Paeds · ent-hearing-and-oral-health
Nasal foreign body and button-battery injury
Also known as Nasal foreign body in children · Button battery in the nose · Intranasal button battery · Paediatric nasal foreign body · Rhinolith · Nasal battery injury · Intranasal button battery injury
Fellowship topic on nasal foreign body and button-battery injury in children — an object lodged in the nasal cavity of a two-to-five-year-old, most often a benign inert bead, food or toy part presenting with unilateral foul-smelling or blood-stained discharge, with a single time-critical subtype, the button (coin) battery, that must be removed immediately because electrolysis at its negative pole generates hydroxide ions and alkaline liquefactive necrosis dissolves tissue within hours. Covers the common objects and the peak toddler age; the unilateral foul-discharge presentation and the rhinolith sequela; the alkaline-electrolysis, thermal and pressure-necrosis cascade that makes a battery burn the septum; the stepwise removal of inert objects by positive pressure (the parent's kiss) and instruments (alligator forceps for graspable objects, a right-angle hook behind a smooth bead, suction, a Katz extractor); the emergency removal of a button battery without waiting for fasting, cavity irrigation, the emerging role of topical neutralising agents, and ENT referral for burn surveillance; the avoidance of a blind finger sweep; the distinction of a battery from a coin by its step-off edge and double-ring sign; the complications of septal perforation, synechiae and stenosis; and ANZ, UK, US and Canadian guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A father brings his three-year-old to the emergency department because "her nose has smelled awful for a week and now there is blood in the tissue when she wipes." She is otherwise well, eating and playing, and she insists she has put nothing up her nose. With a good light and her on her father's lap, anterior rhinoscopy shows a small foam toy piece resting on the floor of the right nasal cavity, surrounded by purulent discharge. Across the corridor, a different family is rushed in: a two-year-old who has just been found with a disassembled remote control and a missing button battery, and a parent who can see something shiny in one nostril. The first child is the common, benign, routine case. The second is the one that cannot wait. [1]
A nasal foreign body is any object, solid or semi-solid, lodged within the nasal cavity of a child. It is overwhelmingly a disease of the toddler and preschool years, when a child explores the world by inserting objects into orifices and lacks the judgement to remove them or to report them honestly. The objects span food, beads, toy parts, crayon, paper and coins, and increasingly button batteries taken from hearing aids, remotes, toys and key fobs. [1] [11]
What makes the topic examinable is the chasm between how benign most cases are and how dangerous one subtype is. The inert object irritates the mucosa and produces a foul unilateral discharge, and once removed the child is well. The button battery, by contrast, sets off a chemical cascade that destroys tissue within hours, turning a removable object into a septal perforation, a synechia or a saddle-nose deformity if it is not recognised. The fellowship task is to read the object, not the child, and to act on the battery immediately. [5] [3]
Classification
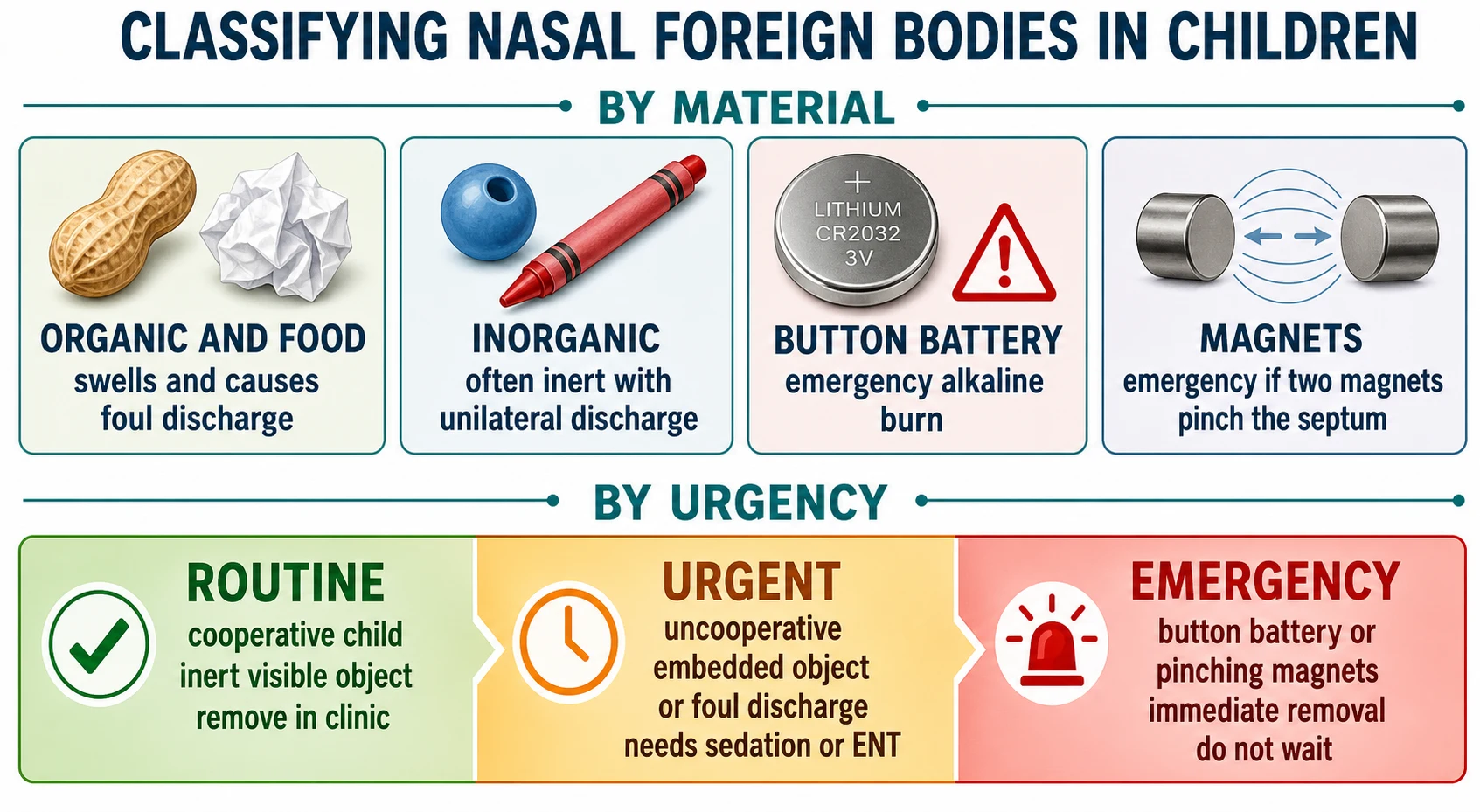
