Paeds · endocrinology-diabetes-and-growth
Type 2 diabetes and metabolic syndrome in youth
Also known as Type 2 diabetes mellitus · Type 2 diabetes · T2DM · Youth-onset type 2 diabetes · Metabolic syndrome in adolescents · Insulin resistance syndrome · Adolescent-onset diabetes · Non-insulin-dependent diabetes mellitus
Fellowship guide to type 2 diabetes and metabolic syndrome in children and adolescents: the insulin-resistance and beta-cell-failure pathophysiology, the acanthosis and metabolic cluster at the bedside, the diagnostic criteria with antibody and C-peptide confirmation, the exclusion of type 1 and monogenic diabetes, the stepwise ladder of lifestyle, metformin, insulin, GLP-1 receptor agonists and SGLT2 inhibitors, and the aggressive comorbidity and complication care that defines the disease as faster and more dangerous than its adult counterpart.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
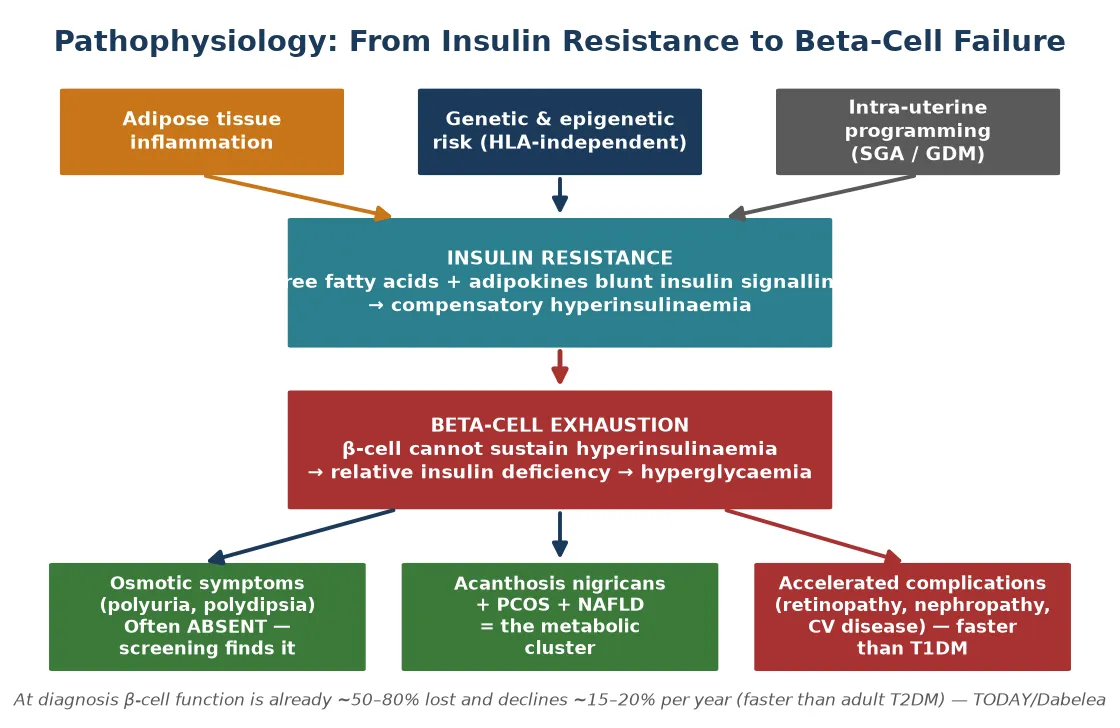
The single idea that organises everything in type 2 diabetes and metabolic syndrome in youth is insulin resistance with progressive beta-cell decline, layered on obesity and the metabolic cluster. Resist insulin and the beta cell drives out ever more of it, producing the acanthosis, ovarian hyperandrogenism, fatty liver, dyslipidaemia and hypertension that travel together. Exhaust the beta cell and glucose rises, because the compensatory output finally falls short. That is why one disease shows up as a whole cluster of metabolic risk, why acanthosis is the bedside clue, and why the complications arrive faster than in type 1 — the disease combines hyperglycaemia with every other cardiovascular risk factor at once. [1] [5]
This page covers the recognition, diagnosis and management of type 2 diabetes and metabolic syndrome in children and adolescents: the pathophysiology of insulin resistance and beta-cell failure, the acanthosis and metabolic cluster at the bedside, the diagnostic criteria with antibody and C-peptide confirmation, the exclusion of type 1 and monogenic diabetes, the stepwise ladder of lifestyle, metformin, insulin, GLP-1 receptor agonists and SGLT2 inhibitors, and the aggressive comorbidity and complication care that defines the disease as faster and more dangerous than its adult counterpart. It links to the dedicated leaves for type 1 diabetes, diabetic ketoacidosis, and monogenic diabetes rather than repeating their full pathways. [1]
Overview & Definition
Type 2 diabetes in youth is defined by insulin resistance combined with progressive beta-cell failure, set against obesity and genetic or ethnic susceptibility. The defining feature is not the absence of insulin but its loss of effect, followed by the exhaustion of the beta cells that try to compensate. Residual insulin usually prevents ketogenesis, which is why presentation is often insidious and picked up on screening rather than at a crisis. [1]
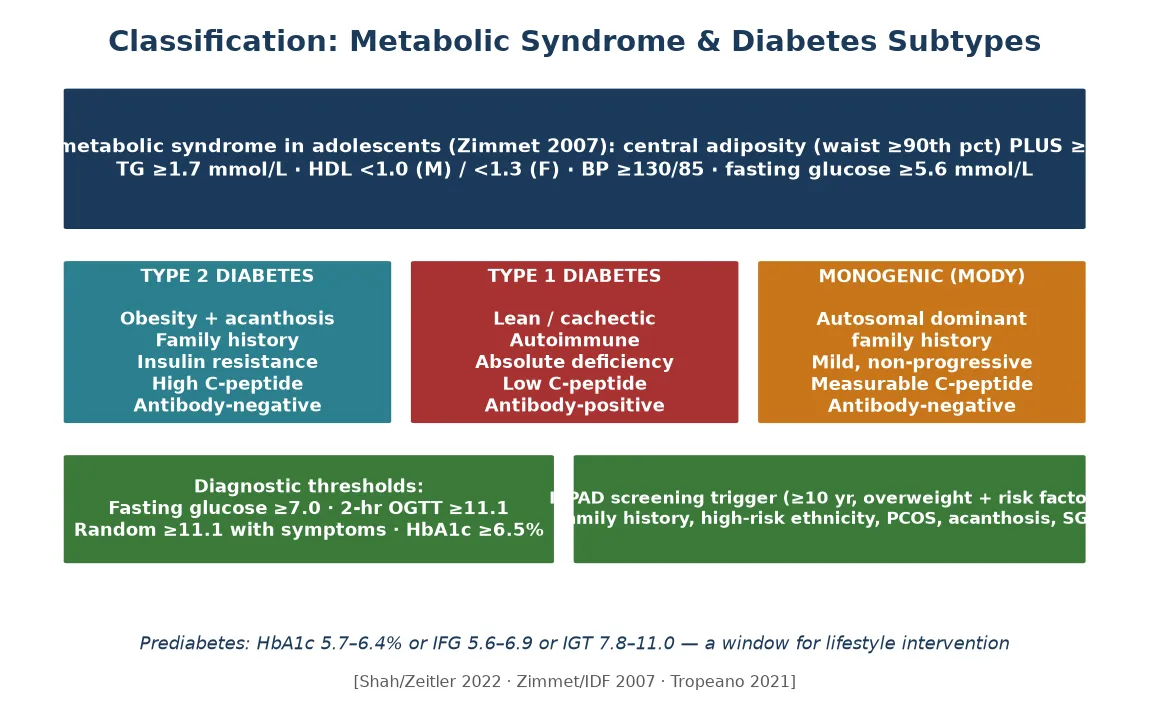
The metabolic syndrome is the constellation that type 2 diabetes belongs to. Central adiposity sits at its core, and it gathers dyslipidaemia, hypertension and raised fasting glucose around it, with insulin resistance as the shared mechanism. The IDF consensus defines it in adolescents as central adiposity with a waist circumference at or above the 90th percentile plus two or more of triglycerides at least 1.7 millimoles per litre, low HDL, blood pressure at least 130 over 85, and fasting glucose at least 5.6 millimoles per litre. [6] [5]
What sets youth-onset type 2 apart is its aggression. Beta-cell function is already roughly 50 to 80 percent reduced at diagnosis, and it declines about 15 to 20 percent per year — far faster than in adults. Half of adolescents fail metformin monotherapy within a few years, and complications appear early. The disease is therefore not a mild or stable version of adult diabetes but a faster, more dangerous variant that demands intensive treatment from the outset. [10] [11]
