Paeds · ent-hearing-and-oral-health
Epistaxis in children
Also known as Childhood nosebleed · Nasal haemorrhage in children · Anterior epistaxis · Little's area bleed · Kiesselbach's plexus bleeding · Recurrent paediatric epistaxis
Fellowship topic on epistaxis in children — bleeding from the nasal mucosa, over 90 percent anterior from Little's area (Kiesselbach's plexus) on the anteroinferior septum. Covers the four-artery anatomy that explains anterior vulnerability and the sphenopalatine origin of posterior bleeds; the digital-trauma, dry-air, allergic-rhinitis and upper-respiratory-tract-infection precipitants; the correct first-aid technique (sit upright, lean forward, pinch the soft part of the nose for 10 to 15 minutes) and the common errors of tilting the head back or pinching the bony bridge; the stepwise escalation from first aid through topical vasoconstriction, silver-nitrate cautery (one side of the septum) and nasal packing; the antiseptic-cream and cautery evidence for recurrent disease; and the red flags of bleeding disorder, juvenile nasopharyngeal angiofibroma in the adolescent male, foreign body and non-accidental injury, with ANZ, UK, US and Canadian guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A mother rings the after-hours line about her four-year-old, frightened because blood is dripping from one nostril after he rubbed it in a warm room. An hour later, in the emergency department, a seven-year-old is brought in tilted backward in a chair, a towel soaked with blood and now vomiting. Both have epistaxis, but the first is the benign anterior majority that first aid settles in minutes, and the second shows how a wrong technique turns a small bleed into a mess. The fellowship skill is to recognise that most childhood epistaxis is benign and anterior, and to teach and apply correct first aid without delay. [1]
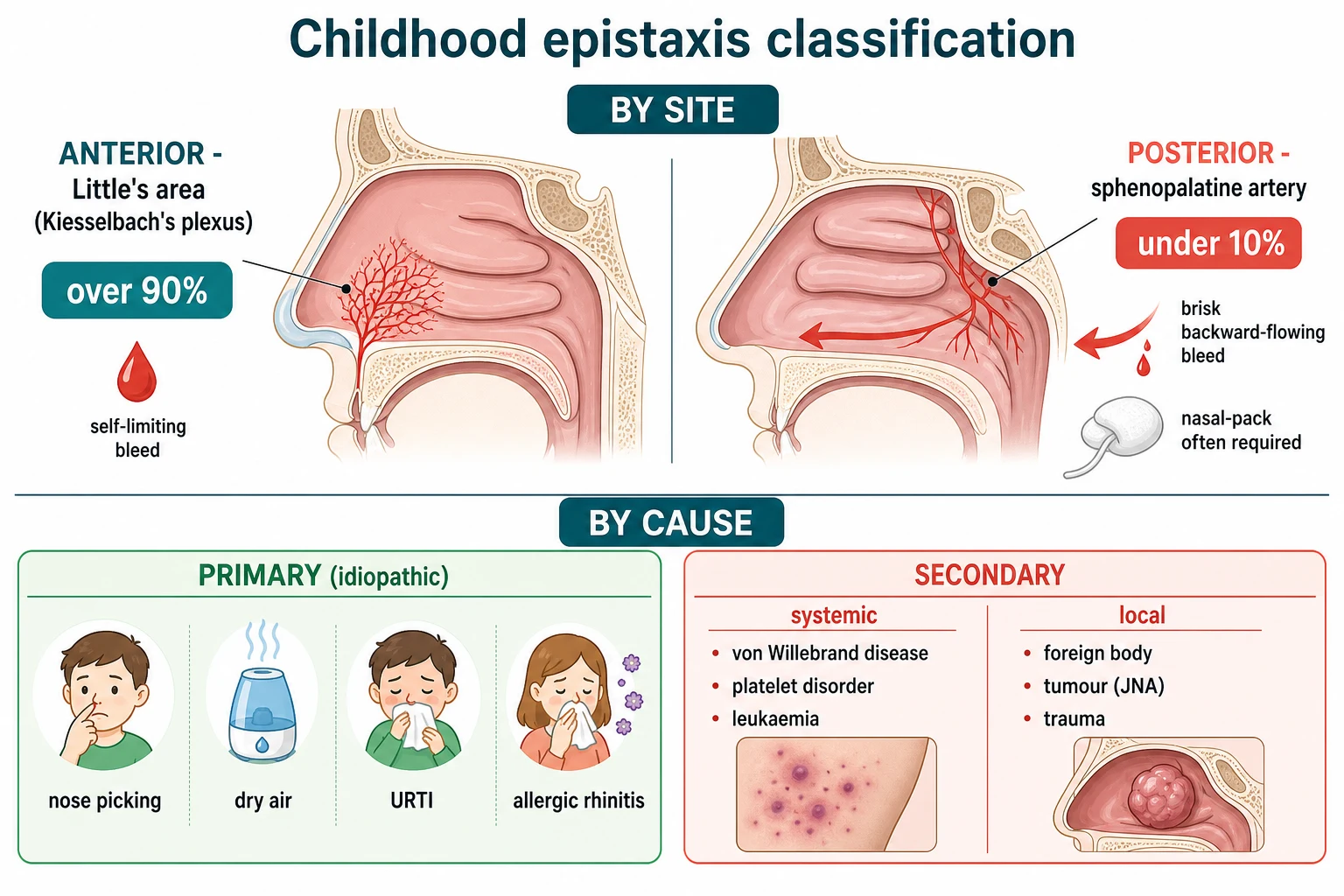
Epistaxis is bleeding from the rich vascular network of the nasal mucosa. The nose is one of the most vascular structures in the child, and its vessels lie under a thin mucosa that dries, cracks and bleeds with the least provocation. The defining anatomy is the division into anterior and posterior bleeds: anterior bleeds, overwhelmingly from Little's area (Kiesselbach's plexus) on the anteroinferior nasal septum, account for over 90 percent of childhood epistaxis and are usually mild and self-limiting; posterior bleeds, typically from the sphenopalatine artery, are rarer in children but more profuse, harder to control, and more likely to need packing or specialist care. [1] [3]
What makes the topic examinable is the gap between how common and how benign it usually is, and the few features that signal danger. Most childhood epistaxis is primary (idiopathic), driven by nose picking and dry air, and resolves with simple measures. The minority that is recurrent, posterior, bilateral, profuse or accompanied by systemic signs forces a different response — a bleeding-disorder work-up, a search for a tumour such as juvenile nasopharyngeal angiofibroma, or escalation to cautery and packing. Reading that distinction, and teaching correct first aid, is the core of the topic. [2]
Classification
Classify epistaxis by where it bleeds from and by what drives it, because the site sets the management and the cause sets the investigation. The single most useful split is anterior versus posterior, and within anterior disease the primary (idiopathic) versus secondary distinction decides whether you investigate. [1]
Epistaxis in children classified by site and cause
The classification does the triage. An unilateral anterior bleed that stops with pressure in a well child is primary and needs only prevention advice. A posterior or uncontrolled bleed moves you to cautery and packing. And recurrent bleeding with systemic signs or an adolescent mass moves you to investigation and specialist referral — never simply label a persistent unilateral adolescent bleed as nose picking. [2] [12]
