Paeds · endocrinology-diabetes-and-growth
Hyperthyroidism and Graves disease
Also known as Thyrotoxicosis · Graves disease · Autoimmune hyperthyroidism · Neonatal thyrotoxicosis · Thyroid storm · Toxic diffuse goitre · TSH-receptor antibody disease
A fellowship approach to childhood thyrotoxicosis: confirm the hormone excess with a suppressed TSH and raised free T4, then make Graves disease the leading diagnosis through a positive TSH-receptor antibody, deliver symptom control with a beta-blocker while antithyroid drugs (carbimazole or methimazole first-line) control the gland, hold propylthiouracil for thyroid storm and first-trimester pregnancy because of hepatotoxicity, recognise the transient transplacental neonatal disease, and reach definitive radioactive iodine or surgery for relapse and non-adherence.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The fellowship mark goes to the candidate who separates two words that are routinely conflated. Thyrotoxicosis is the clinical and biochemical state of too much thyroid hormone in the tissues. Hyperthyroidism is the narrower term for the causes in which the gland itself is over-active — Graves disease, a toxic adenoma, a toxic multinodular goitre. Thyroiditis and exogenous hormone cause thyrotoxicosis but not hyperthyroidism, because the gland is leaking or being fed, not over-producing. The distinction matters because it decides the second-line test: after the suppressed TSH and raised free T4 confirm thyrotoxicosis, you ask whether the gland is over-producing (high radioiodine uptake) or leaking (low uptake), and the TSH-receptor antibody makes Graves the fast, non-radioactive answer in a child. [1] [3]
Overview & Definition
Hyperthyroidism and Graves disease together form the commonest endocrine cause of a thyrotoxic child in paediatric practice. Thyrotoxicosis is the state of excess thyroid hormone in the tissues, whatever its source; hyperthyroidism is the subset caused by true over-production by the gland; and Graves disease is the autoimmune disorder that accounts for the great majority of childhood cases. A stimulating immunoglobulin — the TSH-receptor antibody, also called thyroid-stimulating immunoglobulin — binds and activates the TSH receptor on the thyroid follicular cell, driving hormone synthesis and release without any check from the pituitary. The gland enlarges diffusely, vascularity increases, and free T4 and free T3 rise while TSH falls to undetectable. [1] [12]
The clinical face of the disease is the face of a body running too fast. Thyroid hormone up-regulates the β-adrenergic receptor, so the child is tachycardic, tremulous, heat-intolerant and anxious, with a bounding pulse and a wide pulse pressure. Metabolism speeds up, so appetite increases yet weight falls, and growth and skeletal maturation may accelerate. In the eye, retro-orbital lymphocytic and glycosaminoglycan infiltration produces the proptosis, lid retraction and diplopia that are unique to Graves and mark it out from every other cause of thyrotoxicosis. A fellow should leave the overview holding this image: a thyrotoxic child is, in effect, a child in a β-adrenergic storm, and the antibody is the switch that turned it on. [4] [10]
The disease is uncommon but not rare, and its incidence climbs steeply through childhood toward adolescence. Roughly one in ten thousand children under ten years is affected, rising through the early teenage years, with a strong female predominance and a clustering with other autoimmune diseases, Down syndrome and a family history of autoimmune thyroid disease. The neonate enters the topic through a separate door — the infant of a mother with current or past Graves disease, who may be born thyrotoxic from transplacental passage of maternal TSH-receptor antibody. The overview closes with the recognition that this is a chronic relapsing disease of children and young people, and that the paediatric task is as much about adherence, growth, school function and a safe transition to adult care as it is about the biochemistry. [6] [11]
Classification
The classification that earns marks is the uptake-and-cause classification, because it converts a single biochemical result — a suppressed TSH and a raised free T4 — into a treatable diagnosis. First, confirm thyrotoxicosis. Then divide the causes by whether the gland is over-producing hormone, leaking stored hormone, or being bypassed by external hormone or a TSH-driven process. The discriminator is the radioiodine or technetium uptake and, in practice for children, the TSH-receptor antibody, which is positive in Graves and negative in the leaky and exogenous causes. [1] [3]
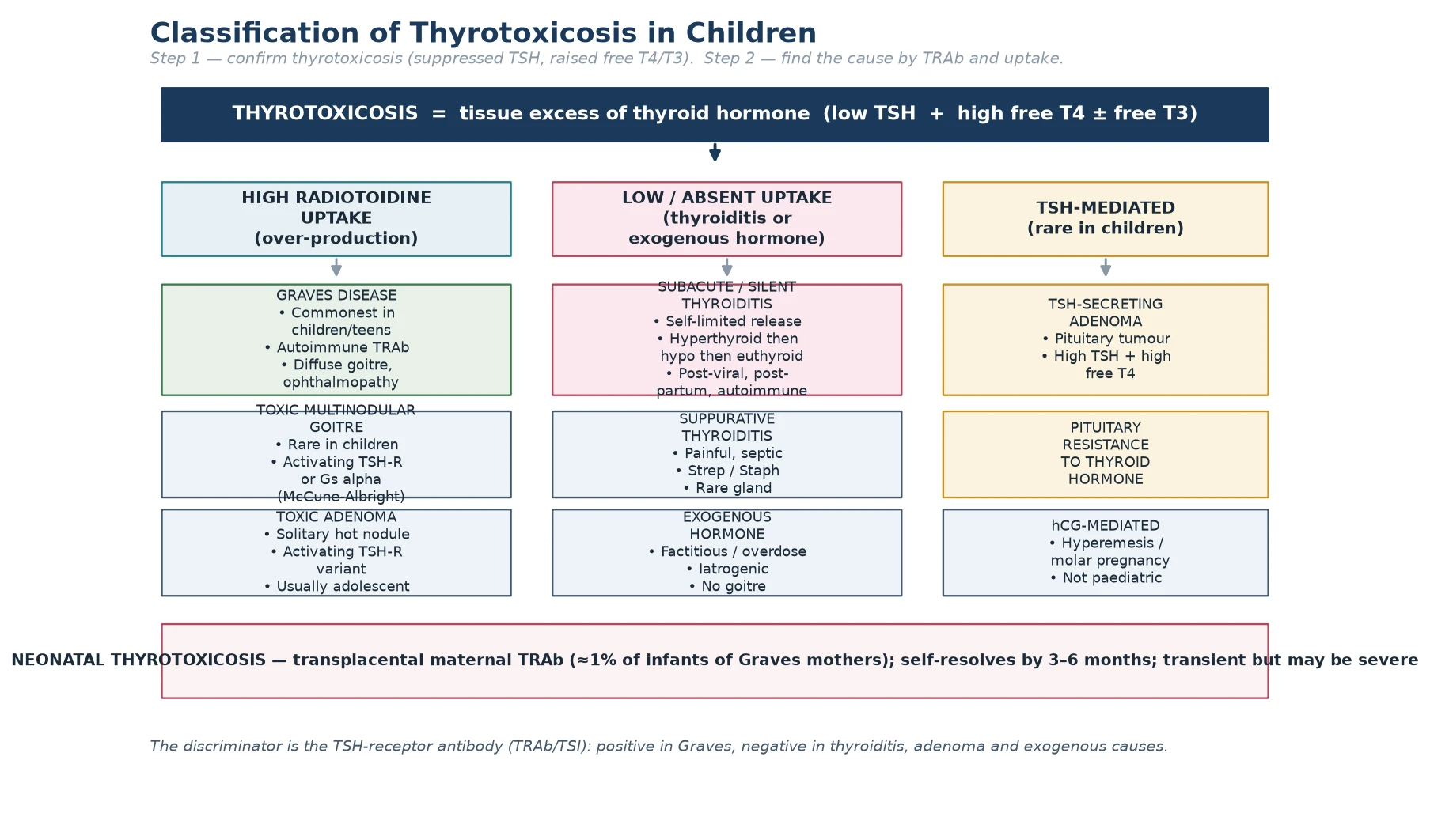
The high-uptake causes are the true hyperthyroidisms — the gland is over-producing. Graves disease dominates the paediatric list and is autoimmune. A toxic adenoma is a solitary, autonomously functioning nodule from an activating TSH-receptor variant, more often seen in adolescents. A toxic multinodular goitre is rare in children but appears in McCune–Albright syndrome, where a post-zygotic Gs-alpha mutation drives autonomous hormone synthesis alongside café-au-lait spots and fibrous dysplasia. The low-uptake causes release pre-formed hormone from a damaged gland and are self-limited — the painless or subacute thyroiditides (post-viral, autoimmune, or post-partum in an adolescent mother), suppurative thyroiditis, and exogenous or factitious hormone. The TSH-mediated causes are vanishingly rare in children — a TSH-secreting pituitary adenoma or pituitary resistance to thyroid hormone. [1] [2]
