Paeds · ent-hearing-and-oral-health
Otitis media with effusion and grommet decisions
Also known as Otitis media with effusion · OME · Glue ear · Serous otitis media · Secretory otitis media · Tympanostomy tube · Ventilation tube · Grommet · Middle ear effusion
Fellowship topic on otitis media with effusion (glue ear) and grommet (tympanostomy tube) decisions in children: the definition of OME as non-purulent fluid behind an intact tympanic membrane without acute infective signs, distinct from acute otitis media; the Eustachian tube dysfunction pathophysiology amplified by the short, horizontal, compliant paediatric tube; the natural-history principle that most effusions resolve within three months and that watchful waiting is the first and default management; the tympanogram (type A normal, type B flat effusion, type C negative pressure) and the typical 20 to 30 dB HL conductive hearing loss; the grommet criterion of bilateral OME persisting three months or longer with documented hearing difficulty, and the rule against inserting tubes for a single episode under three months; the at-risk child (Down syndrome, cleft palate, permanent hearing loss, developmental delay) needing earlier referral; the Paradise developmental trials showing no long-term advantage of early tubes and the Cochrane hearing evidence; autoinflation and the limited role of antibiotics, steroids and adenoidectomy; and culturally safe, region-aware care including the high-burden early-severe disease of Aboriginal and Torres Strait Islander children.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a three-year-old whose parents bring her in because she turns the television up loud, does not always answer when called, and has fallen behind at preschool with her speech. She has had a string of winter colds but is not unwell, has no ear pain and no fever. Looking in her ears you find a dull, slightly retracted, amber-coloured eardrum with a faint fluid level behind it. This is the classic face of glue ear — fluid sitting in the middle ear, conducting sound poorly, but without any of the acute infective signs that would make you think of an acute ear infection. The question is not whether she has fluid — she plainly does — but whether it will clear on its own, how much it is affecting her hearing and development, and whether and when a grommet would help. [2] [8]
Otitis media with effusion (OME) is defined as the presence of non-purulent fluid in the middle ear behind an intact tympanic membrane, without the acute infective features of acute otitis media. The older names — serous otitis media, secretory otitis media, and the everyday "glue ear" — all describe the same thing. The fluid may be thin and straw-coloured, or thick and tenacious (the true "glue"). It is one of the commonest problems of early childhood: most children have at least one episode by their third birthday, and prevalence peaks between six months and four years of age. [5] [2]
The clinician's task runs in three layers. The first is recognition — separating glue ear from acute otitis media, which changes both the urgency and the treatment. The second is documentation — confirming the effusion with tympanometry and measuring the hearing with age-appropriate audiometry, because the surgical decision depends on the hearing level, not on the look of the drum alone. The third is timing — understanding that most effusions resolve within three months, so the default first step is watchful waiting, and that grommets are reserved for the child whose effusion persists and whose hearing or development is affected. [3] [10]
Classification
Glue ear is classified along two axes that together drive the grommet decision — duration and laterality. Neither is academic: the duration tells you whether you are watching or acting, and the bilaterality tells you how much the hearing is likely to be affected and whether both ears meet the surgical criterion. [3]
By duration, OME is described as acute when it has been present for less than three months, and persistent (or chronic) when it has lasted three months or longer. The three-month line is not arbitrary — it is the point at which natural resolution becomes less likely and at which the major guidelines move from watchful waiting to formal hearing testing and consideration of grommets. A child who has had fluid for two weeks is almost certainly going to clear it; a child who still has fluid at three months deserves a hearing test and a plan. [3]
By laterality, OME is unilateral or bilateral. Bilateral disease matters more for hearing and development, because both ears are muffled at once, and the surgical criteria specifically target bilateral OME with hearing difficulty. Unilateral OME is common and often resolves, but a unilateral effusion that persists in an older child, or one with an abnormal drum, prompts a search for underlying middle-ear pathology such as cholesteatoma. [3]