Epidemiology & Risk Factors
Epistaxis is one of the commonest complaints of early childhood. Around half of children will have had at least one nosebleed by the time they finish primary school, with a peak between two and ten years of age, and fewer than one in ten of these bleeds ever reaches a doctor. The vast majority are anterior, brief and benign — which is exactly why the dangerous minority must be actively looked for rather than assumed away. [1]
The core risk factors are mechanical and environmental. Digital trauma (nose picking) is the dominant precipitant, amplified by dry air and low humidity, upper-respiratory-tract infection with its congested inflamed mucosa, and allergic rhinitis with chronic inflammation. Together these thin and crack the mucosa over Little's area and expose the underlying vessels. The seasonal pattern — worse in winter and in heated, dry homes — reflects this drying effect. [1] [3]
The systemic risk factors are less common but define the cases that need investigation. An underlying bleeding disorder, of which von Willebrand disease is the commonest inherited cause, accounts for an appreciable minority of children with recurrent epistaxis, and platelet disorders, haemophilia and, rarely, leukaemia also present this way. Drug exposure — non-steroidal anti-inflammatory drugs and anticoagulants — adds to bleeding tendency, and a family history of bleeding or surgery-related bleeding is the single most useful historical clue to an inherited disorder. [2]
Pathophysiology
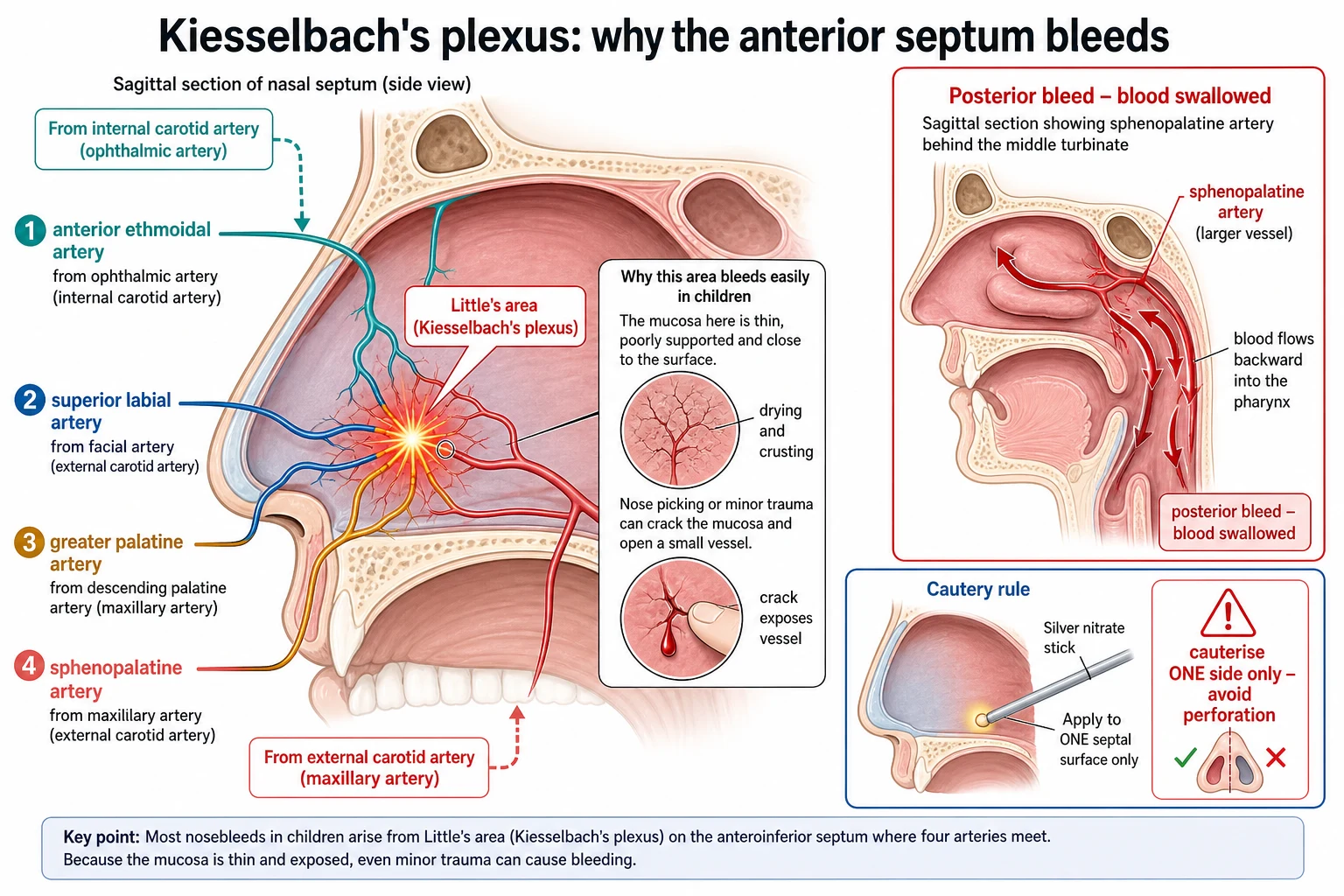
Why does the child bleed from the front of the nose, and why does the anterior septum bleed so readily? The answer is the vascular anatomy of Little's area (Kiesselbach's plexus), and it explains both the site of the common bleed and the strategy of first aid and cautery. [3]
Little's area is a shallow plexus on the anteroinferior nasal septum where four arteries converge: the anterior ethmoidal artery (a branch of the ophthalmic artery, from the internal carotid), and the superior labial artery, the greater palatine artery and the sphenopalatine artery (all branches of the external carotid via the maxillary and facial arteries). This confluence — a watershed between the internal and external carotid circulations — lies directly under a thin, dry mucosa that is exposed to the drying airstream and to the child's finger. That is why digital trauma and dry air produce bleeding here so reliably, and why firm pressure on the soft nose, or cautery of the visible vessel, controls it. [1] [3]
Posterior bleeds behave differently. They arise further back, typically from the sphenopalatine artery as it enters the nose behind the middle turbinate. These vessels are larger, the bleeding is brisker, and blood runs posteriorly into the pharynx to be swallowed and vomited rather than dripping from the nostril. Pressure on the soft nose may not reach the source, so posterior bleeds more often need topical vasoconstriction, cautery under view, or packing. The same thin mucosa that makes the anterior septum vulnerable also explains why cautery must be limited to one side of the septum: devascularising opposing surfaces risks septal perforation, the classic iatrogenic complication of over-zealous bilateral cautery. [6]
Clinical Presentation
Read the bleed by its site, its duration and its company, because the presentation does most of the diagnostic work. [1]
