Paeds · ent-hearing-and-oral-health
Otitis externa
Also known as Swimmer's ear · External otitis · Acute diffuse otitis externa · Necrotising otitis externa · Malignant otitis externa · Otomycosis · Furunculosis of the ear canal
Fellowship topic on otitis externa — inflammation of the external auditory canal. Covers the acute diffuse (swimmer's ear), furuncular, eczematous, fungal and necrotising (malignant) forms; the cerumen-defence and pH pathophysiology that explains why water and trauma drive Pseudomonas and Staphylococcus overgrowth, and why Pseudomonas invades the skull base in the immunocompromised child; the tragal-tenderness and pain-on-pull bedside signs that separate it from acute otitis media; aural toilet, topical antimicrobial drops and ear-wick stepwise care; and the emergency recognition of necrotising otitis externa with prolonged antipseudomonal therapy, cranial-nerve and skull-base imaging, and ANZ, UK, US and Canadian guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A mother brings her eight-year-old to the emergency department after a week of swimming lessons: two days of worsening ear pain, a mucky discharge, and a child who cries when the ear is touched. Pull gently on the pinna and press the tragus, and she flinches — that is the canal, not the middle ear, and it changes everything that follows. The fellowship skill in otitis externa is to localise the disease to the external canal, classify its form, treat it topically, and never miss the one form that invades the skull base. [1] [4]
Otitis externa is inflammation of the skin and subcutaneous tissue of the external auditory canal, from the conchal bowl and meatus in to the tympanic membrane. It is one of the commonest ear complaints of childhood, peaking in swimmers and in hot, humid weather, and it is overwhelmingly manageable in primary care with topical therapy. The term spans a spectrum: the common acute diffuse swimmer's ear, a localised furuncle, an eczematous or dermatitic canal, a fungal (otomycotic) infection, the chronic low-grade form, and the rare but dangerous necrotising (malignant) form that invades the skull base. [1] [3]
What makes the topic examinable is that the same canal anatomy produces behaviours ranging from trivial to life-threatening. Most otitis externa is a surface problem fixed by drops and drying; necrotising otitis externa is a deep, destructive osteomyelitis that needs weeks of systemic therapy and carries real mortality. The clinical hinge between them is the host and the depth of invasion: the well child has a surface infection, while the diabetic or immunocompromised child is the one in whom Pseudomonas reaches bone. Recognising that distinction at the bedside is the point of the topic. [7] [8]
Classification
Picture the six forms laid out by what is growing in the canal and how deep it goes, because that is what drives the treatment. [3]
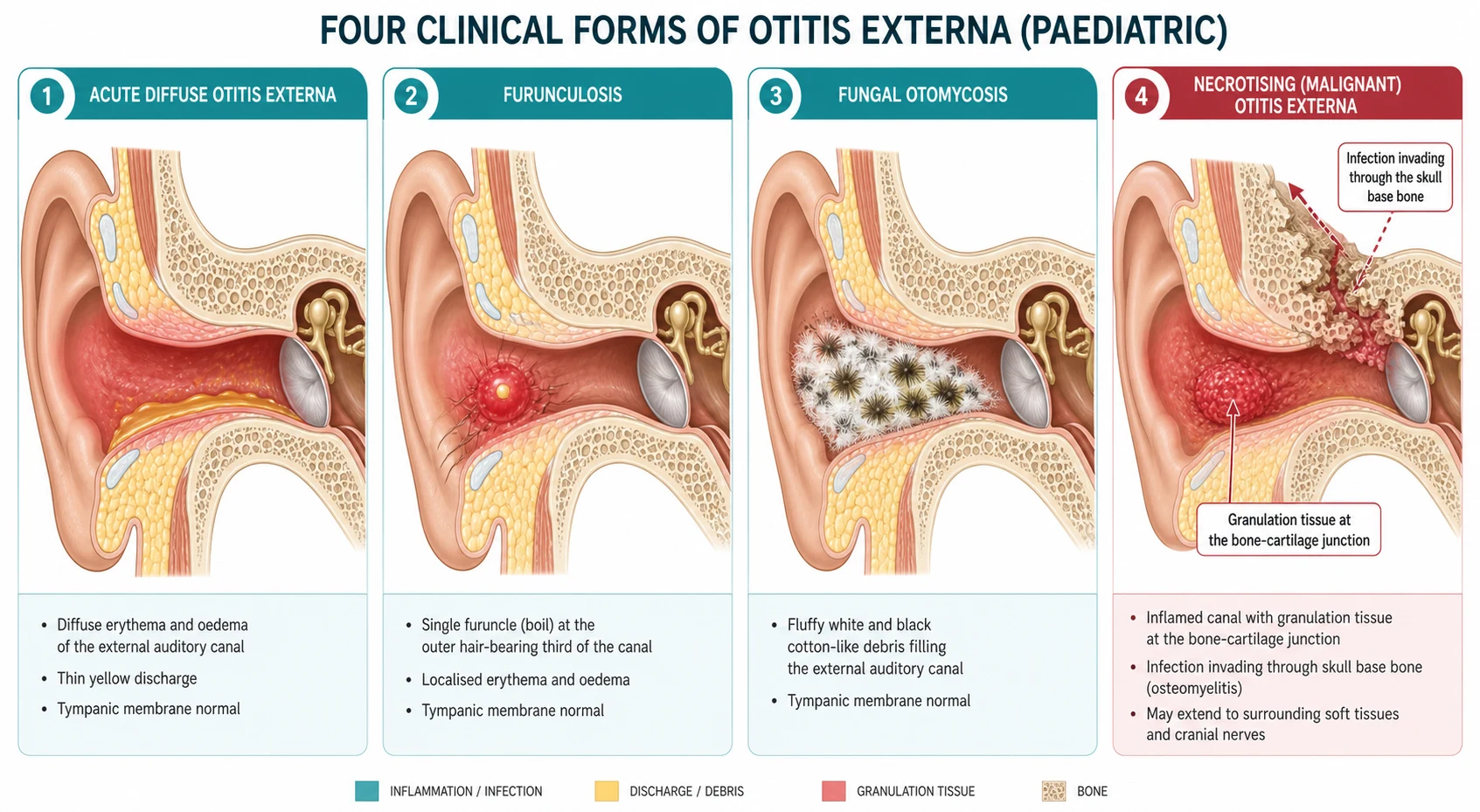
The clinical forms of otitis externa in children
The classification does more than label — it triages. The first four are canal-surface problems managed with topical therapy and ear care. The fifth, chronic otitis externa, signals a persistent insult — a skin disease, a chronically wet canal, a hearing aid — and is managed by removing the driver as much as by drops. The sixth, necrotising otitis externa, is a deep bone infection that bypasses topical care entirely and needs systemic therapy and imaging. The depth of invasion, set by the host's immunity and diabetes status, is the single most important axis of the classification. [7] [11]
Epidemiology & Risk Factors
Otitis externa is common: it accounts for a large share of ear-related primary-care visits in children, and its incidence rises sharply in the swimming months and in hot, humid climates. The lifetime point prevalence is around one in ten, and swimmers develop it several times more often than non-swimmers. Where swimming-pool hygiene is poor or canal trauma is common, the burden climbs further. [1] [4]