Classify a nasal foreign body by its material and by its urgency, because the material sets the mechanism and the urgency sets the clock. The single most useful split is inert versus button battery, and within that the organic-versus-inorganic distinction predicts swelling and discharge. [1]
Nasal foreign bodies in children classified by material and urgency
The classification does the triage. A cooperative child with a visible inert object is a routine clinic removal. An uncooperative child, an embedded object, or a long-standing foul discharge is urgent and may need sedation or ENT. And any button battery, or a missing battery with unilateral symptoms, is an emergency that ends the assessment and goes straight to removal. [3] [9]
Epidemiology & Risk Factors
Nasal foreign bodies are a staple of paediatric acute care because they map onto a developmental stage. The peak age is two to five years, the toddler and preschool years when a child explores orifices and imitates the behaviour of placing objects in the nose, and boys are affected slightly more often. Most are isolated events in a typically developing child, but recurrence and late presentation cluster in children with developmental delay, autism, attention-deficit or pica. [1] [11]
The objects children reach for are the objects in their environment. Food and organic material — peanuts, peas, seeds and paper — sit beside inorganic objects such as beads, plastic toy parts, crayon and chalk. The object whose incidence has risen most sharply is the button battery, drawn from hearing aids, remote controls, toys, key fobs and musical greeting cards, and it is this object that has turned a once-benign complaint into a recognised time-critical injury. [5] [2]
The social risk factors shape when and how the child presents. Unsupervised access to small batteries, low household battery-safety awareness, and developmental conditions all raise the chance of insertion. Families living remotely or in disadvantage, and Aboriginal and Torres Strait Islander, Maori, Pasifika, refugee, asylum-seeking and migrant families, carry a disproportionate burden of late-presenting battery injury and retained rhinoliths, reflecting access gaps rather than biology. [3] [12]
Pathophysiology
Why does a small shiny disc in the nose of a two-year-old become a surgical emergency, when a bead of the same size is harmless? The answer is the electrochemistry of the button battery, and it is the mechanism examiners test most. [5]
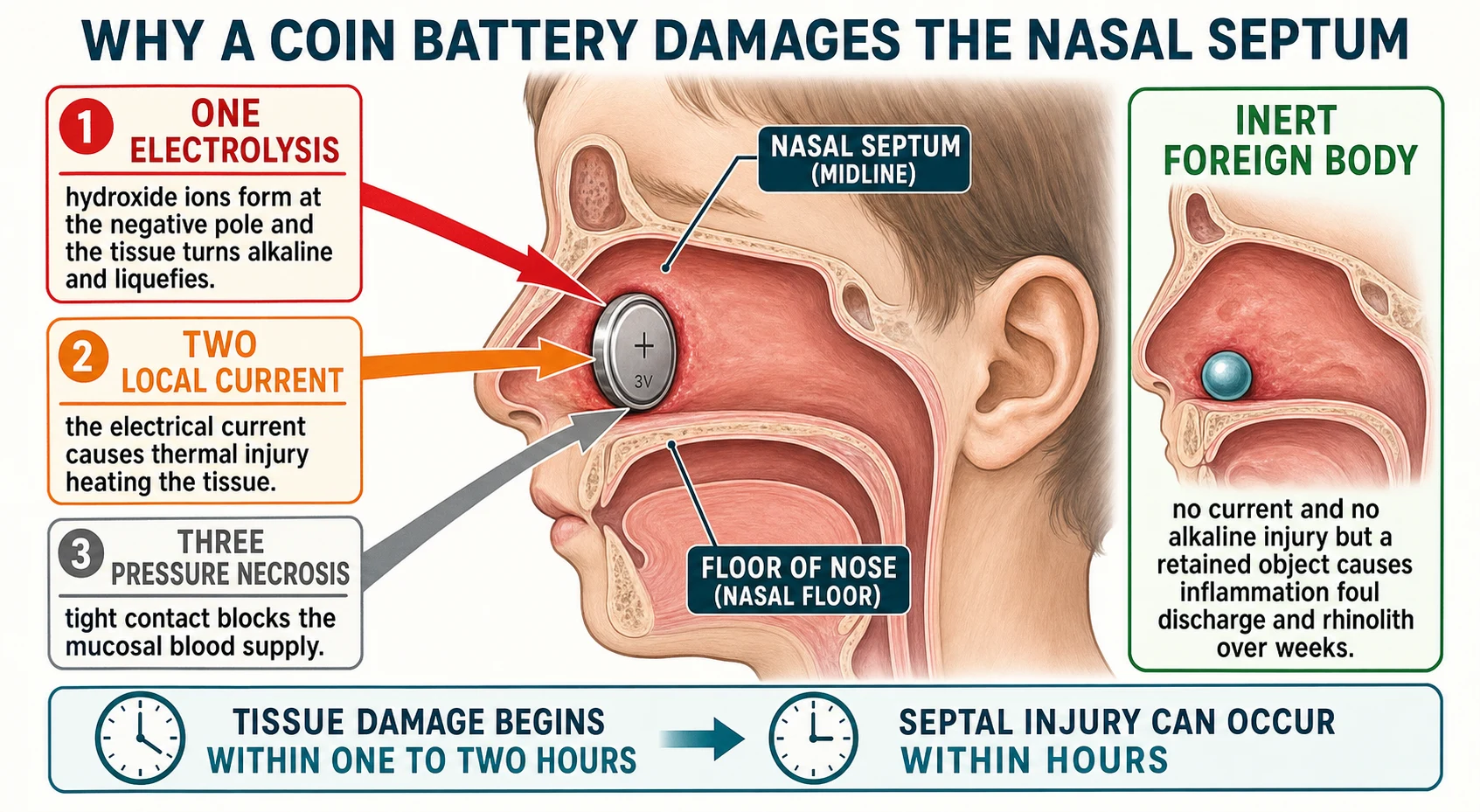
When a button battery is wedged against the moist septal or turbinate mucosa, the tissue fluids complete an electrical circuit and the battery drives an electrolysis current. At the negative pole of the battery this current generates hydroxide ions, the local pH rises sharply, and the tissue undergoes alkaline (liquefactive) necrosis — a rapid chemical dissolution of fat and protein that is far more destructive than a simple burn. Two further mechanisms compound it: the local electrical current causes thermal injury, heating the tissue in contact with the pole, and the tight contact between the battery face and the mucosa causes pressure necrosis by blocking the mucosal blood supply. [5] [6]
The time course is what makes this an emergency and not a clinic appointment. Tissue damage begins within one to two hours of contact, and clinically significant injury — including septal perforation — can develop within hours, well before a child looks unwell. The tight, wedged fit of a coin-shaped battery against the septum is the worst configuration, because it maximises both the current and the pressure. Retrospective series of paediatric nasal button batteries report rapid mucosal injury and long-term complications, which is why the whole approach is built around the earliest possible removal. [3] [2]
