Paeds · ent-hearing-and-oral-health
Dental caries, enamel disease and oral-health prevention
Also known as Early childhood caries · Nursing caries · Baby-bottle tooth decay · Severe early childhood caries · Dental decay · Molar-incisor hypomineralisation · Amelogenesis imperfecta · Dental fluorosis
Fellowship topic on dental caries, developmental enamel disease and oral-health prevention in children. Covers dental caries as the commonest chronic disease of childhood and a biofilm-mediated, sugar-driven, dynamically demineralising disease; the AAPD case-definition of early childhood caries (ECC) and its severe form; the Streptococcus mutans ecological-plaque pathophysiology, the demineralisation-remineralisation cycle and the critical pH of about 5.5 for enamel; the fluoride, diet and dental-home prevention pillars with age-specific fluoride toothpaste guidance, fluoride varnish and silver diamine fluoride; the developmental enamel defects differential of molar-incisor hypomineralisation, amelogenesis imperfecta and fluorosis; the emergency recognition of spreading odontogenic infection; and the ANZ, UK, US and Canadian guidance on community water fluoridation and supervised toothbrushing.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A two-year-old is brought in for a check, and the mother mentions his front teeth are "going brown" since he falls asleep each night with a bottle of sweetened milk. That sentence carries the whole topic: a biofilm disease driven by sugar and a vulnerable host, advancing silently until it is painful, and preventable if the family had been given the fluoride and feeding messages at the right age. The fellowship skill is to recognise caries as a dynamic, reversible-then-irreversible disease, to know its developmental mimics, and to deliver the prevention that works. [6] [8]
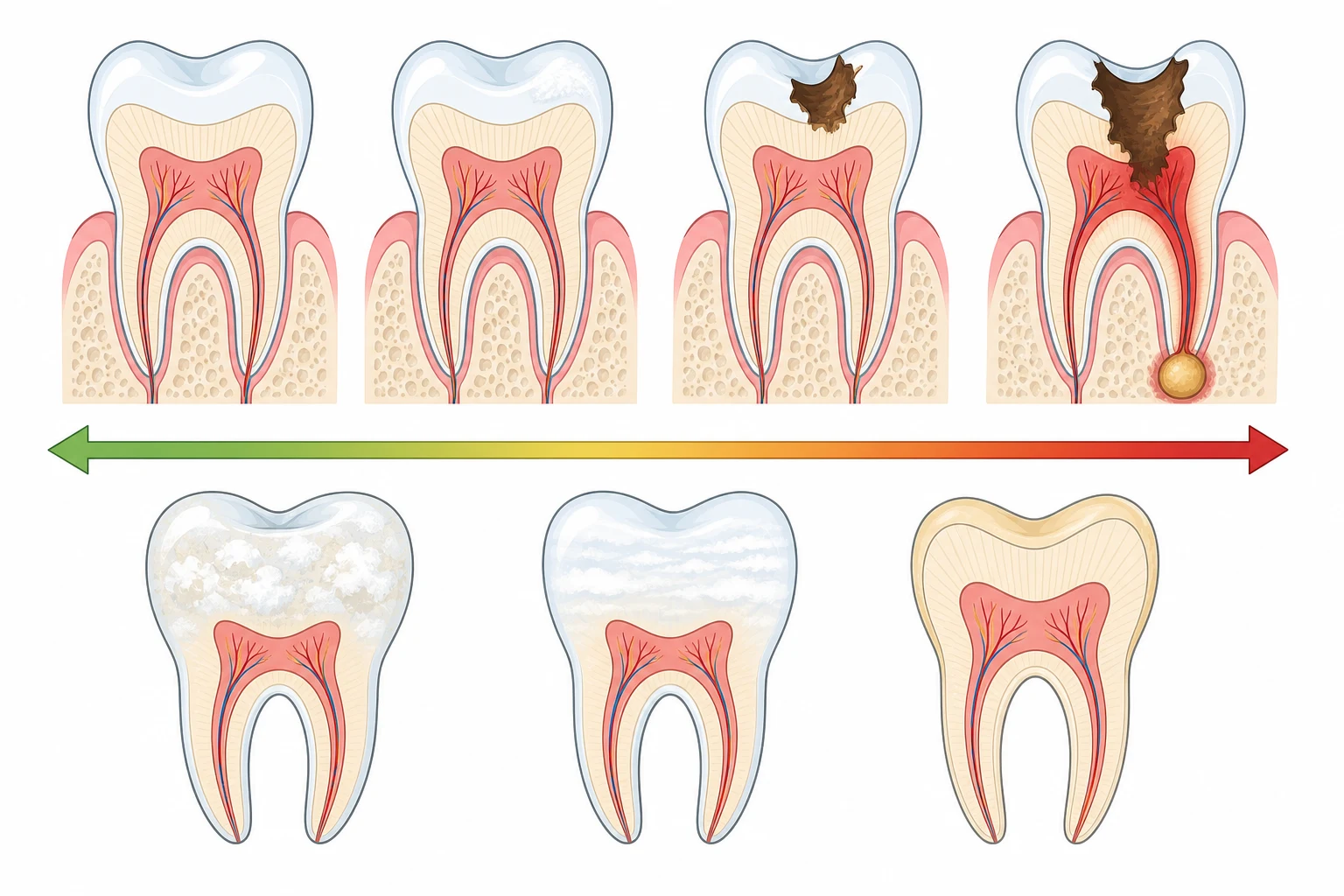
Dental caries is the localised destruction of the hard dental tissues by the acid by-products of bacterial fermentation of dietary carbohydrate. It is not a static hole but a dynamic balance — a demineralisation-remineralisation cycle — that tips toward cavitation when acid attack outstrips repair. Early in the cycle the lesion is a reversible white spot where mineral has been lost from beneath an intact surface; once the surface collapses the lesion cavitates and is no longer self-limiting. This reversibility is the single most important concept, because it is why prevention and early fluoride work. [7] [8]
The paediatric entity is early childhood caries (ECC). The American Academy of Pediatric Dentistry defines ECC as the presence of one or more decayed (d), missing (m) or filled (f) primary tooth surfaces (s) — a dmfs/dmft of one or more — in a child 71 months of age or younger. Its severe form (severe ECC) is defined by age-specific thresholds: any smooth-surface caries in a child under three years, cavitated or filled smooth surfaces of the maxillary anterior primary teeth at ages three to five, or a dmfs of four or more at age three, five or more at age four, or six or more at age five. What examiners reward is the recognition that ECC is a disease of pattern and age, not just a count of holes. [6] [7]
The topic deliberately separates acquired caries from developmental enamel disease. Molar-incisor hypomineralisation, amelogenesis imperfecta, enamel hypoplasia and fluorosis are defects of how enamel was formed, not how it is being dissolved, and they are managed differently — the defect is permanent, and the priority is protection, sensitivity control and staged restoration rather than fluoride-driven remineralisation of an intact surface. [10] [11]
Classification
Caries is classified along two axes that drive management: how deep it goes, and where it sits. A white-spot lesion confined to enamel is reversible; a lesion into dentine has cavitated and needs operative care; a lesion into the pulp causes pulpitis and periapical abscess. By surface, pit-and-fissure caries of the occlusal molar grooves is the commonest site, while smooth-surface caries — especially the maxillary anterior primary teeth bathed in a nocturnal bottle — is the hallmark of early childhood caries. [7] [8]