Classification
The diabetes of youth separates by aetiology, and the discriminator matters because it changes treatment. Type 2 sits at one end, defined by obesity, acanthosis, a family history, measurable or high C-peptide, and negative islet autoantibodies. Type 1 sits at the other, defined by autoimmune absolute deficiency, a lean phenotype, low C-peptide, and positive antibodies. Monogenic diabetes (MODY) sits between, defined by a single-gene beta-cell defect inherited in an autosomal-dominant pattern across generations, with negative antibodies, a mild stable course, and a measurable C-peptide that persists long after the honeymoon. [1]
The metabolic syndrome carries its own classification. The IDF consensus requires central adiposity as the entry criterion and then counts additional abnormalities — high triglycerides, low HDL, hypertension, raised fasting glucose. Two or more abnormalities alongside central obesity make the diagnosis. The definition is contested across the IDF, Cook and NHLBI criteria, which is why some paediatric endocrinologists treat the metabolic syndrome as a useful flag for cardiovascular risk rather than a rigid disease label. [6] [5]
Prediabetes is the window between normal and diabetic glucose handling, defined by an HbA1c of 5.7 to 6.4 percent, an impaired fasting glucose of 5.6 to 6.9 millimoles per litre, or an impaired glucose tolerance on a two-hour oral glucose tolerance test of 7.8 to 11.0. Recognising prediabetes matters because intensive lifestyle intervention in this window can delay or prevent progression to diabetes, and because it identifies the family that needs the same intervention. [1]
Epidemiology & Risk Factors
Type 2 diabetes in youth is rising faster than almost any other chronic disease of childhood. Prevalence and incidence climb in parallel with obesity, and the SEARCH study has documented a steady rise across the first two decades of this century. The trajectory is steepest in the populations most affected by obesity and in whom screening is therefore most urgent. [2] [3]
The risk factors cluster. Obesity, especially central adiposity, is the dominant driver. A family history of type 2 diabetes reflects the shared genetics and environment. High-risk ethnicity — Indigenous Australian, Maori and Pacific, Hispanic, South or East Asian, and African heritage — multiplies the risk. Female sex, pubertal age, a small-for-gestational-age birth, maternal gestational diabetes, polycystic ovary syndrome, and acanthosis nigricans all add to the probability. [1] [4]
In Australia and New Zealand, type 2 diabetes disproportionately affects Indigenous youth, among whom it is now one of the commonest chronic diseases of adolescence. Screening is recommended from age ten in overweight children with one or more risk factors, and the cultural safety, family involvement and remote-access support that frame that screening are central to effective care. [1] [4]
Pathophysiology
Visceral adiposity sets the whole disease in motion. Adipose tissue releases free fatty acids and dysregulated adipokines that blunt insulin signalling in the liver and muscle, producing insulin resistance. The beta cell responds by driving out ever more insulin, and the resulting hyperinsulinaemia holds glucose in check for a time while it leaves its signature on the skin, the ovaries, the liver and the blood vessels. [1]
The beta cell cannot sustain the compensatory output indefinitely. It exhausts, and as it fails the insulin reserve falls below the threshold needed to hold glucose. Beta-cell function is already roughly 50 to 80 percent reduced at diagnosis, and it declines about 15 to 20 percent per year thereafter — far faster than in adult disease. That rapid decline is the biological reason why control deteriorates quickly and why escalation is anticipated from the outset. [10]
