Paeds · ent-hearing-and-oral-health
Tinnitus, vertigo and balance disorders in children
Also known as Paediatric dizziness · Vestibular migraine of childhood · Benign paroxysmal vertigo of childhood · Vestibular neuritis in children · Paediatric BPPV · Childhood tinnitus · Balance disorders in children
Fellowship guide to tinnitus, vertigo and balance disorders in children: separating the common benign causes, benign paroxysmal vertigo of childhood and vestibular migraine, from the acute peripheral vestibular neuritis and the dangerous central mimics, the bedside distinction of peripheral from central nystagmus, the red-flag screen that drives urgent magnetic resonance imaging, and the management built on reassurance, the Epley manoeuvre for positional vertigo, and early vestibular rehabilitation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the three-year-old who freezes mid-play, goes pale, clings to a parent, and looks terrified for half a minute before returning to normal, and whose parents fear a seizure. That child carries the whole teaching point of paediatric dizziness. The episode is alarming to the family but is usually benign. The diagnosis is clinical, and the clinician's job is to confirm the safe pattern and to exclude the small minority that are dangerous. The decisive first question is not which drug to give but whether the vertigo is peripheral or central, and whether red flags are present. That single distinction separates reassurance from urgent imaging. [2] [4]
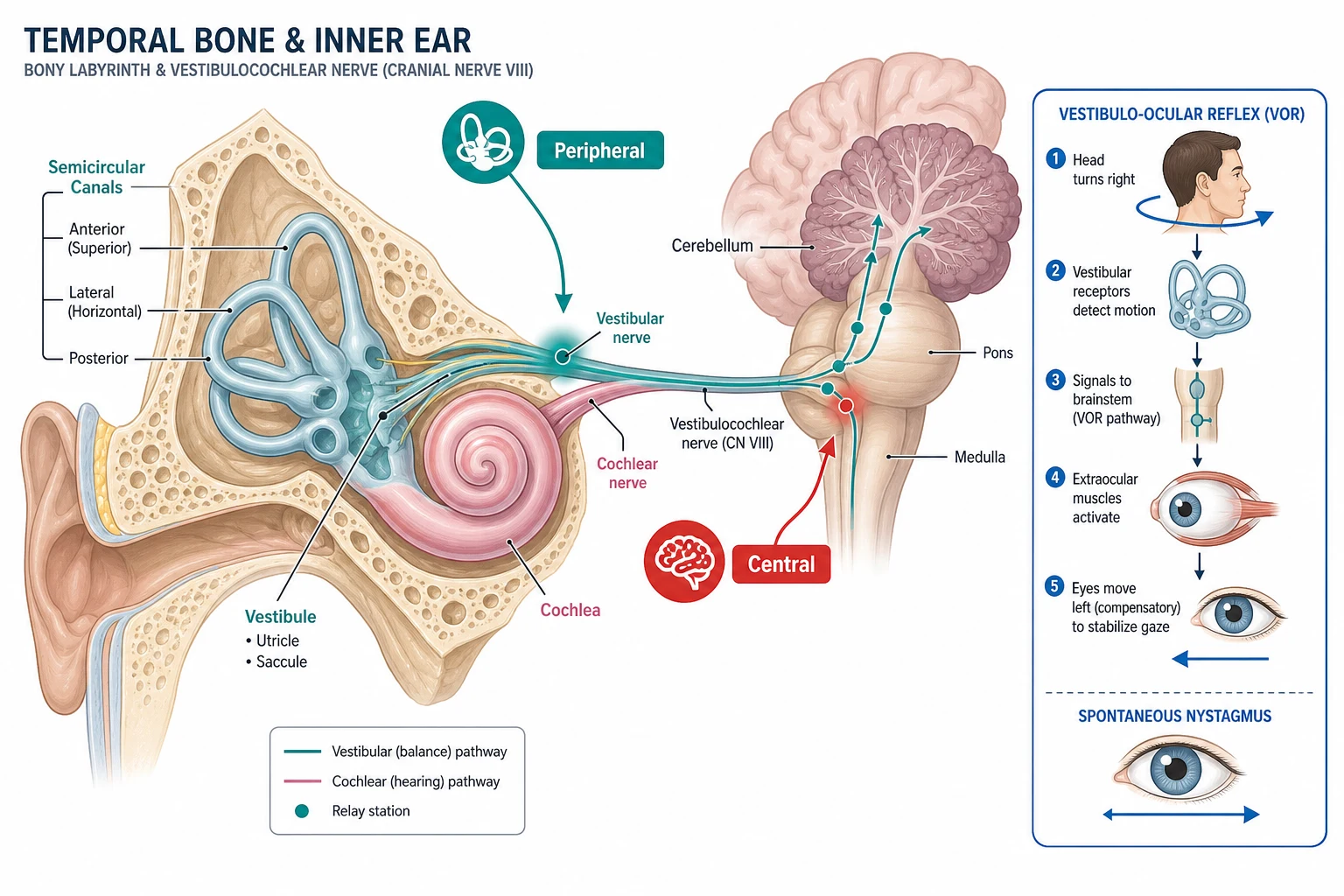
Vertigo is the false sensation of movement, usually a sense of spinning, that arises from a mismatch between the vestibular, visual, and proprioceptive inputs to balance. Dizziness is the broader, non-specific term that children and families use for vertigo, light-headedness, unsteadiness, and a vague floating feeling. The first clinical task is to establish which of these the child means. The vestibular apparatus comprises the three semicircular canals, which sense angular acceleration, and the otolith organs, which sense linear acceleration and gravity. Their signals travel through the vestibulocochlear nerve to the brainstem and cerebellum. A lesion anywhere in this pathway produces vertigo, and the character and duration of the vertigo, the nystagmus pattern, and any hearing loss localise the lesion. [7] [12]
Tinnitus is the perception of sound, such as ringing, buzzing, or hissing, in the absence of an external source, and in children it is common and usually benign. Most paediatric tinnitus arises from a reversible cause, such as cerumen impaction, otitis media with effusion, or noise exposure, and resolves with the cause. A minority signals a serious disorder. Unilateral, pulsatile, or persistent tinnitus, or tinnitus with a hearing loss, is the pattern that demands audiological assessment and, when indicated, imaging to exclude a retrocochlear or a vascular lesion. The framework that unifies vertigo and tinnitus is the peripheral-versus-central split combined with the red-flag screen. The same screen that governs the imaging decision in the dizzy child governs it in the child with troublesome tinnitus. [9] [3]
