Paeds · ent-hearing-and-oral-health
Dental trauma and avulsed teeth
Also known as Avulsed permanent tooth · Knocked-out tooth · Tooth luxation · Crown fracture · Root fracture · Traumatic dental injury · Intrusive luxation
Fellowship topic on dental trauma and avulsed teeth in children. Covers traumatic dental injury as a time-critical emergency in which the management in the first minutes at the scene decides whether an avulsed permanent tooth survives; the Andreasen classification of hard-tissue and periodontal-ligament injuries; the periodontal ligament cell-viability pathophysiology that makes extra-alveolar dry time the dominant prognostic factor; the International Association of Dental Traumatology 2020 first-aid and management protocol of finding the tooth, holding it by the crown, rinsing a dirty root for about ten seconds and replanting a permanent tooth immediately or storing it in milk, HBSS or saliva; the rule that primary teeth are never replanted; flexible splinting, root-canal-treatment timing and systemic antibiotics for the replanted tooth; luxation and fracture subtypes; complications of inflammatory and replacement root resorption; the oral-injury link with non-accidental injury; and the safety-net and dental follow-up plan.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A nine-year-old boy falls off his bicycle and arrives in the emergency department holding his permanent front tooth in a glass of milk, twenty minutes after the fall. What you and his parents did in those twenty minutes will decide whether that tooth is still a living part of his mouth when he is nineteen. That is the whole topic compressed into a single vignette: dental trauma is a time-critical injury in which the correct action is taken at the scene, often by a layperson, long before a clinician is involved. [1] [6]
A traumatic dental injury is damage to the teeth, their supporting structures or the surrounding oral soft tissues caused by an external force. The damage ranges from a chip of enamel, through loosening and displacement of an intact tooth, to the complete avulsion of a tooth from its socket. The fellowship skill is to recognise which of these is the emergency, to know what should have been done at the scene, and to deliver the immediate management that salvages a tooth — or to know when a primary tooth must be left alone. [4] [10]
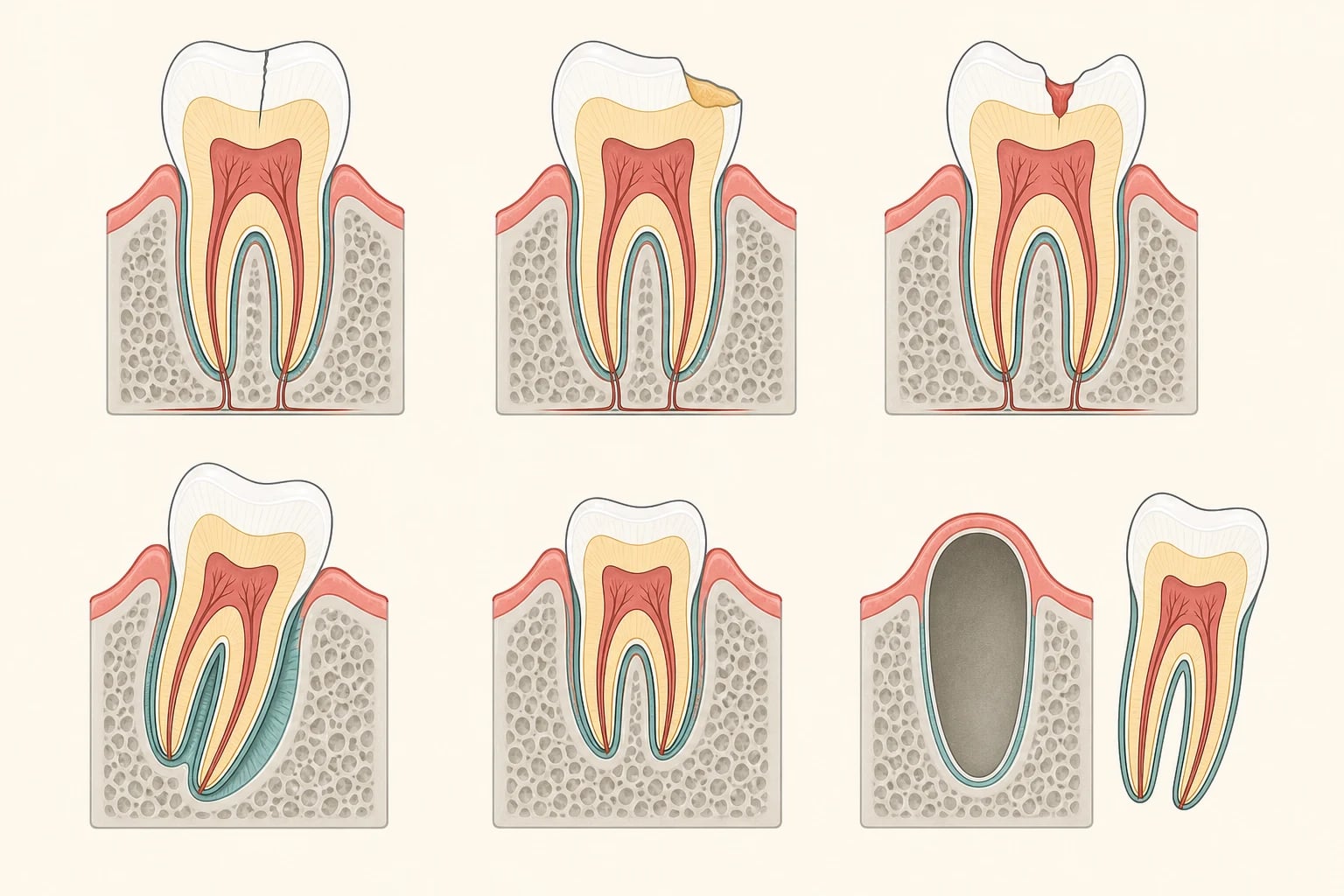
The injuries divide cleanly by what is torn. Hard-tissue injuries fracture the tooth — an enamel infraction, an uncomplicated or complicated crown fracture breaching or not breaching the pulp, a crown-root or root fracture. Periodontal-tissue injuries damage the attachment — a concussion, a subluxation, an extrusive, lateral or intrusive luxation, and finally the complete avulsion. Supporting-bone injuries fracture the alveolar socket wall. This division, the Andreasen classification, is the language examiners expect, and it maps directly onto management. [2] [4]
The central, life-of-the-tooth decision is the avulsed permanent tooth, and it is the one the public most often gets wrong. The cells of the periodontal ligament that remain on the root surface are the only thing that can re-form a healthy attachment; once they dry and die, the body treats the root as a foreign body and resorbs it. Everything in this topic — the first-aid, the storage media, the timing, the rule about primary teeth — flows from that single biological fact. [1] [7]
Classification
The classification that governs management is the Andreasen system, which sorts injuries by the tissue harmed. [2] [4]
