Paeds · ent-hearing-and-oral-health
Ankyloglossia and infant feeding
Also known as Tongue-tie · Lingual frenulum restriction · Tongue-tie and breastfeeding · Posterior tongue-tie · Frenotomy for tongue-tie · Lingual frenectomy · Tongue-tie division · Tethered oral tissues and infant feeding
Fellowship topic on ankyloglossia (tongue-tie) and infant feeding — a congenital short, thick or tight lingual frenulum that tethers the underside of the tongue to the floor of the mouth and restricts tongue mobility. Covers the anterior-versus-posterior and structural-versus-functional classification (Coryllos type one to four, Kotlow free-tongue length, the Hazelbaker Assessment Tool for Lingual Frenulum Function and the TABBY picture tool); the biomechanics of the breastfeeding latch and how a restricted tongue fails to cup, elevate and form a peristaltic wave, causing nipple trauma, poor milk transfer, engorgement and mastitis; the estimated four to eleven percent prevalence with male predominance; the bedside and lactation assessment including observing a feed and testing protrusion, elevation, cupping and lateralisation; the principle of skilled lactation support before any decision to divide; the stepwise move through conservative support, validated assessment and frenotomy (sterile scissors or laser division) for the infant whose feeding difficulty persists; the randomised and systematic-review evidence on frenotomy and its limits; the complications of bleeding, oral ulceration and reattachment and the overdiagnosis and underdiagnosis pitfalls; and the regional guidance from NICE interventional procedures guidance one four nine, the AAO-HNS consensus and the Royal Children's Hospital Melbourne.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A first-time mother brings her ten-day-old baby to clinic in tears: feeds last an hour, the baby clicks and pulls off, he has regained no birth weight, and her nipples are cracked and bleeding. She has read online that he is tongue-tied and wants it snipped today. The fellowship skill is to hold both truths at once — that a tight lingual frenulum can genuinely sabotage a breastfeed, and that the answer is careful assessment and skilled lactation support before any decision to divide. [10]
Ankyloglossia, commonly called tongue-tie, is a congenital condition in which the lingual frenulum — the midline fold of mucosa that tethers the underside of the tongue to the floor of the mouth — is short, thick, tight or inelastic, restricting the tongue's range of movement. The key word is restriction: it is the loss of functional mobility, not the mere presence of a frenulum, that matters, which is why some visibly tight ties feed perfectly well while some barely visible posterior ties cause real difficulty. [9] [12]
