Paeds · ent-hearing-and-oral-health
Acute and chronic rhinosinusitis
Also known as Acute bacterial sinusitis · Acute viral rhinosinusitis · Paediatric sinusitis · Ethmoiditis · Chronic rhinosinusitis · Orbital cellulitis of sinus origin · Subperiosteal abscess · Pott puffy tumour · Cavernous sinus thrombosis · Sinogenic intracranial complication
Fellowship topic on acute and chronic rhinosinusitis in children: the term rhinosinusitis because the nasal and sinus mucosa are one continuous lining; the distinction of acute viral from acute bacterial rhinosinusitis by the AAP criteria of persistence beyond ten days, double worsening, and severe onset; the chronic form lasting twelve weeks or more with impaired mucociliary clearance; the Streptococcus pneumoniae, nontypeable Haemophilus influenzae and Moraxella catarrhalis microbiology; the ostial-obstruction pathophysiology and spread through the lamina papyracea to the orbit by the Chandler stages and through the valveless diploic veins to the brain; the orbital complications of preseptal and orbital cellulitis, subperiosteal and orbital abscess and cavernous sinus thrombosis; the intracranial complications of meningitis, epidural and subdural empyema, brain abscess and Pott puffy tumour; the clinical diagnosis, the contrast CT indication, high-dose amoxicillin-clavulanate, saline irrigation and intranasal corticosteroid, and the medical versus surgical threshold for the medial subperiosteal abscess; and ANZ, UK and North American guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a four-year-old brought in with what sounds like an ordinary cold — a runny nose and a cough for the last twelve days. The family expected it to have settled by now, but the nasal discharge has stayed thick and the cough has not gone, and in the last two days the child has become more miserable with a fever returning. The temptation is to call it "just a cold that is dragging on" and to reach for an antibiotic; the skill is to recognise that the persistent, unremitting course and the late worsening mark the transition from a viral rhinosinusitis, which needs no antibiotic, to an acute bacterial rhinosinusitis, which does. [1]
The term rhinosinusitis is deliberate. The mucosa lining the nasal cavity and that lining the paranasal sinuses are one continuous sheet, and an inflammation that affects one almost always affects the other — which is why nearly every viral upper-respiratory infection briefly involves the sinuses. Rhinosinusitis is therefore defined as symptomatic inflammation of both the nose and the paranasal sinuses: a combination of nasal blockage, discharge, facial pressure or hyposmia. The paranasal sinuses — the maxillary, ethmoid, frontal and sphenoid — are paired, air-filled mucosal outpouchings that drain through narrow ostia into the nasal cavity, all converging at the ostiomeatal complex. [6]
The classification that examiners expect is by duration. Acute rhinosinusitis lasts under twelve weeks and is further split into acute viral (the common cold, by far the commonest) and acute bacterial. Chronic rhinosinusitis lasts twelve weeks or more and reflects persistently impaired mucociliary clearance rather than simple infection; it overlaps heavily with adenoidal hypertrophy, allergic rhinitis and, in a minority, with cystic fibrosis, primary ciliary dyskinesia and immunodeficiency. Recurrent acute rhinosinusitis describes separate acute episodes separated by symptom-free intervals. [6] [7]
Most rhinosinusitis is viral and self-limiting, and the modern challenge is stewardship — reserving antibiotics for the bacterial patterns and reserving imaging for the complication. The danger lies in the orbital and intracranial spread that can follow when an obstructed sinus infects and erodes: a swollen eye in a febrile child, or a severe headache with meningism, turns a routine upper-airway problem into a sight- and life-threatening emergency. The task is layered — make the bacterial diagnosis on clinical grounds, give the right antibiotic, and watch for the red flags that demand imaging and a multidisciplinary response. [4] [11]
Classification
The framework examiners use separates rhinosinusitis first by duration and then by the presence of a complication, because duration decides whether you are treating a viral cold or a chronic mucosal disease, while the complication decides whether the child is going home or to theatre. [6] [1]
By duration, acute rhinosinusitis is symptoms lasting under twelve weeks. Within the acute group, the clinically vital distinction is between acute viral rhinosinusitis — the common cold, which accounts for the overwhelming majority of cases and is clinically indistinguishable from bacterial disease in its first ten days — and acute bacterial rhinosinusitis, which the AAP defines by three patterns: persistent symptoms of nasal discharge or daytime cough for ten or more days without improvement; a worsening or "double worsening" course in which a viral illness improves and then deteriorates; and a severe onset, with fever of at least thirty-nine degrees Celsius and purulent nasal discharge for three or more consecutive days. [1] Chronic rhinosinusitis is the same constellation of symptoms persisting for twelve weeks or more, with impaired mucociliary clearance and often with adenoidal hypertrophy, allergy or an underlying systemic cause. Recurrent acute rhinosinusitis is repeated discrete acute episodes with full recovery between them. [7] [8]