A hard-tissue and pulp injury breaks the tooth itself. An infraction is an incomplete crack of the enamel with no loss of tissue. An uncomplicated crown fracture loses enamel, or enamel and dentine, but leaves the pulp unexposed. A complicated crown fracture exposes the pulp, and is a dental emergency because the pulp will necrose and infect if not promptly sealed. A crown-root fracture or root fracture extends below the gum line, and a root fracture's prognosis depends on its level. [2]
A periodontal-tissue injury damages the ligament that suspends the tooth. Concussion leaves the tooth tender but undisplaced and unmobilised. Subluxation loosens the tooth without displacement. Extrusive luxation partly pulls it out of the socket, lateral luxation displaces it sideways, and intrusive luxation drives it up into the bone. Avulsion is the complete loss of the tooth from its socket. The severity climbs from concussion to avulsion, and so does the threat to the tooth's survival. [2] [4]
The Andreasen classification of traumatic dental injuries
Epidemiology & Risk Factors
Traumatic dental injury is common, and it is commonest at the ages when children are most active and most likely to fall. Around one in four to one in three children sustains some dental trauma by adolescence, with two peak incidence bands: the toddlers, who fall while learning to walk, and the school-age and early-adolescent children, whose injuries come from sport, play, fights and road trauma. The upper central permanent incisors are by far the most commonly injured teeth. [6]
The risk factors are the predictable ones. Increased overjet (prominent upper front teeth, common in thumb-suckers and mouth-breathers) leaves the incisors exposed and doubles or triples the risk of fracture and avulsion. Contact sport without a mouthguard, playground falls, cycling and contact with hard objects account for most mechanisms. The protective factor the examiner wants named is the custom-fitted mouthguard for contact and risky sport, and the early orthodontic correction of a marked overjet. [6] [9]
The burden, and the access to care, are unevenly shared. A child injured in a remote community with no urgent dental service may arrive hours after the tooth has dried, while a child at a well-resourced school with a trained first-aider may have the tooth back in its socket within minutes. This access gap is part of the public-health case for first-aid education in schools and for sporting mouthguard programmes, and it is why a generalist paediatric clinician — often the first professional a family contacts — must know the scene protocol cold. [6] [4]
Pathophysiology
Why does a tooth resorb after avulsion, and why does time matter so much? The answer lies entirely in the periodontal ligament cells clinging to the root surface. [1] [7]
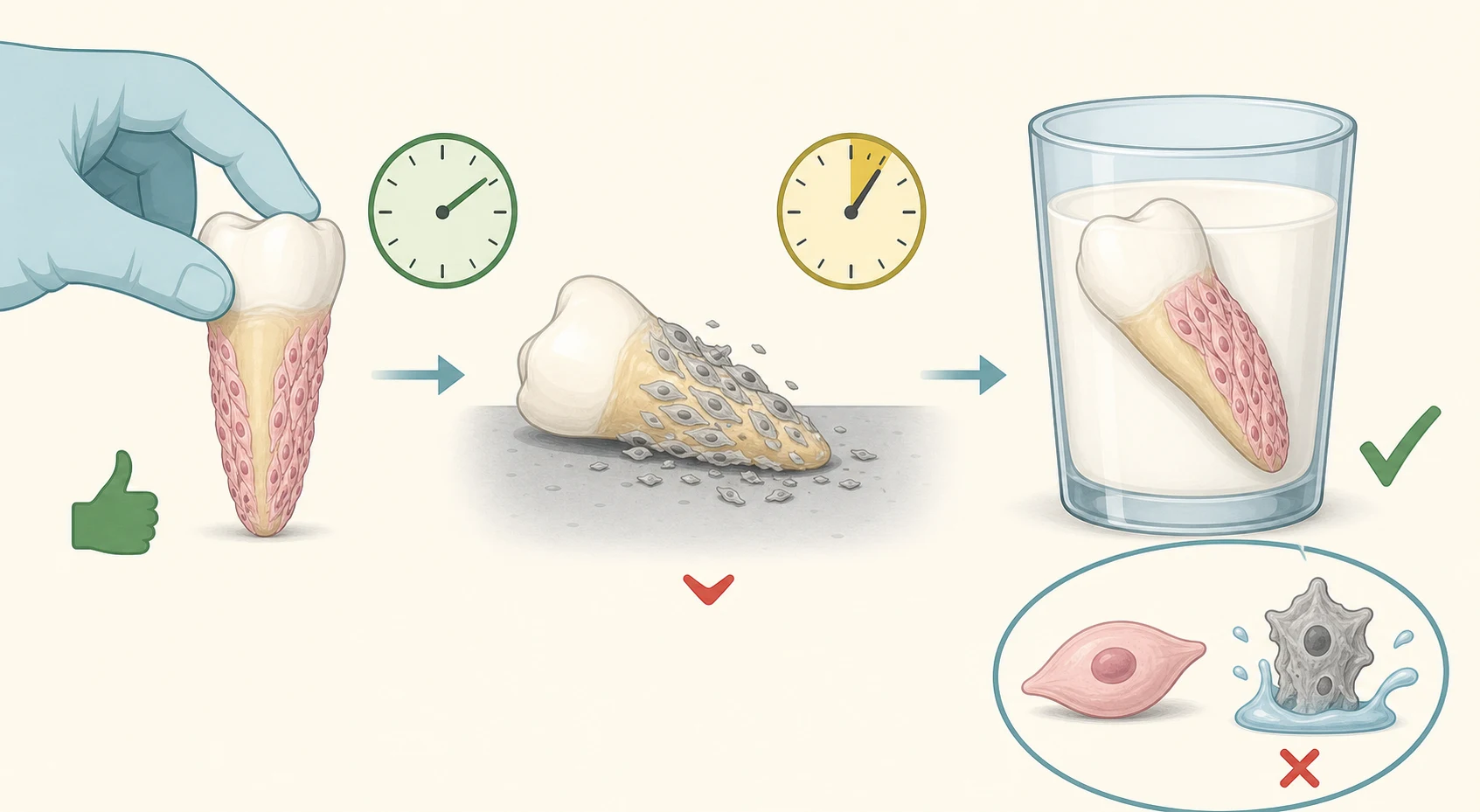
A tooth is not anchored to bone rigidly but suspended within its socket by a fibrous hammock, the periodontal ligament. When the tooth is knocked out, a thin sheet of these ligament cells stays attached to the root, and they are the only cells capable of re-forming a healthy attachment to the bone. If the tooth is replanted while these cells are alive, the ligament can heal and the tooth can function for decades. If the cells dry and die, the attachment cannot re-form, and the body mounts a resorptive response against the now-dead root. [1] [7]
The clock that governs survival is extra-alveolar dry time — the time the tooth spends out of its socket and dry. Periodontal-ligament cells begin to die within minutes on a dry surface, and after about sixty minutes of dry time most are non-viable. A tooth replanted within twenty minutes has an excellent prognosis; one that has been dry for an hour or more is likely to undergo replacement resorption (ankylosis), in which the bone fuses to the root and then slowly resorbs it, or inflammatory resorption, driven by infected necrotic pulp. The storage medium matters for exactly this reason: milk and HBSS keep the cells alive far longer than water, which is hypotonic and ruptures them. [1] [9]