What makes the topic examinable is the tension between how common the finding is and how contested its treatment has become. Tongue-tie is one of the commonest oral findings of the newborn, and rates of frenotomy have risen sharply over the past two decades, prompting genuine concern about overdiagnosis and overtreatment. The fellowship answer threads the needle: recognise the symptomatic tie, give breastfeeding its proper first place, use a validated assessment rather than a glance, divide the tie that is genuinely causing failure after conservative support, and exclude the mimics — above all the submucous cleft. [1] [10]
Classification
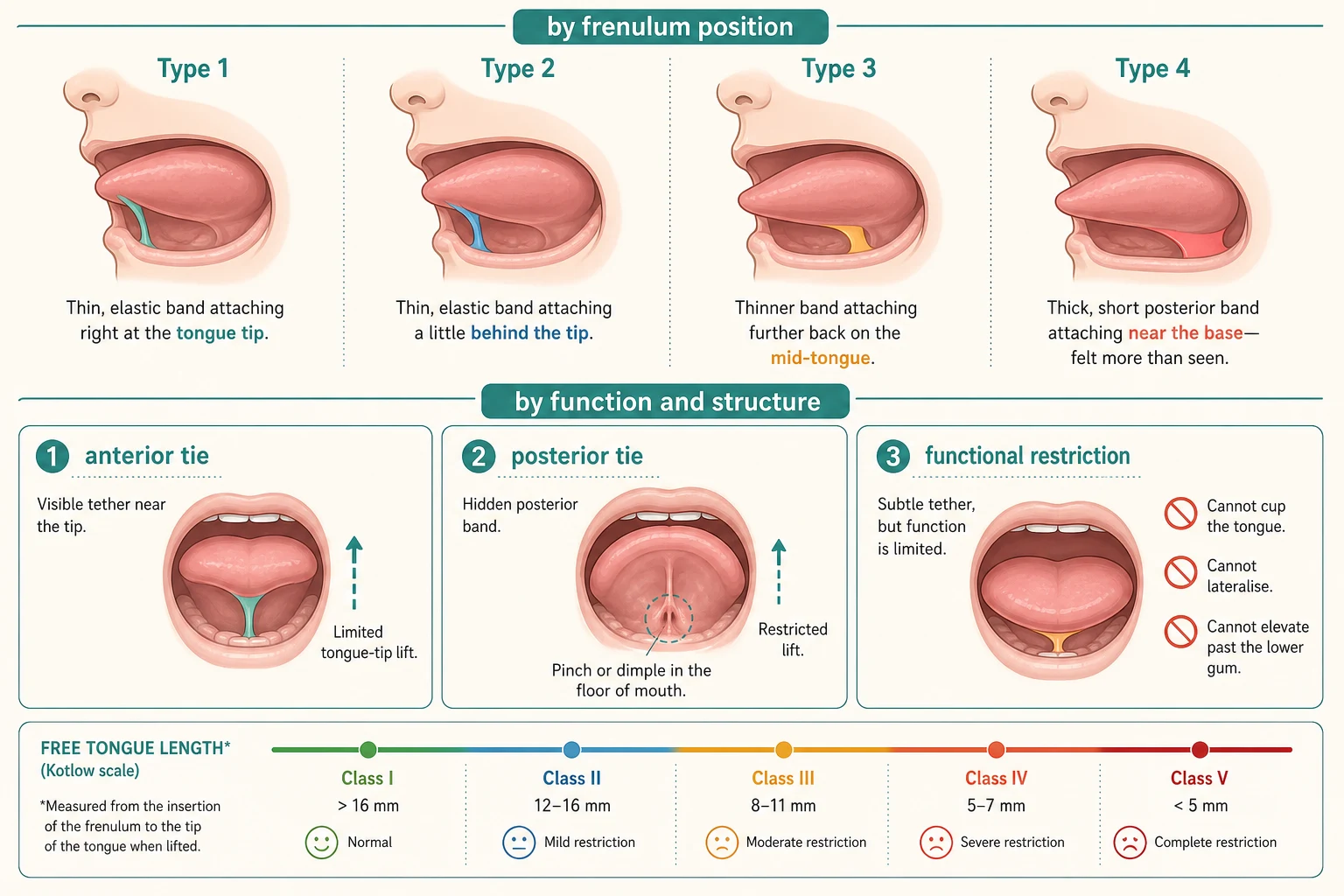
Classify tongue-tie by where the frenulum attaches and by what it does to tongue function, because the site predicts how easy it is to see and the function predicts whether it needs treatment. The two working splits are anterior versus posterior and structural versus functional. [9]
Ankyloglossia classified by frenulum position and function
The named descriptive schemes are the Coryllos type one to four (by where the frenulum inserts, from the tip back to the base) and the Kotlow free-tongue-length grading, which measures the unsupported length of tongue in front of the attachment. None of these appearance scores alone decides treatment. The functional instruments do: the Hazelbaker Assessment Tool for Lingual Frenulum Function (HATLFF) scores both appearance and function items, and the TABBY picture tool brings a simple, validated visual aid to the bedside. The classification that matters clinically is the last one — a tie is treated only when there is objective, function-limiting restriction causing feeding difficulty. [11] [12]
Epidemiology & Risk Factors
Tongue-tie is one of the commonest oral findings of the newborn, but its reported prevalence swings widely — most studies place it between four and eleven percent — because there is no single agreed definition and posterior ties are variably counted. A methodologic review found that the range collapses toward the lower end when stricter, function-based criteria are used. There is a consistent male predominance, often quoted around one and a half to three boys for every girl, and a familial tendency suggesting genetic influence. [8] [9]
The risk factor that actually matters is breastfeeding, because that is where restriction becomes symptomatic. The infants who present are breastfed babies whose latch cannot compensate, and the maternal risk factors are those that make a marginal latch fail — flat or inverted nipples, engorgement, primiparity and limited access to skilled support. Bottle-fed infants rarely present, because a bottle teat requires less tongue excursion, which is why a tongue-tie causing no feeding problem in a bottle-fed baby is generally left alone. [2] [12]
The social and access dimension is real. Families in remote, disadvantaged, Indigenous and migrant-background communities carry a heavier burden of undertreated breastfeeding difficulty through poorer access to lactation consultants and frenotomy services, and they also carry the opposite risk — of a procedure offered where watchful support would do. Equity in this topic means timely access to skilled lactation care for every breastfeeding dyad, with division reserved for the genuinely symptomatic. [10]
