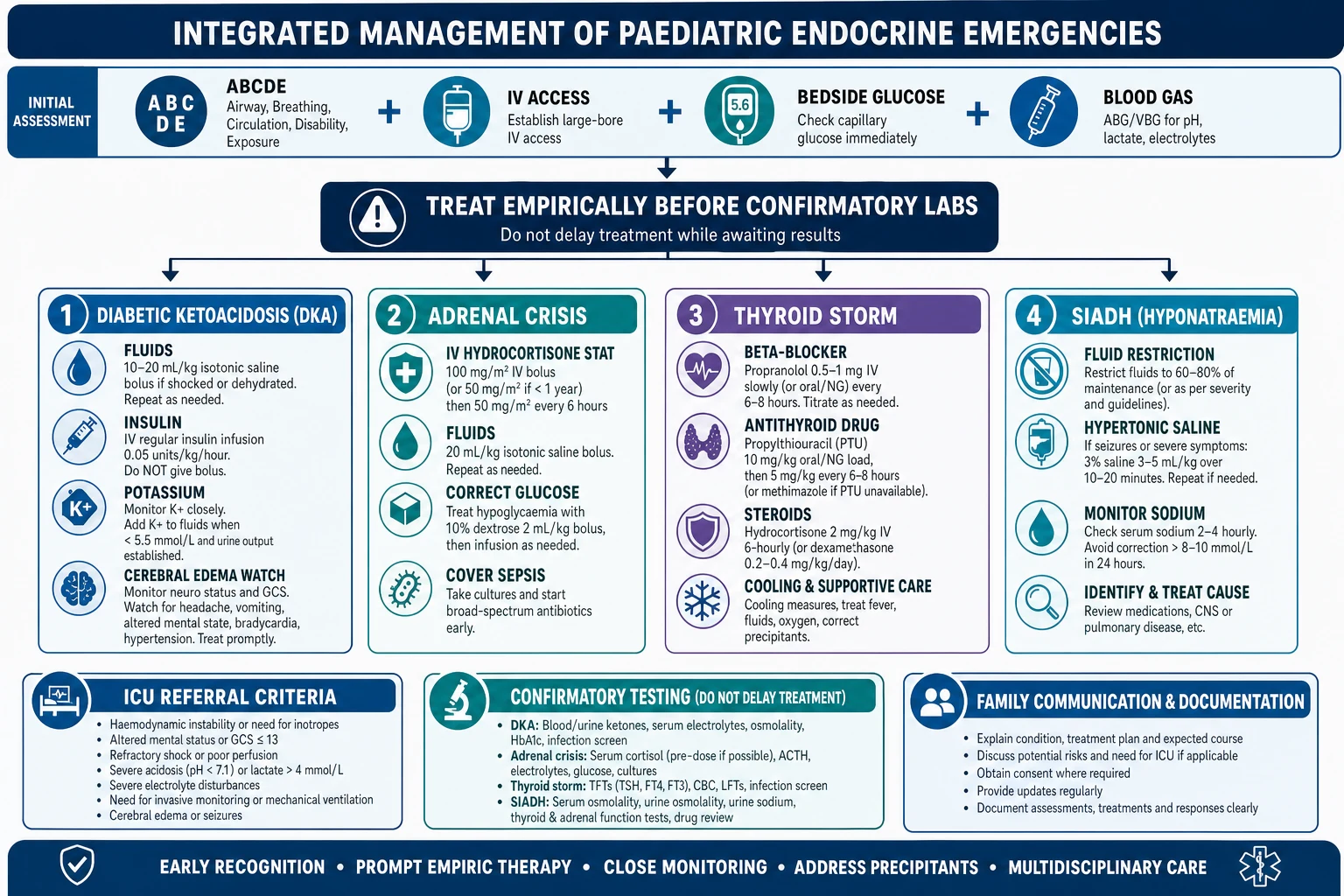
For DKA, resuscitate in three steps: fluids, insulin and potassium. Give a 10 to 20 mL per kg bolus of 0.9 per cent saline only if the child is in shock, then a structured fluid regimen that replaces the deficit plus maintenance minus the bolus over 36 to 48 hours. Start the insulin infusion at 0.05 to 0.1 units per kg per hour after the first fluid — never as a bolus, because a bolus causes dangerous hypokalaemia and increases cerebral-oedema risk. Add potassium (usually 40 mmol per litre in the maintenance fluid) once the serum level is known and the child is urinating, because insulin drives potassium into the cells. The PECARN factorial trial (Kuppermann 2018) showed no difference in cerebral injury by fluid rate or sodium content, but the principle of cautious, structured fluid remains the standard. [1] [4]
Empiric first-hour doses in paediatric endocrine emergencies
For adrenal crisis, resuscitate with three tracks at once: isotonic volume, parenteral hydrocortisone, and glucose and electrolyte correction while you treat the precipitant. Give 10 to 20 mL per kg of 0.9 per cent saline, repeated to perfusion, then rehydrate over the next day. Give parenteral hydrocortisone immediately — 50 to 100 mg for a child, 25 mg for an infant or neonate — then continue as 50 to 100 mg per square metre per 24 hours. Correct the hypoglycaemia with intravenous dextrose, and treat hyperkalaemia expectantly because it usually settles as volume, cortisol and aldosterone activity return. Cover sepsis with cultures and empiric antibiotics, because sepsis and adrenal crisis are clinically indistinguishable and often coexist. [5] [6]
For thyroid storm, the resuscitation has four simultaneous tracks: block the beta-adrenergic drive (propranolol), block the new hormone synthesis (carbimazole or propylthiouracil), block the peripheral conversion of T4 to T3 (hydrocortisone or dexamethasone), and cool the child and treat the precipitant. Give a beta-blocker cautiously if there is heart failure, start the antithyroid drug, give the corticosteroid, and use active cooling with paracetamol and cooling blankets. The paediatric systematic review (Abisad 2023) confirms that the blocking regimen, adapted from the adult ATA guideline, is the standard, and that mortality is driven by cardiovascular collapse and the precipitant. [7]
For the sodium-water emergencies, the emergency is the neurological symptom, not the number. A seizing child with hyponatraemia needs 3 per cent hypertonic saline at 2 mL per kg over 10 minutes, repeated once if still seizing — this is a neurological emergency and the seizure is terminated by raising the sodium by 3 to 5 mmol per litre. Then correct slowly (no more than 8 to 10 mmol per litre in 24 hours) to avoid osmotic demyelination. A collapsed child with hypernatraemic dehydration from diabetes insipidus needs rehydration with isotonic saline and then free-water replacement, with desmopressin once the diagnosis is confirmed. The principle is shared: correct slowly, because the brain has adapted. [9] [10]
Management — Definitive & Stepwise