It helps to remember that OME sits on a continuum rather than in a box. It often appears as residual fluid in the weeks after an episode of acute otitis media — the acute infection has settled but the middle ear has not yet dried out. It can also persist silently between recurrent acute episodes, so a child with frequent ear infections may have underlying glue ear that is never formally diagnosed. Recognising the continuum explains why a single point-in-time examination is not enough: the decision rests on duration and on the hearing level over time. [5] [8]
Epidemiology & Risk Factors
Glue ear is a disease of the Eustachian tube's immaturity, so it is overwhelmingly a disease of early childhood. The Pittsburgh cohort of more than two thousand infants found that the cumulative prevalence of middle-ear effusion during the first two years of life was extraordinarily high, with most infants experiencing effusion at some point and a substantial minority having persistent disease. [5] Prevalence falls steadily as the Eustachian tube lengthens, steepens and stiffens with growth, and by the mid-primary school years persistent OME is far less common. [5]
The risk factors cluster around anything that impairs Eustachian tube function or floods the middle ear with nasopharyngeal contents. The strongest and most consistent are daycare attendance (more viral upper-respiratory infections), older siblings, the autumn and winter season, and parental smoking and household smoke exposure. Bottle feeding and supine feeding contribute, as milk can enter the Eustachian tube. A history of recurrent acute otitis media predicts OME, because each acute episode can leave residual fluid. [5]
[3]A special and pressing category is the Aboriginal and Torres Strait Islander, Maori and Pasifika child. These children carry a markedly higher burden of otitis media than non-Indigenous children — earlier onset, more persistent disease, more suppurative and complications, and worse long-term hearing and educational outcomes. The drivers are household crowding, early and dense bacterial colonisation, reduced access to timely care, and the social determinants of health. The 2021 Australian guidelines make explicit that these children need early, culturally safe assessment and a lower threshold to treat. [4]
Pathophysiology
To understand why fluid collects in the middle ear in young children, picture the Eustachian tube as a narrow ventilation shaft connecting the middle ear to the back of the nose. In a healthy adult it opens briefly with each swallow or yawn, letting air in to replace the gas the middle-ear lining constantly absorbs, and equalising pressure across the eardrum. When that ventilation fails, the middle ear becomes a closed, gas-absorbing cavity, and trouble follows predictably. [5]
The paediatric Eustachian tube is the structural reason children are so susceptible. Compared with an adult's, a young child's tube is shorter, more horizontal, and more compliant (floppier), so it ventilates the middle ear poorly and allows nasopharyngeal contents to reflux in more easily. Add frequent viral upper-respiratory infections that swell the lining and block the tube, and the result is intermittent or persistent Eustachian tube dysfunction throughout the preschool years. As the child grows the tube lengthens, steepens and stiffens, which is why OME becomes uncommon after about age seven or eight. [5]
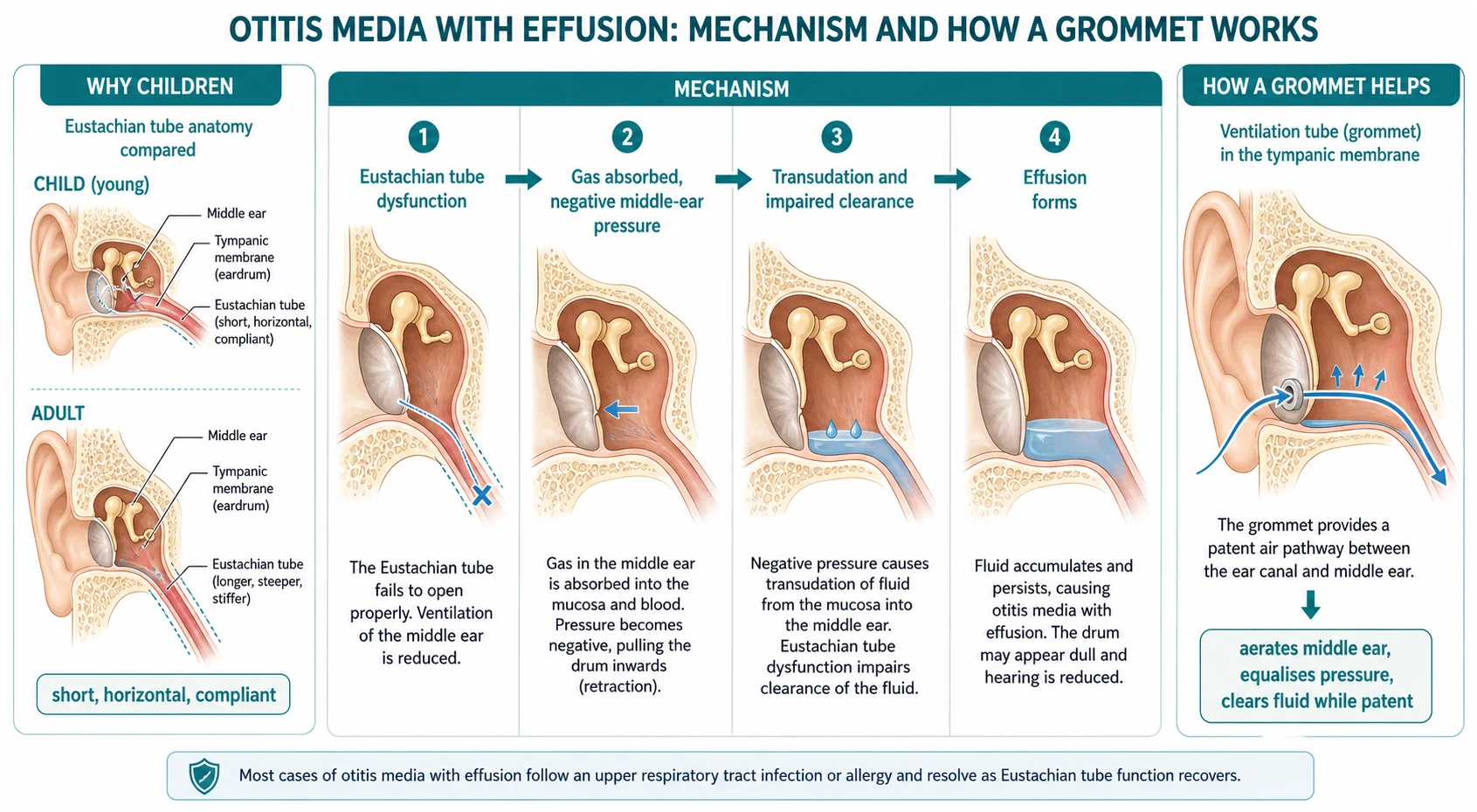
Once the tube fails, the sequence is mechanical and logical. The middle-ear lining keeps absorbing the gases trapped inside, so pressure in the cavity falls below atmospheric. The negative pressure pulls the eardrum inward into retraction. The pressure gradient then drives a transudation of fluid from the inflamed mucosa into the middle-ear space, and because the tube is also the drainage route, impaired mucociliary clearance means the fluid cannot escape. The accumulating fluid dampens the vibration of the eardrum and ossicles, which is the mechanical basis of the conductive hearing loss. [5] [8]
Understanding the mechanism tells you exactly how a grommet works. A tympanostomy tube is a tiny flanged cylinder placed through a small incision in the eardrum. It does not suck fluid out; it bypasses the dysfunctional Eustachian tube by aerating the middle ear and equalising pressure. With pressure normalised, the transudation stops and the existing fluid is reabsorbed and cleared, so the hearing returns to normal while the tube is patent. The tube typically stays in place for six to eighteen months before extruding, by which time the Eustachian tube has often matured enough to manage on its own. [2] [9]
Clinical Presentation
