Paeds · ent-hearing-and-oral-health
Mastoiditis and otogenic complications
Also known as Acute mastoiditis · Coalescent mastoiditis · Masked mastoiditis · Bezold abscess · Gradenigo syndrome · Lateral sinus thrombosis · Otitic hydrocephalus · Otogenic intracranial complications
Fellowship topic on mastoiditis and otogenic complications in children: acute mastoiditis as the commonest suppurative complication of acute otitis media through the contiguous mastoid air-cell system; coalescent and masked forms; the intratemporal complications from subperiosteal and Bezold abscess through Gradenigo petrositis, facial palsy and labyrinthitis to lateral sinus thrombosis; the intracranial complications of meningitis, extradural and subdural empyema, brain abscess and otitic hydrocephalus; the postauricular swelling and the down-and-out pinna, the Streptococcus pneumoniae, pyogenes, Staphylococcus aureus and Pseudomonas microbiology; the contrast temporal-bone CT findings of coalescence; the intravenous antibiotic regimen and the cortical mastoidectomy, myringotomy and needle-aspiration decisions; and ANZ, UK and North American guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a fourteen-month-old brought to the emergency department with three days of fever, a runny nose and ear-pulling. The ear looked red yesterday and the family doctor started oral amoxicillin. Today the child is more unsettled, the temperature is 39.2 degrees Celsius, and behind the right ear the skin is red, swollen and tender to touch, with the pinna sitting lower and jutting further out than the left. This is acute mastoiditis, and the shift from a treatable ear infection to a surgical threat has happened overnight. The clinician's job is to see the postauricular change, to start intravenous antibiotics and to involve the ear-nose-and-throat surgeon before the infection erodes the cortical bone and reaches the neck, the venous sinuses or the brain. [4] [5]
The mastoid process is the bony prominence behind the pinna, and in the older child and adult it is honeycombed with air cells that open into the middle ear through the aditus ad antrum. Because this connection is wide and valveless, middle-ear infection reaches the mastoid in nearly every case of AOM. Acute mastoiditis is symptomatic inflammation and suppuration of these air cells with the clinical signs of postauricular inflammation — the stage at which the inflamed but draining mastoid of simple AOM has become an infected, obstructed cavity. [9] The inflammation moves through a continuum: an early mucosal stage, then empyema of the air cells, then coalescence as the rising pressure and osteitis dissolve the thin bony trabeculae and threaten the cortical plates. [5]
Most acute mastoiditis resolves with prompt intravenous antibiotics, and the modern child who reaches hospital early rarely needs surgery. The danger lies in the complications that follow when the cortical bone is breached: the intratemporal collections in the neck and petrous apex, the facial nerve and labyrinth, and the intracranial structures reached through the tegmen, the sigmoid plate and the valveless venous channels. The task is layered — recognise the postauricular signs, image for the complication, treat with broad intravenous antibiotics, and time the surgical drainage so that the abscess is drained and the sinus decompressed before hearing, the facial nerve or the brain is lost. [1] [3]
Classification
The clinical framework examiners use frames mastoiditis as a continuum of increasing extension, from a confined mucosal infection through cortical breach to intracranial spread, and separates the complications into intratemporal and intracranial groups. Thinking in these layers keeps the assessment and the urgency clear. [5] [2]
At the mastoid itself, the progression runs from acute (mucosal) mastoiditis — inflammation of the air-cell mucosa with periostitis but intact trabeculae and cortex — to acute coalescent mastoiditis, in which osteitis and raised pressure destroy the bony trabeculae and thin the cortical plates. When the lateral cortical plate gives way, pus forms a subperiosteal abscess behind the ear; when the mastoid tip gives way inferiorly, it tracks into the neck as a Bezold abscess. A smouldering, partially treated form called masked (latent) mastoiditis can run a subacute course with minimal signs yet progressive bony destruction, and it is the diagnosis to consider in the child with persistent otalgia and raised inflammatory markers after incomplete antibiotic treatment. [5] [9]
Beyond the mastoid, the intratemporal complications are petrous apicitis producing the Gradenigo triad, suppurative labyrinthitis, facial nerve palsy, and lateral sinus thrombosis arising from erosion of the sigmoid plate. The intracranial complications are meningitis, extradural and subdural empyema, brain abscess, and otitic hydrocephalus from impaired venous drainage. Meningitis is the commonest intracranial complication; lateral sinus thrombosis and brain abscess carry the highest mortality. [1] [2]