Two further biological facts shape management. A closed-apex (mature, fully formed) permanent tooth has no capacity for pulp revascularisation, so its pulp will necrose and must be removed by root canal treatment starting around a week after replantation. An open-apex (immature, still-developing) tooth has an open root end through which new vessels can re-enter, so the goal is to keep it alive and allow revascularisation rather than rush to root-canal treatment. This single distinction — closed versus open apex — drives the entire post-replantation dental plan. [1] [5]
Clinical Presentation
Read the injury the way the mechanism tells you to — a child who fell and knocked a tooth, a chip on the ground beside him, and the question every parent asks: can it be saved? [2]
The presentation of avulsion is unmistakable: a visibly missing tooth, an empty or blood-filled socket, and the tooth itself, often brought in a tissue, a hand, or — correctly — a container of milk. The first questions to the scene are the ones that decide prognosis: when did it happen (the dry time), where is the tooth, how was it stored, and is it a permanent or a primary tooth. A child around seven to eight years old who has just lost a front tooth almost always has a permanent incisor, because the upper central permanent incisors erupt at about six to seven years. [1] [3]
Luxation injuries present with displacement. An extruded tooth looks elongated; a laterally luxated tooth is pushed sideways, often with the edge driven into the lip; an intruded tooth has been driven up into the gum and may look shortened or even absent, sitting hidden in the bone. A subluxed tooth is loose and tender but in place, and a concussed tooth is tender only to tapping. Bleeding from the gum around the tooth, and a lip laceration, commonly accompany the injury. [2]
Fracture injuries present with a visible chip. An uncomplicated fracture shows lost enamel and dentine with the pink pulp protected; a complicated fracture shows a tiny red pinpoint of exposed pulp at the fracture site, which is exquisitely tender to air and cold. Always inspect the inside of a torn lip for embedded tooth fragments, and palpate the lip and chin for full-thickness injury. The presentation that must not be missed alongside the dental injury is an associated head injury, facial fracture, or sign of non-accidental injury — examine the whole child first. [2] [12]
Differential Diagnosis
Build the differential around two questions: is the tooth a primary or a permanent tooth, and is the injury accidental and consistent with the history? [3] [12]
The first fork determines the whole management of avulsion. A permanent tooth is replanted; a primary tooth is not. Distinguishing them at the scene is done by the child's age and the tooth's morphology: the upper central permanent incisors erupt at about six to seven years, so a knocked-out front tooth in a seven-year-old is a permanent tooth to be saved, whereas the same tooth in a three-year-old is a primary tooth to be left alone. A primary incisor is smaller, whiter and has a longer, thinner root relative to its crown. When in doubt, treat it as a permanent tooth and seek urgent dental advice. [1] [3]
The second fork is the safeguarding one. A torn upper labial frenulum in a non-mobile infant, repeated oral injury, a delay in seeking care for a painful injury, or an injury inconsistent with the stated mechanism raise non-accidental injury. Oral and dental signs are increasingly recognised among the markers of child abuse, and the dentist and paediatrician share a duty to look beyond the tooth. The history must be taken carefully and the whole child examined. [12]