The typical anterior bleed is what the worried parent describes on the phone: blood drips from one nostril, often after nose rubbing, a cold, or a hot dry night; it is usually brief, and it settles within minutes if pressure is applied to the soft part of the nose. Between episodes the child is entirely well, and anterior rhinoscopy may show a prominent vessel, a crust or a small telangiectatic point on the anteroinferior septum. This is the benign majority, and the history alone points to it. [1] [4]
The posterior bleed announces itself differently. The bleeding is brisk, the child may swallow large volumes and present with vomiting frank or coffee-ground blood, and blood may come from both nares as it tracks forward from the posterior source. These bleeds do not settle with simple pressure, last longer than 15 to 20 minutes, and may be associated with pallor, tachycardia or signs of significant blood loss. Any child who vomits blood after a nosebleed, or who bleeds from both sides, should be assumed to have a posterior source until proven otherwise. [4]
Recurrent epistaxis is its own presentation. The child has multiple short anterior bleeds over weeks or months, usually from one side, with normal wellbeing between episodes. The questions that matter here are about duration and progression, the family history of bleeding, easy bruising or other bleeding, and drug use — because recurrent disease is the doorway to the bleeding-disorder work-up and to the rare tumour. An adolescent boy with recurrent unilateral epistaxis and progressive nasal obstruction is not a simple nose-picker; think juvenile nasopharyngeal angiofibroma. [2] [12]
Differential Diagnosis
Build the differential by site first, then by cause, and strip out the mimics that are not true epistaxis. [1]
The local causes sit at the top of the list. Digital trauma and dry air account for most anterior bleeds; upper-respiratory-tract infection and allergic rhinitis inflame the mucosa; a foreign body (classically a unilateral, foul-smelling discharge, occasionally bloodstained) must be considered in the younger child; trauma, including the possibility of non-accidental injury and base-of-skull fracture with cerebrospinal-fluid rhinorrhoea, comes from the history; and a nasal or nasopharyngeal tumour, of which juvenile nasopharyngeal angiofibroma is the classic vascular tumour of the adolescent boy, presents with progressive unilateral obstruction and bleeding. [1] [12]
The systemic causes are fewer but more dangerous. An inherited bleeding disorder — von Willebrand disease first, then platelet-function disorders and the haemophilias — presents with recurrent or prolonged bleeding from multiple sites. Acquired disorders include immune thrombocytopenia and, rarely, leukaemia presenting with pancytopenia and petechiae. Drug-induced bleeding from non-steroidal anti-inflammatory drugs or anticoagulants, and rare vascular malformations such as hereditary haemorrhagic telangiectasia, complete the systemic list. The practical pivot is to use the side, frequency, duration and the company the bleed keeps to separate the benign anterior majority from the systemic and structural minority. [2]
The common mimic is blood-stained vomitus or saliva misattributed to the nose: a posterior nosebleed swallowed and vomited, haemoptysis from a chest source, or haematemesis. A careful history of the onset and the colour, and direct examination of the nasal cavity, separates a true epistaxis from these. [4]
Clinical & Bedside Assessment
Begin with the history, because in epistaxis the story directs both the immediate management and the decision to investigate. Ask about the side and frequency of the bleeds, their duration and whether they stop with pressure, any precipitants (picking, colds, allergy, trauma, dry air), the family history of bleeding and any easy bruising, gum bleeding or heavy periods, and the child's medications. A family history of bleeding or surgery-related bleeding is the single most useful clue to an inherited disorder. [1]