Epidemiology & Risk Factors
Acute mastoiditis is overwhelmingly a disease of young children. The peak incidence sits in the first two years of life, and most series report a median age between one and three years, reflecting the early, incomplete pneumatization of the mastoid and the frequency of viral upper-respiratory infection and AOM in infants and toddlers. Boys are affected slightly more often than girls. The complication-pneumatization link matters: the infant mastoid is poorly aerated, so mucosal swelling occludes the aditus more readily and traps pus under pressure. [5] [8]
The incidence of mastoiditis fell steeply through the antibiotic era, and the introduction of pneumococcal conjugate vaccines further reduced the burden of Streptococcus pneumoniae disease. The risk of mastoiditis after AOM remains low — well under one per cent of episodes — but because AOM is so common, mastoiditis is still the most frequent suppurative complication of middle-ear infection that reaches hospital. The systematic review of paediatric management confirmed that incidence figures vary widely by region, immunisation uptake and access to antibiotics. [8] [3]
The children who develop complications rather than simple mastoiditis share recognisable vulnerabilities. Immunocompromise, chronic suppurative otitis media and cholesteatoma predispose to aggressive and Pseudomonas-driven disease; delayed or incomplete antibiotic treatment allows masked mastoiditis; and anatomical anomalies of the ear and eustachian tube impair drainage. Crucially, the burden of otitis media and its complications is far higher in Aboriginal and Torres Strait Islander, Maori and Pasifika children, among whom chronic suppurative otitis media and its sequelae are endemic and the threshold for complication is lower still. [10] [3]
In Australia and Aotearoa New Zealand, the Royal Children's Hospital Melbourne clinical practice guideline frames acute otitis media and its mastoid complication as a high-priority presentation requiring early intravenous antibiotics for the postauricular signs, prompt contrast temporal-bone CT for any complication, and coordinated care between paediatrics, ear-nose-and-throat surgery and audiology. The Australian Therapeutic Guidelines set the empiric antibiotic choices, with regional variation in pneumococcal and staphylococcal susceptibility guiding the regimen. For Aboriginal and Torres Strait Islander children, who carry one of the highest reported rates of otitis media and its suppurative complications in the world, the management pathway is embedded in culturally safe, community-linked care that does not let distance delay treatment. [10]
The microbiology has shifted with vaccination and antibiotic pressure. Streptococcus pneumoniae remains the single most common organism in acute mastoiditis in many series, with Streptococcus pyogenes and Staphylococcus aureus also prominent; non-typeable Haemophilus influenzae contributes in young children. When the source is chronic suppurative otitis media or cholesteatoma, Pseudomonas aeruginosa and anaerobes dominate and demand a different empiric regimen. Haemophilus influenzae type b, once a feared cause of invasive disease, is now rare in immunised populations but must be considered in the unvaccinated child. [3] [5]
Pathophysiology
Why does a child with a common ear infection develop a surgical mastoid disease? The answer lies in the anatomy of the mastoid air-cell system and its wide, valveless connection to the middle ear, and in the routes by which an obstructed, pus-filled mastoid reaches the neck, the venous sinuses and the brain. [5] [4]
In AOM, the middle-ear mucosa becomes inflamed and exudative, and the effusion communicates freely with the mastoid air cells through the aditus ad antrum. In most children the system drains, the infection is contained, and the mastoid inflammation of simple AOM resolves with the ear. The trouble begins when mucosal swelling at the aditus blocks outflow. Trapped pus raises pressure within the air cells, the mucosa becomes an empyema, and the inflammatory osteitis begins to dissolve the thin bony trabeculae that separate the cells. This is coalescence — the histological and radiological point at which acute mastoiditis becomes surgical disease, because the weakened cortical bone is now a route of escape for pus. [9] [5]
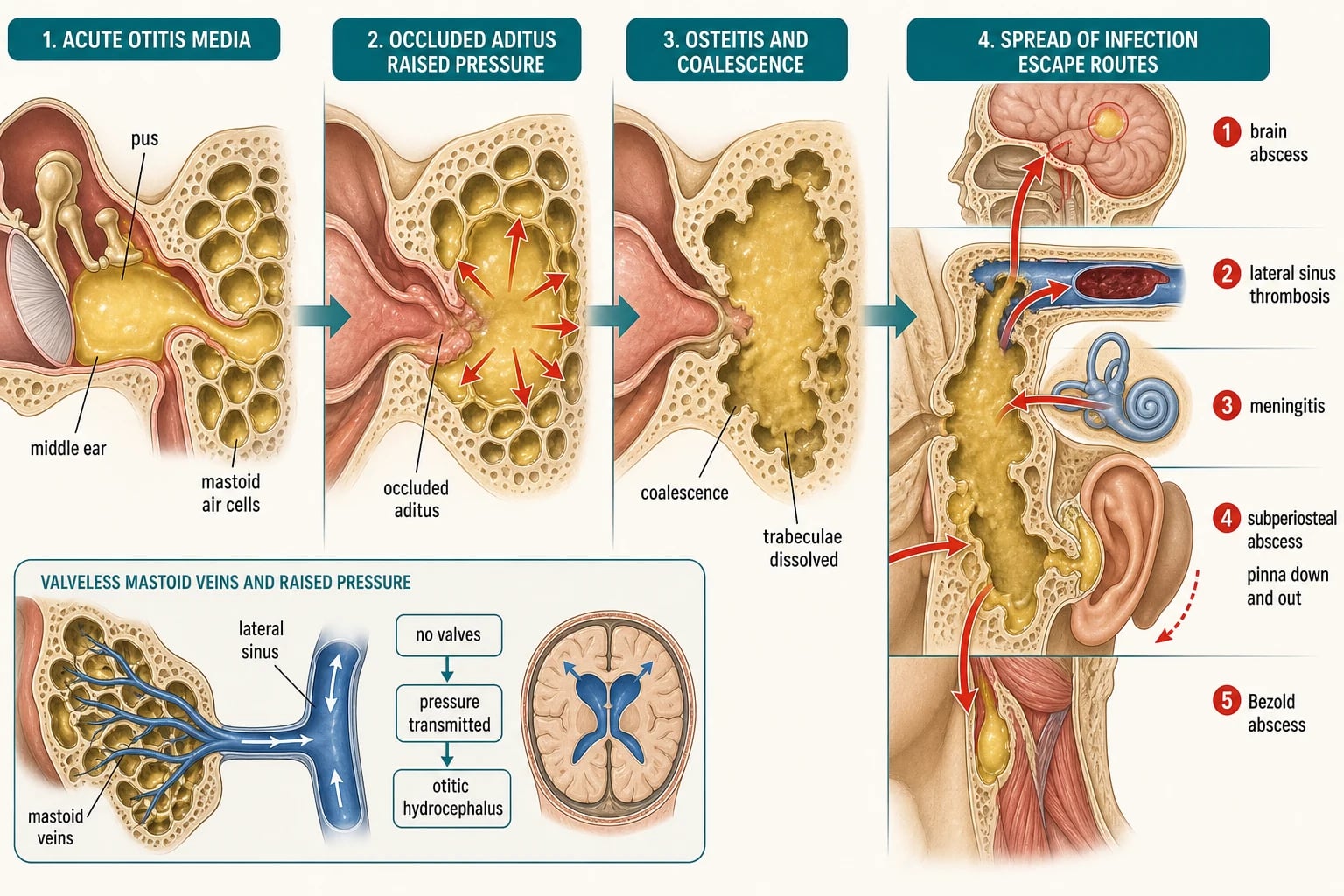