The trap with glue ear is that the child rarely presents with the ear itself. Instead the parents bring concerns about hearing, speech, behaviour or school, and the fluid is found on examination. A four-year-old who keeps turning the television up, who says "what?" all the time, who sits close to the teacher at circle time, or whose speech is hard to understand compared with peers, may well be hearing the world through a layer of fluid. [8] Younger children may show inattentiveness, behavioural change, or delay in reaching speech milestones, while some are detected only at routine infant or preschool hearing screening. [5]
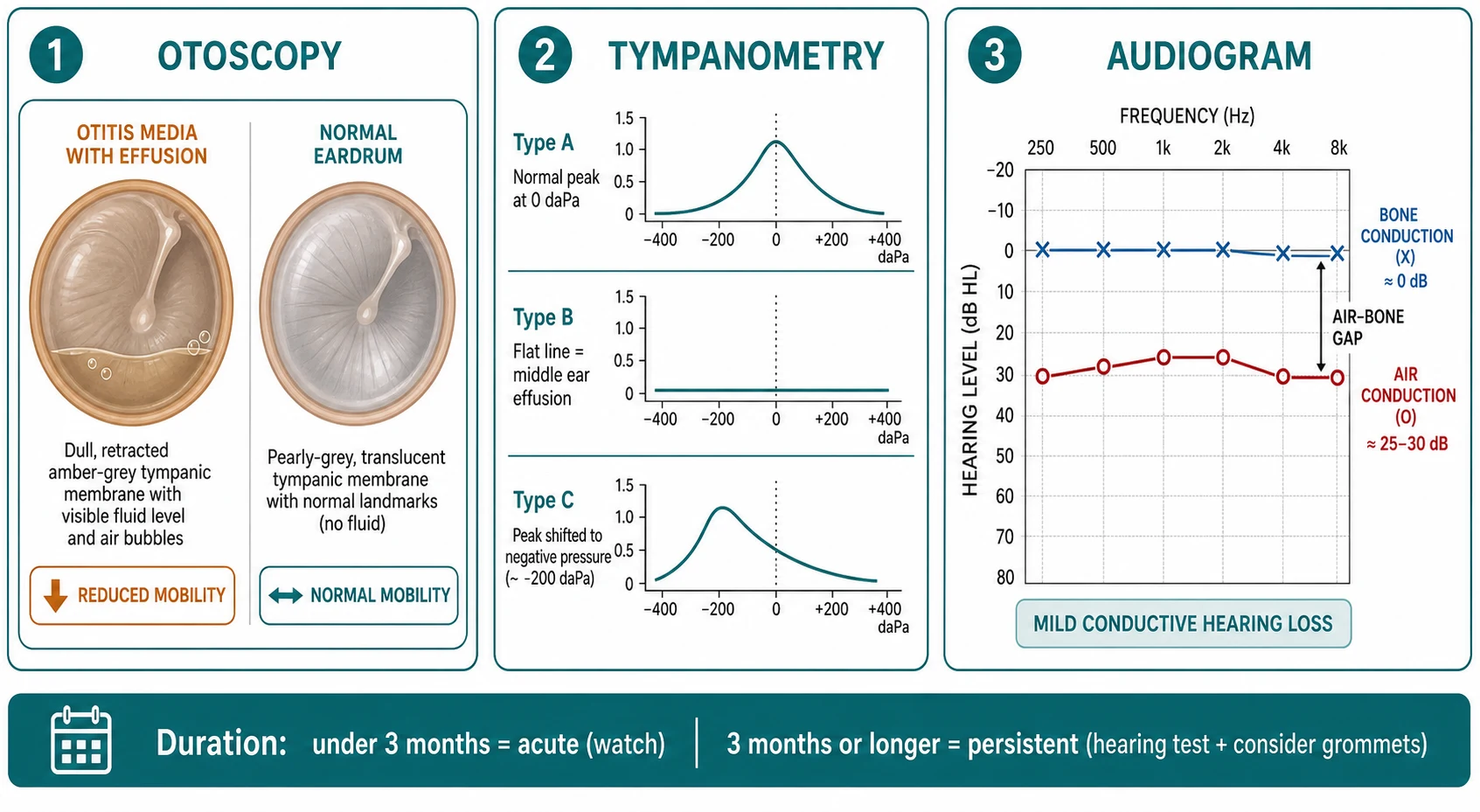
The otoscopic findings are characteristic once you look for them. The eardrum is dull, retracted or opaque, coloured amber, grey or occasionally blue, rather than the normal pearly, translucent, light-reflecting membrane. You may see a fluid level (a meniscus) or air bubbles behind the drum, and the light reflex is altered or absent. On pneumatic otoscopy the drum has reduced mobility — it does not move briskly with gentle puffs of air, because the fluid behind it dampens the excursion. None of these signs is painful, and the child is afebrile and well. [3] [2]
Several presentations deserve particular attention. OME often follows an episode of acute otitis media as residual fluid that has not yet cleared — a child rechecked two to four weeks after an acute ear infection may still have a dull drum, and this is expected rather than alarming. Unilateral OME that fails to resolve, especially in an older child, should prompt thought about underlying middle-ear pathology such as a cholesteatoma, and warrants specialist review rather than simple reassurance. A few children present with balance difficulty or clumsiness rather than obvious deafness, because middle-ear effusion affects vestibular function. [3] [9]
The single most important message is that OME is frequently asymptomatic and found incidentally. This is exactly why the duration and the measured hearing level, rather than the mere presence of fluid, drive every management decision. A child with fluid for two weeks who hears normally needs reassurance; a child with fluid for four months who cannot hear the teacher needs action. [3] [10]
Differential Diagnosis
The first differential is the one that changes everything: is this glue ear, or is it an acute ear infection? Acute otitis media presents with acute ear pain, fever and a systemically unwell child, and the drum is bulging, red and opaque with loss of landmarks — the opposite of the dull, retracted, painless drum of OME. The distinction matters because acute otitis media may need analgesia and antibiotics, while OME needs patience and a hearing test. Residual effusion after a treated acute infection is the bridge between the two. [2] [3]
When the presenting complaint is hearing difficulty rather than a dull drum, you must keep the broader hearing-loss differential in mind and separate a conductive from a sensorineural cause. Permanent sensorineural or mixed hearing loss is the most important not-to-miss alternative, and only formal audiometry will distinguish it from the conductive loss of OME. Cerumen impaction and a foreign body can mimic hearing difficulty and a dull view, and an ossicular abnormality (such as congenital stapes fixation) produces a conductive loss without effusion. [3]
For the dull drum itself, the rare but serious mimic is cholesteatoma — a keratinising squamous epithelial sac in the middle ear or attic that erodes bone. A pearly white mass in the attic or pars tensa, a persistent foul discharge, or unilateral OME in an older child that fails to resolve should raise concern and prompt ENT review. Retraction without effusion, and the dull drum of eustachian tube dysfunction without fluid, are also in the otoscopic differential. [3] [9]
Clinical & Bedside Assessment
The history sets up the whole decision, so take it deliberately. Establish the onset and duration of any hearing or speech concern, recent upper-respiratory infections and acute otitis media episodes, and the child's speech, language and school trajectory. Ask directly about the behaviours families notice: turning up the television, not responding when called, sitting close to the front, asking for repetition, and behavioural or attentional change. Cover the risk factors — daycare, siblings, season, smoke exposure, feeding history — and ask about any syndromal or developmental concern. [5] [8]
Examination is otoscopy and pneumatic otoscopy. Look for the dull, retracted or opaque drum, the amber or grey colour, the fluid level or air bubbles, and the altered or absent light reflex. Test mobility with pneumatic otoscopy — reduced mobility suggests fluid. Then look beyond the ear: examine the palate for a cleft (overt or submucous, including a bifid uvula), the face for the features of Down syndrome or a craniofacial syndrome, and the nose and adenoids. Assess the child's developmental stage and hear the speech for yourself, because a speech delay may be both the presenting feature and the reason to lower your threshold. [3]