Classification
The most useful first cut in a child with vertigo is the duration of the episodes. It sorts the common benign recurrent vertigos from the acute prolonged vestibulopathy and the chronic imbalance. Brief, stereotyped, recurrent episodes that last seconds to minutes point to the periodic syndromes of childhood. These are benign paroxysmal vertigo of childhood in the preschool years and vestibular migraine in the school-age child, and benign paroxysmal positional vertigo, which is triggered by head movement. A single, prolonged attack lasting hours to days points to an acute vestibular syndrome, vestibular neuritis or labyrinthitis. A constant, progressive unsteadiness points to a chronic vestibular hypofunction or a central lesion. The second cut, applied throughout, is peripheral versus central, because the central causes are the ones that harm the child if missed. [1] [7]
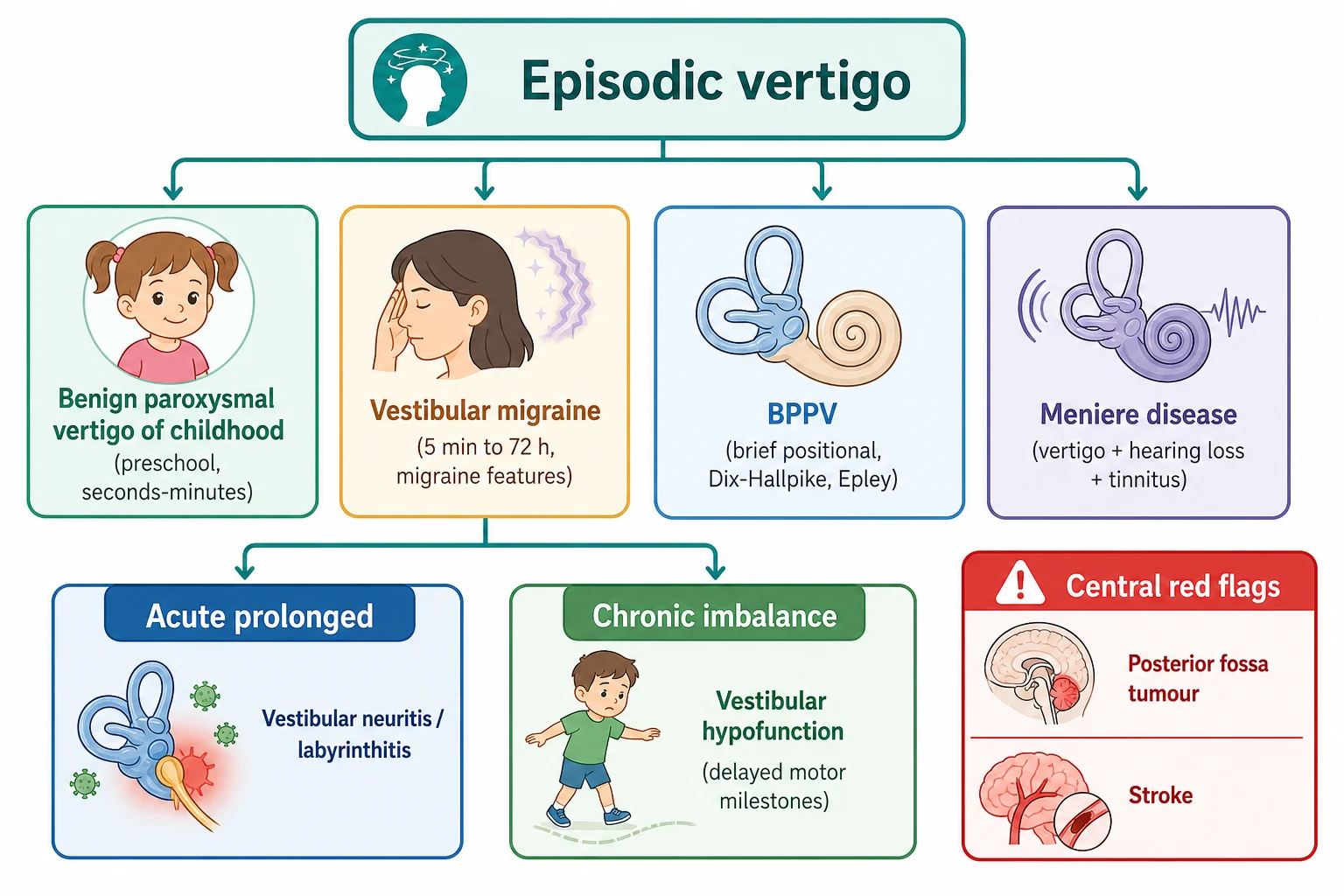
Within the episodic group, benign paroxysmal vertigo of childhood is the commonest cause of vertigo in a preschool child. It presents with sudden, brief episodes that resolve completely and leave a normal examination. Vestibular migraine is the commonest cause of recurrent vertigo in the school-age child and adolescent. It is defined by consensus criteria that require recurrent vestibular symptoms lasting minutes to hours with migraine features. Benign paroxysmal positional vertigo gives brief vertigo, under a minute, triggered by a change in head position, such as rolling over in bed or looking up. It is the one vestibular cause with a curative bedside manoeuvre. Meniere disease is rare in children. It combines episodic vertigo with a fluctuating low-frequency sensorineural hearing loss, tinnitus, and aural fullness. [2] [1] [8]
BPVC
preschool
- Onset one to four years, peak two to three years
- Sudden brief vertigo, seconds to minutes
- Child looks frightened and pale, may vomit
- Normal between attacks, no loss of consciousness
- Strong family history of migraine, resolves before school
Vestibular migraine
school-age
- Commonest recurrent vertigo beyond preschool years
- Vertigo lasting five minutes to seventy-two hours
- Migraine features in at least half of attacks
- Personal or family history of migraine
- Reassurance, lifestyle, prophylaxis if disabling
BPPV
positional
- Brief vertigo under one minute, position-triggered
- Positive Dix-Hallpike with torsional upbeating nystagmus
- Posterior canal most common
- Often post-traumatic or post-concussion in adolescents
- Curative Epley canalith repositioning manoeuvre
Central red flag
dangerous
- Focal neurological sign or ataxia between attacks
- Gaze-evoked or direction-changing nystagmus
- Papilloedema or raised intracranial pressure
- Unilateral or progressive hearing loss
- Urgent magnetic resonance imaging
Epidemiology & Risk Factors