By complication, the orbital and intracranial spread that defines severe disease is classified by where the infection has gone. The orbital complications are graded by the Chandler stages, ascending from preseptal cellulitis through orbital cellulitis, subperiosteal abscess and orbital abscess to cavernous sinus thrombosis. The intracranial complications are meningitis, epidural and subdural empyema, brain abscess and the Pott puffy tumour. A child may present with a complication as the first clear sign of sinus disease, particularly the toddler with ethmoiditis and a swollen eye. [3] [11]

Epidemiology & Risk Factors
Acute rhinosinusitis is one of the commonest reasons children see a doctor, and acute viral rhinosinusitis — the common cold — is almost universal in early childhood, with children averaging six to eight upper-respiratory infections a year in the preschool years. Acute bacterial rhinosinusitis complicates an estimated five to ten per cent of these viral colds, which is why the persistent or worsening cold is the gateway to the bacterial diagnosis. [1] [11]
The children who develop chronic and recurrent disease, and those who suffer complications, share recognisable vulnerabilities. Allergic rhinitis and adenoidal hypertrophy are the commonest predisposing factors in chronic paediatric disease, both by obstructing the ostiomeatal complex and sustaining mucosal inflammation. Exposure to second-hand smoke and attendance at childcare increase the frequency of viral colds and so of bacterial sinusitis. The less common but important systemic causes — cystic fibrosis, primary ciliary dyskinesia and immunodeficiency — produce chronic, recurrent and refractory sinusitis driven by impaired clearance and unusual organisms, and they must be actively excluded when the disease is persistent, severe or out of proportion to the clinical picture. [7] [8]
The age band matters because the sinuses pneumatise at different times. The ethmoid and maxillary sinuses are present at birth and are the dominant sites of paediatric disease, which is why the infant and toddler typically develop ethmoiditis with an orbital complication. The sphenoid sinus pneumatises by around five years, and the frontal sinus is not clinically significant until late childhood, which is why frontal sinusitis and its Pott puffy tumour complication are diseases of the older child and adolescent. The pneumococcal conjugate vaccines have reduced the burden of Streptococcus pneumoniae disease, but pneumococcus remains the single most important organism. [1] [5]
In Australia and Aotearoa New Zealand, the burden of otitis media, rhinosinusitis and their complications is far higher in Aboriginal and Torres Strait Islander, Maori and Pasifika children, in whom chronic suppurative upper-airway disease is endemic and the threshold for complication is lower. The Royal Children's Hospital Melbourne clinical pathway frames sinusitis and its complications as conditions requiring early assessment, a low threshold for antibiotics in the bacterial patterns, prompt contrast CT for any orbital or intracranial feature, and coordinated care between paediatrics, ENT, ophthalmology and, where needed, neurosurgery — delivered with culturally safe, community-linked support so that distance does not delay treatment. [11]
The microbiology has shifted with vaccination and antibiotic pressure. Streptococcus pneumoniae, nontypeable Haemophilus influenzae and Moraxella catarrhalis cause most acute bacterial rhinosinusitis, with M. catarrhalis and a proportion of H. influenzae producing beta-lactamase — the rationale for the amoxicillin-clavulanate choice. In chronic and complicated disease, and in the child with cystic fibrosis or immunodeficiency, Staphylococcus aureus (including methicillin-resistant strains), Pseudomonas aeruginosa and anaerobes become important and demand a different empiric regimen. [2] [7]
Pathophysiology
Why does a common cold become a bacterial sinusitis, and why does it sometimes reach the eye and the brain? The answer lies in the anatomy of the sinus ostia and in the valveless veins that connect the sinuses to the orbit and the cranial cavity. [6] [3]