The remaining differential is anatomical. A tooth that appears missing may be intruded deep into the bone, aspirated, swallowed, or embedded in a lip laceration rather than truly lost — image the chest if a tooth or fragment cannot be accounted for, and examine and palpate the lip. A loosened, tender tooth may be a luxation or a root fracture, and a discoloured tooth that appears unhurt may have suffered a concussion or subluxation with later pulpal necrosis. Spontaneous dental pain without trauma points back to caries or periapical infection rather than injury. [2] [4]
Clinical & Bedside Assessment
Start with the scene history, because it contains the prognosis. Establish the time of injury (to calculate the dry time), the storage medium and handling (was it held by the crown, was it stored in milk, was it scrubbed or left to dry), the mechanism (fall, sport, blow), and any associated head injury, loss of consciousness, or facial fracture. Then confirm whether the tooth is primary or permanent, and whether the child is fully immunised, including tetanus. [1] [4]
Examine the mouth with a good light and suction, once the child is settled. Identify the missing, displaced, fractured or loosened tooth, assess its mobility and displacement, and look for gum and lip lacerations and embedded fragments. Test tenderness to gentle tapping if the child can tolerate it. Record which tooth (by position) is injured, and whether a fragment or whole tooth is unaccounted for. Always inspect the inside of the lip and the floor of the mouth, where fragments hide. [2]
Assess the whole child first — airway, cervical spine, conscious state and facial bones — before focusing on the tooth, because an associated head injury or facial fracture takes priority. Look specifically for the safeguarding signs, and consider tetanus status for a contaminated wound from soil or a dirty surface. The bedside judgement that decides everything is whether a permanent tooth is avulsed and how long it has been dry: if it is still out, the assessment merges straight into management, because the clock is running. [1] [4]
Investigations
Dental trauma is managed on clinical findings; the role of investigation is to find the hidden injury, to stage the dental damage, and to safeguard the child. [2]
Dental radiographs — a periapical or occlusal film, and sometimes more than one angle — confirm the position of a luxated or intruded tooth, reveal a root fracture, and show whether a fragment remains in the lip or gum. They are taken and interpreted by the dental team. For the generalist, the principle is to image where a fragment or whole tooth is unaccounted for, and to image the chest and abdomen if a tooth or fragment may have been aspirated or swallowed. [2] [4]
For the child with an associated head injury or facial fracture, the relevant imaging is clinical-suspicion-led — a facial or skull series, or computed tomography for a suspected facial fracture or intracranial injury. The dental-specific investigation that the generalist must remember is the search for a missing tooth: an intruded tooth can hide entirely within the bone, and a swallowed or aspirated tooth is a real risk in a young, distressed child. Pulp vitality testing at follow-up, performed by the dentist, tracks whether the replanted or luxated tooth's nerve has survived or necrosed, and guides the need for root canal treatment. [1] [2]
[2]Management — Resuscitation
The resuscitation of dental trauma is the resuscitation of the avulsed permanent tooth, and its principles are applied at the scene by the first person present. The hierarchy is the tooth first, then the child's other injuries, then safeguarding — except that a compromised airway, cervical spine or conscious state always takes precedence over the tooth. [1] [4]
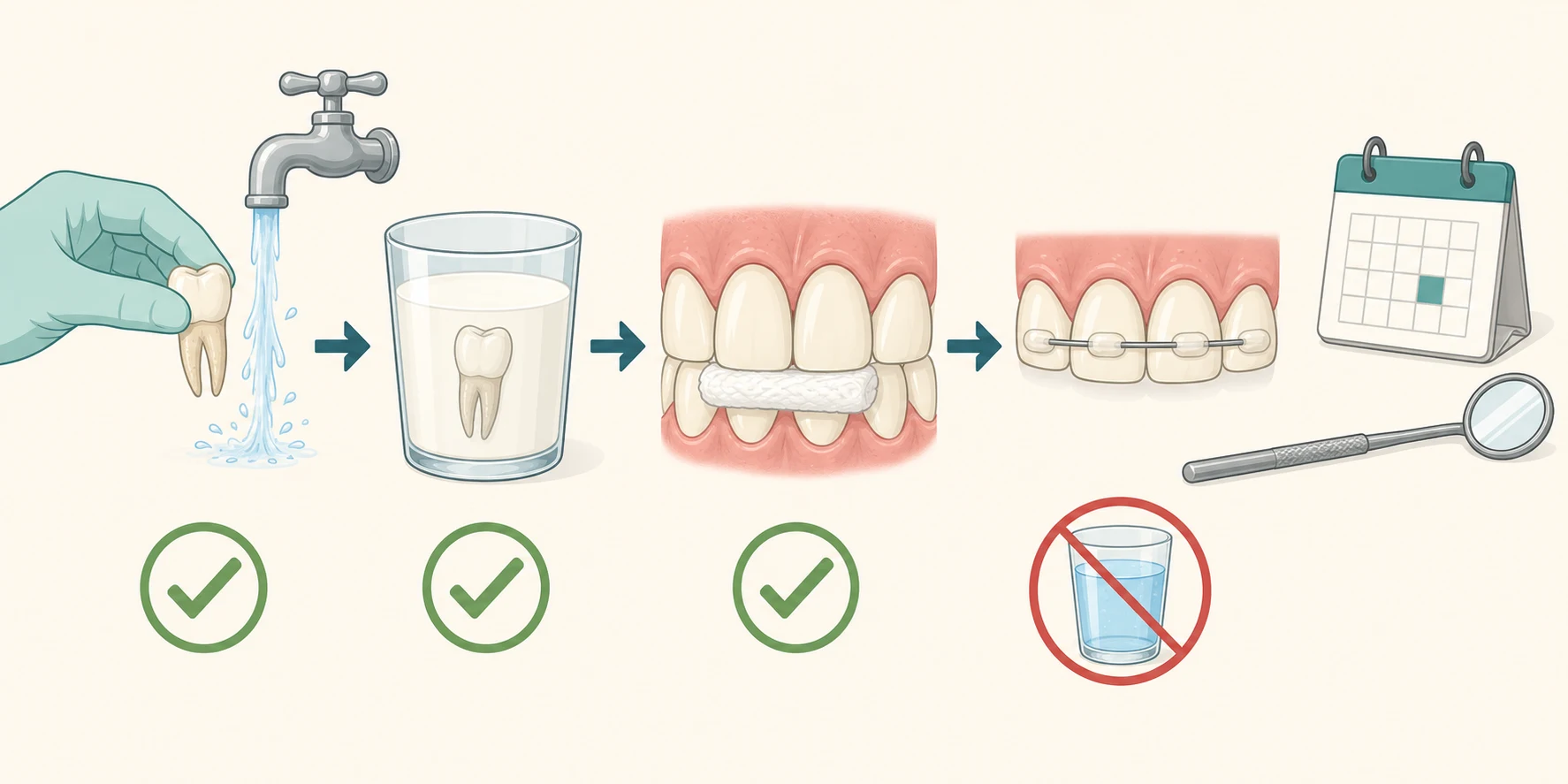