The core risk factors cluster around two themes — a wet canal and a damaged canal. Water exposure from swimming, bathing or humid weather macerates the canal skin; trauma from cotton buds, scratching, earphones or hearing aids removes the protective cerumen and breaches the epithelium; and occlusion by hearing aids, cochlear-implant processors or earplugs traps moisture. These raise the canal pH, strip the acidic cerumen layer, and let Pseudomonas and Staphylococcus overgrow. Underlying skin disease — eczema, psoriasis, seborrhoea — and allergic contact dermatitis to neomycin or hair products produce an eczematous canal that is easily secondarily infected. [1] [3]
Necrotising otitis externa has its own risk profile: diabetes mellitus and immunocompromise. In children the immunocompromised host dominates — oncology patients, post-transplant recipients, neutropenic and HIV-infected children, and those on immunosuppression — alongside the diabetic child. A 2024 paediatric scoping review confirmed that immunocompromise and diabetes are the cardinal paediatric risk factors, and a 15-year Central Australian review documented a disproportionate burden among Aboriginal children in remote settings, where diabetes, water exposure and access barriers converge. Obesity has additionally been linked to poorer treatment outcomes in children. [7] [8] [12]
Pathophysiology
Why does swimmer's ear follow swimming, and why does the same organism, Pseudomonas, sometimes invade the skull base? The answers lie in the canal's defences and in how the host's immunity sets the depth of invasion. [3]
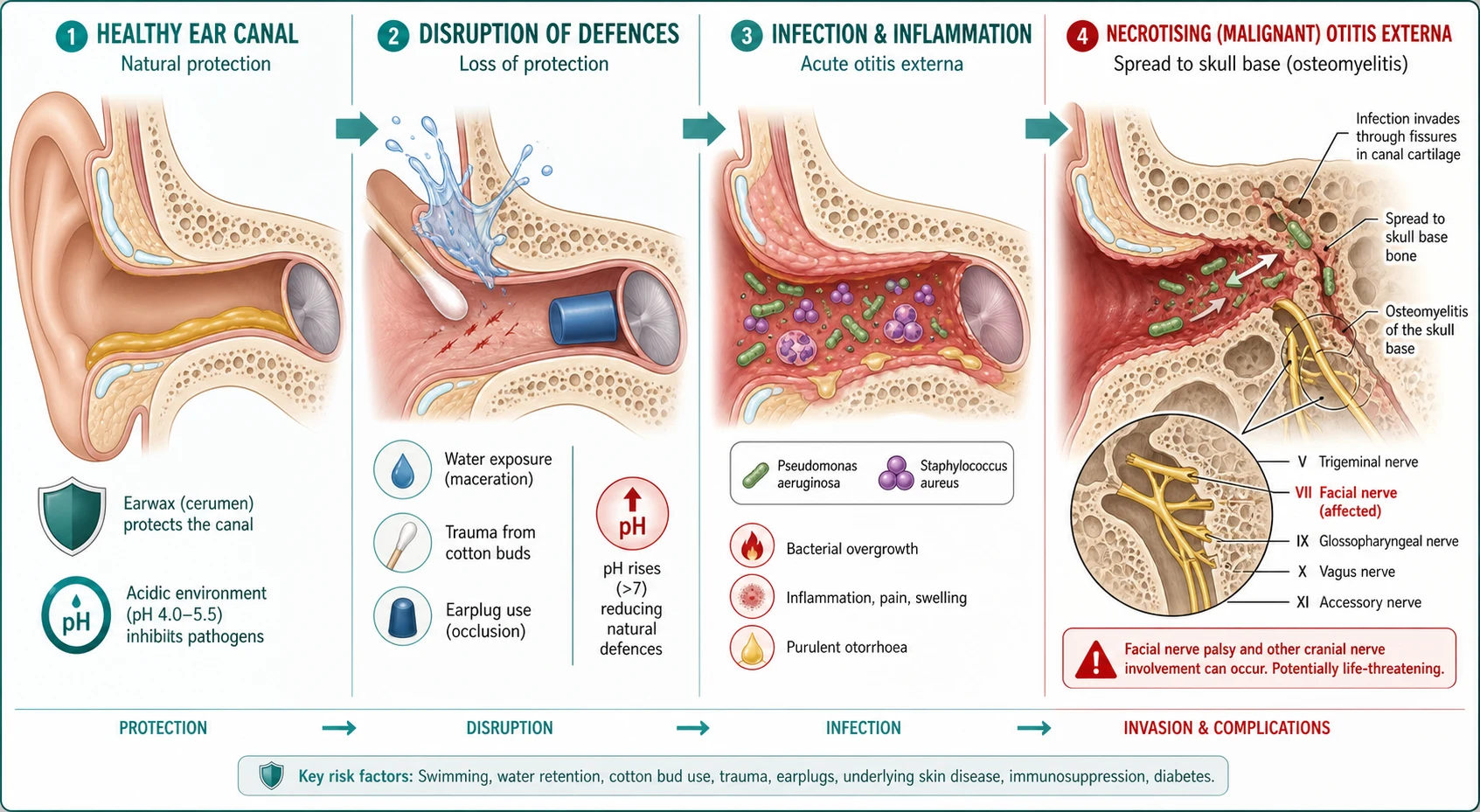
The healthy external canal defends itself with cerumen and epithelial migration. Cerumen is a hydrophobic, mildly acidic (pH around 4 to 5) film that contains lysozyme and fatty acids and repels water; the canal epithelium migrates outward from the eardrum, sweeping debris and desquamated cells towards the meatus. Together these keep the canal dry, acidic and self-cleaning. Water exposure and trauma defeat both mechanisms: they wash away or pack the cerumen, raise the canal pH towards neutral, and macerate or abrade the skin. An alkaline, wet, denuded canal is precisely the environment Pseudomonas aeruginosa and Staphylococcus aureus exploit. [1] [3]
In acute diffuse otitis externa, the bacteria multiply in the now-vulnerable canal, provoking an acute inflammatory response — oedema, erythema, exudate and the characteristic pruritus and otalgia. The swelling narrows the canal lumen, traps debris, and can occlude it entirely so that drops cannot pass. Pseudomonas dominates because it thrives in warm, moist, alkaline conditions; Staphylococcus aureus is the other major pathogen, and is the organism of localised furunculosis in the hair-bearing outer third. Fungal otomycosis follows prolonged moisture or after broad-spectrum antibiotic drops have removed the bacterial competition, with Aspergillus (often niger, producing black fluffy debris) and Candida producing intense pruritus and a cotton-like discharge. [3] [4]
In necrotising otitis externa, the same Pseudomonas aeruginosa crosses a threshold the well child's immunity would have held. In the diabetic or immunocompromised host the organism invades through Santorini's fissures — the small clefts in the cartilaginous canal that lack subcutaneous fat — and reaches the skull base, where it sets up an osteomyelitis of the temporal bone. The infection spreads along the skull base to the cranial-nerve foramina: the facial nerve is affected first and most often, and lower cranial nerves (nine, ten, eleven, twelve) follow as the osteomyelitis extends. This is why a facial palsy with a painful discharging ear in an immunocompromised child is a skull-base emergency rather than a routine complication. [7] [11]