The paranasal sinuses are kept healthy by continuous mucociliary clearance: the ciliated mucosa sweeps mucus, trapped particles and bacteria out through the narrow ostia and the ostiomeatal complex into the nasal cavity. A viral upper-respiratory infection inflames this mucosa, and the swelling narrows and then obstructs the ostium. Once the ostium is blocked, oxygen within the sinus is resorbed, the cilia fail, and secretions accumulate and stagnate. This warm, static, poorly oxygenated environment is the ideal culture medium, and the bacteria that colonise the upper airway — S. pneumoniae, H. influenzae and M. catarrhalis — multiply to produce acute bacterial rhinosinusitis. The same mechanism, sustained by allergic inflammation, adenoidal obstruction or impaired cilia, underlies chronic rhinosinusitis. [1] [6]
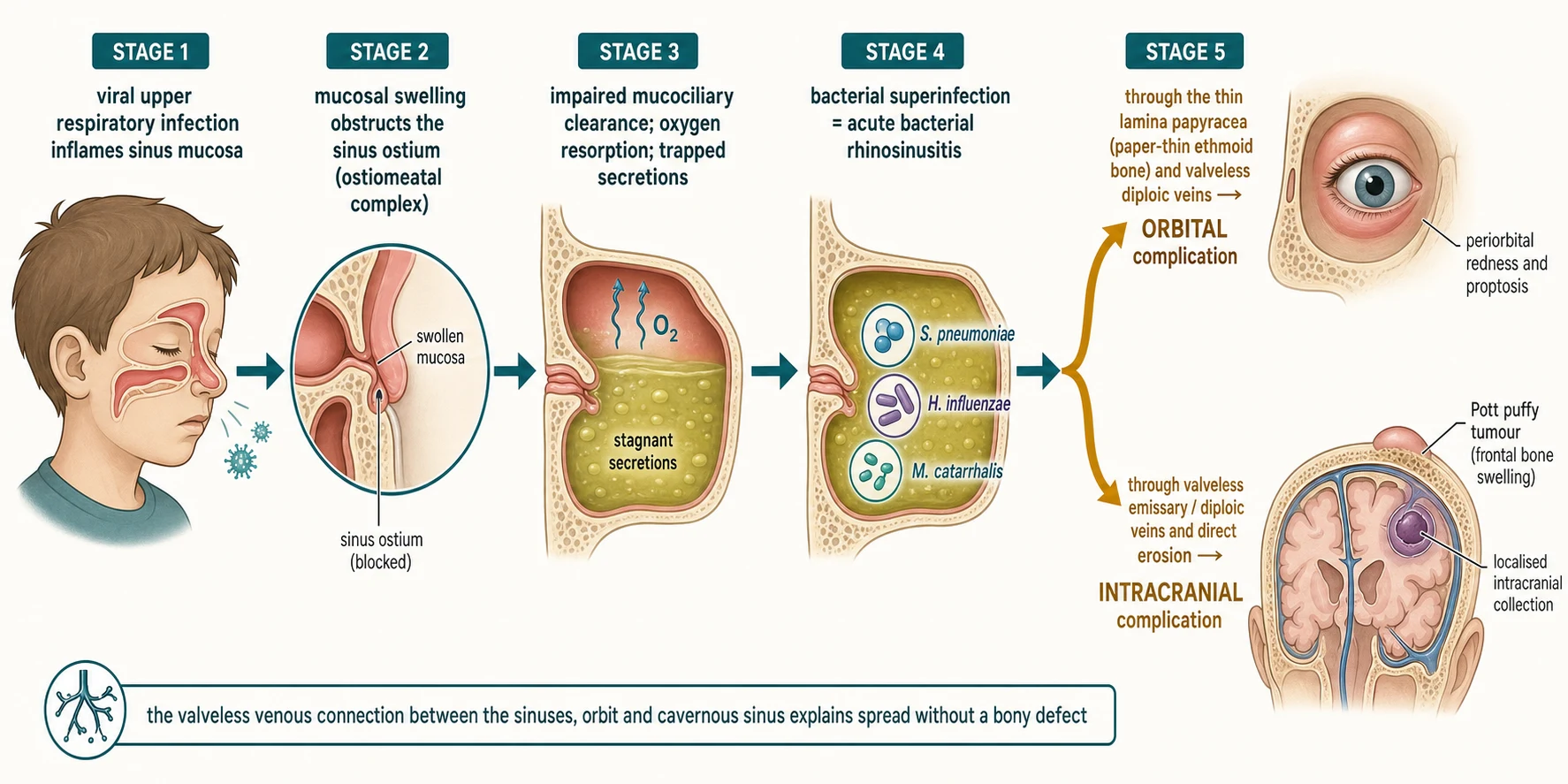
The routes of spread explain every complication. The lamina papyracea is the paper-thin medial wall of the orbit and the lateral wall of the ethmoid sinuses; ethmoid infection erodes or traverses it to reach the orbit, producing the Chandler sequence. Infection passes first into the eyelid as preseptal cellulitis, then into the orbital soft tissue as orbital cellulitis; pus then collects between the periorbita and the bone as a subperiosteal abscess (displacing the eye down and out), within the orbital fat as an orbital abscess (with proptosis, ophthalmoplegia and threatened vision), and finally into the cavernous sinus as cavernous sinus thrombosis with bilateral eye signs, cranial nerve palsies and sepsis. [3] [9]
The intracranial complications are reached through the valveless diploic, emissary and ophthalmic veins that connect the sinuses, orbit and cavernous sinus to the cranial cavity — which is why intracranial spread can occur without a bony defect. Meningitis is the commonest intracranial complication; subdural and epidural empyema and brain abscess carry the highest mortality. Cavernous sinus thrombosis sits at the junction of the orbital and intracranial pathways and is rapidly fatal if missed. The Pott puffy tumour is osteomyelitis of the frontal bone with a subperiosteal abscess, classically a complication of frontal sinusitis in the older child and adolescent, presenting with a boggy forehead swelling, frontal headache and signs of intracranial extension. [4] [5]
Clinical Presentation
The child with acute bacterial rhinosinusitis presents with nasal symptoms that have outlasted a simple cold or that have worsened after initial improvement. The cardinal features are a thick, purulent nasal discharge, nasal obstruction, and a daytime cough that is often worse at night; facial fullness or pain is present in the older child but is unreliable in the young. Fever is variable. The three AAP patterns bring the child to attention: a persistent illness beyond ten days, a double-worsening biphasic course, or a severe onset with high fever and purulent discharge. Hyposmia and halitosis are common. [1]
A child with an orbital complication presents with a swollen, painful eye in the setting of sinus symptoms — most often ethmoiditis in a young child. The findings track the Chandler stage: eyelid swelling and erythema in preseptal cellulitis, proptosis and chemosis as infection enters the orbit, painful or restricted eye movement (ophthalmoplegia) and diplopia, and reduced visual acuity or colour vision as the optic nerve is threatened. A subperiosteal abscess characteristically displaces the globe downward and outward, because the abscess collects along the medial orbital wall. The cardinal step is to measure and document the visual acuity, because a falling acuity marks the transition from a medical to a surgical urgency. [3] [9]
The intracranial complications declare themselves through systemic and neurological deterioration. Meningitis presents with headache, photophobia, neck stiffness and altered consciousness. A subdural or epidural empyema or a brain abscess produces progressive severe headache, fever, vomiting, focal neurology, seizures or a depressed conscious state. Cavernous sinus thrombosis presents with bilateral eye signs, cranial nerve palsies (III, IV, V1, V2 and VI), a toxic appearance and rapid deterioration. Pott puffy tumour presents with a tender, boggy forehead or scalp swelling, frontal headache, fever and often signs of intracranial extension in an older child. Any of these in a child with sinus disease is an emergency of the highest order. [4] [5]
Differential Diagnosis
The differential of persistent nasal discharge and cough turns on whether the course fits a bacterial sinusitis and whether something else explains the picture. Acute viral rhinosinusitis is the commonest mimic and is clinically indistinguishable from bacterial disease in the first ten days; the AAP criteria exist precisely to separate them. Allergic rhinitis produces clear bilateral discharge, sneezing, itching and an atopic background rather than fever and purulence, and it overlaps with chronic rhinosinusitis. Adenoiditis and adenoidal hypertrophy cause chronic mouth-breathing, snoring and nasal obstruction in a young child and are easily confused with chronic sinusitis. [1] [6]