The inert object behaves in the opposite way. A bead, a piece of food or a toy part produces no current and no alkaline burn, but a retained object still irritates the mucosa, generating a unilateral, purulent and often foul-smelling discharge that is frequently blood-stained. Left for weeks to months, mineral salts deposit around the object and a rhinolith — a calcified stone — forms, which itself becomes a source of obstruction, discharge and epistaxis. The contrast is complete: the battery destroys tissue in hours, the inert object annoys for weeks. [12] [1]
Clinical Presentation
Read the presentation by the side and the smell, because a unilateral foul discharge in a young child does most of the diagnostic work. [1]
The classic case is the two-to-five-year-old with unilateral, foul-smelling and often blood-stained nasal discharge, unilateral obstruction and sometimes sneezing. The parent may report that the child inserted something, but very often the child denies it and the object is discovered only on examination. Between episodes the child is usually entirely well, which is why the discharge rather than the child sets off the concern. [1] [11]
Atypical and late presentations test the alertness of the clinician. A long-retained object can present weeks later as a rhinolith with chronic unilateral obstruction, discharge and epistaxis; a child with developmental delay may present with chronic unilateral discharge that has been attributed to recurrent infection; and the unwitnessed insertion may surface only when anterior rhinoscopy is performed for another reason. A proportion of nasal foreign bodies are not visible on simple examination, which is why a strong clinical suspicion still justifies a careful look or imaging. [11] [12]
The button battery presentation is the trap. The child may have discharge, or may look entirely well with a battery only just lodged, and the history may be nothing more than a missing battery from a remote or a hearing aid. Any battery seen in the nose, or any history of a missing battery in a young child with unilateral symptoms, must be treated as an emergency regardless of how well the child looks, because the tissue injury is chemical and evolving, not reflected in the child's appearance. [3] [4]
Differential Diagnosis
Build the differential for a unilateral foul nasal discharge in a young child, and let the foreign body sit at the top. [1]
The first question is whether there is a foreign body, because unilateral foul-smelling discharge in a two-to-five-year-old is a nasal foreign body until proven otherwise. Once an object is excluded, the alternatives are unilateral purulent rhinosinusitis, a nasal polyp or a congenital mass such as a meningoencephalocele, a rhinolith from a long-retained object, and in the neonate a congenital obstruction such as choanal atresia. A polyp or meningocele is pale, glistening and non-purulent, and rhinosinusitis more often carries fever and bilateral features in the older child. [1] [11]
The single most important distinction within the foreign body itself is a button battery from a coin or food, because the two are easily confused on a glance. A battery is thicker than a coin, with a step-off or bevelled edge and, on a plain lateral X-ray, often a double-ring (halo) sign where the two faces of the cell meet the rim. A coin is thin, flat and uniform. When an object cannot be confidently identified as a coin in a child with the right history, treat it as a battery until proven otherwise. [9]