Bedside hearing tests (such as whispered voice or tuning-fork tests) are useful screening but are no substitute for formal age-appropriate audiometry in a child being considered for grommets. The same applies to a parent's report of hearing difficulty: it is valuable and should be taken seriously, but it must be confirmed with a measured hearing level before a surgical decision. This is why the guidelines are explicit that a hearing evaluation is required if OME persists for three months or longer, or before surgery. [3]
Investigations
Two investigations confirm OME and drive the decision, and both should be in place before surgery is considered: tympanometry and age-appropriate audiometry. Neither is invasive, and together they turn a clinical impression into a documented diagnosis. [3] [2]
Tympanometry measures the compliance of the eardrum across a range of pressures, producing a trace that classifies the middle ear. A type A trace has a normal peak at around zero decapascals and means a normally ventilated middle ear. A type B trace is flat — the drum cannot move no matter the pressure — and indicates a middle-ear effusion (or, less commonly, a perforation or a blocked probe). A type C trace has its peak shifted into the negative-pressure range and indicates Eustachian tube dysfunction without a frank effusion. For OME, the type B trace is the confirmation you are looking for, and it correlates well with effusion. [2] [3]
Audiometry documents the degree and type of hearing loss and is matched to the child's developmental age. In a cooperative child, pure-tone audiometry gives the air and bone conduction thresholds across frequencies; the typical OME pattern is a mild to moderate conductive hearing loss of about 20 to 30 dB HL with an air-bone gap, though some children have a larger loss and others hear better than the drum suggests. In infants and young or developmentally delayed children, behavioural observational or visual reinforcement audiometry, and electrophysiological tests such as auditory brainstem response, provide the thresholds when pure-tone testing is not possible. [2] [8]
The duration rule is itself part of the investigation plan: reassess OME at three months to separate the transient effusion that will resolve from the persistent effusion that warrants a hearing test and an intervention decision. Re-evaluate children with chronic OME who do not receive tubes at three- to six-monthly intervals until the effusion resolves, significant hearing loss is detected, or structural abnormality of the drum or middle ear is suspected. Routine imaging is not required for typical OME; reserve it for the atypical case — suspected cholesteatoma, unilateral persistent OME in an older child, or a syndromal workup. [3]
Management — Resuscitation
Otitis media with effusion is not an emergency in the great majority of children, and the most important "immediate" action is often the hardest one for an anxious family to accept: do nothing surgical, and wait. The first step is watchful waiting for three months, combined with clear hearing and speech advice, reassurance about the natural history, and a safety-net for the features that should bring the child back sooner. [2] [3]
There are, however, situations in which earlier action is right. The child with a permanent hearing loss or a developmental concern, the at-risk child (Down syndrome, cleft palate, developmental delay), the child whose OME is causing clear educational or developmental harm, and the Aboriginal or Torres Strait Islander child with persistent disease should not simply be sent away for three months. In these children the developmental cost of waiting is higher, so the threshold to refer early to audiology and ENT is lower. [3] [4]
Recognise also the child who needs separate acute assessment: a child with established OME who develops new ear pain, fever or a bulging red drum has a superimposed acute otitis media that needs its own assessment and, when criteria are met, oral antibiotics (such as amoxicillin at 40 milligrams per kilogram per day in divided doses for five days in the typical child). Treating the acute episode does not, however, change the underlying OME plan. [7] [3]
The key is to separate the watchful-waiting stance from the surgical pathway. Most children will resolve without ever needing an operation. The operation is offered only to the child who meets the duration and hearing criteria — and that decision is made after the three-month reassessment, not at the first visit. [3] [10]
Management — Definitive & Stepwise
The management of OME is a stepwise pathway that moves from conservative watching, through formal audiological documentation, to surgery for the minority who meet the criteria. Each step has a clear trigger, and the discipline lies in not skipping ahead. [3] [2]
Step 1 — Watchful waiting for three months: reassure, give hearing and speech advice, safety-net, and do not operate on a single episode under three months.