Examine the child calmly once the bleed is controlled, or apply first aid while you take the history. Perform anterior rhinoscopy with a headlight and speculum, or gentle examination with an auriscope, looking specifically at Little's area on the anteroinferior septum for a visible vessel, fresh clot, crust or telangiectasia. Check the other nostril, look for a foreign body, polyp or mass, and inspect the oropharynx for blood trickling from the posterior nares that would signal a posterior source. Examine the skin for bruising and petechiae and the gums for bleeding, and take the vital signs to gauge the volume of loss. [1] [4]
Assess and teach first-aid technique at every encounter, because the commonest failure is incorrect technique. The correct sequence is: sit the child upright, lean them forward, and apply firm continuous pressure to the soft, cartilaginous lower part of the nose for at least 10 to 15 minutes while they breathe through the mouth and spit out any blood. The two errors to correct are tilting the head back — which drives blood to the stomach, causing vomiting, and risks aspiration — and pinching the bony bridge, which compresses bone rather than the Little's area vessels and does nothing to stop the bleed. Needs-assessment studies show that even healthcare providers and parents commonly get these steps wrong, which is why explicit teaching is part of the management, not an optional add-on. [8] [9]
Investigations
Most childhood epistaxis needs no investigation at all — the diagnosis and management are clinical. Reserve testing for the recurrent, severe, prolonged or bilateral bleed, and for any child with systemic signs, a family history of bleeding, or an abnormal examination. [1]
For the recurrent case, send a full blood count and film to exclude anaemia from chronic loss and to screen for thrombocytopenia and leukaemia, a coagulation screen (prothrombin time and activated partial thromboplastin time), and iron studies if chronic loss is suspected. Group and save is reserved for the rare, large-volume bleed. These first-line tests catch the common acquired and most inherited disorders and the iron-deficiency anaemia that recurrent epistaxis can produce. [1] [2]
When an inherited bleeding disorder is suspected — a positive family history, prolonged bleeding after cuts or dental work, or recurrent bleeds with an abnormal screen — extend the work-up with von Willebrand factor antigen, ristocetin cofactor activity and factor VIII, and refer to haematology. Von Willebrand disease is the commonest inherited cause of recurrent childhood epistaxis, and it is routinely missed on a basic coagulation screen because the tests can be normal or near-normal. [2]
For the suspected structural cause, imaging is the key investigation. An adolescent boy with unilateral progressive epistaxis and nasal obstruction needs contrast CT and MRI of the nasal cavity and nasopharynx to characterise a juvenile nasopharyngeal angiofibroma before any biopsy is contemplated — biopsy of this highly vascular tumour can cause catastrophic bleeding and must be avoided. Magnetic resonance imaging also defines the vascular extent and the intracranial spread that guide pre-operative embolisation and surgical planning. [12]
[2] [12]Management — Resuscitation
Severe childhood epistaxis is uncommon, but when a bleed will not stop it demands a calm, ordered response that begins with airway, breathing and circulation and ends with definitive control. Apply first aid immediately and correctly — upright, leaning forward, firm continuous pressure on the soft part of the nose — while you assess the child, because correct first aid alone settles the great majority even in the emergency setting. [4]
