Paeds · endocrinology-diabetes-and-growth
Hypoglycaemia in diabetes
Also known as Insulin-induced hypoglycaemia · Severe hypoglycaemia · Impaired awareness of hypoglycaemia · Nocturnal hypoglycaemia · Hypoglycaemia-associated autonomic failure · HAAF · Dead-in-bed syndrome
A fellowship approach to hypoglycaemia in children and adolescents with diabetes: recognise the autonomic-to-neuroglycopenic slide and the silent nocturnal event as the single greatest barrier to safe intensive therapy, classify severity by the ISPAD/ADA levels, understand why the glucagon and adrenaline counter-regulation fails in type 1 diabetes and produces impaired awareness (HAAF), and deliver the rule of 15 for mild events and glucagon or intravenous dextrose for severe events — then prevent recurrence with continuous glucose monitoring, hybrid closed-loop delivery, structured education, and insulin-adjustment skills.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The unifying teaching point is that hypoglycaemia is the single greatest barrier to safe intensive insulin therapy. The Diabetes Control and Complications Trial proved that intensive control prevents long-term microvascular complications, but at the price of a threefold increase in severe hypoglycaemia — a finding that reshaped paediatric diabetes care into a constant negotiation between lowering the HbA1c and protecting the brain. [4] [1]
Overview & Definition
Hypoglycaemia in diabetes is a low blood glucose produced by the imbalance between insulin action and available substrate — too much insulin, too little food, too much exercise, or a combination of all three. The threshold at which harm begins is lower than the threshold at which symptoms appear, which is why the ISPAD guidelines define a glucose below 3.9 millimoles per litre (70 milligrams per decilitre) as an alert value that should prompt review, and below 3.0 millimoles per litre (54 milligrams per decilitre) as a clinically important event that demands action. A severe event is defined not by a number but by the child's functional state: any hypoglycaemia associated with altered mental or physical status that requires another person to administer treatment. [1]
Clinically, the condition matters because the brain depends on glucose as its obligate fuel, and a child with type 1 diabetes has lost the insulin arm of the body's glucose-defence system and partially lost the glucagon arm as well. The result is that each episode is both an immediate emergency — a starved brain can seize and injure itself — and a signal that the therapy has outrun the physiology. The framing matters because it dictates management: the priority is to treat first and analyse the cause afterwards, because the recovery of the brain is time-critical and the analysis can wait. [3] [2]
Classification
The classification that earns marks runs along two axes, because severity and mechanism together predict both the immediate treatment and the risk of recurrence. The first axis is biochemical severity, which the ISPAD and ADA consensus now frame in three levels: a Level 1 alert below 3.9 millimoles per litre, a Level 2 clinically important event below 3.0, and a Level 3 severe event defined by altered consciousness requiring assistance regardless of the actual glucose value. The second axis is the clinical and mechanistic pattern, which tells you why the event happened and how to stop the next one. [1]
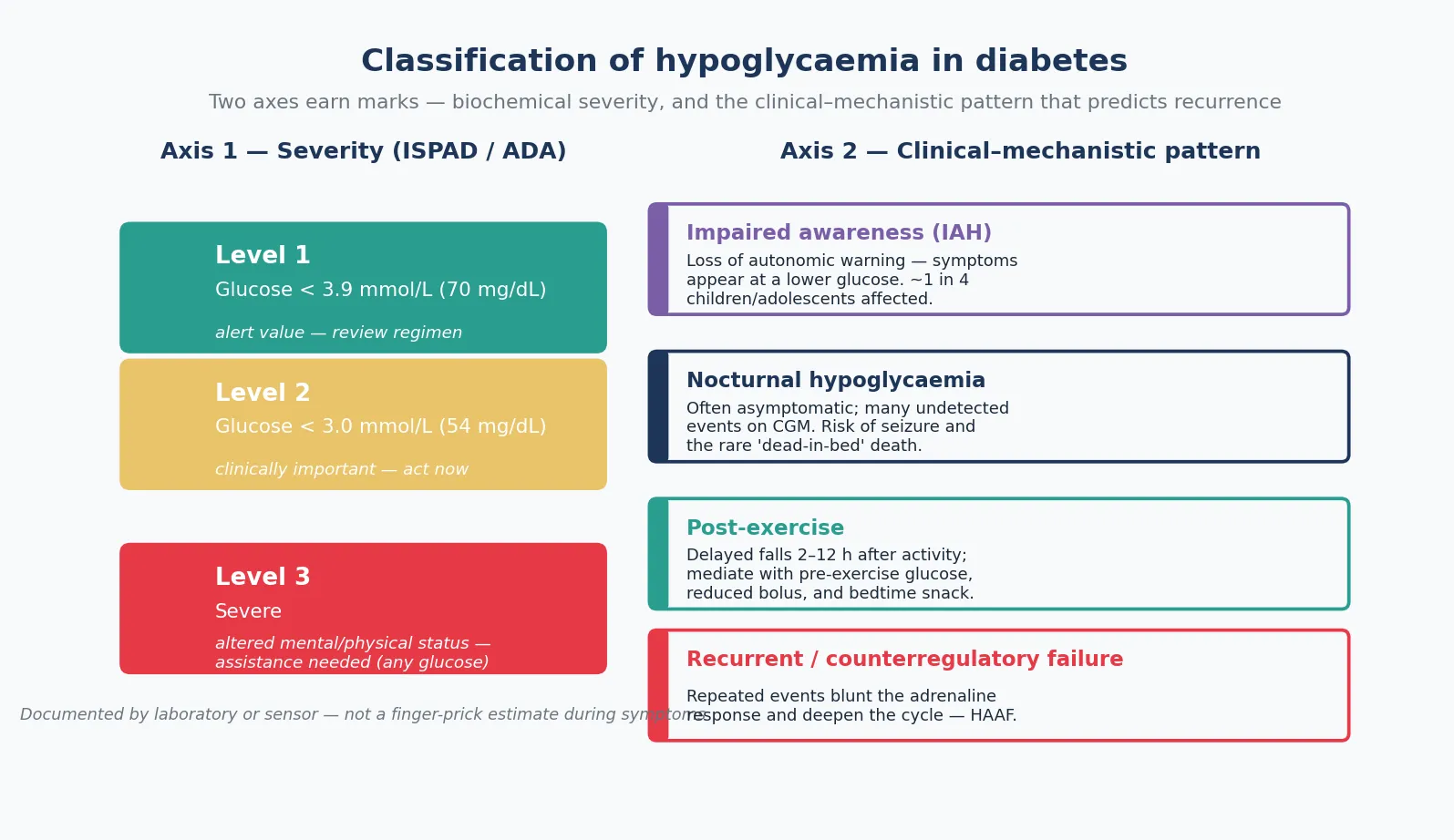