The routes of spread explain every complication. Erosion of the lateral cortical plate produces a subperiosteal abscess behind the ear, the commonest surgical presentation. Erosion inferiorly through the mastoid tip lets pus track down the sternocleidomastoid as a Bezold abscess in the neck. Upward erosion of the tegmen tympani reaches the middle cranial fossa as an extradural collection or a temporal-lobe abscess. Erosion of the sigmoid plate inoculates the lateral (sigmoid) venous sinus, producing septic thrombus, the spiking picket-fence fevers, and — when venous outflow is blocked — otitic hydrocephalus with raised intracranial pressure and papilloedema. Spread through the oval or round window or a preformed labyrinthine pathway causes suppurative labyrinthitis and thence meningitis, while infection tracking along the petrous apex produces petrous apicitis and the Gradenigo triad. [1] [2]
The venous channels are the key to the most dangerous intracranial spread. The mastoid emissary veins and the lateral sinus form a valveless network connecting the mastoid to the intracranial venous system, so thrombophlebitic spread can seed the sinus, the meninges and the brain without a frank cortical defect. This is why a child with mastoiditis can develop lateral sinus thrombosis or a brain abscess even when the cortical bone appears intact, and why the febrile child with headache, papilloedema or focal neurology demands urgent imaging of the venous sinuses and brain as well as the temporal bone. [11] [2]
Clinical Presentation
The child with acute mastoiditis presents with fever, otalgia and the postauricular signs that distinguish it from uncomplicated AOM. The picture is a febrile, irritable infant or toddler with two to four days of ear symptoms, often after an upper-respiratory infection. Behind the affected ear the skin is erythematous, swollen and tender, the postauricular crease is lost, and the pinna is displaced downward and outward — pushed forward and down by the underlying swelling. Otoscopy usually shows a bulging, erythematous, immobile tympanic membrane, though a ruptured drum with purulent otorrhoea may already be present. [4] [5]
A child with a subperiosteal abscess has the postauricular signs plus a fluctuant, sometimes discharging swelling over the mastoid that displaces the pinna more markedly. A Bezold abscess presents as a fluctuant, tender mass deep to the sternocleidomastoid or in the upper neck, often with restricted neck movement, and it may be the presenting feature when the postauricular signs are subtle. The child with petrous apicitis (Gradenigo syndrome) has the classic triad of discharging ear, deep retro-orbital or temporal pain from trigeminal involvement, and a sixth cranial nerve palsy with diplopia and lateral rectus weakness. [1] [5]
The intracranial complications declare themselves through systemic and neurological deterioration. Lateral sinus thrombosis classically produces a picket-fence spiking fever with ear signs, and may progress to otitic hydrocephalus with headache, vomiting, papilloedema and abducens palsy from raised intracranial pressure. Meningitis presents with headache, photophobia, neck stiffness and altered conscious state. An extradural or subdural empyema or a brain abscess produces progressive headache, fever, vomiting, focal neurology, seizures or depressed consciousness; a cerebellar abscess from sigmoid disease causes ataxia and nystagmus. Any of these in a child with ear disease is an emergency of the highest order. [1] [11]
Differential Diagnosis
The differential of the tender postauricular swelling in a febrile child turns on whether the tympanic membrane and the mastoid are involved. Acute otitis media with prominent mastoid tenderness but no postauricular oedema and a normal pinna position is the commonest mimic, and the line between severe AOM and early mastoiditis is clinical — watch for the postauricular change. Otitis externa and a furuncle of the external auditory canal cause a painful, swollen ear and a tender tragus, with an oedematous canal but a normal middle ear and no postauricular oedema. [4] [3]
[3]For the postauricular swelling itself, consider postauricular lymphadenitis from scalp infection, an infected sebaceous cyst or dermoid, cellulitis of the pinna and perichondritis, and parotitis or suppurative cervical lymphadenitis extending up. When the presentation is atypical, recurrent or poorly responsive, raise atypical infections such as nontuberculous mycobacteria, and the rare temporal-bone neoplasms — Langerhans cell histiocytosis, Ewing sarcoma and rhabdomyosarcoma — which can mimic mastoiditis with destructive temporal-bone lesions. A cholesteatoma should be suspected in any child with chronic or recurrent otorrhoea and a complication. [5] [4]
The critical error is to treat a child with the postauricular signs as simple AOM. A febrile child with postauricular oedema, tenderness and a down-and-out pinna has acute mastoiditis until proven otherwise, and sending them home with oral antibiotics allows progression to coalescence, abscess and intracranial spread. The threshold to admit, to assess the mastoid and to image is deliberately low. [1] [8]
