Paeds · ent-hearing-and-oral-health
Salivary gland disorders
Also known as Mumps · Viral parotitis · Juvenile recurrent parotitis · Acute suppurative sialadenitis · Bacterial parotitis · Ranula · Plunging ranula · Sialolithiasis
Fellowship topic on salivary gland disorders in children. Covers mumps and its complications, juvenile recurrent parotitis and sialendoscopy, acute suppurative parotitis with anti-staphylococcal therapy, the simple and plunging ranula, sialolithiasis and neonatal parotitis. Builds the skill of distinguishing the common viral parotitis from the suppurative gland needing antibiotics and the recurrent or cystic lesion needing a different pathway, with ANZ, UK, US and Canadian guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A four-year-old is sent home from childcare with bilateral cheek swelling and a low fever. The mother asks whether it is mumps and what to watch for. The fellowship skill is to read the swelling as viral or bacterial, recurrent or new, cystic or inflammatory — and to act on the few that carry danger. [1]
Salivary gland disorders in children cover any swelling, inflammation or cystic change of the parotid, submandibular, sublingual or minor salivary glands. The task is to separate the common self-limiting viral parotitis from the suppurative gland needing antibiotics, the recurrent pattern needing a work-up, and the cystic or structural lesion needing surgery. Most paediatric salivary swelling is viral and benign. A small minority — the suppurative parotitis of the neonate, the mumps meningitis, the recurrent parotitis that scars the gland — carry real harm. The examining skill is to read the gland, the duct, the host and the time course, because that quartet names the cause. [1] [2]
Classification
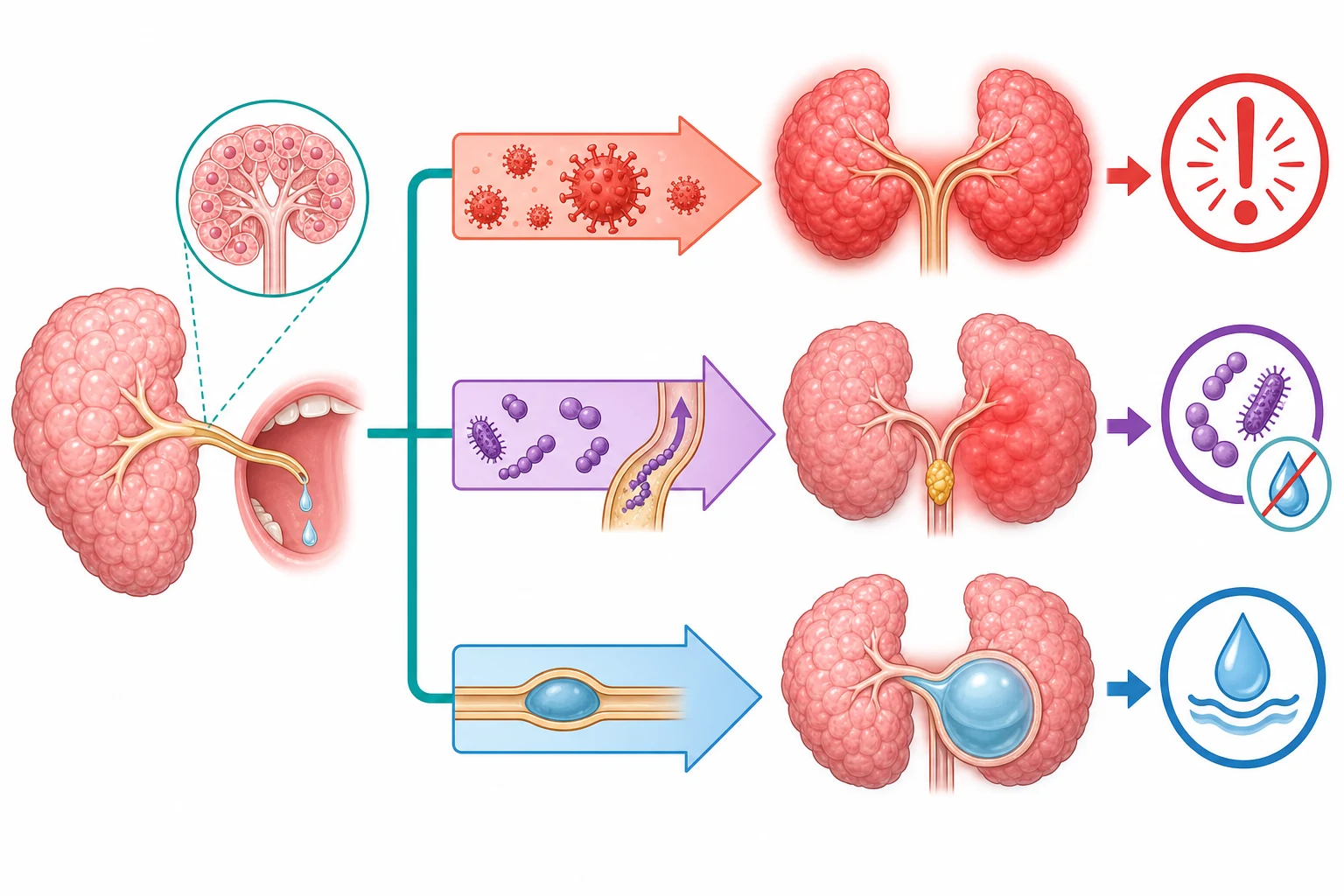
Picture salivary gland disorders by what is causing the swelling and which gland is involved, because the cause and the gland together drive both the treatment and the decision to investigate. [2]
The clinical patterns of paediatric salivary gland disease
Epidemiology & Risk Factors