Pathophysiology
Why does a tight frenulum break a breastfeed when it barely affects a bottle-feed? The answer lies in the latch biomechanics, and it explains both the maternal nipple injury and the infant's poor milk transfer. [9]
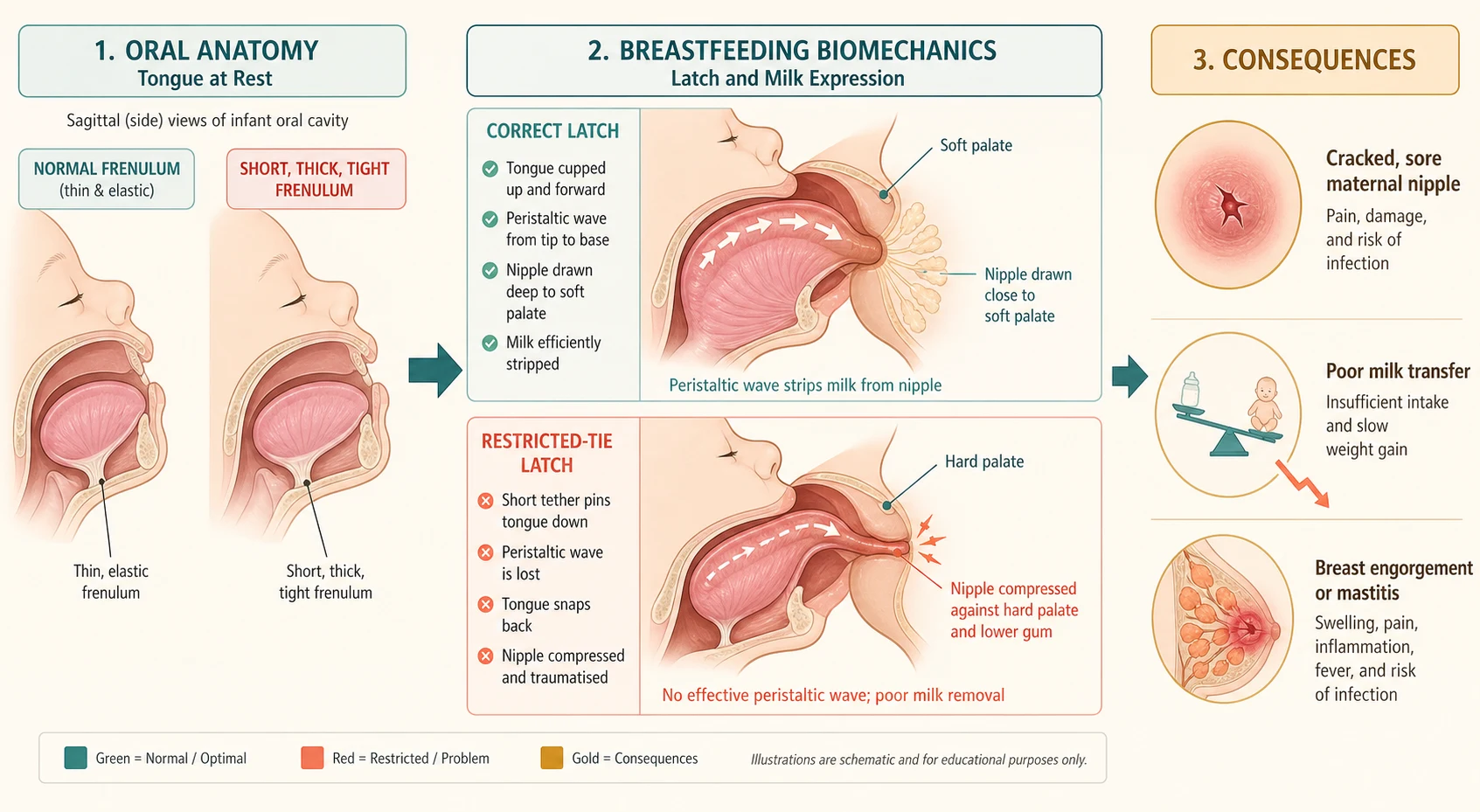
The lingual frenulum is a residual midline fold of oral mucosa. When it is short, thick or inelastic it tethers the tongue and limits four movements that breastfeeding demands — protrusion past the lower gum, elevation to and beyond the palate, cupping to cradle the breast, and lateralisation. To breastfeed well, an infant must bring the tongue forward over the lower gum, cup the underside of the breast and nipple, draw the nipple back to the junction of the hard and soft palate, and then drive a peristaltic wave from the tongue tip toward the base that strips milk from the lactiferous ducts while maintaining an airtight seal. A restricted tongue cannot complete this cycle. [2] [9]
When the tongue cannot cup and wave, two things happen. The infant compensates by chomping or gumming the nipple against the hard palate and lower gum, which traumatises the nipple — producing the classic compression stripe, cracks, bleeding and pain. Milk transfer falls because the peristaltic wave is weak or absent, so feeds are long and frequent, the baby clicks as the seal breaks, and weight gain lags. On the mother's side, incomplete emptying drives engorgement, blocked ducts and mastitis. The same biomechanics explain why a tight tie is often a feeding problem in the first weeks and may matter less as the infant grows and compensates. [12] [2]
Clinical Presentation
Read the tie through the feeding, because the presentation is almost always a breastfeeding story told by a distressed mother rather than an oral finding noticed on routine examination. [10]
The symptomatic infant cannot sustain a deep latch. Feeds are long and frequent, the baby clicks or loses suction, comes on and off the breast, and is unsettled and hungry soon after a feed. On the infant side the consequences are poor milk transfer and poor weight gain, and in the worst cases dehydration and a rising jaundice. The mother's story is the mirror image: nipple pain out of proportion to the latch, a compression stripe or crease across the nipple after a feed, cracked and bleeding nipples, and then engorgement, blocked ducts or mastitis from incomplete emptying. A mother who dreads every feed and is losing confidence in breastfeeding is a clinical signal, not a complaint to be reassured away. [2] [12]
The non-feeding presentation belongs to the older child and is more contested. Ankyloglossia has been blamed for speech articulation difficulties (particularly lingual sounds), dental and periodontal problems from inability to clear food, and mechanical limitations such as licking the lips or an ice-cream, or cleaning the teeth. The evidence linking tongue-tie to speech disorder is weak, and most children with a tie develop normal speech; the tie should not be assumed to explain a speech delay without assessment. [9] [12]
