Paeds · endocrinology-diabetes-and-growth
Type 1 diabetes: diagnosis and initial management
Also known as New-onset type 1 diabetes · Type 1 diabetes mellitus diagnosis · Islet autoantibodies · C-peptide · Diabetes staging · Partial remission · Honeymoon phase · Initial insulin therapy · Diabetes at presentation · Newly diagnosed diabetes in children
Fellowship guide to the diagnosis and first days of type 1 diabetes in children and adolescents who present without ketoacidosis: the classic symptoms and the diagnostic glucose and HbA1c thresholds, the islet autoantibodies and C-peptide that confirm the autoimmune type and separate it from type 2 and monogenic diabetes, the three-stage model of preclinical to clinical disease, the first subcutaneous basal-bolus insulin regimen, structured family education, and the honeymoon phase. The full ketoacidosis protocol lives on its own leaf.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
This page covers the moment a child is found to have type 1 diabetes and the first days that follow, in the common situation where the child presents unwell with hyperglycaemia but without ketoacidosis. It works through how the diagnosis is made and confirmed, how the autoimmune type is separated from type 2 and monogenic diabetes, and how the first insulin regimen and family education are set up. The full ketoacidosis protocol and the ongoing ambulatory care each live on their own dedicated leaf. [10] [6]
Overview & Definition
Type 1 diabetes is an autoimmune disease in which the body destroys its own insulin-producing beta cells until the child can no longer make enough insulin to live. When enough beta cells are lost, glucose rises, the classic symptoms appear, and the child needs exogenous insulin from that day forward. Diagnosis is the act of recognising that picture and confirming it, and initial management is the safe start of insulin and the education that lets a family take the disease home. [10] [5]
Most children present at stage 3, the clinical onset, with a short history of thirst, frequent urination and weight loss. The task at that first contact is twofold: confirm the diagnosis quickly with a glucose measurement, and decide at once whether the child has simple hyperglycaemia or has tipped into ketoacidosis, because that single fork decides everything that follows. [10] [8]
Classification
Type 1 diabetes is now understood as a continuum that begins years before symptoms, and staging that continuum is the modern way to classify it. The figure sets out the three stages and the features that separate type 1 from the other diabetes types a clinician must exclude. [2] [5]
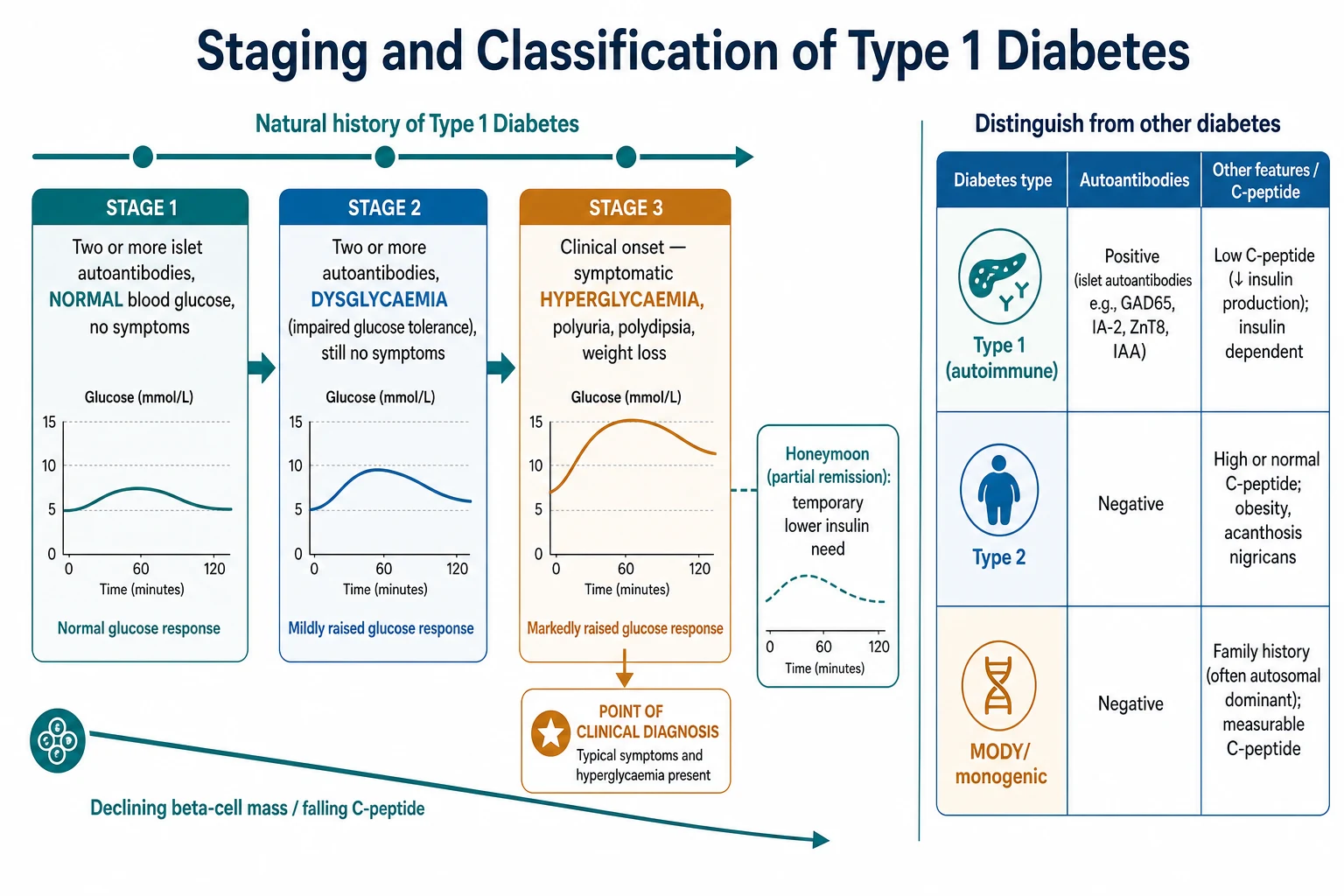
The staging model, defined by JDRF, the Endocrine Society and the American Diabetes Association, uses two variables: the presence of two or more islet autoantibodies, and the glucose status. Stage 1 is two or more autoantibodies with normal glucose and no symptoms. Stage 2 is two or more autoantibodies with dysglycaemia but still no symptoms. Stage 3 is the clinical onset with symptomatic hyperglycaemia, which is where most children are first recognised. [2] [5]