Once the child is stable, the definitive management transitions from the empiric resuscitation to the disease-specific pathway, and each pathway has its own dedicated leaf. The integrated leaf teaches the transition and the shared disposition, not the full pathway. [1] [5]
The shared definitive pathway, from empiric resuscitation to disease-specific care
Resuscitate empirically: ABC, IV access, bedside glucose, gas and electrolytes, then the specific empiric therapy
Confirm the diagnosis with the confirmatory endocrine test (cortisol/ACTH, TSH/T4, osmolality, ketones) once the child is stable
Transition to disease-specific care: DKA to insulin titration and oral refeeding; adrenal crisis to oral hydrocortisone with a stress-dose plan; thyroid storm to blocking therapy and definitive thyrotoxicosis treatment; SIADH to treating the trigger
Build the sick-day or stress-dose plan, the parent-held emergency kit where relevant, and the school care plan
Arrange structured follow-up with the relevant subspecialist and transition to adult endocrinology
In DKA, the definitive care moves from the resuscitation to the insulin titration, the glucose stabilisation, the oral refeeding and the diabetes education. The two-bag fluid system — one bag with dextrose, one without, titrated to the glucose — is a practical method to stabilise the glucose and allow earlier potassium and insulin titration, and the randomised trial (Dhochak 2018) supports its use in resource-limited settings. Once the child is eating and drinking, transition to subcutaneous insulin and begin the diabetes education and the sick-day plan. [1] [15]
In adrenal crisis, the definitive care is the transition to oral hydrocortisone and fludrocortisone with a stress-dose and emergency-injection plan. The stress-dose principle is the part that saves lives between clinics: double or triple the oral hydrocortisone for any febrile illness, give the parenteral dose if the child is vomiting, and teach the family to inject first and call for help second. The full pathway lives in the adrenal insufficiency and adrenal crisis leaf. [5] [6]
In thyroid storm, the definitive care is the blocking therapy continued until the child is stable, then the definitive treatment of the underlying thyrotoxicosis — usually Graves disease, treated with antithyroid medication, radioactive iodine or surgery. The full pathway lives in the hyperthyroidism and Graves disease leaf. [7]
In the sodium-water emergencies, the definitive care is treating the trigger (in SIADH) or confirming the diagnosis and starting desmopressin (in diabetes insipidus), with the slow correction maintained throughout. The full pathway lives in the diabetes insipidus and SIADH leaf. [9] [10]
Specific Subtypes & Scenarios
The scenarios below are the ones that present, collapse and are misdiagnosed, and they are the highest-yield material for the bedside and the written paper because they test the integrated approach rather than a single disease. [1]
The undiagnosed young child with new-onset diabetes presenting as DKA is the classic and dangerous scenario. The polyuria is attributed to a virus, the weight loss to a growth spurt, the vomiting to gastroenteritis, and the deep breathing to pneumonia, until the metabolic collapse arrives. The child under five presents in DKA more often, has a higher cerebral-oedema risk, and needs a developmentally adapted communication and sick-day plan. The countermeasure is the bedside glucose on every sick child — it takes two minutes and it is the single highest-yield habit in paediatric emergency medicine. [1] [13]