Differential Diagnosis
Build the differential around the symptom, because both poor latch and nipple pain have many causes besides tongue-tie, and treating a coincidental tie will not fix them. [2]
The commonest cause of nipple pain and poor latch is not a tongue-tie at all but suboptimal positioning and attachment. Before any frenulum is blamed, the feeding must be observed and the latch corrected by a skilled lactation consultant. Other infant contributors are prematurity with immature feeding coordination, neurological hypotonia, oral aversion, reflux with feeding avoidance, and nasal or nasopharyngeal obstruction that forces the baby to break the latch to breathe. A submucous cleft palate may present as a posterior tie with feeding difficulty and must be excluded before division. [12]
On the maternal side, nipple pain has its own differential: candidal (thrush) infection with shooting, burning pain and a pink shiny nipple; bacterial infection; Raynaud vasospasm of the nipple; eczema and contact dermatitis; and a milk bleb blocking a duct. Each of these can coexist with a tongue-tie, and each needs its own treatment. The protection is to assess the whole feeding dyad rather than anchor on the frenulum — a coincidental asymptomatic tie in a mother with candidal nipple thrush will not be cured by frenotomy. [10] [2]
Clinical & Bedside Assessment
Assessment is lactation-led and functional, and it begins with the feeding, not the mouth. The single most useful step is to observe a full feed — watching the latch, the position, the transfer, and the mother's face — because that is where the diagnosis lives and where most reversible causes are found. [10]
Take a focused feeding history: the quality of the latch, pain (site, severity, a compression crease), the pattern and length of feeds, clicking, the infant's weight trajectory, wet and dirty nappies, and any engorgement, mastitis or cracked nipples. Then examine the oral cavity: inspect the frenulum at rest and on lifting the tongue, looking for a short, thick or inelastic band and any bifid uvula or notched palate that would signal a cleft. Test the four functional movements — protrusion past the lower gum, elevation toward and onto the palate, cupping of the tongue, and lateralisation — looking for a heart-shaped or notched tip, a pinch or dimple at the floor of mouth, and a tongue that cannot sustain a wave. [11] [8]
Use a validated functional tool rather than a glance. The Hazelbaker Assessment Tool for Lingual Frenulum Function (HATLFF) scores both appearance and function, and the TABBY picture tool offers a simple, validated visual aid that supports consistent, teachable assessment. Score the infant, weigh and plot the weight, and re-examine after a trial of skilled lactation support — because the tie is treated only when the restriction is function-limiting and the difficulty persists despite good conservative care. [11] [12]