Classifying the hard-tissue disease of childhood teeth
The classification does more than label — it sets the management. The first two are acquired and fluoride-responsive: the white spot can remineralise, the cavity needs a filling but the rest of the mouth still needs prevention. ECC is the acquired disease of the very young and is the target of the varnish and toothpaste programmes. The last three are developmental and permanent: the enamel was made wrongly or made too little, so the work is protection of what is fragile and staged restoration of what is lost, not remineralisation of an intact surface. [10] [11]
Epidemiology & Risk Factors
Untreated caries in the primary teeth is the single most prevalent disease of childhood worldwide. The Global Burden of Disease 2017 analysis found untreated caries in the primary dentition to be the most common of all human conditions in children, affecting over half a billion, and the 2021 update confirmed oral disorders remain among the dominant causes of non-fatal health loss across childhood. The burden is neither random nor evenly shared — it is concentrated in the disadvantaged. [8] [9]
The risk factors for early childhood caries cluster into a familiar story of sugar, frequency and vulnerability. A 2022 systematic review confirmed the strongest and most consistent predictors: frequent intake of free sugars, nocturnal bottle- or breastfeeding without oral hygiene, low family income and education, enamel hypoplasia, and high maternal caries experience (the mother is the principal source of the child's colonising Streptococcus mutans). Early colonisation by these acidogenic bacteria, before the teeth have matured, is what sets a child on a high-risk trajectory for life. [6] [7]
The burden falls hardest on the children least able to bear it. Indigenous, remote and migrant communities, children in out-of-home care and those with special healthcare needs carry a disproportionate share of severe ECC, driven by poverty, limited access to fluoridated water and dental care, and the legacy of sugary early feeding. The protective factors are the mirror image: optimally fluoridated water, a fluoride toothpaste used correctly, fissure sealants, and a dental home established in the first year of life. [3] [8]
Pathophysiology
Why does a tooth dissolve, and why does fluoride stop it? The answer is a dynamic equilibrium between an acid-producing biofilm and a mineral-rich tooth, played out at a pH threshold. [7]
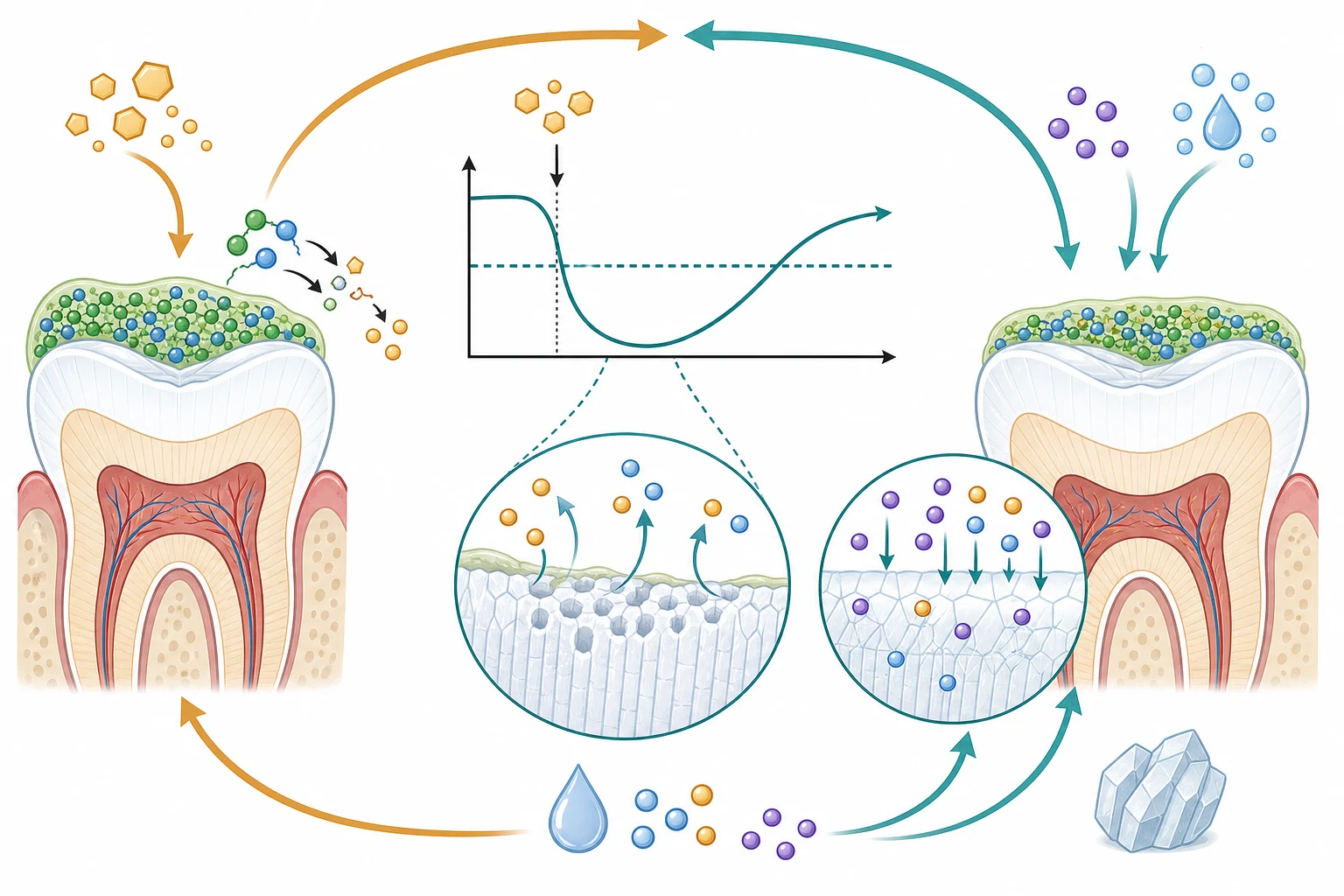
The healthy tooth is bathed in saliva, which is supersaturated with calcium and phosphate and bathes the enamel in a repairing film. Sitting on the enamel is the dental plaque biofilm — a structured community that, in health, is relatively benign. Caries begins when the biofilm becomes dysbiotic and acidogenic: frequent sugar lets acid-tolerant species, especially Streptococcus mutans but also Lactobacillus and Actinomyces, dominate. Every time sugar enters the mouth these bacteria ferment it to acid within minutes, and the plaque pH plunges — the fall and slow recovery is the Stephan curve. [7]
Demineralisation is governed by a single number, the critical pH of about 5.5 for enamel (dentine is more soluble and dissolves nearer 6.5). When the plaque pH drops below about 5.5, the saliva is no longer supersaturated relative to enamel, and calcium and phosphate leave the tooth — this is demineralisation. As the pH climbs again over the next half-hour, minerals return — remineralisation. Caries is the cumulative result of tipping that balance toward demineralisation: too many sugar hits, too little fluoride and saliva, and the white spot deepens until the enamel surface collapses into a cavity. Once into dentine, the softer tissue dissolves faster, and the lesion runs toward the pulp. [7] [8]
Fluoride interrupts this cycle at three points, and that is the whole rationale for fluoride toothpaste and varnish. It inhibits demineralisation by binding to the enamel surface and holding the crystal together; it enhances remineralisation by drawing calcium and phosphate back into a harder, more acid-resistant crystal called fluorapatite; and at high concentration it reduces the bacteria's acid production. The practical consequence is concentration-dependent — a fluoride toothpaste of 1000 parts per million or more is significantly more effective than the lower-strength children's pastes, which is why modern guidance shifted away from low-fluoride toothpastes for the young. [2] [1]