Mumps remains the prototypical viral parotitis of childhood, though widespread two-dose MMR vaccination has reduced incidence by more than 95 per cent in countries with high coverage. Resurgence occurs in under-immunised adolescents and young adults, and in communities with waning immunity or vaccine refusal. The incubation period is 16 to 18 days, with a range of 12 to 25 days. The child is infectious from two days before to five days after the onset of parotid swelling. [1]
Juvenile recurrent parotitis is the second most common inflammatory salivary disease of childhood after mumps, with onset typically between three and six years and a male predominance of roughly two to one. Episodes recur over years and most children resolve spontaneously by puberty. Acute suppurative parotitis is uncommon overall but over-represented in neonates, premature infants, dehydrated children and the immunocompromised. Sialolithiasis is rare in children compared with adults, accounting for under five per cent of all cases. [3] [6]
Neonatal suppurative parotitis is rare, with fewer than a few hundred cases reported in the literature, but prematurity, dehydration, low birth weight and immunocompromise are consistent risk factors. HIV-associated benign lymphoepithelial cysts produce chronic bilateral parotid enlargement in children living with HIV, and respond to antiretroviral therapy rather than surgery. [9] [10]
Pathophysiology
Why does the parotid swell, and why does one child recover while another develops meningitis or a lifetime of recurrent flares? The answers lie in the structure of the salivary gland, in the biology of mumps virus, and in the duct that drains the gland. [1]
Mumps virus is a paramyxovirus that spreads by respiratory droplets and replicates in the upper respiratory tract before seeding the parotid gland through the bloodstream. The virus targets glandular and neural tissue, which is why the parotid is the hallmark organ but the testes, pancreas, meninges and cochlea are vulnerable. The bilateral swelling reflects viral replication in the acinar cells, oedema and periductal inflammation that compresses the duct and traps saliva. [1]