The mechanistic patterns are where the real clinical thinking lives. Impaired awareness of hypoglycaemia is the loss of the autonomic warning — the tremor, sweating and palpitations that normally appear before the brain falters — so the first symptom the child experiences is confusion or collapse itself, and it affects roughly one in four children and adolescents with type 1 diabetes. Nocturnal hypoglycaemia is frequently asymptomatic, detected only on continuous monitoring, and carries the dual dangers of an unwitnessed seizure and, rarely, the dead-in-bed syndrome. Post-exercise hypoglycaemia is delayed, appearing two to twelve hours after activity as muscle continues to take up glucose and replenish glycogen. Recurrent or counterregulatory-failure hypoglycaemia is the engine that powers all the others, because each event blunts the adrenaline response that protects the next one. [8] [2]
| Feature | Autonomic (early) | Neuroglycopenic (late) |
|---|---|---|
| Typical glucose | 3.3–3.8 mmol/L | Below 3.0 mmol/L |
| Symptoms | Tremor, sweating, palpitations, hunger, anxiety | Confusion, drowsiness, blurred vision, slurred speech, unsteadiness |
| In young children | Irritability, pallor, behavioural change | Seizure, collapse, coma |
| Action | Self-treat with fast-acting carbohydrate | May need assistance, glucagon, or IV dextrose |
Epidemiology & Risk Factors
Severe hypoglycaemia remains common in paediatric type 1 diabetes despite modern therapy. The Diabetes Control and Complications Trial established the central trade-off: intensive insulin therapy, which halves the long-term microvascular complications, also triples the rate of severe hypoglycaemia to roughly 0.6 events per patient-year in adolescents. That finding defined the field, because it showed that the brain and the kidney pull in opposite directions, and that the paediatric diabetes team must steer between them. [4]
[7]The risk factors cluster into three groups. The child-related factors are young age (toddlers cannot report symptoms and have erratic intake and activity), a previous severe event, and impaired awareness of hypoglycaemia, which is the single strongest predictor of the next severe event. The regimen-related factors are lower HbA1c combined with unawareness, long-acting or mismatched insulin doses, and the early weeks of pump or closed-loop therapy before settings are tuned. The situational factors are exercise, alcohol in adolescents, missed or delayed meals, gastrointestinal illness, and errors in carbohydrate counting or pump priming. Socioeconomic disadvantage, remote residence, and limited access to technology or education widen the gap further. [8] [1]
Pathophysiology
The normal defence against a falling glucose runs in three tiers, and understanding their order is the key to why type 1 diabetes is so vulnerable. As glucose drops, insulin secretion normally falls first, which both stops further glucose uptake and releases the brake on the liver; glucagon then rises to drive hepatic glucose output; and if those fail, adrenaline, cortisol and growth hormone rise as the back-up system. The autonomic surge that produces tremor, sweating and palpitations is the same adrenaline response, and it is the body's early-warning alarm. [2] [3]
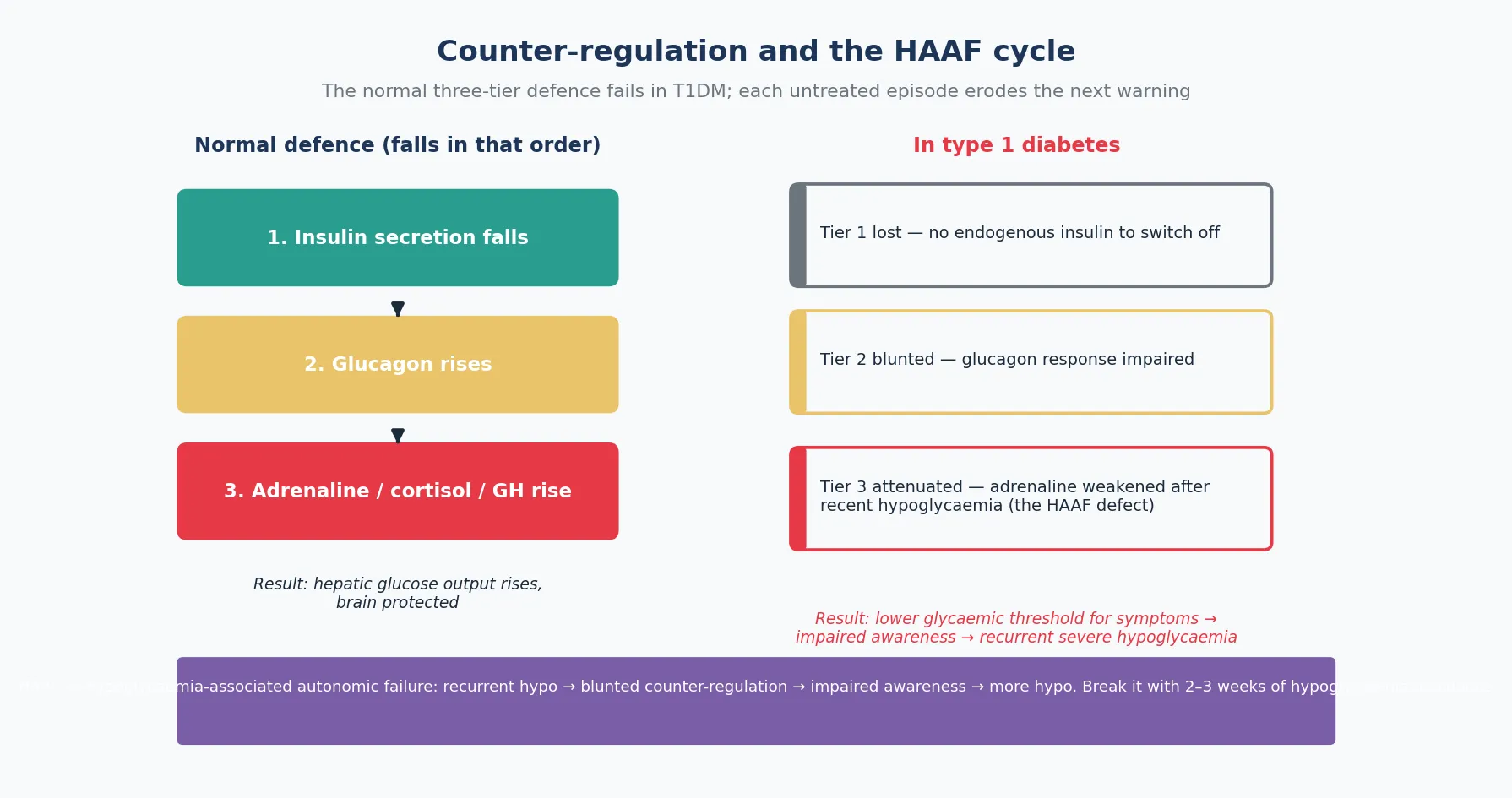
In type 1 diabetes the first tier is lost outright, because the child is delivering insulin from an injection or pump and there is no endogenous insulin to switch off when glucose falls — the insulin keeps working regardless. The second tier is blunted, because the intra-islet insulin signal that normally triggers glucagon release is absent, so the glucagon response to hypoglycaemia is impaired. The third tier, the adrenaline response, is intact early in the disease but becomes attenuated after each episode, so repeated hypoglycaemia steadily lowers the glucose level at which symptoms appear. This erosion is called hypoglycaemia-associated autonomic failure, or HAAF, and it is the mechanism by which hypoglycaemia begets hypoglycaemia: one event weakens the warning, so the next event is silent, so the next event is more severe. [2] [3]