For an avulsed permanent tooth that is still out, act on the IADT 2020 protocol without delay. Find the tooth, pick it up by the crown only, rinse a dirty root under cool running water for about ten seconds, and replant it immediately, orienting it the right way into the socket, then have the child bite gently on a clean handkerchief or gauze to hold it in place. If you cannot replant it — the child is uncooperative or the socket is damaged — store it in cold milk, HBSS, saline, or in the cheek of an cooperative older child, and get to a dentist immediately. Never store the tooth in plain water, never scrub or scrape the root, and never let it dry. [1] [9]
For an avulsed primary tooth, do not replant it. Replanting a primary tooth can damage the developing permanent successor, and the evidence does not support it; control the bleeding, give analgesia, reassure the family that a permanent tooth will still erupt, and arrange dental review. For pain, give weight-based paracetamol 15 mg per kilogram (maximum 1 g) or ibuprofen 5 to 10 mg per kilogram (maximum 400 mg), assess tetanus prophylaxis for a contaminated wound, and refer urgently to dental or maxillofacial services for any displaced, deeply intruded or complicated fracture injury. [3] [1]
Management — Definitive & Stepwise
Once the tooth is replanted (or stored), definitive care is dental and follows the IADT 2020 protocol by apex status and dry time. The generalist's job is to deliver the tooth to the dentist alive, to start analgesia and antibiotics, and to safety-net. [1] [5]
The stepwise management of an avulsed permanent tooth (IADT 2020)
Scene first-aid — find the tooth, hold it by the crown, rinse a dirty root under running water for about ten seconds, and replant it immediately; if you cannot replant, store it in cold milk, HBSS, saline or the cheek, never in water.
Replantation at the clinic — clean the socket if needed, replant the tooth the correct way, and have the child bite on gauze to seat it; confirm position clinically.
Flexible splint — apply a flexible (physiological) splint for about two weeks to hold the tooth while the periodontal ligament heals; longer splinting is used for associated bone or root fractures.
Root canal treatment — for a closed-apex (mature) tooth, start root canal treatment at seven to ten days after replantation, because the pulp will necrose; an open-apex (immature) tooth is managed to allow revascularisation, with treatment only if necrosis or infection develops.
Systemic antibiotics — give a systemic antibiotic course as recommended by the IADT (tetracycline in older children and adults; phenoxymethylpenicillin or amoxicillin in younger children where tetracyclines are avoided), alongside the dental care.
Tetanus prophylaxis and safety-net — assess tetanus status for a contaminated wound, review for infection or resorption at dental follow-up, and give weight-based analgesia.
The evidence base, distilled in the 2019 Cochrane review of interventions for the avulsed and replanted permanent tooth, is limited in the randomised sense but remarkably consistent on the principles that matter: minimise dry time, keep the root hydrated in a physiologically balanced medium, replant promptly, and use a short flexible splint. The Kahler review and the IADT 2020 guidelines moved splinting away from rigid wiring toward flexible splints, which permit the small physiological movement that protects the healing ligament from ankylosis. [5] [8]
Analgesia for acute dental injury (child, weight-based)
Dose
Paracetamol 15 mg per kilogram (maximum 1 g), or ibuprofen 5 to 10 mg per kilogram (maximum 400 mg)
