Paeds · endocrinology-diabetes-and-growth
Osteoporosis and fragility fractures in children
Also known as paediatric osteoporosis · childhood osteoporosis · low bone mass in children · glucocorticoid-induced osteoporosis in children · vertebral compression fracture in children
A fellowship approach to osteoporosis and fragility fractures in children: the ISCD framework that makes a low bone density Z-score only half the diagnosis, the primary-versus-secondary split where the steroid-treated and non-ambulant child dominate, the vertebral fracture that defines osteoporosis on its own, the growing skeleton's peak-bone-mass window, and the weight-based bisphosphonate pathway that now leads with intravenous zoledronic acid.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Picture the child who walks in. A nine-year-old boy with Duchenne muscular dystrophy, on daily prednisolone for two years, complains of back pain and has lost two centimetres of height; the lateral spine shows a wedge fracture at T12. Or a fourteen-year-old girl with Crohn disease on a glucocorticoid wean who fractures her forearm turning over in bed. Or a previously well six-year-old whose recurrent long-bone fractures turn out to be osteogenesis imperfecta rather than misfortune. The fellowship task in each is to read the density and the fracture history together, to image the spine, and to treat the cause and the bone rather than the number alone. [7] [10]
Z-F-V — the three pieces of a paediatric osteoporosis diagnosis
Overview & Definition
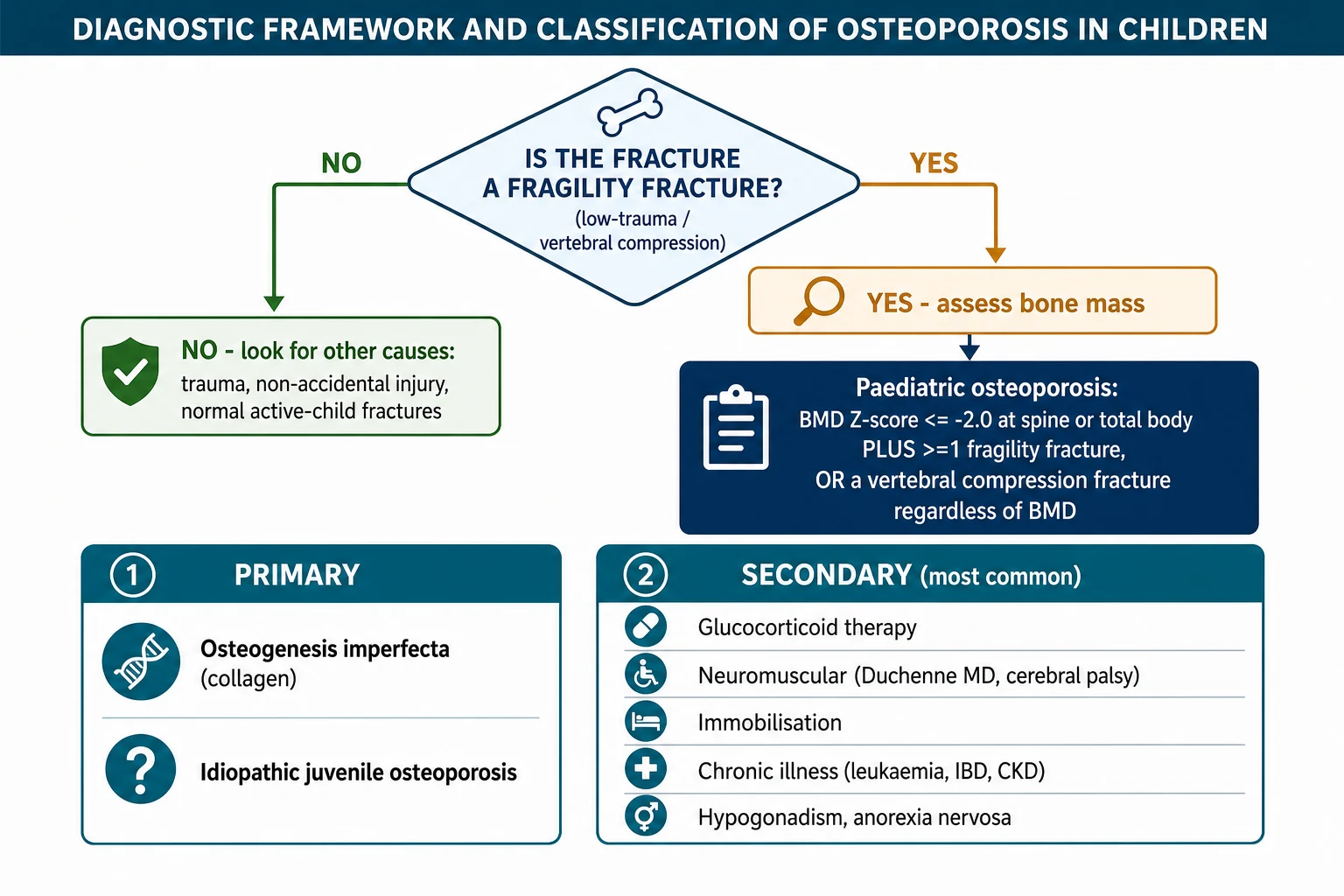
Osteoporosis in a child is a disorder of bone strength in which the skeleton is fragile enough to fracture under forces that a healthy bone would withstand. Bone strength has two parts: how much mineral is packed into the bone, and how well that bone is built — its geometry, its microarchitecture, and the material quality of its matrix. A dual-energy X-ray absorptiometry scan estimates only the first part, which is why the density number alone never makes the diagnosis. The fracture is the proof that the strength has failed. [1] [6]
The definition that fellowship candidates must hold is the International Society for Clinical Densitometry framework, set at the 2013 Pediatric Position Development Conference and carried forward in 2019. A child or adolescent has osteoporosis when they have low bone mass — a BMD Z-score of minus two or lower, adjusted for age and sex — together with a clinically significant fracture history. That fracture history is one or more vertebral compression fractures, or two or more long-bone fractures before age ten, or three or more before age nineteen. Critically, a vertebral compression fracture alone satisfies the definition regardless of the bone density, because the vertebra has demonstrated fragility. [1] [2]
The distinction from adult medicine is the trap that costs marks. Adults use the T-score, which compares bone to a healthy young adult reference, and a T-score of minus two point five or lower is osteoporosis by itself. Children use the Z-score, which compares bone to age- and sex-matched peers, and a low Z-score is labelled low bone mass for age — never osteoporosis — until a fragility fracture is documented. A child is growing and accruing bone, and a low density in a growing skeleton is a risk state, not a disease. [1] [5]
Classification
The classification that earns marks splits osteoporosis by whether the bone is intrinsically defective or is being damaged from outside. Primary osteoporosis arises from an inborn error of bone matrix, and it is dominated by osteogenesis imperfecta, a defect of type one collagen that produces brittle bone from infancy. Idiopathic juvenile osteoporosis is the rarer primary form, a self-limiting but puzzling disorder of prepubertal and early-pubertal children that remits at puberty and that is a diagnosis of exclusion. [10] [6]
Secondary osteoporosis is the larger group and the one a general paediatrician meets. Bone is lost because the child is exposed to something that suppresses bone formation or accelerates resorption, or that removes the mechanical loading the bone needs to stay strong. Glucocorticoid therapy is the single commonest driver, through osteoblast suppression and osteocyte death, and it acts on children with Duchenne muscular dystrophy, inflammatory bowel disease, juvenile arthritis, nephrotic syndrome, leukaemia, and solid-organ transplant. Neuromuscular disease adds reduced loading: boys with Duchenne muscular dystrophy carry both the steroid and the immobility, and non-ambulant children with cerebral palsy lose bone from the lack of weight-bearing alone. [7] [14]