Acute suppurative parotitis follows bacterial ascent up the Stensen duct when the protective flow of saliva is reduced by dehydration, and the organism — usually Staphylococcus aureus — multiplies in the stagnant duct and acini. The gland becomes acutely inflamed and may abscess. Juvenile recurrent parotitis is thought to arise from a combination of sialectasis, parotid duct stricture or reflux, and immune dysregulation that produces recurrent, non-suppurative inflammation — structurally, the gland shows ectatic peripheral ducts on sialography or ultrasound. A ranula forms when the sublingual gland or its duct is injured or obstructed and mucus extravasates into the surrounding tissue, collecting as a pseudocyst in the floor of the mouth or, when it tracks through the mylohyoid muscle, in the neck. [2] [8]
Clinical Presentation
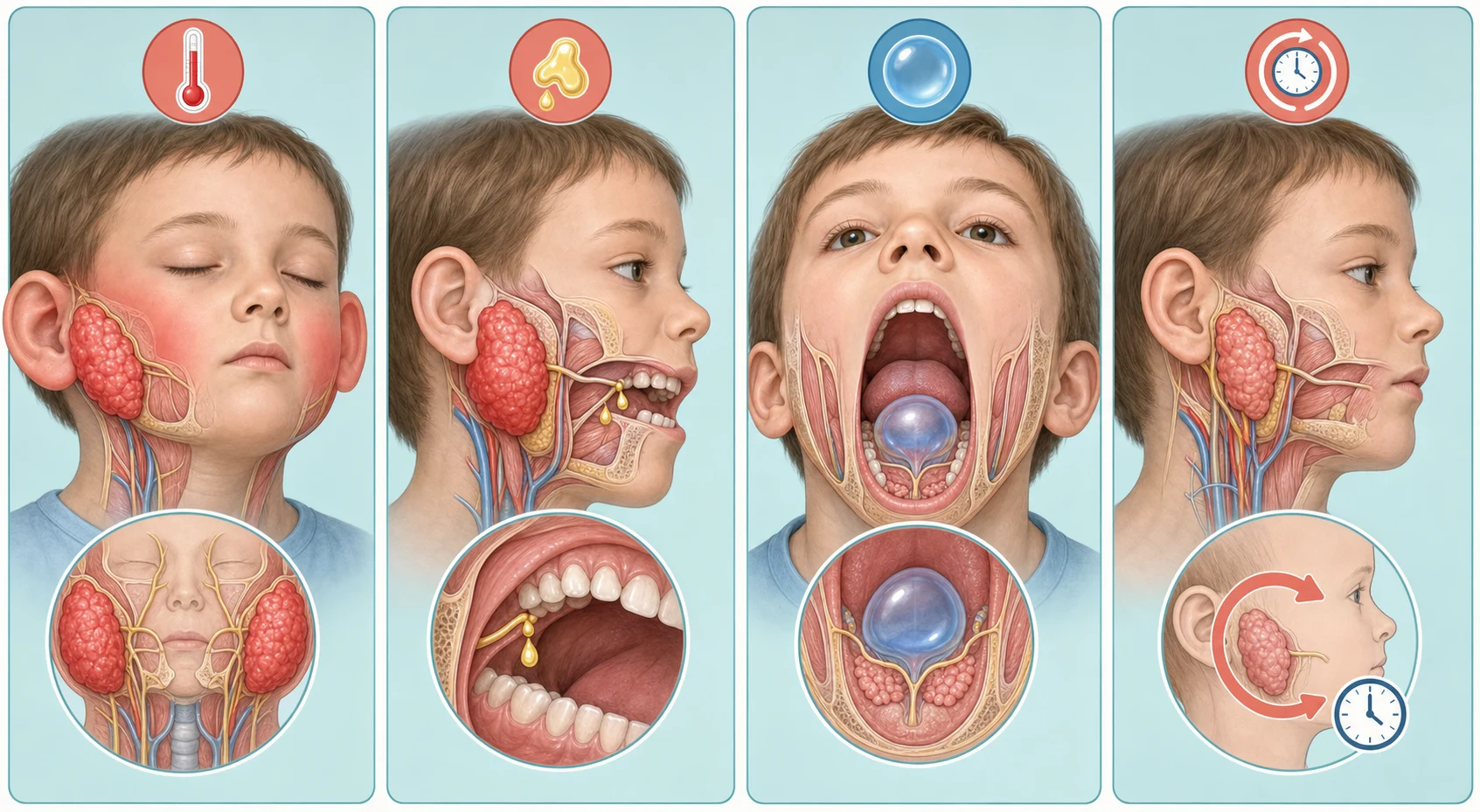
Read the swelling the way the speed, the side and the duct tell you to — a bilateral acute febrile parotitis in an under-immunised child is mumps, a unilateral exquisitely tender gland with pus is suppurative, and a painless bluish floor-of-mouth swelling is a ranula. [1] [2]
Mumps presents with a one- to two-day prodrome of fever, headache, malaise and myalgia, followed by progressive tender swelling of one or both parotid glands. The swelling lifts the ear lobe outward and forward, filling the angle of the jaw. Bilateral involvement occurs in roughly 70 per cent of cases. The child may complain of pain on chewing or swallowing, and the skin over the parotid is warm but not red. The Stensen duct orifice may be inflamed but there is no frank pus — that distinction separates mumps from suppurative parotitis. [1]
Acute suppurative parotitis is unilateral, with an exquisitely tender, firm parotid mass, high fever and systemic toxicity. Gentle pressure on the gland expresses frank pus from the Stensen duct orifice. The overlying skin may be erythematous and indurated, and the child is irritable and unwell. Juvenile recurrent parotitis presents with recurrent episodes of unilateral or bilateral parotid swelling over months to years, each lasting days to weeks, with a relatively well child between flares. A ranula presents as a soft, fluctuant, bluish, translucent swelling in the floor of the mouth lateral to the midline; a plunging ranula presents as a cervical mass in the submandibular or parapharyngeal space. [3] [8]