The brain is acutely vulnerable because, unlike muscle and most organs, it cannot use free fatty acids as fuel and depends on glucose or ketones. When glucose falls and ketogenesis is suppressed by the residual insulin, the brain is doubly exposed, and neuronal injury follows. Cryer framed the continuum precisely: mild hypoglycaemia is functional brain failure, a reversible impairment of cognition and coordination; untreated severe hypoglycaemia can progress, at the extreme, to brain death. [3]
Clinical Presentation
The presentation unfolds in two waves. The first is the autonomic wave — tremor, sweating, palpitations, hunger and anxiety — driven by the adrenaline surge, which normally appears when glucose crosses roughly 3.3 to 3.8 millimoles per litre. The second is the neuroglycopenic wave — confusion, drowsiness, blurred vision, slurred speech, unsteadiness, and at the extreme seizure and coma — driven by the brain running out of fuel, which becomes prominent below 3.0 millimoles per litre. A child who still has their warning feels the first wave and treats themselves; a child with impaired awareness skips straight to the second. [1] [8]
Young children rarely articulate the autonomic symptoms in those terms. Instead the presentation is behavioural — irritability, pallor, sudden mood change, tears out of proportion to events, lethargy, or a "glassy" look — and the family learns to recognise the pattern. Toddlers and children with developmental disability or neurodivergence depend entirely on caregiver observation, so any unexplained behavioural change in a child with insulin therapy demands a glucose check. The nocturnal presentation is the most easily missed: the child is asleep, the event is silent, and the only clues are a morning headache, unexplained lethargy, raised fasting ketones, a wet bed, or a sensor trace that fell overnight. [1] [12]
The behavioural change can be striking and is often misread. An adolescent in a hypoglycaemic lecture or argument may seem angry, uncooperative, or intoxicated, and the family or teachers may mistake the cause. The practical rule in any setting is that a child or adolescent with diabetes who is behaving out of character, or who cannot cooperate with a simple instruction, needs a glucose check immediately. [1]
Differential Diagnosis
The differential splits into three questions. The first is whether the event is truly hypoglycaemia: a finger-prick or sensor glucose confirms it, but a sensor can lag behind a rapid fall by several minutes, so a normal sensor reading during an acute collapse does not exclude hypoglycaemia — if the child is symptomatic and has insulin on board, treat first and let the glucose catch up. The pseudohypoglycaemia of a poorly perfused capillary sample is the other trap, resolved by a laboratory venous or sensor reading. [1]
The second question is the cause within the diabetes regimen. The common drivers are a mismatched or stacked insulin dose, a missed or delayed meal, under-counted or delayed carbohydrate absorption after a high-fat meal, exercise, alcohol, gastrointestinal illness, an error in pump priming or site failure, or a basal rate that is too high overnight. The analysis is a forensic one: review the bolus history, the carbohydrate record, the activity, and the sensor trace for the preceding six hours. [1] [2]
