Paeds · ent-hearing-and-oral-health
Oral ulcers and mucosal disease
Also known as Recurrent aphthous stomatitis · Herpetic gingivostomatitis · Oral candidiasis · Oral thrush · Hand-foot-and-mouth disease · Oral mucositis · Geographic tongue · Benign migratory glossitis
Fellowship topic on oral ulcers and mucosal disease in children. Covers primary herpetic gingivostomatitis with early oral aciclovir, recurrent aphthous stomatitis and its deficiency, coeliac and autoinflammatory associations, oral candidiasis and nystatin dosing in infants, hand-foot-and-mouth disease and herpangina, oral mucositis in oncology with WHO grading and prevention, the PFAPA syndrome triad, and benign geographic tongue. Builds the single-most-important skill of distinguishing the common self-limiting ulcer from the one that signals immunodeficiency, cytopenia, Behcet disease or a dehydrating viral gingivitis, with ANZ, UK, US and Canadian guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A mother brings her two-year-old to the emergency department: three days of fever, drooling, and now refusing all fluids, with gums so inflamed they bleed when touched. Lift the lip and the picture is unmistakable — diffuse vesicles and shallow ulcers across the gingiva, tongue and lips. This is primary herpetic gingivostomatitis, and the fellowship skill is to see it as a hydration problem first and an infection second. [1]
Oral ulcers and mucosal disease in children cover any breach of the oral mucosa — vesicular, aphthous, candidal, traumatic or mucositic. The task is to separate the common self-limiting lesion from the one that dehydrates, recurs systemically, or signals a cytopenia, immunodeficiency or autoinflammatory syndrome. Most oral ulcers in childhood are viral, benign and settle with supportive care. A small minority are the mouth's first warning of systemic disease. The examining skill is to read the site, the distribution and the host, because that trio names the cause. [9] [6]
Classification
Picture oral ulcers by what is causing the breach and where it sits in the mouth, because the cause and the site together drive both the treatment and the work-up. [9]