The practical pivot is to let the object type and its imaging appearance — not the child's wellbeing — separate the routine inert foreign body from the emergency battery, and to look actively for a second battery whenever one is found or removed. [3] [9]
Clinical & Bedside Assessment
Begin with the history, because the suspected object type sets the urgency. Ask about any witnessed insertion, the suspected object (food, toy, bead, or a battery from a hearing aid, remote or toy), the duration of symptoms and the character of the discharge. A history of a missing button battery in a young child is itself an emergency and should be pursued as actively as a visible object. [1] [3]
Examine the child in an adult's lap with good light, immobilising the head gently. Perform anterior rhinoscopy with a headlight and speculum, or a gentle otoscope view, looking specifically at the floor of the nose just inside the vestibule, where most objects lodge. Check both sides, and once an object is found look behind it for a second foreign body, because a missed second battery is a recurring source of delayed injury. Assess the oropharynx for an object that has slipped posteriorly. [1] [9]
The finding of a button battery ends the assessment and mandates immediate removal; further outpatient work-up only wastes the hours during which the septum is being dissolved. Decide the setting for removal from the child's cooperation and the object's position: a cooperative child with an anterior inert object can be managed in clinic, while an uncooperative child, a posterior or embedded object, or any battery moves to sedation or ENT theatre. [1] [3]
[5]Investigations
Most nasal foreign bodies need no investigation — the diagnosis is made and resolved at anterior rhinoscopy. Reserve testing for the object that cannot be seen but is strongly suspected, the object that must be identified on imaging, and the complicated or long-standing case. [1] [11]
The key imaging question is whether an unseen or unidentifiable object is a battery. A plain lateral X-ray of the nasal cavity and nasopharynx identifies radiopaque objects and, critically, distinguishes a button battery from a coin by the battery's step-off edge and double-ring (halo) sign. Imaging is also used specifically to search for a second battery when one has been found or removed, because multiple and missed batteries drive much of the delayed injury in the literature. [9]
Reserve bloods (a full blood count and inflammatory markers) and cross-sectional imaging for the complicated case — a retained rhinolith, suspected deep infection, or to plan removal of a long-embedded object. For the straightforward inert foreign body and the recognised battery, the diagnosis is clinical or radiographic and the response is operative, not investigative. [12] [8]
Management — Resuscitation
There is one resuscitation-level decision in this topic, and it is the single fact that defines it: a button battery in the nose is an emergency, and it must be removed immediately, without waiting for a fasting period. Every hour the battery sits against the septum is an hour of alkaline liquefactive necrosis, so the response is operative, not expectant. [3] [5]
Protect the airway and set up for controlled removal. For the uncooperative child or a posterior battery, arrange urgent ENT removal in theatre with a shared-airway plan, rather than repeated traumatic attempts in clinic that push the object deeper and distress the child. Apply a topical decongestant such as oxymetazoline and topical anaesthesia to reduce mucosal swelling and pain before instrumentation of any foreign body, which improves the chance of a clean, single-pass removal. [1] [3]
