Paeds · endocrinology-diabetes-and-growth
Type 1 diabetes: insulin therapy, technology and ambulatory care
Also known as Insulin therapy in type 1 diabetes · Basal-bolus regimen · Multiple daily injections · Insulin pump therapy · Continuous subcutaneous insulin infusion · Continuous glucose monitoring · Hybrid closed-loop · Automated insulin delivery · Diabetes ambulatory care · Sick-day management
Fellowship guide to ongoing insulin therapy, diabetes technology and ambulatory care in children and adolescents with type 1 diabetes: the insulin pharmacology that drives regimen choice, the basal-bolus and pump pathways, continuous glucose monitoring and hybrid closed-loop systems, sick-day and exercise rules, hypoglycaemia prevention, school care plans, HbA1c targets, and structured transition to adult care.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
This page covers the ongoing care of children and adolescents with established type 1 diabetes: the insulin pharmacology that decides the regimen, the basal-bolus and pump pathways, continuous glucose monitoring and hybrid closed-loop systems, and the ambulatory framework of sick-day rules, exercise planning, hypoglycaemia prevention, school care and transition. It assumes the diagnosis has been made and the first days managed on the dedicated diagnosis leaf, and it links to the diabetic ketoacidosis and hypoglycaemia leaves rather than repeating their protocols. [1] [12]
Overview & Definition
Type 1 diabetes is a lifelong insulin-deficiency disease. Once the honeymoon fades, the child depends entirely on exogenous insulin to survive, and the work of ongoing care is to deliver that insulin in a way that holds glucose near normal without trading control for hypoglycaemia or quality of life. [1] [12]
The goal of therapy has shifted over a generation. Where the target was once to avoid ketoacidosis and gross symptoms, the modern aim is an HbA1c below 7 percent, a time-in-range above 70 percent, and the lowest possible burden of severe hypoglycaemia — all while the child grows, learns, plays and moves toward independence. Technology has made that aim reachable for more children, but it has not removed the need for disciplined daily decisions. [4]
Classification
Insulin therapy in young people is best classified along two axes: the insulin-delivery method, and the glucose-monitoring method that augments it. The figure below sets out the delivery tiers from conventional injections through to hybrid closed-loop, paired with the monitoring that each tier relies on. [2] [3]
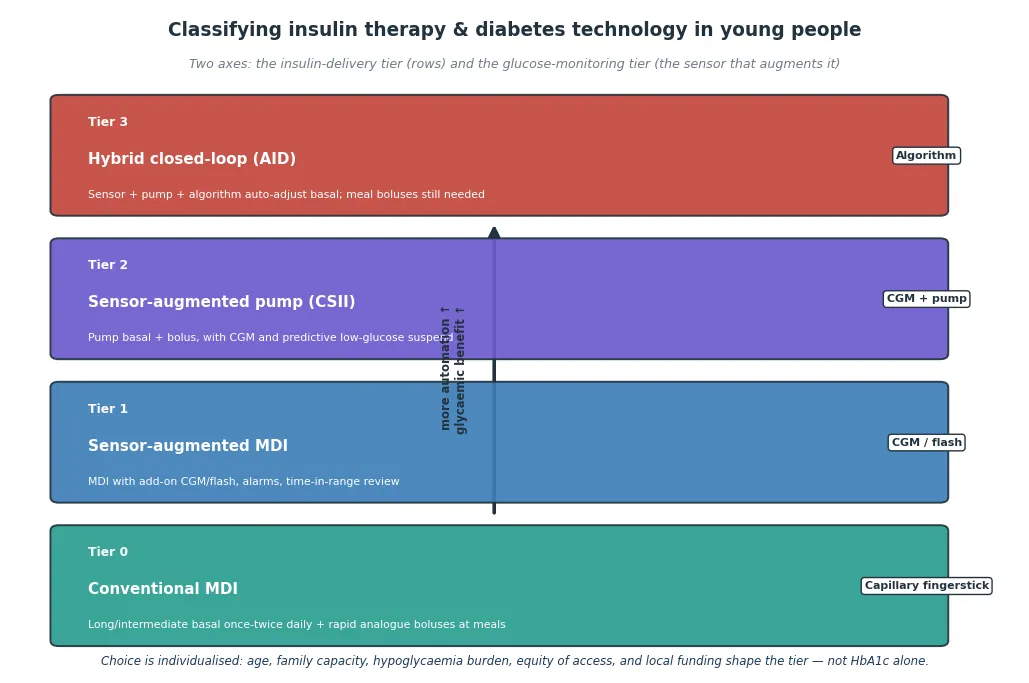
Conventional MDI
- Long-acting basal once or twice daily plus rapid boluses at meals
- Fingerstick glucose; lowest hardware barrier
- Flexible, cheap, widely available
- More daily injections; higher hypoglycaemia risk
Sensor-augmented MDI
- Same injections with continuous glucose monitoring added
- Alarms, trend arrows and time-in-range feedback
- Improves HbA1c and hypoglycaemia without a pump
- Requires sensor adherence and data interpretation
Sensor-augmented pump
- Programmable basal plus meal boluses from one device
- Predictive low-glucose suspend reduces nocturnal lows
- One cannula site every 2-3 days instead of daily injections
- Site failure can cause rapid ketoacidosis
Hybrid closed-loop
- Algorithm auto-adjusts basal from sensor glucose
- Greatest time-in-range and lowest nocturnal hypoglycaemia
- Meal and correction boluses still required
- Highest setup, cost and family-capacity demand