Type 1 diabetes
- Islet autoantibodies positive in most children
- Low or falling C-peptide from insulin deficiency
- Insulin dependent from diagnosis
- Any body habitus; ketosis-prone
Type 2 diabetes
- Autoantibodies negative
- High or normal C-peptide early on
- Obesity, acanthosis nigricans, family history
- Often responds initially to metformin
Monogenic (MODY/neonatal)
- Autoantibodies negative
- Measurable C-peptide beyond the honeymoon
- Strong autosomal-dominant family history
- Onset under six months points to neonatal diabetes
The clinical value of staging is that it names what a positive antibody screen in a well child actually means. Such a child has preclinical type 1 diabetes, not a false alarm, and needs surveillance and family education rather than reassurance. The staging language also frames the emerging option of therapy that delays the move from stage 2 to stage 3. [1] [9]
Epidemiology & Risk Factors
Type 1 diabetes is one of the commonest chronic diseases of childhood, and its incidence has risen steadily across recent decades in most high-income countries. Population surveillance in the United States confirms a climbing prevalence of youth-onset type 1 diabetes over the last twenty years, so the number of new diagnoses a general paediatrician must recognise keeps growing. [11]
The main risk factor is genetic, carried largely in the HLA class II region, with a smaller contribution from other genes. A child with an affected first-degree relative has a several-fold higher risk than the background population, though most new cases occur in children with no family history at all. Environmental triggers, including viral infections, are thought to initiate the autoimmunity in a susceptible child, but no single trigger is established. [10] [3]
The peak ages at diagnosis are the early school years and again around puberty, but type 1 diabetes occurs at every age including infancy. The rate of progression from autoantibody positivity to clinical disease is fastest in the youngest children and in those with the most autoantibodies, which is why a toddler with multiple antibodies warrants closer surveillance than an older child with one. [3] [5]
Pathophysiology
To understand the diagnosis, follow the disease from its silent start to the day glucose rises. In a genetically susceptible child, an environmental trigger sets off a T-cell-mediated attack on the pancreatic islets, an inflammatory process called insulitis. Over months to years the attack destroys beta cells while sparing the other islet cells, and the child makes progressively less insulin. [10] [3]
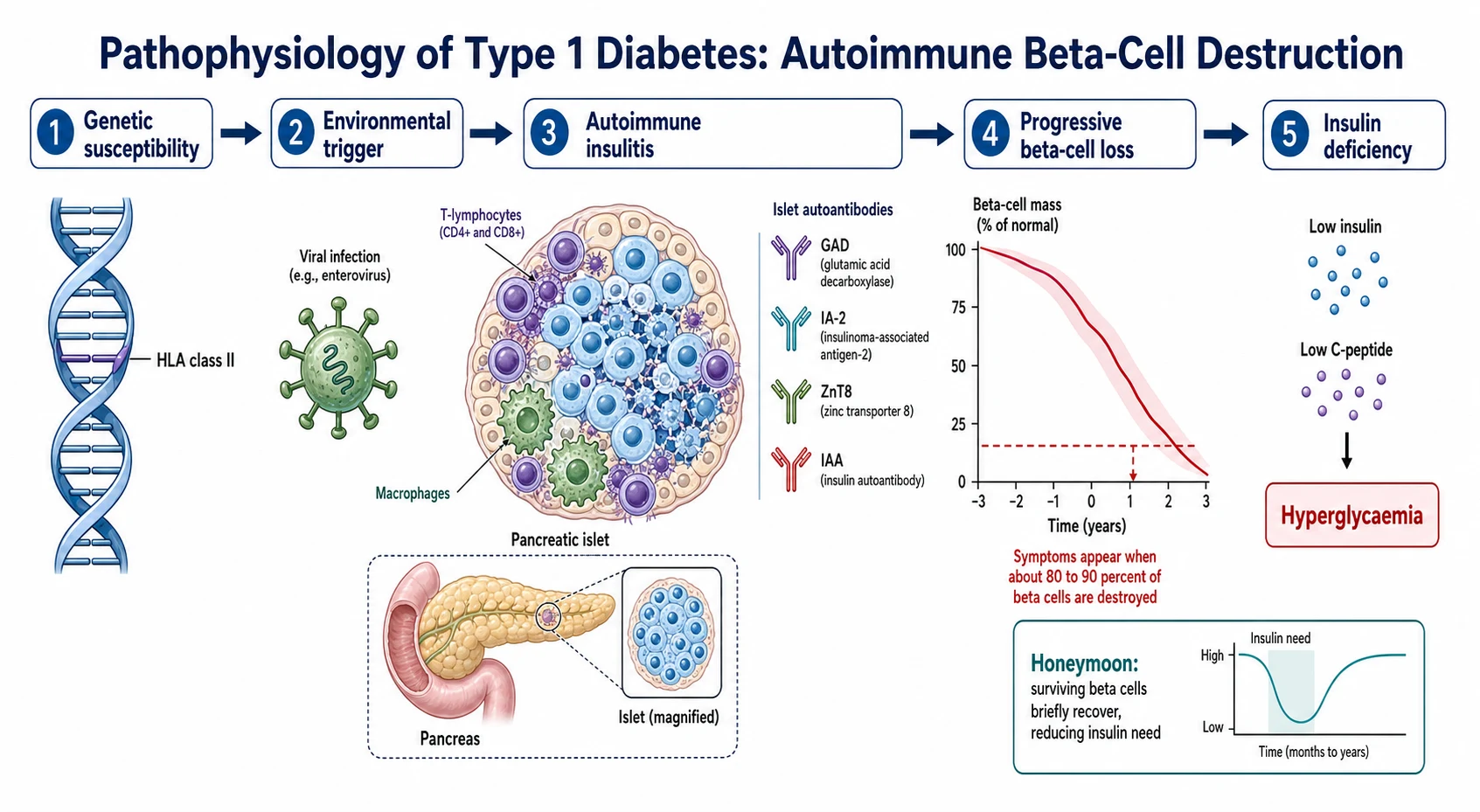
Symptoms appear only when about 80 to 90 percent of beta-cell function is lost, which is why a child can look completely well until a short, dramatic final decline. Once insulin falls below the level needed to move glucose into cells, glucose accumulates in the blood, spills into the urine, and drags water with it, producing the osmotic diuresis that causes the polyuria, thirst and dehydration. Fat is broken down for fuel, generating the ketones that, if unchecked, lead to ketoacidosis. [10] [8]