The known diabetic child with DKA from pump failure or insulin omission during illness is the recurring-presentation scenario. The onset is rapid, the precipitant is identifiable, and the lesson is to always ask about insulin delivery in a diabetic child who is unwell — an omitted dose, a disconnected pump, or an expired cartridge. The family needs a sick-day plan that tells them to check ketones and give correction insulin, and the registrar needs to know that a diabetic child who is vomiting is DKA until proven otherwise. [1] [2]
The adrenal crisis in the undiagnosed child is the preventable-death scenario. The child may have months of fatigue and progressive pigmentation (autoimmune Addison disease), or may be a neonate presenting with salt-wasting and ambiguous genitalia or a salt-losing crisis at one to three weeks (congenital adrenal hyperplasia). The cortisol-deficient child who is treated as gastroenteritis or sepsis while the adrenal fails is the preventable death, and the countermeasure is a low threshold for one dose of empiric intravenous hydrocortisone. [5] [6]
The thyroid storm in the adolescent with known or undiagnosed Graves disease, triggered by infection, non-adherence or thyroid surgery, is the rare-but-lethal scenario. The presentation is high fever, severe tachycardia or an atrial arrhythmia, and altered consciousness. The registrar must reach for the four-track blocking regimen — beta-blocker, antithyroid drug, corticosteroid and cooling — and must treat the precipitant. [7]
The hospital-acquired SIADH in the child with a CNS insult (meningitis, head injury, post-neurosurgery) who develops symptomatic hyponatraemia and seizures is the ward scenario that is often missed until the seizure. The countermeasure is to check the sodium in any child with a CNS insult who becomes drowsy or agitated, and to treat the seizure with hypertonic saline. The diabetes insipidus child who develops hypernatraemic dehydration post-pituitary surgery is the mirror scenario, and the registrar must monitor the sodium and urine output closely in any child after pituitary or hypothalamic surgery. [9] [10]
Complications & Pitfalls
The complications of paediatric endocrine emergencies divide into those of the untreated disease and those of its treatment, and the integrated approach must know both. The untreated disease kills — DKA cerebral oedema, adrenal-crisis shock, thyroid-storm cardiovascular collapse, and the seizing child with hyponatraemia are all lethal when missed. The treatment also injures — the insulin bolus, the bicarbonate, the over-rapid sodium correction, and the missed hypoglycaemia are the iatrogenic complications that the registrar controls. [1] [3]
Mortality of DKA cerebral oedema
critical
Cerebral oedema complicates roughly 0.5–1% of paediatric DKA episodes but carries a 20–40% mortality, making it the leading cause of diabetes-related death in children. The modifiable risk factors are bicarbonate use, high fluid rates, insulin bolus and severe acidosis or hyponatraemia at presentation.