The cardinal error to avoid at every stage is the blind finger sweep. A finger pushed into the nose without vision compresses the object posteriorly toward the nasopharynx and the airway, converting a removable foreign body into an airway threat. Removal must always be under direct vision, with the right instrument, by a clinician who can see the object throughout. [1] [6]
Management — Definitive & Stepwise
Once the urgency is set, definitive management moves in a clear stepwise order for the inert object, and along a separate emergency lane for the battery. The aim is to remove the object cleanly in a single pass with the least trauma. [1]
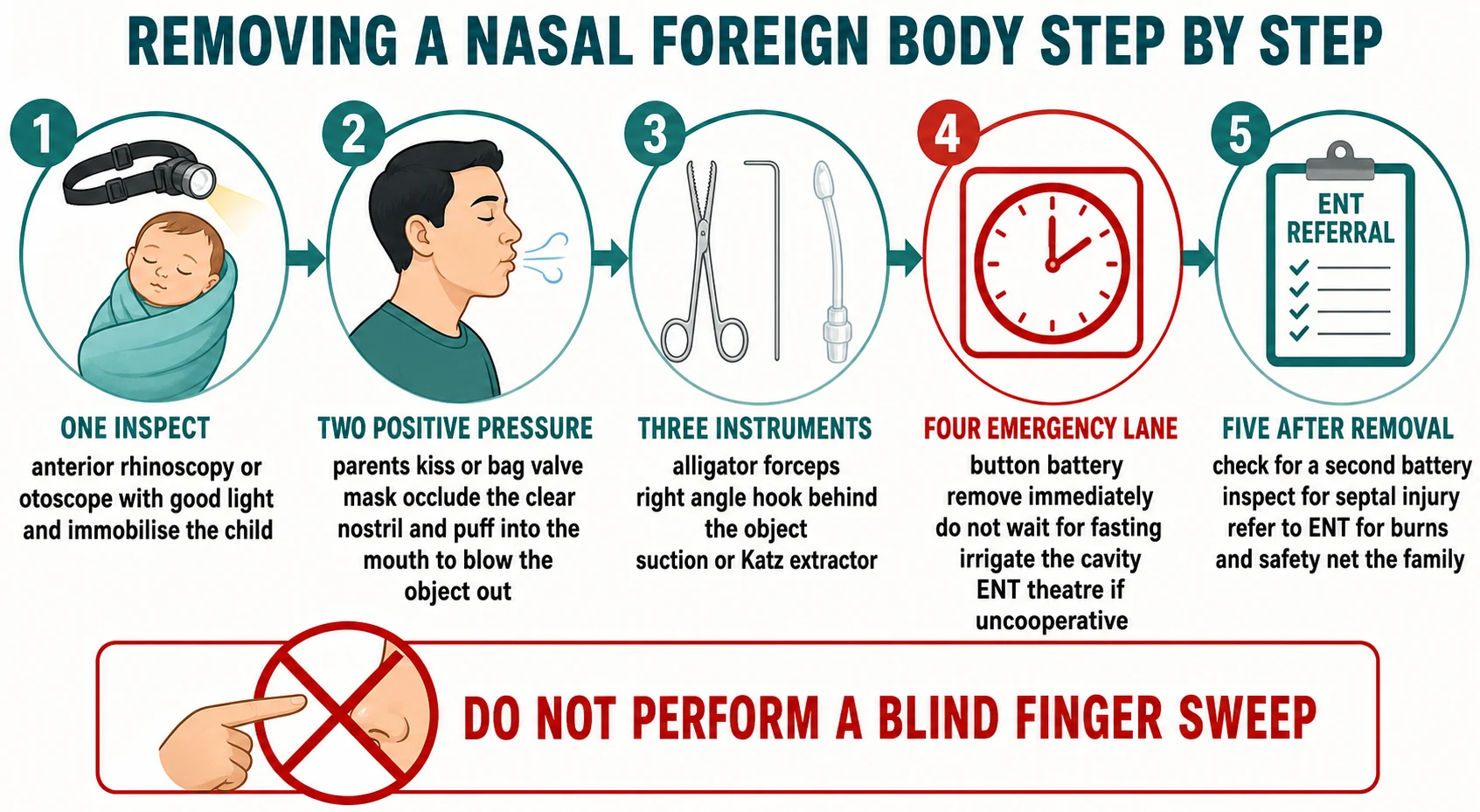
Stepwise removal of a nasal foreign body
Inspect — anterior rhinoscopy or otoscopy with good light, immobilise the child in an adult's lap, identify the object and look behind it for a second foreign body.
Positive pressure — for an anterior, non-battery object, occlude the clear nostril and deliver a short puff of air to the child's mouth via the parent's kiss (parent's mouth sealed over the child's) or a bag-valve-mask; apply topical decongestant and anaesthesia first.
Instruments — match the tool to the object: alligator (Tilley) forceps for soft, irregular or graspable objects such as paper and food; a right-angle hook or Jobson Horne probe passed gently behind a smooth round bead; suction for small loose objects; a Katz extractor or cyanoacrylate on an applicator for smooth round objects.
Sedation or ENT — for the uncooperative child, a posterior or embedded object, or a failed attempt, move to sedation or ENT theatre with a shared-airway plan.
Button battery emergency lane — remove immediately under direct vision without waiting for fasting, irrigate the cavity, consider a topical neutralising agent where available, and refer to ENT for burn surveillance.
After removal — re-inspect for a second battery and septal injury, treat any mucosal burn, and give the family safety-net and battery-safety advice.
Positive pressure is the elegant first move for an anterior inert object and the technique examiners love. Occlude the clear nostril, and deliver a short puff of air to the child's mouth — classically the parent's kiss, in which the parent seals their mouth over the child's open mouth and gives a brisk puff, blowing the object out of the blocked nostril. A bag-valve-mask over the mouth achieves the same. It is quick, atraumatic and avoids instrumentation, and a topical decongestant beforehand shrinks the mucosa to give the object room to exit. [10]
The instrument must match the object — this is where most failures and complications begin. Alligator (Tilley) forceps work for soft, irregular or graspable objects such as paper, food and crayon. A smooth round bead defeats forceps, which slip off and push it deeper; the answer is a right-angle hook or a Jobson Horne probe passed gently behind the object to lever it forward, or a Katz extractor (a catheter balloon or umbrella) and, in experienced hands, a cyanoacrylate-on-an-applicator trick for a smooth sphere. Suction (a Frazier tip) retrieves small loose objects. Matching the tool to the shape is the skill. [1]
Topical decongestant and anaesthesia (before instrumentation)
Dose
Oxymetazoline 0.05 percent nasal solution with a topical anaesthetic such as lidocaine, applied to the nasal mucosa