The islet autoantibodies are the fingerprints of this attack. Antibodies to glutamic acid decarboxylase, to insulinoma-associated antigen-2, to the zinc transporter ZnT8, and to insulin itself appear as beta cells are destroyed, and their presence marks the autoimmune process rather than causing it. C-peptide, released in equal amounts to insulin when the pancreas secretes it, is the mirror measure: as beta cells fail, C-peptide falls, which is why a low level supports the diagnosis of insulin deficiency. [3] [4]
Clinical Presentation
The classic presentation is a short history, often only a few weeks, of the triad of polyuria, polydipsia and weight loss in a previously well child. A younger child may present with new bed-wetting after being dry, or with recurrent nappy rash or candidal infection. Parents frequently describe a child who is drinking constantly, tired, and losing weight despite a normal or increased appetite. [10]
The pivotal branch at presentation is whether the child has uncomplicated hyperglycaemia or has progressed to ketoacidosis. Vomiting, abdominal pain, deep sighing Kussmaul breathing, a fruity smell on the breath, dehydration or any alteration in conscious level signal ketoacidosis and demand the emergency pathway. The child on this page is alert, tolerating fluids, and not acidotic, which is what allows a more measured, often ward-based or ambulatory start to treatment. [8] [10]
A distinct and growing group presents with no symptoms at all: the well child found to have islet autoantibodies through family screening or a research study. This child has stage 1 or stage 2 disease and needs education, a plan for surveillance, and clear advice on the symptoms that herald stage 3, so that clinical onset is caught early and before ketoacidosis. [2] [1]
Differential Diagnosis
The first differential is the type of diabetes, because the treatment and prognosis diverge. Type 2 diabetes is increasingly common in adolescents and is suggested by obesity, acanthosis nigricans, a strong family history and negative autoantibodies with a preserved C-peptide. Monogenic diabetes is suggested by an autosomal-dominant family history, a measurable C-peptide beyond the honeymoon, and negative antibodies, and neonatal diabetes must be assumed in any infant diagnosed under six months. [10] [4]
The second differential is the cause of the presenting symptoms before diabetes is confirmed. Polyuria and polydipsia can arise from a urinary tract infection, from diabetes insipidus, or from primary polydipsia, but a single raised glucose settles the question immediately, which is why the finger-prick test is the first and decisive step. Weight loss with fatigue has a broad differential that narrows the moment glucose is measured. [10] [8]
Points to type 1
- Short symptomatic history, weight loss
- Ketosis or ketoacidosis at onset
- Positive islet autoantibodies
- Low C-peptide relative to glucose
