Paeds · endocrinology-diabetes-and-growth
SIADH and disorders of water balance
Also known as SIADH · Syndrome of inappropriate antidiuretic hormone secretion · Syndrome of inappropriate antidiuresis · Hyponatraemia · Dilutional hyponatraemia · Cerebral salt wasting · Water intoxication · Hyponatraemic encephalopathy
Fellowship guide to SIADH and disorders of water balance in children: the antidiuretic hormone axis from hypothalamic osmoreceptor to renal aquaporin-2, the volume-status approach to hyponatraemia, the euvolaemic dilutional picture of SIADH versus the dry salt-losing picture of cerebral salt wasting, fluid restriction for chronic disease, hypertonic 3 per cent saline for the seizing child, and the sodium correction rate that must stay under 8 mmol per litre a day to avoid osmotic demyelination.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The organising principle is water, not salt. Serum sodium is a ratio of sodium to water, so a low sodium usually means the body is holding on to free water it should be excreting. The gatekeeper of that free water is antidiuretic hormone (ADH, also called arginine vasopressin), released from the posterior pituitary when the hypothalamic osmoreceptors sense a rising osmolality. When ADH is switched on inappropriately, the kidney reabsorbs water it should be losing, the urine stays concentrated, and the serum dilutes. Read every hyponatraemia through the question "why is this child not excreting free water?" and the diagnosis follows. [3] [8]
This page covers the full breadth of paediatric water-balance disorders on the low-sodium side: the ADH axis, the volume-status approach to hyponatraemia, SIADH and its causes, the crucial distinction from cerebral salt wasting, hospital-acquired hyponatraemia from hypotonic fluids, acute management with hypertonic saline, chronic management with fluid restriction and urea, and the sodium correction rate that governs the risk of osmotic demyelination. It deliberately stops at the water-losing disorders: diabetes insipidus and the polyuria-polydipsia workup are owned by their own leaf and only cross-referenced here. [1] [8]
Overview & Definition
Hyponatraemia is a serum sodium below 135 mmol per litre, and it is the commonest electrolyte disturbance in hospitalised children. [4] Severity is graded by the number and by the symptoms: mild is roughly 130 to 134, moderate 125 to 129, and profound under 125 mmol per litre, but the sodium value alone never dictates urgency — a child who is seizing at 128 is a bigger emergency than a well child at 118. [1] [2]
SIADH is the syndrome of inappropriate antidiuretic hormone secretion, more precisely called the syndrome of inappropriate antidiuresis. It is euvolaemic hypotonic hyponatraemia caused by ADH acting when the low osmolality should have switched it off. The kidney cannot dilute the urine, free water is retained, and the serum sodium falls even though total body sodium is close to normal. [8] [12]
The two numbers that anchor the whole topic are chronicity and rate. Acute hyponatraemia (developed over under 48 hours) causes cerebral oedema because the brain has not had time to adapt, so it presents with encephalopathy and tolerates faster correction. Chronic hyponatraemia (over 48 hours or unknown duration) is far more dangerous to correct, because the adapted brain is vulnerable to osmotic demyelination if the sodium rises too fast. Assume any hyponatraemia of unknown duration is chronic. [3] [10]
Classification
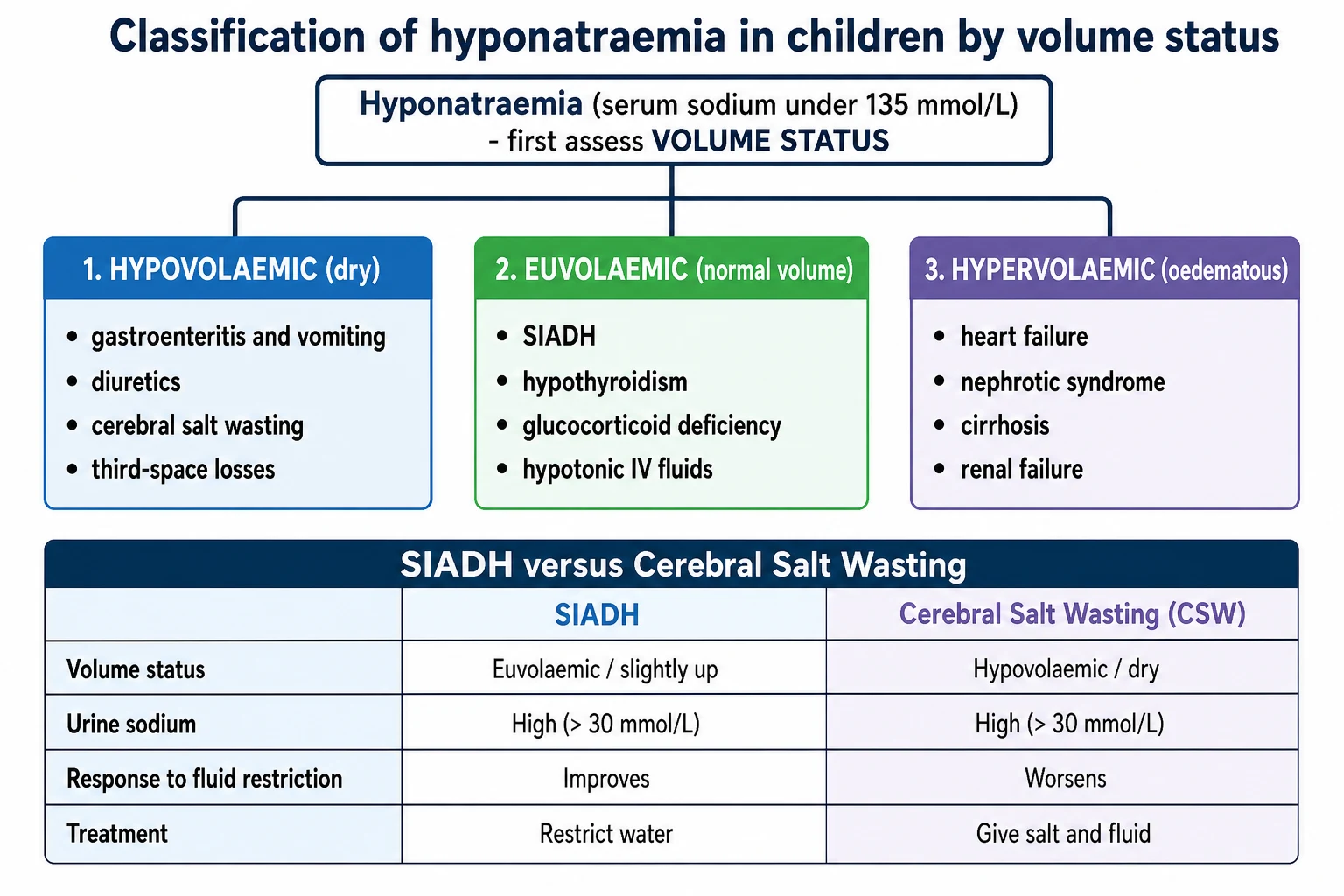
The first question at the bedside is not "what is the number" but "is this child dry, normal, or overloaded" — because volume status splits hyponatraemia into three clean groups and points straight at the mechanism. [1] [2] A dry (hypovolaemic) child has lost both salt and water and is holding water back through volume-driven ADH; a normal-volume (euvolaemic) child is retaining pure water, which is SIADH until proven otherwise; an overloaded (hypervolaemic) child has an excess of total body water that outstrips their sodium, as in heart failure or nephrotic syndrome. [3]