The paediatric classification adds one entity that has no place in the adult list: neonatal thyrotoxicosis, a transient disorder of the newborn caused by transplacental passage of maternal TSH-receptor antibody. It affects about one per cent of infants born to mothers with current or past Graves disease, it resolves as the maternal antibody clears over three to six months, and it can be severe enough to cause heart failure, craniosynostosis and developmental delay if missed. Placing neonatal thyrotoxicosis in the classification — alongside Graves, the toxic nodular diseases, the thyroiditides and the rare TSH-driven causes — is the move that shows the examiner you think across the whole age range. [11] [12]
Epidemiology & Risk Factors
Graves disease is the commonest cause of hyperthyroidism in children and adolescents, with an incidence of roughly 0.1 to 0.3 per thousand children per year in iodine-replete populations. The disease is uncommon before the age of five, rises through mid-childhood, and peaks in adolescence, with a female-to-male ratio around five to one. The peak incidence falls squarely in the early teenage years, so a thyrotoxic adolescent girl is the canonical presentation that a fellow should be able to generate from the epidemiology alone. [1] [12]
The strongest risk factors are female sex, adolescence, a family history of autoimmune thyroid disease, and the company of other autoimmune conditions — type 1 diabetes, Addison disease, coeliac disease and vitiligo — that mark a child with a biased immune system. Two chromosomal disorders raise the risk in a way that earns exam marks: Down syndrome and Turner syndrome both carry an excess of autoimmune thyroid disease, and a thyrotoxic girl with short stature and a Turner phenotype, or a thyrotoxic child with Down syndrome, should prompt both the thyroid panel and the chromosomal consideration. A maternal history of Graves disease is the defining risk factor for neonatal thyrotoxicosis, and the key teaching point is that the risk attaches to the antibody, not the mother's current thyroid status — a mother rendered hypothyroid after radioactive iodine still harbours the antibody and can still pass it to her fetus. [6] [11]
Recognition is unevenly distributed across the population. In remote and Indigenous communities, and in migrant and refugee families, the interval between symptom onset and a measured thyroid panel is longer, the access to paediatric endocrinology and nuclear medicine is narrower, and the burden of a daily, years-long drug regimen falls hardest on families with the least support. Non-adherence is the single biggest driver of relapse and of thyroid storm, and it clusters where health literacy, stable housing and continuity of care are weakest. A fellow who names this in a long case — and responds with a written plan, a single point of contact and a retrieval partnership — earns marks for the social as well as the biochemical dimension of the disease. [6] [7]
Pathophysiology
The pathophysiology of Graves disease is the pathophysiology of an antibody that does the pituitary's job without the pituitary's brake. In health, the hypothalamus releases thyrotropin-releasing hormone, the pituitary releases thyroid-stimulating hormone, and TSH binds the TSH receptor on the thyroid follicular cell to drive hormone synthesis and release; the rising free T4 then feeds back on the pituitary to suppress further TSH. In Graves disease, a stimulating immunoglobulin — the TSH-receptor antibody — binds the same receptor and activates it constitutively. The gland synthesises and releases T4 and T3 without any regard for the suppressed TSH, the follicles hypertrophy and become vascular, and the patient becomes biochemically and clinically thyrotoxic. [1] [4]
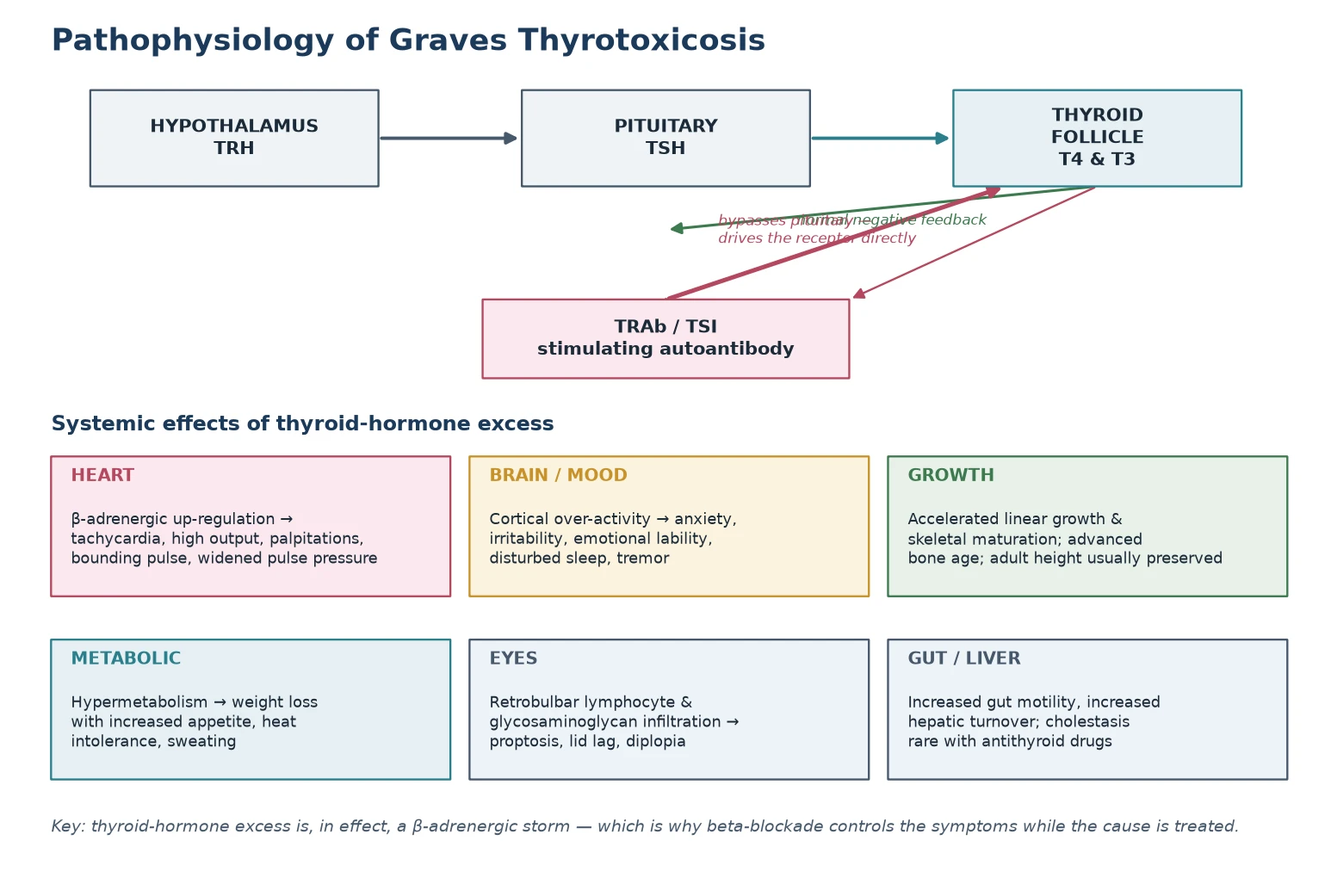
The systemic phenotype is the phenotype of thyroid-hormone excess acting on every tissue. In the heart, thyroid hormone up-regulates the β-adrenergic receptor and increases cardiac contractility and heart rate, producing tachycardia, a high-output circulation, a bounding pulse and a widened pulse pressure. In the brain and nervous system, cortical over-activity produces anxiety, irritability, emotional lability, a fine tremor and disturbed sleep — symptoms that are easily misread in an adolescent as a primary mental-health presentation. In the growing child, thyroid hormone accelerates bone turnover and skeletal maturation, so bone age advances and linear growth may transiently outpace peers, though final adult height is usually preserved once the disease is controlled. The metabolic effects — heat intolerance, sweating, weight loss with increased appetite — round out the picture of a body burning fuel too fast. [3] [4]
The eye is the one tissue where the antibody does damage that the hormone itself cannot explain. In Graves ophthalmopathy, TSH-receptor-bearing retro-orbital fibroblasts and adipocytes are infiltrated by lymphocytes and activated to produce glycosaminoglycans, which draw in water and swell the orbital contents within the rigid bony orbit. The result is proptosis, lid retraction, lid lag, conjunctival injection, and — when the swollen muscles impinge on the optic nerve — diplopia and even sight-threatening compressive optic neuropathy. This is why eye disease is unique to Graves and absent from every other cause of thyrotoxicosis: the antibody, not the hormone, drives it, and controlling the thyroid does not always control the eye. [10]
