Paeds · endocrinology-diabetes-and-growth
Endocrine late effects of cancer treatment
Also known as Endocrine late effects of childhood cancer · Cancer survivor endocrinopathy · Radiation-induced hypopituitarism · Chemotherapy-induced gonadal failure · Cranial irradiation endocrinopathy · Childhood cancer survivor endocrine surveillance · Radiation-induced growth hormone deficiency · Treatment-related central hypothyroidism · Secondary thyroid cancer after neck radiation · Paediatric oncology long-term follow-up
A fellowship approach to the endocrine late effects of childhood cancer treatment: recognise that the survivor who slows on the growth chart, develops central hypothyroidism, adrenal insufficiency, gonadotropin deficiency or paradoxical precocious puberty after cranial irradiation, or primary thyroid dysfunction, gonadal failure, metabolic syndrome and reduced bone density after neck radiation and alkylating chemotherapy, is showing the most common and earliest complications of cure — then risk-stratify by exposure, screen the vulnerable axes with a structured long-term follow-up programme, and replace each deficiency in the correct order with hydrocortisone before thyroxine and sex steroids and recombinant growth hormone only after magnetic resonance imaging excludes recurrence.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The mark goes to the candidate who reasons along three axes at once. The first is the exposure history: the radiation dose to the hypothalamic-pituitary axis, the radiation field to the neck and spine, and the cumulative dose of alkylating chemotherapy. The second is the axis physiology: which hormone is lost depends on which neurone population is most vulnerable to fractionated radiation, and the growth-hormone axis is the most radiosensitive. The third is the whole survivor: endocrine late effects accumulate over decades, they interact with other late effects (cardiac, neurocognitive, second malignancy), and they are entirely treatable when caught early — which is why surveillance fidelity, not clever rescue, is what determines outcome. [1] [3]
Overview & Definition
Endocrine late effects are the structural and functional disorders of the endocrine system that appear months to decades after successful treatment of childhood cancer. They arise from direct damage to the hypothalamic-pituitary axis by cranial or craniospinal radiation and surgery, and from direct damage to the peripheral glands by neck radiation, by gonadotoxic chemotherapy, and by stem cell transplantation conditioning. They are the single most common group of late complications of childhood cancer therapy, affecting roughly forty to fifty percent of long-term survivors, and they are the earliest to declare themselves — growth failure from growth hormone deficiency can appear within the first year after cranial irradiation. Because cure of childhood cancer is now the expected outcome in the majority of patients, the population of survivors at risk is large and growing, and endocrine late effects have moved from a curiosity to the central clinical problem of survivorship. [1] [4]
The endocrine system is vulnerable for two reasons. First, the hypothalamic-pituitary axis sits in the central nervous system where it receives the full dose of cranial radiation given for brain tumours, leukaemia prophylaxis and transplant conditioning. Its neurone populations are exquisitely sensitive to fractionated radiation in a dose-dependent hierarchy. Second, the peripheral glands — thyroid and gonads especially — sit in or near radiation fields used for head and neck, mediastinal, craniospinal, and total-body irradiation, and the gonads are additionally damaged by alkylating chemotherapy that targets rapidly dividing cells. The bone and the metabolic system are injured more indirectly, through growth hormone deficiency, glucocorticoid exposure, and the inflammatory and nutritional consequences of cancer and its treatment. [2] [7]
Classification
Endocrine late effects are best classified by the gland or axis affected and by the treatment exposure that caused them, because the surveillance schedule and the screening tests follow directly from the exposure rather than from a symptom-driven search. The hypothalamic-pituitary axis late effects include growth hormone deficiency, thyroid-stimulating hormone deficiency (central hypothyroidism), adrenocorticotropic hormone deficiency (central adrenal insufficiency), gonadotropin deficiency (hypogonadotropic hypogonadism), and the paradoxical central precocious puberty that follows lower-dose cranial radiation. The peripheral gland late effects include primary hypothyroidism, thyroid nodules and secondary differentiated thyroid cancer, primary ovarian failure, primary testicular failure, and the metabolic consequences of insulin resistance and dyslipidaemia. The skeletal and body-composition late effects include reduced bone mineral density and the hypothalamic obesity that follows surgery or high-dose radiation to the hypothalamus. [1] [6]