Clinical Presentation
Read the ear the way the history tells you to — water and trauma point to a surface infection, while severe pain in a vulnerable host points to the skull base. [1]
Acute diffuse otitis externa presents with otalgia, otorrhoea and pruritus, a feeling of fullness, and a mild conductive hearing loss from debris and canal oedema. The pain is characteristically worsened by movement of the jaw or by touching the ear, and the discharge may be serous early and mucopurulent later. The two bedside signs that localise the problem to the canal are tenderness on pressing the tragus and pain on pulling the pinna backwards and upwards — positive in otitis externa and notably absent in acute otitis media, where the canal is painless. The canal is erythematous, oedematous and partly occluded with debris, and once cleaned the tympanic membrane is normal. [1] [4]
Acute localised otitis externa (furunculosis) is a tender, discrete red swelling in the hair-bearing outer third of the canal, caused by Staphylococcus aureus. The pain is often severe and focal, and the boil may point and discharge. Fungal otomycosis presents with intense itching, a sense of fullness, and fluffy white (Candida) or black-and-white (Aspergillus niger) cotton-like debris resembling wet newspaper. Eczematous or dermatitic otitis externa presents with a dry, scaly, fissured and itchy canal in a child with eczema, psoriasis or a reaction to a topical agent such as neomycin. [3] [4]
The presentation that must never be missed is necrotising otitis externa. The red-flag features are severe, unremitting, often nocturnal otalgia that is out of proportion to the visible canal signs, persistent purulent otorrhoea, granulation tissue at the bony-cartilaginous junction, and — critically — a cranial-nerve palsy, most often the facial nerve. The child is usually diabetic or immunocompromised, and may have systemic upset and elevated inflammatory markers. Any painful discharging ear with a facial palsy in such a child is necrotising otitis externa with skull-base osteomyelitis until proven otherwise. [7] [9]
Differential Diagnosis
Build the differential around the single most important distinction — a canal problem versus a middle-ear problem — then strip out the mechanical and dermatological mimics. [3]
The cardinal differential is acute otitis media. Both cause ear pain and discharge, but acute otitis media has a painless canal with negative tragal tenderness, a bulging, erythematous or perforated tympanic membrane, and systemic features such as fever. Otitis externa has the opposite: marked tragal tenderness and pain on pinna traction, a swollen debris-filled canal, and a normal eardrum once cleared. When the canal is too swollen to see the drum, treat the canal but keep acute otitis media on the differential and review. [1] [4]
The mechanical and dermatological group includes a retained foreign body (a bead, a piece of cotton, or the classic button battery, which causes a blackened, caustic canal that is an emergency in itself), impacted cerumen causing fullness and mild pain, and contact dermatitis from a topical agent or hair product. A cholesteatoma can present with chronic otorrhoea and canal granulation, and mastoiditis with postauricular pain, swelling and a forward-displaced pinna. The practical pivot is to clear the canal and view the eardrum: a normal drum with a tender canal is otitis externa; a middle-ear finding changes the diagnosis entirely. [3] [4]
Use the history, the tragal-tenderness sign, and a cleared view of the tympanic membrane to separate the canal from the middle ear, and the host and the depth of pain to separate the surface forms from necrotising disease. A retained foreign body or a button battery must always be excluded in a child with a unilateral painful discharging ear. [1] [3]