The two axes combine freely. A child can be on injections with a sensor, a pump with fingersticks, or any pairing that fits the family, because the delivery and monitoring choices are independent. The remainder of this page works through what each choice offers and how to run it safely. [1] [2]
Epidemiology & Risk Factors
Type 1 diabetes is the commonest chronic disease of childhood after asthma in many high-income countries, and its incidence continues to rise, which means the population needing skilled insulin therapy and ambulatory care keeps growing. Population surveillance in the United States confirms climbing prevalence and incidence of youth-onset type 1 diabetes across the last two decades. [10]
The burden of poor control is unevenly shared. Children in remote areas, Indigenous families, migrants, and those in socioeconomic disadvantage have higher HbA1c and more diabetes-related hospital admissions, reflecting gaps in access to specialist teams, to technology, and to the education and food environments that make intensive therapy feasible. Equity is therefore a clinical variable, not a footnote, in ambulatory diabetes care. [9] [10]
Registry data from more than 100,000 children show that pump use, continuous glucose monitoring and closed-loop systems have spread steadily over the last decade, and that their adoption tracks with better glycaemic outcomes at the population level. The same data show that a substantial minority of children still do not meet HbA1c targets, which is why technology is an opportunity rather than a complete answer. [9]
Pathophysiology
To choose an insulin regimen well, hold the shape of normal insulin secretion in mind. A healthy pancreas secreures a flat trickle of basal insulin through the day and night, holding glucose steady between meals and overnight, and adds sharp spikes at each meal to dispose of the absorbed carbohydrate. The whole point of every regimen and every technology is to recreate that two-part profile from outside the body. [1] [12]
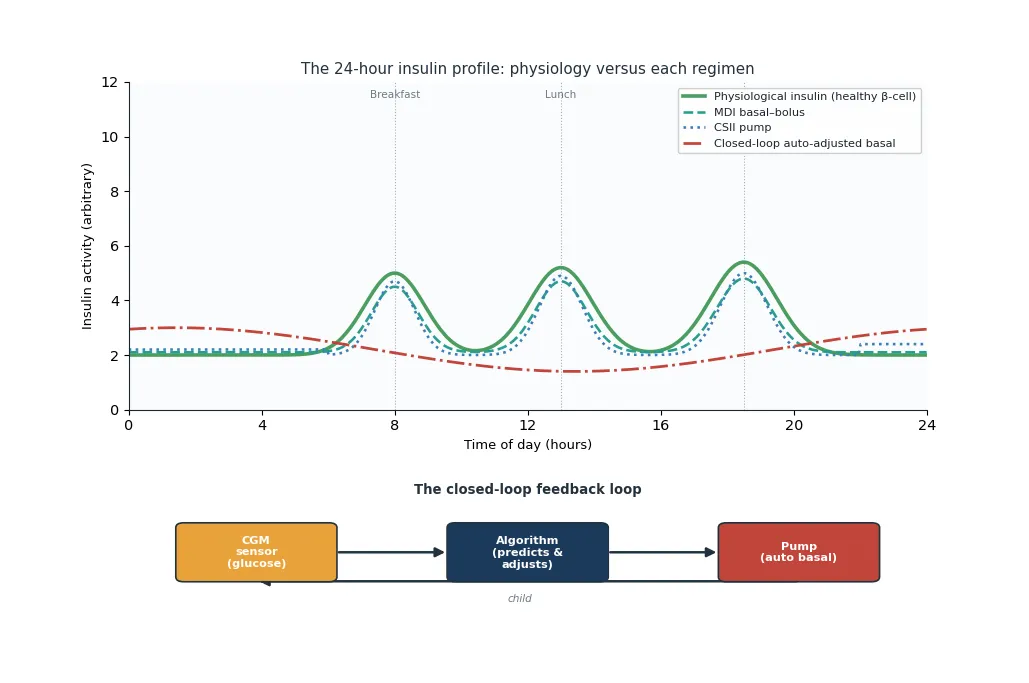
The insulin analogues determine how faithfully a regimen can copy the profile. Rapid-acting analogues such as lispro, aspart and glulisine peak within an hour and cover a meal bolus; faster aspart and ultra-rapid formulations act even more quickly to better match rapid carbohydrate absorption. Long-acting basal analogues such as glargine, detemir and degludec provide a flat depot for up to 24 hours or longer, while pumps deliver only a rapid analogue but in a micro-pulsed basal stream that mimics the flat depot without an injection. [1] [2]
The closed-loop feedback loop is the mechanistic advance that distinguishes automated insulin delivery from earlier technology. A continuous sensor reads interstitial glucose every few minutes, a control algorithm predicts where glucose is heading, and the pump raises, lowers or suspends basal insulin accordingly. The meal spikes still need a manual bolus, which is why these systems are called hybrid, but the background control they achieve overnight and between meals is what drives the time-in-range gains. [3] [6]
Clinical Presentation
The "presentation" of the child needing insulin therapy and ambulatory care is the everyday clinic encounter, not the acute first diagnosis. The recurring questions are whether the current regimen fits the child's life, whether the HbA1c and time-in-range meet target, and whether hypoglycaemia or distress has appeared. The stable child asks one set of questions; the child whose control has drifted asks another. [4] [9]