[11]The critical bedside pitfall is the unilateral foul-smelling discharge. A unilateral, purulent, foul-smelling nasal discharge in a child is a nasal foreign body until proven otherwise, and treating it as sinusitis with antibiotics simply delays removal and, in the case of a button battery, allows liquefactive necrosis of the septum. Always examine the nose and consider the foreign body before prescribing. [11]
For the swollen eye, the key distinction is preseptal (periorbital) cellulitis — infection of the eyelid skin and subcutaneous tissue, often from a skin lesion, insect bite or conjunctivitis, with a normal eye and normal vision — from orbital (post-septal) cellulitis, which arises from ethmoid sinusitis, has proptosis, chemosis, ophthalmoplegia or reduced vision, and is a surgical emergency. Headache and facial pain may also be from migraine, tension-type headache or a dental infection referring to the maxillary sinus, and a careful history separates these. [9] [12]
The cardinal error is overdiagnosing bacterial sinusitis in the first ten days of a viral cold and prescribing antibiotics that do not help, while missing the complication in the child whose swollen eye or headache is attributed to a minor illness. The AAP clinical-criteria approach is the defence against the first error, and a low threshold for imaging and referral is the defence against the second. [1] [4]
Clinical & Bedside Assessment
The assessment is a structured search for the bacterial pattern and for any complication, because their presence determines the antibiotic, the imaging and the referral. Begin with the history: the duration and trajectory of the nasal discharge and cough, any preceding cold, the character of the discharge, the presence and height of fever, and the three AAP patterns specifically. Ask about headache, eye symptoms — pain, swelling, double vision, reduced vision — photophobia, neck stiffness, vomiting and altered consciousness, because these flag the orbital and intracranial complications. [1] [9]
The examination is built around the nose, the eyes and the nervous system. Perform anterior rhinoscopy or, where available, nasal endoscopy, looking for purulent discharge in the middle meatus, mucosal oedema and polyps; note the laterality, because a unilateral purulent discharge raises a foreign body. For the eye, inspect the lids and periorbita for swelling and erythema, measure proptosis, assess eye movements for the limitation of ophthalmoplegia, and — above all — measure and document the visual acuity and colour vision and perform fundoscopy for papilloedema. A full neurological examination looks for meningism, focal deficits and a depressed conscious state. [3] [9]
The sinusitis assessment — DRAIN
Assess the systemic state directly. Fever, tachycardia and a toxic appearance signal invasive disease, and the child should be assessed and resuscitated alongside the upper-airway examination. In the very young child, who cannot localise facial pain and in whom the sinuses are incompletely pneumatized, the threshold to treat as bacterial sinusitis and to image for a complication is lower. A child with sinus symptoms who develops eye signs, a severe headache or any neurological symptom has an orbital or intracranial complication until imaging proves otherwise. [4] [11]
Investigations
Investigation is driven by the clinical stage, and the central principle is that acute bacterial rhinosinusitis is a clinical diagnosis that needs no routine imaging and no routine cultures. In the uncomplicated case, no test adds to the history: the AAP and EPOS guidance both stress that plain sinus radiographs are unhelpful — the mucosal thickening and opacification they show are present in most uncomplicated viral colds — and that cultures of nasal discharge are unreliable because they are contaminated by colonising flora. [1] [6]
The key investigation for any suspected complication is contrast-enhanced computed tomography of the sinuses, orbits and brain. The indications are a suspected orbital complication — periorbital swelling with proptosis, ophthalmoplegia or reduced vision, or a subperiosteal or orbital abscess — and any suspected intracranial extension. Contrast CT shows the sinus opacification, the subperiosteal or orbital abscess as a rim-enhancing collection, bony erosion, and intracranial collections; it is fast, available and the modality of choice in the acutely unwell child. [9] [11]
At the Royal Children's Hospital Melbourne and across Australian and New Zealand practice, contrast CT of the sinuses and orbits is obtained for any suspected orbital complication — the child with proptosis, ophthalmoplegia, reduced vision, or a swollen eye that does not settle on intravenous antibiotics. Magnetic resonance imaging with venography is reserved for suspected intracranial extension, cavernous sinus thrombosis, brain abscess or empyema, where it defines the thrombus, the venous anatomy and the parenchymal lesion better than CT, and avoids radiation. Imaging must never delay intravenous antibiotics in the deteriorating child. [4] [11]