Step 2 — Reassess at three months with tympanometry and age-appropriate audiometry: confirm whether the effusion has persisted and document the hearing level.
Step 3 — Apply the grommet criterion: offer bilateral tympanostomy tubes to children with bilateral OME for three months or longer and documented hearing difficulty.
Step 4 — Refer the at-risk child earlier: Down syndrome, cleft palate, permanent hearing loss, developmental delay, or Indigenous heritage warrant a lower threshold and early audiology and ENT referral.
Step 5 — Re-evaluate non-operated chronic OME at three- to six-monthly intervals until resolution, significant hearing loss, or structural abnormality appears.
The grommet criterion is the heart of the topic and the most examined fact. The American Academy of Otolaryngology-Head and Neck Surgery 2022 guideline is explicit: clinicians should offer bilateral tympanostomy tube insertion to children with bilateral OME persisting three months or longer and documented hearing difficulties, and should not insert tubes in a child with a single episode of OME of less than three months' duration. Clinicians should also obtain a hearing evaluation if OME persists for three months or longer, or before surgery when a child becomes a candidate for tubes. [3]
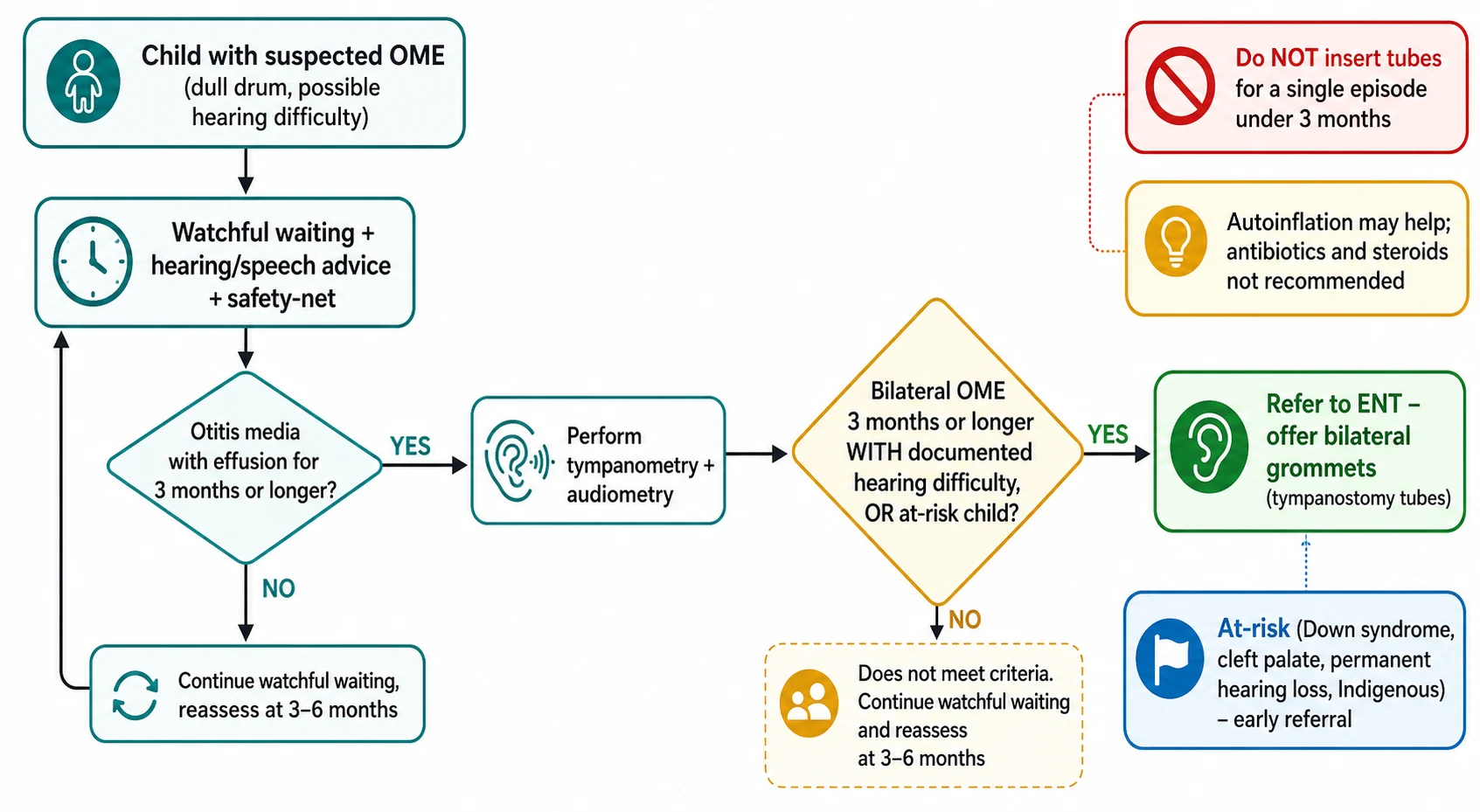
Several adjuncts and non-treatments deserve precise positioning. Autoinflation — using a nasal balloon device (such as Otovent) that the child inflates through the nose to force air up the Eustachian tube — has modest evidence of benefit in children old enough to perform it reliably, and is a low-harm option worth offering during the watchful-waiting period. Antibiotics have no lasting benefit in OME: the Cochrane review found they may produce short-term resolution but the effect is small, does not persist, and the harms of antibiotic use outweigh any benefit, so they are not recommended for routine OME. Oral or topical steroids similarly lack a durable effect and are not recommended. [7] [2]
Adenoidectomy has a defined but limited place. The individual-patient-data meta-analysis found that adding adenoidectomy to grommets (or using it in selected older children) produced a modest additional benefit on effusion resolution, with the clearest effect in children around four years and older. It is not routinely added for a first set of tubes in a young child without nasal symptoms, but it enters the discussion for older children with persistent or recurrent disease. Hearing aids are a reasonable alternative when surgery is declined or contraindicated, restoring audibility while the effusion persists. [6] [2]
The choice of grommet (short-term versus long-term or T-tube) balances the expected duration of Eustachian tube immaturity against the greater risk of persistent perforation with longer tubes. Most first insertions use a short-term tube that extrudes in six to eighteen months. After grommets, review the ears within three months of insertion, educate the family on water precautions and the management of tube otorrhoea (topical antibiotic drops, not oral antibiotics, for uncomplicated tube otorrhoea), and arrange periodic review until the tubes extrude and hearing is confirmed normal. [3] [9]
Specific Subtypes & Scenarios
A well child with a single episode of OME under three months is the commonest scenario and the one most often mismanaged by over-treatment. The correct plan is reassurance, watchful waiting, hearing and speech advice, and a safety-net, with reassessment at three months. No antibiotics, no steroids, no tubes — and a clear explanation that most effusions clear on their own as the child recovers from the cold that caused them. [2] [3]