Dizziness and vertigo are common in childhood, though far less often the reason for a medical consultation than in adults, because young children struggle to articulate the symptom. Community-based studies place the lifetime prevalence of dizziness or vertigo at roughly a quarter of children and adolescents. Vertigo severe enough to bring a child to medical attention accounts for a meaningful minority of paediatric neurology and otolaryngology referrals. The epidemiology review by Neuhauser framed dizziness and vertigo as a problem across the life course. It emphasised that the causes shift with age, from the periodic syndromes of the young child to migraine and the trauma-related causes in the adolescent. [12] [4]
Benign paroxysmal vertigo of childhood is the commonest cause of vertigo in a preschool child, with an onset typically between one and four years of age and a peak around two to three years. The episodes are brief and recurrent. The strongest risk factor is a family history of migraine, because the condition is an episodic syndrome that may be associated with migraine. A substantial proportion of affected children go on to develop migraine or vestibular migraine later in childhood. The condition resolves spontaneously in most children before they start school, which is the foundation of the reassuring family consultation. [2]
Vestibular migraine is the commonest cause of recurrent vertigo in the school-age child and adolescent. Its risk factors are those of migraine itself, a family history of migraine, female sex after the peripubertal years, and the common triggers of sleep deprivation, stress, and screen time. Benign paroxysmal positional vertigo is uncommon in young children but becomes a recognisable cause of vertigo in the adolescent, particularly after a head injury or a sports-related concussion. The displacement of otoconia into a semicircular canal produces the characteristic brief positional vertigo. The studies of positional vertigo after paediatric concussion confirmed that it is an under-recognised and treatable consequence of head injury in young athletes. [1] [6]
The numbers that anchor your viva
Pathophysiology
The sense of balance is built from the fusion of three sensory inputs, the vestibular, the visual, and the proprioceptive. A lesion or mismatch in any one produces the sensation of vertigo or dizziness. The vestibular end organ in the inner ear comprises the three semicircular canals, which detect angular acceleration through the deflection of hair cells by the moving endolymph, and the otolith organs, which detect linear acceleration and head tilt relative to gravity. The vestibular nerve carries these signals to the vestibular nuclei in the brainstem and to the cerebellum. There they are integrated with visual and proprioceptive input to stabilise gaze through the vestibulo-ocular reflex and to maintain posture through the vestibulospinal reflex. Understanding this three-neuron arc lets the clinician localise the lesion from the bedside examination alone. [7] [11]
The mechanism of an acute unilateral vestibular loss, whether from vestibular neuritis or labyrinthitis, is a sudden asymmetry of vestibular input between the two ears. The brain interprets this asymmetry as a violent spinning toward the healthy side. The affected ear stops firing, so the intact ear dominates. The resulting imbalance of tonic neural activity produces a spontaneous nystagmus that beats away from the affected ear, toward the healthy side. Nausea, vomiting, and