Investigations
Tongue-tie is a clinical diagnosis: there is no blood test, swab or imaging that confirms it, and the indication to treat rests on the functional assessment and the feeding history. Reserve laboratory testing for the failing infant — a weight, a capillary or serum bilirubin if jaundiced, and electrolytes if dehydrated — and for the mother with mastitis, who may need a milk culture only if not responding to first-line measures. [10] [12]
The one imaging consideration is the submucous cleft palate. A bifid uvula, a notched or grooved hard palate, or a zona pellucida in a baby labelled posterior tongue-tie should prompt referral to a cleft team and palatal assessment before any frenotomy, because the frenulum and surrounding tissue may be needed for later repair and division can distort the repair. Otherwise, investigation in tongue-tie means serial weight monitoring and feeding review, not scans. [12]
[10] [12]Management — Resuscitation
Most tongue-tie is managed electively, but the failing infant and the acutely unwell mother need prompt stabilisation before any decision about the frenulum. The infant who is dehydrated, losing weight, markedly jaundiced or unable to sustain a feed is treated as feeding failure: establish adequate intake with supplemental expressed breast milk or formula by cup, syringe, supply-line or bottle as appropriate, correct dehydration, and arrange urgent lactation support and paediatric review. [10]
The mother with acute mastitis or an abscess is managed in her own right — continued milk removal (feeding or expressing), analgesia, and antibiotics when there is systemic upset, spreading erythema or a bacterial infection, with surgical review if an abscess is suspected. Relieving the underlying milk stasis may require frenotomy once the infant can feed effectively, but the acute infection is treated first. Keeping the mother breastfeeding through the crisis — with skilled support, pumping to protect supply, and reassurance — is part of the resuscitation, because abandoning breastfeeding is rarely necessary and often preventable. [2] [12]
The principle is that division of a tie is elective, while dehydration, jaundice and mastitis are not. Stabilise the dyad, secure feeding and milk removal, and then make the frenotomy decision in the cold light of a full functional assessment rather than in the middle of an acute crisis. [10]
Management — Definitive & Stepwise
Once the dyad is stable, definitive management is a clear stepwise path whose first and most powerful step is conservative, and whose operative step is reserved for persistent, function-limiting restriction. [10]
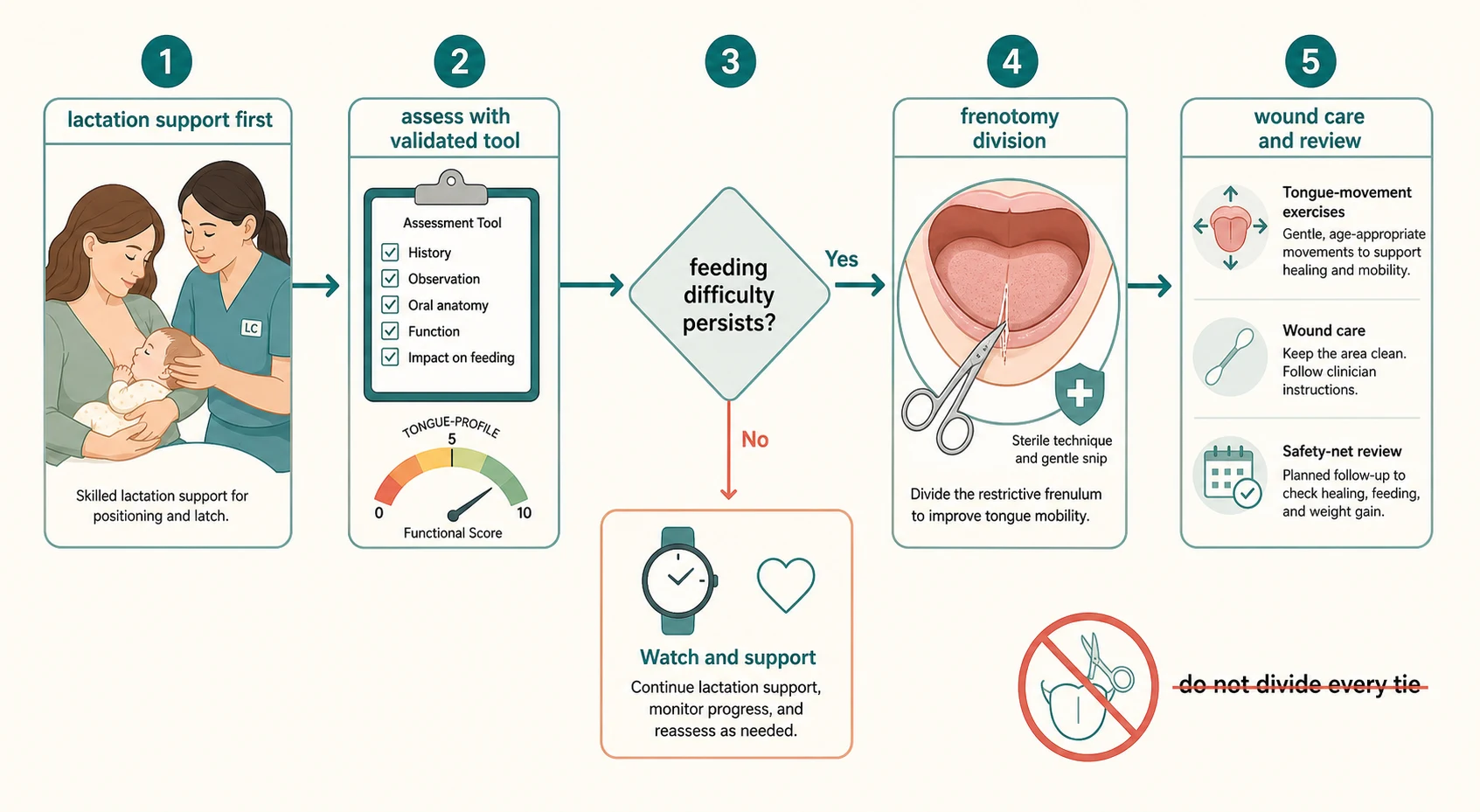
Stepwise management of ankyloglossia and infant feeding
Skilled lactation support first — observe a feed, correct positioning and attachment, manage engorgement and mastitis, and protect milk supply; many symptomatic babies settle with good support alone.