Differential Diagnosis
Build the differential around the speed of onset, whether the swelling is unilateral or bilateral, whether the gland is tender, and whether the Stensen duct expresses pus — because that quartet narrows a long list to a workable few. [2]
Separate the bilateral acute febrile parotitis of mumps from the unilateral exquisitely tender parotitis with purulent discharge of suppurative disease, and from the recurrent non-suppurative pattern of juvenile recurrent parotitis. Then separate the inflammatory from the structural: a painless, slowly growing, firm mass is a tumour until proven otherwise, a soft bluish floor-of-mouth swelling is a ranula, and meal-time swelling points to a stone. Cervical lymphadenopathy can be confused with parotid swelling — the parotid swelling lifts the ear lobe, whereas cervical nodes sit below and behind the angle of the jaw and do not move with the gland. [2] [3]
The causes of paediatric parotid swelling — MUMPS-S
Clinical & Bedside Assessment
Start with the history, because the immunisation status, the speed of onset and the recurrence pattern usually name the pattern before the gland is examined. Ask about MMR vaccination (mumps), the speed of onset and whether the swelling is one-sided or both (mumps is usually bilateral; suppurative is unilateral), whether episodes recur (juvenile recurrent parotitis), whether the swelling worsens with meals (sialolithiasis), and the systemic clues of testicular pain, headache, neck stiffness, abdominal pain and hearing change that signal complications of mumps. [1] [3]