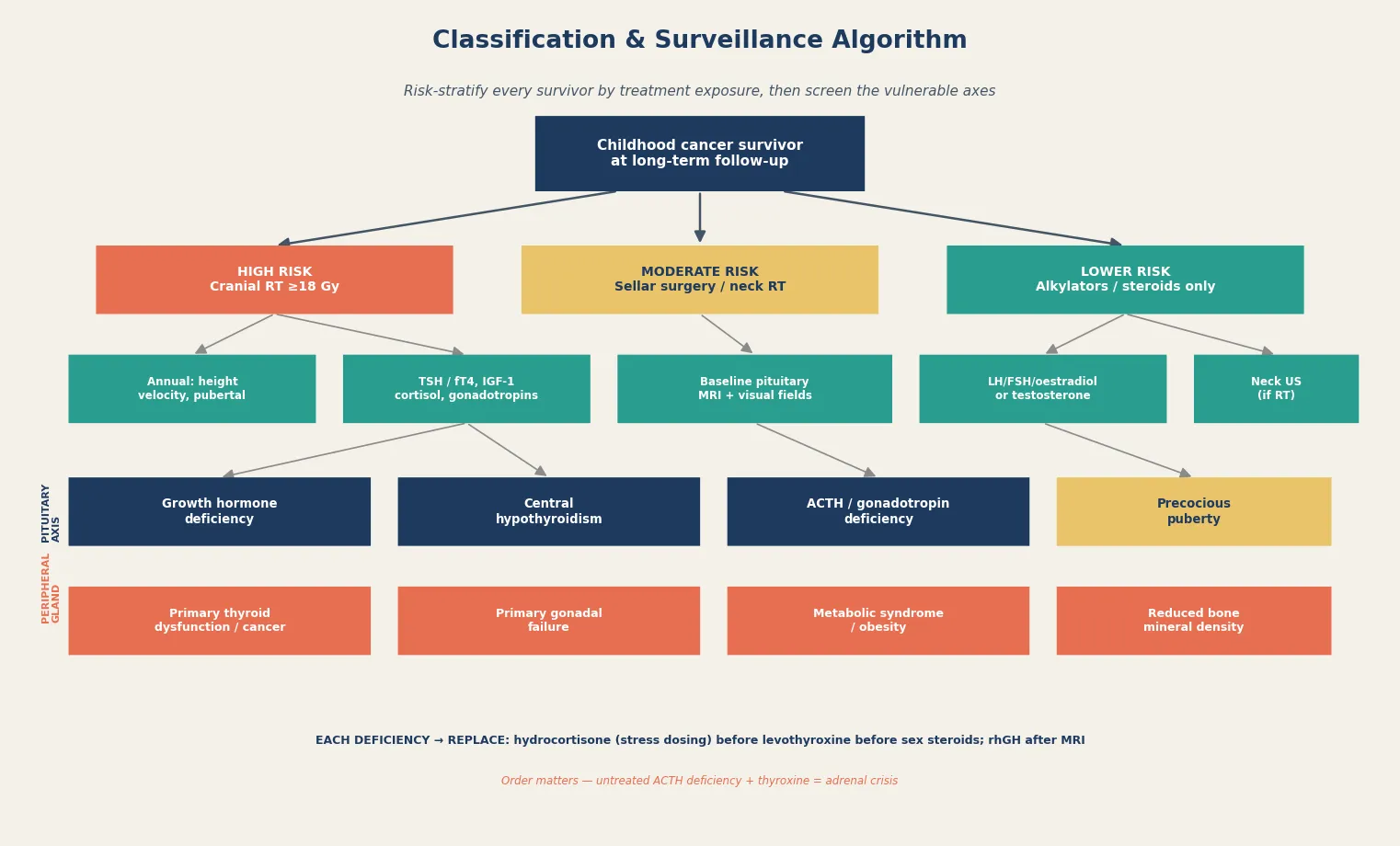
A parallel classification applies to the risk stratification that drives surveillance. The high-risk group received cranial radiation at or above 18 Gy for a brain tumour or as central nervous system leukaemia prophylaxis; the moderate-risk group received sellar or suprasellar surgery, neck radiation, or craniospinal radiation; and the lower-risk group received alkylating chemotherapy or prolonged glucocorticoids without central nervous system radiation. The surveillance intensity, the screening intervals, and the specific axes monitored follow from this tiering, which is the practical heart of the long-term follow-up programme and the construct the exam rewards. [2] [6]
Epidemiology & Risk Factors
Endocrine late effects are the most prevalent group of chronic health conditions in adult survivors of childhood cancer, and their prevalence rises with time since treatment. The Childhood Cancer Survivor Study reported that endocrine abnormalities become more common as survivors age, with growth hormone deficiency, thyroid dysfunction, hypogonadism and metabolic syndrome each contributing to a cumulative burden that affects the majority of survivors by the third decade of life. The Armstrong analysis of severe, life-threatening and fatal events in the same cohort confirmed that endocrine disorders are among the most common serious late effects, alongside cardiac and second-malignancy events, and that they cluster with other chronic conditions in the ageing survivor. [4] [5]
The risk factors are the treatment exposures themselves, and they are cumulative. The strongest predictor of hypothalamic-pituitary late effects is the radiation dose to the axis. Growth hormone deficiency appears at 18 Gy and above. The gonadotropin axis is disturbed at 24 to 30 Gy. The thyroid-stimulating hormone and adrenocorticotropic hormone axes fail above 30 to 40 Gy, with panhypopituitarism at the highest doses. Surgery on the hypothalamic-pituitary axis — for craniopharyngioma, germinoma, medulloblastoma or glioma — adds direct mechanical injury on top of any radiation. For the peripheral glands, the risk factors are neck or craniospinal radiation for thyroid disease, and cumulative alkylating chemotherapy dose and total-body irradiation conditioning for gonadal failure. Younger age at treatment and female sex amplify the gonadotoxic effect of alkylators. [1] [8]
Pathophysiology
The pathophysiology of the central late effects is the dose-dependent destruction of hypothalamic and pituitary neurone populations by fractionated radiation. The somatotroph axis is the most radiosensitive, so growth hormone deficiency appears first and at the lowest radiation dose. The growth-hormone-releasing-hormone neurones of the hypothalamus and the somatotrophs of the anterior pituitary lose their capacity to generate the pulsatile signal that drives insulin-like growth factor 1. The growth plate is then starved of its proliferative signal, and linear growth slows. At higher doses the gonadotroph axes are lost, producing gonadotropin deficiency and hypogonadotropic hypogonadism; at still higher doses the thyrotroph and corticotroph axes fail, producing central hypothyroidism and central adrenal insufficiency. [2] [7]
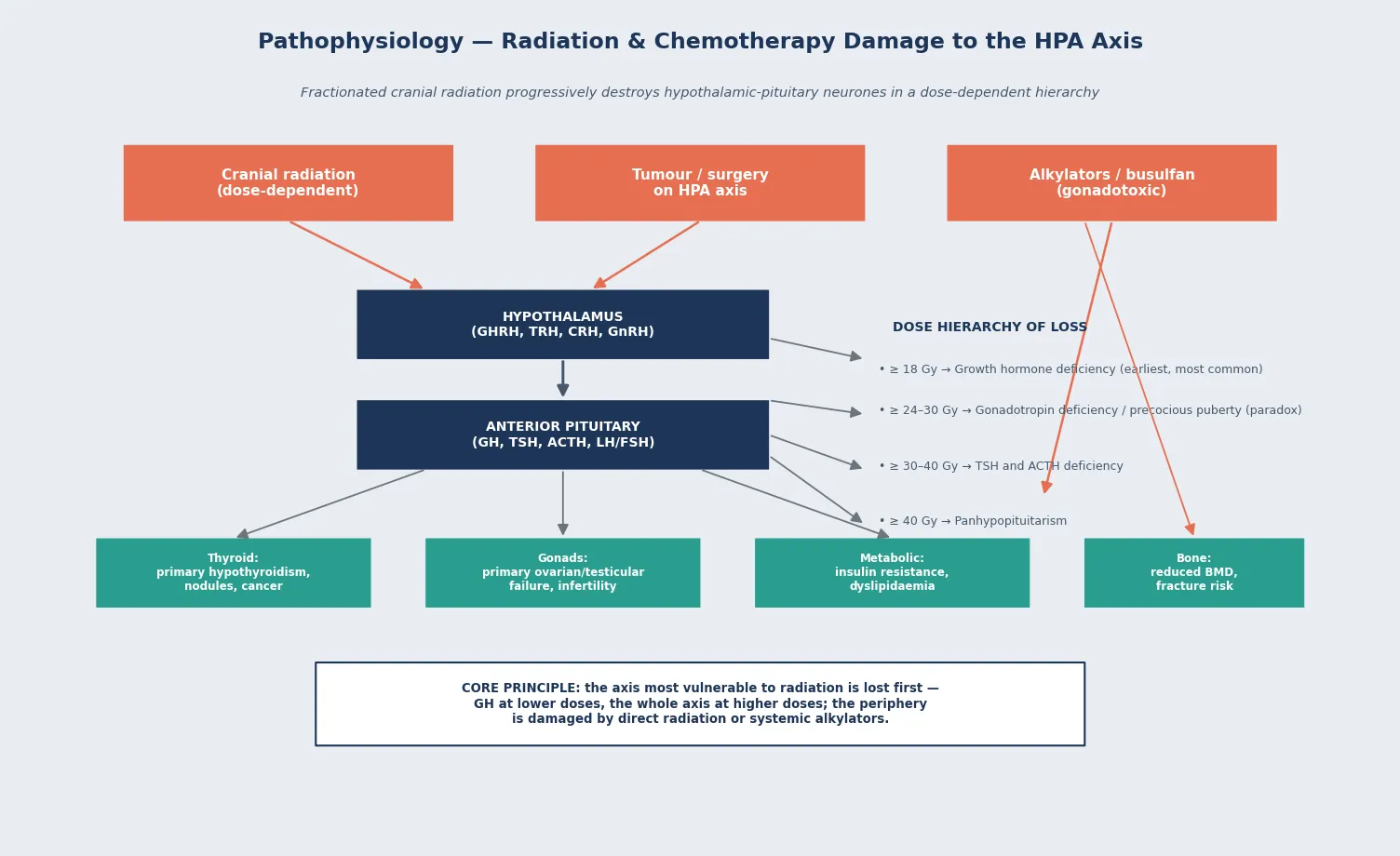
A paradox sits inside this hierarchy that the exam rewards the candidate who names it. At lower cranial radiation doses, between roughly 18 and 24 Gy, some children develop central precocious puberty rather than gonadotropin deficiency, because the radiation disinhibits the hypothalamic pulse generator and triggers early activation of the gonadotropin axis before it is destroyed. This paradoxical precocious puberty accelerates bone-age advancement and compromises final adult height, and it must be distinguished from the gonadotropin deficiency that appears at higher doses. The net effect is that the same exposure can produce opposite gonadal phenotypes depending on the dose and the timing, which is why the gonadotropin axis must be assessed biochemically in every survivor rather than inferred from the radiation dose alone. [1] [2]
The pathophysiology of the peripheral late effects is direct glandular injury. Neck and craniospinal radiation damages the thyroid follicular epithelium, producing a rising thyroid-stimulating hormone from the intact pituitary (primary or compensated hypothyroidism) and, over years, an increased incidence of thyroid nodules and secondary differentiated thyroid cancer. Alkylating chemotherapy and total-body irradiation damage the oocytes and the spermatogonia, producing primary ovarian failure with amenorrhoea and infertility, and primary testicular failure with small testes and azoospermia. Bone mineral density is reduced through a combination of growth hormone deficiency, glucocorticoid exposure, hypogonadism, and the nutritional and inflammatory consequences of cancer, and the metabolic syndrome of insulin resistance and dyslipidaemia emerges from radiation-induced hypothalamic injury, growth hormone deficiency, and the body-composition changes of survivorship. [3] [11]