Functional assessment — score the tie with a validated tool (Hazelbaker HATLFF or TABBY), test protrusion, elevation, cupping and lateralisation, and exclude a submucous cleft palate.
Trial of conservative care — monitor weight and feeding over an adequate trial; reassure and continue support if feeding is effective and weight gain adequate.
Frenotomy for persistent difficulty — if function-limiting restriction and feeding difficulty persist despite good support, divide the frenulum with sterile scissors or laser, with appropriate consent and aftercare.
Post-procedure care and review — lactation support to re-establish the latch, gentle wound care and tongue-movement exercises, and a weight and feeding review to confirm improvement and watch for reattachment.
The operative step is frenotomy — division of the lingual frenulum — performed with sterile scissors or a laser, in the outpatient setting or at the bedside for a newborn, with or without local anaesthetic according to local practice and the infant's age. The technique divides the tight band to release the tongue, with careful attention to avoiding the submandibular (Wharton) duct orifices on either side of the frenulum. The United Kingdom's NICE interventional procedures guidance (IPG149) considers division of tongue-tie a safe procedure that is efficacious for breastfeeding in suitably selected infants, and may be performed without anaesthetic in young infants. [12]
The evidence for frenotomy is encouraging but bounded. A Cochrane review concluded that frenotomy may reduce maternal nipple pain, but found limited and low-certainty evidence for its effect on infant breastfeeding outcomes. Individual randomised trials — by Buryk, Berry and colleagues, and Emond's Bristol team — showed short-term improvements in maternal pain and breastfeeding measures after division, and a trial of posterior tongue-tie reported objective improvement after frenotomy. A recent meta-analysis found frenotomy associated with improved breastfeeding outcomes. The honest synthesis is that frenotomy helps the genuinely symptomatic infant but offers little where the tie is not the problem, which is exactly why selection matters. [1] [3] [4] [5] [6] [7]
Specific Subtypes & Scenarios
The scenarios below are the ones examiners reach for, because each forces a different judgement about when to divide and when to wait. [10]
A classic anterior tongue-tie with significant feeding difficulty is the clearest case. A short frenulum at the tongue tip, a painful clicking latch, cracked nipples and poor weight gain that persist despite skilled positioning. Here the answer is frenotomy after a trial of conservative support, with lactation follow-up to rebuild the latch. The benefit is well supported and the diagnosis is secure. [3] [4]
A suspected posterior tongue-tie is the contested case. The diagnosis is harder — the band is felt more than seen — and overdiagnosis is common, so an experienced assessor and a functional tool are essential. If objective restriction and persistent feeding difficulty are confirmed, division can help, as shown in a randomised trial of posterior ties; if not, watchful support is correct. The skill is to resist dividing on appearance alone. [6] [10]
A mild tie with good feeding is the reassurance case. A visible frenulum with a deep, painless, effective latch and normal weight gain needs no intervention — reassure the family, support breastfeeding, and monitor growth. This is also the case that protects against overdiagnosis: a tie that is not function-limiting is not treated. [9] [12]
An older child with a tie and speech or mechanical concerns is the referral case. Speech delay should prompt a hearing assessment and speech-language review before any frenulum is blamed, because the link between tongue-tie and speech disorder is weak. Refer to a specialist cleft, ENT or oral team for a considered plan rather than offering division for an unproven indication. [12] [9]
Complications & Pitfalls
The complications of frenotomy are usually minor but real, and the pitfalls are mostly about judgement — dividing too readily or not readily enough. [12]
Procedural complications include minor bleeding (the most common, usually settling with pressure), infection (rare), oral ulceration or aphthous-type sores where the wound rubs, and injury to the submandibular (Wharton) ducts if the cut strays laterally. Reattachment — healing of the divided ends back together with recurrent restriction — is a recognised late failure that may require revision or post-procedure exercises to prevent. Serious complications such as significant haemorrhage or damage to deeper structures are rare but described, which is why the procedure is done by trained practitioners with consent and aftercare. [12] [1]