For the severe or uncontrolled bleed, establish intravenous access, send blood for a full blood count, coagulation screen and group and save, and give fluid resuscitation for signs of significant volume loss. Reassess the airway constantly: a child swallowing large volumes of blood can vomit and aspirate, which is why the upright, forward position is not just a comfort measure but an airway protection measure. Do not allow the child to lie supine and bleed. [4] [2]
Escalate beyond first aid when the bleed persists after 15 to 20 minutes of correct pressure. The next steps are topical vasoconstriction, then silver-nitrate cautery of the identified bleeding point, then nasal packing, with ENT referral for the posterior or refractory bleed. The decision to escalate is made on the duration and severity of the bleed and on whether a bleeding point is visible, not on a fixed protocol — and it is always paired with explicit first-aid teaching for the family before discharge. [1] [8]
Management — Definitive & Stepwise
Once the bleed is controlled, definitive management moves in a clear stepwise order, and for the recurrent case it adds prevention. The aim is to stop the current bleed with the least invasive effective measure and to reduce recurrence. [1]
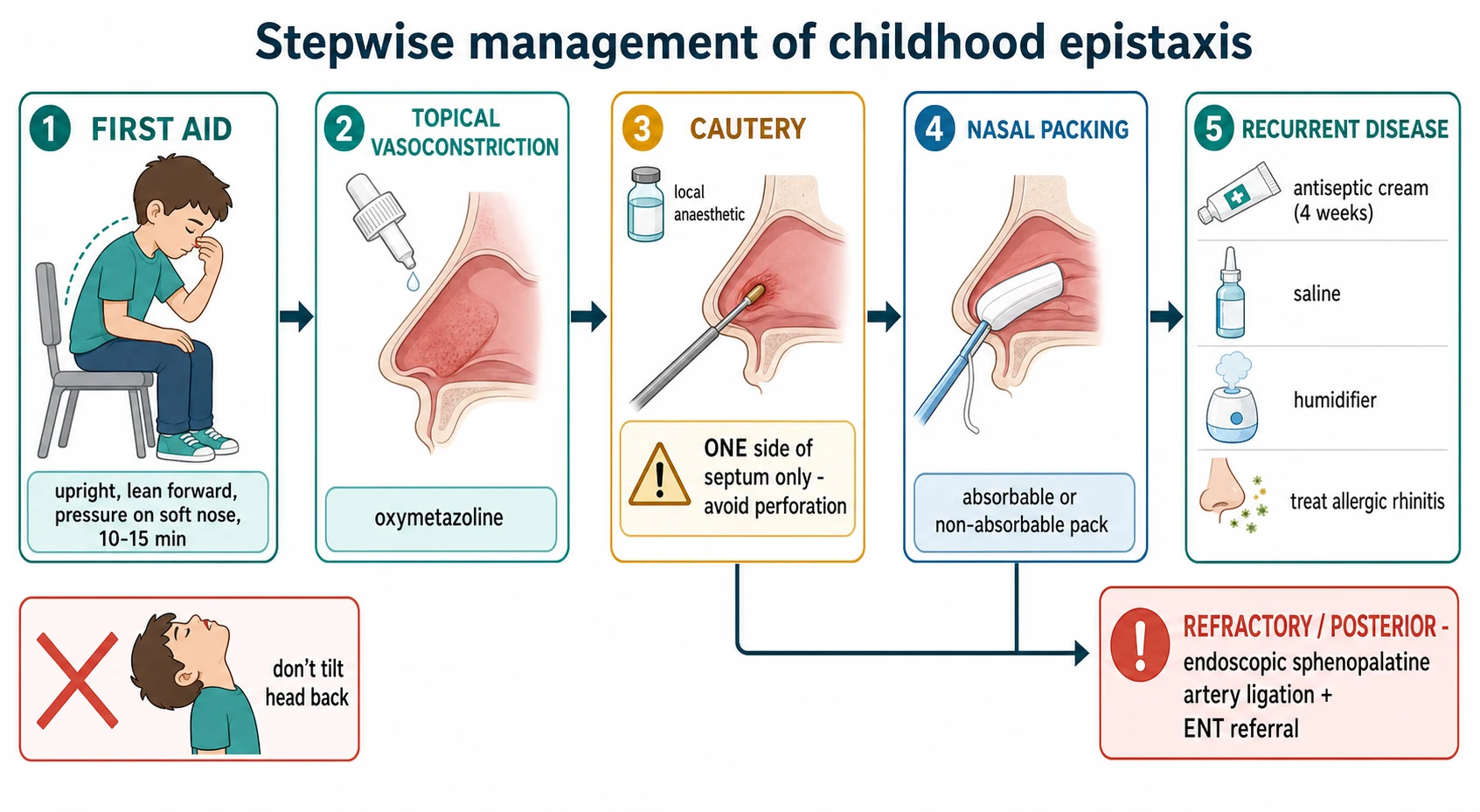
Stepwise management of childhood epistaxis
First aid — sit upright, lean forward, apply firm continuous pressure to the soft part of the nose for at least 10 to 15 minutes, breathe through the mouth and spit out blood; teach the family the technique.
Topical vasoconstriction — apply a topical decongestant such as oxymetazoline to the bleeding mucosa to constrict the vessel, with appropriate age caution in infants.
Silver-nitrate cautery — under topical local anaesthesia, apply silver nitrate to the visible bleeding point on the anterior septum, cauterising one side of the septum to avoid perforation.
Nasal packing — if cautery fails or no point is visible, insert an absorbable or non-absorbable nasal tampon; consider antibiotic cover for packs left beyond 24 to 48 hours and arrange ENT review.
Recurrent disease — antiseptic or antibiotic nasal cream to the septum, cautery of a persistent vessel, treat allergic rhinitis and dry air, and safety-net advice.
Refractory or posterior — urgent ENT referral for endoscopic sphenopalatine artery cautery or ligation, and rarely embolisation.
For recurrent childhood epistaxis, the evidence supports two simple, effective measures. A randomised controlled trial showed that antiseptic nasal cream (chlorhexidine with neomycin) applied to the anterior septum significantly reduces the frequency of bleeds, and a systematic review and meta-analysis confirmed that adding silver-nitrate cautery to antiseptic cream further reduces recurrence when a visible vessel persists. These measures, combined with treating allergic rhinitis with intranasal steroid and saline, humidifying dry air, and discouraging nose picking, form the backbone of recurrent-disease management — and most children simply grow out of it. [11] [5]
The principle that protects the septum is the one-side rule of cautery. Silver-nitrate cautery works by chemical devascularisation, and applying it to opposing surfaces of the septum strips both sides of their blood supply and risks septal perforation — so cauterise the identified bleeding point on one surface only, under topical local anaesthesia, for a brief controlled application. A study of bilateral septal cauterisation in children found it effective when carefully applied, but the conservative default taught to trainees remains single-surface cautery of the bleeding vessel. [6] [7]
Silver nitrate cautery (anterior epistaxis)
Dose
75 percent silver nitrate applicator, brief application to the bleeding point
Topical vasoconstrictor (severe or persistent anterior bleed)
Dose
Oxymetazoline 0.05 percent nasal solution applied to the bleeding mucosa