Clinical Presentation
The presentation of endocrine late effects is shaped by the axis affected and the time since treatment, and the central rule is that the survivor rarely presents with a symptom the clinician expects — the clinician must go looking. Growth hormone deficiency presents as a slowing of growth velocity, a height crossing centiles downward, and a delayed bone age, typically emerging within the first year after cranial irradiation and worsening with time. Central hypothyroidism presents with fatigue, cold intolerance, weight gain, constipation, and bradycardia, and it is often picked up on surveillance biochemistry before it is symptomatic. Central adrenal insufficiency is the most dangerous presentation, because it is asymptomatic until the survivor is stressed by an intercurrent infection, when it declares itself as hypotension, hyponatraemia, vomiting, and collapse — a true adrenal crisis. [1] [7]
Gonadal late effects present differently by sex and by whether the lesion is central or peripheral. Central gonadotropin deficiency presents as arrested or absent puberty in a survivor of high-dose cranial radiation; paradoxical central precocious puberty presents as early and rapid pubertal progression in a survivor of lower-dose cranial radiation, with accelerated bone age that threatens final height. Primary ovarian failure presents with primary or secondary amenorrhoea, absent breast development, and hot flushes; primary testicular failure presents with absent testicular growth, lack of pubertal progression, and gynaecomastia. Thyroid late effects present with a palpable nodule, a growing goitre, or an asymptomatic thyroid-stimulating hormone elevation on surveillance biochemistry, and the metabolic and bone late effects are usually silent until they are screened for. [3] [4]
Differential Diagnosis
The differential diagnosis of an endocrine finding in a childhood cancer survivor always runs in two directions: the late effect must be distinguished from a tumour recurrence or progression, and from a coincidental endocrine disorder unrelated to the cancer or its treatment. Growth failure in a brain-tumour survivor is growth hormone deficiency until proven otherwise. Progressive tumour in the hypothalamic-pituitary region and spinal cord compression from recurrence must be excluded with imaging first. Recombinant growth hormone should not be given until a magnetic resonance imaging scan confirms stable disease. A rising thyroid-stimulating hormone in a survivor of neck radiation is primary hypothyroidism from radiation damage, but the same survivor may have autoimmune Hashimoto thyroiditis, and the thyroid nodule may be a radiation-induced differentiated thyroid cancer rather than a benign adenoma. [2] [9]
The differential of the gonadal finding depends on the gonadotropin level. A low or inappropriately normal gonadotropin with a low sex steroid in a survivor of high-dose cranial radiation is central hypogonadotropic hypogonadism, whereas a raised gonadotropin with a low sex steroid in a survivor of alkylating chemotherapy is primary gonadal failure. The two have the same symptom — arrested puberty or amenorrhoea — but different management, because central hypogonadism may recover and demands reassessment, whereas primary gonadal failure is usually permanent and demands early fertility counselling. Adrenal insufficiency in a survivor may be central (ACTH deficiency from cranial radiation) or reflect ongoing glucocorticoid taper or suppression, and the morning cortisol and the cosyntropin test sort the mechanism out. [3] [11]
Clinical & Bedside Assessment
The bedside assessment of a childhood cancer survivor begins with the treatment exposure record, because every screening decision follows from it. Establish the cancer diagnosis, the cumulative dose of cranial radiation and the field, the cumulative dose of alkylating chemotherapy, the use of total-body irradiation and the conditioning regimen for any stem cell transplantation, and the history of surgery on the hypothalamic-pituitary axis. Then measure the height and weight and plot them on a growth chart, calculate the growth velocity from a measurement at least six months earlier, and assess the pubertal stage against age references. Examine the thyroid for nodules and goitre, examine the skin for striae and acanthosis suggesting metabolic syndrome, and measure the blood pressure and body mass index. [1] [6]