The lethal pitfall across all endocrine emergencies is the missed diagnosis — the child treated as sepsis or gastroenteritis while the endocrine axis fails. The countermeasure is the bedside glucose, gas and electrolytes on every sick child, and a low threshold for the empiric treatment: one dose of intravenous hydrocortisone in suspected adrenal crisis, one fluid bolus and insulin infusion in suspected DKA, one hypertonic saline bolus in a seizing hyponatraemic child, and one glucose bolus in severe hypoglycaemia. Each is harmless if wrong and life-saving if right. [5] [1]
The DKA-specific treatment pitfalls are the highest-yield material for the written paper. Insulin given as a bolus causes dangerous hypokalaemia and increases cerebral-oedema risk — it is never given as a bolus. Bicarbonate is almost never used in paediatric DKA because it increases cerebral-oedema risk and masks the acidosis without treating the cause — it is reserved for the child with a pH below 6.9 and cardiovascular instability, and even then it is controversial. Large-volume or hypotonic fluid resuscitation raises the cerebral-oedema risk — the PECARN trial (Kuppermann 2018) refined but did not abolish the cautious-fluid principle. [4] [3]
The sodium-correction pitfalls cut across SIADH and diabetes insipidus. Rapid correction of hyponatraemia (more than 8 to 10 mmol per litre in 24 hours) causes osmotic demyelination syndrome; too-slow correction of symptomatic hyponatraemia allows ongoing seizures and brain injury. The principle is to correct the seizure rapidly (the hypertonic saline bolus raises the sodium by 3 to 5 mmol per litre and terminates the seizure), then correct slowly. The same principle applies to the hypernatraemic child: correct slowly (no more than 0.5 mmol per litre per hour, or 10 to 12 mmol per litre in 24 hours) to avoid cerebral oedema from rapid descent. [9] [10]
Prognosis & Disposition
With early recognition, correct resuscitation and adherence to the ISPAD and BSPED guidelines, the mortality from paediatric DKA is below 0.5 per cent — but cerebral oedema remains the exception, with its 20 to 40 per cent mortality. The modifiable factor is whether the diagnosis is made early and the fluid and insulin protocol is followed correctly, which is why the DKA protocol is one of the highest-yield topics in the written paper. [1] [12]
Adrenal crisis mortality per episode is 0.5 to 10 per cent, and the modifiable factor is whether the diagnosis and emergency plan are built before the crisis. Thyroid storm mortality in children is significant but less well quantified because of its rarity; the paediatric systematic review (Abisad 2023) calls for better data. The sodium-water emergencies have an excellent prognosis when the sodium is corrected slowly and the trigger is treated, but a poor prognosis when the seizure or the rapid correction is missed. [5] [7]
Across the ISPAD 2022 consensus (Glaser), the BSPED UK guideline (Heddy 2021) and the Endocrine Society adrenal guideline (Bornstein 2016), the shared principle is the same: recognise early, resuscitate with the empiric therapy before the confirmatory test, follow the structured fluid and insulin protocol in DKA, give the empiric hydrocortisone in suspected adrenal crisis, use the four-track blocking regimen in thyroid storm, and correct sodium slowly. Local protocols differ on the DKA fluid regimen and the cerebral-oedema treatment (mannitol versus hypertonic saline), but the shared principle is universal. [1] [6] [12]