Clinical & Bedside Assessment
Start with the history, because the precipitant usually names the form. Ask about water exposure (swimming, bathing), canal trauma (cotton buds, scratching, earbuds), occluding devices (hearing aids, earplugs, cochlear-implant processors), underlying skin disease or dermatitis, any topical agent already used, and — crucially — diabetes or immunocompromise. In the immunocompromised or diabetic child with severe pain, switch your threshold for escalation immediately. [1] [7]
On examination, document the two localising signs first: tenderness on pressing the tragus, and pain on gently pulling the pinna backwards and upwards. Both point to the canal. Examine the pinna and periauricular skin for cellulitis or perichondritis, and palpate for preauricular or cervical lymphadenopathy. Then perform otoscopy — the canal is erythematous, oedematous and narrowed, with debris and discharge; note the character and colour of the discharge (serous, mucopurulent, fluffy-fungal, blood-stained). Clear the canal gently to view the tympanic membrane, which is normal in uncomplicated otitis externa; a bulging or perforated drum redirects the diagnosis to acute otitis media. [1] [4]
Look specifically for the necrotising-otitis-externa signs: granulation tissue at the bony-cartilaginous junction (the deep junction of cartilaginous and bony canal), a facial-nerve palsy, and any lower cranial-nerve deficit. Perform a cranial-nerve examination in any immunocompromised or diabetic child with severe otalgia. The granulation at that junction is the single most specific bedside finding for skull-base involvement, and a facial palsy in this context is an emergency. [7] [11]
For most acute otitis externa no investigations are needed — it is a clinical diagnosis. Send an ear-canal swab for culture when the disease is recurrent, severe, not responding to first-line drops, fungal is suspected, or the child is immunocompromised. In suspected necrotising otitis externa, the work-up changes scale: inflammatory markers (C-reactive protein and erythrocyte sedimentation rate, typically markedly elevated), a blood glucose and HbA1c, and skull-base imaging, with ENT and infectious-diseases involvement. [3] [10]
Investigations
Uncomplicated acute otitis externa is diagnosed and treated clinically — the role of investigation is to sort out the atypical, recurrent and dangerous cases. [1]
For the recurrent, severe or non-responsive case, send an ear-canal swab for bacterial and fungal culture to direct topical or systemic therapy and to identify resistant organisms or unexpected fungi. A swab is also reasonable before starting treatment in the immunocompromised child, where the organism and its sensitivities matter more. Culturing every simple case adds nothing and is not recommended. [1] [3]
For suspected necrotising otitis externa, the laboratory panel centres on C-reactive protein and erythrocyte sedimentation rate, which are characteristically high and serve both as diagnostic support and as the key markers of treatment response over weeks of therapy. Add a blood glucose and HbA1c to detect or characterise diabetes, a full blood count, and renal function if an aminoglycoside or nephrotoxic agent is contemplated. Biopsy of the granulation tissue excludes a malignancy or an unusual organism and is recommended when the response is poor or the diagnosis uncertain. [7] [11]