The history captures the symptoms of each axis. Ask about growth and shoe size, fatigue and cold intolerance, weight change and appetite, menstrual cycle and pubertal progression, hot flushes, polyuria and polydipsia, and — critically — the response to intercurrent illness, because a survivor who reports severe fatigue or collapse during a fever may have occult adrenal insufficiency. Ask about headaches and visual change (possible recurrence), and about fertility intentions, because fertility counselling is now an expected part of survivorship care. The examination is completed with a focused neurological and visual field assessment if the survivor had a brain tumour, and with a developmental and psychosocial screen, because cognitive late effects compound the endocrine burden. [3] [5]
The bedside assessment converts directly into the surveillance plan. The exposure record determines which axes are at risk and at what interval; the growth velocity and pubertal stage determine the timing of growth hormone and gonadotropin evaluation; and the examination findings trigger the confirmatory tests. The candidate who links the exposure to the next best investigation — rather than ordering a blanket endocrine panel on every survivor — demonstrates the reasoning the exam rewards. [2] [6]
Investigations
The first-tier surveillance tests for the hypothalamic-pituitary axis are insulin-like growth factor 1 (with a stimulation test if low), thyroid-stimulating hormone and free thyroxine, a morning cortisol, and gonadotropins with a sex steroid. These are drawn annually after cranial radiation and interpreted against age-, sex- and pubertal-stage-specific reference ranges. A low insulin-like growth factor 1 with a subnormal growth velocity triggers a growth hormone stimulation test, with a peak growth hormone below the age-appropriate cutoff confirming deficiency. A low morning cortisol triggers a dynamic test of the axis — a low-dose cosyntropin or an insulin tolerance test — and a low thyroid-stimulating hormone with a low free thyroxine confirms central hypothyroidism. [2] [7]
Why the magnetic resonance imaging scan comes before the recombinant growth hormone — and why the cortisol comes before the thyroxine
Two ordering rules govern hormone replacement in the survivor, and the exam rewards the candidate who names and justifies them. First, a magnetic resonance imaging scan of the hypothalamic-pituitary axis must be obtained before recombinant growth hormone is started, because growth hormone is a mitogen and a residual or recurrent tumour in the region must be excluded — giving growth hormone into an unimaged sella is a classic and avoidable error. Second, hydrocortisone must be started before levothyroxine in any survivor with combined ACTH and TSH deficiency, because thyroxine increases cortisol clearance and precipitates an adrenal crisis in the cortisol-deficient patient. The replacement order — hydrocortisone, then levothyroxine, then sex steroids, then recombinant growth hormone after the magnetic resonance imaging — is the single highest-yield management fact in this topic. [2] [7]
The investigations for the peripheral late effects follow the exposure. Survivors of neck or craniospinal radiation have an annual thyroid-stimulating hormone and free thyroxine, a baseline neck ultrasound, and lifelong surveillance for thyroid nodules, with fine-needle aspiration of any nodule meeting the size or sonographic criteria. Survivors of alkylating chemotherapy or total-body irradiation have gonadotropins and sex steroids at the expected age of puberty and again at the transition to adult care, with anti-Müllerian hormone in girls to estimate ovarian reserve. Every survivor has a baseline bone density scan (dual-energy X-ray absorptiometry) and a metabolic panel of fasting glucose, insulin and lipids, repeated at intervals set by the exposure and the findings. [6] [10]
Management — Resuscitation
Endocrine late effects rarely require resuscitation in the way an adrenal crisis from primary adrenal insufficiency does, but the survivor with undiagnosed adrenocorticotropic hormone deficiency is exactly that patient when stressed by an intercurrent infection. The acute presentation is hypotension, hyponatraemia, hypoglycaemia, vomiting and collapse — a true adrenal crisis — and the management is immediate intravenous hydrocortisone at stress doses, intravenous fluid resuscitation with normal saline, and treatment of the precipitating infection. The diagnosis of central adrenal insufficiency is then confirmed once the survivor is stable, with a morning cortisol and a dynamic test. Every survivor with confirmed ACTH deficiency must wear medical alert identification and carry a hydrocortisone emergency injection, and the family must be taught the sick-day rules for doubling or tripling the oral dose during febrile illness. [2] [3]