The insulin resistance and hyperinsulinaemia produce the metabolic cluster through shared tissue-level signalling defects. Acanthosis nigricans marks the skin, ovarian hyperandrogenism drives polycystic ovary syndrome, fat accumulates in the liver as non-alcoholic fatty liver disease, the lipid profile tilts toward high triglycerides and low HDL, and the blood pressure climbs. These are not separate diseases but different faces of the same resistance. [7] [5]
Intra-uterine programming adds a generational dimension. A small-for-gestational-age birth and maternal gestational diabetes both programme later insulin resistance, and a high-risk family layers genetics on top of environment. The result is a disease that tends to travel through families and across generations, which is why the family is both the screening trigger and the unit of treatment. [4]
Clinical Presentation
Most youth with type 2 diabetes are detected through screening of an overweight child with risk factors rather than through the dramatic osmotic symptoms of type 1. The disease declares itself slowly because residual insulin keeps ketogenesis at bay, and the family and clinician may not recognise the metabolic drift until a routine glucose or HbA1c is checked. This is why the screening trigger in an overweight adolescent matters so much. [1]
When osmotic symptoms do appear they are usually less pronounced than in type 1. Polyuria, polydipsia and a change in weight can occur, but they are often subtle and attributed to adolescence. A minority present with a ketoacidotic or hyperosmolar crisis, and a small but important group show a ketosis-prone type 2 phenotype in which obesity and antibodies coexist — a source of diagnostic confusion at the bedside. [1]
The metabolic cluster provides the physical signs. Acanthosis nigricans appears at the neck, axillae, groins and knuckles as a dark velvety thickening. Central obesity dominates the body habitus, with striae across the abdomen. Hirsutism, acne and oligomenorrhoea mark the polycystic ovary syndrome. Hepatomegaly suggests fatty liver disease. Each sign is a clue to the same insulin resistance. [7]
Differential Diagnosis
The first decision at the bedside is whether the hyperglycaemia is type 2, type 1, or monogenic. Obesity, acanthosis and a strong family history point to type 2, supported by a normal or high C-peptide and negative antibodies. A lean phenotype with an acute presentation, low C-peptide and positive antibodies points to type 1. An autosomal-dominant family history across generations with a mild stable course, negative antibodies and a measurable C-peptide beyond the honeymoon points to monogenic diabetes. [1]
The distinction is not academic. Suspecting monogenic diabetes changes treatment, because many MODY subtypes respond to a sulfonylurea and can be released from insulin. Suspecting type 2 changes the emphasis from insulin alone to metformin, lifestyle and the management of the metabolic cluster. Getting the type right at the outset protects the adolescent from years of the wrong regimen. [1]
The metabolic syndrome itself must be separated from other causes of obesity and acanthosis. Cushing syndrome produces central obesity, striae and hypertension but adds a cushingoid facies, growth failure and a high cortisol. Hypothyroidism adds weight gain but also short stature, bradycardia and a low thyroxine. Corticosteroid therapy produces a reversible insulin resistance. Growth, blood pressure, fat distribution and biochemistry resolve these. [5]
The two-hour oral glucose tolerance test resolves indeterminate HbA1c or fasting glucose values. Polycystic ovary syndrome screening, a liver assessment, and a lipid and blood pressure profile belong in the same work-up, because the metabolic cluster is the context in which the diabetes sits and the target of much of the treatment. [1] [6]