Clinical Presentation
Read the mouth the way the history tells you to — a young child with brown upper front teeth and a bedtime bottle has ECC; a six-year-old with a single sensitive, chalky molar has a developmental defect. [6]
The earliest sign of caries is the painless white-spot lesion — a chalky, matte opacity where the enamel has lost subsurface mineral but the surface is still intact and can remineralise. With continued acid attack it turns brown, then cavitated, the soft dentine exposed. At this stage the child may complain of pain on sweet, hot or cold stimuli that settles when the stimulus goes — reversible pulpitis. Once the pulp is infected the pain becomes spontaneous and throbbing, keeps the child awake, and signals irreversible pulpitis; a necrotic pulp may then form a periapical abscess, seen as a gingival swelling or a draining pustule on the gum (a parulis). [7] [8]
Early childhood caries has a characteristic pattern the examiner expects you to name: white-spot and then cavitated lesions of the maxillary anterior primary teeth — the upper front teeth bathed in the nocturnal bottle — followed by decay of the occlusal surfaces of the first primary molars, and later the second molars as the child grows. The lower anterior primary teeth are typically spared because they sit under the tongue and are bathed in saliva. A young child with decayed, brown or missing upper front teeth has ECC until proven otherwise. [6] [7]
The presentation that must not be missed is the spreading odontogenic infection. A necrotic tooth seeds a periapical abscess that can track into the facial, buccal or submandibular spaces, producing facial swelling, fever, trismus, dysphagia or dyspnoea — an emergency that can compromise the airway, especially in a young child. A draining sinus on the gum of a primary molar is the quiet version of the same process. Developmental enamel defects present differently: MIH shows chalky, demarcated opacities (white, cream, yellow or brown) on the first permanent molars, often with the incisors, with the affected enamel brittle and sensitive; amelogenesis imperfecta shows thin, discoloured or soft enamel across most or all the teeth; and fluorosis shows fine white mottling in its mild form and brown pitting when severe. [8] [11]
Differential Diagnosis
Build the differential around the single most important distinction — an acquired lesion (caries) versus a developmental defect of enamel — then strip out the mimics of each. [10]
The first fork is between active caries and the developmental enamel defects. Caries tracks the plaque-retentive sites (molar pits and fissures, the interproximal surfaces, the maxillary anterior teeth in ECC) and progresses. Molar-incisor hypomineralisation gives sharply demarcated opacities of the first permanent molars (erupting around age six) and the incisors, in a child whose other teeth are normal — the hallmark is the asymmetry and the specific teeth affected. Amelogenesis imperfecta is pan-dental and often familial; fluorosis is bilaterally symmetrical mottling in a child from a high-fluoride water area. The decisive question is whether the enamel was formed wrongly (developmental, permanent) or is being dissolved (caries, progressive). [10] [11]
The non-caries mimics of tooth damage include erosion from dietary acid (citrus, carbonated drinks) or gastric acid in gastro-oesophageal reflux and eating disorders, producing smooth, saucer-shaped loss of enamel without the soft, stained base of caries; extrinsic staining (iron, chlorhexidine) that wipes the surface but does not breach it; and dental trauma, which fractures or displaces a tooth rather than dissolving it and is covered in the dental-trauma topic. Aphthous or herpetic ulceration, teething discomfort and eruptive pain can mimic dental pain but have their own mucosal or eruptive signature on examination. [8] [11]