A child with bilateral OME persisting three months or longer and documented hearing difficulty is the child who meets the grommet criterion. Document the effusion with a type B tympanogram, document the hearing with audiometry, and refer to ENT for consideration of bilateral tympanostomy tubes. Counsel the family honestly: the tubes will restore hearing to normal in the short term, but in an otherwise normal child the long-term developmental outcome is the same with or without early surgery, so the operation is justified by the current impact on hearing and development, not by the mere presence of fluid. [1] [3]
The at-risk child is the scenario where the standard three-month threshold is too blunt. In a child with Down syndrome, cleft palate, a permanent sensorineural hearing loss, developmental delay, autistic spectrum disorder, or blindness, even a mild conductive loss adds to an already vulnerable developmental trajectory, so the threshold to refer early and to intervene is lower. Many centres adopt a proactive grommet and audiology pathway for children with cleft palate because of the near-universal OME and its additive effect on speech. [3]
A child with recurrent acute otitis media superimposed on OME needs both problems addressed. Manage each acute episode on its merits, and consider the role of grommets in reducing the frequency of acute episodes — but only where middle-ear effusion is also present at the time of evaluation, because the guideline is explicit that tubes are not indicated for recurrent acute otitis media without effusion in either ear. [3]
An Aboriginal or Torres Strait Islander child with persistent ear disease is the scenario where the stakes are highest. These children experience early, persistent and often suppurative disease with serious long-term hearing, language and educational consequences. Provide culturally safe care, engage Aboriginal health workers and trained interpreters, address household crowding and access, arrange timely audiology and ENT services including outreach and telehealth for rural and remote children, and adopt a lower threshold to assess and to treat. The 2021 Australian guidelines are the operative reference. [4]
A child with unilateral persistent OME in an older child, or one that fails to resolve, is the scenario that should make you think beyond glue ear. Reassess, and consider imaging or specialist review to exclude underlying middle-ear pathology such as a cholesteatoma, particularly if there is attic or pars-tensa abnormality or a history of discharge. Unilateral OME in an adult prompts imaging for nasopharyngeal pathology; in a child it is less often sinister but still warrants a considered review rather than dismissal. [3] [9]
Complications & Pitfalls
The principal consequence of persistent untreated OME is the conductive hearing loss itself and its developmental ripple effects. A child who hears through fluid for months may lag in speech and language, show behavioural change or inattention, and struggle at school — effects that are usually reversible as the hearing improves but that matter most in the at-risk child and the child with prolonged bilateral disease. Less commonly, OME causes balance clumsiness and a measurable impact on quality of life. [8] [10]
The potential harms of grommets are real but usually minor. Tympanosclerosis (white scarring of the drum) is common after tubes and usually of no functional consequence. Persistent tympanic membrane perforation — a drum that does not heal after the tube extrudes — is uncommon with short-term tubes but rises with long-term and T-tubes, and may need a later myringoplasty. Tube otorrhoea (discharge through a patent tube) is common, usually settles with topical antibiotic drops, and rarely needs oral antibiotics or tube removal. [9] [3]
In Australia and Aotearoa New Zealand the Royal Children's Hospital Melbourne guidance and the Therapeutic Guidelines frame the pathway, with the AAO-HNS 2022 criteria mirrored in practice: bilateral OME three months or longer with hearing difficulty for grommets, and the explicit recognition that Aboriginal and Torres Strait Islander children need early, culturally safe care and a lower threshold to treat.