Clinical Presentation
The clinical presentation is the face of a body running too fast, and a fellow should be able to generate it from the pathophysiology. The adolescent with Graves disease typically presents with a goitre, palpitations, tremor, weight loss despite an increased appetite, heat intolerance and sweating, and a change in mood or behaviour — anxiety, irritability, emotional lability, falling school performance or disturbed sleep. The heart is fast, the pulse is bounding, the systolic pressure is up and the diastolic is down, widening the pulse pressure, and a thyroid bruit may be audible over the diffusely enlarged, soft or slightly firm goitre. The eye signs — proptosis, lid retraction, lid lag and diplopia — are the feature that marks the disease as Graves and not merely thyrotoxic. [4] [12]
In the younger child the presentation is less articulate and the diagnosis is more often missed. A pre-school or school-age child may present with behaviour change — hyperactivity, emotional lability, declining school performance — that is attributed to attention-deficit disorder or a family stressor until the growth chart reveals accelerated linear growth and the examination reveals a tachycardia and a goitre. Accelerated growth and advanced bone age are the paediatric signature that a thyrotoxic adult can never show, and they are the clue that turns a behavioural referral into an endocrine diagnosis. The family will often describe a child who is always hot, who eats voraciously yet thins, who trembles and sleeps badly, and whose energy is described as "wired" rather than healthy. [3] [6]
Neonatal thyrotoxicosis presents in the first days to weeks of life in an infant of a mother with current or past Graves disease. The transplacentally acquired TSH-receptor antibody drives the fetal and neonatal thyroid, producing tachycardia (often over 160 beats per minute), irritability, poor weight gain despite a voracious appetite, a goitre that may obstruct the airway, and — in severe cases — heart failure, hepatosplenomegaly, thrombocytopenia and premature craniosynostosis. The disease is transient, resolving as the maternal antibody clears over three to six months, but it can be fatal if unrecognised, and every infant of a mother with Graves disease — whether the mother is currently thyrotoxic, on antithyroid drugs, hypothyroid after treatment, or in remission — must have thyroid function and a TSH-receptor antibody checked at birth and monitored through the first months. [11] [12]
Why a mother who is now hypothyroid can still have a thyrotoxic baby
Because the risk travels with the antibody, not the mother's thyroid status. A woman treated with radioactive iodine or surgery for Graves disease no longer has a functioning thyroid and may be on thyroxine, but she still harbours the TSH-receptor antibody, and that antibody still crosses the placenta. Any maternal history of Graves disease — treated or untreated, active or burnt-out — is a risk factor for neonatal thyrotoxicosis, and the neonatal thyroid function and antibody must be checked regardless of the mother's current thyroid state. [11]
Differential Diagnosis
The differential depends on whether the child has true hyperthyroidism or one of the thyrotoxic-but-not-hyperthyroid causes. For the thyrotoxic child, the first divider is the TSH-receptor antibody and, where needed, the radioiodine or technetium uptake. Graves disease is positive for the antibody with a high, diffuse uptake. A toxic adenoma shows a single hot nodule on uptake with suppression of the rest of the gland. Subacute (de Quervain) thyroiditis presents with a painful, tender goitre, fever and a high erythrocyte sedimentation rate, and a low uptake that reflects the leaky gland. Painless or silent thyroiditis — autoimmune or post-partum — behaves the same way but without the pain. Exogenous hormone (factitious or iatrogenic) gives a flat uptake and no goitre. [1] [3]
The behavioural and cardiovascular presentation brings a wider differential. In an adolescent, the anxiety, tremor, palpitations and weight loss can be mistaken for a primary anxiety or panic disorder, an eating disorder with hyperactivity, or substance use (caffeine, sympathomimetics, cocaine). A tachycardia with hypertension raises phaeochromocytoma. In the younger child, the hyperactivity, inattention and emotional lability overlap with attention-deficit hyperactivity disorder. The discriminating move is always the thyroid panel: a suppressed TSH with a raised free T4 narrows the field instantly, and the TSH-receptor antibody then separates Graves from the rest. A fellow who reaches for the blood test early — rather than treating the behaviour — earns the mark. [4] [12]
For the neonate, the differential of a tachycardic, irritable, poorly growing infant includes sepsis, congenital heart disease and congenital hyperthyroidism. Congenital hyperthyroidism from a germline activating TSH-receptor variant is rare but persists beyond the neonatal period and shows a family pattern, distinguishing it from transient neonatal thyrotoxicosis. The discriminating test is again the TSH-receptor antibody — high in both mother and baby in the transient transplacental form — together with the time course, as the transplacental antibody wanes over months. [11] [1]