Clinical & Bedside Assessment
The assessment of the child with suspected mastoiditis is a structured search for the postauricular signs and for any complication, because their presence determines admission, imaging and the surgical referral. Begin with the history: the onset and duration of ear symptoms and fever, any preceding upper-respiratory infection, prior ear disease or surgery, otorrhoea, antibiotic treatment and its timing, the immunisation status, and any immunocompromise or chronic illness. Ask specifically about headache, vomiting, photophobia, neck stiffness, diplopia, facial weakness and balance — the symptoms that flag intracranial spread. [4] [5]
The examination is built around the ear and the mastoid. Inspect and palpate the postauricular region for erythema, oedema, tenderness, fluctuance and a lost postauricular crease, and note the pinna position — the downward-and-outward displacement is the key sign in a young child. Perform otoscopy, recognising that the canal may be oedematous or filled with pus; the tympanic membrane is usually bulging, erythematous and immobile, though it may be perforated. Examine the face for a facial nerve palsy, the eyes for a sixth-nerve palsy or papilloedema, the neck for a Bezold abscess, and perform a full neurological examination for meningism, focal signs and altered consciousness. [1] [5]
The mastoiditis assessment — PAST EAR
Assess the systemic state directly. Fever, tachycardia, hypotension and lethargy signal invasive disease and sepsis, and the child should be assessed and resuscitated alongside the ear examination. In the very young infant, who cannot localise pain and in whom the mastoid is poorly pneumatized, the threshold to treat as mastoiditis and to image is lower, because the signs may be subtle and the progression to complication rapid. A child with ear disease who develops headache, neck stiffness, diplopia or a falling conscious state has an intracranial complication until imaging proves otherwise. [1] [3]
Investigations
Investigation is driven by the clinical stage. The child with uncomplicated acute mastoiditis needs blood tests but imaging may be deferred if the response to intravenous antibiotics is prompt. A full blood count, C-reactive protein and blood cultures are obtained before antibiotics; the inflammatory markers are also a baseline against which the response at 48 hours is judged. A pus swab from a discharging ear or a draining abscess, and middle-ear fluid from a myringotomy, should always be sent for Gram stain, culture and susceptibility to guide de-escalation. [5] [8]
The key investigation for any complication is contrast-enhanced computed tomography of the temporal bone and brain. The indications are a suspected subperiosteal or Bezold abscess, lateral sinus thrombosis or intracranial extension; failure to improve or deterioration after 48 hours of intravenous antibiotics; any neurological sign; and any uncertainty about the diagnosis. CT identifies coalescence (destruction of the air-cell trabeculae), fluid in the air cells, cortical erosion, a subperiosteal collection, and intracranial collections. The radiological review of acute mastoiditis established that the coalescent pattern and cortical erosion are the imaging hallmarks that separate surgical from medical disease. [9] [6]
At the Royal Children's Hospital Melbourne and across Australian and New Zealand practice, contrast temporal-bone CT is obtained when postauricular signs are marked, when a subperiosteal or Bezold abscess is suspected, when the child fails to improve on intravenous antibiotics, or when any intracranial feature is present. Magnetic resonance imaging with venography is reserved for suspected lateral sinus thrombosis, otitic hydrocephalus, brain abscess or subdural empyema, where it defines the thrombus, the venous anatomy and the parenchymal lesion better than CT. Imaging must never delay intravenous antibiotics in the deteriorating child. [9] [11]
A lumbar puncture is performed when meningitis is suspected and there is no evidence of raised intracranial pressure or a mass lesion on imaging; in the child with focal neurology, papilloedema or a depressed conscious state, CT precedes the lumbar puncture to avoid herniation. A pure-tone audiogram is arranged once the child is stable and the acute infection controlled, because the sensorineural and conductive consequences of mastoiditis and its treatment must be documented and followed up. [3] [5]
Management — Resuscitation
Resuscitation belongs to the child with mastoiditis and systemic compromise, and to any child with an intracranial complication. The red flags are a febrile, toxic child with marked postauricular signs; a child with a rapidly enlarging subperiosteal or Bezold abscess; and a child with headache, meningism, diplopia, papilloedema or a falling conscious state suggesting lateral sinus thrombosis or intracranial extension. Any of these warrants urgent assessment, intravenous access and senior paediatric, ENT and — where the brain is involved — neurosurgical review. [1] [5]