Points to type 2
- Adolescent with obesity
- Acanthosis nigricans, insulin resistance
- Negative autoantibodies
- Preserved or high C-peptide
Points to monogenic
- Autosomal-dominant family history
- Onset under six months (neonatal)
- Persistently measurable C-peptide
- Mild stable hyperglycaemia, antibody negative
The practical rule is that the diagnosis of diabetes is made on glucose alone, but the type is settled by the antibodies and C-peptide read together with the clinical picture. When the type is genuinely unclear, the child is treated as type 1 with insulin until the results and the course clarify things, because under-treating a true type 1 is far more dangerous than over-treating a type 2. [4] [10]
Clinical & Bedside Assessment
The bedside assessment has one urgent purpose first: to grade how unwell the child is and to detect ketoacidosis. Assess hydration, conscious level, respiratory pattern and abdominal signs, and quantify the illness with a capillary glucose and, critically, a capillary blood ketone level. A child who is alert, well perfused and tolerating oral fluids with only mildly raised ketones is suitable for the uncomplicated pathway. [8] [10]
Once safety is established, the history fills in the picture. Ask about the duration of symptoms, the pattern of thirst and urination, the amount of weight lost, and any preceding illness. Ask about family history of type 1 and type 2 diabetes and of autoimmune disease, and about features suggesting an alternative type, such as obesity or a striking dominant family history. Examine for acanthosis nigricans, plot the growth and weight, and note the pubertal stage, all of which shape the type and the insulin needs. [10] [6]
The bedside assessment also begins the therapeutic relationship. A calm, structured explanation to a frightened family that the diagnosis is serious but manageable, and that they will be taught everything they need, sets the tone for the education that follows and improves the family's ability to absorb the flood of new information. [6] [5]
Investigations
The diagnosis of diabetes rests on the glucose, and the thresholds are fixed. A random plasma glucose of 11.1 millimoles per litre or higher with classic symptoms confirms diabetes, as does a fasting plasma glucose of 7.0 millimoles per litre or higher. An HbA1c of 48 millimoles per mole (6.5 percent) or higher also meets the criterion, and it usefully shows that the hyperglycaemia has been present for weeks rather than hours. In a symptomatic child, a single high reading is enough to act on. [10] [7]
The investigations that establish the type are the islet autoantibodies and the C-peptide. A panel including antibodies to glutamic acid decarboxylase, IA-2, ZnT8 and insulin will be positive in most children with type 1 diabetes, and two or more positive antibodies make the autoimmune type near-certain. A C-peptide that is low relative to the concurrent glucose confirms insulin deficiency, while a preserved C-peptide should prompt consideration of type 2 or monogenic diabetes. These tests confirm the type but never delay treatment. [3] [4]