A few patterns recur and each points to a different problem. Persistently high morning glucose suggests insufficient overnight basal or the dawn phenomenon. Wide post-meal swings point to a mismatch between bolus timing and carbohydrate counting. Recurrent hypoglycaemia at the same time of day signals a basal or bolus excess. The child whose HbA1c has risen sharply without an obvious explanation often has a new stressor, a change in adherence, an emerging comorbidity such as thyroid dysfunction, or disordered eating. [1] [12]
The pump-treated child who becomes unwell presents a special pattern. Because a pump carries no long-acting depot, a blocked or dislodged cannula produces insulin deficiency within hours, and the child can develop ketones and ketoacidosis far faster than a child on injections. Any unwell pump-treated child must have ketones checked, and a site problem must be assumed and corrected before it progresses. [2] [8]
Differential Diagnosis
The differential in ongoing care is less about the type of diabetes, which is usually settled, and more about the cause of a control problem. A rising HbA1c can reflect incorrect dosing, adherence difficulty, injection into lipohypertrophic sites, an intercurrent illness, psychological distress, or a comorbidity. Working through these in turn beats simply raising the dose. [1] [12]
When hypoglycaemia dominates, the differential includes an insulin dose that is now too high, intensified exercise without carbohydrate cover, missed meals, alcohol in older adolescents, declining insulin needs at the end of puberty, over-correction of highs, and developing impaired awareness of hypoglycaemia. Recurrent lows warrant a structured review and often a regimen simplification before any tightening of targets. [4]
A small number of children with apparent type 1 diabetes who never seem to need much insulin, or who have a strong family history, may actually have monogenic diabetes that would respond to sulfonylureas rather than insulin. Reconsidering the diagnosis is reasonable when the clinical pattern does not fit, particularly if antibodies were never positive and C-peptide remains measurable. [5] [12]
High HbA1c causes
- Under-dosing or missed injections
- Injection into lipohypertrophy
- Adherence difficulty or insulin omission
- New comorbidity: thyroid, coeliac, stress
Recurrent hypo causes
- Basal or bolus dose now too high
- Unplanned or intense exercise
- Declining needs after puberty or honeymoon
- Emerging impaired hypoglycaemia awareness
Reconsider the diagnosis
- Antibody-negative from the outset
- Measurable C-peptide beyond honeymoon
- Autosomal-dominant family history
- Stable mild hyperglycaemia on tiny doses
Clinical & Bedside Assessment
The clinic review is the core of ambulatory diabetes care, and its quality determines outcomes more than any single tool. Plot growth and weight at every visit, because growth and puberty shift insulin needs week to week and a child whose dose has not kept pace with a growth spurt will drift hyperglycaemic. Review the injection or infusion sites for lipohypertrophy, which silently absorbs insulin unpredictably and is a leading correctable cause of erratic control. [1]
Ask specifically about hypoglycaemia using a structured question, because families under-report it unless prompted. Document the number of mild episodes, any severe episode needing assistance, and whether the child has lost the early warning symptoms, which signals impaired awareness and predicts the next severe event. Screen for diabetes distress and, in adolescents, for disordered eating and insulin omission, which are common, dangerous, and easily missed without direct questioning. [4] [12]