Antiseptic nasal cream (recurrent epistaxis)
Dose
Chlorhexidine with neomycin cream applied to the anterior nasal septum
Specific Subtypes & Scenarios
The scenarios below are the ones examiners reach for, because each forces a different decision under pressure. [1]
The typical anterior bleed at home is the commonest scenario. Blood drips from one nostril after nose rubbing in a warm room; the child is well. The answer is correct first aid — upright, leaning forward, firm pressure on the soft part of the nose for at least 10 to 15 minutes — followed by prevention advice: saline, a thin smear of cream or petroleum jelly to the septum, humidification, and discouraging nose picking. Most of these never need a doctor. [8]
Recurrent epistaxis in a well child is the outpatient scenario. Multiple short anterior bleeds over weeks, a visible vessel on the septum, and a normal systemic examination. The answer is antiseptic nasal cream for about four weeks, cautery of the visible vessel if bleeds persist, treatment of allergic rhinitis, and a first-line work-up (full blood count, coagulation screen, iron studies) to catch the bleeding disorder and iron-deficiency anaemia. Reassure the family that most children grow out of it. [11] [1]
Recurrent epistaxis with bruising and a family history of bleeding is the work-up scenario. Here the answer is to stop and investigate before cautery: a full blood count and coagulation screen, then von Willebrand factor antigen, ristocetin cofactor and factor VIII, and haematology referral. Von Willebrand disease is the commonest inherited cause, and cautery without a work-up can both miss the diagnosis and cause prolonged post-procedural bleeding. [2]
Unilateral progressive epistaxis with obstruction in an adolescent boy is the tumour scenario. The answer is juvenile nasopharyngeal angiofibroma until proven otherwise: contrast CT and MRI of the nasopharynx, no clinic biopsy, and ENT referral for embolisation and surgical resection. Missing this vascular tumour, or biopsying it and provoking catastrophic bleeding, is the cardinal error. [12]
Complications & Pitfalls
The cardinal pitfall is wrong first-aid technique, taught or allowed to persist. Tilting the head back drives blood to the stomach — causing vomiting, distress and the small but real risk of aspiration — and pinching the bony bridge fails to compress the Little's area vessels, so the bleed continues. Needs-assessment studies confirm these errors are common even among healthcare providers, which is why explicit technique teaching is part of the management. [8] [9]
The iatrogenic complication is septal perforation from bilateral or over-zealous silver-nitrate cautery. Cautery works by chemical devascularisation, and stripping both sides of the septal blood supply kills the cartilage and leaves a permanent perforation. The rule is to cauterise the identified bleeding point on one surface of the septum only, under topical local anaesthesia, for a brief controlled application. [6]
The systemic complications are iron-deficiency anaemia from chronic recurrent blood loss — easily missed because each individual bleed is small — and, in the rare large-volume posterior bleed, haemodynamic compromise requiring resuscitation. A full blood count and iron studies are part of the recurrent-disease work-up precisely to catch the anaemia. [1]
The diagnostic pitfall is labelling a persistent or recurrent bleed as simple nose picking and missing the underlying cause. A bleeding disorder missed because no family history was taken, a juvenile nasopharyngeal angiofibroma dismissed as a blocked nose, and a foreign body overlooked in the unilateral case are the recurring errors. The protection is to investigate the recurrent, prolonged or unilateral bleed and to look for the systemic and structural red flags at every encounter. [2] [12]