Clinical & Bedside Assessment
The assessment begins with measurement and plotting. Height, weight, body mass index and waist circumference are plotted on age- and sex-specific charts, and pubertal stage is documented, because type 2 diabetes is predominantly a disorder of puberty. The pattern of growth and the timing of puberty frame the risk and the targets. [1]
The skin examination is the single most rewarding manoeuvre. Acanthosis nigricans at the neck, axillae and knuckles is the bedside marker of insulin resistance, and its presence in an obese adolescent should trigger the full assessment. The dark velvety thickening is easy to miss in good light and easy to dismiss as poor hygiene, and neither omission is acceptable. [7]
Blood pressure is measured against age-, sex- and height-specific percentiles. Hypertension is a diagnostic criterion of the metabolic syndrome and a target of treatment, so a single elevated reading demands repeat measurement and follow-up. The blood pressure is as much a part of the metabolic assessment as the glucose. [6] [9]
A systematic search for comorbidity completes the examination. Hepatomegaly suggests fatty liver disease. Hirsutism, acne and a menstrual history point to polycystic ovary syndrome. Striae and a fat distribution pattern distinguish Cushing syndrome. Each finding shifts the emphasis of the management plan toward the comorbidity that drives the long-term cardiovascular risk. [5]
Investigations
The diagnosis of diabetes rests on biochemical thresholds. A fasting plasma glucose at or above 7.0 millimoles per litre, a two-hour post-load glucose at or above 11.1, a random glucose at or above 11.1 with symptoms, or an HbA1c at or above 6.5 percent make the diagnosis, confirmed on a second sample unless the symptoms are unequivocal. These are the same thresholds as for adults, applied to youth. [1]
The islet autoantibody panel and a C-peptide resolve the type. Glutamic acid decarboxylase, insulinoma-associated antigen 2, insulin and zinc transporter 8 antibodies confirm or exclude autoimmunity, and a C-peptide measured with a simultaneous glucose quantifies residual beta-cell function. A measurable or high C-peptide with negative antibodies in an obese adolescent confirms type 2, while a low C-peptide with positive antibodies confirms type 1. [1]
The metabolic-syndrome and comorbidity panel completes the first assessment. A fasting lipid profile (triglycerides and HDL), liver function tests for fatty liver disease, a urine albumin-to-creatinine ratio, and where indicated an oral glucose tolerance test and a polycystic ovary syndrome hormone profile map the cluster. Thyroid function and coeliac serology are added where type 1 remains in the differential. [5] [6]
A baseline for the annual complication screen is set at diagnosis. Retinal photography, the urine albumin-to-creatinine ratio, a lipid profile and a blood pressure are documented, and the schedule of annual review is fixed from that point. Complications appear early in youth-onset type 2 diabetes, so the complication screen cannot wait for adulthood. [11]
[1]Management — Resuscitation
The great majority of youth with type 2 diabetes present without acute decompensation and begin definitive stepwise care without resuscitation. The glucose and ketone check must not be omitted in any unwell obese adolescent, however, because the minority who present in ketoacidosis or a hyperosmolar state need the standard paediatric emergency protocol. [1]
Ketoacidosis in a youth with type 2 diabetes is managed exactly as in type 1. Isotonic saline restores the circulating volume, intravenous insulin is deferred until after the first hour of fluids, potassium is replaced from the start of insulin, and the conscious level is watched for cerebral oedema. The protocol does not change with the diabetes type, and the presence of obesity does not exclude ketoacidosis. [1]