The third question is whether a co-morbidity is amplifying the risk. Coeliac disease, adrenal insufficiency, growth hormone deficiency, and thyroid disease all increase insulin sensitivity or impair counter-regulation and can turn a stable regimen into a recurrent-hypoglycaemia pattern; they should be screened when events cluster without a clear regimen cause. Factitious insulin administration — the surreptitious injection or pump bolus — must be considered in the adolescent with recurrent unexplained severe hypoglycaemia, and it raises a safeguarding rather than a punitive response. [1] [12]
Clinical & Bedside Assessment
The bedside assessment begins with the recognition that an altered child is hypoglycaemic until proven otherwise. Confirm the glucose with a sensor or finger-prick if the child can cooperate, but never delay treatment to obtain a reading in a child who is seizing or unconscious — the diagnosis is in the history of diabetes, and the treatment is safe to give empirically. Assess the severity by the child's functional state, not the number alone: a child who can swallow and cooperate has a mild or moderate event; a child who cannot needs glucagon or intravenous dextrose. [1]
The history is then taken in parallel with treatment. The four questions are what the child last ate and when, what insulin was given and when (including any stacked bolus or pump priming), what activity preceded the event and how long ago, and whether alcohol or illness is in the picture. The past pattern matters as much as the index event: a first severe episode in a previously well-controlled child points to a discrete precipitant, whereas a cluster of events points to impaired awareness or a regimen that has outrun the child's intake. [1] [8]
Examination during recovery focuses on confirming the return of normal cognition and excluding a residual neurological deficit, an injury from a fall or seizure, and signs of a precipitant such as a pump-site infection or an intercurrent illness. The disposition decision turns on whether the cause is identified and fixed, the child can eat and keep down carbohydrate, and a reliable adult will observe them — most events are managed at home or school, but a severe event with a seizure, a head injury, or a persistent cause warrants observation. [1]
Investigations
The principal investigation is the glucose measurement itself, taken at the time of the event. A laboratory venous glucose is the gold standard, but a calibrated sensor or finger-prick is acceptable in real time; the key is that the measurement is tied to the symptoms, because a normal glucose when the child is well excludes nothing about the event that brought them in. A blood or urine ketone is useful in the recovery analysis: hypoglycaemia without ketones suggests excess insulin action, while ketones with a low glucose suggest missed substrate. [1]
The retrospective investigation is the continuous glucose monitoring download, which has transformed the assessment of recurrent hypoglycaemia. The ambulatory glucose profile reveals the time below range, the timing of nocturnal events, the post-exercise pattern, and the glycaemic variability that drives both highs and lows. In a child with impaired awareness, the download often exposes a burden of asymptomatic hypoglycaemia far greater than the family or clinician realised, and it converts a vague history into actionable data. [5] [1]
When to investigate beyond the diabetes regimen
Investigate for a co-morbidity when hypoglycaemia clusters without a clear regimen cause: coeliac serology and tissue transglutaminase IgA, thyroid function, a morning cortisol, and in the adolescent with recurrent unexplained events a consideration of factitious insulin. A low C-peptide or insulin level during a documented event distinguishes exogenous from endogenous hyperinsulinaemia when factitious use is suspected. [1] [12]
Management — Resuscitation