When a child presents with facial swelling, the urgent differential is the source of the infection. An odontogenic abscess points to a tender, mobile or discoloured tooth with a gingival swelling or sinus; a periorbital cellulitis sits beside the eye, often from skin or sinus origin; and a salivary or lymph-node swelling has its own anatomical logic. The trap is attributing a spreading facial cellulitis to a skin cause when the engine is a necrotic molar — examine every tooth in a child with unexplained facial swelling. [8] [9]
Clinical & Bedside Assessment
Start with the history, because the feeding story usually names the disease. Ask about nocturnal bottle or breastfeeding, what goes in the bottle (milk, juice, sweetened drinks), the frequency of sugary foods and drinks, toothbrushing habits (who brushes, how often, what toothpaste), fluoride exposure (water supply, supplements), and any maternal caries history. In a child with pain, characterise it — provoking stimuli, spontaneity, sleep disturbance — and ask the red-flag questions of swelling, fever, and difficulty swallowing or breathing. [6]
Examine the mouth systematically, with the child's head supported and a good light: the lips, buccal mucosa, tongue, floor of mouth, palate and gingivae, then each tooth surface, lifting the lip away to see the maxillary anterior teeth where ECC declares itself. Look for the white-spot lesions, brown discolouration, cavitation, gingival swelling or a draining sinus, and chart decayed, missing and filled surfaces using the dmfs/dmft index for the primary dentition (DMFT for the permanent dentition). The ICDAS system codes the visual severity of each lesion from an intact first-visible sign through extensive cavitation, and is the standard for coded caries assessment. Note any developmental defect by its distribution — the symmetric mottling of fluorosis versus the asymmetric, molar-and-incisor pattern of MIH. [7] [8]
Assess caries risk at the bedside using the American Academy of Pediatric Dentistry Caries-risk Assessment Tool (CAT) or CAMBRA, which stratify a child into low, moderate or high risk from the caries experience, the fluoride exposure, the diet, the family's caries history and the clinical findings. The risk level sets the recall interval, the fluoride varnish frequency and the decision to radiograph — it turns a screening examination into a preventive plan. Always look specifically for the red-flag signs of spreading infection — facial or cervical swelling, trismus, dysphagia, dyspnoea and systemic toxicity — because these change the disposition from routine to emergency. [6] [8]
Investigations
Most dental caries is diagnosed clinically — the role of investigation is to find the hidden interproximal lesion, to stratify risk, and to work up the spreading infection. [8]
Dental radiographs are selective, not routine, and guided by caries risk and the stage of dental development. Bitewings detect the interproximal decay that is invisible to the eye and are taken at intervals set by risk — more often for high-risk children, less often for low. A panoramic radiograph surveys the developing dentition, eruption and any pathology. The principle is the principle of all radiography: image only when it will change management, and at the lowest dose. Intra-oral and panoramic dental imaging are performed and interpreted in primary dental care. [8] [9]
Caries-risk assessment (AAPD CAT, CAMBRA) is itself the key "investigation" of paediatric dentistry — it identifies the child who needs intensive fluoride, frequent recall and dietary intervention, and it is repeated as circumstances change. For the child with a spreading odontogenic infection, the work-up changes scale: a full blood count and C-reactive protein to gauge severity and systemic involvement, blood glucose where indicated, and facial and dental imaging — a panoramic or facial radiograph, and computed tomography where a deep-space infection, abscess or airway compromise is suspected. [8] [9]
[8]Management — Resuscitation
The only manifestation of dental caries that needs resuscitation is the spreading odontogenic infection, and the resuscitation mindset is "airway first, then source control". The child with an uncomplicated cavity needs no resuscitation — start definitive prevention and restorative care. [8]