Disposition from the emergency department runs on two tracks: severity and follow-up. Any child with DKA and altered consciousness, refractory shock, thyroid storm or symptomatic hyponatraemia needs PICU involvement. The child with mild to moderate DKA and a stable conscious level can be managed on the ward with a structured protocol and hourly observations. Every child needs structured outpatient follow-up with the relevant subspecialist — diabetes, endocrinology, or nephrology — and a sick-day or stress-dose plan that prevents the next emergency. [1] [12]
Special Populations
The young child under five with new-onset diabetes is the population most at risk of DKA and of cerebral oedema, because the diabetes is often undiagnosed and the metabolic collapse can be rapid. The communication and sick-day plan must be developmentally adapted, the family must be taught to recognise the signs, and the school or childcare must have a care plan. The countermeasure is the bedside glucose on every sick young child. [1] [13]
The adolescent at transition carries the cumulative burden of a chronic endocrine disease into independence. The challenges are adherence (to insulin, to hydrocortisone, to antithyroid medication), the carry-over of a parent-managed emergency plan into self-management, the risk-taking and alcohol exposure that can precipitate crisis (alcohol-induced hypoglycaemia in the diabetic adolescent, or a missed hydrocortisone dose), and the reproductive and bone-health questions that attend chronic hormone replacement. A structured, honest transition that rehearses the sick-day rules and the emergency plan is the standard of care. [5] [1]
The child with known adrenal insufficiency or congenital adrenal hyperplasia on hydrocortisone is the population whose stress-dose plan and parent-held emergency kit are the difference between a managed illness and a crisis. The family must know to double or triple the oral hydrocortisone for any febrile illness, to give the parenteral dose if the child vomits, and to inject first and call for help second. The school must have a care plan and a trained staff member who can give the emergency injection. [5] [6]
In Australia and Aotearoa New Zealand, the commonest paediatric endocrine emergency is DKA in new-onset diabetes, and the highest-yield habit is the bedside glucose on every sick child. Adrenal crisis is less common but carries the same preventable-death risk, especially in remote and Indigenous communities where the logistics of accessing hydrocortisone and emergency care are harder. Thyroid storm is rare. The sodium-water emergencies are common on the ward. Equity of access to insulin, hydrocortisone, emergency care and structured follow-up is a determinant of endocrine-emergency outcomes in remote and Indigenous communities. [1] [5]
The child in a resource-limited or remote setting faces both a higher infective burden and the logistics of accessing insulin, hydrocortisone and emergency care. The two-bag fluid system (Dhochak 2018) was designed for and validated in resource-limited settings, and it is a practical method to manage DKA where intensive monitoring is limited. Advocacy for a reliable supply of insulin, hydrocortisone and emergency care, and for school-based education and a parent-held emergency kit, is part of the medical care in every setting. [15]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric endocrine emergencies is dominated by the ISPAD consensus guidelines and a growing trial and registry tradition. The ISPAD 2022 DKA consensus (Glaser, PMID 36250645) is the current standard for DKA recognition and management, building on the 2018 iteration (Wolfsdorf, PMID 29900641). The BSPED UK guideline (Heddy 2021, PMID 33627326) is the operational standard for the UK. The two share the same principles: cautious fluid, insulin as an infusion only, potassium replacement, no bicarbonate, and the cerebral-oedema watch. [1] [2] [12]