The resuscitation principle is that treatment is time-critical and safe to give empirically. A child who is seizing or unconscious is placed in the recovery position, the airway is secured, help is summoned, and glucagon is given intramuscularly or intranasally — or, where intravenous access is available, dextrose is given at 0.2 to 0.3 grams per kilogram. The response to glucagon is typically within ten to fifteen minutes, and intravenous dextrose acts within minutes; if there is no response, reconsider the diagnosis and look for an alternative cause of collapse. [1] [11]
Glucagon is the community rescue drug because it does not require intravenous access. Intramuscular glucagon has been the standard for decades, and intranasal glucagon powder is now an established alternative that a caregiver or school staff member can administer without reconstitution or injection, with meta-analytic evidence of comparable success to the injectable form. The practical teaching point is that every family, school, and carer of a child with type 1 diabetes should hold glucagon, know where it is, and have rehearsed its use, because the window between a severe event and recovery is short and the first responder is rarely a clinician. [11] [1]
Once the child is awake and able to swallow safely, follow with oral complex carbohydrate and protein to sustain the recovery, because the effect of glucagon is transient and the glucose will fall again as the insulin continues to act. After any severe event, observe the child, review the cause, adjust the insulin regimen, and reinforce the prevention plan before discharge — a severe event that is treated and sent home without an analysis will recur. [1]
Management — Definitive & Stepwise
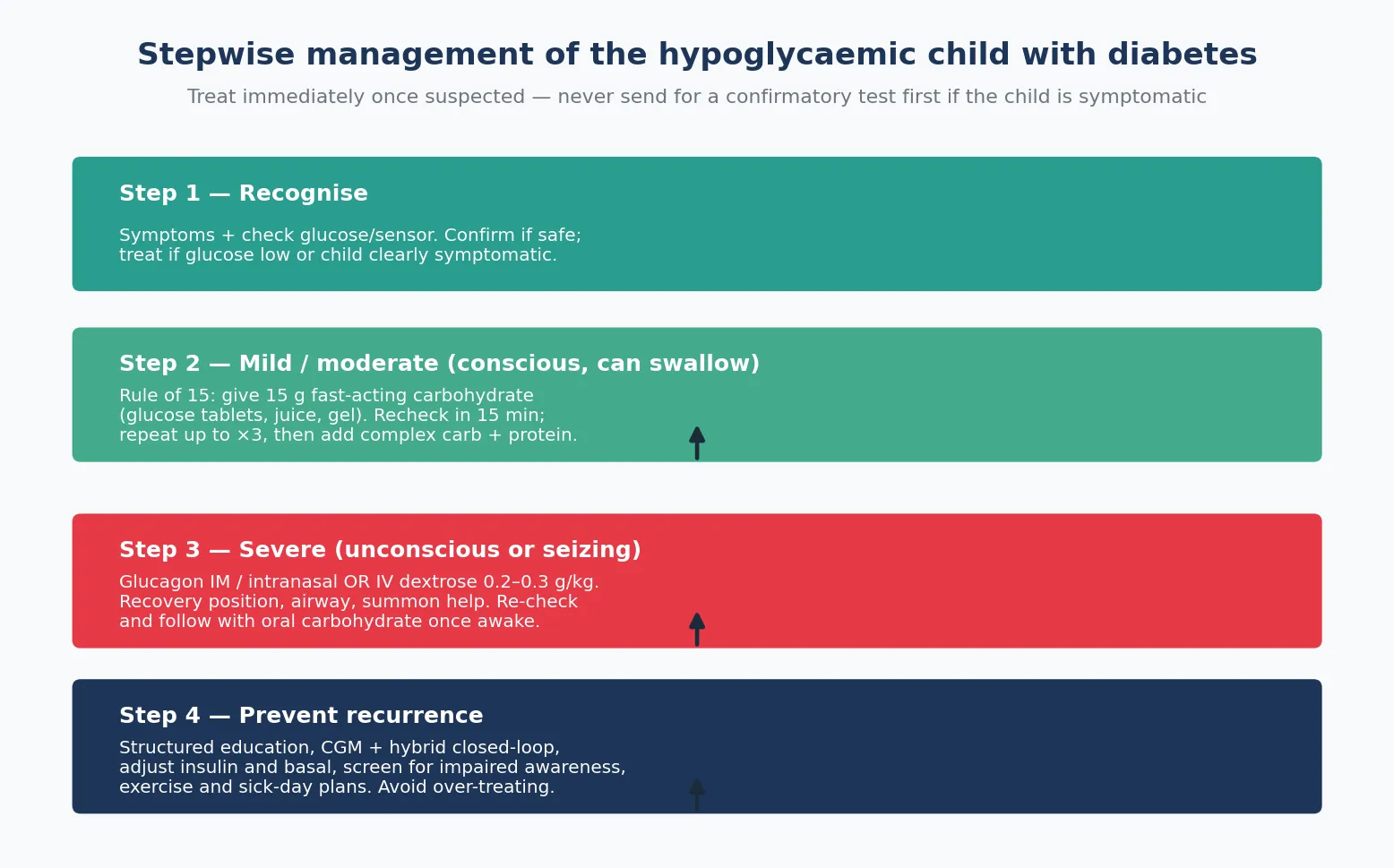
For the conscious child who can swallow, the rule of 15 is the cornerstone. Give 15 grams of fast-acting carbohydrate — glucose tablets, a glucose gel, or 100 to 150 millilitres of juice or sugary drink — wait 15 minutes, then recheck the glucose. If it remains below the target, repeat the dose up to three times; once the glucose recovers, follow with a snack of complex carbohydrate and protein to sustain it. Glucose is preferred over other sugars because it does not depend on a first-pass metabolic step, and fat-containing foods such as chocolate are avoided because fat delays absorption. [1]
The rule of 15 — mild to moderate hypoglycaemia
Give 15 g fast-acting carbohydrate (glucose tablets, gel, or 100–150 mL juice / sugary drink).
Wait 15 minutes, then recheck the glucose.
If still below target, repeat up to three times.
Once recovered, give complex carbohydrate + protein to sustain the glucose.
Review the cause and adjust the insulin regimen before the next event.
The definitive management, however, is prevention, and this is where modern diabetes care has moved furthest. Continuous glucose monitoring exposes the asymptomatic burden, and the JDRF study established that its use improves HbA1c and time-in-range without increasing hypoglycaemia. Threshold-suspend and predictive low-glucose suspend technology — in which the pump interrupts insulin delivery when a low is predicted — reduces nocturnal and exercise-related events, and hybrid closed-loop systems now autonomously reduce basal delivery as glucose falls, providing the closest approximation yet to the lost first tier of defence. [5] [6] [1]
Specific Subtypes & Scenarios