Imaging is the cornerstone of necrotising-otitis-externa diagnosis and follows the ACR Appropriateness Criteria for inflammatory ear disease. Computed tomography of the temporal bone is first-line, showing bony erosion and cortical destruction; magnetic resonance imaging adds soft-tissue, skull-base and cranial-nerve detail and detects intracranial extension; and a technetium-99m bone scan is highly sensitive for osteomyelitis (staying positive long after healing), while a gallium-67 scan tracks active inflammation and is used to monitor treatment response. The standard teaching is a technetium scan to diagnose and serial gallium scans (or CRP) to confirm resolution before stopping therapy. [10] [11]
[11]Management — Resuscitation
The only form of otitis externa that needs resuscitation is necrotising otitis externa, and the resuscitation mindset is "recognise, then escalate". The well child with acute diffuse otitis externa needs no resuscitation — start definitive topical care. [1]
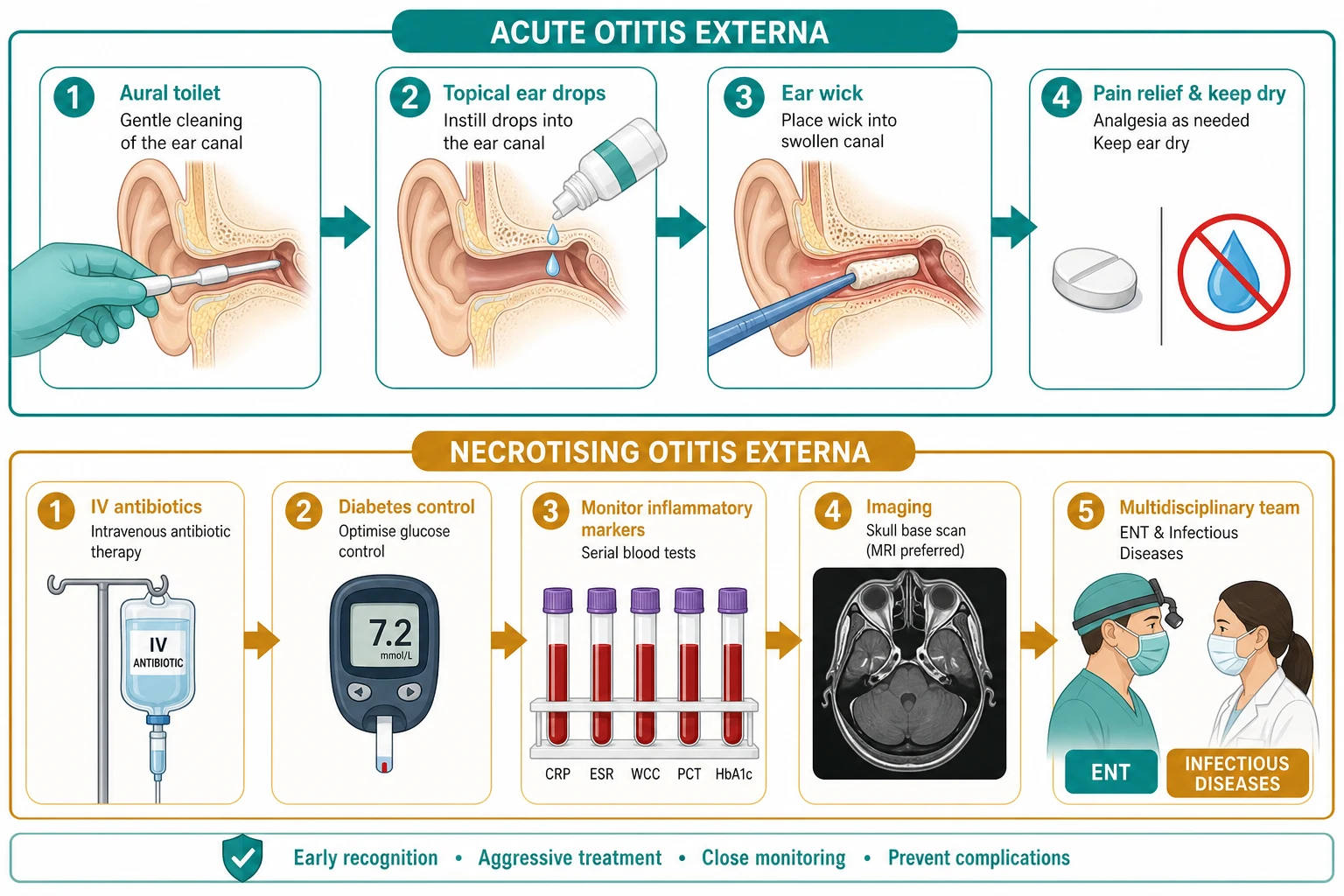
Recognise necrotising otitis externa from the red-flag triad — severe unremitting otalgia, granulation at the bony-cartilaginous junction, and a cranial-nerve palsy in a diabetic or immunocompromised child — and act. Admit the child, take an ear swab and granulation biopsy, send inflammatory markers and a blood glucose, arrange urgent skull-base imaging, and start systemic antipseudomonal therapy. Secure pain control, treat hyperglycaemia tightly, and involve ENT and infectious diseases immediately. [7] [11]
The first-line systemic agent is classically oral ciprofloxacin, chosen for its anti-pseudomonal activity and excellent bone penetration and bioavailability, at 10 to 20 mg per kilogram (maximum 750 mg) every 12 hours for many weeks, guided by the clinical response and serial inflammatory markers. For the severely ill, resistant organism, or where oral therapy is not feasible, use an intravenous antipseudomonal beta-lactam such as ceftazidime or cefepime under infectious-diseases guidance. Therapy continues until the pain and cranial-nerve signs resolve and the C-reactive protein and erythrocyte sedimentation rate normalise — typically six or more weeks — with a gallium scan confirming resolution before stopping. [7] [9]
The key principle is to separate resuscitation from definitive care. The surface forms need topical therapy and analgesia; necrotising otitis externa needs immediate admission, imaging, biopsy and prolonged systemic therapy. The decision is made on the host and the depth of pain, not on the culture plate, and a delay to "see if the drops work" in an immunocompromised child can be fatal. [8] [11]
Management — Definitive & Stepwise
Once the form is named, acute otitis externa is managed topically and analgesia-first, with oral antibiotics reserved for extension beyond the canal. [1]
Stepwise management of acute diffuse otitis externa
Analgesia — paracetamol 15 mg/kg (maximum 1 g) and ibuprofen 5 to 10 mg/kg every six to eight hours; add a stronger agent for severe pain, because the AAO-HNS guideline makes adequate pain control a key action statement.
Aural toilet — gently clear canal debris and discharge so the topical agent reaches the skin; repeat as needed.
Topical antimicrobial, usually with a corticosteroid — instil two to three drops into the affected ear two to three times daily for about seven days; options include an aminoglycoside (neomycin, polymyxin B, with a corticosteroid) or a fluoroquinolone (ciprofloxacin, with or without hydrocortisone or dexamethasone).
If the canal is too swollen to admit drops — insert an ear wick, moisturise it with the drops, leave it two to three days, and review.
Ear care and safety-net — keep the ear dry (no swimming), avoid cotton buds, and return for spreading redness, fever, or severe worsening pain.