The second resuscitation scenario is the survivor with a large secondary thyroid cancer from neck radiation presenting with airway compromise or stridor, which requires urgent imaging, a protected airway, and surgical and endocrine involvement. Central precocious puberty causing rapid bone-age advancement and a threatened final height is not a resuscitation emergency but is an urgent endocrine problem that demands prompt gonadotropin-releasing-hormone analogue therapy to halt progression. Across all scenarios, the principle is that the survivor with a known or suspected endocrine late effect who decompensates must be assumed to have adrenal insufficiency until proven otherwise, because missing it is the avoidable death of survivorship. [1] [9]
Management — Definitive & Stepwise
The definitive management of endocrine late effects is hormone replacement, delivered in the correct order and titrated to the age- and sex-appropriate target. Hydrocortisone is given for ACTH deficiency at a replacement dose of 8 to 12 milligrams per square metre per day in divided doses, with a written plan for stress-dose triple during febrile illness and an emergency injection kit. Levothyroxine is given for central hypothyroidism (after cortisol cover) at a weight- and age-based dose, titrated to a free thyroxine in the upper half of the reference range — the thyroid-stimulating hormone cannot guide dosing in central disease. Sex steroids are introduced at the physiological pubertal age for central hypogonadism, escalated to adult replacement doses, and coordinated with fertility counselling. [2] [7]
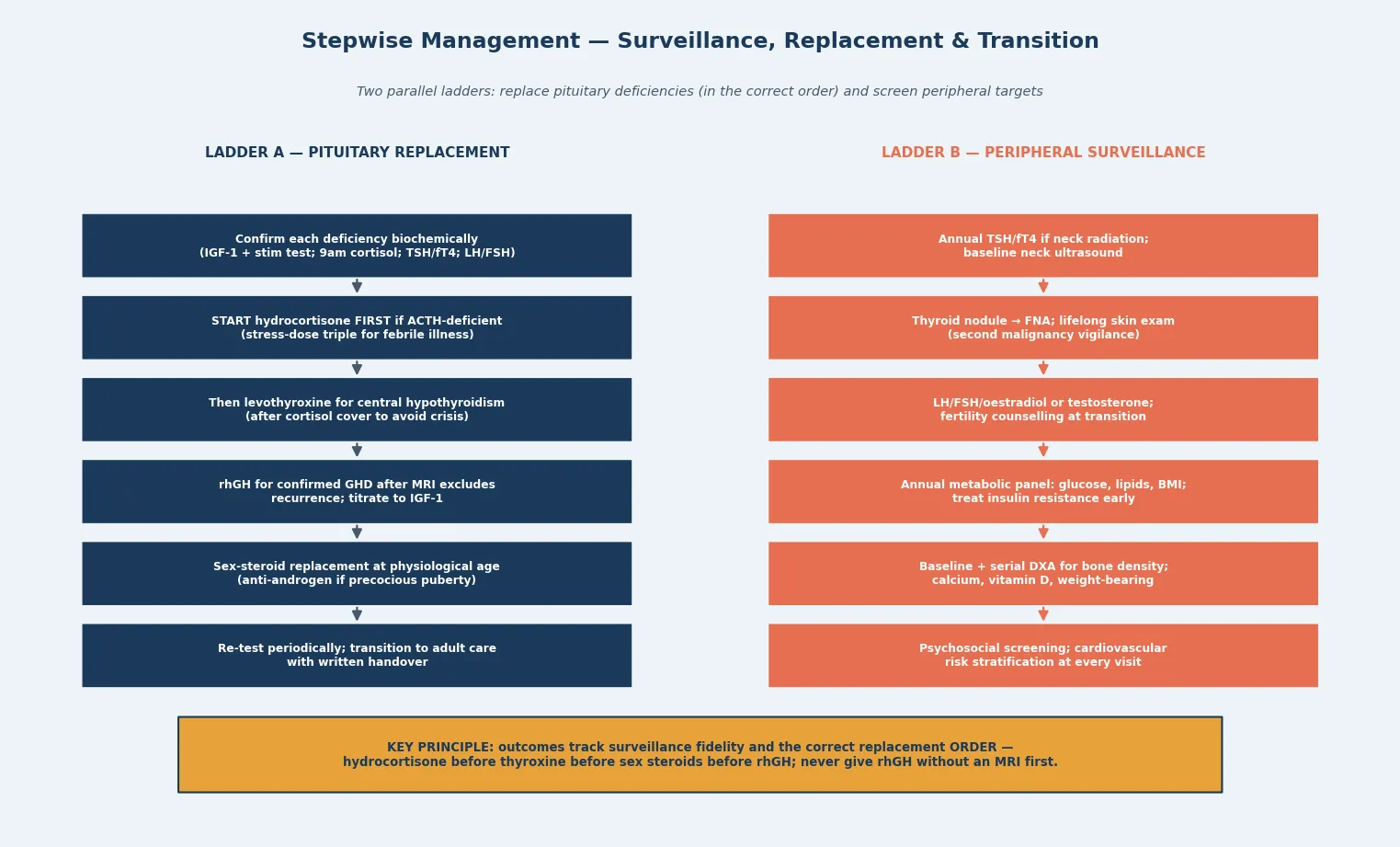
Recombinant growth hormone is given for confirmed growth hormone deficiency, but only after a magnetic resonance imaging scan has excluded tumour recurrence, and it is titrated to the insulin-like growth factor 1 in the age-appropriate range, with monitoring of growth velocity, glucose, thyroid function and intracranial pressure. Central precocious puberty is treated with a gonadotropin-releasing-hormone analogue to halt bone-age advancement and preserve final height. Secondary differentiated thyroid cancer is managed by total thyroidectomy and radioactive iodine as indicated, with lifelong thyroglobulin surveillance. The metabolic and bone late effects are managed with lifestyle intervention, treatment of insulin resistance and dyslipidaemia, calcium and vitamin D supplementation, and weight-bearing exercise, with pharmacotherapy for osteoporosis when the bone density deficit is severe. [1] [10]
C.O.R.T.E.X. \u2014 the replacement order in the cancer survivor
Specific Subtypes & Scenarios
The brain-tumour survivor after cranial radiation is the highest-yield scenario because every hypothalamic-pituitary axis is at risk and the dose hierarchy applies in full. A child treated for medulloblastoma with craniospinal radiation and a posterior fossa boost will typically develop growth hormone deficiency first, from the cranial component. Growth failure is then compounded by the spinal radiation effect on the growth plates and the vertebral bodies. Gonadotropin disturbance, TSH deficiency and ACTH deficiency follow in the dose-dependent order. The craniopharyngioma survivor is the archetype of combined surgical and radiation injury, with panhypopituitarism and hypothalamic obesity, diabetes insipidus from posterior pituitary damage, and visual loss from chiasmal involvement — a scenario the long-case examiner favours because it tests the whole axis at once. [1] [8]
The leukaemia survivor after haematopoietic stem cell transplantation is the second archetypal scenario, with the conditioning regimen — total-body irradiation and alkylating chemotherapy — driving primary gonadal failure and infertility, growth hormone deficiency from the cranial component of the conditioning or from prior central-nervous-system leukaemia prophylaxis, and thyroid dysfunction from the thyroid exposure. The Vatanen study of ovarian function after allogeneic stem cell transplantation in childhood documented the high rate of primary ovarian failure and the dependence on the conditioning regimen and the age at transplantation, underpinning the move toward fertility preservation counselling before conditioning begins. The metabolic and bone late effects cluster in this group and demand integrated surveillance. [3] [11]
The survivor of neck-irradiated disease — Hodgkin lymphoma, head and neck rhabdomyosarcoma, neuroblastoma — carries the thyroid and second-malignancy risk specifically. The Clement surveillance recommendations from the International Guideline Harmonization Group and PanCareSurFup set out the thyroid cancer surveillance schedule by exposure, with baseline neck ultrasound and lifelong clinical and biochemical surveillance for the irradiated survivor, and fine-needle aspiration of any nodule meeting sonographic criteria. This is the survivor in whom a new thyroid nodule is differentiated thyroid cancer until proven otherwise, and the candidate who names the exposure and the surveillance schedule earns the mark. [9]