Review the glucose data as the family experiences it. With fingersticks, look at the logbook and the patterns; with continuous monitoring, read the ambulatory glucose profile for time-in-range, time-below-range and the shape of the daily curve. The ambulatory profile is the most informative single document in modern diabetes care, and the ability to read it is now a core skill for any clinician looking after these children. [3]
Investigations
The single most important investigation in routine diabetes care is the HbA1c, measured every three months. It summarises mean glucose over the preceding eight to twelve weeks and is the headline outcome that guidelines track against target. The ISPAD 2024 glycemic targets recommend an HbA1c below 7 percent for most children, individualised to the child's hypoglycaemia risk and circumstances. [4]
Where continuous monitoring is used, the ambulatory glucose profile adds information that HbA1c cannot give. Time-in-range, the percentage of readings between 3.9 and 10.0 millimoles per litre, is the modern target, with a goal above 70 percent and time-below-range kept below 4 percent and severe lows eliminated. Mean glucose, glucose management indicator and the coefficient of variation quantify stability and the burden of swings. [3] [4]
Annual complication and comorbidity screening begins in later childhood and adolescence. Retinal photography or examination, urinary albumin-to-creatinine ratio, blood pressure, lipid profile, thyroid function and coeliac screening are standard, because retinopathy, nephropathy, thyroiditis and coeliac disease are the silent companions of long-standing type 1 diabetes and each changes management when found. [1] [12]
Management — Resuscitation
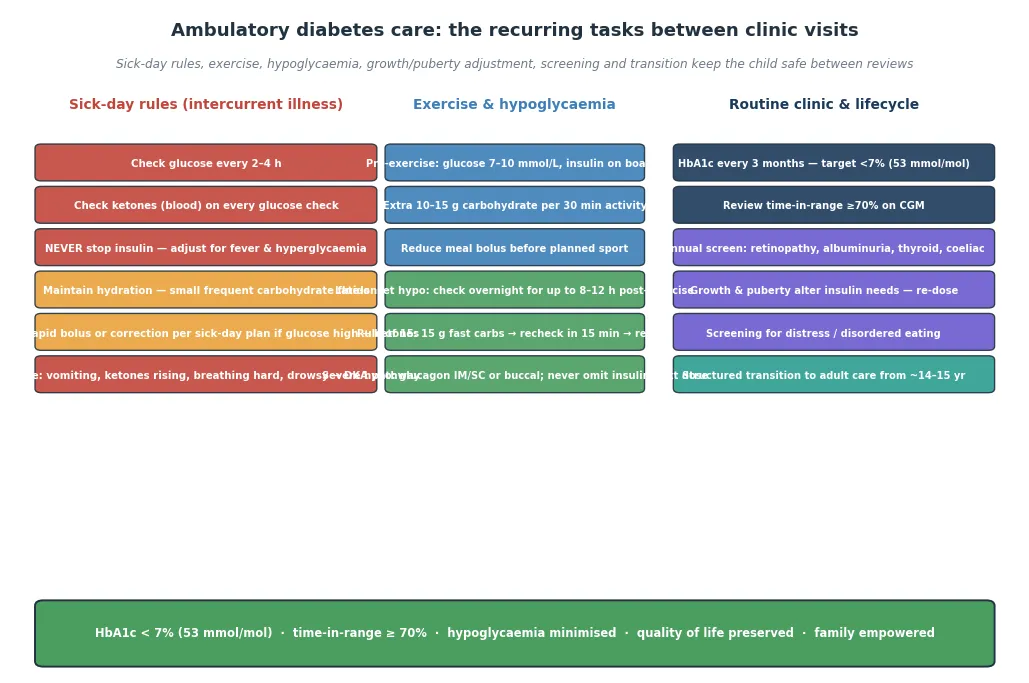
The "resuscitation" question in ambulatory diabetes care is the sick child at home: when does an intercurrent illness threaten ketoacidosis, and what must the family do in the first hours? The principle that governs the answer is that insulin is never stopped during illness. Fever, infection and the stress response raise insulin needs, so the dose is usually increased, and withholding insulin is the single most common precipitant of sick-day ketoacidosis. [8]
The sick-day routine the family follows has fixed steps. Check glucose every two to four hours, check blood ketones at every glucose check, keep up hydration with small frequent carbohydrate-containing fluids, give extra rapid-acting insulin for hyperglycaemia with ketones according to the sick-day plan, and never omit the basal insulin. A child on a pump who develops ketones should switch to a pen correction and change the cannula, because a site problem is the likely cause. [2] [8]
Escalation criteria send the family to hospital before ketoacidosis develops. Vomiting that prevents fluid retention, ketones that rise despite extra insulin, deep or rapid breathing, drowsiness, or persistent hyperglycaemia above 15 to 20 millimoles per litre all warrant urgent review. The goal of good sick-day teaching is that the family calls early, in the ketotic-but-not-acidotic window, when a little fluid and a correction can turn the tide. [8] [12]
Management — Definitive & Stepwise
The definitive pathway begins at diagnosis and is refined at every visit. Calculate the total daily insulin dose by weight, split it into roughly half basal and half bolus, and deliver the basal as a once or twice daily long-acting analogue and the bolus as a rapid analogue with each meal, dosed by carbohydrate counting and a correction factor. This basal-bolus or multiple daily injection regimen is the foundation because it reproduces physiology and teaches flexible eating from the start. [1]