The biochemical and endocrine causes sit beside these. Hypogonadism, delayed puberty, anorexia nervosa, and the cytokines of chronic inflammation all erode bone, and they are most active during the adolescent years when bone should be accruing fastest. Chronic kidney disease produces renal osteodystrophy, a mixed picture that overlaps with and must be distinguished from straightforward osteoporosis. Recognising the secondary group matters because the treatment of the cause — lowering the steroid dose, treating the inflammation, restoring gonadal status — is as important as any drug the bone team prescribes. [5] [6]
Epidemiology & Risk Factors
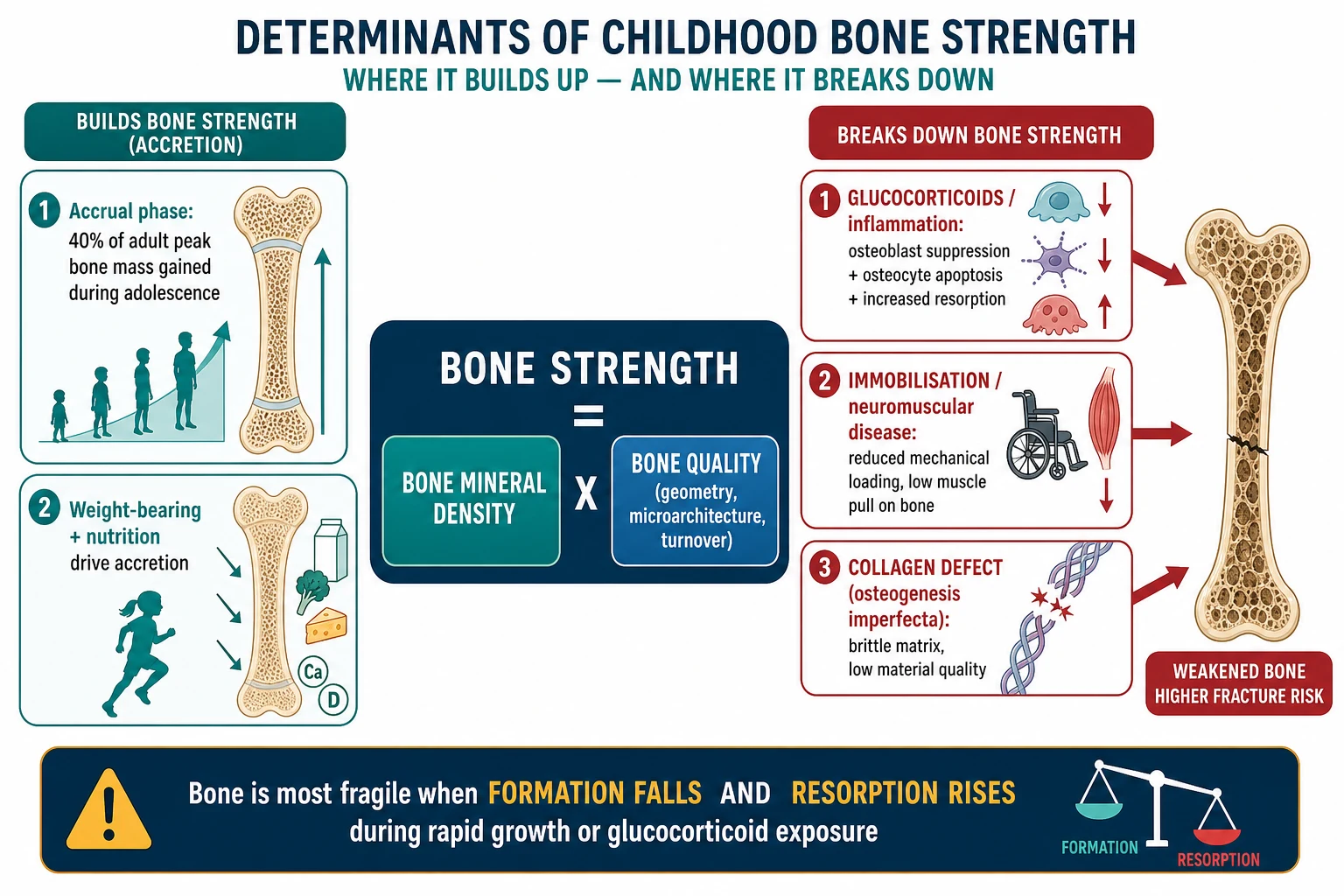
Childhood and adolescence are the decisive years for lifelong skeletal health, because peak bone mass is built then. About forty per cent of adult peak bone mass is accrued during adolescence, and the child who fails to accrue — through chronic illness, glucocorticoids, poor nutrition, or immobilisation — reaches a lower peak and carries a higher fracture and osteoporosis risk for the rest of life. This is why bone health in a sick child is a long-term investment, not a side issue. [6] [5]
Glucocorticoid exposure is the most quantified risk. In a cohort of children starting glucocorticoids for rheumatic disease, incident vertebral fractures clustered in the first one to three years after treatment began, and the risk was driven by the cumulative dose and by the underlying disease activity rather than by the bone density at baseline. The practical message is to image the spine early after steroids start, not to wait for years of accumulated exposure before screening. [8] [7]
The neuromuscular populations carry a compounded risk. Boys with Duchenne muscular dystrophy lose ambulation in childhood and are usually treated with glucocorticoids to preserve muscle, so the bone faces reduced loading and steroid toxicity together, and vertebral and long-bone fractures become common in the second decade. Non-ambulant children with cerebral palsy have low bone density from reduced weight-bearing, and fractures of the femur from routine care or low-impact falls are a recognised burden. The international Duchenne workshops now treat endocrine and bone surveillance as part of standard care. [14] [2]
The numbers that anchor a fellowship answer
Pathophysiology
Bone strength is the product of bone mineral density and bone quality, and a fellowship answer walks both. Mineral density is what the DXA estimates — the grams of mineral per unit area at the spine or total body. Quality is what the DXA cannot see: the macro-geometry of the bone, the microarchitecture of the trabeculae, the turnover rate, and the material properties of the collagen matrix. A bone can fail at a normal density if its quality is poor, which is exactly what happens in osteogenesis imperfecta. [6] [10]
Glucocorticoids erode bone through several mechanisms at once. They suppress osteoblast formation and drive osteoblast and osteocyte apoptosis, so new bone is not laid down and the mechanosensing cells that maintain bone die. They shift the balance toward resorption early in treatment by increasing receptor activator of NF-kB ligand activity, and they reduce muscle mass, which lowers the mechanical load the bone needs to stay strong. The net effect is a skeleton that loses mineral and quality together, fastest in the first months of exposure. [7] [8]
Immobilisation works through the mechanostat. Bone remodels to the loads placed on it, so a child who does not stand or bear weight loses the signal that maintains cortical and trabecular bone, and resorption outstrips formation. This is why non-ambulant cerebral palsy and late-stage Duchenne muscular dystrophy produce bone that fractures under care, and why a standing program and safe weight-bearing are part of the treatment as much as any drug. The collagen defects of osteogenesis imperfecta, by contrast, produce a matrix that is brittle at any density, because the type one collagen that should toughen the bone is malformed. [10] [14]
The growing skeleton is the unifying thread. Because children are accruing bone, anything that disrupts accrual during the adolescent window — glucocorticoids, cytokines, hypogonadism, anorexia, or immobilisation — lowers the peak bone mass they carry into adult life. The skeleton is most vulnerable precisely when it is growing fastest, which is why surveillance focuses on the steroid-treated and the chronically ill adolescent as much as on the infant with a genetic bone disease. [6] [5]