Recognise the threat from the red flags: facial, submandibular or cervical swelling with trismus, dysphagia or dyspnoea in a child with a painful tooth. Assess and secure the airway first — a deep-space infection can obstruct a young child's airway frighteningly fast. Establish intravenous access, give analgesia, and start intravenous antibiotics with anaerobic cover — a common choice is amoxicillin with clavulanate, or clindamycin in penicillin allergy — and refer urgently to dental or maxillofacial surgery for imaging, drainage and extraction or root-treatment of the source tooth. Involving the surgeon early is part of the resuscitation, not a later step. [8] [9]
For acute dental pain without spreading infection, analgesia is the immediate measure: paracetamol 15 mg per kilogram (maximum 1 g) and ibuprofen 5 to 10 mg per kilogram (maximum 400 mg) every six to eight hours, with a clear safety-net to return for facial swelling, difficulty swallowing or breathing, or uncontrolled pain. Severe early childhood caries with pain, infection or failure to thrive is urgent rather than routine — arrange prompt dental review. The key principle is to separate the airway-threatening infection, which is an emergency, from the cavity, which is a planned dental problem. [8] [9]
Management — Definitive & Stepwise
Once the risk is stratified, the management of dental caries is prevention-led, fluoride-centred and stepwise, with non-operative measures for the reversible lesion and restorative care for the cavity. [2]
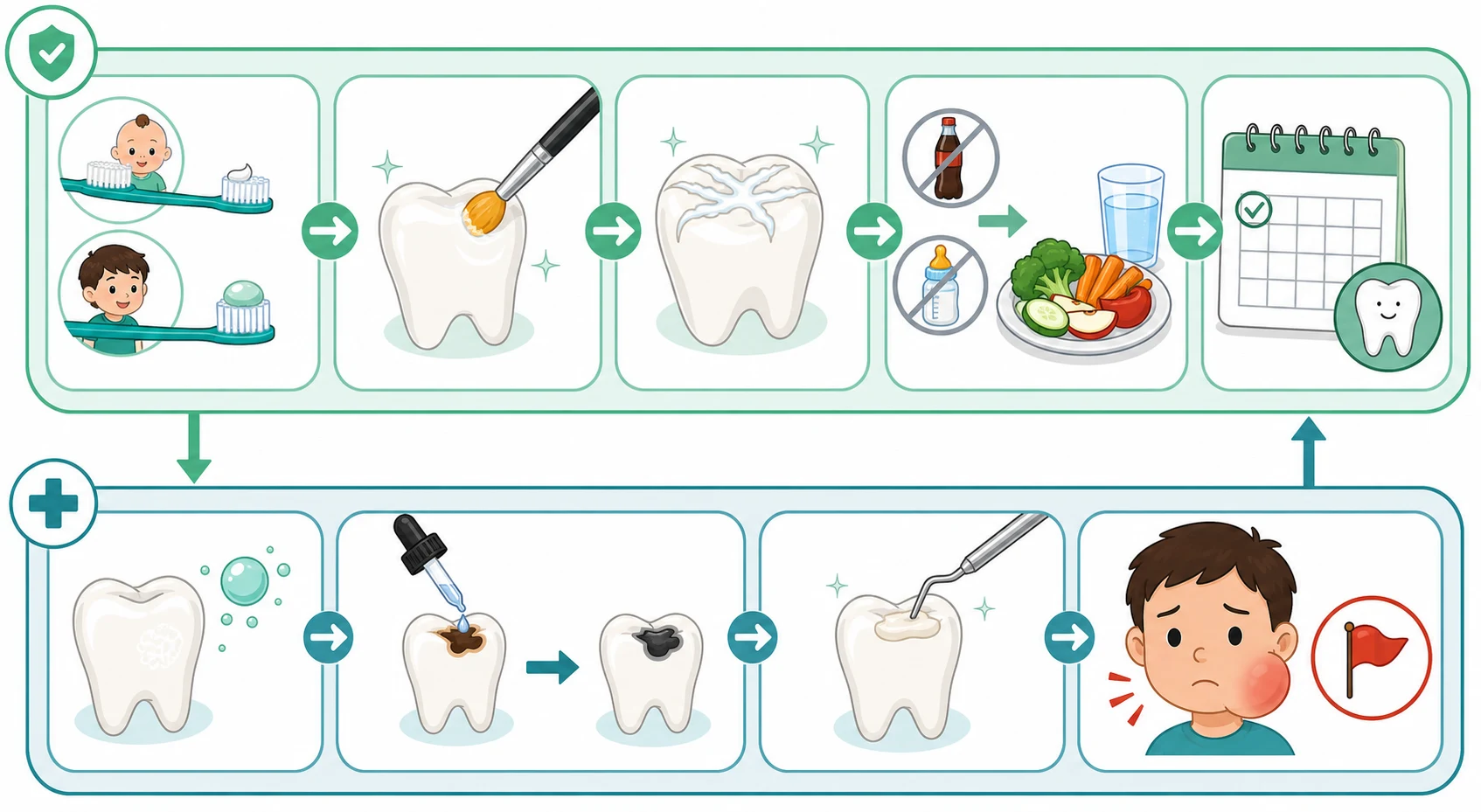
The stepwise prevention and management of childhood dental caries
Twice-daily brushing with a fluoride toothpaste of at least 1000 parts per million — a rice-grain smear under three years, a pea-sized amount from three to six years, and a full strip of 1350 to 1500 parts per million from six years; supervise until around seven to eight years, and spit, do not rinse.
Diet — reduce the frequency of free sugars, avoid a sugary bottle in bed, keep sugary drinks to mealtimes, and favour water and milk; aim for free sugars below 10 percent of energy intake, ideally below 5 percent.
Fluoride varnish — apply 5 percent sodium fluoride varnish (22600 parts per million) two to four times a year to the primary teeth of children at moderate or high caries risk; the USPSTF recommends varnish from tooth eruption through age five.
Fissure sealants — place a resin sealant in the deep pits and fissures of the permanent molars soon after eruption for children at elevated risk.
Establish a dental home by the first birthday, and set the recall interval by caries risk — three to six months for high risk, six to twelve months for low risk.
For established caries — non-operative remineralisation of the white spot, silver diamine fluoride to arrest a cavity, restorative care for the cavitated lesion, and theatre-based comprehensive care under general anaesthesia for extensive early childhood caries.
The evidence underpinning these steps is strong. The 2019 Cochrane review of fluoride toothpastes of different concentrations found that toothpastes of 1000 parts per million and above are significantly more effective at preventing caries than the lower-strength pastes of 250 to 440 parts per million, with a further dose-response to 1500 and 2800 parts per million — which is why modern guidance uses at least 1000 parts per million even for the youngest children, adjusting the amount (smear, pea, full strip) rather than the concentration. Fluoride varnish was confirmed by the 2013 Cochrane review to reduce the caries increment in both the primary and permanent dentition, and community water fluoridation at an optimal concentration of about 0.7 mg per litre was shown to increase the proportion of caries-free children and reduce decayed, missing and filled teeth. [1] [2] [3]
Fluoride toothpaste (age-based, child)
Dose
Rice-grain smear (under 3 years) or pea-sized (3 to 6 years) of at least 1000 ppm; full strip of 1350 to 1500 ppm from 6 years
Silver diamine fluoride 38 percent (caries arrest, child)
Dose