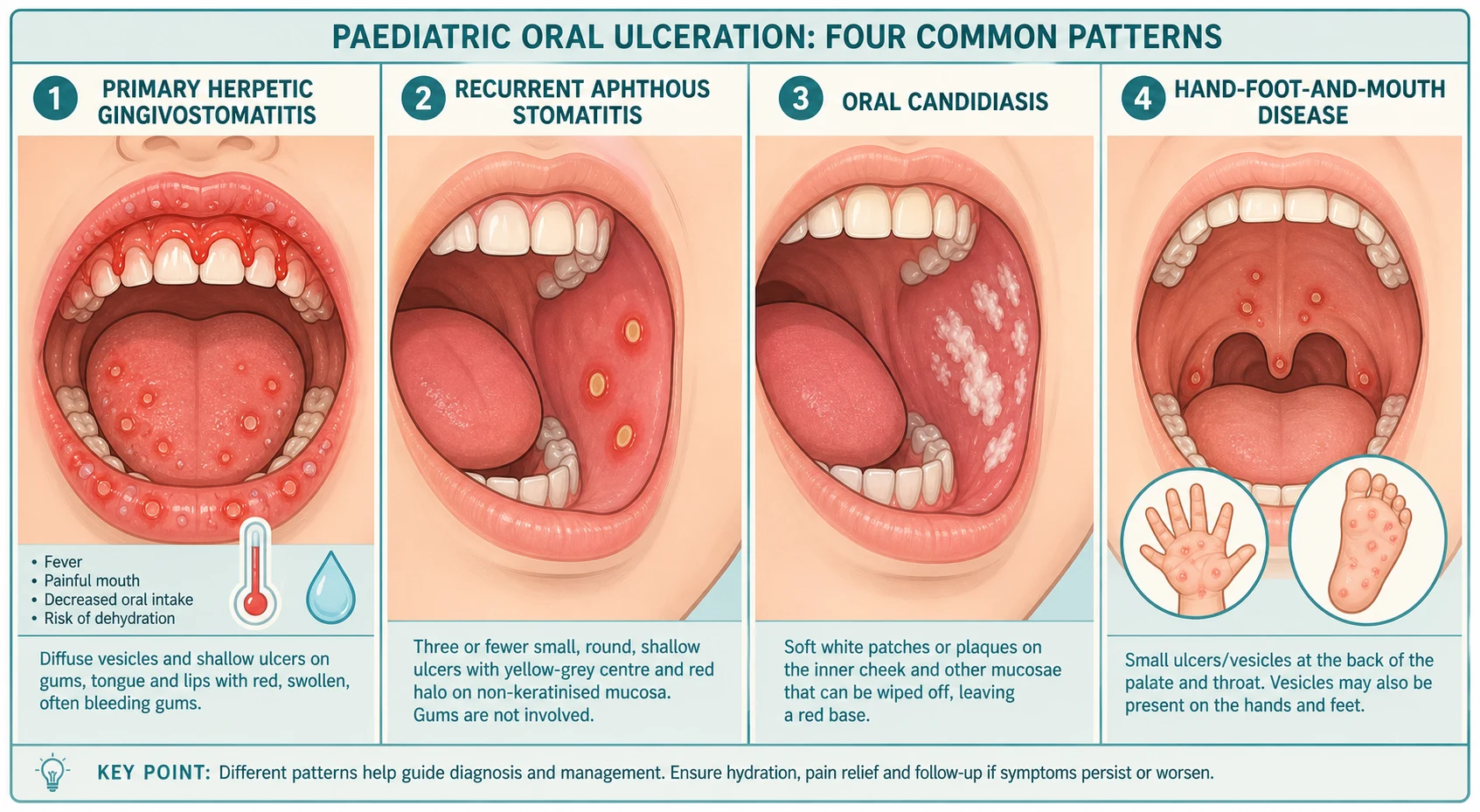
The clinical patterns of paediatric oral ulceration
Epidemiology & Risk Factors
Primary herpetic gingivostomatitis is the commonest cause of severe oral ulceration in young children, peaking between six months and five years, when maternal antibody wanes and the child first meets herpes simplex virus type 1. Most children weather it with supportive care, but dehydration from refusal to drink is the leading reason for admission. [1] [2]
Recurrent aphthous stomatitis is the commonest non-infectious ulcer of childhood, affecting up to one in five children at some point, with a family history in many. Minor aphthae dominate; major and herpetiform forms are uncommon but matter because they scar, recur and overlap with systemic disease. Hand-foot-and-mouth disease sweeps through childcare in warm months in epidemic waves driven by Coxsackievirus A16 and Enterovirus 71. [9] [6]
The recurring and refractory lesions share a set of systemic risk factors that the work-up targets: iron, folate and vitamin B12 deficiency, coeliac disease, inflammatory bowel disease, cyclic neutropenia, Behcet disease, HIV and primary immunodeficiency. Oral thrush clusters where the normal flora is disturbed — after antibiotics or inhaled or systemic corticosteroids, in the immunocompromised, and in breastfed infants of mothers with untreated nipple candidiasis. [9] [8]
Pathophysiology
Why do so many childhood ulcers gather in the mouth, and why does the same aphthous pattern sometimes signal systemic disease? The answers lie in how the oral mucosa is built and in what breaks it. [9]
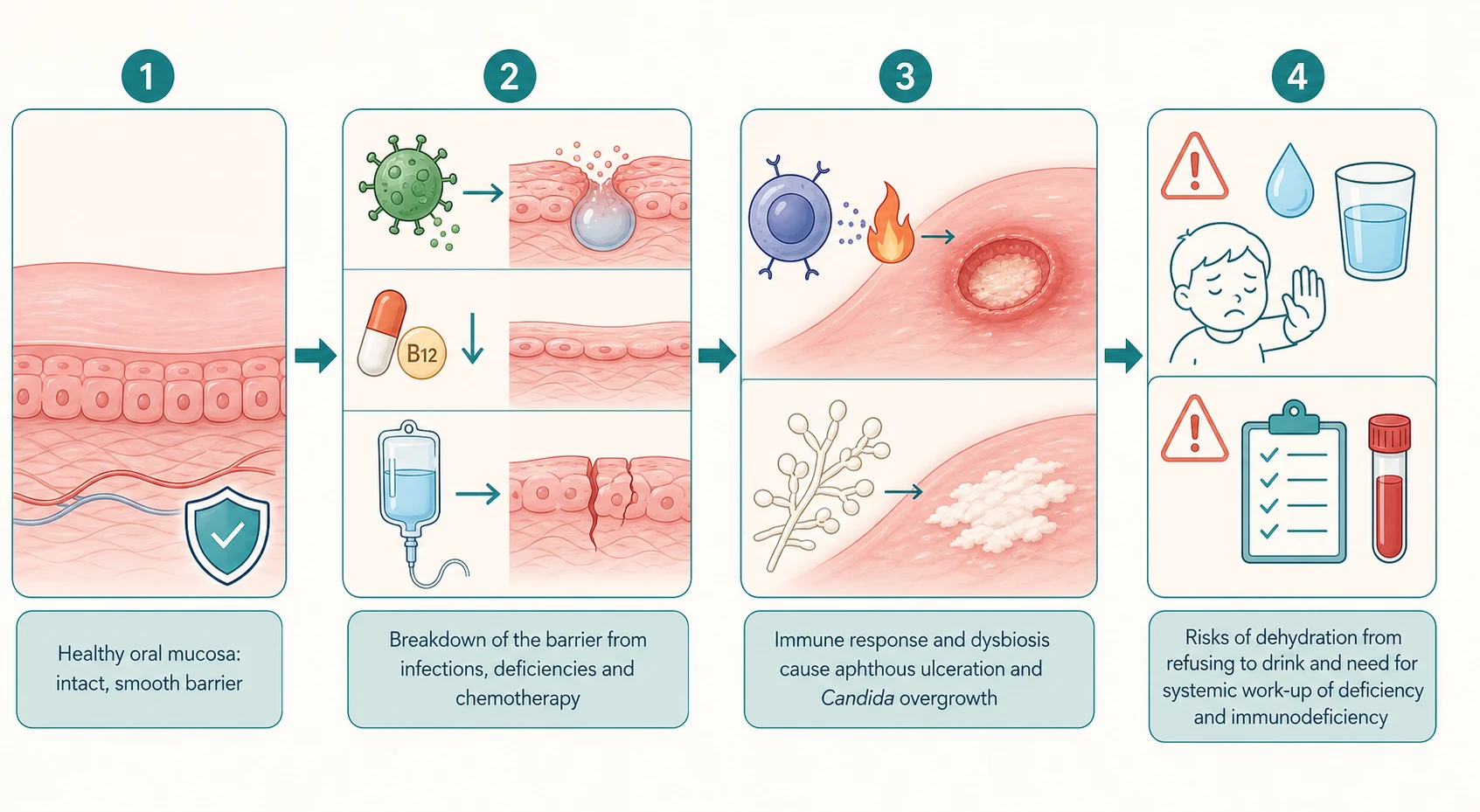
The oral mucosa renews fast and is constantly exposed to thermal, mechanical and microbial insult, so any failure of the epithelial barrier — from a viral cytopathic effect to a nutritional deficiency to a chemotherapeutic hit — shows up quickly as an ulcer. Herpes simplex virus invades and lyses oral keratinocytes, forming vesicles that rupture into the shallow, painful ulcers of gingivostomatitis; enteroviruses do the same in the posterior pharynx of herpangina and hand-foot-and-mouth disease. [2]