Clinical Presentation
The presentation is usually the fracture, because bone fragility is silent until the skeleton fails. A vertebral compression fracture may announce itself with back pain, a loss of height, or a new kyphosis, but a substantial proportion are asymptomatic and are found only on surveillance imaging of a steroid-treated child. The fellowship habit is to measure height at every visit in a steroid-treated child and to image the spine when height velocity falters or pain appears. [8] [7]
Long-bone fragility fractures present after low-trauma mechanisms. A forearm that breaks turning over in bed, a femur that fractures during a seizure or a transfer, or repeated fractures in a steroid-treated boy with Duchenne muscular dystrophy are the patterns that should trigger a bone assessment rather than orthopaedic closure alone. The child who fractures from a genuine high-energy mechanism — a fall from a bike at speed, a motor-vehicle collision — does not have a fragility fracture, and the bone work-up is framed by the mechanism, not the fracture. [5] [14]
The primary bone diseases declare themselves differently. Osteogenesis imperfecta presents from infancy with fractures, blue or grey sclerae, dentinogenesis imperfecta, joint hypermobility, hearing loss in older children, and a positive family history. The fracture pattern is out of proportion to the trauma, and the child may already be in the system when the bone density question arises. Idiopathic juvenile osteoporosis presents in the years before puberty with new fractures and a declining density, and it is defined by the exclusion of osteogenesis imperfecta and every secondary cause. [10] [6]
Differential Diagnosis
The differential turns on three questions: is the fracture a fragility fracture, what is wrong with the bone, and is this non-accidental. The first separates low-trauma and fragility fractures from the high-energy fractures of an active child. The mechanism and the fracture site matter: a femur shaft fracture from a short fall, a vertebral wedge in a steroid-treated child, or a forearm fracture from rolling in bed point toward fragility, whereas a clavicle or distal radius from a fall at play does not. [5] [1]
The bone pathology is read from the biochemistry and the radiograph. Nutritional rickets and metabolic bone disease produce widened, frayed metaphyses and a high alkaline phosphatase with abnormal calcium, phosphate, or vitamin D, and they are a separate pathway. Hypophosphatasia is the opposite trap: a fracturing child with an inappropriately low alkaline phosphatase, in whom bisphosphonates worsen the disease. Osteogenesis imperfecta shows osteopenia and thin cortices with a collagen- defect history, and chronic kidney disease produces renal osteodystrophy with a disordered parathyroid axis. The biochemistry and the skeletal survey separate these before any bone-density interpretation. [6] [10]
Non-accidental injury must always be held alongside osteogenesis imperfecta when fractures appear in a pre-mobile infant or when the history and the injury do not fit. The skeletal survey, the pattern of fractures (classic metaphyseal lesions, rib fractures, fractures of different ages), the biochemistry, and the safeguarding assessment are all required, and the collagen testing for osteogenesis imperfecta is sent when the picture is ambiguous. The two diagnoses are not mutually exclusive in the mind, and a child can be both at risk and bone-diseased, so the assessment runs both in parallel. [10] [5]
Causes of low bone mass and fractures in children
Clinical & Bedside Assessment
The bedside move is to combine the fracture history with the growth chart and the disease context. Take a fracture inventory: how many, which bones, and the mechanism of each, and separate the high-energy from the low-trauma. Plot the height and weight, because a child losing height on glucocorticoids may have an unrecognised vertebral fracture, and a child with faltering growth may be losing bone along with weight. Examine the spine for tenderness and kyphosis, the sclerae for the blue-grey of osteogenesis imperfecta, the teeth for dentinogenesis, the joints for hypermobility, and the gait and muscle power for the neuromuscular substrate. [1] [14]