The immediate priorities are to secure the airway and circulation if the child is shocked, to obtain intravenous access, to take blood cultures, and to start broad-spectrum intravenous antibiotics without delay. Do not wait for imaging or culture results in the deteriorating child — the empiric regimen must cover Streptococcus pneumoniae, Streptococcus pyogenes, Staphylococcus aureus and non-typeable Haemophilus influenzae, with anaerobic cover when chronic disease or an intracranial collection is suspected and Pseudomonas-directed cover when chronic suppurative otitis media or cholesteatoma is the source. Give analgesia and antipyretics, and watch the fluid balance. [8] [3]
Escalate to intensive care for the child with septic shock, lateral sinus thrombosis with raised intracranial pressure, a brain abscess, or a depressed conscious state. Assess and document the facial nerve function and the hearing at presentation and serially, because a new facial palsy or a deteriorating conscious state is the trigger for urgent imaging and surgical intervention. Separate resuscitation from definitive therapy in your mind: the well child with early mastoiditis needs intravenous antibiotics and observation, while the child with an abscess, sinus thrombosis or intracranial spread needs the hospital, the scan, the multidisciplinary team and often the operating theatre. [1] [2]
Management — Definitive & Stepwise
Definitive management is a stepwise pathway matched to how far the infection has spread. Uncomplicated acute mastoiditis takes admission and intravenous antibiotics with close observation; a subperiosteal abscess takes drainage alongside antibiotics; and lateral sinus thrombosis or intracranial spread takes cortical mastoidectomy and multidisciplinary surgery. The art is to recognise the stage, to choose the right intensity, and to reassess at 48 hours so that the medical failure becomes a surgical success. [7] [8]
For uncomplicated acute mastoiditis, admit and start intravenous antibiotics after blood cultures. The standard empiric regimen combines ceftriaxone 50 mg per kilogram (maximum 2 g) once daily intravenously with flucloxacillin 50 mg per kilogram (maximum 2 g) every six hours intravenously, covering the streptococci and staphylococci that dominate paediatric disease. If the tympanic membrane is intact, an early myringotomy (with or without tympanostomy tube insertion) relieves the middle-ear pressure, samples the organism, and is part of first-line management in many units. Add metronidazole 7.5 mg per kilogram (maximum 500 mg) every eight hours intravenously when an intracranial collection or anaerobic disease is suspected, and switch to vancomycin when MRSA is a concern or the child is critically ill. [8] [3]
Mastoiditis and otogenic complications — antibiotic pathway (eTG / RCH / BNFc — confirm locally)
For a subperiosteal abscess, the surgical approach is individualised. Many units drain the abscess and perform a cortical mastoidectomy to clear the diseased mastoid and the source, while selected small abscesses in a young child respond to needle aspiration combined with intravenous antibiotics and close observation — an approach the immediate-needle-aspiration series validated and that may spare some children an operation. The systematic review confirmed that no single strategy fits every child, and that the decision turns on abscess size, the child's clinical state and the local surgical culture. [7] [8]
The stepwise mastoiditis pathway
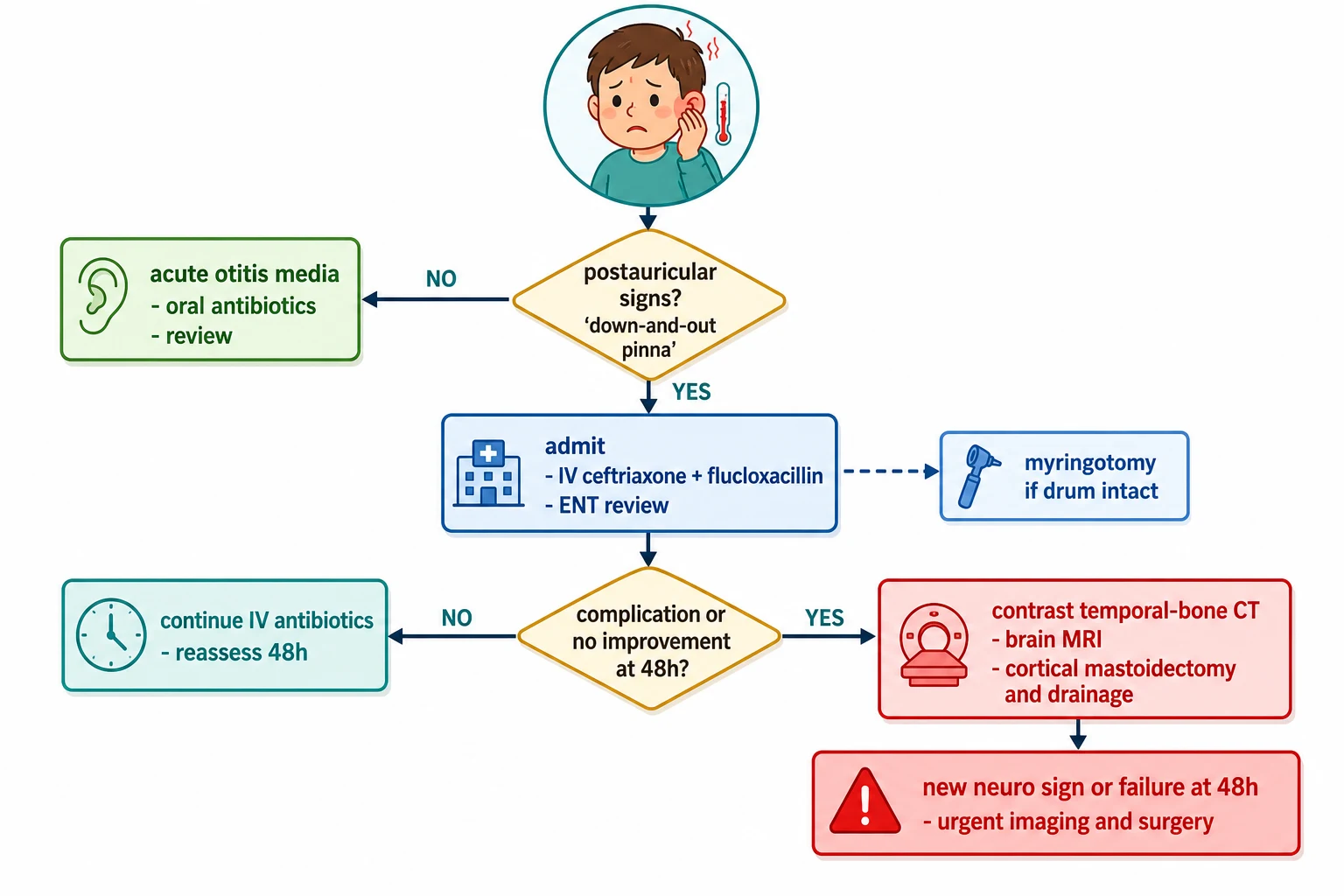
Assess the postauricular signs: fever with postauricular erythema, swelling, tenderness and a down-and-out pinna is acute mastoiditis — admit for intravenous antibiotics and ENT review.
Take blood cultures, start intravenous ceftriaxone 50 mg/kg (max 2 g) once daily plus flucloxacillin 50 mg/kg (max 2 g) every six hours; add metronidazole for intracranial or anaerobic concern and vancomycin for suspected MRSA.
If the tympanic membrane is intact, perform a myringotomy to relieve pressure and sample the organism.
Obtain contrast temporal-bone CT for a suspected subperiosteal or Bezold abscess, lateral sinus thrombosis, intracranial extension, failure to improve at 48 hours, or any neurological sign.
Refer urgently to ENT for combined assessment of the need for drainage or cortical mastoidectomy.
Cortical mastoidectomy and drainage for a subperiosteal or Bezold abscess, lateral sinus thrombosis, facial palsy, Gradenigo syndrome, intracranial extension, or failure of medical therapy at 48 hours.
Add brain MRI with venography for suspected lateral sinus thrombosis, otitic hydrocephalus, brain abscess or subdural empyema, and involve neurosurgery.