Aphthous ulcers sit on the non-keratinised mucosa and follow an immune-mediated, T-cell-driven inflammatory pattern rather than direct infection. That is why deficiency, stress, trauma and food triggers all provoke them. It is also why systemic diseases of immune dysregulation — Behcet, inflammatory bowel disease, the autoinflammatory syndromes — declare themselves through recurrent aphthae. Oral candidiasis is an overgrowth of Candida albicans when the bacterial flora that normally holds it in check is stripped by antibiotics or corticosteroids, or when cell-mediated immunity fails. [9] [8]
Clinical Presentation
Read the mouth the way the age and the distribution tell you to — a febrile toddler with anterior ulceration is herpetic, a school-age child with a few round non-keratinised ulcers is aphthous, and an infant with white plaques is candidal. [1] [9]
Primary herpetic gingivostomatitis opens with high fever, malaise and cervical lymphadenopathy, followed within a day or two by painful vesicles on the gingiva, tongue, lips and buccal mucosa that rupture into shallow ulcers; the gums are swollen, red and bleed easily, the child drools, refuses to eat or drink, and dehydration is the practical threat. Herpangina and hand-foot-and-mouth disease instead cluster small ulcers on the posterior palate, tonsillar pillars and pharynx, and the latter adds the characteristic rash on the palms, soles and buttocks. [1] [6]
Recurrent aphthous stomatitis presents with one to several shallow, round or oval ulcers with a yellow-grey base and an erythematous halo on the non-keratinised mucosa — the buccal and labial mucosa, the floor of the mouth and the ventral tongue, sparing the keratinised gingiva and palate. Minor aphthae are under ten millimetres and heal in ten to fourteen days without scarring; major aphthae exceed ten millimetres, last weeks and scar; herpetiform aphthae are crops of tiny, painful ulcers. Oral candidiasis shows as soft white plaques on the buccal mucosa, tongue or palate that wipe off to leave an erythematous, sometimes bleeding base, most often in infants. [9] [8]
Differential Diagnosis