The DKA fluid evidence was transformed by the PECARN factorial trial (Kuppermann 2018, PMID 29897851), which randomised children to fast or slow fluid rehydration and to 0.9 per cent saline or a mixed-salt solution, and found no difference in neurological outcomes by either arm. The trial refined the fluid debate but did not abolish the cautious-fluid principle — the cerebral-oedema risk persists, and the ISPAD 2022 guideline continues to recommend structured, cautious fluid. The cerebral-oedema pathophysiology is reviewed by Azova (2021, PMID 33197066) and the early identification by Muir (2004, PMID 15220225). [4] [13] [14]
The adrenal crisis evidence rests on the Endocrine Society guideline (Bornstein 2016, PMID 26760044) and the NEJM review (Rushworth 2019, PMID 31461595), both of which codify the empiric hydrocortisone-first resuscitation. The paediatric thyroid storm evidence is less mature — the systematic review (Abisad 2023, PMID 36318760) found only case reports and small series — and the treatment is adapted from the adult ATA guideline. The ISPAD hypoglycaemia guideline (Abraham 2022, PMID 36537534) is the standard for the diabetic child, and the paediatric hyponatraemia framework is set by Zieg (2014, PMID 24862500) and Moritz (2019, PMID 30454744). [5] [7] [8] [10]
The remaining controversies are practical. The optimal DKA fluid regimen after PECARN, the role of the two-bag system, the bicarbonate question (almost never), the mannitol-versus-hypertonic-saline question for cerebral oedema, and the vaptan question in paediatric SIADH are all live debates. A fellowship candidate names the debate and the standard, not a false consensus. The shared principle — empiric treatment before the confirmatory test — is the one thing that is not controversial. [1] [4]
Exam Pearls
One-sentence answer: the integrated approach to a paediatric endocrine emergency
A sick child with an unexplained glucose, sodium or potassium derangement has an endocrine emergency until proven otherwise: secure the airway and IV access, check the bedside glucose, blood gas and electrolytes, and give the empiric life-saving therapy — fluids and an insulin infusion for DKA, hydrocortisone and fluids for adrenal crisis, a beta-blocker with an antithyroid drug for thyroid storm, hypertonic saline for seizures from hyponatraemia, and dextrose for severe hypoglycaemia — all before the confirmatory endocrine tests return.
The triage
- Bedside glucose + blood gas + electrolytes split the four emergencies within minutes
- High glucose + acidosis + ketones = DKA; low glucose = hypoglycaemia
- Low sodium + normal/high potassium + shock = adrenal crisis; low sodium alone = SIADH; high sodium + dilute urine = DI
- Sepsis coexists with and mimics every endocrine emergency — cover it
The empiric treatments (before the confirmatory test)
- DKA: 10–20 mL/kg saline if shock + insulin 0.05–0.1 U/kg/hr infusion (never a bolus)
- Adrenal crisis: IV hydrocortisone child 50–100 mg, infant/neonate 25 mg stat + fluids
- Thyroid storm: beta-blocker + antithyroid drug + steroid + cooling
- SIADH seizure: 3% saline 2 mL/kg; hypoglycaemia: 10% dextrose 2–5 mL/kg
The pitfalls
- Insulin bolus in DKA — NEVER (hypokalaemia, cerebral oedema risk)
- Bicarbonate in DKA — almost never (cerebral oedema risk)
- Falling corrected sodium or headache during DKA = cerebral oedema until proven otherwise
- Rapid sodium correction in SIADH = osmotic demyelination; too slow = ongoing seizure
The cerebral-oedema protocol
- Signs: headache, altered consciousness, bradycardia + hypertension (Cushing), pupillary change
- Treat immediately: mannitol 0.5–1 g/kg OR 3% saline 2–5 mL/kg, reduce fluid rate, intubate
- Do not wait for a CT to treat — delay is the preventable cause of death