The management of the other injuries follows the same priority of early dental involvement. Crown fractures — especially a complicated fracture with exposed pulp — need prompt dental coverage of the pulp to prevent necrosis. Luxation injuries need repositioning and flexible splinting by the dentist; an intruded permanent tooth may be allowed to re-erupt or be orthodontically repositioned depending on the degree and apex. The role of the generalist is to recognise the injury, deliver the tooth or tooth fragment to the dentist promptly, and never let an avulsed permanent tooth sit dry while waiting. [2] [4]
Specific Subtypes & Scenarios
The scenarios below are the ones examiners reach for, because each turns on a single decision. [1]
The avulsed permanent tooth is the archetype and the emergency. The IADT 2020 avulsion guideline is explicit: the dry extra-alveolar time is the dominant prognostic factor, the tooth should be replanted at the scene wherever possible, and the storage medium is milk, HBSS, saline or saliva — never water. A closed-apex tooth receives root canal treatment starting at seven to ten days; an open-apex tooth is managed for revascularisation, with treatment only if the pulp necroses. A tooth that was dry for over sixty minutes has a poor prognosis and is managed knowing ankylosis and replacement resorption are likely. [1] [7]
The avulsed primary tooth is the mirror-image decision: it is never replanted. The 2020 primary-dentition guideline is clear that replanting a primary tooth offers no benefit and risks injuring the developing permanent successor, so management is reassurance, bleeding control, analgesia and dental review. The same guideline directs that an intruded primary tooth near the developing permanent successor is often left to re-erupt, but one driven directly into the permanent tooth germ may need extraction by a specialist. [3]
Luxation and fracture injuries need prompt dental involvement rather than scene surgery. A complicated crown fracture with exposed pulp is a dental emergency for pulp coverage. A laterally or extrusively luxated permanent tooth is repositioned and flexibly splinted. An intruded permanent tooth with a closed apex is unlikely to re-erupt spontaneously and is orthodontically or surgically repositioned, while an immature open-apex intruded tooth may be watched for spontaneous re-eruption. The generalist's role is recognition, fragment care and timely referral. [2] [4]
The child with a missing tooth fragment and a torn lip must be examined for an embedded fragment, which is radio-opaque and visible on a soft-tissue radiograph. And the child whose oral injury is unexplained, repeated or age-inconsistent must trigger a safeguarding assessment: oral and dental injuries are documented markers of child abuse, and a torn frenulum in a non-ambulant infant is a particular red flag. [2] [12]
Complications & Pitfalls
The cardinal pitfall is letting an avulsed permanent tooth dry while deciding what to do — the single most damaging error in paediatric dental trauma, because every dry minute kills the cells the tooth needs to survive. [1] [7]
The complications are the resorptive processes that follow a damaged or necrotic periodontal ligament. Inflammatory resorption follows infection of a necrotic pulp, eroding root and bone around an infected tooth, and is limited by timely root canal treatment. Replacement resorption (ankylosis) follows death of the periodontal ligament: the bone fuses directly to the root and then slowly replaces it, so the tooth becomes solid, fails to grow with the jaw in a child, and is eventually lost. Pulp necrosis and discolouration complicate luxated and fractured teeth, and a complicated crown fracture left untreated leads to pulp infection and periapical abscess. [11] [1]
The management pitfalls are specific and common. Storing the tooth in water ruptures the ligament cells by osmosis. Scrubbing or scraping the root strips off the very cells needed for healing. Replanting a primary tooth endangers the permanent successor. Using a rigid splint instead of a flexible one promotes ankylosis. Delaying root canal treatment in a closed-apex tooth allows inflammatory resorption. And missing an associated head injury, facial fracture, aspirated tooth, or non-accidental injury by focusing only on the tooth harms the whole child. [1] [12]