Build the differential around the site of the ulcer, the distribution across the mouth, and the host, because that trio narrows a wide list to a workable few. [9]
Distinguish the anterior, diffuse, febrile gingivitis of herpes simplex from the posterior palate ulcers with a rash of enteroviral disease, and from the few round non-keratinised aphthae of recurrent aphthous stomatitis. Then separate the common from the systemic: recurrent major aphthae, genital ulcers, eye inflammation, skin lesions or joint pain point to Behcet disease, inflammatory bowel disease or a vasculitis; thrush in an unexpected host points to immunodeficiency; and a single ulcer persisting beyond two to three weeks despite removing trauma needs referral to exclude a neoplastic or non-healing lesion. [9] [10]
The systemic causes of recurrent oral ulcers — SOFT-CELL
Clinical & Bedside Assessment
Start with the history, because the age, the prodrome and the recurrence pattern usually name the pattern before the mouth is even examined. Ask about fever and drooling (herpetic or enteroviral), the number, size and site of the ulcers and whether they recur (aphthous), any rash on the hands and feet (hand-foot-and-mouth), recent antibiotics or inhaled or systemic steroids (candida), and the systemic clues of weight loss, recurrent infection, genital ulcers, eye, skin or joint problems. [1] [9]
Examine the whole mouth with a good light: the gingiva, tongue, buccal mucosa, palate and oropharynx, noting the site, size, number and morphology of the lesions and whether they sit on keratinised or non-keratinised mucosa. Look for the diffuse bleeding gingivitis of HSV, the white wipeable plaques of thrush, the round yellow-based aphthae on non-keratinised mucosa, and the posterior palate lesions with a hand-and-foot rash of enteroviral disease. Palpate for cervical lymphadenopathy, check for dehydration (moist mucous membranes, capillary refill, urine output), and look beyond the mouth for skin, genital and joint signs that turn a local lesion into a systemic one. [8] [6]
Investigations
Most oral ulcers in children are diagnosed clinically and need no investigation; the role of testing is to sort out the recurrent, refractory, major or systemically-flagged lesions. [9]