Before any of that, a fast check rules out the impostors. True hyponatraemia is hypotonic, so measure the serum osmolality: a normal or high osmolality means the sodium is not really low in a biological sense. [12] Pseudohyponatraemia (a lab artefact of high lipids or protein) has a normal measured osmolality, and translocational hyponatraemia from hyperglycaemia has a high osmolality because glucose pulls water into the blood and dilutes the sodium. Correct the measured sodium up by about 2.4 mmol per litre for every 5.5 mmol per litre that glucose sits above normal. [3] [12]
Hypovolaemic (dry)
- Salt and water both lost, water lost less than salt
- Renal losses: diuretics, cerebral salt wasting, salt-losing nephropathy
- Extrarenal losses: gastroenteritis, vomiting, third-space, burns
- Volume-driven ADH holds water back, worsening the low sodium
Euvolaemic (normal volume)
- Pure water retention with near-normal total body sodium
- SIADH is the archetype and a diagnosis of exclusion
- Also hypothyroidism, glucocorticoid deficiency, hypotonic fluids
- No oedema, no signs of dehydration
Hypervolaemic (overloaded)
- Total body water rises more than total body sodium
- Heart failure, nephrotic syndrome, cirrhosis, renal failure
- Oedema, effusions, weight gain
- Effective circulating volume is low, so ADH is on
Not truly hypotonic (impostors)
- Check serum osmolality first to confirm hypotonicity
- Pseudohyponatraemia: high lipids or protein, normal osmolality
- Hyperglycaemia: glucose pulls water in, high osmolality
- Correct sodium up 2.4 mmol/L per 5.5 mmol/L glucose over normal
Epidemiology & Risk Factors
Hyponatraemia is common and mostly made in hospital. Up to a quarter of acutely unwell children develop a low sodium during admission, and the dominant driver is the combination of a stimulus to ADH release (pain, nausea, surgery, respiratory or central nervous system illness) with the administration of hypotonic intravenous fluid. [4] [6] This is why isotonic maintenance fluid is now the standard of care: it removes the free-water load that turns a physiological ADH surge into a dangerous dilutional fall. [5]
The children most at risk of symptomatic disease are the postoperative child, the child with a central nervous system insult (meningitis, encephalitis, head injury, brain tumour, neurosurgery), the child with significant respiratory illness (pneumonia, bronchiolitis), and any child receiving hypotonic fluids. [7] [8] SIADH specifically clusters around these same triggers, because they all stimulate non-osmotic ADH release. [8]
The causes of SIADH follow four families that are worth memorising, because naming the trigger is half the management. [8] [12] The dangerous shared feature is that the trigger is often obvious once looked for — a chest full of pneumonia, a recent craniopharyngioma resection, a new anticonvulsant — so the diagnosis is usually made by recognising the setting, not by a rare test. [8]
SIADH
Postoperative pain, nausea, and stress are the commonest non-osmotic ADH triggers in hospital
Meningitis, encephalitis, head injury, tumours, and neurosurgery — the CNS drives inappropriate ADH
Pneumonia, bronchiolitis, and positive-pressure ventilation all stimulate ADH release
Carbamazepine, oxcarbazepine, vincristine, cyclophosphamide, SSRIs, and desmopressin
Consider malignancy in adults; in children, rare gain-of-function V2 receptor mutations cause nephrogenic SIAD
Cerebral salt wasting shares the same high-risk population — the neurosurgical and brain-injured child — which is exactly why it is so easily confused with SIADH. [9] A series of children with intracranial disorders showed that renal salt wasting is a real and distinct entity in this group, presenting with hyponatraemia, high urine sodium, polyuria, and clinical volume depletion, and that mislabelling it as SIADH and restricting fluid is harmful. [9]
Pathophysiology
Antidiuretic hormone is the master switch for free water. When plasma osmolality rises, hypothalamic osmoreceptors trigger ADH release from the posterior pituitary; ADH binds V2 receptors on the renal collecting duct, drives aquaporin-2 water channels into the apical membrane, and reabsorbs water, concentrating the urine and diluting the blood back to normal. When osmolality falls, ADH switches off, the collecting duct becomes water-impermeable, and the child excretes dilute urine to shed the excess water. [3] [8]