Prognosis & Disposition
The prognosis of an avulsed permanent tooth depends almost entirely on extra-alveolar dry time and the storage medium. A tooth replanted within twenty minutes, or kept moist in milk or HBSS, has a good chance of long-term function; one that was dry for over an hour is likely to undergo ankylosis and replacement resorption and to be lost over years. The Pohl survival analysis confirmed dry time as the dominant predictor of tooth loss after replantation. [1] [7]
Disposition is urgent dental or maxillofacial referral for any avulsed, luxated, intruded or complicated-fracture permanent tooth, and dental review for primary-tooth and minor injuries. Every child needs scheduled dental follow-up — typically at one to two weeks for splint removal and root canal assessment in a closed-apex tooth, then at intervals over months and years to monitor for resorption and pulp vitality. The follow-up is part of the management, not an afterthought, because resorption can declare itself months later. [1] [2]
Discharge every family with a safety-net for the red flags: return for facial swelling, spreading infection, fever, worsening pain, a loosening or lost replanted tooth, or any new symptom. Counsel families that an avulsed tooth, even well managed, may discolour, require later root treatment, or be lost to resorption over time — honest expectation-setting is part of good care. The developmental enamel defects are not at issue here, but the injured young tooth's long-term behaviour is. [1] [11]
Special Populations
Toddlers and preschool children most often injure primary teeth through falls, and their management hinges on the never-replant rule and on distinguishing a primary from a permanent tooth by age and morphology. Because a primary tooth sits directly above the developing permanent successor, even a non-avulsion injury — a deep intrusion — must be assessed for threat to the permanent tooth, and intrusive primary teeth near the permanent germ may need specialist extraction. [3]
School-age children and early adolescents are the population in whom permanent-tooth avulsion is commonest, through sport, play and road trauma. This is the group for whom scene first-aid education and custom-fitted mouthguards pay the greatest dividend, and the group whose parents, teachers and coaches must know the protocol. A permanent central incisor avulsed at age eight is a tooth meant to last seventy years, and its loss carries a lifelong restorative burden. [6] [1]
Children with special healthcare needs or complex chronic disease, and children in remote communities with limited urgent dental access, are at risk of worse outcomes from the same injury because of delayed presentation and reduced access to timely replantation and follow-up. The child with an unexplained oral injury is the safeguarding population, for whom a torn frenulum in a non-mobile infant, delayed presentation or an inconsistent history mandates a whole-child assessment and safeguarding referral. Public-health first-aid education and equitable dental access narrow these gaps. [6] [12]
Evidence, Guidelines & Regional Differences
The named guidance is the International Association of Dental Traumatology (IADT) 2020 guidelines, published as a set — the general introduction, fractures and luxations, avulsion of permanent teeth, and injuries in the primary dentition — and introduced to the field in the accompanying editorial. These are the international standard that examiners expect, superseding the 2012 and 2007 guidelines. [1] [2] [3] [4] [10]