Clinical & Bedside Assessment
The bedside assessment has two speeds. In the thyrotoxic or thyroid-storm presentation, the immediate questions are the haemodynamics and the brain: heart rate, rhythm, blood pressure, temperature, perfusion and conscious state, while drawing blood for thyroid function and a beta-natriuretic peptide if heart failure is suspected. A thyrotoxic child who is febrile, markedly tachycardic and confused is thyroid storm until proven otherwise, and the assessment moves straight to PICU resuscitation rather than waiting for the laboratory. In the more common elective presentation, the assessment is a careful history and a focused examination that documents the features that will guide treatment and that the examiner listens for in a long or short case. [1] [3]
The thyroid examination sits at the centre of the short case. Inspect from the front for a goitre, eye signs and a flushed face; palpate from behind with the child sitting upright, swallowing sips of water, to assess the size, consistency and surface of the gland and to feel for nodules; auscultate for a bruit over each lobe, which reflects the increased vascularity of Graves. Document the eye signs specifically — proptosis (measured with an exophthalmometer where available), lid retraction and lid lag, conjunctival injection, chemosis, and diplopia on cardinal positions of gaze — because their presence and severity drive the ophthalmology referral. The cardiovascular examination documents the heart rate, rhythm, blood pressure, pulse character and any signs of heart failure, and the neurological examination documents the fine tremor, the brisk reflexes and the proximal muscle strength. [2] [10]
The history and growth assessment is where the paediatric mark is won. Plot the height and weight on an age-appropriate growth chart and note accelerated linear growth; assess pubertal stage using Tanner staging, because thyroid disease disturbs the timing of puberty; take a dietary and weight history that captures the paradox of weight loss with increased appetite; and take a careful family history of autoimmune thyroid disease and other autoimmune conditions. Document the school and behavioural history — declining performance, anxiety, irritability, sleep — because these are often the presenting complaint and the marker of treatment response. The problem representation that follows should be one sentence: for example, "A thirteen-year-old girl with a diffuse goitre, proptosis, tachycardia, weight loss and behavioural change, biochemically thyrotoxic with a positive TSH-receptor antibody, consistent with Graves disease." [6] [12]
Investigations
The investigation strategy is tiered and, in a child, usually settles the diagnosis without a radioiodine scan. The first tier is the thyroid function panel: TSH is suppressed to undetectable, free T4 is raised, and free T3 is raised — sometimes disproportionately (T3 toxicosis) in early or mild disease. A suppressed TSH with a high free T4 confirms thyrotoxicosis, and the degree of elevation reflects the severity. The same sample should carry the TSH-receptor antibody, which is now both diagnostic and prognostic: a positive result confirms Graves disease, and a high titre predicts a lower chance of remission and a higher risk of relapse after antithyroid drugs are stopped. [1] [5]
The second tier settles the rare or ambiguous case. When the TSH-receptor antibody is negative, the discriminator is the radioiodine or technetium-99m uptake scan: a high diffuse uptake confirms Graves, a single hot focus a toxic adenoma, a low or absent uptake a thyroiditis or exogenous hormone. A painful tender goitre with a raised erythrocyte sedimentation rate and C-reactive protein points to subacute thyroiditis. Thyroid peroxidase antibodies are positive in both Graves and Hashimoto thyroiditis and are not diagnostic on their own, but they support an autoimmune background and, in the mother, help estimate the risk of neonatal disease. Thyroid ultrasound is useful to characterise a nodule or a multinodular goitre but is not needed to diagnose Graves, which is an antibody diagnosis. [1] [3]
Once the diagnosis is confirmed, the monitoring panel follows the treatment and the adverse effects. Repeat the free T4 every four to six weeks during dose titration, then every three months once stable, and check the full blood count and liver function at baseline and whenever a child on an antithyroid drug develops fever, sore throat, jaundice or abdominal pain. The bone age, growth and pubertal assessment are the paediatric markers of long-term control, and the school and behavioural history is the functional marker. The recognition that investigation is not a one-off but a years-long monitoring programme is the mark of a paediatric endocrine mindset. [6] [7]
Management — Resuscitation
The resuscitation move is to quiet the β-adrenergic storm. A beta-blocker — propranolol at a paediatric dose of around 0.5 to 2 mg/kg per day in divided doses — controls the tachycardia, tremor, anxiety and heat intolerance within hours, and it is the bridge that carries the child safely while the antithyroid drugs take effect over weeks. In a child with asthma, a cardioselective agent such as atenolol is preferred, and in the neonate a beta-blocker is used cautiously because of the risk of hypoglycaemia and bradycardia. [1] [7]