Prognosis & Disposition
The prognosis of childhood epistaxis is excellent, because the overwhelming majority are anterior, benign and self-limiting, and most children simply grow out of the recurrent pattern by their early teens. Reassurance is a legitimate and important part of the disposition, provided the red flags have been excluded. [1]
Discharge the well child with controlled anterior epistaxis on correct first-aid teaching and prevention advice, with a clear safety-net: return if a bleed does not stop after 15 to 20 minutes of correct pressure, if bleeds become frequent or prolonged, or if there is bruising, pallor or systemic upset. The safety-net is what makes outpatient management safe for a condition whose dangerous minority cannot always be predicted at the first encounter. [8]
Admit or refer the child with a posterior or uncontrolled bleed, significant blood loss, an underlying bleeding disorder, or a suspected tumour. These children need cautery, packing, transfusion or specialist imaging and surgery. The durable interventions that reduce recurrence — antiseptic cream, cautery of a visible vessel, allergic-rhinitis treatment, humidification, and first-aid education — keep most children out of hospital and reduce re-presentation. [2] [4]
Special Populations
Children with an inherited bleeding disorder, above all von Willebrand disease, are over-represented among recurrent epistaxis presentations; identify them by the family history and the pattern of multi-site bleeding, and manage jointly with haematology, because standard cautery may be followed by prolonged oozing without factor or desmopressin cover. [2]
The adolescent boy with unilateral progressive epistaxis and obstruction defines the juvenile-nasopharyngeal-angiofibroma risk; the protection is to image rather than assume, and to refer to ENT for embolisation and resection. Never biopsy this tumour in clinic. [12]
Aboriginal and Torres Strait Islander, Maori, Pasifika, refugee, asylum-seeking and migrant families, and children in remote and disadvantaged communities, carry a disproportionate burden of undertreated allergic rhinitis, dry overcrowded housing and limited access to first-aid education, all of which drive recurrent epistaxis. Provide culturally safe care, trained interpreters, and practical first-aid and humidification advice, and treat the household's allergic and infectious disease — the nosebleed is often a marker of broader access gaps. [1]
Children with disability or neurodevelopmental difference may have persistent nose picking or self-injury that drives recurrent bleeding; behavioural strategies, protective measures and carer education sit alongside the standard management. Telehealth and rural pathways can deliver first-aid teaching and triage to families far from specialist services, reserving travel for the child who genuinely needs cautery, packing or imaging. [8]
Evidence, Guidelines & Regional Differences
The named regional guidance is the AAO-HNS Clinical Practice Guideline: Nosebleed (Epistaxis), the Royal Children's Hospital Melbourne epistaxis guideline and eTG, ENT UK, and NICE Clinical Knowledge Summaries. In ANZ the RCH and eTG guidance is the practical reference, and it emphasises correct first aid, cautious use of cautery and packing, and a low threshold for the bleeding-disorder work-up in recurrent disease. [2]
The recurrent-disease evidence is strong and practical. A randomised controlled trial established that antiseptic nasal cream reduces the frequency of recurrent childhood epistaxis, and a systematic review and meta-analysis confirmed that adding silver-nitrate cautery to antiseptic cream further reduces recurrence when a visible vessel persists. Studies comparing cautery techniques and agents in paediatric epistaxis continue to refine practice, with silver nitrate remaining the standard chemical cautery. [11] [5]