The button battery runs on a separate, faster track. It is removed immediately under direct vision, without waiting for fasting, and once it is out the cavity is irrigated to clear alkaline residue. In-vitro and early-clinical work supports the adjunctive use of a topical neutralising agent — medical honey or a carbomer (carboxymethylcellulose) gel applied to the lodged or just-removed battery area — to reduce tissue injury, but these agents are adjuncts to urgent removal, not substitutes for it. [7] [4]
After removal, re-inspect for a second battery and for septal injury, treat any visible mucosal burn, and refer to ENT for burn surveillance, because septal perforation, synechiae and stenosis can continue to evolve for days after the battery is out. For the routine inert object, the family is given safety-net advice — return for recurrent unilateral discharge, fever or bleeding — and household button-battery safety education. [3] [6]
Specific Subtypes & Scenarios
The scenarios below are the ones examiners reach for, because each forces a different decision under pressure. [1]
The routine anterior inert object in a cooperative child is the commonest case. A bead, a piece of food or a toy part sits on the floor of the nose with a foul unilateral discharge. The answer is positive pressure or the right instrument in clinic, with topical decongestant and anaesthesia, a check for a second object, and discharge with safety-net advice. Most of these never need a theatre. [1] [10]
The button battery in the nose is the defining emergency. The answer is immediate removal under direct vision without waiting for fasting, theatre for the uncooperative child, cavity irrigation, an adjunctive neutralising agent where available, and ENT follow-up for burn surveillance. There is no role for a wait-and-see approach, and a well-looking child does not change this. [3] [7]
The smooth round bead that forceps push deeper is the instrument trap. The answer is to abandon forceps and use a right-angle hook passed behind the object or a Katz extractor, because forceps cannot grip a sphere and only drive it toward the airway. [1]
The long-retained object presenting as a rhinolith is the late scenario. A child with weeks of unilateral obstruction, foul discharge and epistaxis is found to have a calcified stone. The answer is ENT referral for removal of the rhinolith and management of any cavity damage, because these objects are embedded and bleed. [12]
Complications & Pitfalls
The cardinal pitfall is the blind finger sweep. A finger pushed in without vision compresses the object posteriorly toward the nasopharynx and airway, converting a removable foreign body into an airway threat. Removal must always be under direct vision. [1]
The diagnostic error that does the most harm is mistaking a button battery for a coin or food. A battery mistaken for a coin is left for hours while alkaline liquefactive necrosis dissolves the septum. The protection is to read the step-off edge and double-ring sign and to treat any unidentifiable round metallic object in a young child as a battery until proven otherwise. [9] [6]
The battery complications are the legacy of delayed removal: septal perforation, synechiae between opposing mucosal surfaces, nasal stenosis and saddle-nose deformity from loss of septal support, all driven by alkaline liquefactive necrosis, thermal and pressure injury. A missed second battery is a separate, recurring source of delayed injury, which is why the post-removal search for a second battery is non-negotiable. [3] [8]