Complications & Pitfalls
The complications of untreated endocrine late effects are the complications of untreated endocrine deficiency itself, magnified by the survivor's other late effects. Untreated growth hormone deficiency produces a final adult height far below the genetic potential, compounding the psychosocial burden of cancer survivorship. Untreated central hypothyroidism produces developmental slowing, hyperlipidaemia and a worsening of the neurocognitive late effects that already burden the brain-tumour survivor. The lethal complication is untreated ACTH deficiency, which declares itself as a fatal adrenal crisis during the first significant stress — an infection, an injury, an anaesthetic — and this is the single most important avoidable death in survivorship. The metabolic and bone complications accumulate silently: insulin resistance progresses to type 2 diabetes, dyslipidaemia accelerates the cardiovascular risk that is already elevated by anthracycline cardiotoxicity and chest radiation, and reduced bone mineral density predisposes to early osteoporotic fracture. [5] [10]
The pitfalls are the cognitive traps that cost marks and harm patients. The first is giving recombinant growth hormone before a magnetic resonance imaging scan has excluded tumour recurrence — the growth hormone is a mitogen, and a residual or recurrent tumour in the hypothalamic-pituitary region must be excluded first. The second is starting levothyroxine before hydrocortisone in a survivor with combined central hypothyroidism and ACTH deficiency — the thyroxine increases cortisol clearance and precipitates an adrenal crisis. The third is assuming that a normal thyroid-stimulating hormone excludes central hypothyroidism — the thyroid-stimulating hormone is low or inappropriately normal in central disease, and the free thyroxine is the diagnostic test, and it is also the target for titration rather than the thyroid-stimulating hormone. The fourth is missing the paradoxical precocious puberty of lower-dose cranial radiation by assuming the gonadotropin axis can only be deficient after radiation. [2] [7]
Prognosis & Disposition
The prognosis of endocrine late effects is good when they are caught early and replaced correctly, because the hormone deficiencies are the same as those in any patient with hypopituitarism or primary gland failure, and the replacement regimens are well established. Final adult height in the growth-hormone-deficient survivor depends on the age at starting recombinant growth hormone, the dose, the adherence, and the competing effect of spinal radiation on the growth plates. Quality of life and metabolic outcomes track the fidelity of surveillance and the completeness of replacement, and the untreated or under-treated survivor accumulates the cardiovascular, metabolic and skeletal burden that drives the excess mortality documented in the ageing Childhood Cancer Survivor Study cohort. The Armstrong analysis confirmed that endocrine disorders rank among the most common serious late effects in the ageing survivor, alongside cardiac and second-malignancy events, and that they interact with those events to drive cumulative morbidity. [4] [5]
Disposition is shared, lifelong, multidisciplinary care. The paediatric oncologist and the long-term follow-up programme own the exposure record, the surveillance schedule, and the integration of endocrine with cardiac, neurocognitive and psychosocial care. The paediatric endocrinologist owns the hormone evaluation and the replacement. The general paediatrician or family doctor owns the front-line recognition of decompensation and the sick-day hydrocortisone education. The reproductive endocrinologist and the fertility service join for the gonadal-failure survivor. The transition from paediatric oncology to adult survivorship care is the highest-risk moment in the pathway, because surveillance adherence falls, the young adult disengages from care, and the late effects continue to accumulate — a written handover, a named adult provider, and a structured transition clinic are the interventions that matter most. [6] [8]
Special Populations
The same endocrine late effects behave differently across populations because access, recognition and service models are unevenly distributed. In remote and Indigenous communities, the demands of attending a specialist survivorship clinic are amplified by distance, and the sick-day hydrocortisone education that prevents the fatal adrenal crisis is harder to deliver and sustain; telehealth-supported shared care with a regional centre, and a clear retrieval plan for the decompensating survivor, are disproportionately important. In migrant, refugee and asylum-seeking families, language barriers complicate the consent for recombinant growth hormone and the fertility counselling, and the treatment exposure record may be incomplete, so an interpreter-mediated structured history and a written surveillance plan are essential. [6]