In chronic rhinosinusitis, nasal endoscopy documents mucosal disease, polyps and purulent discharge, and allergy testing identifies the atopic child. When chronic disease is severe, recurrent, out of proportion, or accompanied by other features, the underlying causes must be excluded: a sweat test for cystic fibrosis, nasal nitric oxide and ciliary studies for primary ciliary dyskinesia, and immune function tests for immunodeficiency. Blood cultures and a pus swab from any drained collection guide antimicrobial de-escalation in the complicated case. [7] [8]
Management — Resuscitation
Resuscitation belongs to the child with an orbital or intracranial complication, and to any child who is systemically unwell. The red flags are a febrile child with periorbital or orbital signs, eye pain or visual change; a child with a severe headache, meningism, focal neurology or a depressed conscious state; and a child with a boggy forehead swelling suggesting a Pott puffy tumour. Any of these warrants urgent assessment, intravenous access and senior paediatric, ENT, ophthalmology and — where the brain is involved — neurosurgical review. [4] [9]
The immediate priorities are to secure the airway and circulation if the child is shocked, to obtain intravenous access, to take blood cultures, and to start broad-spectrum intravenous antibiotics without delay. The empiric regimen must cover the streptococci, staphylococci and anaerobes of complicated sinus disease, with Pseudomonas-directed cover added when the child has cystic fibrosis, immunodeficiency or chronic disease. A regimen such as intravenous ceftriaxone 50 mg per kilogram (maximum 2 g) once daily with metronidazole 7.5 mg per kilogram (maximum 500 mg) every eight hours, adding vancomycin for suspected methicillin-resistant Staphylococcus aureus or critical illness, is a reasonable empiric start; some units use ampicillin-sulbactam or cefotaxime. Do not wait for imaging or culture results in the deteriorating child. [2] [9]
Escalate to intensive care for the child with cavernous sinus thrombosis, raised intracranial pressure, a brain abscess or a depressed conscious state. Protect the threatened vision by involving ophthalmology early and by imaging and draining a post-septal abscess before the optic nerve is injured. Separate resuscitation from definitive therapy in your mind: the well child with uncomplicated acute bacterial rhinosinusitis goes home on oral antibiotics with a safety-net, while the child with an orbital or intracranial complication needs the hospital, the scan, the multidisciplinary team and often the operating theatre. [4] [11]
Management — Definitive & Stepwise
Definitive management is a stepwise pathway matched to whether the disease is viral, acute bacterial, or complicated, and to whether a chronic underlying cause is present. Uncomplicated viral rhinosinusitis takes supportive care; acute bacterial rhinosinusitis takes a targeted antibiotic with adjuncts; an orbital or intracranial complication takes intravenous antibiotics and surgery; and chronic rhinosinusitis takes medical therapy with surgery reserved for failure. [1] [7]
For acute viral rhinosinusitis, manage supportively. Saline irrigation (isotonic or hypertonic, by spray or rinse appropriate to age), analgesia, antipyretics and adequate fluids relieve symptoms; decongestants and antihistamines are not routinely recommended in young children. Give a clear safety-net for the red flags of orbital and intracranial spread, and review if the symptoms persist beyond ten days or worsen. [1] [6]
For acute bacterial rhinosinusitis, the first-line antibiotic is high-dose amoxicillin-clavulanate 90 mg per kilogram per day of the amoxicillin component in two divided doses (maximum 4 g per day of amoxicillin) for ten to fourteen days. The high dose overcomes penicillin-resistant pneumococci and the clavulanate covers the beta-lactamase-producing H. influenzae and M. catarrhalis. For the child with a penicillin allergy, use cefdinir 14 mg per kilogram per day in one or two doses or cefuroxime 30 mg per kilogram per day in two divided doses, and clindamycin with consideration of a third-generation cephalosporin in the setting of a severe beta-lactam allergy. Add an intranasal corticosteroid and continue saline irrigation as adjuncts. [1] [2]
Acute bacterial rhinosinusitis — antibiotic pathway (AAP 2013 / IDSA 2012 / NICE / eTG — confirm locally)
The stepwise rhinosinusitis pathway
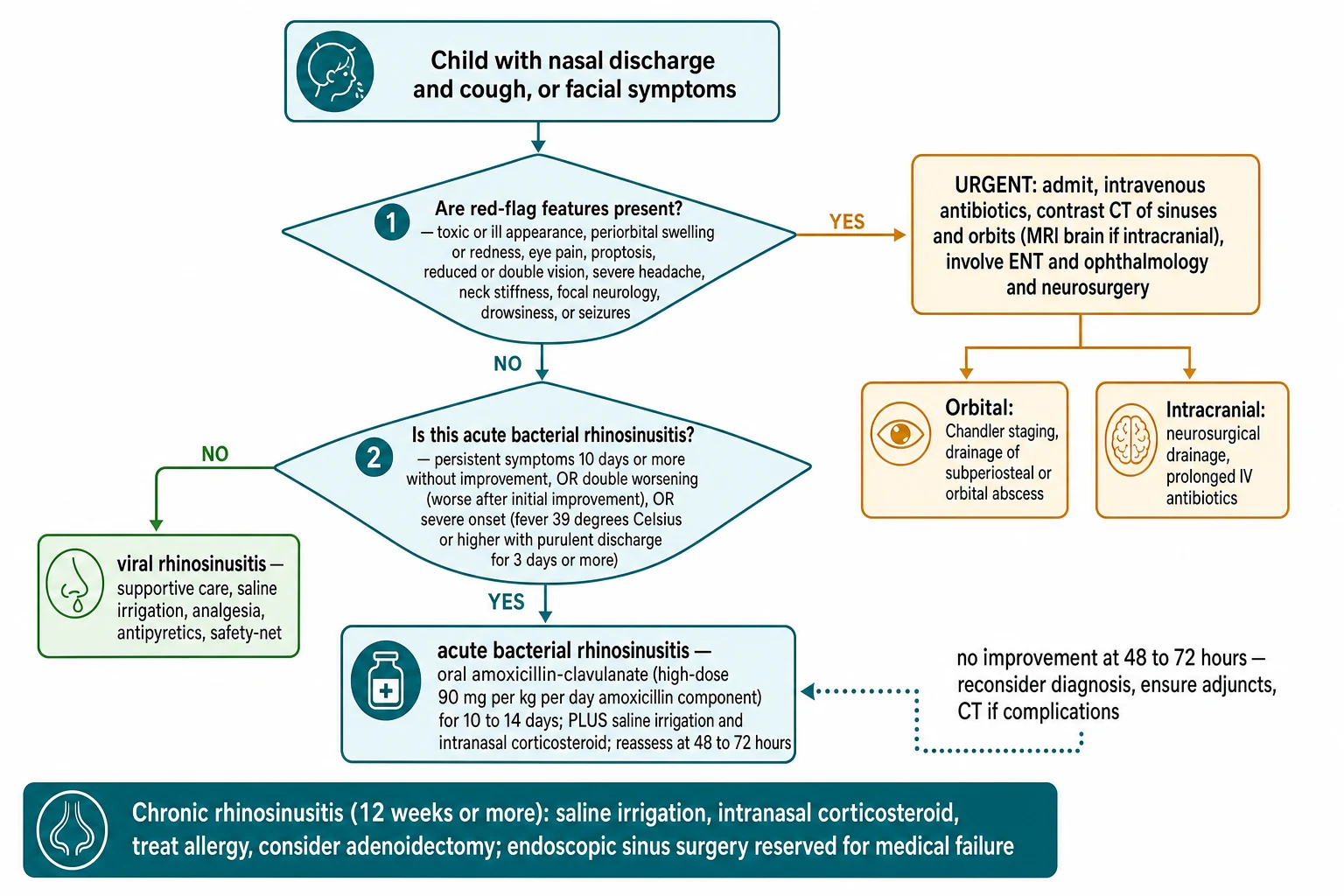
Apply the AAP criteria: persistent symptoms beyond ten days, double worsening, or severe onset with fever and purulent discharge — absent, manage as viral rhinosinusitis with supportive care and a safety-net.
For acute bacterial rhinosinusitis, give high-dose amoxicillin-clavulanate 90 mg/kg/day of the amoxicillin component in two divided doses (max 4 g/day) for ten to fourteen days, with saline irrigation and an intranasal corticosteroid.