In SIADH, that off-switch fails. ADH keeps acting despite a low osmolality, so the collecting duct stays water-permeable, free water is retained, and the serum sodium falls. Because volume expansion triggers a compensatory natriuresis, the child does not become oedematous; they stay euvolaemic with a near-normal total body sodium but an increased total body water. The urine is inappropriately concentrated (osmolality over 100 mOsm per kg) and the urine sodium is high (over 30 mmol per litre) because the kidney is excreting the small sodium load it is given. [8] [12]
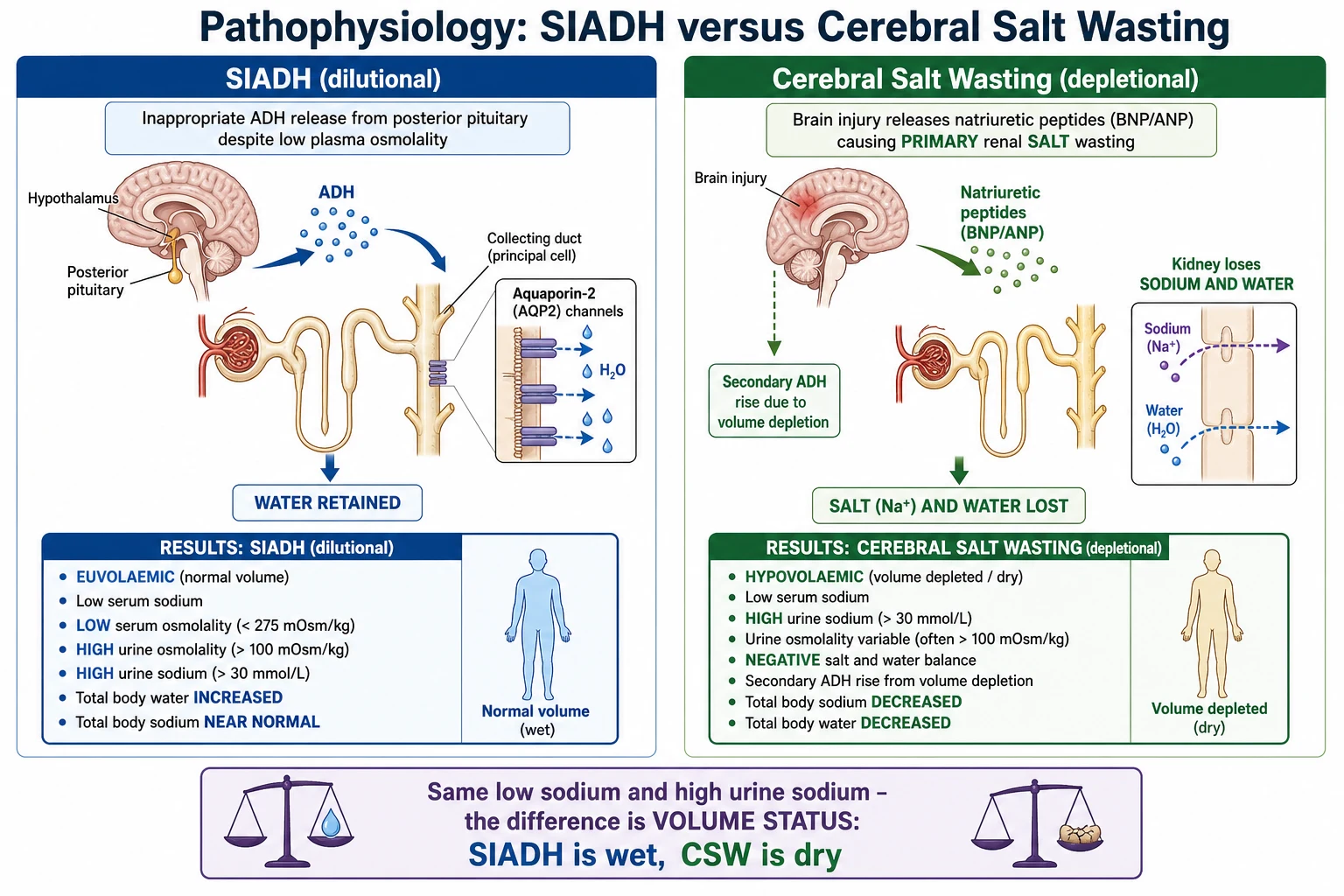
Cerebral salt wasting inverts the primary event. Here the problem starts in the kidney, not the pituitary: a brain insult drives excessive renal sodium excretion (natriuretic peptides are implicated), so the child loses sodium and water together and becomes genuinely volume depleted. The falling circulating volume then switches ADH on appropriately as a secondary event, which holds water back and deepens the hyponatraemia. The result mimics SIADH biochemically — low sodium, high urine sodium — but the child is dry, and giving fluid restriction removes the volume they are already losing. [9] [3]
Hospital-acquired hyponatraemia is the third mechanism, and it is the most preventable. A sick child almost always has a non-osmotic stimulus to ADH (pain, nausea, illness), so their kidney cannot excrete free water normally. Give that child a hypotonic maintenance fluid and the retained free water dilutes the serum sodium directly. The physiology is simple and the consequence can be fatal, which is why isotonic fluid is the default. [6] [7]
Clinical Presentation
Hyponatraemia is a brain disease before it is anything else, because the falling serum osmolality pulls water into brain cells and causes cerebral oedema. Mild or slowly developing hyponatraemia may be silent or cause only headache, nausea, lethargy, and irritability. As the sodium falls further or faster, the child becomes confused and obtunded, then develops vomiting, seizures, respiratory depression, and finally brainstem herniation. [7] [3]
The single most important modifier is speed. In acute hyponatraemia the brain has no time to adapt, so a child can seize at a sodium that a chronically adapted child tolerates while walking around. This is why symptoms, not the number, drive the urgency of treatment, and why any child on intravenous fluids who becomes headachey, drowsy, or starts vomiting must have an immediate sodium checked. [7] [6]
The presentation also carries clues to the cause. A dry child with sunken eyes, delayed capillary refill, and a history of gastroenteritis has hypovolaemic hyponatraemia; a child with oedema and a raised jugular venous pressure has hypervolaemic hyponatraemia; a well-perfused, normal-volume child with a pneumonia or a recent neurosurgery is the SIADH picture. A brain-injured child who is passing large volumes of urine and looks dry, rather than dry from vomiting, should raise cerebral salt wasting. [9] [8]
Differential Diagnosis
The differential of a low sodium is built on the same axis that classifies it: confirm true hypotonicity, then read the volume status. [12] [3] Start by excluding the impostors with a serum osmolality — a normal or high value points to pseudohyponatraemia or hyperglycaemia rather than a genuine water excess. Only once the osmolality is low (under 275 mOsm per kg) is this a true hypotonic hyponatraemia worth working through. [12]
The critical paediatric distinction is SIADH versus cerebral salt wasting, because they share a low sodium and a high urine sodium yet demand opposite treatments. [9] The discriminator is volume status, supported by the trend in urine output and fluid balance: the SIADH child is euvolaemic or mildly water-loaded with a low or normal urine output, while the salt-wasting child is volume depleted with a high urine output and a negative sodium and water balance. If in genuine doubt, a cautious fluid challenge helps — the salt-waster improves with saline, the SIADH child does not. [9] [3]
Points to SIADH
- Euvolaemic: no dehydration, no oedema
- Low or normal urine output, positive or neutral fluid balance
- Urine osmolality over 100, urine sodium over 30 mmol/L
- Improves with fluid restriction; a known ADH trigger present
Points to cerebral salt wasting
- Hypovolaemic: dry, tachycardic, weight loss
- High urine output with a negative sodium and water balance
- Urine sodium high (often very high), urine osmolality variable
- Worsens with fluid restriction; improves with salt and volume
Points to hypovolaemic non-renal loss