Nocturnal hypoglycaemia is the commonest and most easily missed subtype, because the child is asleep and the autonomic response is physiologically blunted overnight. The clues are a morning headache, lethargy, raised fasting ketones, mood change, or a sensor trace that dipped below range; the dangers are an unwitnessed seizure and, rarely, the dead-in-bed syndrome. The prevention levers are a sensor with alarms or predictive low-glucose suspend, a measured bedtime glucose with a snack if low or with rapid-acting insulin on board, and a basal-rate review — never a blanket increase in food, and never an omission of basal insulin. [1] [10]
Exercise-related hypoglycaemia is delayed as well as immediate, because muscle continues to take up glucose and replenish glycogen for hours after activity, and the risk peaks two to twelve hours afterwards — often overnight. The management is anticipatory: check the glucose before exercise, take fast-acting carbohydrate if it is below 7 millimoles per litre, reduce the pre-exercise bolus or the pump basal rate during activity, and plan a bedtime snack with sustained carbohydrate after intense or prolonged exercise. [1]
Impaired awareness and recurrent severe hypoglycaemia form the highest-risk subtype. The first step is to confirm the burden with a continuous glucose monitoring download, the second is to run two to three weeks of strict hypoglycaemia avoidance to restore the adrenaline warning, and the third is to deploy technology — hybrid closed-loop delivery most effectively — to prevent the events that the restored warning cannot reach. The perioperative and acutely ill child is a distinct scenario: fasting with insulin on board is the classic setup for hypoglycaemia, managed by a variable-rate intravenous insulin and dextrose protocol with hourly glucose monitoring rather than by subcutaneous insulin sliding scales. [2] [1]
Complications & Pitfalls
The acute complications are the seizure, the head injury from a fall, and the rare progression to coma or death. The subacute and long-term complications are the neurocognitive burden of recurrent severe hypoglycaemia on the developing brain and the psychological consequence of fear of hypoglycaemia. The DCCT/EDIC neuropsychological follow-up reassured the field that a moderate number of severe events does not measurably damage cognition in older children, but the effect of recurrent severe events in very young children, whose brains are still myelinating, remains an area of active concern. [4] [9]
The Lancet Child and Adolescent Health review of type 1 diabetes and the developing brain framed the nuance: hypoglycaemia is part of the villain, but chronic hyperglycaemia and glycaemic variability also shape neuroanatomical and cognitive differences, so the risk cannot be read off the hypoglycaemia count alone. The practical implication is that the prevention plan targets all three — hypoglycaemia, hyperglycaemia, and variability — rather than buying fewer lows at the price of chronically high glucose. [9] [12]
The pitfall to name explicitly is the rebound from over-treatment. Giving too much carbohydrate, or escalating insulin fearfully afterwards, produces a hyperglycaemic swing that worsens glycaemic variability and, paradoxically, sets up the next low. The disciplined response is to treat with 15 grams and recheck, not to pour in food, and to reduce rather than omit the next insulin dose. The dead-in-bed syndrome is the catastrophic end of the spectrum — an unexpected overnight death in a young person with type 1 diabetes, linked to profound nocturnal hypoglycaemia and QT prolongation — and it is the reason nocturnal hypoglycaemia is never dismissed as trivial. [1] [10]
Prognosis & Disposition