For the common viral and candidal lesions, the clinical picture is sufficient — swabs and cultures are reserved for atypical, severe, non-healing or immunocompromised children, where a viral PCR or culture of a vesicle, a fungal swab or, rarely, a biopsy of a persistent ulcer can redirect treatment. Send the recurrent aphthae panel when ulcers recur, are major, scar or sit with systemic clues: a full blood count with differential (cyclic neutropenia, cytopenias), iron studies, serum folate and vitamin B12, coeliac serology with total IgA, and a C-reactive protein; add HIV testing and immunology referral where the host suggests it. [9] [10]
Management — Resuscitation
The only oral mucosal disease that commonly needs resuscitation is primary herpetic gingivostomatitis, and the resuscitation mindset is "hydrate first, antiviral second". Most other oral ulcers need definitive topical or supportive care, not resuscitation. [1]
Assess the drooling, febrile child for dehydration — moist mucous membranes, capillary refill, urine output and weight — and correct fluid deficits early, because refusal to drink is the leading reason these children come to hospital. Antiviral therapy does not substitute for fluids: a child who cannot maintain oral hydration needs nasogastric or intravenous fluid while the aciclovir and analgesia take effect. [1] [2]
Management — Definitive & Stepwise
Once the pattern is named, oral ulceration is managed with hydration and analgesia first, then a topical or antiviral agent matched to the cause, with a systemic work-up held in reserve for the recurrent or refractory lesion. [9]
Stepwise management of paediatric oral ulceration
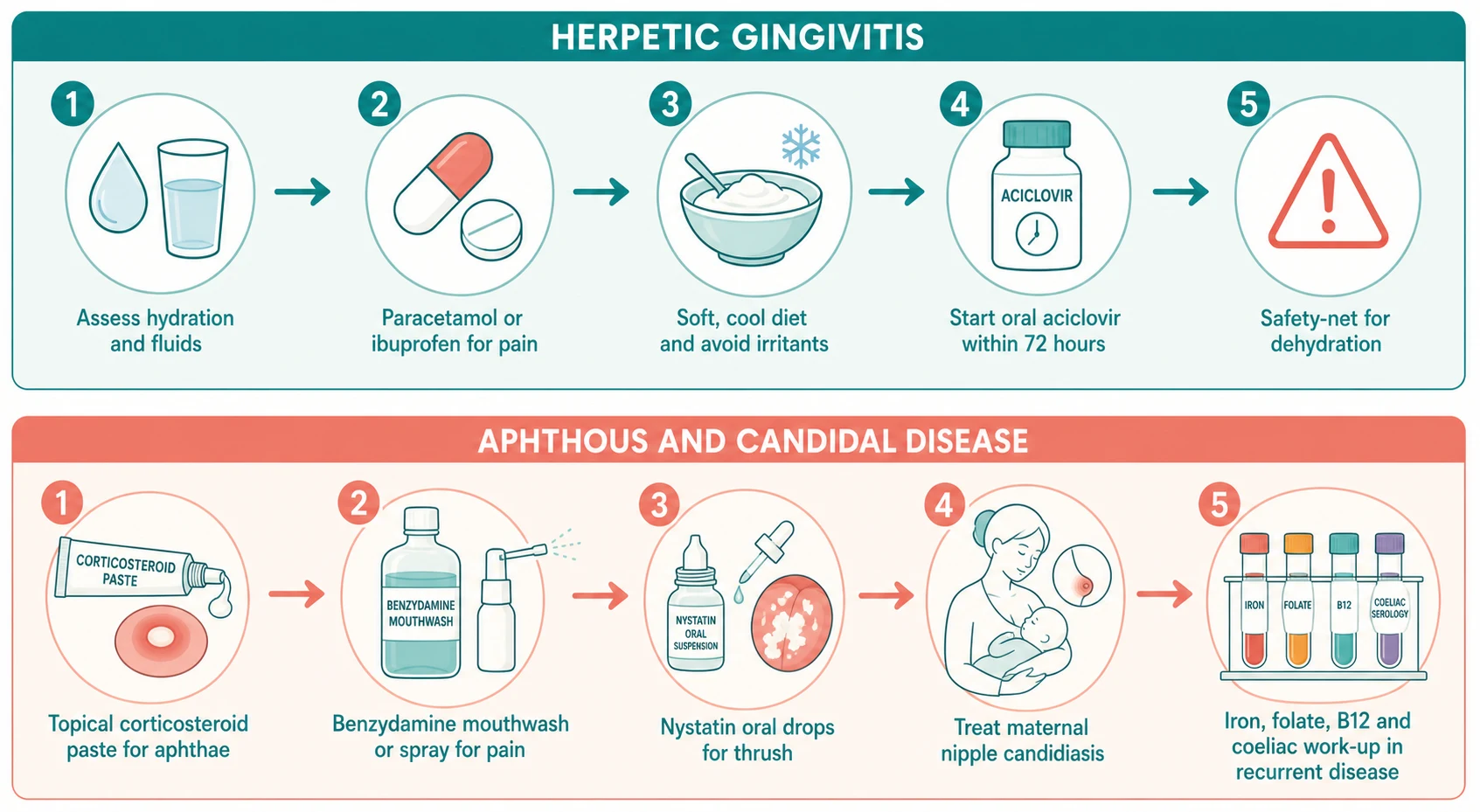
Analgesia and hydration first — paracetamol 15 mg/kg (maximum 1 g) and ibuprofen 5 to 10 mg/kg, a soft bland diet, cool fluids and, where the child refuses to drink, nasogastric or intravenous fluid to protect hydration.
Match the cause — early oral aciclovir for primary herpetic gingivostomatitis within 72 hours; a topical antifungal for oral candidiasis; supportive care only for enteroviral disease; and a topical corticosteroid for aphthous ulcers.