Reassess at forty-eight to seventy-two hours; if there is no improvement, reconsider the diagnosis, ensure saline and corticosteroid adherence, and image if a complication is suspected.
For any orbital or intracranial red flag, admit, start intravenous ceftriaxone plus metronidazole (add vancomycin for MRSA or critical illness), and obtain contrast CT of the sinuses and orbits — MRI brain if intracranial.
Refer urgently to ENT and ophthalmology for orbital complications; Chandler stage 3–5 typically needs surgical drainage of the subperiosteal or orbital abscess, with selected small medial abscesses managed medically.
Involve neurosurgery for intracranial extension — empyema, brain abscess, cavernous sinus thrombosis and Pott puffy tumour need drainage and prolonged intravenous antibiotics.
Manage chronic rhinosinusitis with saline irrigation, an intranasal corticosteroid and treatment of allergy; exclude cystic fibrosis, primary ciliary dyskinesia and immunodeficiency; reserve adenoidectomy and endoscopic sinus surgery for medical failure.
Give a clear safety-net at discharge for the red flags of orbital and intracranial spread, and arrange follow-up to confirm resolution.
For the orbital complication, the approach is graded by the Chandler stage. Preseptal cellulitis and uncomplicated orbital cellulitis usually respond to intravenous antibiotics. A subperiosteal abscess (stage 3) classically needs surgical drainage, but a carefully selected small medial abscess in a young child with normal vision and no intracranial feature may be managed with intravenous antibiotics and close observation, with a low threshold to operate if vision deteriorates, the abscess is large, or there is no prompt improvement. The prognostic-cohort study of paediatric medial subperiosteal abscesses confirmed that age, abscess size and the clinical state guide the medical-versus-surgical decision. An orbital abscess (stage 4) and cavernous sinus thrombosis (stage 5) are surgical and intensive-care emergencies. [9] [12]
For the intracranial complication, a subdural or epidural empyema, a brain abscess and a Pott puffy tumour need urgent neurosurgical drainage alongside prolonged intravenous antibiotics that cross the blood-brain barrier. Cavernous sinus thrombosis is managed with prolonged intravenous antibiotics and intensive-care support; anticoagulation is individualised and controversial. The intracranial-complications series confirmed that these complications, though uncommon, carry the highest morbidity and mortality and demand a combined ENT, neurosurgical and infectious-diseases response. [4] [5]
For chronic rhinosinusitis, the mainstays are saline irrigation, an intranasal corticosteroid and treatment of any allergic component, with adenoidal disease addressed. The AAO-HNS consensus statement frames paediatric chronic rhinosinusitis as a primarily medical disease in which adenoidectomy is the first-line surgical step for persistent disease and endoscopic sinus surgery is reserved for children who fail maximal medical therapy and have documented disease on imaging or endoscopy. Exclude and treat the underlying systemic causes. [7] [8]
Specific Subtypes & Scenarios
A child with the severe-onset form of acute bacterial rhinosinusitis. A fever of at least thirty-nine degrees Celsius with purulent nasal discharge for three or more consecutive days, from the outset, distinguishes this from a typical viral cold and is an AAP criterion in its own right. Treat with high-dose amoxicillin-clavulanate and adjuncts, and maintain a low threshold for imaging if any red flag appears, because the severe onset overlaps with early complication. [1] [11]
A toddler with ethmoiditis and an orbital complication. Because the ethmoid sinuses are present at birth, ethmoiditis is the typical paediatric sinusitis and the source of most orbital complications in the infant and young child. A febrile, irritable toddler with periorbital swelling needs prompt assessment of the eye and vision, intravenous antibiotics, contrast CT and ENT and ophthalmology review. [3] [9]
A child with a medial subperiosteal abscess. The commonest surgical orbital complication, a medial subperiosteal abscess displaces the eye down and out. While the historical default was drainage, selected small abscesses in young children (often under about nine years) with normal vision, no intracranial feature and an unambiguous organism response can be managed with intravenous antibiotics and close observation; large abscesses, abscesses above the optic nerve, vision compromise, failure to improve or any intracranial feature mandate drainage. [9] [12]
A child with Pott puffy tumour. A boggy, tender forehead or scalp swelling with frontal headache and fever in an older child or adolescent marks osteomyelitis of the frontal bone with a subperiosteal abscess, a complication of frontal sinusitis. Urgent contrast CT and MRI, intravenous antibiotics covering Staphylococcus aureus and anaerobes, and combined ENT and neurosurgical drainage are required, because intracranial extension — an epidural empyema or brain abscess — is common. [4] [5]
A child with cavernous sinus thrombosis. Bilateral eye signs, ophthalmoplegia with cranial nerve III, IV, V1, V2 and VI palsies, chemosis, proptosis, a toxic appearance and rapid deterioration mark septic thrombosis of the cavernous sinus. This is a life-threatening emergency requiring intensive care, prolonged intravenous antibiotics, urgent imaging and a combined ENT, neurosurgical and ophthalmological response, with anticoagulation individualised. [4] [5]
A child with cystic fibrosis, primary ciliary dyskinesia or immunodeficiency. Chronic rhinosinusitis in these children is driven by impaired clearance and unusual organisms — Pseudomonas aeruginosa and Staphylococcus aureus in cystic fibrosis. Use a Pseudomonas-directed empiric regimen such as ceftazidime, image early, involve a multidisciplinary team, and actively exclude the underlying diagnosis in any child with chronic, recurrent or refractory disease. [7] [8]
A child with a nasal foreign body and unilateral discharge. A unilateral foul-smelling purulent discharge, with or without epistaxis, in an otherwise well child is a retained nasal foreign body until proven otherwise. Examine the nose, remove the object promptly, and remember that a button battery is an emergency causing liquefactive necrosis of the nasal septum within hours. Do not treat as sinusitis. [11]
Complications & Pitfalls