A thin layer applied to the cleaned, dried cavitated lesion
For the established cavity, the modern paradigm adds silver diamine fluoride (SDF) — a 38 percent solution applied to the cleaned lesion. A 2017 systematic review and meta-analysis found SDF prevented progression of around two-thirds of active carious lesions in primary teeth, and the 2018 evidence appraisal confirmed it as an effective agent for arresting primary-tooth caries. Its great advantage is that it is non-invasive and painless, suiting the young, the anxious and those without access to operative dentistry; its chief drawback is that it permanently stains the arrested lesion black, which must be discussed and consented. It is avoided in documented silver allergy and applied with mucosal protection. Restorative care — tooth-coloured or amalgam fillings, and fissure sealants for the at-risk permanent molars — follows for the cavitated but unarrested lesion, and theatre-based comprehensive care under general anaesthesia is reserved for the young child with extensive early childhood caries that cannot be managed in the chair. [4] [5] [12]
Specific Subtypes & Scenarios
The scenarios below are the ones examiners reach for, because each forces a different decision. [6]
Early childhood caries is the archetype of the topic. Its mechanism is the prolonged bathing of the maxillary anterior primary teeth in a cariogenic substrate — milk, juice or sweetened drink in a bedtime or on-demand bottle, or prolonged nocturnal breastfeeding without oral hygiene. The resulting white-spot-to-cavitation pattern of the upper front teeth, sparing the lower front, is the signature. Management combines immediate cessation of the nocturnal bottle (switch to water), twice-daily fluoride toothpaste, fluoride varnish, silver diamine fluoride for the cavitated lesions, restorative or theatre-based care for extensive disease, and establishment of a dental home. The preventive message that the first dental visit should occur within six months of the first tooth or by the first birthday exists precisely to head this off. [6] [12]
Molar-incisor hypomineralisation (MIH) presents when the first permanent molars erupt around age six with chalky, demarcated opacities — white, cream, yellow or brown — that break down under occlusal load, often with matching opacities on the permanent incisors. The affected enamel is porous and soft, the teeth are often hypersensitive, and the child develops rapid caries and severe restorative problems in adolescence. A 2026 Cochrane review found the evidence for the various non-invasive strategies (desensitising agents, sealants, fluoride) still maturing, so management is individualised — early diagnosis, protection of the fragile enamel, sensitivity control, and staged restorative care under paediatric dental supervision. [10]
Amelogenesis imperfecta is an inherited defect of enamel formation with autosomal-dominant, autosomal-recessive and X-linked patterns, conventionally grouped into hypoplastic (too little enamel), hypomaturation (soft, mottled enamel) and hypocalcified (poorly mineralised, easily lost) forms, with a combined form with taurodontism. The teeth are discoloured, sensitive and prone to rapid wear and caries across most or all of the dentition, and affected children carry a lifelong, multidisciplinary restorative burden; some syndromic forms are associated with renal disease and other comorbidities, which the clinician must not miss. [11]
The child with special healthcare needs or complex chronic disease is at elevated caries risk from dietary softening, reduced oral hygiene, medication-induced dry mouth, and sugar-containing or acidic long-term medicines (anticonvulsant syrups, formulations for children with feeding difficulties), and needs a tailored preventive programme with more frequent recall and fluoride varnish. Dental fluorosis is the developmental consequence of excessive fluoride intake during enamel formation; the modern optimal water fluoride concentration of about 0.7 mg per litre balances caries prevention against the risk of fluorosis, and is why the age-appropriate amount (not a lower concentration) of toothpaste is recommended for the young. [3] [11]