The thyroid-storm resuscitation is the one place where propylthiouracil still leads. Thyroid storm is rare in children but lethal when missed, and it presents with hyperpyrexia, severe tachycardia or arrhythmia, heart failure, agitation, delirium or coma. The treatment is four-pronged and given together: block synthesis with propylthiouracil (which also blocks the peripheral conversion of T4 to T3); block release with iodine ( Lugol's solution or saturated potassium iodide) given at least one hour after the thionamide; block the peripheral effects with a beta-blocker and corticosteroids (hydrocortisone, which also blocks T4-to-T3 conversion); and support the child with cooling, fluids, oxygen and treatment of the precipitant. Admission to PICU is mandatory. [1] [3]
Resuscitation is not finished until the precipitant is found and the family is enrolled in the long-term plan. In a child presenting with storm, the common precipitants are non-adherence to antithyroid drugs, intercurrent infection, surgery, and diabetic ketoacidosis — each of which must be addressed. The acute phase settles over days, the propylthiouracil is converted to carbimazole or methimazole for maintenance, and the family is given a clear written emergency plan, a single point of contact and a date for endocrine follow-up. The resuscitation phase is the bridge into the definitive management ladder, and the fellow who treats it as a system rather than a single prescription earns the mark. [1] [7]
Management — Definitive & Stepwise
The definitive management of Graves disease in a child is a three-option ladder — antithyroid drugs, radioactive iodine, and surgery — built on a foundation of symptom control and delivered over years. Antithyroid drugs are the first-line choice for nearly every child, because they preserve the gland, are reversible, and avoid lifelong thyroxine. The thionamides are carbimazole (or its active metabolite methimazole), which block the organification of iodide and the coupling of iodotyrosines, and propylthiouracil, which additionally blocks the peripheral conversion of T4 to T3. In children, carbimazole or methimazole is preferred at a starting dose of roughly 0.25 to 1 mg/kg per day, because it is dosed once daily, is more effective, and carries a lower risk of liver failure than propylthiouracil. [1] [8]
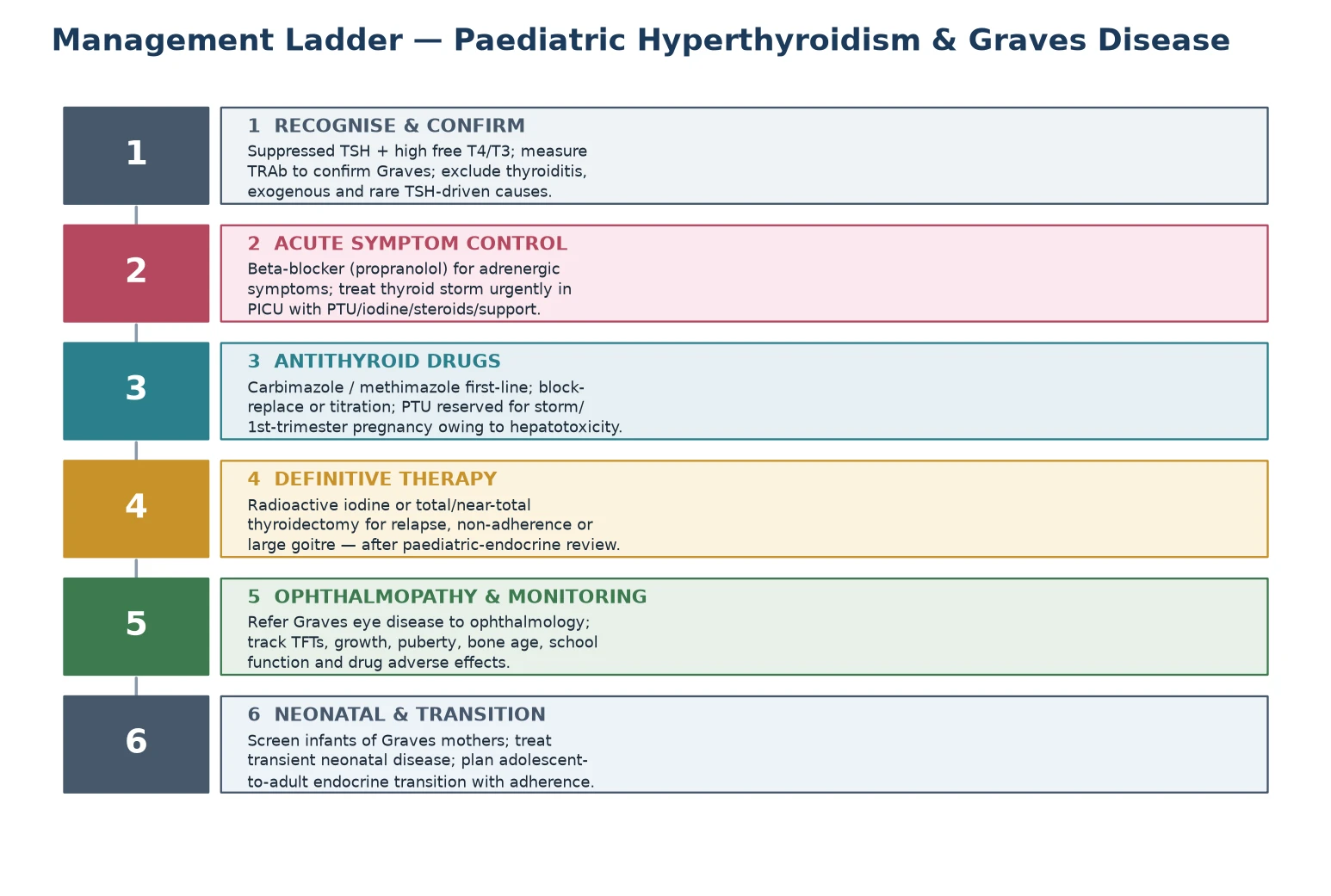
There are two dosing strategies. In the titration regimen, the thionamide is started at a standard dose and tapered as the patient becomes euthyroid, aiming for the lowest dose that maintains normal thyroid function. In the block-and-replace regimen, a higher dose of thionamide fully suppresses endogenous hormone while replacement levothyroxine is added back; this avoids over-treatment hypothyroidism but uses two drugs and more clinic visits. Current paediatric practice favours the titration regimen with carbimazole or methimazole, given once daily, with free T4 checked every four to six weeks during titration and every three months once stable. Treatment is typically continued for two to three years before a trial of withdrawal, because roughly half to two-thirds of children relapse after the drugs are stopped, and the relapse rate is highest in those with a large goitre, a high TSH-receptor antibody titre, and severe biochemical disease at diagnosis. [1] [5] [6]
The definitive therapies — radioactive iodine and surgery — are held in reserve for the child who relapses, cannot adhere to or tolerate the drugs, or has a large or symptomatic goitre. Radioactive iodine (I-131) ablates the gland and renders the patient hypothyroid, requiring lifelong levothyroxine; it is highly effective and, in children old enough to swallow the capsule, avoids surgery, though it is generally avoided in very young children and in active, severe ophthalmopathy. Total or near-total thyroidectomy is the surgical alternative, performed by a high-volume endocrine surgeon, with the risks of recurrent laryngeal nerve injury, hypoparathyroidism and the need for lifelong thyroxine and calcium. In a child, the choice between drugs, iodine and surgery is made jointly with a paediatric endocrinologist, the family and — for surgery — a specialist surgeon, and the decision turns on the likelihood of remission, the burden of years of drugs, and the local availability of nuclear medicine and expert surgery. [1] [7]
Specific Subtypes & Scenarios
Neonatal thyrotoxicosis is the transient disease of the infant born to a mother with current or past Graves disease. Transplacentally acquired TSH-receptor antibody drives the fetal and neonatal thyroid, producing tachycardia, irritability, poor weight gain, a goitre and, in severe cases, heart failure, craniosynostosis and developmental delay. Treatment is methimazole (or propylthiouracil if the mother is breastfeeding and the clinical situation demands), a beta-blocker for symptom control, and supportive care; the dose is tapered as the maternal antibody clears over three to six months. The key teaching point is surveillance: every infant of a mother with a history of Graves disease — treated or untreated — has thyroid function and a TSH-receptor antibody checked at birth and monitored through the first months, because the disease can be fatal if missed yet self-resolves if found. [11] [12]