Reassess inflammation, facial nerve and hearing serially; transition to oral antibiotics on improvement to complete a three- to four-week course with audiology follow-up.
A cortical mastoidectomy is indicated for failure to improve after 48 hours of intravenous antibiotics, a subperiosteal or Bezold abscess (in most units), lateral sinus thrombosis, Gradenigo syndrome, a facial nerve palsy, suspected cholesteatoma, and any intracranial extension. For lateral sinus thrombosis, the mainstay is cortical mastoidectomy with evacuation of infected clot and granulations alongside prolonged intravenous antibiotics; anticoagulation is controversial and individualised, and sinus decompression or thrombectomy is reserved for selected cases with propagation or persisting raised pressure. The systematic review emphasised that the surgical threshold varies but that the deteriorating child should never be watched for long. [2] [8]
Specific Subtypes & Scenarios
A child with uncomplicated acute mastoiditis. This is the bread-and-butter case. Recognise the postauricular signs, take blood cultures, start intravenous ceftriaxone plus flucloxacillin, perform a myringotomy if the drum is intact, and observe closely. Most children improve within 48 hours and avoid surgery; the inflammatory markers and the clinical state at 48 hours decide the next step. [8] [5]
A child with a subperiosteal abscess. The postauricular swelling is fluctuant and the pinna is markedly displaced. Confirm with contrast temporal-bone CT, and arrange surgical drainage with a cortical mastoidectomy in most units. In a carefully selected young child with a small abscess and no intracranial feature, immediate needle aspiration plus intravenous antibiotics and close observation is a reasonable alternative, with a low threshold to convert to surgery if there is no prompt improvement. [6] [7]
A child with a Bezold abscess. Pus has tracked from the mastoid tip into the neck, presenting as a fluctuant upper-neck or sternocleidomastoid mass. This needs contrast CT of the neck and temporal bone, intravenous antibiotics, and surgical drainage of the neck collection together with a cortical mastoidectomy to clear the source. A Bezold abscess can compromise the airway, so assess and secure the airway early. [1] [5]
A child with lateral sinus thrombosis and otitic hydrocephalus. The febrile child with ear signs develops spiking picket-fence fevers, headache, vomiting, papilloedema and sometimes an abducens palsy from raised intracranial pressure. Contrast CT and MRI with venography confirm the thrombus and the impaired venous outflow. Management is admission, prolonged intravenous antibiotics, cortical mastoidectomy with evacuation of infected clot, and neurosurgical and haematology input — anticoagulation is individualised. The otitic-hydrocephalus series confirmed that recognition and surgical source control underpin a good outcome. [11] [2]
A child with Gradenigo syndrome. The triad of discharging ear, deep retro-orbital pain and a sixth-nerve palsy signals petrous apicitis. Obtain contrast temporal-bone CT and MRI, give intravenous antibiotics, and involve ENT for cortical mastoidectomy and drainage of the petrous apex. The sixth-nerve palsy often resolves once the infection is controlled. [1] [5]
A child with an intracranial complication. Meningitis, extradural or subdural empyema, and a temporal-lobe or cerebellar abscess are the feared spread of mastoiditis to the brain. A child with severe headache, neck stiffness, seizures, focal neurology or a falling conscious state needs urgent brain imaging, neurosurgical involvement, prolonged intravenous antibiotics that cross the blood-brain barrier, and surgical source control. The intracranial-complications series confirmed that these complications, though uncommon, carry the highest morbidity and mortality. [1] [2]
A child with masked mastoiditis. A child treated with an incomplete antibiotic course for AOM may have persistent low-grade otalgia and raised inflammatory markers with minimal postauricular signs but progressive bony destruction. Maintain a high index of suspicion, obtain contrast temporal-bone CT if the inflammatory markers do not settle, and treat with intravenous antibiotics with a low threshold to surgery. [9] [5]
A child with chronic suppurative otitis media or cholesteatoma. Here the organism shifts to Pseudomonas aeruginosa and anaerobes, the disease is more destructive, and the complications are more frequent. Use a Pseudomonas-directed empiric regimen such as ceftazidime, image early for cholesteatoma and complication, and involve ENT for definitive surgery. Immunocompromised children behave similarly and warrant a lower threshold to image and to broaden cover. [3] [10]
Complications & Pitfalls
The most feared complications are intracranial. Meningitis is the commonest intracranial spread; extradural and subdural empyema and brain abscess (temporal lobe from tegmen spread, cerebellum from sigmoid disease) carry the highest mortality; and lateral sinus thrombosis with otitic hydrocephalus raises intracranial pressure and threatens vision. The intratemporal complications — facial nerve palsy, suppurative labyrinthitis with permanent sensorineural hearing loss, Bezold abscess, and petrous apicitis — threaten function and the airway. The intracranial-complications series confirmed that these are the events that turn a treatable ear infection into a life-threatening one. [1] [2]
The cardinal pitfall is treating mastoiditis as simple AOM. A febrile child with postauricular oedema, tenderness and a down-and-out pinna has mastoiditis, and managing them with oral antibiotics and outpatient review — as one might appropriately do for uncomplicated AOM — allows progression to coalescence, abscess and intracranial spread. The single most important habit is to look behind every febrile child's ear for the postauricular signs, and to admit and treat as mastoiditis when they are present. [4] [8]
A second pitfall is delaying imaging. The child with a suspected abscess, lateral sinus thrombosis or any neurological sign needs contrast temporal-bone CT without waiting to see whether 48 hours of intravenous antibiotics will resolve the picture, because a collection or a thrombus may already be present. Imaging when the complication is suspected, and again if the child fails to improve, is the discipline that catches the collection in time. [9] [1]
A third pitfall is inadequate empiric cover. The regimen must cover the streptococci and staphylococci at a minimum, with anaerobic cover for an intracranial collection and Pseudomonas-directed cover when chronic suppurative otitis media or cholesteatoma is the source — a beta-lactam such as ceftriaxone alone will miss Pseudomonas and leave a reservoir of infection. Knowing the source of the mastoiditis is part of the prescription. [3] [8]