The most feared complications are the orbital and intracranial. Of the orbital complications, cavernous sinus thrombosis carries the highest mortality, and an orbital abscess threatens vision through optic nerve compromise; a subperiosteal abscess threatens vision if it enlarges above the optic nerve or fails to drain. Of the intracranial complications, a subdural empyema and a brain abscess carry the highest mortality, and meningitis is the commonest. The Pott puffy tumour, though classically a frontal-bone entity, is frequently associated with an intracranial collection at presentation. The intracranial-complications series confirmed that these are the events that turn a treatable sinus infection into a life-threatening one. [4] [5]
The cardinal pitfall is overdiagnosing bacterial sinusitis in the first ten days of a viral cold. Because a viral rhinosinusitis and an early bacterial one are clinically indistinguishable for the first ten days, prescribing antibiotics early does not help and drives resistance; the AAP clinical-criteria approach exists to reserve antibiotics for the persistent, double-worsening or severe-onset patterns. The discipline is to wait, to use the criteria, and to give a clear safety-net. [1] [2]
A second pitfall is missing a post-septal orbital cellulitis as a simple lid swelling. Preseptal cellulitis looks like a swollen lid and is managed with oral antibiotics, but a post-septal orbital cellulitis or abscess — signalled by proptosis, chemosis, ophthalmoplegia or reduced vision — is a surgical emergency. The single most important habit is to assess and document the visual acuity and eye movements in every child with a swollen eye, and to image and refer when any post-septal sign is present. [9] [12]
A third pitfall is attributing intracranial signs to a minor illness. A severe headache, meningism, focal neurology or a depressed conscious state in a child with sinus disease is an intracranial complication until imaging proves otherwise, and a low threshold for contrast CT and MRI is the defence. A fourth pitfall is treating a unilateral foul discharge as sinusitis and missing a nasal foreign body — particularly a button battery, which causes rapid liquefactive necrosis. [4] [11]
Prognosis & Disposition
Most children with uncomplicated acute viral or bacterial rhinosinusitis recover fully, and the outlook with appropriate antibiotics and supportive care is excellent. The morbidity and mortality rise sharply when an orbital or intracranial complication is missed or treated late. The complications-of-acute-sinusitis series confirmed that outcomes are consistently good when the bacterial diagnosis is made on clinical criteria, the complication is recognised early, and the multidisciplinary response is timely. [11] [1]
Disposition follows the stage. Manage the child with a clear viral cold and the child who meets the AAP criteria but is systemically well in the community with supportive care or oral antibiotics and a clear safety-net. Admit any child with an orbital or intracranial complication, any systemic toxicity, and any child in whom the diagnosis or the safety-net cannot be reliably maintained. The threshold for admitting the very young, the systemically unwell and the child with underlying chronic disease is deliberately low. [9] [11]
At discharge, complete the antibiotic course, confirm resolution of the nasal symptoms and any eye signs, and arrange follow-up. After an orbital complication, document and monitor the vision; after an intracranial complication, arrange neurological and audiometric follow-up as indicated. Address any underlying allergic, adenoidal or systemic cause to prevent recurrence, and give a clear safety-net for recurrent fever, a swollen eye, severe headache or any neurological symptom. Chronic and recurrent disease warrants ENT referral and, where indicated, allergy testing and exclusion of cystic fibrosis, primary ciliary dyskinesia and immunodeficiency. [7] [8]
Special Populations
Infants and toddlers are at higher risk of the orbital complication because the ethmoid sinuses are present at birth and the lamina papyracea is thin, and they cannot localise facial pain. A febrile, irritable young child with periorbital swelling is assumed to have ethmoiditis with an orbital complication until assessed, and the threshold to image and to treat with intravenous antibiotics is lower. [3] [11]
Children with cystic fibrosis, primary ciliary dyskinesia or immunodeficiency develop chronic, recurrent and refractory rhinosinusitis driven by impaired clearance and unusual organisms such as Pseudomonas aeruginosa and Staphylococcus aureus. They need early imaging, broad empiric cover, a lower surgical threshold and active exclusion and management of the underlying disease. [7] [8]
Aboriginal and Torres Strait Islander, Maori and Pasifika children carry a far higher burden of upper-airway infection and its complications, with chronic suppurative disease endemic in many communities. The threshold to investigate and treat aggressively is lower, and the management pathway must be embedded in culturally safe, community-linked care delivered with the family, with trained interpreters, and with retrieval and telehealth support for rural and remote children so that distance does not delay treatment. [11]
Atopic children with allergic rhinitis and asthma have a higher risk of chronic rhinosinusitis through sustained mucosal inflammation and ostial obstruction. Treat the allergic component with intranasal corticosteroids and allergen avoidance, and manage the sinus disease in parallel, because uncontrolled allergic rhinitis perpetuates chronic sinus disease and its complications. [6] [7]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric rhinosinusitis rests on clinical practice guidelines, consensus statements and observational cohort series rather than large randomised trials. The AAP 2013 clinical practice guideline defines the three diagnostic patterns and the antibiotic pathway; the IDSA 2012 guideline aligns with it across children and adults; the EPOS 2020 European position paper sets the international framework for acute and chronic disease; and the AAO-HNS consensus statement frames the surgical management of paediatric chronic rhinosinusitis. [1] [2] [6]
AAP clinical practice guideline: acute bacterial sinusitis in children aged 1 to 18 years
Population: Children aged 1 to 18 years presenting with acute bacterial sinusitis, addressed by an AAP subcommittee through a structured review of the evidence.
Key finding
Acute bacterial sinusitis is a clinical diagnosis based on persistent symptoms beyond ten days, a worsening (double-worsening) course, or severe onset with fever and purulent discharge; high-dose amoxicillin with or without clavulanate is first-line, with imaging reserved for suspected complications.
Practice change
A criteria-based approach reserves antibiotics for the bacterial patterns and imaging for the complication, supporting antimicrobial stewardship and the early recognition of orbital and intracranial spread.