The instrument pitfall is using forceps on a smooth round bead, which slip off and push the object deeper. The rule is to match the tool to the object — forceps for graspable paper and food, a hook behind a smooth sphere — and to escalate to sedation or ENT rather than repeat traumatic attempts. [1] [6]
Prognosis & Disposition
The prognosis of a routine inert nasal foreign body is excellent once removed. Most children are discharged from clinic the same day with safety-net advice and battery-safety education, and the episode resolves without sequelae. [1]
Discharge the child with a removed inert object on advice to prevent re-insertion, to keep small batteries secured out of reach, and to return for recurrent unilateral discharge, fever or bleeding. The safety-net is what makes outpatient management safe, because a missed second object or a late-presenting rhinolith can surface days to weeks later. [11] [12]
Refer every nasal button battery to ENT after removal for burn surveillance, because septal perforation, synechiae and stenosis can evolve over days even after the battery is out. Refer the long-retained object or rhinolith, and any case with a cavity defect or deep infection, for ENT assessment and definitive removal. The durable interventions — direct-vision removal, the second-battery check, and household battery-safety education — are what keep children out of theatre and prevent the next injury. [3] [6]
Special Populations
Children with developmental delay, autism, attention-deficit or pica are over-represented for recurrent foreign-body insertion and for late presentation. Combine removal with behavioural and carer education and a concrete home battery-safety plan, because recurrence is the rule in this group without it. [1] [11]
Aboriginal and Torres Strait Islander, Maori, Pasifika, refugee, asylum-seeking and migrant families, and children in remote and disadvantaged communities, present later with retained objects and battery injury, reflecting access and safety-education gaps rather than biology. Provide culturally safe care, trained interpreters and practical safety education, and act on the same clinical rules — the object type sets the urgency. [3] [12]
Children with complex chronic conditions and technology dependence, above all hearing-aid users, have higher exposure to button batteries from their devices. Secure the devices and spare batteries, and counsel carers explicitly on the nasal-battery emergency so that a missing battery triggers an immediate call rather than a wait. [5] [4]
Use telehealth and rural retrieval pathways to triage the suspected battery early, moving the child to theatre rather than attempting repeated traumatic removals far from specialist services. The earlier the battery is out, the less tissue is lost, so distance must not become delay. [3] [8]
Evidence, Guidelines & Regional Differences
The named regional guidance is the Royal Children's Hospital Melbourne foreign-body-in-the-nose guideline and eTG, the AAO-HNS button-battery guidance, NICE and ENT UK, and the National Capital Poison Center button-battery triage and treatment guideline. Across all of these the core message is consistent: an inert nasal foreign body is removed by direct-vision technique, and a button battery is removed immediately. [1] [5]
The button-battery mechanism and outcome evidence is strong and practice-defining. Case series and retrospective analyses of paediatric nasal button batteries report rapid mucosal injury and long-term complications including septal perforation, synechiae and stenosis, which underpins the immediate-removal rule and the absence of any wait-and-see approach. A ten-year series of nasal button battery injuries and a large 176-case analysis of nasal foreign bodies with batteries have characterised the presentation, the injury and the outcomes in detail. [3] [2]