Topical therapy for aphthae — a topical corticosteroid such as hydrocortisone or triamcinolone dental paste, a chlorhexidine mouthwash where the child can rinse, and a topical analgesic such as benzydamine for pain.
Treat the source for thrush — treat any maternal nipple candidiasis and sterilise dummies and bottle teats alongside the topical antifungal, because reinfection otherwise recurs.
Safety-net and review — review the well child in 48 to 72 hours, with return for dehydration, spreading lesions, refusal to drink or persistent ulcers beyond two to three weeks.
For primary herpetic gingivostomatitis, give oral aciclovir 15 mg/kg per dose (maximum 200 mg per dose) five times daily for five to seven days, starting within 72 hours of onset, alongside analgesia, a soft diet and hydration; the original randomised trial showed earlier resolution of fever, pain and feeding difficulty, and shorter viral shedding. [1] [2]
Aciclovir (primary herpetic gingivostomatitis, child)
Dose
15 mg/kg per dose (maximum 200 mg per dose)
For oral candidiasis in infants, give nystatin oral suspension 100,000 units per millilitre, 1 mL applied to each side of the mouth four times daily after feeds for seven days, and treat any maternal nipple candidiasis; miconazole oral gel is an alternative in older infants and children but is avoided in young infants who cannot control the gel at the gum. For recurrent aphthous stomatitis, a topical corticosteroid (hydrocortisone or triamcinolone paste), chlorhexidine mouthwash and a topical analgesic shorten healing and ease pain, with the deficiency and systemic work-up reserved for the recurrent or major case. [8] [10]
Specific Subtypes & Scenarios
The scenarios below are the ones examiners reach for, because each forces a different decision between supportive care, an antiviral or antifungal, and a systemic work-up. [9]
The drooling febrile toddler with diffuse anterior gingivitis is primary herpetic gingivostomatitis — hydrate, give analgesia and weigh early oral aciclovir within 72 hours, because the practical danger is dehydration. The school-age child with a few recurrent round ulcers on the buccal mucosa has minor aphthous stomatitis — a topical corticosteroid, chlorhexidine and analgesia, with the deficiency and coeliac work-up reserved for recurrence. [1] [10]
The infant with white wipeable plaques has oral candidiasis — topical nystatin for seven days and treatment of any maternal nipple candidiasis, with a low threshold to investigate if the thrush is unexpected or refractory. The child on chemotherapy with a painful breaking-down mucosa has oral mucositis — graded with the World Health Organization scale and managed with structured oral care, analgesia, and, where appropriate, cryotherapy or palifermin, because prevention beats treatment. [8] [4]
The child with clockwork fevers, pharyngitis, cervical adenitis and aphthae has the PFAPA syndrome — a single dose of corticosteroid at flare onset usually aborts the attack, colchicine prophylaxis reduces recurrence in some, and tonsillectomy is considered for refractory disease. The child with wandering red patches and white borders on the tongue has geographic tongue — it is benign and needs only reassurance. [3] [7]
Complications & Pitfalls
The cardinal pitfall is treating every oral ulcer as a self-limiting lesion and missing the dehydrating herpetic gingivitis, the systemic aphthosis or the immunodeficient thrush. A febrile drooling toddler who will not drink is a hydration problem until proven otherwise, and recurrent major aphthae are a systemic work-up, not a stronger mouthwash. [1] [9]
Recognise the local complications of dehydration and secondary bacterial infection in herpetic gingivitis, scarring and recurrence in major aphthae, and the pain, bleeding and infection that complicate oncology mucositis. The dangerous systemic associations are Behcet disease with eye and vascular disease, inflammatory bowel disease, cyclic neutropenia with sepsis, and HIV or primary immunodeficiency presenting through the mouth. Avoid routine antibiotics for uncomplicated viral ulcers, avoid inhaled corticosteroids without a spacer and mouth-rinse in the child with recurrent thrush, and never let a single persistent ulcer drift past the two-to-three-week review without referral. [4] [9]
Prognosis & Disposition