At diagnosis it is also standard to screen for the autoimmune comorbidities that accompany type 1 diabetes, chiefly thyroid function and coeliac disease, and to check baseline renal function and electrolytes. Capillary or blood ketones are measured at presentation and used to confirm that the child is not in ketoacidosis and to guide the sick-day teaching that begins straight away. [1] [8]
Management — Resuscitation
The word resuscitation here means the acute assessment and stabilisation at first presentation, and its dominant question is disposition: does this child need the emergency ketoacidosis pathway, or can treatment start on the uncomplicated route? A child who is acidotic, vomiting, dehydrated or drowsy is diverted immediately to the dedicated ketoacidosis protocol, which is not covered here. [8] [10]
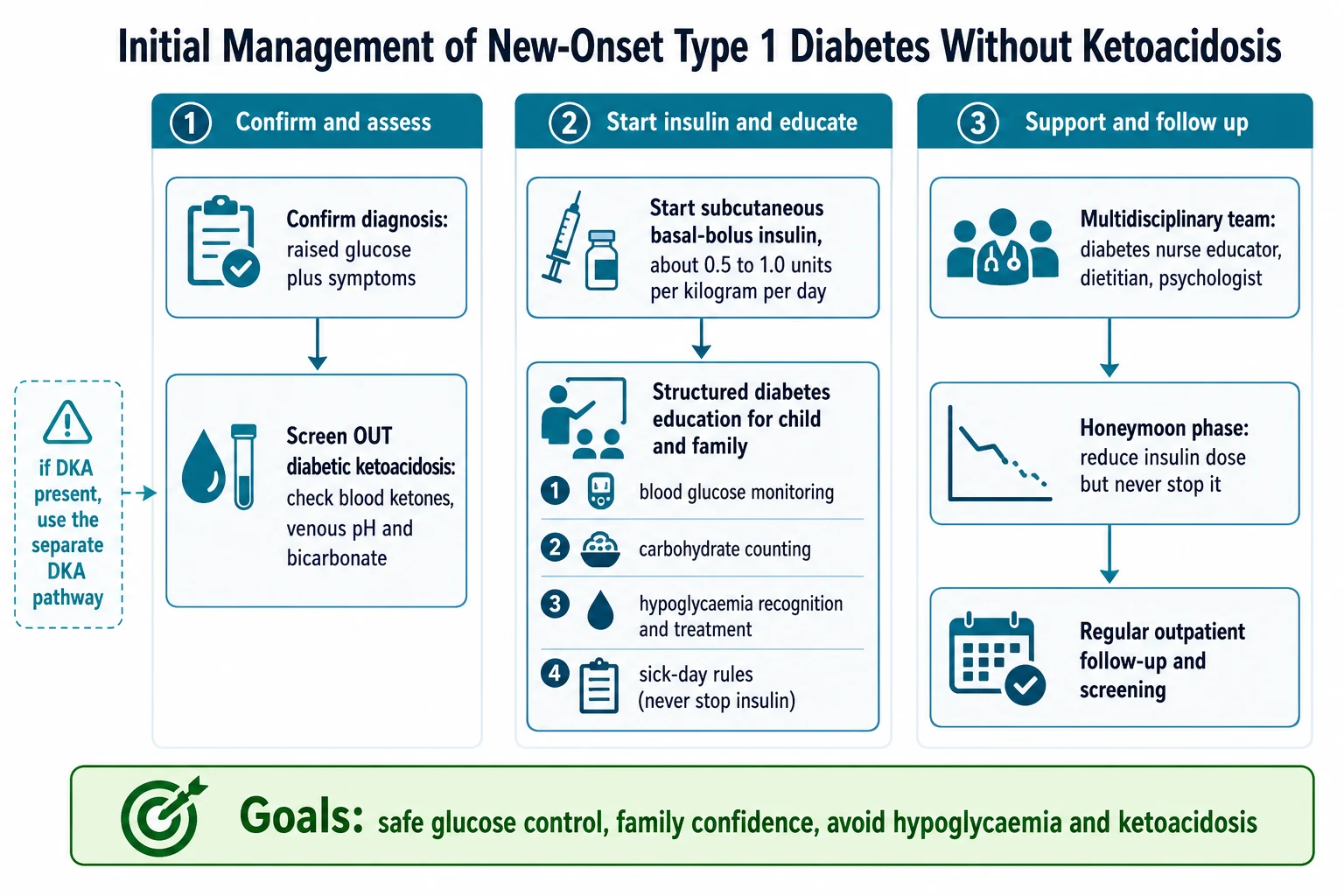
For the child who is alert and not acidotic, the acute management is gentle. Oral fluids maintain hydration, and the first dose of subcutaneous insulin can be given once the diagnosis is confirmed, without the intravenous fluids and insulin infusion that ketoacidosis demands. Many centres admit these children briefly for initial stabilisation and intensive education, while some experienced services with strong ambulatory support begin management at home; the choice depends on local resources and the family's circumstances. [6] [10]
Management — Definitive & Stepwise
The definitive treatment of type 1 diabetes is insulin, started as a subcutaneous basal-bolus regimen from the day of diagnosis. Calculate a total daily dose by weight, commonly in the range of 0.5 to 1.0 units per kilogram per day, higher in pubertal children and lower in the very young, and split it into roughly half basal and half bolus. The basal is given as a once or twice daily long-acting analogue and the bolus as a rapid analogue with each meal. [6]
Total daily insulin (new-onset, no ketoacidosis)
Dose
Start about 0.5 to 1.0 units per kilogram per day; lower in the very young, higher in puberty
The stepwise plan pairs the insulin with structured education, because a family that cannot manage the disease at home has not been safely treated. The education covers blood glucose monitoring, the principles of carbohydrate counting and dosing, the recognition and treatment of hypoglycaemia, and the sick-day rules built on the principle that insulin is never stopped during illness. This teaching is delivered by a diabetes nurse educator and dietitian and reinforced over the first weeks. [6] [8]
Rapid-acting insulin (lispro, aspart, glulisine)
Dose
Meal bolus by carbohydrate ratio plus correction factor; the bolus half of the total daily dose
Dose adjustment is expected and continuous in the first weeks. Glucose readings are used to tune each component: fasting values guide the overnight basal, pre-meal patterns guide the daytime basal, and post-meal excursions guide the bolus ratios. As the child stabilises and the honeymoon begins, the total dose often falls, and the family is taught to reduce rather than stop insulin. The child then transitions to the ongoing ambulatory care and technology described on the dedicated therapy leaf. [6] [5]