Typical total daily doses run 0.7 to 0.9 units per kilogram per day before puberty and rise to 1.0 to 1.5 units per kilogram per day during the pubertal growth spurt, driven by growth-hormone-mediated insulin resistance. In the honeymoon, needs fall and may sit below 0.5 units per kilogram per day, but insulin is never stopped. Adjustments are made from the pattern of glucose readings: fasting targets guide the overnight basal, pre-meal to pre-meal patterns guide the day basal, and post-meal excursions guide the bolus ratios. [1] [4]
The insulin pump delivers the same rapid analogue as a programmable micro-pulsed basal with meal boluses, replacing four or more daily injections with a cannula site changed every two to three days. Pumps suit children with unpredictable routines, frequent hypoglycaemia, a need for very small basal increments, or a desire to avoid injections, but they demand a family able to manage the device, count carbohydrates and respond to alarms and site failures. The basal rate, carbohydrate ratios, correction factors and active insulin time are the pump parameters that are tuned at each visit. [2]
Rapid-acting insulin (lispro, aspart, glulisine)
Dose
Meal bolus: carbohydrate ratio + correction factor; pump basal typically 0.5–1.5 U/h
Long-acting basal insulin (glargine, degludec, detemir)
Dose
~50% of total daily dose; glargine/degludec once daily, detemir often twice
Hybrid closed-loop systems combine the pump with a continuous sensor and a control algorithm that automatically adjusts the basal rate every few minutes. Trials in school-age children and adolescents, and in very young children aged two to six, show meaningful gains in time-in-range and reductions in nocturnal hypoglycaemia compared with sensor-augmented pumps. The meal bolus remains manual, so carbohydrate counting and pre-meal dosing stay essential, but the burden of background control falls to the algorithm. [6] [7]
The choice among regimens is individualised and revisited over time. Age, daily routine, hypoglycaemia burden, family capacity, access and funding all weigh on the decision, and the best regimen is the one the family can and will use consistently. Registry evidence shows that the gap between technologies is smaller than the gap between using any tool well and using it badly, which keeps the skilled team central to every choice. [9]
Specific Subtypes & Scenarios
The very young child carries special management considerations. Tiny total daily doses demand half-unit pens or pumps that deliver in fractions of a unit, unpredictability of appetite and activity makes hypoglycaemia a constant risk, and the child cannot report symptoms. Continuous glucose monitoring and closed-loop systems have shown particular benefit in the two-to-six age group, reducing both hyperglycaemia and the feared nocturnal lows. [6] [7]
The adolescent faces the opposite problem: rising insulin resistance from puberty, competing priorities, burnout after years of disease, and the peak risk of disordered eating and insulin omission for weight control. Intensive support, psychology input, and technology that reduces daily burden all help, but the relationship with the team and a non-judgemental stance toward adherence are what keep an adolescent engaged through the riskiest years. [1] [12]