The hyperosmolar hyperglycaemic state is more typical of type 2 and demands a more gradual approach. Fluid correction is slower, the sodium is watched closely, and the high risk of thrombosis is anticipated. The principle is to lower the osmolality carefully rather than to drive the glucose down rapidly, because rapid shifts endanger the brain. [1]
Metformin and insulin are complementary, not alternatives, in the acutely hyperglycaemic or symptomatic patient. Insulin is started early when ketosis or a very high glucose is present, metformin is introduced as the acute phase resolves, and the insulin is tapered as the metabolic stress settles. Holding insulin for fear of misclassifying the type is a dangerous error. [1]
Management — Definitive & Stepwise
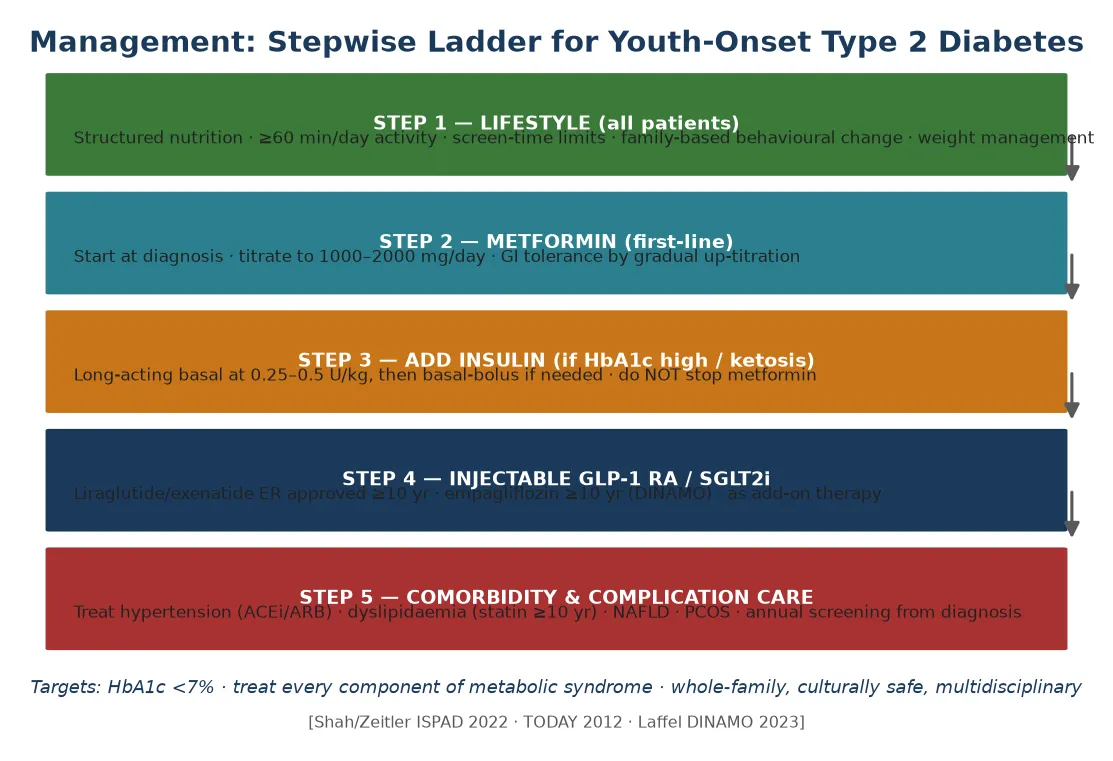
Definitive management follows a stepwise ladder. The first step is structured family-based lifestyle change for every patient. The second is metformin as first-line pharmacotherapy. The third adds insulin for inadequate control, ketosis or a very high HbA1c. The fourth introduces GLP-1 receptor agonists and SGLT2 inhibitors as add-on therapy. The fifth is aggressive comorbidity and complication care. No drug replaces the lifestyle foundation that sits beneath all of them. [1]
Lifestyle is the foundation of the ladder. Structured nutrition with family involvement, at least 60 minutes per day of moderate-to-vigorous physical activity, screen-time limits, behavioural change and weight management address the insulin resistance at its root. The TODAY experience showed that weight matters: weight loss improves glycaemic control, and weight gain accelerates failure, so the lifestyle prescription is not a soft option but a clinical intervention. [12]
Metformin is the first-line drug. Treatment starts at 500 milligrams once daily and is titrated over weeks to 1000 milligrams twice daily, for a target of 1500 to 2000 milligrams per day. Gastrointestinal tolerance is managed by gradual up-titration and an extended-release formulation. Metformin reduces hepatic glucose output and improves insulin sensitivity, and it is continued even when insulin or other agents are added. [1]
Insulin is added when metformin alone is inadequate, when ketosis is present, or when the HbA1c is very high at diagnosis. A long-acting basal is started at 0.25 to 0.5 units per kilogram per day and escalated to a basal-bolus regimen if control is inadequate, with metformin continued throughout. The TODAY finding that roughly half of adolescents fail metformin monotherapy within a few years sets the expectation of escalation rather than stability. [10]
Newer agents extend the ladder. Liraglutide and exenatide extended-release are approved from age ten, and empagliflozin is approved from age ten on the strength of the DINAMO trial, which showed a meaningful HbA1c reduction for the SGLT2 inhibitor in youth with type 2 diabetes. These agents are add-ons rather than first-line therapy, and they address different parts of the pathophysiology. [8]
Metabolic syndrome in adolescents — IDF criteria
Comorbidity control is not optional. Hypertension is treated with an ACE inhibitor or angiotensin receptor blocker, which also protects the kidney. Dyslipidaemia is treated with a statin from age ten where indicated. Non-alcoholic fatty liver disease and polycystic ovary syndrome are managed alongside the glucose. Treating only the glucose while ignoring the cluster leaves the cardiovascular risk untouched. [1] [9]
Specific Subtypes & Scenarios