Primary herpetic gingivostomatitis resolves within ten to fourteen days with supportive care and early aciclovir, and recurrence later in life usually takes the milder form of cold sores rather than a repeat gingivitis. Minor aphthous ulcers heal in ten to fourteen days without scarring, and the prognosis is excellent once the precipitant or deficiency is addressed; hand-foot-and-mouth disease is self-limiting in seven to ten days. [1] [6]
Discharge the well-hydrated child on supportive care, analgesia and a topical or antiviral agent with a clear safety-net for dehydration, spreading lesions, refusal to drink and ulcers persisting beyond two to three weeks. Admit the dehydrated or young child with herpetic gingivitis for fluid and analgesia, and refer the child with recurrent major aphthae, systemic signs or a non-healing ulcer for the deficiency, coeliac and immunology work-up. [9]
Special Populations
Immunocompromised children — oncology patients, post-transplant recipients, neutropenic and HIV-infected children — are the population in whom oral mucosal disease crosses from nuisance to danger: thrush becomes refractory, herpes reactivates and extends, and mucositis runs a severe, prolonged course. Investigate and escalate aggressively, and use intravenous aciclovir and systemic antifungals where the host demands it. [4] [8]
Aboriginal and Torres Strait Islander and other remote-community children carry a disproportionate burden of enteroviral and herpetic oral disease where crowding, climate and access barriers converge. Provide culturally safe care with trained interpreters, linked to oral-health and chronic-disease programs. Children with recurrent thrush from inhaled corticosteroids need a spacer and a post-inhaler mouth-rinse, not just more antifungal. Children with recurrent aphthae and a deficiency or coeliac disease need the underlying condition treated alongside the topical care. [6] [9]
Evidence, Guidelines & Regional Differences
The named regional guidance is the RCH Melbourne guideline on stomatitis and on herpes simplex virus infections, the NICE CKS on oral candidiasis, and the eTG antimicrobial guidance in ANZ, with the AAP and Red Book guidance on paediatric oral infections in North America. The cornerstone evidence for early aciclovir in herpetic gingivitis is the 1997 Amir randomised controlled trial, updated by a 2023 systematic review of supportive care and antivirals in primary herpetic gingivostomatitis. [1] [2]
The evidence base for recurrent aphthous stomatitis favours topical corticosteroids, chlorhexidine and topical analgesics, with the systemic work-up driven by the deficiency, coeliac and autoinflammatory associations. For PFAPA, corticosteroids abort flares, colchicine offers prophylaxis in some, and tonsillectomy is reserved for refractory disease. For oncology mucositis, structured oral care, cryotherapy and palifermin lead the prevention evidence. There is genuine controversy over the role of "magic mouthwash" combination rinses, where evidence is limited and sedation or aspiration risk in young children is a concern. [3] [4] [10]
[2] [8]Exam Pearls
References
- [1]Amir J; Harel L; Smetana Z; et al Treatment of herpes simplex gingivostomatitis with aciclovir in children: a randomised double blind placebo controlled study. BMJ, 1997.PMID 9224082
- [2]Coppola N; Cantile T; Adamo D; et al Supportive care and antiviral treatments in primary herpetic gingivostomatitis: a systematic review. Clin Oral Investig, 2023.PMID 37733027
- [3]Anselmi F; Dusser P; Kone-Paut I Periodic Fever, Aphthous Stomatitis, Pharyngitis, and Cervical Adenitis (PFAPA) Syndrome in Children-From Pathogenesis to Treatment Strategies: A Comprehensive Review. Paediatr Drugs, 2025.PMID 40632467
- [4]Mulinda C; Kinariwalla N; DeFelice AR; et al Management of Oral Mucositis in Pediatric Patients: A Practical Overview of Available Treatment. Pediatr Dermatol, 2025.PMID 40358941
- [5]Dipasquale RF; Sinopoli P; Mendicino A; et al Colchicine prophylaxis in pediatric PFAPA: a systematic review. Eur J Pediatr, 2026.PMID 41495479
- [6]Selene NB; Situmorang NY Preventive Strategies of Hand, Foot, and Mouth Disease in Children: A Review. Turk Arch Pediatr, 2025.PMID 42391430
- [7]Bakshi SS Benign migratory glossitis. Turk J Pediatr, 2019.PMID 31990488
- [8]Pankhurst CL Candidiasis (oropharyngeal). BMJ Clin Evid, 2013.PMID 24209593
- [9]Lau CB; Smith GP Recurrent aphthous stomatitis: A comprehensive review and recommendations on therapeutic options. Dermatol Ther, 2022.PMID 35395126
- [10]Barrons RW Treatment strategies for recurrent oral aphthous ulcers. Am J Health Syst Pharm, 2001.PMID 11194135