Exercise is a scenario that crosses every age group and needs a plan, not a reaction. Activity lowers glucose both during and for many hours afterward, so the family plans carbohydrate intake, adjusts the pre-exercise bolus, sets a temporary lower basal on a pump, and checks overnight glucose for late hypoglycaemia. A structured exercise plan lets the child play sport safely instead of being restricted by fear of lows. [8] [12]
The school scenario depends on a documented school care plan. The plan tells teachers when the child checks glucose, how meals and boluses are handled, how hypoglycaemia is recognised and treated, and who to call. A child who cannot manage diabetes safely at school cannot be said to have a complete care plan, and the general paediatrician often coordinates this across the school and the family. [1]
Complications & Pitfalls
List the day-to-day complications of intensive therapy. Hypoglycaemia is the commonest and most feared, ranging from mild self-treated episodes to severe events causing seizure or unconsciousness; recurrent hypoglycaemia erodes the early-warning symptoms and produces impaired awareness, which then predicts further severe events. Lipohypertrophy from poor site rotation causes erratic absorption and is correctable with technique teaching. Weight gain accompanies intensive insulin and is a particular concern in adolescence. [1] [4]
Identify the technology pitfalls. A blocked pump cannula causes rapid ketoacidosis because there is no depot. Sensor inaccuracy in the first hours of wear, during rapid glucose change, or with paracetamol interference can mislead. Alert fatigue from excessive alarms leads families to silence the device and miss the warning they needed. Data overwhelm a family that has not been taught to act on it, producing anxiety without improved control. [2] [3]
Identify the human pitfalls. Stopping insulin during illness precipitates ketoacidosis. Omitting boluses for weight control produces chronic hyperglycaemia and early complications. Failing to adjust the dose to a growth spurt allows silent deterioration. Losing the child to follow-up at the transition to adult care interrupts the care that prevents long-term complications. Each is preventable with structured education, active screening and a plan that the family owns. [8] [12]
The long-term complications of inadequately controlled diabetes appear later but are seeded early. Retinopathy, nephropathy, neuropathy and cardiovascular disease all track with cumulative hyperglycaemia from childhood, which is the rationale for aiming for target from diagnosis and for the annual screening that detects the earliest, treatable changes. Good control in childhood buys decades of healthier life. [9] [12]
Prognosis & Disposition
With disciplined insulin therapy, appropriate technology and a skilled team, a child with type 1 diabetes can expect a near-normal lifespan, normal intellectual and physical development, and full participation in education, work and family life. The prognosis has improved generation on generation with intensive therapy, and closed-loop technology now offers the best glycaemic control yet achieved in young children. [6] [12]
The modifiable prognostic factors sit in the ambulatory space. Meeting HbA1c target from early in the disease, minimising severe hypoglycaemia, attending regular clinic review, completing annual screening, and sustaining engagement through adolescence and transition are the behaviours that protect long-term outcomes. Disposition is therefore lifelong specialist follow-up, not a one-off discharge, with a named team and clear safety-nets. [1] [9]