Examine the face and neck with the child sitting upright and a good light: inspect the parotid region for symmetry and overlying skin change, palpate the gland bimanually (one finger intra-orally, one hand extra-orally) for tenderness, consistency and size, and milk the Stensen duct by gentle pressure on the gland to check for purulent discharge. Look for the ear-lobe sign — mumps lifts the ear lobe outward and forward — and distinguish parotid swelling from cervical lymphadenopathy, which sits below and behind the jaw angle. Assess hydration (moist mucous membranes, capillary refill, urine output), look for testicular swelling or tenderness in post-pubertal boys, and perform a focused neurological examination for meningism, ataxia or cranial nerve deficit. [1] [9]
Investigations
Most salivary gland disorders in children are diagnosed clinically and need no investigation; the role of testing is to confirm mumps in the public-health context, to identify the organism in suppurative disease, and to image the recurrent, structural or atypical lesion. [2]
For mumps, the clinical picture is sufficient in a child with the classic bilateral parotitis and a compatible epidemiology, but buccal swab for mumps RNA by RT-PCR or a paired serum IgM and IgG supports public-health reporting, especially in outbreak settings and in previously vaccinated children whose serology may be atypical. For suppurative parotitis, send a Gram stain and culture of pus from the Stensen duct and blood cultures in the systemically unwell child, and image with ultrasound to detect abscess or stone. For juvenile recurrent parotitis, ultrasound is the first-line imaging tool, showing sialectasis, gland heterogeneity and ductal dilation; sialography and MRI sialography are reserved for detailed anatomical assessment before sialendoscopy. [3] [4]
Management — Resuscitation
The salivary gland disorder that most commonly needs resuscitation is acute suppurative parotitis in the neonate or immunocompromised child, and the resuscitation mindset is antibiotics and hydration first, drainage second. Mumps rarely needs resuscitation in the immunocompetent child, but the child who cannot maintain oral hydration from parotid pain, or who presents with meningitis, pancreatitis or severe orchitis, needs supportive care in hospital. [9] [10]