- History of vomiting, diarrhoea, or third-space loss
- Clinically dry with delayed capillary refill
- Urine sodium low (under 20) as the kidney conserves sodium
- Corrects with isotonic volume replacement
Must-exclude endocrine mimics
- Adrenal insufficiency: hyperkalaemia, hypoglycaemia, hypotension
- Hypothyroidism: goitre, growth failure, bradycardia
- Both can mimic SIADH biochemically
- Do not diagnose SIADH until these are excluded
The endocrine mimics deserve their own attention because they are treatable and dangerous if missed. Glucocorticoid deficiency (secondary adrenal insufficiency) causes a euvolaemic hyponatraemia that looks exactly like SIADH, because cortisol lack removes the tonic suppression of ADH. Hypothyroidism does the same. Both should be excluded with a cortisol and thyroid function before the label SIADH is applied, particularly in a child with no obvious ADH trigger. [8] [12]
Clinical & Bedside Assessment
The bedside assessment starts with the brain and the airway, because a hyponatraemic child can seize and lose their airway without warning. Assess conscious level, look for headache, vomiting, and focal signs, and be ready to treat encephalopathy before the workup is complete. A child who is drowsy or fitting from a low sodium is a resuscitation, not a puzzle. [7] [3]
The second task is the volume examination, because it is the single most decisive clinical judgement in the whole topic. Look for the dry signs (sunken eyes and fontanelle, dry mucous membranes, prolonged capillary refill, tachycardia, weight loss, low urine output) and the wet signs (peripheral or periorbital oedema, raised jugular venous pressure, hepatomegaly, ascites, weight gain). A child who is neither dry nor overloaded, with a normal capillary refill and no oedema, is euvolaemic — the SIADH picture. [1] [9]
Take a focused history that hunts for the ADH trigger and the salt-wasting setting: recent surgery or neurosurgery, a central nervous system or chest illness, new drugs (carbamazepine, oxcarbazepine, vincristine, cyclophosphamide, desmopressin), the type and volume of any intravenous fluid, and the pattern of urine output. The context usually names the cause: a child on hypotonic maintenance fluid after an appendicectomy who becomes drowsy has hospital-acquired hyponatraemia, not a rare syndrome. [6] [8]
Investigations
The investigation of hyponatraemia is a short, logical bundle that confirms hypotonicity, classifies by the paired serum and urine chemistry, and excludes the endocrine mimics. The three tests that do most of the work are the serum osmolality, the urine osmolality, and the urine sodium, all sent before any fluid is changed. [12] [1]
Investigation bundle for hyponatraemia
Serum sodium and serum osmolality — confirm a true hypotonic hyponatraemia (osmolality under 275 mOsm/kg)
Urine osmolality — high (over 100 mOsm/kg) means ADH is acting; a maximally dilute urine points to water overload or reset osmostat
Urine sodium — over 30 mmol/L in SIADH and salt wasting; under 20 mmol/L in hypovolaemic non-renal loss
Glucose — exclude translocational hyponatraemia and correct the sodium for it
Paired volume assessment — the clinical read that separates SIADH from cerebral salt wasting
Morning cortisol and thyroid function — exclude adrenal insufficiency and hypothyroidism before labelling SIADH
Urea, creatinine, and fluid balance chart with daily weight — track the trend and effective circulating volume
Look for the trigger: chest imaging, neuroimaging, and a drug review as the context demands
The classic SIADH biochemistry is a low serum sodium, a low serum osmolality under 275 mOsm per kg, an inappropriately concentrated urine over 100 mOsm per kg, a urine sodium over 30 mmol per litre, in a euvolaemic child who is not on diuretics and who has normal thyroid, adrenal, and renal function. [8] [12] The low serum urate that often accompanies SIADH is a useful supporting clue but not a diagnostic one. Because SIADH is a diagnosis of exclusion, the negative tests (cortisol, thyroid, renal function) matter as much as the positive ones. [12]
PIMS — isotonic versus hypotonic maintenance fluid (McNab 2015)
Lancet
Randomised, double-blind trial in 690 hospitalised children comparing maintenance intravenous fluid containing 140 mmol/L of sodium (isotonic) with 77 mmol/L of sodium (hypotonic), with the development of hyponatraemia as the primary outcome.