The first-aid evidence is sobering and practice-defining. Needs-assessment and knowledge studies show that a large proportion of healthcare providers and parents apply incorrect first aid — tilting the head back, pinching the bony bridge, or releasing pressure too soon — which is why explicit technique teaching is treated as a clinical intervention, not an optional courtesy. The evidence supports firm continuous pressure on the soft part of the nose for at least 10 to 15 minutes, leaning forward, as the single most effective first-aid measure. [8] [9]
[2] [8]Exam Pearls
Epistaxis in children is bleeding from the nasal mucosa, and the exam lives on the anterior-versus-posterior and primary-versus-secondary distinctions. Over 90 percent are anterior, from Little's area (Kiesselbach's plexus), driven by nose picking, dry air, infection and allergy, peaking at two to ten years. [1]
Correct first aid is the most tested skill: sit upright, lean forward, and apply firm continuous pressure to the soft part of the nose for at least 10 to 15 minutes. Escalation moves from topical vasoconstriction through silver-nitrate cautery of the visible point on one side of the septum to nasal packing, with ENT referral for the refractory or posterior bleed. [8] [6]
Recurrent disease responds to antiseptic nasal cream for about four weeks and cautery of a visible vessel, with a first-line work-up of full blood count, coagulation screen and iron studies. The red flags are the bleeding disorder (von Willebrand disease is the commonest inherited cause), the adolescent boy with unilateral obstruction (juvenile nasopharyngeal angiofibroma — image, never biopsy), and the uncontrolled posterior bleed. [11] [12]
References
- [1]Svider P; Arianpour K; Mutchnick S; et al Management of Epistaxis in Children and Adolescents: Avoiding a Chaotic Approach. Pediatr Clin North Am, 2018.PMID 29803286
- [2]Tunkel DE; Anne S; Payne SC; et al Clinical Practice Guideline: Nosebleed (Epistaxis). Otolaryngol Head Neck Surg, 2020.PMID 31910111
- [3]Melia L; McGarry GW Epistaxis: update on management. Curr Opin Otolaryngol Head Neck Surg, 2011.PMID 21150620
- [4]Béquignon E; Teissier N; Gauthier A; et al Emergency Department care of childhood epistaxis. Emerg Med J, 2017.PMID 27542804
- [5]Alsaif A; Karam M; Alhaider A; et al The addition of silver nitrate cautery to antiseptic nasal cream for patients with epistaxis: A systematic review and meta-analysis. Int J Pediatr Otorhinolaryngol, 2020.PMID 32998847
- [6]Link TR; Conley SF; Flanary V; et al Bilateral epistaxis in children: efficacy of bilateral septal cauterization with silver nitrate. Int J Pediatr Otorhinolaryngol, 2006.PMID 16621035
- [7]Schafer AD; McNutt M; Fulmer A; et al Comparing recurrence between cautery techniques in pediatric epistaxis. Int J Pediatr Otorhinolaryngol, 2024.PMID 37979255
- [8]Sowerby L; Rajakumar C; Davis M; et al Epistaxis first-aid management: a needs assessment among healthcare providers. J Otolaryngol Head Neck Surg, 2021.PMID 33573695
- [9]Boldes T; Zahalka N; Kassem F; et al Epistaxis first-aid: a multi-center knowledge assessment study among medical workers. Eur Arch Otorhinolaryngol, 2024.PMID 38748311
- [10]Ahmed AE; Abo El-Magd EA; Hasan GM; et al A comparative study of propranolol versus silver nitrate cautery in the treatment of recurrent primary epistaxis in children. Adolesc Health Med Ther, 2015.PMID 26457059
- [11]Kubba H; MacAndie C; Botma M; et al A prospective, single-blind, randomized controlled trial of antiseptic cream for recurrent epistaxis in childhood. Clin Otolaryngol Allied Sci, 2001.PMID 11843924
- [12]Singh RK; Lakhkar BB; Patwa PA; et al Juvenile nasopharyngeal angiofibroma. BMJ Case Rep, 2022.PMID 35260405