Assess the febrile, irritable neonate with parotid swelling for dehydration and systemic sepsis — moist mucous membranes, capillary refill, urine output and temperature — and correct fluid deficits early, because dehydration both predisposes to and complicates suppurative parotitis. Start intravenous anti-staphylococcal antibiotics promptly after taking cultures, and image with ultrasound to look for abscess. Antibiotic therapy does not substitute for drainage if an abscess has formed. [9]
Management — Definitive & Stepwise
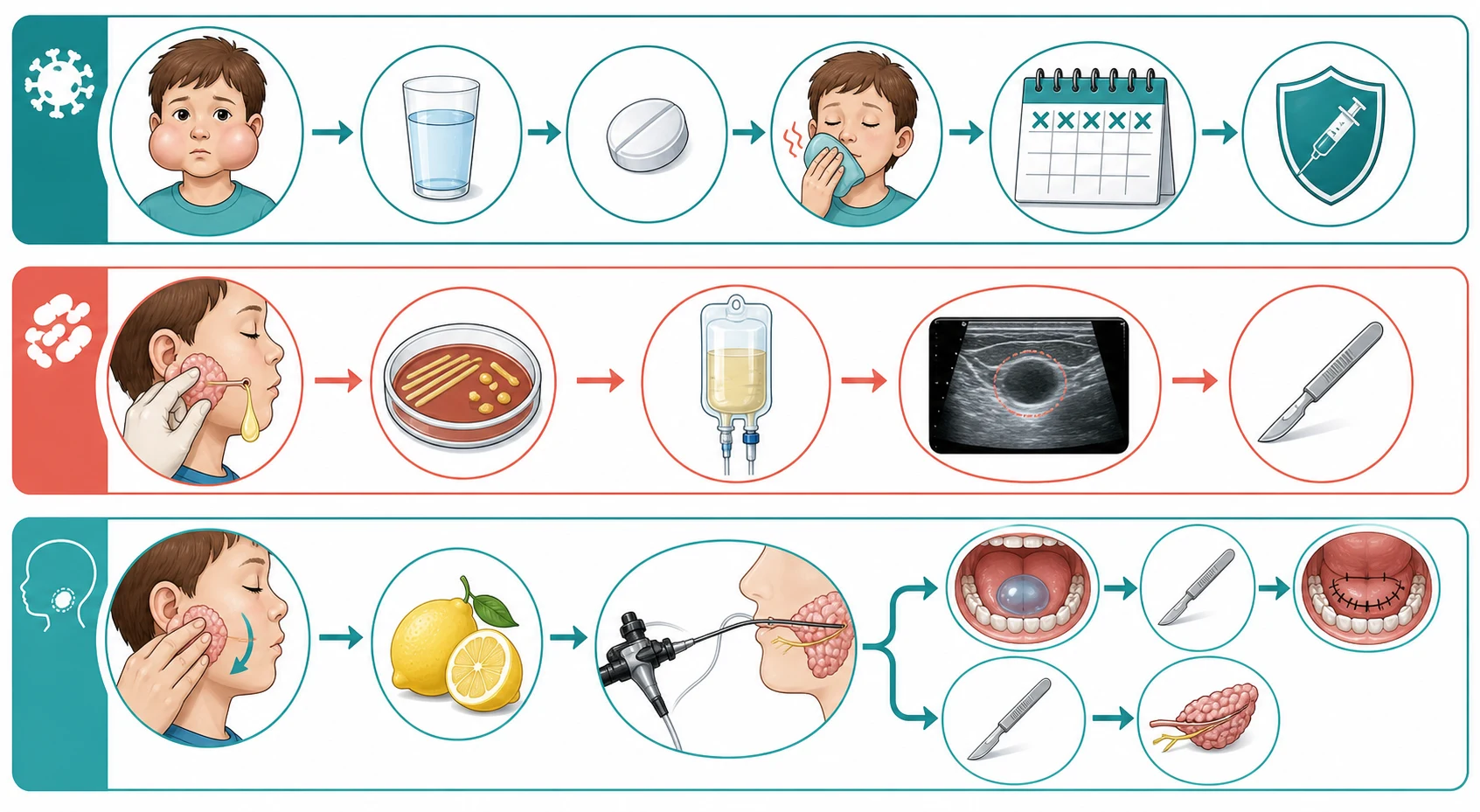
Once the pattern is named, salivary gland disease is managed with supportive care first, then antibiotics for suppurative parotitis, massage and sialendoscopy for recurrent disease, and surgery for the ranula or tumour. [2]
Stepwise management of paediatric salivary gland disorders
Hydration and analgesia first — encourage oral fluids, give paracetamol 15 mg per kilogram (maximum 1 g) and ibuprofen 5 to 10 mg per kilogram, and apply warm compresses to the tender gland.
Match the cause — supportive care for mumps; anti-staphylococcal antibiotics for suppurative parotitis; gland massage, hydration and sialogogues for juvenile recurrent parotitis; surgical referral for ranula or tumour.
Suppurative parotitis — intravenous flucloxacillin 25 to 50 mg per kilogram per dose (maximum 2 g) every six hours, with ultrasound-guided drainage if an abscess forms; switch to oral therapy once the child defervesces and the swelling subsides.
Juvenile recurrent parotitis — gland massage, warm compresses, sialogogues (sour sweets, lemon, chewing gum), analgesia, and a short course of antibiotics if secondary bacterial infection is suspected; refer for sialendoscopy if flares are frequent or severe.
Ranula — small asymptomatic lesions can be observed; marsupialisation or excision of the ipsilateral sublingual gland for symptomatic, recurrent or plunging ranula, coordinated with the paediatric otolaryngology team.
Safety-net and review — review the well child in 48 to 72 hours, with return for spreading redness, increasing pain, high fever, refusal to drink, testicular pain, headache or neck stiffness.