A fourth pitfall is missing an intracranial complication in a child who looks well enough. Lateral sinus thrombosis and a brain abscess can develop with subtle early signs, and the only clue may be a persistent headache, a low-grade fever or a raised inflammatory marker. The threshold to image the brain and venous sinuses is deliberately low in any child with mastoiditis and a new neurological symptom, however minor it seems. [1] [11]
Prognosis & Disposition
Most children with uncomplicated acute mastoiditis recover fully with prompt intravenous antibiotics, with or without a myringotomy, and the outlook is excellent when treatment begins early. The morbidity and mortality rise sharply when the presentation is delayed, when an abscess or sinus thrombosis is missed, or when an intracranial complication develops. The systematic review confirmed that outcomes are consistently good when the postauricular signs are recognised early and the surgical threshold is respected. [8] [5]
Disposition follows the stage. Admit any child with the postauricular signs for intravenous antibiotics, close observation and ENT review, with imaging and surgery for the complication or the medical failure at 48 hours. Manage only the child in whom the postauricular signs are truly absent and the tympanic membrane findings fit uncomplicated AOM in the community with oral antibiotics and review — and give a clear safety-net for the postauricular change. The threshold for admitting the very young, the systemically unwell and the child who cannot be reliably examined is deliberately low. [4] [3]
At discharge, transition to oral antibiotics to complete a total course of three to four weeks guided by the severity and the culture results, confirm resolution of the postauricular signs, and arrange audiology follow-up to document and monitor the hearing, because conductive and occasionally permanent sensorineural loss can follow. Address any underlying chronic suppurative otitis media or cholesteatoma that predisposes to recurrence, and give the family a clear safety-net for recurrent fever, postauricular swelling, headache or any neurological symptom. Recurrence is uncommon but reflects uncontrolled middle-ear or mastoid disease and warrants ENT reassessment. [5] [10]
Special Populations
Infants are at higher risk of rapid progression and atypical presentation. The mastoid is poorly pneumatized in early infancy, the signs may be subtle, and the inability to localise pain means otalgia is expressed only as irritability. A febrile, irritable infant with ear-pulling and any postauricular change is assumed to have mastoiditis until imaging proves otherwise, and the threshold to admit and to image is lower. [5] [4]
Immunocompromised children are at risk of severe, persistent and atypical infection. The organism may be unusual, the disease more invasive, and the response to standard therapy slower. Early imaging, broad empiric cover and a lower surgical threshold are appropriate when these children present with mastoiditis. [3] [2]
Aboriginal and Torres Strait Islander, Maori and Pasifika children carry one of the highest burdens of otitis media and its suppurative complications in the world, with chronic suppurative otitis media endemic in many communities. The threshold to investigate and treat aggressively is lower, and the management pathway must be embedded in culturally safe, community-linked care delivered with the family, with trained interpreters, and with early retrieval and telehealth support for rural and remote children so that distance does not delay treatment. [10]
Children with chronic suppurative otitis media or cholesteatoma develop more destructive disease driven by Pseudomonas and anaerobes. Image early for cholesteatoma and complication, use a Pseudomonas-directed empiric regimen, and involve ENT for definitive surgery, because these children are the ones who recur and who sustain the permanent hearing loss. [3] [10]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric mastoiditis is built on large retrospective case series and systematic reviews rather than randomised trials, reflecting the nature of the disease. The series of intracranial complications of acute mastoiditis defined the clinical course and the mortality of intracranial spread, while the fifteen-year experience of intracranial complications of otitis media in thirty-three patients consolidated the modern surgical and medical approach. The complications-of-paediatric-otitis-media review and the intratemporal-and-intracranial-complications series defined the contemporary epidemiology and the relative frequency of each complication. [1] [2] [3]
Management of paediatric acute mastoiditis: systematic review
Population: Children with acute mastoiditis across the published literature, assessed for the medical-versus-surgical management, the role of myringotomy, the surgical threshold and the outcomes.
Key finding
Most children with uncomplicated acute mastoiditis responded to intravenous antibiotics, with myringotomy when the drum was intact; cortical mastoidectomy and drainage were reserved for subperiosteal abscess, lateral sinus thrombosis, intracranial extension and failure of medical therapy, with no single strategy fitting every child.
Practice change
A stepwise approach — intravenous antibiotics first, myringotomy for the intact drum, surgery for the abscess, sinus thrombosis or intracranial spread — is supported, with the surgical threshold driven by the complication and the 48-hour response.
The advanced-paediatric-mastoiditis series defined the features that separate the child with and without an intracranial complication, while the radiological review established the coalescent pattern and cortical erosion as the imaging hallmarks of surgical disease. The subperiosteal-abscess series of one hundred and fifteen Swedish children refined the management of the commonest surgical presentation, and the immediate-needle-aspiration series validated a less invasive option for selected abscesses. The otitic-hydrocephalus series characterised the raised-pressure syndrome of lateral sinus thrombosis. [5] [9] [11]
Subperiosteal abscesses in acute mastoiditis in 115 Swedish children
Population: Children with acute mastoiditis and a subperiosteal abscess, reviewed for the clinical features, the management — conservative, needle aspiration or surgical drainage — and the outcomes.
Key finding
Subperiosteal abscess was the commonest surgical presentation of acute mastoiditis; selected children responded to intravenous antibiotics with or without needle aspiration, while surgical drainage with cortical mastoidectomy was reserved for larger abscesses, failure of conservative therapy and intracranial extension.