A 2023 systematic review and meta-analysis found topical antimicrobials effective for acute otitis externa, with no benefit from adding oral antibiotics in uncomplicated disease, supporting the topical-first approach. A randomised trial likewise confirmed the efficacy of a ciprofloxacin-corticosteroid combination. Choose a fluoroquinolone drop (such as ciprofloxacin with dexamethasone or hydrocortisone) when the tympanic membrane may be perforated or is not fully visible, because of the ototoxicity concern with aminoglycosides in the presence of a middle-ear breach. Aminoglycoside drops remain widely used but are best avoided where the eardrum is known or likely to be ruptured. [5] [6]
For the too-swollen canal, an ear wick (a compressed sponge or ribbon) is placed into the canal, expanded by the drops, and left for two to three days to deliver medication beyond the stenosis; this is the standard step when drops cannot pass. Reserve oral antibiotics for spreading periauricular cellulitis, perichondritis, systemic features, or a child who cannot use topical therapy — a first-generation cephalosporin such as cephalexin 25 mg per kilogram (maximum 500 mg) every six hours, or flucloxacillin for staphylococcal disease, is appropriate. Furunculosis is usually managed with warmth and analgesia, with flucloxacillin if it is spreading or recurrent. [1] [4]
Cephalexin (spreading cellulitis from otitis externa, child)
Dose
25 mg/kg (maximum 500 mg) orally
Ciprofloxacin oral (necrotising otitis externa, child)
Dose
10 to 20 mg/kg (maximum 750 mg) every 12 hours
Specific Subtypes & Scenarios
The scenarios below are the ones examiners reach for, because each forces a different decision. [3]
Acute diffuse otitis externa after swimming is the archetype: otalgia, otorrhoea and pruritus with tragal tenderness and a swollen canal. Manage with analgesia, aural toilet and a topical antimicrobial with corticosteroid for about seven days, keeping the ear dry. The chief error is prescribing oral antibiotics for a canal-surface infection that topical therapy treats effectively. [1] [5]
The too-swollen canal that will not admit drops needs an ear wick — placed into the canal, expanded by the drops, and left for two to three days with review. Forgetting the wick and relying on drops that never reach the skin is a common reason for apparent treatment failure. Once the oedema settles, complete the course with direct drops. [1] [4]
Furunculosis presents with a focal, exquisitely tender swelling in the outer hair-bearing third of the canal, caused by Staphylococcus aureus. Most settle with warmth and analgesia; add oral flucloxacillin if it is spreading, recurrent or accompanied by systemic features. Eczematous or dermatitic otitis externa is managed by removing the trigger (a neomycin-containing drop, a hair product), topical corticosteroid to the canal, and treating the underlying dermatosis. [3] [4]
The immunocompromised or diabetic child with severe ear pain is the scenario that defines the topic. Severe unremitting otalgia with granulation at the bony-cartilaginous junction, or any cranial-nerve palsy, is necrotising otitis externa with skull-base osteomyelitis until proven otherwise. Admit, image, biopsy, and start prolonged systemic antipseudomonal therapy; the cost of treating such a child with drops alone is osteomyelitis, cranial-nerve loss and death. [7] [8]
Complications & Pitfalls
The cardinal pitfall is treating otitis externa as a one-size-fits-all canal infection and missing necrotising disease in the immunocompromised or diabetic child. Severe pain in a vulnerable host is not "bad swimmer's ear" — it is skull-base osteomyelitis until excluded. [7]
The local complications of acute otitis externa are canal stenosis, chronicity, pinna cellulitis and perichondritis, and rarely an external-canal cholesteatoma from chronic obstruction. These follow neglected or recurrent surface disease and reinforce the importance of aural toilet and completing the topical course. [1] [3]