In adolescents and young adults transitioning to adult survivorship care, the move is the highest-risk point in the pathway: adherence to surveillance and replacement falls, the rationale for continued hormone therapy may seem less compelling once growth is complete, and the metabolic and fertility consequences of gonadal failure become the dominant concerns. In survivors with complex chronic disease and disability — the craniopharyngioma survivor with panhypopituitarism and hypothalamic obesity, the brain-tumour survivor with neurocognitive and visual impairment — fragmentation of care across endocrinology, oncology, neurosurgery, ophthalmology and rehabilitation is the chief threat, and a written, reconciled shared-care plan with a named coordinator is the intervention that matters most. Socioeconomic disadvantage compounds all of these by limiting access to specialist endocrine care, growth hormone supply and the ongoing surveillance that survivorship demands. [5] [8]
In the young survivor identified early in surveillance with a single deficiency, the priority is to establish the full axis status and to start replacement in the correct order. The surveillance schedule must anticipate the further deficiencies that will accumulate with time. A normal early axis does not exclude a developing deficit, and the axes must be re-tested throughout childhood and into adult life. [2]
Evidence, Guidelines & Regional Differences
The evidence base rests on three pillars: the international clinical practice guidelines, the large survivor-cohort studies, and the exposure-specific surveillance and outcome literature. The Endocrine Society clinical practice guideline (Sklar and colleagues, 2018) is the contemporary framework for the central late effects. It sets out the screening tests, the diagnostic thresholds and the replacement regimens. The van Iersel Endocrine Reviews surveillance synthesis (2022) extended this across all endocrine late effects and set the integrated surveillance schedule. The Chemaitilly and Sklar concise guide (2019) distils the field for the practising paediatric endocrinologist. [2] [6] [1]
The cohort evidence is dominated by the Childhood Cancer Survivor Study. The Mostoufi-Moab analysis of endocrine abnormalities in ageing survivors (2016) documented the rising prevalence of endocrine disorders with time since treatment, and the Armstrong analysis of severe, life-threatening and fatal events (2014) placed endocrine disorders among the most common serious late effects in the ageing survivor. The van Iersel St. Jude Lifetime analysis (2019) defined the prevalence, risk factors and long-term health outcomes of hypothalamic-pituitary disorders, and the Cohen review (2005) remains the foundational synthesis of the endocrine late effects. The Goodenough JAMA Network Open analysis (2025) quantified the attributable risk and consequences of bone mineral density deficits, anchoring the skeletal surveillance schedule. [4] [5] [8] [7] [10]
The exposure-specific evidence includes the Clement International Guideline Harmonization Group and PanCareSurFup recommendations on thyroid cancer surveillance (2018), which set out the benefit-and-harm-balanced surveillance schedule for the irradiated survivor, and the Vatanen study of ovarian function after allogeneic stem cell transplantation (2014), which underpins the fertility-preservation counselling before conditioning. The Chemaitilly, Cohen, Mostoufi-Moab and Patterson review of endocrine late effects in childhood cancer survivors (2018) integrated the field for the oncology audience. [9] [11] [3]
In Australia and New Zealand, long-term follow-up of childhood cancer survivors is coordinated through the paediatric oncology long-term follow-up clinics at the major children's hospitals and the regional cancer services, aligned with the International Guideline Harmonization Group recommendations and the Endocrine Society guideline. Recombinant growth hormone for radiation-induced growth hormone deficiency is funded through the Pharmaceutical Benefits Scheme and the New Zealand equivalent under the growth-hormone programmes, contingent on a documented stimulation-test-confirmed deficiency and a stable magnetic resonance imaging scan. Fertility preservation counselling and, where appropriate, referral for oocyte or sperm cryopreservation before gonadotoxic conditioning is an expected standard, and the transition to adult survivorship care is supported by the state-based adolescent and young adult cancer services. Telehealth-shared care with regional and remote centres is the model that delivers surveillance to the survivor who cannot travel to the metropolitan clinic.