Describe the structured transition to adult care. Beginning in the early to mid-teens, the adolescent is prepared for the move to an adult endocrinology service through joint clinics, skills checklists, and a formal handover that carries the medical summary, the regimen and the psychosocial context. Poorly managed transition is a well-recognised cause of lost follow-up, deteriorating control and early complications, so the handover itself is treated as a clinical intervention. [1] [12]
Special Populations
Describe the very young child on technology. The two-to-six age group has the most unpredictable eating and activity, the highest hypoglycaemia risk, and the least ability to communicate symptoms, and trials of closed-loop in this group show clear gains in time-in-range and overnight safety. Tiny doses need precise delivery, and the family carries the entire management burden, which makes technology that reduces decision load especially valuable. [6] [7]
Describe the adolescent at transition. The legacy of a childhood of chronic disease, the surge in insulin resistance, the peak in disordered eating and insulin omission, and the danger of being lost at the adult handover combine to make the teenage years the highest-risk period after diagnosis. Psychology input, technology that reduces daily burden, a non-judgemental stance toward adherence, and a planned transition are the protective factors. [1] [12]
Describe Indigenous, migrant and remote populations. Higher HbA1c and more diabetes-related admissions reflect gaps in access to specialist teams, to technology funding, and to the food and education environments that intensive therapy assumes. Telehealth, local diabetes educator support, culturally safe and family-centred teaching, and deliberate funding of technology access narrow the gap, because the disease is the same but the access is not. [9] [10]
Describe the child with a comorbidity. Coeliac disease, autoimmune thyroiditis and asthma all co-occur and each changes management: coeliac disease demands a gluten-free diet that alters carbohydrate sources, thyroid dysfunction destabilises glucose, and asthma medications and exercise patterns shift insulin needs. A child whose control has drifted should be re-screened for a new comorbidity before the dose alone is changed. [1] [12]
Evidence, Guidelines & Regional Differences
Summarise the guideline base. The ISPAD 2024 consensus guidelines on insulin and adjunctive treatments, on insulin-delivery and glucose-monitoring technologies, on glycemic targets, and on screening and beta-cell preservation set the international standard for ambulatory paediatric diabetes care. National bodies such as the American Diabetes Association, the Australasian Paediatric Endocrine Group and the National Institute for Health and Care Excellence broadly align with ISPAD. [1] [2] [4]
Summarise the technology evidence. The landmark JDRF continuous glucose monitoring trial established that sensor use with intensive therapy improves HbA1c in adults and older children who use it regularly. The trial of hybrid closed-loop control in young children demonstrated major time-in-range gains in the two-to-six age group, and the LENNY trial extended automated insulin delivery evidence to the very youngest. Registry data from over 100,000 children show that technology adoption tracks with population-level glycaemic improvement. [6] [9] [11]
INSULIN
Never stop insulin in illness; adjust the dose up for fever and hyperglycaemia
Check glucose every 2–4 hours on a sick day and ketones at every check
Rotate injection and pump sites to prevent lipohypertrophy and erratic absorption