Specific Subtypes & Scenarios
The infant or toddler diagnosed with diabetes needs special thought. Under six months of age the diagnosis is neonatal (monogenic) diabetes rather than type 1, and genetic testing is essential because some forms respond to a sulfonylurea and do not need insulin at all. In older infants and toddlers with true type 1, tiny doses demand half-unit pens or diluted insulin, and the inability to report hypoglycaemia makes cautious targets and close monitoring essential. [4] [6]
The adolescent with new hyperglycaemia raises the type 1 versus type 2 question most sharply. Obesity, acanthosis nigricans and a strong family history point toward type 2, but many adolescents with type 1 are also overweight, so the autoantibodies and C-peptide are decisive. When the picture is mixed, the child is treated with insulin as type 1 until the results clarify the diagnosis. [10] [4]
The well child found antibody-positive on screening is a scenario that will grow as family and population screening spreads. This child has preclinical type 1 diabetes and is managed with education, metabolic surveillance to detect the move to stage 3, and a discussion of the emerging option to delay clinical onset. Recognising this stage prevents the child later presenting in ketoacidosis. [2] [9]
Complications & Pitfalls
The gravest early pitfall is missing the diagnosis. A child with the classic triad who is sent away without a glucose check can return days later in ketoacidosis, so any suggestive symptom warrants a same-day finger-prick. The second pitfall is treating a child who is actually in ketoacidosis as if they had uncomplicated diabetes, which is why ketones and acid-base status are checked before the subcutaneous pathway is chosen. [8] [10]
Hypoglycaemia is the commonest complication of starting insulin, and it frightens families badly in the first weeks. Careful initial dosing, clear teaching on recognising and treating lows with fast-acting carbohydrate, and honest discussion of the risk all reduce both the events and the fear. The related pitfall is over-correction of highs, which drives the glucose into hypoglycaemia and destabilises the early control. [6] [7]
The honeymoon phase is a classic trap. As surviving beta cells recover after the acute illness, insulin needs fall, sometimes dramatically, and a family may conclude that the diabetes has resolved. Insulin is never stopped, however small the dose, because the beta cells will fail again and stopping insulin is a direct route back to ketoacidosis. Framing the honeymoon as a temporary reprieve, not a cure, is essential family education. [5] [8]
Prognosis & Disposition
The immediate prognosis of uncomplicated new-onset type 1 diabetes is excellent when insulin is started and the family is well taught. The child who avoids ketoacidosis at onset has a smoother start and, on average, better early glycaemic outcomes than one who presents critically unwell, which is one more reason early recognition matters. [10] [7]