The overdiagnosis pitfall is the dominant one of the modern era. Rates of frenotomy have risen sharply, driven in part by the internet and by the legitimate rise of lactation awareness, and many ties are now divided that are not function-limiting — exposing infants to procedural risk for no benefit and undermining confidence in breastfeeding. The protection is the principle of persistent, function-limiting restriction after conservative support: a tie is treated for what it does, not how it looks. [10] [1]
The underdiagnosis pitfall is its mirror. A genuine posterior tie can be missed because it is felt rather than seen, leaving a mother with months of painful feeding, cracked nipples and recurrent mastitis and an infant who fails to thrive. Missing the diagnosis delays relief that frenotomy reliably provides. The protection is to reassess tongue mobility functionally in any mother with persistent painful feeding, and to involve a lactation consultant early. [2] [6]
The mimic pitfall is treating a coincidental tie for the wrong diagnosis. A submucous cleft palate, candidal nipple thrush, Raynaud vasospasm, or simply poor attachment can all coexist with a visible frenulum; dividing the tie will not cure them. The protection is to assess the whole feeding dyad and treat each problem on its own merits. [12] [10]
Prognosis & Disposition
The prognosis is excellent when the right infants are selected: most breastfed babies with a genuinely symptomatic tongue-tie improve promptly with skilled support and, where needed, frenotomy, and most ties that cause no problem are simply outgrown or compensated for as the child matures. [10] [12]
Discharge and monitor the asymptomatic or mildly symptomatic tie with effective feeding and normal weight gain — support breastfeeding, plot the weight, and give a clear safety-net to return for poor weight gain, painful feeding or mastitis. Manage in the outpatient lactation clinic the symptomatic tie, with a trial of conservative support and a functional assessment, and proceed to frenotomy in the suitable setting if difficulty persists. [10]
Admit or escalate the rare failing infant with dehydration or jaundice and the mother with acute mastitis or abscess — these are the cases where the feeding crisis, not the frenulum, drives the disposition. The durable interventions — skilled lactation support, validated assessment, conservative care first, and judicious frenotomy — keep most dyads breastfeeding and out of hospital. [2] [12]
Special Populations
Premature infants carry a double burden of feeding immaturity and, sometimes, a tongue-tie; assessment must distinguish the contribution of prematurity from that of restriction, and division is weighed against the infant's stability and corrected age. A conservative, lactation-led approach, with frenotomy only for clear persistent difficulty, is the safe default. [12]
The infant with a cleft or suspected submucous cleft palate needs the frenulum left intact and referred to the cleft team. Division near a cleft can compromise later repair, and a posterior tie here may be part of the anomaly rather than a separate problem — exclude the cleft before any cut. [12]
Aboriginal and Torres Strait Islander, Maori, Pasifika, refugee, asylum-seeking and migrant families, and families in remote and disadvantaged communities, deserve equitable access to skilled lactation consultation and frenotomy, delivered with cultural safety and trained interpreters. Breastfeeding has particular cultural and health significance in these communities, and the unequal access to lactation support is itself a driver of both undertreated difficulty and inappropriate division. Telehealth lactation support can extend reach to families far from services. [10]
Families of infants with disability or feeding aversion may face a tie superimposed on complex feeding needs; a coordinated feeding-team assessment, rather than a procedural shortcut, protects these infants from both over- and under-treatment. The guiding principle across all groups is the same: assess the feeding, support the latch, and divide only for persistent function-limiting restriction. [12] [10]
Evidence, Guidelines & Regional Differences
The named regional guidance is the AAO-HNS Clinical Consensus Statement: Ankyloglossia in Children, the NICE Interventional Procedures Guidance (IPG149) on division of tongue-tie for breastfeeding, and the Royal Children's Hospital Melbourne tongue-tie fact sheet. NICE IPG149 judges the procedure safe and efficacious for breastfeeding in suitably selected infants and notes it may be performed without anaesthetic in young infants, while the AAO-HNS consensus addresses diagnosis, assessment and the decision to operate across the age range. [12]