The history gathers the drivers of bone loss. Ask about glucocorticoids — the drug, the dose, the duration, and the cumulative exposure — because this is the commonest single driver. Ask about the underlying disease: Duchenne muscular dystrophy, cerebral palsy, inflammatory bowel disease, juvenile arthritis, nephrotic syndrome, leukaemia, transplant, and anorexia nervosa each carry their own bone-risk profile. Ask about puberty and menses, because delayed puberty and hypogonadism erode the adolescent bone-accrual window. Ask about diet, sunlight, and a family history of fractures, hearing loss, or blue sclerae. [7] [5]
The capacity to sustain treatment is assessed at the first visit, because bisphosphonate therapy is a long programme of infusions, monitoring, and adherence. Identify who administers the supplement and the infusion, the transport needs, the interpreter and health-literacy requirements, and the coordination between the treating team and the bone or endocrine service. The family is counselled that bone health is a marathon alongside the primary disease, and a named coordinator and a clear surveillance plan are set up early. [4] [12]
Investigations
The core investigation is dual-energy X-ray absorptiometry, and it is reported as a Z-score, read alongside the fracture history. The standard sites are the lumbar spine (L1 to L4) and the total body less head, both reported as age- and sex-adjusted Z-scores. Where size is an issue — a small-for-age child, or a steroid-treated child with short stature — the result is size-adjusted, because a small bone reads as a low density and overstates the risk. The ISCD 2019 positions confirm the spine and total body as the primary sites and add the lateral distal femur for children in whom the spine and hip are uninterpretable or impossible. [2] [3]
The vertebral fracture assessment is the second pillar and the one most often missed. A lateral thoracolumbar spine, performed by DXA vertebral fracture assessment or by a conventional lateral radiograph, images T4 to L4 for wedge, biconcave, and compression deformities. In steroid-treated children, the spine is imaged at baseline and then at intervals, because a new vertebral fracture changes the diagnosis and the management immediately — it makes osteoporosis regardless of the density. The 2019 ISCD position endorses vertebral fracture assessment in the paediatric population, particularly for the glucocorticoid-exposed child. [2] [8]
The biochemistry excludes the mimics and prepares the child for treatment. Send calcium, phosphate, alkaline phosphatase, parathyroid hormone, 25-hydroxyvitamin D, renal and liver function, thyroid function, and, in the adolescent, sex hormones and inflammatory markers. A low alkaline phosphatase points to hypophosphatasia and changes everything, because bisphosphonates harm that disease. The 24-hour urinary calcium or a spot calcium-to-creatinine ratio checks for hypercalciuria, and bone turnover markers can track the response to bisphosphonate. When a primary bone disease is suspected, type one collagen analysis and the relevant gene panel for osteogenesis imperfecta are sent. [5] [10]
Management — Resuscitation
There is no intravenous-resuscitation emergency in osteoporosis to match the hypocalcaemic infant of rickets, but the acute scenarios are real. A painful vertebral compression fracture causes back pain and immobility, and the immediate management is analgesia, a period of rest, and protection of the spine while the bisphosphonate pathway is opened. A long-bone fragility fracture is stabilised by the orthopaedic team, and the bone assessment is initiated before discharge so the cause is not lost in the orthopaedic follow-up. [4] [12]
The acute bisphosphonate decision belongs to the vertebral fracture and the recurrent long-bone fracture. An intravenous bisphosphonate is started once the diagnosis is made and the child is calcium and vitamin D replete, because the first infusion predictably lowers the serum calcium through acute suppression of bone resorption. Ensuring vitamin D sufficiency and an adequate calcium intake in the days before the infusion prevents symptomatic hypocalcaemia, and the first-dose flu-like reaction — fever, myalgia, and malaise in the first one to two days — is anticipated and managed with paracetamol and hydration. [12] [4]