The dangerous complications are those of necrotising otitis externa: skull-base osteomyelitis, cranial-nerve palsies (the facial nerve first, then the lower cranial nerves), meningitis, brain abscess, sigmoid-sinus thrombosis and death. A mortality meta-analysis confirmed that malignant otitis externa retains real mortality even with modern therapy, underscoring early recognition. Missing a retained button battery foreign body masquerading as otitis externa is another recurrent, avoidable error that causes liquefactive canal damage. [9] [11]
Avoid aminoglycoside drops when the tympanic membrane may be perforated, because of the ototoxicity concern; use a fluoroquinolone drop instead. Do not prescribe oral antibiotics for uncomplicated canal-surface disease, and do not insert a cotton bud into a child's ear — patient and parent education on ear care is part of the treatment and the prevention of recurrence. [1] [5]
Prognosis & Disposition
Acute diffuse otitis externa has an excellent prognosis: most children settle within seven to ten days of topical therapy, with full recovery and no long-term sequelae. Recurrence is common when the precipitant — swimming, trauma, an occluding device, a skin disease — persists, which is why ear-care advice is as important as the drops. [1] [3]
Discharge the well child with acute otitis externa on topical therapy, analgesia and a clear safety-net for spreading redness, fever, severe worsening pain, or any facial weakness. The parents must know to keep the ear dry and to avoid cotton buds, and that a swimmer's ear can recur with further water exposure. [4] [12]
Admit the child with necrotising otitis externa, spreading cellulitis or perichondritis, or significant systemic upset. Necrotising disease needs inpatient systemic therapy, imaging, tight glycaemic control and serial inflammatory-marker monitoring, often for many weeks, and the durable message is that early recognition transforms the outcome — mortality falls sharply with prompt, prolonged antipseudomonal therapy. [7] [9]
Special Populations
Diabetic and immunocompromised children — oncology patients, post-transplant recipients, neutropenic and HIV-infected children, and those on immunosuppression — are the population in whom otitis externa crosses into necrotising disease. In any such child, a painful discharging ear is investigated and escalated aggressively, and tight glycaemic control is part of the treatment. [7]
Aboriginal and Torres Strait Islander, and other remote-community children, carry a disproportionate burden of necrotising otitis externa. A 15-year Central Australian review documented malignant otitis externa in this population, where diabetes, water exposure, humidity and access barriers converge; care must be culturally safe, with trained interpreters, and linked to chronic-disease and ear-health programs. [8]
Children with hearing aids, cochlear-implant processors and earplugs develop otitis externa from occlusion and trapped moisture; managing it means device hygiene, drying periods, and treating the canal, not simply stopping the device where it is developmentally essential. Swimmers and children in humid climates benefit from preventive ear care — drying the canal after swimming and avoiding cotton buds — and from swimming-pool water-quality measures. [1] [3]
Children with chronic skin disease (eczema, psoriasis) and those with obesity or socioeconomic and linguistic barriers have poorer treatment outcomes and higher recurrence; address the dermatosis and the access barriers alongside the drops, and ensure the family can obtain and use the topical agent correctly. [12]
Evidence, Guidelines & Regional Differences
The named regional guidance is the AAO-HNS 2014 Clinical Practice Guideline on acute otitis externa (Rosenfeld et al), the NICE CKS on otitis externa, the RCH Melbourne and eTG guidance in ANZ, and the ACR Appropriateness Criteria for inflammatory ear disease imaging. [1] [10]