The frenotomy evidence is the heart of the topic. The Cochrane review by O'Shea and colleagues found that frenotomy may reduce maternal nipple pain but provided only low-certainty evidence for infant breastfeeding outcomes. Individual randomised controlled trials — Buryk (neonatal release), Berry (a double-blind trial of immediate division) and Emond (early frenotomy for mild–moderate ties) — reported short-term improvements in maternal pain and breastfeeding measures, and Ghaheri showed objective improvement after frenotomy for posterior tongue-tie. A recent meta-analysis by Cordray and colleagues found frenotomy associated with improved breastfeeding outcomes. The synthesis is that the genuinely symptomatic infant benefits, while the asymptomatic tie does not. [1] [3] [4] [5] [6] [7]
The controversy is real and examinable. Rising frenotomy rates, the contested diagnosis of posterior tongue-tie, internet-driven demand, and the difficulty separating the tie's effect from that of skilled lactation support all fuel overdiagnosis, while the genuine morbidity of an untreated symptomatic tie fuels underdiagnosis. The balance is struck by validated assessment, conservative support first, and division reserved for persistent, function-limiting restriction. [10] [1]
[12] [1]Exam Pearls
Ankyloglossia is a feeding problem first and a procedure second. The tie is a short, thick or tight lingual frenulum that restricts tongue mobility, affects an estimated four to eleven percent of newborns, and becomes symptomatic when it breaks the latch — compressing the nipple, dropping milk transfer, and driving maternal pain, engorgement and mastitis. [8] [9]
The skill is the balance. Skilled lactation support comes first, and most symptomatic babies settle with good positioning and attachment. For the infant whose function-limiting restriction and feeding difficulty persist, frenotomy — sterile scissors or laser division — reduces maternal nipple pain and improves breastfeeding measures, with the evidence supporting its use in genuinely symptomatic ties. The Cochrane review's caution on infant outcomes and the rising rates of division together warn against treating appearance rather than function. [1] [10]
The red flags are the failing infant (dehydration, jaundice, poor weight gain), the mother with acute mastitis, and the submucous cleft palate that must be excluded before any cut. The pitfall is overdiagnosis — dividing ties that are not function-limiting — alongside its mirror of missing a genuine posterior tie. The fellowship answer threads it all: assess the feeding, support the latch, use a validated tool, exclude the cleft, and divide only for persistent, function-limiting restriction. [12] [2]
References
- [1]O'Shea JE; Foster JP; O'Donnell CP; et al Frenotomy for tongue-tie in newborn infants. Cochrane Database Syst Rev, 2017.PMID 28284020
- [2]Francis DO; Krishnaswami S; McPheeters M Treatment of ankyloglossia and breastfeeding outcomes: a systematic review. Pediatrics, 2015.PMID 25941303
- [3]Buryk M; Bloom D; Shope T Efficacy of neonatal release of ankyloglossia: a randomized trial. Pediatrics, 2011.PMID 21768318
- [4]Berry J; Griffiths M; Westcott C A double-blind, randomized, controlled trial of tongue-tie division and its immediate effect on breastfeeding. Breastfeed Med, 2012.PMID 21999476
- [5]Emond A; Ingram J; Johnson D; et al Randomised controlled trial of early frenotomy in breastfed infants with mild-moderate tongue-tie. Arch Dis Child Fetal Neonatal Ed, 2014.PMID 24249695
- [6]Ghaheri BA; Lincoln D; Mai TNT; Mace JC Objective Improvement After Frenotomy for Posterior Tongue-Tie: A Prospective Randomized Trial. Otolaryngol Head Neck Surg, 2022.PMID 34491142
- [7]Cordray H; Raol N; Mahendran GN; et al Quantitative impact of frenotomy on breastfeeding: a systematic review and meta-analysis. Pediatr Res, 2024.PMID 37608056
- [8]Segal LM; Stephenson R; Dawes M; Feldman P Prevalence, diagnosis, and treatment of ankyloglossia: methodologic review. Can Fam Physician, 2007.PMID 17872781
- [9]Lalakea ML; Messner AH Ankyloglossia: does it matter? Pediatr Clin North Am, 2003.PMID 12809329
- [10]Power RF; Murphy JF Tongue-tie and frenotomy in infants with breastfeeding difficulties: achieving a balance. Arch Dis Child, 2015.PMID 25381293
- [11]Ingram J; Copeland M; Johnson D; Emond A The development and evaluation of a picture tongue assessment tool for tongue-tie in breastfed babies (TABBY). Int Breastfeed J, 2019.PMID 31346346
- [12]Messner AH; Walsh J; Rosenfeld RM; et al Clinical Consensus Statement: Ankyloglossia in Children. Otolaryngol Head Neck Surg, 2020.PMID 32283998