The must-not-miss acute task is to exclude hypophosphatasia and unrecognised hypocalcaemia before the bisphosphonate is given. A low alkaline phosphatase in a fracturing child is hypophosphatasia, where bisphosphonates worsen the mineralisation defect, and a low baseline calcium or vitamin D must be corrected first. The safeguarding assessment runs in parallel whenever the fracture pattern or the history raises non-accidental injury, because a bone-disease diagnosis never closes that enquiry on its own. [10] [6]
Management — Definitive & Stepwise
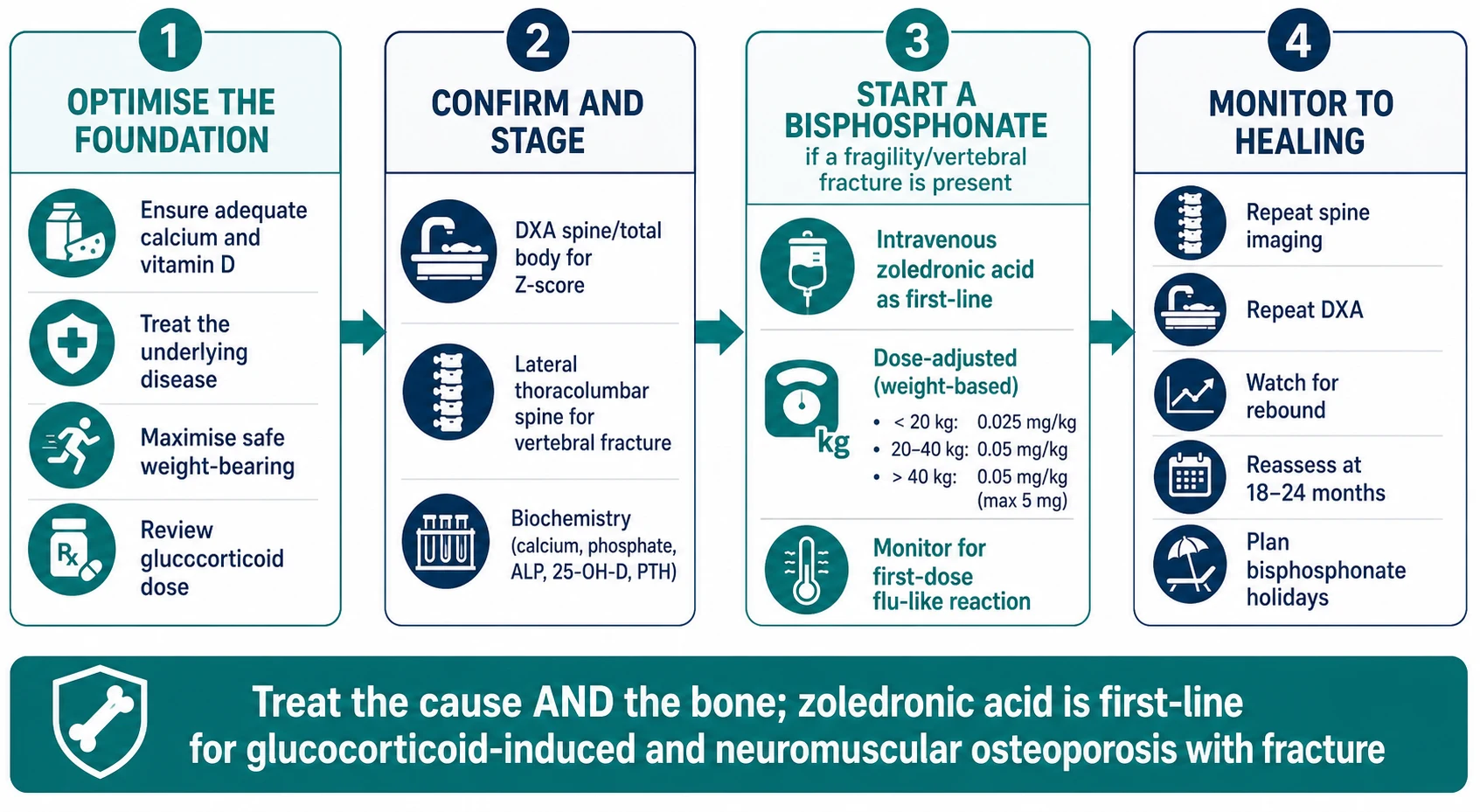
Definitive management begins with the foundation, because the bone will not heal on a drug alone. Correct calcium and vitamin D intake to the age-appropriate target, ensure the 25-hydroxyvitamin D is replete before any bisphosphonate, and treat the underlying disease — reduce the glucocorticoid dose where possible, control the inflammation, restore gonadal status, and treat the endocrine complications of Duchenne muscular dystrophy. For the non-ambulant child, a standing and weight-bearing program and optimised nutrition are part of the prescription as much as the infusion. [4] [14]
A bisphosphonate is added when a fragility or vertebral fracture is present, and intravenous zoledronic acid is now first-line. The randomised, double-blind, phase three trial of zoledronic acid against placebo in paediatric glucocorticoid-induced osteoporosis established its efficacy in this population, and the consensus guidelines endorse intravenous bisphosphonates — zoledronic acid or pamidronate — as the agents of choice for secondary osteoporosis with fracture. The dosing is weight-based and given at intervals of several months, with the dose and schedule determined by the treating endocrine or metabolic bone service and monitored against the bone turnover markers and the density response. [11] [12]
The glucocorticoid-induced pathway has its own evidence and its own guideline. The 2022 American College of Rheumatology guideline for the prevention and treatment of glucocorticoid-induced osteoporosis frames the oral and intravenous therapy options and the fracture-risk assessment, and the 2025 clinical approach to the paediatric glucocorticoid-induced patient integrates the zoledronic acid evidence with the practical surveillance of the spine. The principle is to treat the bone prophylactically in the high-risk steroid-exposed child and to escalate to a bisphosphonate as soon as a fracture appears. [9] [7]
The stepwise pathway from the fragility fracture to the healing bone
Confirm the diagnosis: a Z-score <= -2.0 plus a fragility fracture, or a vertebral compression fracture at any density
Lay the foundation: correct calcium and vitamin D, treat the underlying disease, reduce the steroid dose, maximise safe weight-bearing
Start an intravenous bisphosphonate when a fragility or vertebral fracture is present — zoledronic acid first-line, weight-based, calcium and vitamin D replete first
Manage the first-dose reaction: premedicate with paracetamol, hydrate, monitor calcium for the acute post-infusion dip
Monitor to healing: repeat the lateral spine and the DXA at intervals, track bone turnover markers down, reassess at 18 to 24 months for a treatment holiday
Specific Subtypes & Scenarios
Glucocorticoid-induced osteoporosis is the prototype secondary subtype and the one with the strongest recent evidence. The child on long-term steroids — for juvenile arthritis, inflammatory bowel disease, nephrotic syndrome, leukaemia, or transplant — is screened with a baseline DXA and lateral spine at the start of steroids and at intervals thereafter, because the vertebral-fracture risk clusters in the first years. Once a fracture appears, intravenous zoledronic acid is the first-line agent, supported by the phase three randomised trial, and the glucocorticoid dose is reviewed and reduced wherever the disease allows. [8] [11]
The neuromuscular child carries a compounded risk that needs a tailored assessment. Boys with Duchenne muscular dystrophy face glucocorticoid toxicity and progressive immobility together, and the international workshop now frames endocrine and bone surveillance — DXA, lateral spine, and fracture prevention — as part of standard care from the steroid years onward. The non-ambulant child with cerebral palsy is assessed with the lateral distal femur DXA, validated for this population, and treated with a standing program, nutrition, and a bisphosphonate when a fragility fracture occurs. [14] [2]