Practice change
The management of the subperiosteal abscess can be individualised — a trial of intravenous antibiotics with needle aspiration is reasonable in selected young children with a small abscess, provided the threshold for cortical mastoidectomy is preserved for failure or for high-risk features.
The regional policy structure is consistent in principle and varies in detail. In the UK, NICE antimicrobial-prescribing guidance and the Royal College of Paediatrics and Child Health guidance set the empiric antibiotic choices and the imaging indications. In Australia and New Zealand, the Royal Children's Hospital Melbourne clinical practice guideline and the Therapeutic Guidelines set the local pathway, with ceftriaxone plus flucloxacillin as the standard empiric regimen and Pseudomonas-directed cover added when chronic disease is the source. In North America, the American Academy of Pediatrics and the American Academy of Otolaryngology guidance set the management framework. The controversies — the optimal duration of therapy, the precise surgical threshold for subperiosteal abscess, the role of anticoagulation in lateral sinus thrombosis, and the place of routine myringotomy — are resolved by the same principle in every region: recognise the postauricular signs, treat with broad intravenous antibiotics, image for any complication, and drain the abscess or decompress the sinus that fails or threatens the brain. [8] [10]
Exam Pearls
- Acute mastoiditis is suppuration in the mastoid air cells and the commonest suppurative complication of acute otitis media, reached through the valveless aditus ad antrum. [4] [5]
- The postauricular signs are erythema, swelling and tenderness with a lost postauricular crease and a pinna pushed downward and outward, plus a bulging erythematous tympanic membrane — any of these in a febrile child means admission and intravenous antibiotics. [4] [8]
- Coalescence — destruction of the air-cell trabeculae on contrast temporal-bone CT — is the imaging hallmark that separates surgical from medical disease. [9]
- The organisms are Streptococcus pneumoniae, Streptococcus pyogenes, Staphylococcus aureus and non-typeable Haemophilus influenzae, with Pseudomonas aeruginosa and anaerobes in chronic suppurative otitis media or cholesteatoma. [3]
- The intratemporal complications are subperiosteal and Bezold abscess, petrous apicitis (Gradenigo triad), facial palsy, labyrinthitis and lateral sinus thrombosis. [1]
- The intracranial complications are meningitis (commonest), extradural and subdural empyema, brain abscess and otitic hydrocephalus. [1] [2]
- The Gradenigo triad is discharging ear, retro-orbital pain and a sixth-nerve palsy, signalling petrous apicitis. [1]
- The picket-fence spiking fever of lateral sinus thrombosis can progress to otitic hydrocephalus with papilloedema and a sixth-nerve palsy from raised intracranial pressure. [11]
- Management is intravenous ceftriaxone plus flucloxacillin, with metronidazole for intracranial or anaerobic concern, vancomycin for suspected MRSA, and Pseudomonas-directed cover for chronic disease; add myringotomy for the intact drum. [8] [3]
- Contrast temporal-bone CT is indicated for a suspected abscess, lateral sinus thrombosis, intracranial extension, failure at 48 hours, or any neurological sign; MRI with venography for sinus thrombosis and brain abscess. [9]
- Cortical mastoidectomy is indicated for failure to improve at 48 hours, a subperiosteal or Bezold abscess, lateral sinus thrombosis, Gradenigo syndrome, facial palsy, cholesteatoma and intracranial extension. [6] [2]
- The burden of otitis media and its complications is far higher in Aboriginal and Torres Strait Islander, Maori and Pasifika children, among whom the threshold to investigate and treat is lower. [10]
References
- [1]Go C; Bernstein JM; de Jong AL; Sulek M; et al Intracranial complications of acute mastoiditis. Int J Pediatr Otorhinolaryngol, 2000.PMID 10767461
- [2]Penido Nde O; Borin A; Iha LC; Suguri VM; et al Intracranial complications of otitis media: 15 years of experience in 33 patients. Otolaryngol Head Neck Surg, 2005.PMID 15632907
- [3]Lavin JM; Rusher T; Shah RK Complications of Pediatric Otitis Media. Otolaryngol Head Neck Surg, 2016.PMID 26494054
- [4]Mattos JL; Colman KL; Casselbrant ML; Chi DH Intratemporal and intracranial complications of acute otitis media in a pediatric population. Int J Pediatr Otorhinolaryngol, 2014.PMID 25447953
- [5]Zevallos JP; Vrabec JT; Williamson RA; Giannoni C; et al Advanced pediatric mastoiditis with and without intracranial complications. Laryngoscope, 2009.PMID 19504555
- [6]Enoksson F; Groth A; Hultcrantz M; Stalfors J; et al Subperiosteal abscesses in acute mastoiditis in 115 Swedish children. Int J Pediatr Otorhinolaryngol, 2015.PMID 26022749
- [7]Bartov N; Lahav Y; Lahav G; Zloczower E; et al Management of Acute Mastoiditis With Immediate Needle Aspiration for Subperiosteal Abscess. Otol Neurotol, 2019.PMID 31135677
- [8]Loh R; Phua M; Shaw CL Management of paediatric acute mastoiditis: systematic review. J Laryngol Otol, 2018.PMID 28879826
- [9]Minks DP; Porte M; Jenkins N Acute mastoiditis--the role of radiology. Clin Radiol, 2013.PMID 22980753
- [10]O'Connor TE; Perry CF; Lannigan FJ Complications of otitis media in Indigenous and non-Indigenous children. Med J Aust, 2009.PMID 19883359
- [11]Kuczkowski J; Dubaniewicz-Wybieralska M; Przewoźny T; Narozny W; et al Otitic hydrocephalus associated with lateral sinus thrombosis and acute mastoiditis in children. Int J Pediatr Otorhinolaryngol, 2006.PMID 16899305