Key finding
Children given the hypotonic fluid were significantly more likely to develop hyponatraemia than those given the isotonic fluid, with no increase in adverse effects from the isotonic solution.
Practice change
Isotonic maintenance fluid became the default for hospitalised children, and the American Academy of Pediatrics guideline now recommends it — directly preventing hospital-acquired hyponatraemia.
Management — Resuscitation
Acute symptomatic hyponatraemia — a seizure, coma, or a depressed conscious level from a low sodium — is a medical emergency treated with hypertonic saline, not with slow fluid restriction. The goal in the seizing child is small and specific: raise the serum sodium by 4 to 6 mmol per litre, which is enough to reverse the cerebral oedema and stop the fit, and then stop the rapid correction. [7] [3]
The standard emergency drug is intravenous 3 per cent saline, given as a bolus of about 2 mL per kilogram (commonly capped near 100 mL) over 10 to 15 minutes, repeated once or twice if seizures continue, until the sodium has risen by the target 4 to 6 mmol per litre or the seizure stops. [7] [3] Each 2 mL per kilogram bolus of 3 per cent saline raises the serum sodium by roughly 2 mmol per litre. Alongside the saline, manage the seizure and airway as for any seizing child, and get senior and intensive care help early. [7]
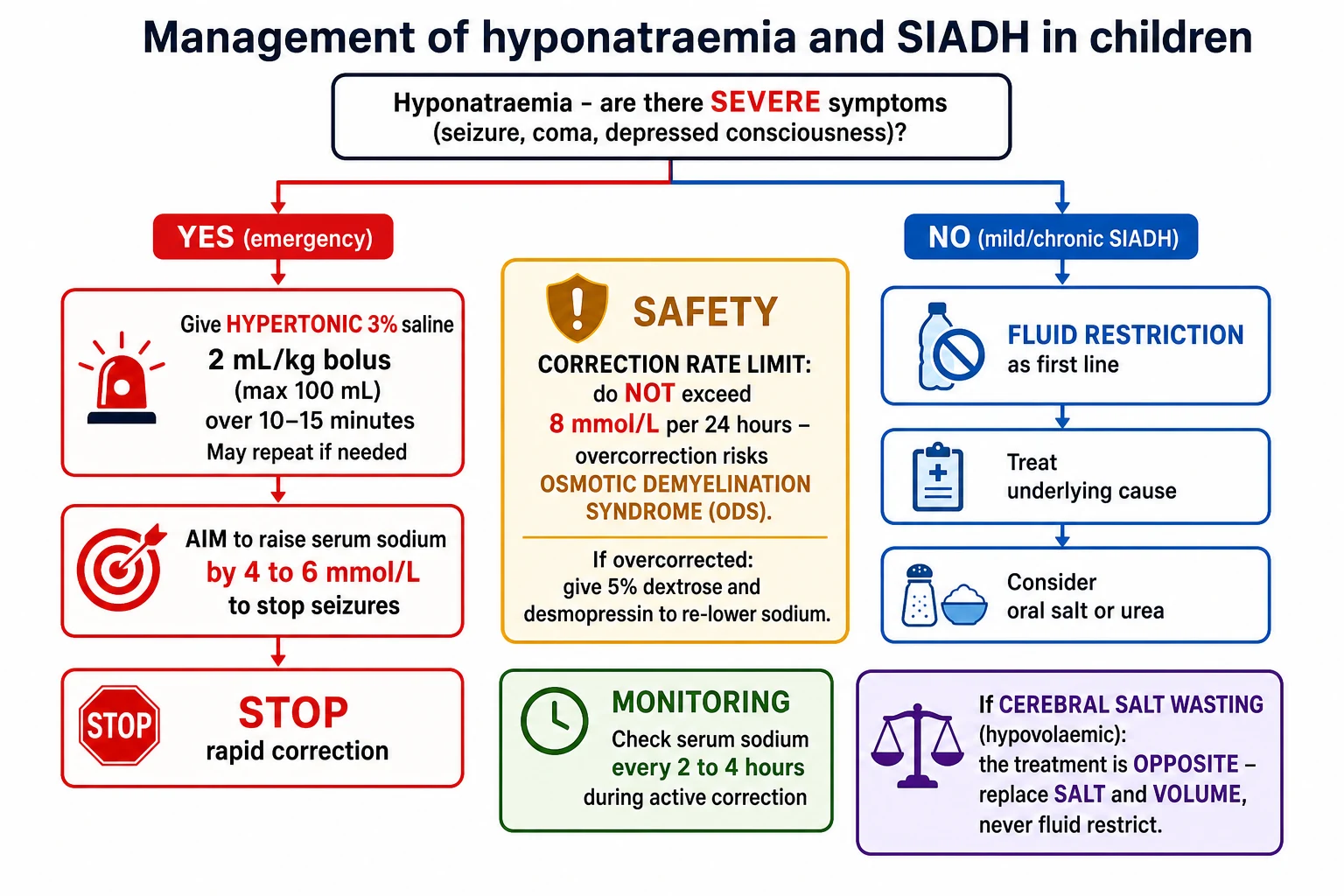
Once the child is out of danger, the pace changes completely. The emergency correction buys time; it does not license continued rapid correction. After the target rise is achieved and the seizure has stopped, hold further hypertonic saline and switch to careful, slow management guided by frequent sodium measurements, checking the level every 2 to 4 hours during active correction. The total rise over the first 24 hours must still respect the ceiling that protects against osmotic demyelination. [10] [3]
Hypertonic 3% saline (acute symptomatic hyponatraemia)
Management — Definitive & Stepwise
Once the emergency is over, the definitive management is driven by the cause and the volume status, and for SIADH the first-line treatment is fluid restriction. Restricting free-water intake to below the child's insensible plus urinary losses allows the retained water to be excreted and the sodium to drift up slowly and safely. Treating the underlying trigger — the pneumonia, the drug, the postoperative pain and nausea — is just as important, because SIADH resolves when its stimulus is removed. [8] [12]
Definitive pathway once the emergency is controlled
Confirm the diagnosis and volume status: euvolaemic SIADH versus hypovolaemic salt wasting versus hypervolaemic states
For SIADH: restrict free-water intake below insensible plus urinary losses
Treat the trigger: the chest illness, the CNS insult, the offending drug
Switch any hypotonic intravenous fluid to isotonic fluid
Recheck the sodium every 2–4 hours while actively correcting, then space out as it stabilises
For refractory or chronic SIADH: add oral salt, and consider oral urea under specialist care
For cerebral salt wasting: replace salt and volume — do the opposite of fluid restriction
Cap the total sodium rise at 8 mmol/L in 24 hours; if exceeded, re-lower with dextrose and desmopressin
For chronic or refractory SIADH where fluid restriction alone cannot maintain a safe sodium, the next steps are oral salt supplementation and, under specialist care, oral urea, which produces an osmotic diuresis that offloads free water. A paediatric case series showed oral urea to be an effective, safe, and inexpensive long-term treatment for chronic syndrome of inappropriate antidiuresis in children, restoring and maintaining a normal sodium. [11] Vasopressin receptor antagonists (the vaptans) are used in adults but are not established in children and are generally avoided in paediatric practice. [8]
Oral urea (chronic or refractory SIADH)
The management of the impostors is different by design. The hypovolaemic child (gastroenteritis, salt wasting) needs isotonic volume and salt, never restriction. [9] The hypervolaemic child (heart failure, nephrotic syndrome) needs treatment of the underlying disease with sodium and water restriction and often a diuretic. The hyperglycaemic child needs their glucose corrected. Naming the box on the volume-status figure names the treatment. [3] [12]
The European guideline (Spasovski 2014), the United States expert panel (Verbalis 2013), and the guideline compilation (Hoorn 2017) agree on the core principles: confirm hypotonicity, classify by volume status, treat symptomatic disease with hypertonic saline aiming for a small initial rise, treat SIADH with fluid restriction and cause removal, and respect a strict correction-rate ceiling to prevent osmotic demyelination. They differ in the fine detail of thresholds and of urea and vaptan use, but the direction of travel is shared. [1] [2] [12]