Osteogenesis imperfecta is the primary subtype that demands its own pathway. The diagnosis rests on the clinical phenotype — recurrent fractures, blue sclerae, dentinogenesis imperfecta, hearing loss, and a family history — and on type one collagen gene analysis, which identifies the majority of cases. Treatment is intravenous or oral bisphosphonate therapy to increase bone density and reduce fracture pain, combined with multidisciplinary care from orthopaedics, rehabilitation, audiology, dentistry, and genetics, and the transition to adult care is planned through adolescence. [10] [12]
Idiopathic juvenile osteoporosis is the rare subtype that is a diagnosis of exclusion. It presents in the years before puberty with new fractures and a declining density, and it is defined only after osteogenesis imperfecta and every secondary cause have been excluded. It often remits at puberty as the adolescent growth and sex-steroid surge restores bone accrual, and the role of the bisphosphonate is debated and reserved for the child with severe, progressive disease, which is why the distinction from osteogenesis imperfecta — which does not remit and does need treatment — is so important. [6] [10]
Complications & Pitfalls
The complications divide into those of the untreated disease and those of the bisphosphonate. Untreated osteoporosis produces progressive vertebral collapse with pain, kyphosis, and height loss, recurrent long-bone fractures with cumulative disability, and, in the chronic-disease child, a further erosion of mobility and quality of life. The orthopaedic management of a fracture in fragile bone must be paired with the metabolic treatment, because operating on bone that is still losing mineral risks fixation failure and refracture. [4] [6]
The bisphosphonate complications are predictable and largely avoidable. The acute phase brings a flu-like reaction with fever and myalgia in the first one to two days, managed with paracetamol and hydration, and a transient fall in calcium that is prevented by ensuring vitamin D and calcium sufficiency beforehand. Symptomatic hypocalcaemia after the first infusion is the classic avoidable error of treating an unprepared child. Nephrocalcinosis is a recognised concern with some regimens and is monitored by renal ultrasound where relevant, and the theoretical long-term risks — atypical femoral fracture and osteonecrosis of the jaw — are rare in children but inform the move toward treatment holidays and planned discontinuation. [12] [13]
The diagnostic pitfalls are the ones that misdirect treatment. The first is labelling any low Z-score osteoporosis, which over-treats a child who needs only the foundation and under-recognises the child whose normal density hides a vertebral fracture. The second is treating hypophosphatasia with a bisphosphonate, which worsens it. The third is missing osteogenesis imperfecta behind a secondary label, because the primary disease carries its own multidisciplinary and genetic counselling pathway. The fourth is treating a low-trauma fracture as an orthopaedic event alone and never asking why the bone broke. Each is avoided by reading the density and the fracture together and by completing the biochemistry before the drug. [1] [10]
Prognosis & Disposition
The prognosis depends almost entirely on the underlying cause and on whether the bone-accrual window can be protected. Secondary osteoporosis treated early — with the cause addressed, the foundation laid, and a bisphosphonate given when a fracture is present — improves bone density, relieves fracture pain, and allows vertebral fractures to remodel as the child grows, and the child who reaches a near-normal peak bone mass by the end of adolescence carries a markedly lower lifelong risk. The child whose underlying disease progresses, such as advanced Duchenne muscular dystrophy, faces ongoing bone loss despite treatment, and the prognosis is framed honestly alongside the primary disease. [4] [14]
Osteogenesis imperfecta carries a variable prognosis that tracks the severity and the type. The milder type one disease, treated with bisphosphonates and multidisciplinary care, allows near-normal mobility and lifespan, whereas the severe perinatal forms carry substantial morbidity and mortality in infancy. The bisphosphonate improves density, reduces fracture pain, and remodels vertebrae, but it does not cure the collagen defect, and the child is managed for life with a combination of medication, orthopaedics, rehabilitation, and surveillance. [10] [13]