Complications & Pitfalls
The cardinal pitfall is treating dental caries as a cosmetic problem rather than a disease, and missing the spreading infection in the child who is "just a bit swollen". Severe pain or facial swelling from a necrotic tooth is a deep-space infection until excluded. [8]
The local complications of untreated caries are pain, pulpitis, periapical abscess and facial cellulitis, with their knock-on effects on eating, sleeping, growth, school attendance and oral-health-related quality of life — a young child with severe ECC may fail to thrive. The rare but serious complications are the deep-space neck infections, Ludwig's angina, orbital cellulitis from maxillary dental infection, and haematogenous or contiguous intracranial spread. These are the reasons a swollen face from a tooth is an emergency. [8] [9]
The preventive pitfalls are specific and common. Using a low-fluoride (250 to 440 parts per million) children's toothpaste sacrifices the caries-preventive effect that 1000 parts per million and above provides. Advising the child to rinse after brushing washes away the very fluoride that should linger. Delaying the first dental visit until school age misses the window in which ECC is preventable. And mistaking a developmental enamel defect for active caries leads to inappropriate operative treatment of a permanent defect — or, conversely, attributing a spreading facial cellulitis to a skin cause when the source is a necrotic molar. [2] [10]
Prognosis & Disposition
The prognosis of dental caries depends entirely on how early it is caught. The white-spot lesion is reversible with fluoride and dietary change; once cavitated into dentine the lesion needs restoration; and a necrotic, abscessed tooth needs drainage and extraction or root treatment. Early establishment of the preventive pillars sets the child on a low-risk trajectory for life. [7] [8]
Disposition and recall are stratified by caries risk. The low-risk child is recalled every six to twelve months; the moderate- and high-risk child every three to six months with more frequent fluoride varnish and dietary review. Discharge every child with a safety-net for the red flags: return for facial swelling, difficulty swallowing or breathing, fever, or uncontrolled pain. The developmental enamel defects — MIH and amelogenesis imperfecta — are permanent, lifelong conditions managed through a staged, multidisciplinary restorative pathway rather than cured. [8] [11]
Special Populations
Infants and toddlers are the population in whom prevention pays the greatest dividend: establishment of the dental home by 12 months, weaning from the nocturnal bottle, the introduction of a cup, and a rice-grain smear of 1000 ppm fluoride toothpaste from the first tooth. This is the window in which ECC is preventable, and it is the window most often missed. [6]
Children with special healthcare needs and complex chronic disease carry elevated caries risk from reduced oral hygiene, soft diets, medication-induced dry mouth, and sugar-containing syrups; they need tailored preventive programmes, more frequent recall, and fluoride varnish, often delivered with sedation or theatre-based care. Indigenous, remote and disadvantaged communities carry the disproportionate burden of severe ECC, addressed through community water fluoridation, supervised school toothbrushing and fluoride varnish programmes, delivered in culturally safe ways. [3] [8]
The adolescent faces new risks — dietary independence, sugary and acidic drinks, orthodontic appliances that retain plaque, and the eating-disorders and reflux that erode enamel — and benefits from continued fluoride toothpaste, sealants on the permanent molars, dietary counselling, and a planned transition to adult dental care. Children on long-term sugar-containing or acidic medication (anticonvulsant and antibiotic syrups) accumulate caries and erosion risk that the prescriber should mitigate by favouring sugar-free formulations. [2] [8]
Evidence, Guidelines & Regional Differences