The classic pitfalls to avoid are three. The first is operating on otoscopy alone without tympanometry and audiometry, or before the three-month threshold. The second is assuming OME is harmless: in the at-risk child and the child with clear developmental or educational impact, persistent conductive hearing loss has real consequences and warrants earlier action. The third is over-treating: because the long-term developmental outcome is the same with or without early tubes in otherwise normal children, the operation must be justified by current hearing and developmental impact, not by the mere presence of fluid. [1] [3]
Prognosis & Disposition
The natural history of OME is the foundation of its management and the reason watchful waiting comes first. Most effusions resolve within three months, and the resolution rate continues to rise with time as the Eustachian tube matures and upper-respiratory infections become less frequent. The Pittsburgh cohort showed how common and how self-limiting early-childhood effusion is, which is why a single point-in-time finding of fluid is not, by itself, an indication to operate. [5] [2]
For the child who does have grommets, the tubes restore hearing to normal while they are patent, typically for six to eighteen months. The hearing advantage over no-treatment is clearest in the first months and narrows by around twelve months as the non-operated ear also resolves on its own. Crucially, the Paradise randomised trials following children to age nine to eleven years found no difference in developmental, language, academic or behavioural outcomes between early and delayed tube insertion, which is why the operation is justified by current impact rather than by fear of future developmental harm. [1] [11]
Disposition runs along the stepwise pathway. Primary care manages watchful waiting and the three-month reassessment. ENT referral is for the child who meets the grommet criteria or who is at-risk, and audiology underpins every decision with the measured hearing level. After grommets, review within three months of insertion, educate on water precautions and tube otorrhoea, and arrange periodic review until the tubes extrude and hearing is confirmed normal. Give a clear safety-net for hearing or developmental change and for any acute ear infection. [3] [10]
Special Populations
The at-risk child is the population in whom the standard stance is adjusted most. For children with Down syndrome, cleft palate, a permanent sensorineural hearing loss, developmental delay, autistic spectrum disorder, or blindness, even a mild additive conductive hearing loss compounds an already vulnerable developmental trajectory, so the threshold for early audiology and ENT referral and for intervention is lower, and many of these children are on proactive hearing-surveillance pathways. [3]
Aboriginal and Torres Strait Islander, Maori and Pasifika children carry the highest burden of otitis media in Australia and the Pacific region, with early onset, persistent and often suppurative disease and serious long-term hearing, language and educational consequences. Provide culturally safe care, engage Aboriginal health workers and trained interpreters, address the social determinants including household crowding, and arrange equitable access to timely assessment and treatment. The 2021 Australian otitis media guidelines for Aboriginal and Torres Strait Islander children are the operative reference, and they call for early detection and a lower threshold to treat. [4]
For children in rural and remote areas, geography must not delay the three-month reassessment or the intervention. Arrange timely audiology and ENT access through outreach clinics, visiting specialist services and telehealth, so that the stepwise pathway runs on the same timeline as it would in the city. For migrant, refugee and asylum-seeking families, ensure equitable access, use trained interpreters, and address the social determinants — including missed screening and late presentation — that worsen otitis media outcomes. [4] [3]
Evidence, Guidelines & Regional Differences
The modern evidence base rests on three pillars: the Cochrane review of ventilation tubes, the Paradise randomised trials of developmental outcomes, and the major clinical practice guidelines. The 2023 Cochrane review (MacKeith and colleagues) pooled nineteen randomised trials of ventilation tubes for OME of three months or longer and found that, compared with no treatment or watchful waiting, tubes produced a hearing benefit that was clearest in the short term and narrowed by around twelve months; the overall certainty of the evidence was very low, reflecting wide confidence intervals and few participants. [2]
Ventilation tubes (grommets) for OME in children — Cochrane 2023
Population: Children aged six months to twelve years with OME for three months or longer, across nineteen randomised trials comparing ventilation tubes with no treatment, watchful waiting, myringotomy, hearing aids and other non-surgical treatments.
Key finding
Ventilation tubes versus no treatment gave an odds ratio of 1.13 (95% confidence interval 0.46 to 2.74) for return to normal hearing at twelve months — a narrowing of the early hearing advantage — and the overall certainty of the evidence was very low.
Practice change
Grommets deliver a real but time-limited hearing benefit; in otherwise normal children the developmental outcome is not improved in the long term, so the operation is justified by current hearing and developmental impact, not by the mere presence of fluid.
The Paradise randomised trials are the definitive answer to whether early surgery improves development. Children with persistent OME were randomised to early or delayed tympanostomy tube insertion and followed to age three, four, six and finally nine to eleven years. At every time point — including the long-term nine-to-eleven-year follow-up — there was no difference between the groups in developmental, language, academic or behavioural outcomes. This single body of evidence is why every modern guideline frames grommets as a treatment for current hearing and developmental impact rather than as a preventive against future cognitive harm. [1] [11]
Tympanostomy tubes and developmental outcomes at 9 to 11 years — Paradise
Population: Children with persistent early-childhood OME randomised to early or delayed tympanostomy tube insertion, followed to age nine to eleven years.
Key finding
There was no significant difference between the early- and delayed-insertion groups in any measure of hearing, speech, language, cognition, academic achievement or behaviour at nine to eleven years of age.
Practice change
In otherwise normal children, early insertion of grommets does not improve long-term developmental outcomes; the decision to operate should rest on the current hearing and developmental impact, not on fear of future harm.