The disposition is shared between the general paediatric team, paediatric endocrinology or the metabolic bone service, orthopaedics, and the disease-specific specialty. The acute fracture is managed by orthopaedics with the bone team involved before discharge; the steroid-exposed child is co-managed with rheumatology, gastroenterology, or neurology; and the genetic bone disease is managed with genetics and the metabolic bone team. Transition to adult care is planned through adolescence, because the bone health built — or lost — in childhood determines the adult osteoporosis risk, and the young person who leaves paediatric care without a plan is the one who reappears later with fractures. [6] [12]
Special Populations
The steroid-treated child with Duchenne muscular dystrophy is the population in whom bone health most changes the lived experience of the disease. Boys on daily glucocorticoids to preserve muscle simultaneously lose bone through the steroid and through progressive immobility, and vertebral and long-bone fractures become a leading source of pain and hospitalisation in the second decade. The international Duchenne workshop now frames endocrine and bone surveillance — DXA, lateral spine, vitamin D, and fracture prevention — as standard care, and the bisphosphonate is integrated into the multidisciplinary plan alongside the cardiology, respiratory, and rehabilitation input. [14] [11]
The non-ambulant child with cerebral palsy and the technology-dependent child form a further population. Reduced weight-bearing lowers bone density, and fractures from routine care, transfers, or seizures are common and painful. The lateral distal femur DXA, validated for this group, assesses the bone, and a standing program, optimised nutrition, and a bisphosphonate after a fracture are the pillars. Socioeconomic disadvantage shapes outcome through the practical determinants — access to infusions, transport, and the standing equipment — and the team's role is to remove those barriers as much as to prescribe. [2] [4]
Indigenous, migrant, refugee, and socioeconomically disadvantaged families face compounded risk through vitamin D deficiency, lower calcium intake, reduced access to DXA and infusions, and the demands of coordinating bone care alongside a complex primary disease. Telehealth and outreach extend specialist bone surveillance into rural and remote communities, and interpreter-supported, trauma-informed communication is the thread through the whole programme, because the conversation about a child's fragile bones is also a conversation about fear, guilt, and the long road of a chronic disease. [12] [5]
Evidence, Guidelines & Regional Differences
The foundational evidence is the International Society for Clinical Densitometry framework. The 2013 Pediatric Official Positions, published in 2014, established the definition of osteoporosis in children and adolescents as a low bone mass plus a clinically significant fracture history, and they set the Z-score thresholds and the fracture criteria that still anchor practice. The 2019 Position Development Conference extended the framework, confirming the spine and total body less head as the primary DXA sites, endorsing vertebral fracture assessment in the paediatric population, and adding the lateral distal femur for children in whom the spine and hip are uninterpretable. [1] [2]
The treatment evidence is led by the bisphosphonate trials and guidelines. The randomised, double-blind, phase three trial of zoledronic acid against placebo in paediatric glucocorticoid-induced osteoporosis established the first-line intravenous agent for the steroid-exposed child, and the Cochrane review of bisphosphonate therapy for secondary osteoporosis in children and adolescents framed the evidence base for the wider population. The 2018 Australasian consensus guidelines on bisphosphonate therapy in children and the 2022 American College of Rheumatology guideline for glucocorticoid-induced osteoporosis translate the evidence into operational practice. [11] [13]
The contemporary reviews consolidate the field. The 2023 European review of how to treat and monitor childhood osteoporosis, the 2024 overviews of bone fragility and diagnostic and treatment strategies in children, and the 2025 clinical approach to the paediatric glucocorticoid-induced patient bring the definition, the surveillance, and the drug pathway together for the practising clinician. The 2017 Nature Reviews Disease Primers article on osteogenesis imperfecta remains the definitive reference for the primary bone disease. [4] [10]
[1]Exam Pearls