A blocked pump cannula causes ketoacidosis in hours — check the site in any unwell pump user
Loss of hypoglycaemia warning predicts the next severe event — restore it before tightening
Match the regimen and technology tier to the child, the family capacity and access
A planned handover to adult care in the mid-teens prevents lost follow-up and early complications
Discuss current controversies. Funding and reimbursement of continuous monitoring and closed-loop systems vary widely, creating an equity gap in which the children most likely to benefit are often the least able to access the technology. The degree to which very young children should be started on closed-loop from diagnosis remains under active study. The role of adjunctive therapies such as SGLT inhibitors and glucagon analogues in youth is still being defined. Regional differences turn on technology funding, the organisation of transition care, and access to multidisciplinary teams and telehealth in remote areas. [5] [9]
Exam Pearls
The one-sentence exam answer is that ongoing type 1 diabetes care delivers lifelong insulin by the regimen the family can use best, augmented by continuous glucose monitoring and closed-loop technology where available, held to an HbA1c below 7 percent and a time-in-range above 70 percent, and protected between visits by sick-day rules, exercise and hypoglycaemia plans, school care, annual screening and a structured transition to adult care. [1] [4]
References
- [1]Cengiz E; Danne T; et al ISPAD Clinical Practice Consensus Guidelines 2024: Insulin and adjunctive treatments in children and adolescents with diabetes. Horm Res Paediatr, 2024.PMID 39884261
- [2]Biester T; Berget C; et al ISPAD Clinical Practice Consensus Guidelines 2024: Diabetes technologies — insulin delivery. Horm Res Paediatr, 2024.PMID 39657603
- [3]Tauschmann M; Cardona-Hernandez R; et al ISPAD Clinical Practice Consensus Guidelines 2024: Diabetes technologies — glucose monitoring. Horm Res Paediatr, 2024.PMID 39884260
- [4]de Bock M; Agwu JC; et al ISPAD Clinical Practice Consensus Guidelines 2024: Glycemic targets. Horm Res Paediatr, 2024.PMID 39701064
- [5]Haller MJ; Bell KJ; et al ISPAD Clinical Practice Consensus Guidelines 2024: Screening, staging, and strategies to preserve beta-cell function in children and adolescents with type 1 diabetes. Horm Res Paediatr, 2024.PMID 39662065
- [6]Wadwa RP; Reed ZW; et al Trial of hybrid closed-loop control in young children with type 1 diabetes. N Engl J Med, 2023.PMID 36920756
- [7]Battelino T; Kuusela S; et al Efficacy and safety of automated insulin delivery in children aged 2-6 years (LENNY): an open-label, multicentre, randomised, crossover trial. Lancet Diabetes Endocrinol, 2025.PMID 40544853
- [8]Phelan H; Hanas R; et al Sick day management in children and adolescents with diabetes. Pediatr Diabetes, 2022.PMID 36093857
- [9]Zimmermann AT; Lanzinger S; et al Treatment regimens and glycaemic outcomes in more than 100 000 children with type 1 diabetes (2013-22): a longitudinal analysis of data from paediatric diabetes registries. Lancet Diabetes Endocrinol, 2025.PMID 39622257
- [10]Lawrence JM; Divers J; et al Trends in prevalence of type 1 and type 2 diabetes in children and adolescents in the US, 2001-2017. JAMA, 2021.PMID 34427600
- [11]Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study Group; Tamborlane WV; et al Continuous glucose monitoring and intensive treatment of type 1 diabetes. N Engl J Med, 2008.PMID 18779236
- [12]DiMeglio LA; Evans-Molina C; Oram RA Type 1 diabetes. Lancet, 2018.PMID 29916386