The prognosis with modern therapy is good. Population-based registry data show that the modern era has decoupled HbA1c from hypoglycaemia, so most children can achieve lower average glucose without a higher rate of severe events, provided the regimen is supported by education, continuous monitoring, and technology. The single most important prognostic factor is the presence of impaired awareness: a child with intact awareness and an identified precipitant has an excellent outlook, while a child with impaired awareness and recurrent severe events carries a substantially higher risk and warrants an active prevention plan. [7] [8]
The disposition is usually home or school for a mild or moderate event that has been treated and explained, provided the cause is identified and fixed and a reliable adult will observe the child. A severe event — especially with a seizure, a head injury, a persistent cause, or a young child — warrants observation, and any event followed by a prolonged recovery or a residual neurological sign needs assessment before discharge. The recurrent or impaired-awareness child is referred to the diabetes team for a structured prevention plan rather than discharged on incremental adjustments. [1]
The long-term disposition is the diabetes-care partnership itself. The child and family need the skills — carbohydrate counting, insulin adjustment, exercise and sick-day planning, glucagon use — and the technology — continuous monitoring and hybrid closed-loop — that make intensive therapy safe, and they need a team that reviews the ambulatory glucose profile at every visit and treats hypoglycaemia as a solvable engineering problem rather than an inevitable cost of the disease. [1] [5]
Special Populations
The toddler is the highest-vigilance group because they cannot report symptoms, their intake and activity are unpredictable, and their brains are still developing. The prevention strategy leans heavily on continuous glucose monitoring with alarms, on conservative glucose targets, and on caregiver education that treats any behavioural change as a potential low. The same principle applies to children with developmental disability or neurodivergence, who may not articulate symptoms and whose behaviour may be attributed to their baseline condition rather than to hypoglycaemia. [1] [12]
The adolescent faces the intersecting risks of risk-taking behaviour, alcohol, irregular meals, and the transition toward self-management without full adult oversight. Alcohol suppresses gluconeogenesis and masks the autonomic warning, so an alcohol-related hypoglycaemia can present hours after drinking and during sleep; the practical teaching is to eat carbohydrate with alcohol, to check glucose before sleep, and never to omit the basal insulin. The transition-age young person moving from paediatric to adult care is a period of heightened risk, and the structured handover must include a hypoglycaemia-prevention review. [1]
Socioeconomic disadvantage, remote residence, and limited access to technology widen the gap in outcomes, because continuous monitoring and hybrid closed-loop systems are expensive and their funding varies by region. Indigenous, migrant, refugee and asylum-seeking families may face language, health-literacy and access barriers that compound the risk; the response is interpreter-supported education, community-based support, and active advocacy for technology access. The technology-dependent child on a hybrid closed-loop system has a different set of scenarios — sensor failure, pump occlusion, algorithm limits — and the family must rehearse the manual fallback of injection therapy and the rule of 15. [1] [5]
Evidence, Guidelines & Regional Differences