The five anchors of a fellowship answer are: osteoporosis in a child needs a low bone mass plus a fragility fracture, the Z-score never the T-score, a vertebral compression fracture defines osteoporosis at any density, secondary causes dominate and the glucocorticoid-exposed child is the prototype, and intravenous zoledonic acid is the first-line bisphosphonate when a fracture is present. Hold these five and the topic holds together under any examiner pressure, because they map the definition, the diagnostic move, the cause, and the treatment. [1] [11]
The diagnostic anchors are the Z-score of minus two or lower for low bone mass, the fracture criteria of one vertebral compression fracture or two long-bone fractures before age ten or three before age nineteen, and the absolute rule that a vertebral fracture alone is osteoporosis. The treatment anchor is the foundation first — calcium, vitamin D, weight-bearing, and the cause — with the bisphosphonate added only when a fracture is present, and zoledronic acid first-line. The safety anchor is ensuring calcium and vitamin D repletion before the first infusion to avoid symptomatic hypocalcaemia. [2] [12]
The traps are the mirror image of the anchors. Calling any low Z-score osteoporosis over-treats a child; using the T-score in a child is always wrong; missing a vertebral fracture behind a reassuring density delays the drug; treating hypophosphatasia with a bisphosphonate worsens it; and giving a bisphosphonate to a calcium- or vitamin D-deficient child causes symptomatic hypocalcaemia. The single most preventable error is reading the density number alone and ignoring the lateral spine, because the spine — not the density — decides whether the child has osteoporosis. [1] [10]
References
- [1]Bishop N, Arundel P, Clark E, et al. Fracture prediction and the definition of osteoporosis in children and adolescents: the ISCD 2013 Pediatric Official Positions. J Clin Densitom, 2014.PMID 24631254
- [2]Weber DR, Boyce A, Gordon C, et al. The Utility of DXA Assessment at the Forearm, Proximal Femur, and Lateral Distal Femur, and Vertebral Fracture Assessment in the Pediatric Population: 2019 ISCD Official Position. J Clin Densitom, 2019.PMID 31421951
- [3]Shuhart CR, Yeap SS, Anderson PA, et al. Executive Summary of the 2019 ISCD Position Development Conference on Monitoring Treatment, DXA Cross-calibration and Least Significant Change, Spinal Cord Injury, Peri-prosthetic and Orthopedic Bone Health, Transgender Medicine, and Pediatrics. J Clin Densitom, 2019.PMID 31400968
- [4]Ciancia S, Högler W, Sakkers RJB, et al. Osteoporosis in children and adolescents: how to treat and monitor? Eur J Pediatr, 2023.PMID 36472650
- [5]Cannalire G, Biasucci G, Bertolini L, et al. Osteoporosis and Bone Fragility in Children: Diagnostic and Treatment Strategies. J Clin Med, 2024.PMID 39201093
- [6]Formosa MM, Christou MA, Mäkitie O Bone fragility and osteoporosis in children and young adults. J Endocrinol Invest, 2024.PMID 37668887
- [7]Ward LM, Bakhamis SA, Koujok K Approach to the Pediatric Patient With Glucocorticoid-Induced Osteoporosis. J Clin Endocrinol Metab, 2025.PMID 39126675
- [8]LeBlanc CM, Ma J, Taljaard M, et al. Incident Vertebral Fractures and Risk Factors in the First Three Years Following Glucocorticoid Initiation Among Pediatric Patients With Rheumatic Disorders. J Bone Miner Res, 2015.PMID 25801315
- [9]Humphrey MB, Russell L, Danila MI, et al. 2022 American College of Rheumatology Guideline for the Prevention and Treatment of Glucocorticoid-Induced Osteoporosis. Arthritis Rheumatol, 2023.PMID 37845798
- [10]Marini JC, Forlino A, Bächinger HP, et al. Osteogenesis imperfecta. Nat Rev Dis Primers, 2017.PMID 28820180
- [11]Ward LM, Choudhury A, Alos N, et al. Zoledronic Acid vs Placebo in Pediatric Glucocorticoid-induced Osteoporosis: A Randomized, Double-blind, Phase 3 Trial. J Clin Endocrinol Metab, 2021.PMID 34228102
- [12]Simm PJ, Biggin A, Zacharin MR, et al. Consensus guidelines on the use of bisphosphonate therapy in children and adolescents. J Paediatr Child Health, 2018.PMID 29504223
- [13]Ward L, Tricco AC, Phuong P, et al. Bisphosphonate therapy for children and adolescents with secondary osteoporosis. Cochrane Database Syst Rev, 2007.PMID 17943849
- [14]Ward LM, Weber DR, Wong SC, et al. A Parent Project Muscular Dystrophy-sponsored International Workshop Report on Endocrine and Bone Issues in Patients with Duchenne Muscular Dystrophy: An Ever-changing Landscape. J Neuromuscul Dis, 2025.PMID 39973454