Specific Subtypes & Scenarios
The four scenarios below are the ones that come up on the ward, in retrieval, and in the exam. [8] [9]
Postoperative and hospital-acquired hyponatraemia is the commonest and most preventable. A child after surgery has pain, nausea, and stress driving ADH, so any hypotonic maintenance fluid is retained as free water and dilutes the sodium. The countermeasure is isotonic maintenance fluid as standard and a low threshold to check the sodium in any child who deteriorates neurologically on fluids. [6] [5]
SIADH from a central nervous system or chest illness is the archetypal euvolaemic picture. Meningitis, encephalitis, head injury, brain tumours, pneumonia, and bronchiolitis all stimulate ADH; the child is well perfused and not oedematous, the urine is concentrated with a high sodium, and the treatment is fluid restriction plus treatment of the underlying illness. Naming the trigger settles the diagnosis. [8] [12]
Cerebral salt wasting is the trap. It occurs in the same neurosurgical and brain-injured children as SIADH and looks identical on the blood and urine chemistry, but the child is volume depleted with a high urine output and a negative salt and water balance. Fluid restriction — the correct SIADH treatment — worsens salt wasting by removing volume the child is already losing. The treatment is salt and volume replacement, and the tie-breaker is the fluid balance chart and daily weight. [9] [3]
The postneurosurgical triphasic response ties this leaf to its diabetes-insipidus neighbour. After pituitary or hypothalamic surgery (for example, craniopharyngioma), the child may pass through an initial diabetes insipidus phase (polyuria, high sodium), then an interim SIADH phase (as stored ADH is released, causing hyponatraemia around days 5 to 10), and then a return to diabetes insipidus. Anticipating the swing prevents both overtreatment of the transient SIADH and undertreatment of the recurrent diabetes insipidus. [8]
Complications & Pitfalls
Untreated hyponatraemic encephalopathy kills through cerebral oedema — seizures, respiratory arrest, permanent brain injury, and herniation — and young children are especially vulnerable because their brain-to-skull ratio leaves little room to swell. [7] The danger, though, is double: the low sodium harms the child, and so does correcting it wrongly. [3]
Harms of the low sodium
- Cerebral oedema, seizures, and respiratory arrest
- Obtundation progressing to herniation if untreated
- Children at higher risk than adults for a given sodium
- Acute falls are more dangerous than chronic ones
Harms of correcting it wrongly
- Overcorrection causes osmotic demyelination syndrome
- Fluid restriction in salt wasting deepens the deficit
- Chasing the sodium to normal after the seizure has stopped
- Missing adrenal insufficiency and treating as SIADH
The gravest iatrogenic complication is osmotic demyelination syndrome, caused by correcting a chronic hyponatraemia too fast. The adapted brain has extruded osmolytes to shrink back to normal size; a rapid rise in serum sodium then pulls water out of neurons and demyelinates the pons and other regions. The injury is delayed by days, often irreversible, and can leave a locked-in state or death — which is why the correction rate matters as much as the treatment. [10] [3] The countermeasure is a hard ceiling on the rate, frequent monitoring, and the willingness to actively re-lower the sodium with dextrose and desmopressin if the child overshoots. [10]
The commonest cognitive pitfall is diagnosing SIADH without excluding its mimics or without confirming euvolaemia — restricting fluid in a child who is actually salt wasting or adrenally insufficient. The second is treating the number rather than the child: giving hypertonic saline to a well, chronically hyponatraemic child, or conversely delaying it in a seizing one. The third is continuing hypotonic maintenance fluid in a sick child and manufacturing the problem. [9] [6]
Prognosis & Disposition
The prognosis of hyponatraemia depends on how fast it developed, how deep it fell, whether encephalopathy occurred, and — crucially — how it was corrected. Mild, slowly developing, promptly treated hyponatraemia recovers fully. Severe acute hyponatraemic encephalopathy carries a real risk of death or permanent neurological injury, and a proportion of the worst outcomes are iatrogenic, from either untreated cerebral oedema or overcorrection. [7] [10]
SIADH itself usually resolves when its trigger resolves, so most hospital SIADH is transient and the long-term outlook is that of the underlying illness. Chronic SIADH — from a persistent central nervous system lesion or a rare genetic cause — needs ongoing fluid management and monitoring but is compatible with a normal life when the sodium is kept safe. [8] [11]