Disposition is lifelong specialist follow-up, not discharge. The child moves from the intensive first days into a structured ambulatory programme with a named multidisciplinary team, regular review, and the graduated introduction of technology, all covered on the ongoing therapy leaf. The long-term outlook depends on sustained glycaemic control, and aiming for target from diagnosis protects against the microvascular and macrovascular complications that track with cumulative hyperglycaemia. [7] [6]
The honeymoon shapes the early prognosis conversation. Families should understand that a period of low insulin need is expected and welcome, that it does not mean cure, and that it will pass. Setting that expectation at diagnosis prevents the disappointment and the dangerous insulin omission that can otherwise follow when the honeymoon ends. [5] [8]
Special Populations
Indigenous, migrant and socioeconomically disadvantaged children are more likely to present late and in ketoacidosis, reflecting gaps in access to care and in awareness of the early symptoms. Targeted community awareness, low-threshold glucose testing and culturally safe, family-centred education at diagnosis narrow that gap, because the disease is the same but the pathway to diagnosis is not. [11] [10]
The infant under six months is a special population of its own, because the diagnosis is neonatal monogenic diabetes rather than type 1. Genetic testing is essential, and identifying an activating potassium-channel mutation can allow a switch from insulin to an oral sulfonylurea, a treatment change that transforms daily life. Any diabetes diagnosed in the first six months should trigger this pathway. [4] [10]
The relative of a person with type 1 diabetes is a special population in the era of screening and prevention. First-degree relatives carry a raised risk, can be offered autoantibody screening, and if found to have stage 2 disease may be candidates for therapy that delays clinical onset. This reframes the family conversation at diagnosis from one purely about the affected child to one that may include the wider family. [1] [9]
Evidence, Guidelines & Regional Differences
The guideline base is anchored by the ISPAD 2024 consensus, whose chapters on screening, staging and beta-cell preservation, on insulin and adjunctive treatments, and on glycaemic targets set the international standard for diagnosis and initial management. The JDRF, Endocrine Society and American Diabetes Association staging statement defines the three-stage model that now frames classification. National bodies broadly align with these standards. [1] [2] [6]
DIAGNOSE
Polyuria, polydipsia and weight loss mean a same-day glucose check
Start subcutaneous basal-bolus once ketoacidosis is excluded; do not wait for antibodies
Ketones, venous pH and bicarbonate decide the pathway
Random over 11.1 or fasting over 7.0 millimoles per litre, or HbA1c over 48
Islet autoantibodies and C-peptide separate type 1 from type 2 and monogenic