The adolescent girl with polycystic ovary syndrome is a common and important scenario. Oligomenorrhoea, hirsutism and acanthosis mark the insulin resistance, and metformin, lifestyle and where indicated hormonal contraception are part of the same treatment. The reproductive and metabolic consequences of the syndrome are managed together, not separately. [1] [6]
The child with non-alcoholic fatty liver disease belongs to the same cluster. Liver function tests flag the disease, elastography quantifies the fibrosis where indicated, and the primary treatment is weight loss through the same lifestyle prescription that addresses the diabetes. The fatty liver is both a complication and a marker of the shared insulin resistance. [5]
The Indigenous or high-risk-ethnicity youth is the population in whom type 2 diabetes is most prevalent and most aggressive. Screening is indicated from age ten, culturally safe family-based care is central, and remote-access support extends the reach of the team. The SEARCH lessons on the disproportionate burden and the earlier complications in these populations frame the urgency. [4]
The obese adolescent with metabolic syndrome who does not yet meet diabetes criteria is a prevention opportunity. Intensive lifestyle intervention, and metformin in selected cases, aim to delay or prevent progression, and the same intervention benefits the parents who often share the risk. The window of prediabetes is the most cost-effective point in the whole trajectory. [1] [5]
Complications & Pitfalls
The complications of youth-onset type 2 diabetes arrive early and fast. Retinopathy, nephropathy, neuropathy and early cardiovascular disease appear sooner than in type 1, because the disease layers hyperglycaemia on top of the full metabolic cluster. The comparison between type 1 and type 2 in youth shows that the type 2 group accumulates complications at least as quickly despite a shorter duration, which is the core of the prognosis. [11]
[11]The TODAY trial defined the central pitfall of the disease. Roughly half of adolescents fail metformin monotherapy within a few years, and glycaemic control deteriorates rapidly without escalation. Reassuring a family that the diabetes is mild or stable is a clinical error that delays the intensification the disease requires. Anticipate escalation, set the expectation early, and intensify at the first sign of drift. [10]
Misclassification is the other lethal pitfall. A ketosis-prone type 2 adolescent may be labelled as type 1 and under-treated for the insulin resistance, or a type 1 adolescent may be labelled as type 2 and denied the insulin that keeps them alive. The antibody panel and the C-peptide, read against the phenotype, resolve the ambiguity and protect the adolescent from years of the wrong regimen. [1]
The comorbidity pitfall is the quiet one. Treating only the glucose while ignoring the hypertension, the dyslipidaemia, the fatty liver and the polycystic ovary syndrome leaves the cardiovascular risk untouched, and cardiovascular disease is what ultimately shortens life in these patients. The metabolic syndrome is the context of the diabetes, and every component is a target. [9] [6]
Prognosis & Disposition
Youth-onset type 2 diabetes carries a more aggressive course than type 1. Beta-cell decline is faster, complications appear earlier, and the lifetime cardiovascular burden is higher, so intensive multimodal treatment from diagnosis is the norm rather than the exception. The prognosis is shaped by how early and how aggressively the disease and its cluster are addressed. [11]
The TODAY evidence frames the trajectory. Metformin alone often fails, and many patients need combination therapy within a few years. The disease is progressive rather than stable, and the prognosis improves only with active escalation, comorbidity control, and sustained family engagement. A single prescription at diagnosis is not a management plan. [10]