Disposition depends on severity. A child with symptomatic hyponatraemia or one requiring hypertonic saline needs high-dependency or intensive care with frequent sodium monitoring during correction. A child with mild, asymptomatic SIADH can often be managed on the ward with fluid restriction and treatment of the cause. Every child leaves with the trigger addressed, a plan for isotonic fluids if further intravenous therapy is needed, and — for chronic disease — a named specialist and a monitoring schedule. [1] [12]
Special Populations
The neonate and young infant is especially vulnerable to water intoxication, because incorrectly reconstituted formula, excessive water feeds, or hypotonic fluids can rapidly dilute a small circulating volume. A neonate with hyponatraemia and seizures may have been overdiluted, and the same hypertonic-saline and slow-correction principles apply, scaled to size. Prevention through correct formula preparation and isotonic fluids is the priority. [7] [6]
The neurosurgical and brain-injured child carries the highest burden of both SIADH and cerebral salt wasting, and often swings between water-retaining and salt-wasting states, including the triphasic response after pituitary surgery. These children need meticulous fluid balance charting, daily weights, and frequent paired serum and urine chemistry, because the correct treatment can invert from day to day. [9] [8]
The child with malignancy is at risk from both the disease and its treatment: central nervous system tumours drive SIADH, and chemotherapy agents such as vincristine and cyclophosphamide are classic drug causes. In these children, hyponatraemia may be the first clue to a new intracranial problem or a drug effect, and the fluid plan around chemotherapy must account for the ADH stimulus. [8] [12]
The child on chronic anticonvulsants or psychotropics can develop drug-induced SIADH, particularly with carbamazepine and oxcarbazepine. A gradual, asymptomatic hyponatraemia in a child on these agents is common; the response is to recognise the drug cause, monitor, and adjust rather than to reflexively restrict fluid or escalate. [8] [2]
Evidence, Guidelines & Regional Differences
The evidence base rests on two major clinical practice guidelines — the European guideline (Spasovski 2014) and the United States expert panel (Verbalis 2013) — synthesised in the guideline compilation by Hoorn and Zietse (2017), together with the paediatric-specific work of Moritz and Ayus on hyponatraemic encephalopathy and maintenance fluids, and Sterns on sodium correction and osmotic demyelination. [1] [2] [12] These sources converge on confirming hypotonicity, classifying by volume status, treating symptoms with hypertonic saline for a small initial rise, and respecting a strict correction-rate ceiling. [3] [10]
The largest practice change in children came from the maintenance-fluid literature. The PIMS randomised trial and subsequent evidence showed that hypotonic maintenance fluid causes hyponatraemia, and the American Academy of Pediatrics guideline now recommends isotonic maintenance fluid for most hospitalised children — a simple change that prevents a common and sometimes fatal hospital-acquired condition. [5] [4] [6]
Australia and Aotearoa New Zealand adopted isotonic maintenance fluids early, and paediatric services across the region use isotonic solutions as the default for hospitalised children, informed by the Melbourne-led PIMS trial. Acute symptomatic hyponatraemia is managed with hypertonic 3 per cent saline in emergency and intensive care settings, and cerebral salt wasting is a recognised entity in the neurosurgical population. [5] [9]
The genuine controversies are practical: the exact bolus size and cap for 3 per cent saline in children, whether the ceiling should be 8 or 10 mmol per litre in a given child, the reliability of distinguishing SIADH from cerebral salt wasting at the bedside, and the place of urea in paediatric chronic SIADH. A fellowship candidate names the direction of travel — isotonic fluids, small initial correction, hard rate ceiling — rather than pretending the fine numbers are settled. [10] [11]
Exam Pearls
One-sentence answer: the approach to a hyponatraemic child
A child with hyponatraemia is managed by treating encephalopathy first (hypertonic 3 per cent saline to raise the sodium by only 4 to 6 mmol per litre to stop the seizure), then confirming true hypotonicity and classifying by volume status (euvolaemic points to SIADH, treated by fluid restriction and removing the trigger; hypovolaemic points to salt loss or cerebral salt wasting, treated by giving salt and volume; hypervolaemic points to heart, kidney, or liver disease), while excluding adrenal insufficiency and hypothyroidism, and always keeping the total correction under 8 mmol per litre in 24 hours to avoid osmotic demyelination.