Frequently misremembered facts, stated correctly: insulin is never given as a bolus in DKA; bicarbonate is almost never used in paediatric DKA because it increases cerebral-oedema risk; a random stress cortisol above 500 nanomoles per litre in a sick child effectively excludes adrenal insufficiency; one dose of empiric intravenous hydrocortisone is harmless if wrong and life-saving if right; and the corrected sodium (measured sodium plus 0.016 times (glucose minus 5.5)) must be tracked with every gas in DKA because a falling corrected sodium is the cerebral-oedema red flag. [1] [5] [11]
The lesion-to-sign pairings are the fastest route to a bedside answer and the highest-yield material for a written or oral question: deep sighing breathing with dehydration and a high glucose is DKA; shock with hyponatraemia, hyperkalaemia and hyperpigmentation is adrenal crisis; high fever with severe tachycardia, a goitre and altered consciousness is thyroid storm; a seizing child with a low sodium is SIADH or cerebral salt wasting; and a dehydrated child with a high sodium and dilute urine is diabetes insipidus. Each is one hormone failing, and each has one targeted treatment. [1] [7] [10]
References
- [1]Glaser N; Barnett P; McCaslin I; et al ISPAD clinical practice consensus guidelines 2022: Diabetic ketoacidosis and hyperglycemic hyperosmolar state. Pediatr Diabetes, 2022.PMID 36250645
- [2]Wolfsdorf JI; Glaser N; Agus M; et al ISPAD Clinical Practice Consensus Guidelines 2018: Diabetic ketoacidosis and the hyperglycemic hyperosmolar state. Pediatr Diabetes, 2018.PMID 29900641
- [3]Glaser N; Barnett P; McCaslin I; et al Risk factors for cerebral edema in children with diabetic ketoacidosis. The Pediatric Emergency Medicine Collaborative Research Committee of the American Academy of Pediatrics. N Engl J Med, 2001.PMID 11172153
- [4]Kuppermann N; Ghetti S; Schunk JE; et al Clinical Trial of Fluid Infusion Rates for Pediatric Diabetic Ketoacidosis. N Engl J Med, 2018.PMID 29897851
- [5]Rushworth RL; Torpy DJ; Falhammar H Adrenal Crisis. N Engl J Med, 2019.PMID 31461595
- [6]Bornstein SR; Allolio B; Arlt W; et al Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab, 2016.PMID 26760044
- [7]Abisad DA; Tiu MCF; del Rosario RR; Lazaro JG Thyroid storm in pediatrics: a systematic review. J Pediatr Endocrinol Metab, 2023.PMID 36318760
- [8]Abraham MB; Jones TW; Naranjo D; et al ISPAD Clinical Practice Consensus Guidelines 2022: Assessment and management of hypoglycemia in children and adolescents with diabetes. Pediatr Diabetes, 2022.PMID 36537534
- [9]Moritz ML; Ayus JC Syndrome of Inappropriate Antidiuresis. Pediatr Clin North Am, 2019.PMID 30454744
- [10]Zieg J Evaluation and management of hyponatraemia in children. Acta Paediatr, 2014.PMID 24862500
- [11]Glaser NS; Marcin JP; Wootton-Gorges SL; et al Serum Sodium Concentration and Mental Status in Children With Diabetic Ketoacidosis. Pediatrics, 2021.PMID 34373322
- [12]Heddy N; Sood S; Gevers E; et al Guideline for the management of children and young people under the age of 18 years with diabetic ketoacidosis (British Society for Paediatric Endocrinology and Diabetes). Arch Dis Child Educ Pract Ed, 2021.PMID 33627326
- [13]Azova S; Ratner R; Kuelbs C; Bhasin M; Buonocore C; Cohen M; Glaser N Brain injury in children with diabetic ketoacidosis: Review of the literature and a proposed pathophysiologic pathway for the development of cerebral edema. Pediatr Diabetes, 2021.PMID 33197066
- [14]Muir AB; Quisling RG; Yang MC; Rosenbloom AL Cerebral edema in childhood diabetic ketoacidosis: natural history, radiographic findings, and early identification. Diabetes Care, 2004.PMID 15220225
- [15]Dhochak N; Singhi S; Kaur N; Jayashree M; Kumar M A randomized controlled trial of one bag vs. two bag system of fluid delivery in children with diabetic ketoacidosis: Experience from a developing country. J Crit Care, 2018.PMID 29066219