The mitigation evidence is emerging rather than established. In-vitro and early-clinical studies of topical neutralising agents — medical honey and carbomer or acetic-acid gels applied to a lodged or just-removed battery — show reduced tissue injury, and clinical application of tissue pH neutralisation after battery removal has been reported. These agents are adjuncts to urgent removal, not substitutes for it, and where a neutralising agent is not immediately available it must never delay operative removal. [7] [4]
[1] [6]Exam Pearls
[1] [3]BATTERY
Nasal foreign body and button-battery injury is, at its core, the contrast between a benign removable object and a chemical burn on a clock. Most cases are inert beads and food in a two-to-five-year-old with a unilateral foul discharge, removed by positive pressure or the right instrument. [1]
The fellowship-defining skill is the button-battery rule: electrolysis at the negative pole generates hydroxide and alkaline liquefactive necrosis within hours, so the battery is removed immediately without waiting for fasting, the cavity is irrigated, and the child goes to ENT for burn surveillance. [3] [5]
For every object, removal is under direct vision with the tool matched to the shape — forceps for graspable objects, a hook behind a smooth bead — and a blind finger sweep is never done, because it pushes the object toward the airway. The durable protections are the second-battery check, the battery-from-coin distinction on the step-off edge and double-ring sign, and household battery-safety education that prevents the next injury. [9] [1]
References
- [1]Lane Wilson J; et al Foreign Bodies in the Ear, Nose, and Throat. Am Fam Physician, 2025.PMID 40736491
- [2]Yan S; et al Characteristics and treatment of pediatric nasal foreign bodies with button batteries-A retrospective analysis of 176 cases. PLoS One, 2024.PMID 39208061
- [3]Heilig Y; et al Long-term outcomes following nasal button battery foreign body injuries in children: a 10-year retrospective analysis of 45 patients. Int J Pediatr Otorhinolaryngol, 2026.PMID 41985339
- [4]Xueyou L; et al Pediatric nasal button battery injuries: a 10-year retrospective study and in vitro evaluation of prehospital mitigation strategies. Eur J Med Res, 2026.PMID 41742308
- [5]Craft A; et al Current State of Button Battery Ingestion Injuries. Otolaryngol Clin North Am, 2026.PMID 42342488
- [6]Sethia R; et al Current management of button battery injuries. Laryngoscope Investig Otolaryngol, 2021.PMID 34195377
- [7]Jatana KR; et al Initial clinical application of tissue pH neutralization after esophageal button battery removal in children. Laryngoscope, 2019.PMID 30835848
- [8]Shaffer AD; et al Management and Outcomes of Button Batteries in the Aerodigestive Tract: A Multi-institutional Study. Laryngoscope, 2021.PMID 32068903
- [9]Bance RRR; et al To X-Ray or Not to X-Ray? Discussing Unknown Nasal Foreign Bodies and Button Batteries. Ear Nose Throat J, 2024.PMID 34338035
- [10]de la O-Cavazos M; et al A new positive-pressure device for nasal foreign body removal. Pediatr Emerg Care, 2014.PMID 24457495
- [11]Thompson J; et al Pediatric nasal foreign body not visible on simple exam: Incidence and patient characteristics. Am J Emerg Med, 2025.PMID 40803278
- [12]AlZabin A; et al Paediatric rhinolith: Case report and literature review. Int J Surg Case Rep, 2024.PMID 39522412