The ISPAD Clinical Practice Consensus Guidelines 2022 on the assessment and management of hypoglycaemia are the global reference, setting the severity levels, the rule of 15, and the technology recommendations. The underlying evidence spans the DCCT, which defined the intensive-therapy trade-off; the JDRF continuous glucose monitoring study and the ASPIRE threshold-suspend trial, which established that technology reduces hypoglycaemia without sacrificing control; and the population-based registry data, which showed that the modern era has improved HbA1c without raising the severe-hypoglycaemia rate. [1] [4] [5] [6] [7]
[1]The regional differences lie in technology funding and in the structure of diabetes care. Where continuous monitoring is funded universally, the asymptomatic burden is exposed and treated; where it is not, nocturnal and exercise-related hypoglycaemia remain hidden and the severe-event rate is higher. The controversies are narrower than they were — the value of continuous monitoring and of hybrid closed-loop is now settled — but the question of how aggressively to lower HbA1c in very young children, and whether to use do-it-yourself closed-loop systems, remains live. The guideline message is consistent: lower the HbA1c as far as is safe, protect the brain, and deploy every available technology to reconcile the two. [1] [5]
Exam Pearls
The three tiers of defence — and why they fail in T1DM
The fellowship candidate who names the trade-off, delivers the rule of 15 and the glucagon dose, explains the HAAF cycle, and prescribes continuous monitoring with hybrid closed-loop as the prevention — and who frames the whole plan around protecting the developing brain — has the full mark. The deeper candidate adds the equity point: that the technology which makes intensive therapy safe is not universally accessible, and that advocacy for access is part of paediatric diabetes care. [1] [5]
References
- [1]Abraham MB, Karges B, Dovc K, et al. ISPAD Clinical Practice Consensus Guidelines 2022: Assessment and management of hypoglycemia in children and adolescents with diabetes Pediatr Diabetes, 2022.PMID 36537534
- [2]McCrimmon RJ, Sherwin RS. Hypoglycemia in type 1 diabetes Diabetes, 2010.PMID 20876723
- [3]Cryer PE. Hypoglycemia, functional brain failure, and brain death J Clin Invest, 2007.PMID 17404614
- [4]The Diabetes Control and Complications Trial Research Group, Nathan DM, Genuth S, et al. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus N Engl J Med, 1993.PMID 8366922
- [5]Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study Group, Tamborlane WV, Beck RW, et al. Continuous glucose monitoring and intensive treatment of type 1 diabetes N Engl J Med, 2008.PMID 18779236
- [6]Bergenstal RM, Klonoff DC, Garg SK, et al. Threshold-based insulin-pump interruption for reduction of hypoglycemia N Engl J Med, 2013.PMID 23789889
- [7]Haynes A, Hermann JM, Clapin H, et al. Decreasing Trends in Mean HbA1c Are Not Associated With Increasing Rates of Severe Hypoglycemia in Children: A Longitudinal Analysis of Two Contemporary Population-Based Pediatric Type 1 Diabetes Registries From Australia and Germany/Austria Between 1995 and 2016 Diabetes Care, 2019.PMID 31213467
- [8]Ly TT, Gallego PH, Davis EA, Jones TW. Impaired awareness of hypoglycemia in a population-based sample of children and adolescents with type 1 diabetes Diabetes Care, 2009.PMID 19587370
- [9]Cameron FJ, Northam EA, Ryan CM. The effect of type 1 diabetes on the developing brain Lancet Child Adolesc Health, 2019.PMID 30987935
- [10]Jones J, James S, Brown F, et al. Dead in bed - A systematic review of overnight deaths in type 1 diabetes Diabetes Res Clin Pract, 2022.PMID 36007797
- [11]Pontiroli AE, Tagliabue E. Intranasal versus injectable glucagon for hypoglycemia in type 1 diabetes: systematic review and meta-analysis Acta Diabetol, 2020.PMID 32025860
- [12]Northam EA, Lin A. Hypoglycaemia in childhood onset type 1 diabetes--part villain, but not the only one Pediatr Diabetes, 2010.PMID 19538515