[2][6]Exam Pearls
A fellowship candidate answering on endocrine late effects of cancer treatment should land six anchor points and avoid four classic traps. The anchors are the exposure-based risk stratification (cranial radiation dose and field, alkylator cumulative dose, total-body irradiation, surgery) and the dose-dependent hierarchy of hypothalamic-pituitary damage — growth hormone at 18 Gy, gonadotropins at 24 to 30 Gy, TSH and ACTH above 30 to 40 Gy, panhypopituitarism at the highest. The remaining anchors are the paradoxical central precocious puberty of lower-dose cranial radiation, the structured surveillance schedule, the replacement order of hydrocortisone before levothyroxine before sex steroids with recombinant growth hormone only after magnetic resonance imaging, and the sick-day hydrocortisone education that prevents the fatal adrenal crisis. The traps are giving growth hormone before the MRI, giving thyroxine before cortisol, using the TSH to diagnose or titrate central hypothyroidism, and waiting for symptoms before screening. [1] [2] [6]
References
- [1]Chemaitilly W, Sklar CA. Childhood Cancer Treatments and Associated Endocrine Late Effects: A Concise Guide for the Pediatric Endocrinologist. Horm Res Paediatr, 2019.PMID 30404091
- [2]Sklar CA, Antal Z, Chemaitilly W, Cohen LE, Esiashvili N, Greenfield DM, et al. Hypothalamic-Pituitary and Growth Disorders in Survivors of Childhood Cancer: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab, 2018.PMID 29982476
- [3]Chemaitilly W, Cohen LE, Mostoufi-Moab S, Patterson BC. Endocrine Late Effects in Childhood Cancer Survivors. J Clin Oncol, 2018.PMID 29874130
- [4]Mostoufi-Moab S, Seidel K, Leisenring WM, Armstrong GT, Stovall M, Dietz AC, et al. Endocrine Abnormalities in Aging Survivors of Childhood Cancer: A Report From the Childhood Cancer Survivor Study. J Clin Oncol, 2016.PMID 27382091
- [5]Armstrong GT, Kawashima T, Leisenring W, Stratton K, Stovall M, Weathers RE, et al. Aging and risk of severe, disabling, life-threatening, and fatal events in the childhood cancer survivor study. J Clin Oncol, 2014.PMID 24638000
- [6]van Iersel L, Mulder RL, Denzer C, Cohen LE, Sklar CA, Edgar AB, et al. Hypothalamic-Pituitary and Other Endocrine Surveillance Among Childhood Cancer Survivors. Endocr Rev, 2022.PMID 34962573
- [7]Cohen LE. Endocrine late effects of cancer treatment. Endocrinol Metab Clin North Am, 2005.PMID 16085170
- [8]van Iersel L, Li Z, Srivastava DK, Brinkman TM, Wilson CL, Robison LL, et al. Hypothalamic-Pituitary Disorders in Childhood Cancer Survivors: Prevalence, Risk Factors and Long-Term Health Outcomes. J Clin Endocrinol Metab, 2019.PMID 31373627
- [9]Clement SC, Kremer LCM, Verburg FA, Simmons JH, Goldsby R, Links TP, et al. Balancing the benefits and harms of thyroid cancer surveillance in survivors of Childhood, adolescent and young adult cancer: Recommendations from the international Late Effects of Childhood Cancer Guideline Harmonization Group in collaboration with the PanCareSurFup Consortium. Cancer Treat Rev, 2018.PMID 29202445
- [10]Goodenough CG, Baedke JL, Delaney AM, Wilson CL, Bassetti MF, Lu Z, et al. Attributable Risk and Consequences of Bone Mineral Density Deficits in Childhood Cancer Survivors. JAMA Netw Open, 2025.PMID 39792384
- [11]Vatanen A, Wilhelmsson M, Borgström B, Gustafsson B. Ovarian function after allogeneic hematopoietic stem cell transplantation in childhood and adolescence. Eur J Endocrinol, 2014.PMID 24179099