The antibiotic and adenoidectomy evidence defines what does not work and what works a little. The Cochrane review of antibiotics for OME found no durable benefit and concluded they should not be used routinely, given the harms of resistance and side effects. The individual-patient-data meta-analysis of adenoidectomy found a modest additional benefit on effusion resolution, clearest in children around four years and older, which positions adenoidectomy as an adjunct in selected older children rather than a routine addition. The earlier Cochrane review of grommets for hearing loss established the short-term hearing benefit that the 2023 update refined. [7] [6] [10]
The regional guidelines agree in principle and vary in detail. In the United States, the American Academy of Otolaryngology-Head and Neck Surgery 2022 tympanostomy tube guideline sets the duration, laterality and hearing-difficulty criteria described throughout this page. In the United Kingdom, NICE Clinical Guideline CG60 sets the surgical criteria for OME, with a hearing loss of around 25 to 30 dB HL or worse affecting development or schooling after watchful waiting. In Australia and Aotearoa New Zealand, the Royal Children's Hospital Melbourne guidance and the Therapeutic Guidelines mirror the pathway, with the 2021 otitis media guidelines for Aboriginal and Torres Strait Islander children providing the culturally specific, high-burden context. [3] [4]
The controversies are now largely settled. The question of whether early surgery improves development in normal children — the great hope of an earlier era — has been answered "no" by the Paradise trials. The role of adenoidectomy is defined as a modest adjunct in older children. The place of autoinflation is as a low-harm option with modest benefit. The management of the at-risk and Indigenous child is the active frontier, where the threshold to refer and intervene is deliberately lower than for the general population, and where equity of access is part of the treatment. [1] [4]
Exam Pearls
- OME is glue ear: non-purulent fluid behind an intact tympanic membrane without acute infective signs; it is not an acute ear infection. [2]
- Most OME resolves within three months; the first and default management is watchful waiting, not surgery. [2] [5]
- The grommet criterion is bilateral OME for three months or longer with documented hearing difficulty; do not insert tubes for a single episode under three months. [3]
- Always document the effusion with tympanometry and the hearing with audiometry before any surgical decision. [3]
- Tympanogram types: A is normal, B is flat and indicates effusion, C shows negative middle-ear pressure. [2]
- The typical OME hearing loss is a conductive loss of about 20 to 30 dB HL. [8] [2]
- Grommets give a short-term hearing benefit that narrows by twelve months and no long-term developmental advantage in otherwise normal children (Paradise, age nine to eleven). [1] [11]
- Antibiotics and steroids have no lasting role in OME; autoinflation has modest benefit; adenoidectomy adds a small benefit in older children. [7] [6]
- The at-risk child (Down syndrome, cleft palate, permanent hearing loss, developmental delay, blind) needs a lower threshold for early referral and intervention. [3]
- Aboriginal and Torres Strait Islander children carry a high burden of early, persistent, severe otitis media; provide culturally safe, early, accessible care. [4]
- A grommet works by aerating the middle ear and equalising pressure, bypassing the dysfunctional Eustachian tube while it is patent. [2]
- For uncomplicated tube otorrhoea, use topical antibiotic ear drops, not oral antibiotics. [3]
References
- [1]Paradise JL; Feldman HM; Campbell TF; et al Tympanostomy tubes and developmental outcomes at 9 to 11 years of age. N Engl J Med, 2007.PMID 17229952
- [2]MacKeith S; Mulvaney CA; Galbraith K; et al Ventilation tubes (grommets) for otitis media with effusion (OME) in children. Cochrane Database Syst Rev, 2023.PMID 37965944
- [3]Rosenfeld RM; Tunkel DE; Schwartz SR; et al Clinical Practice Guideline: Tympanostomy Tubes in Children (Update). Otolaryngol Head Neck Surg, 2022.PMID 35138954
- [4]Leach AJ; Morris PS; Coates HL; et al Otitis media guidelines for Australian Aboriginal and Torres Strait Islander children: summary of recommendations. Med J Aust, 2021.PMID 33641192
- [5]Paradise JL; Rockette HE; Colborn DK; et al Otitis media in 2253 Pittsburgh-area infants: prevalence and risk factors during the first two years of life. Pediatrics, 1997.PMID 9041282
- [6]Boonacker CW; Rovers MM; Browning GG; et al Adenoidectomy with or without grommets for children with otitis media: an individual patient data meta-analysis. Health Technol Assess, 2014.PMID 24438691
- [7]Venekamp RP; Burton MJ; van Dongen TM; et al Antibiotics for otitis media with effusion in children. Cochrane Database Syst Rev, 2016.PMID 27290722
- [8]Roberts JE; Burchinal MR; Zeisel SA; et al Otitis media, the caregiving environment, and language and cognitive outcomes at 2 years. Pediatrics, 1998.PMID 9685437
- [9]Johnston LC; Feldman HM; Paradise JL; et al Tympanic membrane abnormalities and hearing levels at the ages of 5 and 6 years in relation to persistent otitis media and tympanostomy tube insertion in the first 3 years of life: a prospective study incorporating a randomized clinical trial. Pediatrics, 2004.PMID 15231974
- [10]Browning GG; Rovers MM; Williamson I; et al Grommets (ventilation tubes) for hearing loss associated with otitis media with effusion in children. Cochrane Database Syst Rev, 2010.PMID 20927726
- [11]Paradise JL; Campbell TF; Dollaghan CA; et al Developmental outcomes after early or delayed insertion of tympanostomy tubes. N Engl J Med, 2005.PMID 16093466