Thyroid storm is the decompensated extreme of thyrotoxicosis and the one true endocrine emergency in this topic. It presents with hyperpyrexia, severe tachycardia or arrhythmia, heart failure, agitation, delirium or coma, and it is triggered by non-adherence, infection, surgery or diabetic ketoacidosis. Management is four-pronged and simultaneous — propylthiouracil, iodine, a beta-blocker with corticosteroids, and supportive care in PICU — and the diagnosis is clinical, made and treated before the laboratory confirms it. The fellow who recognises storm in a thyrotoxic child who is febrile and confused, and who delivers the four-pronged regimen without waiting, is the one who saves the life. [1] [3]
Severe Graves eye disease is less common in children than in adults, but when it occurs it demands ophthalmology input — for proptosis measurement, diplopia assessment, corneal protection and, rarely, urgent decompression for sight-threatening compressive optic neuropathy. Smoking is the chief modifiable risk factor for ophthalmopathy progression in adults and older adolescents, so smoking-cessation counselling is part of the management. In ANZ, paediatric ophthalmology and endocrine services are co-located in the major children's hospitals, and children in remote regions are supported by telehealth between visits; the written plan should name the local eye service and the threshold for urgent review. [10]
Hashitoxicosis is the transient thyrotoxic phase of autoimmune (Hashimoto) thyroiditis, in which the gland leaks stored hormone before progressing to hypothyroidism. It is distinguished from Graves by a negative or modest TSH-receptor antibody, a low radioiodine uptake, and a self-limited course — management is a beta-blocker for symptoms and watchful waiting, not antithyroid drugs, with the expectation that the child will move through a hypothyroid phase and may need thyroxine. Subacute (de Quervain) thyroiditis follows a viral illness with a painful tender goitre, fever, a high erythrocyte sedimentation rate and a low uptake; treatment is analgesia, a beta-blocker and, in severe cases, corticosteroids. Both remind the fellow that not every thyrotoxic child needs a thionamide. [1] [3]
Complications & Pitfalls
The complications divide into those of the disease and those of its treatment. Disease complications include heart failure and arrhythmia from uncontrolled tachycardia, growth and pubertal disturbance, school and behavioural dysfunction, the cosmetic and visual burden of ophthalmopathy, and the psychosocial burden of a chronic relapsing illness in an adolescent. Drug complications are the two dangers that must never be missed: agranulocytosis (fever, sore throat, sepsis — stop the drug, check the neutrophils) and hepatotoxicity, which is the central reason propylthiouracil is no longer first-line in children and carries a boxed warning for fulminant liver failure. The shift in paediatric prescribing from propylthiouracil to carbimazole and methimazole, documented across two decades, was driven entirely by the liver-failure signal in children. [8] [9]
The surgical complications of thyroidectomy are recurrent laryngeal nerve injury (hoarseness, airway compromise), hypoparathyroidism (hypocalcaemia), scar, and the guaranteed need for lifelong thyroxine; these are minimised by a high-volume endocrine surgeon. Radioactive iodine renders the patient hypothyroid and lifelong levothyroxine-dependent, and it can transiently worsen ophthalmopathy if the eye disease is active and severe. The cognitive traps that cost marks are three: treating a thyroiditis with antithyroid drugs; missing the diagnosis in a younger child because the presentation is behavioural; and forgetting that a mother rendered hypothyroid by treatment still carries — and still passes — the antibody to her fetus. [1] [7]
After two to three years of antithyroid drugs, roughly half to two-thirds of children relapse, and the relapse is predicted by a large goitre, a high TSH-receptor antibody titre, severe biochemical disease at diagnosis and young age at onset. The response to relapse is not automatic re-prescription but a shared decision: continue the drugs long-term (the argument advanced for children, because remission can come with time), or move to definitive radioactive iodine or surgery. Families value being told early that this is a years-long, sometimes lifelong, disease, and that the goal is a euthyroid, thriving child — however that is achieved. [5] [6]
The surveillance programme for a child with Graves disease tracks more than the free T4. It includes growth and pubertal progress, bone age, school and behavioural function, the eye examination, the full blood count and liver function while on drugs, and — for the adolescent — reproductive and bone-health counselling and a planned transition to adult endocrine care. Setting up this surveillance at the first visit, naming the team members (paediatric endocrinologist, general paediatrician, ophthalmologist, primary care, nurse specialist, psychologist), and giving the family a single written plan is the disposition that prevents the complications. [6] [12]
Prognosis & Disposition
The prognosis of childhood Graves disease is the prognosis of a chronic, relapsing but treatable disease. With antithyroid drugs, most children achieve biochemical control within weeks and remain euthyroid while on treatment, though roughly half to two-thirds relapse when the drugs are withdrawn, and those with a large goitre, a high antibody titre and severe disease at diagnosis relapse most often. Long-term medical therapy — continuing the thionamide for years or indefinitely — is an increasingly accepted strategy in children, because the relapse rate after a standard two-year course is high and the alternative is definitive ablation and lifelong thyroxine. [5] [6]