The evidence underpinning the avulsion protocol was distilled in the 2019 Cochrane review of interventions for the avulsed and replanted permanent tooth, which found a limited randomised evidence base but consistent observational support for prompt replantation and physiologic storage media. The Pohl 2005 survival analysis established extra-alveolar dry time as the dominant predictor of tooth loss, and the Kahler 2016 review drove the shift toward short flexible splinting. The storage-media literature, summarised in the Ballal 2011 review, ranks milk and HBSS as the practical physiologic media that keep periodontal-ligament cells viable, in contrast to water. [5] [7] [8] [9]
[1] [6]Exam Pearls
Dental trauma is a time-critical injury whose outcome is decided at the scene, before the child reaches a clinician. The avulsed permanent tooth survives only if its periodontal-ligament cells are kept alive — by immediate replantation within about twenty minutes, or storage in milk or HBSS, never in water or dry — because extra-alveolar dry time is the dominant prognostic factor. [1] [9]
The IADT 2020 protocol is the standard: hold by the crown, rinse a dirty root for about ten seconds, replant a permanent tooth, flexible splint for about two weeks, root canal treatment at seven to ten days for a closed apex, and systemic antibiotics with tetanus prophylaxis where indicated. The two unbreakable rules are to replant a permanent tooth and to never replant a primary tooth, and the long-term enemies are inflammatory and replacement root resorption. [1] [8]
References
- [1]Fouad AF; Abbott PV; Tsilingaridis G; Cohenca N; Lauridsen E; Bourguignon C; O'Connell A; Flores MT; Day PF; Hicks L; Andreasen JO; Cehreli ZC; Harlamb S; Kahler B; Oginni A; Semper M; Levin L International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teeth. Dent Traumatol, 2020.PMID 32460393
- [2]Bourguignon C; Cohenca N; Lauridsen E; Flores MT; O'Connell AC; Day PF; Tsilingaridis G; Abbott PV; Fouad AF; Hicks L; Andreasen JO; Cehreli ZC; Harlamb S; Kahler B; Oginni A; Semper M; Levin L International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations. Dent Traumatol, 2020.PMID 32475015
- [3]Day PF; Flores MT; O'Connell AC; Abbott PV; Tsilingaridis G; Fouad AF; Cohenca N; Lauridsen E; Bourguignon C; Hicks L; Andreasen JO; Cehreli ZC; Harlamb S; Kahler B; Oginni A; Semper M; Levin L International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 3. Injuries in the primary dentition. Dent Traumatol, 2020.PMID 32458553
- [4]Levin L; Day PF; Hicks L; O'Connell A; Fouad AF; Bourguignon C; Abbott PV International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: General introduction. Dent Traumatol, 2020.PMID 32472740
- [5]Day PF; Duggal M; Nazzal H Interventions for treating traumatised permanent front teeth: avulsed (knocked out) and replanted. Cochrane Database Syst Rev, 2019.PMID 30720860
- [6]Lam R Epidemiology and outcomes of traumatic dental injuries: a review of the literature. Aust Dent J, 2016.PMID 26923445
- [7]Pohl Y; Wahl G; Filippi A; Kirschner H Results after replantation of avulsed permanent teeth. III. Tooth loss and survival analysis. Dent Traumatol, 2005.PMID 15773889
- [8]Kahler B; Hu JY; Marriot-Smith CS; Heithersay GS Splinting of teeth following trauma: a review and a new splinting recommendation. Aust Dent J, 2016.PMID 26923448
- [9]Ballal V; V J Storage media. Br Dent J, 2011.PMID 21869779
- [10]Abbott PV; Levin L Introducing the revised IADT Guidelines for the management of traumatic dental injuries. Dent Traumatol, 2020.PMID 32959640
- [11]de Gregorio C; Tewari N Management of Complications in Dental Traumatology. Dent Traumatol, 2025.PMID 39578670
- [12]Mele F; Introna F; Santoro V Child abuse and neglect: oral and dental signs and the role of the dentist. J Forensic Odontostomatol, 2023.PMID 37634173