Think neonatal monogenic diabetes and test genetically
Teach that insulin is never stopped, including in the honeymoon
Monitoring, carbohydrate counting, hypoglycaemia and follow-up with the team
The disease-modifying frontier is the main area of change. The teplizumab trial in relatives at risk showed that an anti-CD3 antibody can delay progression from stage 2 to clinical stage 3 disease, which has moved prevention from theory toward practice in screened relatives. Regional differences turn on how far screening programmes have spread, on access to genetic testing for monogenic diabetes, and on whether services admit new diagnoses or manage them in the ambulatory setting, all of which shape the initial pathway a child follows. [9] [1]
Exam Pearls
The one-sentence exam answer is that new-onset type 1 diabetes without ketoacidosis is diagnosed on glucose thresholds and confirmed by islet autoantibodies (C-peptide is supportive, not required), managed after excluding ketoacidosis by starting subcutaneous basal-bolus insulin at about 0.5 to 1.0 units per kilogram per day with structured family education, and safeguarded by the rule that insulin is never stopped, including through the honeymoon. [6] [5]
References
- [1]Haller MJ; Bell KJ; et al ISPAD Clinical Practice Consensus Guidelines 2024: Screening, Staging, and Strategies to Preserve Beta-Cell Function in Children and Adolescents with Type 1 Diabetes. Horm Res Paediatr, 2024.PMID 39662065
- [2]Insel RA; Dunne JL; et al Staging presymptomatic type 1 diabetes: a scientific statement of JDRF, the Endocrine Society, and the American Diabetes Association. Diabetes Care, 2015.PMID 26404926
- [3]Ziegler AG; Rewers M; et al Seroconversion to multiple islet autoantibodies and risk of progression to diabetes in children. JAMA, 2013.PMID 23780460
- [4]Leighton E; Sainsbury CA; Jones GC A Practical Review of C-Peptide Testing in Diabetes. Diabetes Ther, 2017.PMID 28484968
- [5]Couper JJ; Haller MJ; et al ISPAD Clinical Practice Consensus Guidelines 2018: Stages of type 1 diabetes in children and adolescents. Pediatr Diabetes, 2018.PMID 30051639
- [6]Cengiz E; Danne T; et al International Society for Pediatric and Adolescent Diabetes Clinical Practice Consensus Guidelines 2024: Insulin and Adjunctive Treatments in Children and Adolescents with Diabetes. Horm Res Paediatr, 2024.PMID 39884261
- [7]de Bock M; Agwu JC; et al International Society for Pediatric and Adolescent Diabetes Clinical Practice Consensus Guidelines 2024: Glycemic Targets. Horm Res Paediatr, 2024.PMID 39701064
- [8]Phelan H; Hanas R; et al Sick day management in children and adolescents with diabetes. Pediatr Diabetes, 2022.PMID 36093857
- [9]Herold KC; Bundy BN; et al An Anti-CD3 Antibody, Teplizumab, in Relatives at Risk for Type 1 Diabetes. N Engl J Med, 2019.PMID 31180194
- [10]DiMeglio LA; Evans-Molina C; Oram RA Type 1 diabetes. Lancet, 2018.PMID 29916386
- [11]Lawrence JM; Divers J; et al Trends in Prevalence of Type 1 and Type 2 Diabetes in Children and Adolescents in the US, 2001-2017. JAMA, 2021.PMID 34427600