Definitive therapy changes the prognosis from relapsing to stable hypothyroidism. Radioactive iodine and surgery both render the patient thyroxine-dependent, and the prognosis then turns on adherence to once-daily levothyroxine and annual monitoring — a simpler regimen than years of thionamides, but one that demands lifelong engagement. Neonatal thyrotoxicosis carries the best prognosis of all once recognised: it is transient, resolving over three to six months as the maternal antibody clears, and the infant is typically euthyroid thereafter, though severe unrecognised disease can leave residual developmental and cardiac effects. The disposition for every child is lifelong endocrine follow-up, structured around the growth, pubertal, school and transitional milestones of childhood and adolescence. [11] [12]
The adolescent-to-adult transition is the disposition point that most often fails, because the late teenage years are exactly when non-adherence peaks and continuity of care fragments. A structured transition — begun in early adolescence, with a named adult endocrinologist, a written summary, a reproductive and bone-health discussion, and a handover that does not assume the young person will re-present — is the single intervention most likely to preserve the gains of paediatric care. The fellow who frames the disposition around the whole developmental trajectory — not just the next free T4 — earns the mark that separates a competent from a thoughtful candidate. [6] [7]
Special Populations
In remote and Indigenous communities, and in migrant and refugee families, the barriers to good Graves care are concrete: distance from paediatric endocrinology and nuclear medicine, language and health-literacy barriers to a years-long drug regimen, and the social determinants that drive non-adherence and relapse. The practical response is a written location-specific plan, a single point of contact, telehealth linkage to the tertiary endocrine service, a low threshold to test a thyrotoxic presentation, and a retrieval partnership for thyroid storm. Recognising that non-adherence in these settings is a systems problem rather than a personal failing — and designing the plan around it — is the paediatric response that earns marks for equity. [6] [7]
The adolescent-to-young-adult transition is the population that owns the highest risk of disengagement, relapse and storm. Structured transition planning, reproductive and bone-health counselling (thyroid disease and its treatment affect menstruation, fertility and bone density), mental-health support for the anxiety and mood components of the disease, and a named adult provider are the elements of a transition that holds. The pregnant adolescent with Graves disease needs special attention, because propylthiouracil is preferred in the first trimester (to minimise teratogenic risk) and carbimazole or methimazole thereafter, and because the TSH-receptor antibody crosses the placenta and threatens the fetus — making the obstetric–endocrine liaison and the neonatal surveillance essential. [1] [11]
The neonate is the population in whom the disease is most easily missed. Every infant of a mother with a history of Graves disease — treated or untreated, active or burnt-out — has cord-blood or neonatal thyroid function and a TSH-receptor antibody checked, and is monitored through the first months for the transient disease. The child with Down syndrome or Turner syndrome is at increased risk of autoimmune thyroid disease and is usually under surveillance already, so a thyrotoxic presentation in these children should prompt the full panel and the antibody rather than being attributed to the baseline phenotype. Multidisciplinary team members — paediatric endocrinologist, general paediatrician, ophthalmologist, primary care, nurse specialist, dietitian, psychologist and, for surgery, a high-volume endocrine surgeon — are essential to the outcome, and naming them in a long case demonstrates the systems thinking that the examination rewards. [12] [6]
Evidence, Guidelines & Regional Differences
The two guidelines that anchor practice are the 2016 American Thyroid Association hyperthyroidism guidelines (Ross and colleagues), which set out the diagnosis, the antithyroid-drug-first strategy, the propylthiouracil caveat and the role of definitive therapy, and the earlier 2011 ATA/AACE guidelines (Bahn and colleagues) that preceded them. The 2016 document remains the working standard for paediatric and adult practice and is the citation to give for the treatment ladder. The 2023 Lancet Diabetes and Endocrinology review (Wiersinga and colleagues) and the 2016 Lancet review (De Leo and colleagues) are the two modern overviews that a fellow should cite for mechanism and differential. [1] [2] [3]
The paediatric evidence base is built on three strands. The Kaguelidou relapse-prediction study quantified the factors that predict relapse after antithyroid drugs — large goitre, high antibody titre, severe disease, young age — and gives the fellow the numbers to counsel a family on the likelihood of remission. The Léger and Carel argument for prolonged antithyroid drugs in children reframed paediatric management away from an early drive toward definitive ablation and toward a recognition that children relapse often and that years of medical therapy are reasonable. And the propylthiouracil hepatotoxicity work of Rivkees and Mattison, together with the prescribing-shift data of Emiliano and Cooper, drove the move away from propylthiouracil in children — the clearest example in the topic of a pharmacovigilance signal changing practice. [5] [6] [8] [9]