The named regional guidance is the American Academy of Pediatric Dentistry (AAPD) policies on ECC and caries-risk assessment, the US Preventive Services Task Force (USPSTF) recommendation on fluoride varnish, the Royal Children's Hospital Melbourne and NICE CKS dental-caries guidance in ANZ and the UK, and the World Health Organization guidance on free-sugar intake. [3] [8]
The Cochrane evidence base is the backbone of the prevention guidance: the 2019 review of fluoride toothpastes of different concentrations confirmed the 1000 ppm and above concentration effect; the 2013 review of fluoride varnishes confirmed their caries-preventive effect in children; and the 2015 review of community water fluoridation confirmed an increase in caries-free children and a reduction in decayed, missing and filled teeth, alongside an association with fluorosis at higher water fluoride levels. The silver diamine fluoride evidence — a 2017 meta-analysis and the 2018 evidence appraisal — established it as an effective, non-operative agent for arresting primary-tooth caries. [1] [2] [4]
[2] [3]Exam Pearls
Dental caries is a biofilm-mediated, sugar-driven disease in which acid from a Streptococcus mutans-dominated plaque dissolves enamel below the critical pH of about 5.5, and its paediatric form is early childhood caries — any decayed, missing or filled primary tooth surface in a child 71 months or younger. It is preventable through twice-daily fluoride toothpaste of at least 1000 ppm (a rice-grain smear under three, a pea-sized amount from three to six), fluoride varnish two to four times a year for children at risk, a low-sugar diet, and a dental home by the first birthday. [6] [7]
For the established lesion, silver diamine fluoride 38 percent arrests around two-thirds of active primary-tooth caries at the cost of a permanent black stain, and restorative or theatre-based care follows for the unarrested cavity. The emergency is the spreading odontogenic infection — facial swelling with trismus, dysphagia or dyspnoea — managed by securing the airway, giving intravenous antibiotics with anaerobic cover, and urgent dental or maxillofacial referral for drainage and source control. [4] [8]
References
- [1]Marinho VC; Worthington HV; Walsh T; Clarkson JE Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev, 2013.PMID 23846772
- [2]Walsh T; Worthington HV; Glenny AM; Marinho VC; et al Fluoride toothpastes of different concentrations for preventing dental caries. Cochrane Database Syst Rev, 2019.PMID 30829399
- [3]Iheozor-Ejiofor Z; Worthington HV; Walsh T; O'Malley L; et al Water fluoridation for the prevention of dental caries. Cochrane Database Syst Rev, 2015.PMID 26092033
- [4]Chibinski AC; Wambier LM; Waltmann TM; et al Silver Diamine Fluoride Has Efficacy in Controlling Caries Progression in Primary Teeth: A Systematic Review and Meta-Analysis. Caries Res, 2017.PMID 28972954
- [5]Horst JA; Ellenikiotis H; Milgrom PL Silver Fluoride as a Treatment for Dental Caries. Adv Dent Res, 2018.PMID 29355428
- [6]Kimmie-Dhansay F; Asawa N; Chikte UMA; Naidoo S; et al Maternal and infant risk factors and risk indicators associated with early childhood caries in South Africa: a systematic review. BMC Oral Health, 2022.PMID 35585594
- [7]Duque C; Calgarotto AK; Ilha CS; et al Understanding the Predictive Potential of the Oral Microbiome in the Development and Progression of Early Childhood Caries. Curr Pediatr Rev, 2023.PMID 35959611
- [8]Bernabe E; Marcenes W; Hernandez CR; Bailey J; et al Global, Regional, and National Levels and Trends in Burden of Oral Conditions from 1990 to 2017: A Systematic Analysis for the Global Burden of Disease 2017 Study. J Dent Res, 2020.PMID 32122215
- [9]GBD 2021 Oral Disorders Collaborators Trends in the global, regional, and national burden of oral conditions from 1990 to 2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet, 2025.PMID 40024264
- [10]Kumari P; Collard DC; Elhaddad SA; et al Non-invasive management strategies for molar-incisor hypomineralization (MIH) in children. Cochrane Database Syst Rev, 2026.PMID 42454625
- [11]Chu KY; Bhatt DK; Wright JT Hereditary enamel defects with comorbidities. J Am Dent Assoc, 2026.PMID 42240524
- [12]Crystal YO; Marghalani AA; Ureles SD; et al Silver Diamine Fluoride is Effective in Arresting Caries Lesions in Primary Teeth. J Evid Based Dent Pract, 2018.PMID 29747804