a falling tendency toward the affected side accompany it. When the lesion spares the cochlea the hearing is preserved and the syndrome is vestibular neuritis. When the cochlea is involved a sensorineural hearing loss appears and the syndrome is labyrinthitis. The head impulse test is abnormal toward the affected ear, because the damaged canal cannot generate the vestibulo-ocular reflex. The eyes then drift back to the target with a corrective saccade that the clinician sees. [7]
The mechanism of vestibular migraine is an abnormal processing of vestibular and sensory information within a brain that is predisposed to migraine, rather than a structural lesion of the vestibular apparatus. This explains why the vertigo of vestibular migraine can occur with or without headache. It also explains why migraine features such as photophobia, phonophobia, and visual aura accompany the attacks, and why the condition shares its triggers and its prophylactic treatment with migraine headache. The mechanism of benign paroxysmal positional vertigo is mechanical and discrete. Otoconia dislodged from the utricle enter a semicircular canal, most often the posterior canal, and move under gravity with head position change. This produces a brief, intense vertigo and the characteristic fatigable nystagmus. The success of the Epley manoeuvre follows directly from this mechanism, because repositioning the otoconia back out of the canal cures the vertigo. [11] [5]
[7]Clinical Presentation
The typical story of benign paroxysmal vertigo of childhood is a previously well toddler or preschool child who suddenly stops, goes pale, looks frightened or unsteady, and may clutch a parent or vomit, before returning to normal within seconds to minutes. Between the attacks the child is entirely well, the neurological examination is normal, and there is no loss of consciousness. That last feature separates the condition from a seizure. The episodes are stereotyped and recurrent over weeks to months, and a careful history reveals a family history of migraine in many cases. The onset is in the preschool years, the episodes resolve before the child starts school in most cases, and the child may later develop vestibular migraine or migraine headache. [2]
The child with vestibular migraine presents with recurrent episodes of vertigo that last minutes to hours, sometimes up to seventy-two hours. Nausea accompanies them, and in at least half of the attacks so do migraine features such as headache, photophobia, phonophobia, or a visual aura. The vertigo may be spontaneous, triggered by head movement, or brought on by visual stimulation, and the child is normal between the attacks. A personal history of migraine, or a strong family history, supports the diagnosis, which rests on the consensus criteria rather than on a single test. The presentation overlaps with benign paroxysmal vertigo of childhood in the younger child. The two are best understood as a continuum of the migraine spectrum across childhood. [1] [11]