For mumps, management is entirely supportive — analgesia, hydration, warm compresses and soft diet — with no role for antiviral therapy. Exclude the child from school or childcare for five days from the onset of parotid swelling, and notify public health. The cornerstone of prevention is the MMR vaccine, given in two doses. In Australia the schedule is MMR at 12 months and MMRV at 18 months; in the UK at 12 to 13 months and at 3 years and 4 months; in the US at 12 to 15 months and 4 to 6 years. Two doses provide approximately 88 per cent protection against mumps. [1]
For acute suppurative parotitis, give intravenous flucloxacillin to cover Staphylococcus aureus, the leading organism, switching to a broader regimen if group B streptococcus or gram-negative organisms are suspected in the neonate. Ultrasound-guided drainage is needed if an abscess has formed. For juvenile recurrent parotitis, conservative measures — gland massage, hydration, sialogogues and analgesia — are first-line, with a short course of oral antibiotics for suspected secondary infection; sialendoscopy with duct lavage and steroid installation reduces flare frequency and severity in refractory cases. [3] [5]
Specific Subtypes & Scenarios
The scenarios below are the ones examiners reach for, because each forces a different decision between supportive care, antibiotics, sialendoscopy and surgery. [2]
The under-immunised child with bilateral parotitis and fever has mumps — supportive care, isolate for five days, notify public health, and watch for orchitis in post-pubertal boys, meningitis, pancreatitis and hearing loss. The neonate with unilateral parotid swelling, fever and irritability has neonatal suppurative parotitis — intravenous anti-staphylococcal antibiotics, blood cultures, ultrasound, and a low threshold for drainage. [1] [9]
The child with recurrent parotid swelling between flare-ups has juvenile recurrent parotitis — ultrasound to document sialectasis, conservative management with massage and sialogogues, and sialendoscopy for frequent or severe flares. The child with a soft bluish swelling in the floor of the mouth has a ranula — observe if small and asymptomatic, refer to paediatric otolaryngology for marsupialisation or sublingual gland excision if symptomatic or recurrent, and image a suspected plunging ranula with ultrasound or MRI to define the neck extension. [3] [7]
The child with meal-time submandibular swelling and pain has sialolithiasis — encourage hydration and gland massage, image with ultrasound, and refer for stone removal or sialendoscopy if the stone does not pass. The child with a firm, painless, slowly growing parotid mass has a possible tumour — ultrasound and fine-needle aspiration or biopsy coordinated with the otolaryngology team, because a pleomorphic adenoma can recur and a mucoepidermoid carcinoma can metastasise. [2] [8]
Complications & Pitfalls
The cardinal pitfall is treating every parotid swelling as mumps and missing the suppurative gland needing antibiotics, the recurrent pattern needing a work-up, or the firm mass that is a tumour. The child with unilateral, exquisitely tender parotid swelling and pus from the Stensen duct does not have mumps — milking the duct prevents that error at the bedside. [2] [9]
Recognise the complications of mumps that bring the child back: orchitis in up to a third of post-pubertal males, which can cause testicular atrophy; meningitis in 1 to 10 per cent and aseptic meningitis as the most common neurological complication; encephalitis in roughly 0.03 per cent, which can be fatal or leave permanent neurological deficit; pancreatitis, usually mild and self-limiting; and sensorineural hearing loss, rare but permanent, occurring in approximately 1 in 20,000 cases. Avoid routine antibiotics for uncomplicated viral parotitis, and never assume a firm parotid mass is inflammatory without imaging and, if needed, biopsy. [1]
Prognosis & Disposition
Mumps resolves within seven to ten days with supportive care, and lifelong immunity follows infection. Orchitis resolves over days to weeks with conservative support; testicular atrophy occurs in up to half of affected testes but bilateral disease and infertility are uncommon. Juvenile recurrent parotitis follows a relapsing course over years, but the majority of children resolve spontaneously by puberty, with or without sialendoscopy. [1] [3]