The long-term complication trajectory runs toward retinopathy, nephropathy, neuropathy, fatty liver disease and premature cardiovascular events in early adulthood. Annual complication screening from diagnosis — retinal photography, albuminuria, lipids and blood pressure — is the safeguard that catches the drift early, because waiting for symptoms is waiting too long. [11] [9]
Disposition rests on lifelong specialist follow-up, structured transition to adult endocrinology in late adolescence, an annual complication screen, a whole-family approach to lifestyle, and a named safety-net for emergencies. The transition to adult care is a high-risk moment for loss to follow-up, and a structured handover is the countermeasure that keeps the young person engaged. [1]
Special Populations
The Indigenous Australian, Maori and Pacific youth carry the highest burden of type 2 diabetes and its most aggressive course. Culturally safe, family-centred and remote-access care is central, screening from age ten is non-negotiable, and the local Aboriginal medical service or Maori health provider is part of the team. The disease is common enough in these populations to shape the whole adolescent clinic. [1] [4]
The adolescent girl with polycystic ovary syndrome carries the metabolic and reproductive consequences of insulin resistance together. Metformin, lifestyle and hormonal contraception address both, and the long-term cardiovascular risk is part of the same conversation. The syndrome is a window onto the metabolic syndrome as much as a reproductive diagnosis. [6]
The child from a high-risk family in whom a parent and grandparent also have type 2 diabetes is the clearest case for a family-based approach. The family history is both the screening trigger and the treatment, because the same lifestyle prescription that helps the child helps the parents. The unit of care is the family, not the patient alone. [4]
The migrant or socioeconomically disadvantaged youth faces the practical barriers that shape the lifestyle prescription. Food security, the opportunity for activity, and health literacy all frame what is possible, and school-based and telehealth support extend the reach of the team beyond the clinic. The prescription that cannot be followed will not work. [1]
Evidence, Guidelines & Regional Differences
The guideline base rests on the ISPAD 2022 consensus on type 2 diabetes in children and adolescents, which sets the diagnostic thresholds, the screening trigger and the stepwise ladder. The IDF consensus on the metabolic syndrome in children and adolescents provides the cluster definition, and the systematic review of paediatric metabolic-syndrome criteria maps the contestation across IDF, Cook and NHLBI definitions. [1] [6] [5]
The epidemiological evidence comes from the SEARCH for Diabetes in Youth study, which has documented the rising prevalence and incidence, the cardiovascular risk-factor trends, and the lessons on the disproportionate burden in high-risk populations. These data frame the urgency of screening and the aggression of the disease. [2] [3] [9]
The treatment and complications evidence comes from the TODAY clinical trial of glycaemic control and the TODAY weight-change analysis, the DINAMO trial of empagliflozin and linagliptin in youth, and the comparison of complications between type 1 and type 2 in youth. TODAY defined the rapid failure of metformin monotherapy, DINAMO established the SGLT2 inhibitor in youth, and the comparison study set the prognosis. [10] [12] [8] [11]
The current controversies include the optimal first regimen and the early use of newer agents in children, whether HbA1c or the oral glucose tolerance test best defines diabetes and prediabetes in youth, whether to screen the general adolescent population or only high-risk groups, and the metabolic-syndrome definition itself. Regional differences in screening intensity, in the availability of newer agents, and in the transition to adult care shape practice across Australia, New Zealand, North America and Europe. [1] [5]