The child with vestibular neuritis presents with the acute onset of severe, continuous vertigo, nausea, and vomiting that lasts for hours to days, with a marked unsteadiness and a preference to lie still. The spontaneous nystagmus is horizontal and torsional, beats away from the affected ear, and is present even when the child fixes on a target. The head impulse test is abnormal toward the affected ear, and there is no hearing loss. The child with labyrinthitis tells the same story but adds an acute sensorineural hearing loss or tinnitus, which localises the lesion to the labyrinth rather than the nerve alone. The clinical danger in the acute vestibular syndrome is the posterior circulation stroke that mimics neuritis. The head impulse, nystagmus, test of skew rule is the bedside safeguard that separates them. [7]
| Clinical picture | What it implies | Act |
|---|
The child with tinnitus most often has a readily identifiable and benign cause, such as cerumen impaction, otitis media with effusion, or noise exposure, and the symptom resolves with the cause. Troublesome tinnitus is less common in children than in adults but is under-recognised, because young children rarely report it spontaneously. A direct question to the child and the family is part of the assessment. The pattern that demands investigation is unilateral or pulsatile tinnitus, tinnitus with a hearing loss, or tinnitus that is persistent and progressive, because these patterns raise a retrocochlear or a vascular lesion. The history of the tinnitus, its laterality, its quality, and its association with hearing loss direct the audiological and imaging workup. [9]
Differential Diagnosis
The first differential question is whether the symptom is vertigo at all, because presyncope, disequilibrium, and a vague light-headedness all produce a dizziness that the family labels as vertigo. A child with presyncope describes a light-headed, fading feeling on standing, often with a visual dimming, and the history of postural provocation and the cardiovascular examination separate it. A child with disequilibrium describes an unsteadiness without a spinning sensation, often worse in the dark, and the examination for ataxia and proprioception directs the workup toward a cerebellar or a sensory cause. Establishing the quality of the dizziness, its duration, and its triggers is the first step that frames the whole differential. [4] [7]
The second and dangerous question is whether an acute vestibular syndrome is peripheral or central, and the head impulse, nystagmus, test of skew rule answers it at the bedside. A peripheral cause gives an abnormal head impulse, a unidirectional nystagmus, and no skew. A central cause gives a normal head impulse, a direction-changing nystagmus, or a skew deviation. The central mimics of an acute vestibular syndrome are the posterior circulation stroke, a demyelinating lesion, and a posterior fossa tumour. Any central sign on the rule is an indication for urgent magnetic resonance imaging. The peripheral causes are vestibular neuritis and labyrinthitis, and they are diagnosed on the clinical pattern once the central signs are excluded. [7]
Peripheral vertigo
- Unidirectional horizontal-torsional nystagmus, fast phase away from lesion
- Abnormal head impulse test toward affected ear
- No skew deviation
- Hearing loss only if labyrinth involved