The AAO-HNS guideline makes adequate pain control a key action statement, recommends topical antimicrobial therapy (with or without a corticosteroid) for the diffuse acute form, advises aural toilet, and cautions against routine systemic antibiotics for uncomplicated disease. It also flags the ear wick for the occluded canal and emphasises patient education to keep the ear dry and avoid self-instrumentation. [1] [2]
The evidence base now supports the topical-first approach: a 2023 systematic review and meta-analysis found topical antimicrobials effective for acute otitis externa with no added benefit from oral antibiotics in uncomplicated disease, and a randomised trial confirmed the efficacy of a ciprofloxacin-fluocinolone combination. The paediatric necrotising-otitis-externa evidence was consolidated in a 2024 scoping review, and a mortality meta-analysis quantified the residual mortality that justifies aggressive early therapy. [5] [6] [9]
[1] [4]Exam Pearls
Otitis externa is inflammation of the external canal, and the bedside skill is localising it there with tragal tenderness and pain on pinna traction, then classifying the form. The common acute diffuse swimmer's ear is driven by Pseudomonas aeruginosa and Staphylococcus aureus after water and trauma strip the acidic cerumen layer, and it is managed analgesia-first and topically for about seven days, with an ear wick when the canal is too swollen for drops. [1] [5]
The dangerous form is necrotising (malignant) otitis externa, in which the same Pseudomonas invades the skull base in the diabetic or immunocompromised child, producing severe unremitting otalgia, granulation at the bony-cartilaginous junction and a cranial-nerve palsy (facial first). It is treated with prolonged systemic antipseudomonal therapy — classically oral ciprofloxacin 10 to 20 mg per kilogram (maximum 750 mg) every 12 hours, or intravenous ceftazidime or cefepime — guided by serial C-reactive protein and erythrocyte sedimentation rate. [7] [9]
References
- [1]Rosenfeld RM; Schwartz SR; Cannon CR; et al Clinical practice guideline: acute otitis externa. Otolaryngol Head Neck Surg, 2014.PMID 24491310
- [2]Rosenfeld RM; Schwartz SR; Cannon CR; et al Clinical practice guideline: acute otitis externa executive summary. Otolaryngol Head Neck Surg, 2014.PMID 24492208
- [3]Hajioff D; MacKeith S Otitis externa. BMJ Clin Evid, 2015.PMID 26074134
- [4]McWilliams CJ; Smith CH; Goldman RD Acute otitis externa in children. Can Fam Physician, 2012.PMID 23152458
- [5]Di Traglia R; Tudor-Green B; Muzaffar J; et al Antibiotics versus non-antibiotic treatments for acute otitis externa: A systematic review and meta-analysis. Clin Otolaryngol, 2023.PMID 37550850
- [6]Chu L; Acosta AM; Aazami H; et al Efficacy and Safety of Ciprofloxacin Plus Fluocinolone Acetonide Among Patients With Acute Otitis Externa: A Randomized Clinical Trial. JAMA Netw Open, 2022.PMID 35834251
- [7]Khokhar ZA; Mills JF; Nguyen SA; et al Pediatric Necrotizing Otitis Externa: A Scoping Review. Ann Otol Rhinol Laryngol, 2024.PMID 39289874
- [8]Drewett GP; Jacob M; Culhane B; et al Malignant Otitis Externa in Central Australia: A 15-Year Retrospective Review Between 2009 and 2024. Med J Aust, 2026.PMID 41837387
- [9]Aljariri AA; Al-Qudimat AR; Hammoud R; et al Mortality of malignant otitis externa: A prevalence meta-analysis. Qatar Med J, 2025.PMID 40765727
- [10]Expert Panel on Neurological Imaging; Agarwal M; Juliano AF; et al ACR Appropriateness Criteria: Inflammatory Ear Disease. J Am Coll Radiol, 2025.PMID 40409884
- [11]Patel S; Owen GS; Vivas EX; et al Otitis Externa and Malignant Otitis Externa-for the Hospitalist/Internist. Med Clin North Am, 2026.PMID 41206199
- [12]Osterbauer B; Durazo-Arvizu R; Hochstim C; et al Influence of obesity and socio-linguistic factors on otitis externa treatment outcomes in children. Int J Pediatr Otorhinolaryngol, 2025.PMID 40926434