Exam Pearls
[10] [11]The frequently misremembered facts are worth fixing. Antibodies are usually negative in type 2 but can be positive in overlap, so a positive antibody does not by itself exclude type 2. The C-peptide is measurable and often high, in contrast to the low value of type 1. The metabolic cluster drives complications as much as the glucose does, and treating the glucose alone is not enough. [1]
The high-yield thresholds recur across the exam. The IDF metabolic syndrome needs central adiposity plus two of triglycerides at least 1.7, low HDL, blood pressure at least 130 over 85, and fasting glucose at least 5.6. Diabetes is fasting at least 7.0, two-hour or random at least 11.1, and HbA1c at least 6.5 percent. Metformin targets 1500 to 2000 milligrams per day, and basal insulin starts at 0.25 to 0.5 units per kilogram per day. [1] [6]
The high-yield lesion-sign pairings close the topic. Acanthosis nigricans in an obese adolescent is insulin resistance until assessed. An overweight child with a family history meets the ISPAD screening trigger. A C-peptide that stays measurable beyond the honeymoon with negative antibodies is type 2 or monogenic. A rising blood pressure and urine albumin in youth-onset type 2 is early nephropathy demanding an ACE inhibitor. [7] [11]
From screening to complications — the youth-onset type 2 diabetes trajectory
References
- [1]Shah AS; Zeitler PS; Wong J; et al ISPAD Clinical Practice Consensus Guidelines 2022: Type 2 diabetes in children and adolescents. Pediatr Diabetes, 2022.PMID 36161685
- [2]Lawrence JM; Divers J; Isom S; et al Trends in Prevalence of Type 1 and Type 2 Diabetes in Children and Adolescents in the US, 2001-2017. JAMA, 2021.PMID 34427600
- [3]Wagenknecht LE; Lawrence JM; Isom S; et al Trends in incidence of youth-onset type 1 and type 2 diabetes in the USA, 2002-18: results from the population-based SEARCH for Diabetes in Youth study. Lancet Diabetes Endocrinol, 2023.PMID 36868256
- [4]Jensen ET; Dabelea D Type 2 Diabetes in Youth: New Lessons from the SEARCH Study. Curr Diab Rep, 2018.PMID 29737424
- [5]Tropeano A; Corica D; Li Pomi A; et al The metabolic syndrome in pediatrics: do we have a reliable definition? A systematic review. Eur J Endocrinol, 2021.PMID 34061767
- [6]Zimmet P; Alberti KG; Kaufman F; et al The metabolic syndrome in children and adolescents - an IDF consensus report. Pediatr Diabetes, 2007.PMID 17850473
- [7]Maguolo A; Maffeis C Acanthosis nigricans in childhood: A cutaneous marker that should not be underestimated, especially in obese children. Acta Paediatr, 2020.PMID 31560795
- [8]Laffel LM; Danne T; Klingensmith GJ; et al Efficacy and safety of the SGLT2 inhibitor empagliflozin versus placebo and the DPP-4 inhibitor linagliptin versus placebo in young people with type 2 diabetes (DINAMO): a randomised trial. Lancet Diabetes Endocrinol, 2023.PMID 36738751
- [9]Kim G; Divers J; Fino NF; et al Trends in prevalence of cardiovascular risk factors from 2002 to 2012 among youth early in the course of type 1 and type 2 diabetes. The SEARCH for Diabetes in Youth Study. Pediatr Diabetes, 2019.PMID 30903717
- [10]TODAY Study Group; Zeitler P; Hirst K; et al A clinical trial to maintain glycemic control in youth with type 2 diabetes. N Engl J Med, 2012.PMID 22540912
- [11]Dabelea D; Stafford JM; Mayer-Davis EJ; et al Association of Type 1 Diabetes vs Type 2 Diabetes Diagnosed During Childhood and Adolescence With Complications During Teenage Years and Young Adulthood. JAMA, 2017.PMID 28245334
- [12]Marcus MD; Wilfley DE; El Ghormli L; et al Weight change in the management of youth-onset type 2 diabetes: the TODAY clinical trial experience. Pediatr Obes, 2017.PMID 27161901