- Vestibular neuritis, labyrinthitis, BPPV, Meniere
Central vertigo
- Direction-changing or gaze-evoked nystagmus
- Normal head impulse test
- Skew deviation may be present
- Focal neurological signs or ataxia
- Stroke, demyelination, posterior fossa tumour
Non-vestibular dizziness
- Presyncope, light-headedness on standing
- Disequilibrium, worse in the dark
- No true spinning sensation
- Cardiovascular, cerebellar, or sensory cause
- Hypoglycaemia and anxiety are mimics
Seizure mimic
- Episodic unsteadiness with altered awareness
- Loss of consciousness separates it from BPVC
- Abnormal electroencephalogram
- Benign paroxysmal vertigo has no loss of consciousness
- Normal EEG in BPVC
The differential of recurrent vertigo in childhood is dominated by benign paroxysmal vertigo of childhood and vestibular migraine. The distinction rests on the age of the child and the duration and the accompaniments of the attacks. Benign paroxysmal vertigo of childhood presents in the preschool years with attacks lasting seconds to minutes and a normal interictal examination. Vestibular migraine presents in the older child with attacks lasting minutes to hours and migraine features. Meniere disease is rare in children and is distinguished by the fluctuating low-frequency sensorineural hearing loss. The episodic ataxias and the cardiac causes of presyncope complete the differential. The principle is that a recurrent vertigo with a normal interictal examination and a negative red-flag screen is managed with reassurance, while any progressive course or focal sign redirects the workup. [2] [8]
Clinical & Bedside Assessment
The assessment of the dizzy child begins with the tempo and the duration, because these two features alone frame the differential. Establish whether the vertigo is episodic and brief, single and prolonged, or constant and progressive, and whether the episodes are improving, static, or worsening. Ask the child to describe the quality of the dizziness, whether it is a true spinning, a light-headedness, or an unsteadiness. Ask about the triggers, the position change, the visual stimulation, and the association with headache or hearing change. A history of a recent viral illness, a head injury, or a concussion, and a personal or family history of migraine, are the high-yield elements that the targeted history reveals. [3] [4]
The nystagmus examination is the single most informative bedside test in the dizzy child, and the character of the nystagmus separates the peripheral from the central cause. Observe for spontaneous nystagmus in the primary position. Then ask the child to look to the left, the right, and up, and note whether the nystagmus is unidirectional or direction-changing. A peripheral vestibular lesion produces a unidirectional horizontal-torsional nystagmus that beats away from the affected ear. It is present in the primary position and enhanced by looking in the direction of the fast phase. A central lesion produces a direction-changing or a gaze-evoked nystagmus. A vertical, purely downbeating or upbeating nystagmus is a central sign and an indication for imaging. [7] [11]