The Chandler classification of orbital complications, now over fifty years old, remains the international standard for grading the orbital spread of sinusitis and frames the surgical decision. The orbital-cellulitis-and-abscess management reviews and the prognostic-cohort study of paediatric medial subperiosteal abscesses have refined the medical-versus-surgical decision, validating a trial of intravenous antibiotics for selected small medial abscesses with normal vision. [3] [9] [12]
Prognostic factors of paediatric medial subperiosteal orbital abscess
Population: Children with acute ethmoidal rhinosinusitis and an orbital subperiosteal abscess, reviewed for the clinical, laboratory and imaging factors predicting the need for surgical drainage.
Key finding
Younger age, smaller abscess size, absence of intracranial extension, normal vision and an unequivocal response to intravenous antibiotics identified children who could be managed medically, while large abscesses, vision compromise and intracranial extension mandated drainage.
Practice change
The management of the paediatric medial subperiosteal abscess can be individualised — a trial of intravenous antibiotics is reasonable in selected young children with a small abscess and normal vision, provided the threshold for surgical drainage is preserved for failure or for high-risk features.
The regional policy structure is consistent in principle and varies in detail. In the UK, NICE antimicrobial-prescribing guidance sets the empiric antibiotic choices and the imaging indications. In Australia and New Zealand, the Royal Children's Hospital Melbourne clinical pathway and the Therapeutic Guidelines set the local approach, with high-dose amoxicillin-clavulanate as first-line and Pseudomonas-directed cover added when chronic disease is the source. In North America, the AAP and the American Academy of Otolaryngology guidance set the management framework. The controversies — the routine use of antibiotics, the precise surgical threshold for the medial subperiosteal abscess, and the role of anticoagulation in cavernous sinus thrombosis — are resolved by the same principle in every region: use the AAP criteria, treat the bacterial disease with the right antibiotic and adjuncts, and recognise the complication early enough to image, refer and operate. [1] [11]
Exam Pearls
- Rhinosinusitis is inflammation of the nasal cavity and paranasal sinuses together; the term reflects their continuous mucosa. [6]
- The three AAP patterns for acute bacterial rhinosinusitis are persistent symptoms beyond ten days, double worsening, and severe onset with fever and purulent discharge for three or more days. [1]
- The causative organisms are Streptococcus pneumoniae, nontypeable Haemophilus influenzae and Moraxella catarrhalis; Staphylococcus aureus, Pseudomonas aeruginosa and anaerobes appear in chronic and complicated disease. [2]
- First-line treatment is high-dose amoxicillin-clavulanate 90 mg per kilogram per day of the amoxicillin component in two divided doses for ten to fourteen days, with saline irrigation and an intranasal corticosteroid. [1]
- The lamina papyracea is the paper-thin medial orbital wall of the ethmoid and the route of orbital spread. [3]
- The Chandler classification is preseptal cellulitis, orbital cellulitis, subperiosteal abscess, orbital abscess and cavernous sinus thrombosis. [3]
- The valveless diploic and emissary veins connect the sinuses, orbit and cavernous sinus and explain intracranial spread without a bony defect. [4]
- The intracranial complications are meningitis (commonest), epidural and subdural empyema, brain abscess, cavernous sinus thrombosis and Pott puffy tumour. [4] [5]
- Pott puffy tumour is osteomyelitis of the frontal bone with a subperiosteal abscess, a complication of frontal sinusitis in the older child. [5]
- Acute bacterial rhinosinusitis is a clinical diagnosis; routine imaging is not indicated unless a complication is suspected. [1]
- Contrast CT of the sinuses and orbits is the investigation for a suspected orbital or intracranial complication; MRI with venography for cavernous sinus thrombosis and brain abscess. [9] [11]
- A unilateral foul-smelling purulent nasal discharge in a child is a nasal foreign body until proven otherwise — never treat as sinusitis. [11]
References
- [1]Wald ER; Applegate KE; Bordley C; et al Clinical practice guideline for the diagnosis and management of acute bacterial sinusitis in children aged 1 to 18 years. Pediatrics, 2013.PMID 23796742
- [2]Chow AW; Benninger MS; Brook I; et al IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis, 2012.PMID 22438350
- [3]Chandler JR; Langenbrunner DJ; Stevens ER The pathogenesis of orbital complications in acute sinusitis. Laryngoscope, 1970.PMID 5470225
- [4]Jones NS; Walker JL; Bassi S; et al The intracranial complications of rhinosinusitis: can they be prevented? Laryngoscope, 2002.PMID 11802039
- [5]Giannoni C; Sulek M; Friedman EM Intracranial complications of sinusitis: a pediatric series. Am J Rhinol, 1998.PMID 9653474
- [6]Fokkens WJ; Lund VJ; Hopkins C; et al European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology, 2020.PMID 32077450
- [7]Ramadan HH Pediatric chronic rhinosinusitis. Eur Arch Otorhinolaryngol, 2024.PMID 37899371
- [8]Brietzke SE; Shin JJ; Choi S; et al Clinical consensus statement: pediatric chronic rhinosinusitis. Otolaryngol Head Neck Surg, 2014.PMID 25274375
- [9]Bedwell J; Bauman NM Management of pediatric orbital cellulitis and abscess. Curr Opin Otolaryngol Head Neck Surg, 2011.PMID 22001661
- [10]Lu NE; Gardiner LA; McCoy JL; et al Characteristics and management of pediatric medial subperiosteal orbital abscesses. Int J Pediatr Otorhinolaryngol, 2024.PMID 38852548
- [11]Oxford LE; McClay J Complications of acute sinusitis in children. Otolaryngol Head Neck Surg, 2005.PMID 16025049
- [12]Moreddu E; Rossi ME; Bellal D; et al Prognostic Factors of Pediatric Acute Ethmoidal Rhinosinusitis With Orbital Subperiosteal Abscess: A Retrospective Cohort Study. J Otolaryngol Head Neck Surg, 2025.PMID 40652356