Discharge the well-hydrated child with viral parotitis on supportive care and a clear safety-net for orchitis, meningitis, pancreatitis and hearing loss. Admit the neonate or immunocompromised child with suppurative parotitis for intravenous antibiotics and imaging. Refer the child with recurrent parotitis for ultrasound and otolaryngology assessment, and refer any child with a firm, painless parotid mass, a recurrent or plunging ranula, or a persistent floor-of-mouth swelling for surgical evaluation. [9] [8]
Special Populations
Immunocompromised children — oncology patients, post-transplant recipients, and children with HIV — are the population in whom salivary gland disease crosses from nuisance to danger: suppurative parotitis runs a severe course, mumps can reactivate or present atypically, and HIV-associated lymphoepithelial cysts produce chronic bilateral parotid enlargement that responds to antiretroviral therapy. Investigate and escalate aggressively with broad-spectrum antibiotics and imaging where the host demands it. [10]
Neonates are uniquely vulnerable to suppurative parotitis because of their immature immune defences, tendency to dehydration, and the colonisation of the oral cavity with Staphylococcus aureus and group B streptococcus. The threshold for intravenous antibiotics and imaging is low. Under-immunised and migrant or refugee children carry a disproportionate burden of mumps where vaccine access, cold-chain integrity or vaccine hesitancy converge; provide catch-up MMR vaccination and culturally safe care with trained interpreters. Aboriginal and Torres Strait Islander and other remote-community children benefit from coordinated oral-health, immunisation and otolaryngology services that address salivary and ear disease together. [1] [9]
Evidence, Guidelines & Regional Differences
The named regional guidance is the CDC guidance on mumps for healthcare providers, the UKHSA Green Book Chapter 23 on mumps immunisation, and the RCH Melbourne clinical practice guidelines for parotitis and salivary gland swelling. The evidence base for mumps rests on decades of surveillance data confirming that two-dose MMR vaccination reduces mumps incidence by over 95 per cent, and on outbreak investigations that document waning immunity as the driver of resurgence in young adults. [1]
The evidence base for juvenile recurrent parotitis is built on systematic reviews of treatment studies showing that conservative measures — massage, hydration, sialogogues and analgesia — are first-line, with sialendoscopy reducing flare frequency and severity in refractory disease. For ranula, systematic review and meta-analysis evidence favours excision of the sublingual gland over marsupialisation alone for reducing recurrence. The evidence for neonatal parotitis is limited to case series and literature reviews that consistently identify Staphylococcus aureus as the leading organism and prematurity and dehydration as the leading risk factors. [4] [5] [7]
[1] [2]Exam Pearls
References
- [1]Hviid A; Rubin S; Mühlemann K Mumps. Lancet, 2008.PMID 18342688
- [2]Kim MJ; Milliren A Salivary Gland Disorders: Rapid Evidence Review. Am Fam Physician, 2024.PMID 38905553
- [3]Wood J; Toll EC; Gregory S; Little C Juvenile recurrent parotitis: Review and proposed management algorithm. Int J Pediatr Otorhinolaryngol, 2021.PMID 33421670
- [4]Garavello W; Redaelli M; Galli A Juvenile recurrent parotitis: A systematic review of treatment studies. Int J Pediatr Otorhinolaryngol, 2018.PMID 30055724
- [5]Soriano-Martín D; García-Consuegra L; Peña-García P; et al Sialendoscopy approach in treating juvenile recurrent parotitis: a systematic review. J Otolaryngol Head Neck Surg, 2023.PMID 37598195
- [6]Singh P; Gupta D Juvenile Recurrent Parotitis. Indian J Pediatr, 2019.PMID 30788670
- [7]Nguyen K; Goodman E; Chhith S; et al Systematic Review and Meta-Analysis of the Management and Outcomes of Recurrent Ranulas. Oral Dis, 2026.PMID 41841403
- [8]Bowers EMR; Schaitkin B Management of Mucoceles, Sialoceles, and Ranulas. Otolaryngol Clin North Am, 2021.PMID 34024482
- [9]Mori T; Shimomura R; Himoto S; et al Neonatal suppurative parotitis: Case reports and literature review. Pediatr Int, 2022.PMID 33955624
- [10]Pollenus J; Van Lierde S Neonatal Parotitis: A Case Report and Review of the Literature. Pediatr Infect Dis J, 2023.PMID 37171966