Definition and the water principle
- Hyponatraemia: serum sodium under 135 mmol/L, usually too much water not too little salt
- Confirm true hypotonicity: serum osmolality under 275 mOsm/kg
- Classify by volume status: dry, euvolaemic, or overloaded
- SIADH is euvolaemic hyponatraemia and a diagnosis of exclusion
SIADH biochemistry
- Low serum sodium and low serum osmolality
- Inappropriately concentrated urine (over 100 mOsm/kg)
- High urine sodium (over 30 mmol/L)
- Euvolaemic, not on diuretics, normal thyroid, adrenal, and renal function
Acute emergency management
- Seizure or coma: hypertonic 3% saline 2 mL/kg over 10–15 min
- Aim to raise the sodium by only 4–6 mmol/L to stop the fit, then stop
- Check sodium every 2–4 hours during active correction
- Get senior and intensive care help early
The two great traps
- Cerebral salt wasting mimics SIADH but is dry — give salt and volume, do not restrict
- Overcorrection over 8 mmol/L per 24 h causes osmotic demyelination
- If overcorrected, re-lower with 5% dextrose and desmopressin
- Hypotonic maintenance fluid causes hospital-acquired hyponatraemia — use isotonic
Frequently misremembered facts, stated correctly: in SIADH the urine is inappropriately concentrated, not dilute, because active ADH concentrates it. SIADH and cerebral salt wasting both show a high urine sodium, so urine sodium cannot separate them — only volume status can. The initial correction target in the seizing child is a rise of just 4 to 6 mmol per litre, not a return to normal. And the danger of chronic hyponatraemia is in the correction, not just the low number — keep it under 8 mmol per litre a day. [8] [10]
The one framework that answers everything for the exam is the water-balance loop: osmoreceptor senses osmolality, pituitary releases ADH, ADH drives aquaporin-2 to reabsorb water. SIADH is that switch stuck on despite a low osmolality; cerebral salt wasting is a primary renal salt leak that switches ADH on secondarily through volume depletion; hospital-acquired hyponatraemia is that switch on in a sick child who is then given free water to retain. Know where the water is going, and the diagnosis and the treatment follow. [3] [9]
References
- [1]Spasovski G; Vanholder R; Allolio B; et al Clinical practice guideline on diagnosis and treatment of hyponatraemia. Nephrol Dial Transplant, 2014.PMID 24569496
- [2]Verbalis JG; Goldsmith SR; Greenberg A; et al Diagnosis, evaluation, and treatment of hyponatremia: expert panel recommendations. Am J Med, 2013.PMID 24074529
- [3]Sterns RH Disorders of plasma sodium--causes, consequences, and correction. N Engl J Med, 2015.PMID 25551526
- [4]Feld LG; Neuspiel DR; Foster BA; et al Clinical Practice Guideline: Maintenance Intravenous Fluids in Children. Pediatrics, 2018.PMID 30478247
- [5]McNab S; Duke T; South M; et al 140 mmol/L of sodium versus 77 mmol/L of sodium in maintenance intravenous fluid therapy for children in hospital (PIMS): a randomised controlled double-blind trial. Lancet, 2015.PMID 25472864
- [6]Moritz ML; Ayus JC Maintenance Intravenous Fluids in Acutely Ill Patients. N Engl J Med, 2015.PMID 26422725
- [7]Moritz ML; Ayus JC New aspects in the pathogenesis, prevention, and treatment of hyponatremic encephalopathy in children. Pediatr Nephrol, 2010.PMID 19894066
- [8]Driano JE; Lteif AN; Creo AL Vasopressin-Dependent Disorders: What Is New in Children? Pediatrics, 2021.PMID 33795481
- [9]Bettinelli A; Longoni L; Tammaro F; et al Renal salt-wasting syndrome in children with intracranial disorders. Pediatr Nephrol, 2012.PMID 22237777
- [10]Sterns RH Adverse Consequences of Overly-Rapid Correction of Hyponatremia. Front Horm Res, 2019.PMID 32097948
- [11]Huang EA; Feldman BJ; Schwartz ID; et al Oral urea for the treatment of chronic syndrome of inappropriate antidiuresis in children. J Pediatr, 2006.PMID 16423613
- [12]Hoorn EJ; Zietse R Diagnosis and Treatment of Hyponatremia: Compilation of the Guidelines. J Am Soc Nephrol, 2017.PMID 28174217