In Australia and New Zealand, paediatric Graves disease is managed in tertiary children's-hospital endocrine services with linked nuclear medicine and ophthalmology, and infants of Graves mothers are screened through established maternal–neonatal pathways. Radioactive iodine is available but used selectively in children, and surgery is centralised to high-volume centres — a pattern that supports the antithyroid-drug-first default. In regions without paediatric nuclear medicine or paediatric surgical expertise, the long-term medical strategy dominates by necessity, and the written plan and telehealth linkage are the tools that close the gap. The fellow should name the local pathway in a long case. [1] [6]
The controversies that a higher-level candidate should hold are three. First, the duration of antithyroid therapy: the traditional two-year course against the prolonged or indefinite strategy, given the high relapse rate. Second, the role of radioactive iodine in young children: highly effective but generally avoided in the very young, and debated in the context of long-term safety. Third, the management of mild or subclinical disease and of Graves ophthalmopathy in childhood, where the evidence is thinner and practice varies. Holding these openly — rather than pretending the answers are settled — is the mark of a candidate who reads the literature rather than memorises it. [3] [6]
Exam Pearls
The six anchor points a fellowship candidate should land are these. First, the definition split: thyrotoxicosis is the state, hyperthyroidism is the over-production subset, Graves is the autoimmune antibody-driven cause. Second, the diagnostic trio: suppressed TSH, raised free T4, positive TSH-receptor antibody — which usually settles the diagnosis in a child without a scan. Third, the drug rule: carbimazole or methimazole first-line, propylthiouracil reserved for thyroid storm and first-trimester pregnancy because of fulminant liver failure in children. Fourth, the two drug dangers: agranulocytosis with fever or sore throat, hepatotoxicity with jaundice or abdominal pain — warn every family, check the relevant test. Fifth, the neonatal rule: every infant of a mother with a history of Graves disease — treated or not — is screened, because the antibody travels with the history, not the current thyroid status. Sixth, the relapse reality: half to two-thirds of children relapse after two years, predicted by goitre size, antibody titre and severity, and the response is a shared decision between prolonged drugs and definitive therapy. [1] [6] [9]
T.H.Y.R.O.I.D. — the paediatric Graves work-up
The high-yield one-liners that earn the mark: a thyrotoxic child is Graves until proven otherwise; the eye signs are the fingerprint of Graves; thyroid storm is clinical, treated before the lab confirms it; propylthiouracil causes fulminant liver failure in children — that is why it is not first-line; neonatal thyrotoxicosis is transient and resolves as the maternal antibody clears over three to six months; and the disposition is a years-long, sometimes lifelong, endocrine programme built around the developmental trajectory of the child. The fellow who can generate the whole topic from the single image of an antibody switching on the gland — and who lands each of these six anchor points — will pass the station. [3] [4] [12]
References
- [1]Ross DS, Burch HB, Cooper DS, Greenlee MC, Laurberg P, Maia AL, et al. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid, 2016.PMID 27521067
- [2]Bahn RS, Burch HB, Cooper DS, Garber JR, Greenlee MC, Klein I, et al. Hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Endocr Pract, 2011.PMID 21700562
- [3]Wiersinga WM, Poppe KG, Effraimidis G. Hyperthyroidism: aetiology, pathogenesis, diagnosis, management, complications, and prognosis. Lancet Diabetes Endocrinol, 2023.PMID 36848916
- [4]De Leo S, Lee SY, Braverman LE. Hyperthyroidism. Lancet, 2016.PMID 27038492
- [5]Kaguelidou F, Alberti C, Castanet M, Guitteny MA, Czernichow P, Léger J. Predictors of autoimmune hyperthyroidism relapse in children after discontinuation of antithyroid drug treatment. J Clin Endocrinol Metab, 2008.PMID 18628515
- [6]Léger J, Carel JC. MANAGEMENT OF ENDOCRINE DISEASE: Arguments for the prolonged use of antithyroid drugs in children with Graves' disease. Eur J Endocrinol, 2017.PMID 28381452
- [7]Rivkees SA. Pediatric Graves' disease: management in the post-propylthiouracil Era. Int J Pediatr Endocrinol, 2014.PMID 25089127
- [8]Emiliano AB, Governale L, Parks M, Cooper DS. Shifts in propylthiouracil and methimazole prescribing practices: antithyroid drug use in the United States from 1991 to 2008. J Clin Endocrinol Metab, 2010.PMID 20335447
- [9]Rivkees SA, Mattison DR. Propylthiouracil (PTU) Hepatoxicity in Children and Recommendations for Discontinuation of Use. Int J Pediatr Endocrinol, 2009.PMID 19946400
- [10]Bahn RS. Graves' ophthalmopathy. N Engl J Med, 2010.PMID 20181974
- [11]Polak M. Hyperthyroidism in early infancy: pathogenesis, clinical features and diagnosis with a focus on neonatal hyperthyroidism. Thyroid, 1998.PMID 9920374
- [12]Léger J. Graves' disease in children. Endocr Dev, 2014.PMID 25231452