The head impulse test assesses the vestibulo-ocular reflex of each horizontal canal and is the cornerstone of the peripheral-versus-central distinction. The examiner turns the child's head rapidly by a small angle toward one side while the child fixes on a target. A normal response keeps the eyes on the target. An abnormal response allows the eyes to drift with the head, which then snaps back to the target with a corrective saccade. An abnormal head impulse toward the affected ear is a peripheral sign. A normal head impulse in a child with an acute vestibular syndrome is a central sign that demands imaging. The test of skew, looking for a vertical misalignment of the eyes on alternate cover, completes the rule. Any skew deviation is a central sign. [7]
The Dix-Hallpike manoeuvre tests for benign paroxysmal positional vertigo and should be performed in any child with brief positional vertigo. The examiner turns the child's head to one side, then lays the child back rapidly with the head extended over the edge of the bed. The manoeuvre elicits the characteristic latent, torsional upbeating nystagmus that fatigues on repetition. A positive Dix-Hallpike on one side localises the posterior canal, and the manoeuvre doubles as the starting position for the curative Epley repositioning. The bedside examination is completed by an assessment of gait and balance, the cerebellar signs, the hearing, the ear, and the fundoscopy for papilloedema. [5] [3]
[3] [7]Investigations
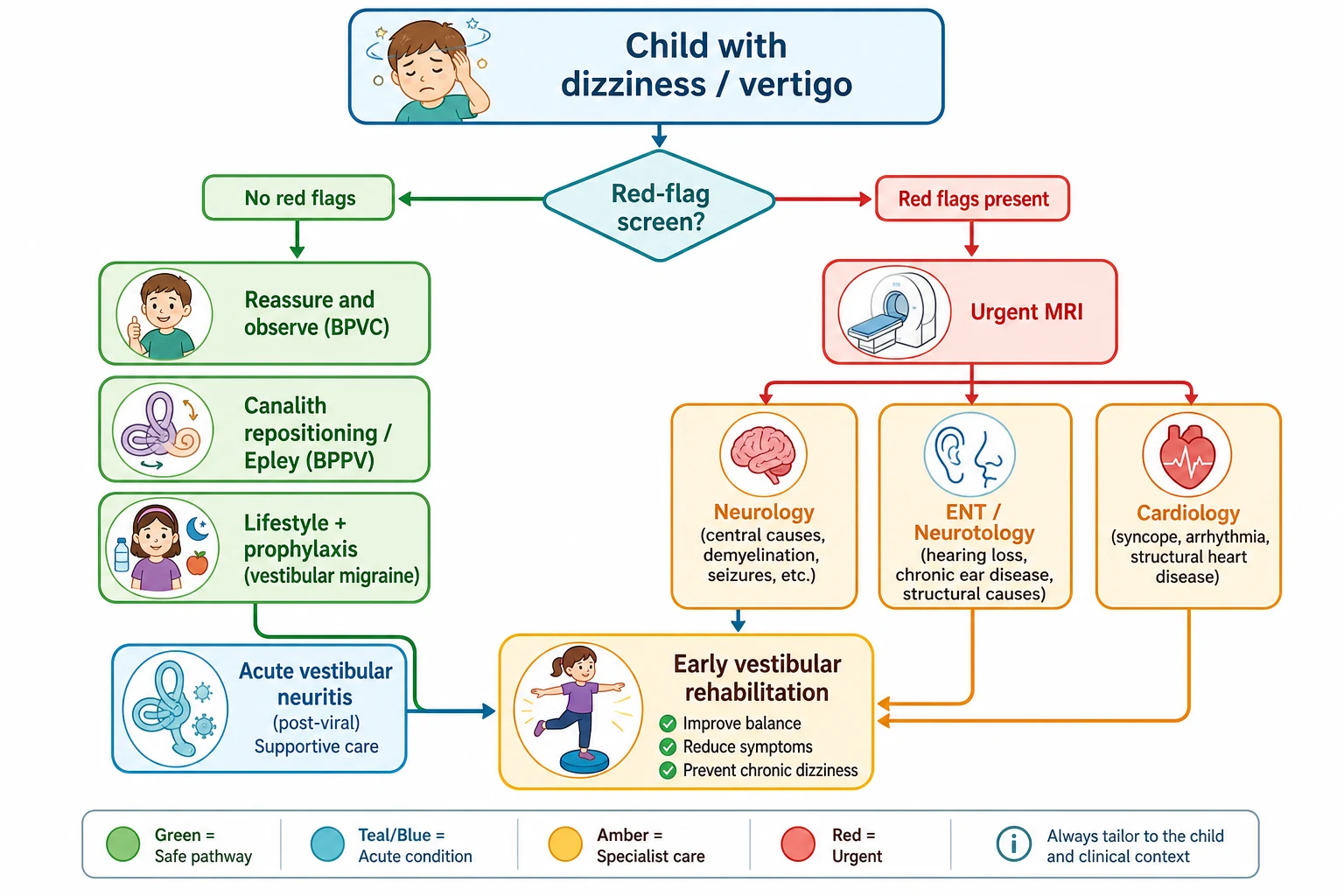
The guiding principle for a child who meets a benign recurrent pattern, with a normal interictal examination and a negative red-flag screen, is that investigation is minimal and imaging is not routine. Benign paroxysmal vertigo of childhood and vestibular migraine are clinical diagnoses that rest on the consensus criteria. A child with the classic pattern does not need a scan, a blood test, or an electroencephalogram to confirm them. Over-investigation exposes the child to radiation, to the sedation of computed tomography, and to incidental findings that raise anxiety. It also delays the reassurance that is the treatment. The pure-tone audiogram is the one test performed for most dizzy children, because an unsuspected hearing loss redirects the workup toward a cochlear or a retrocochlear cause. [3] [2]
Neuroimaging is reserved for the child with a red flag, an acute vestibular syndrome that fails the head impulse, nystagmus, test of skew rule, a focal deficit, or a progressive or unexplained course. The modality is magnetic resonance imaging whenever possible. Computed tomography is reserved for the acute emergency where magnetic resonance imaging is unavailable or where the immediate question is an acute haemorrhage, because it delivers less detail of the posterior fossa and a radiation dose. A child with unilateral, asymmetric, or progressive sensorineural hearing loss, with or without tinnitus, has a retrocochlear lesion until proven otherwise. The child needs a gadolinium-enhanced magnetic resonance imaging of the internal auditory meati and the brain to exclude a vestibular schwannoma, particularly in a child with neurofibromatosis type 2. [7] [9]
Vestibular function testing refines the peripheral diagnosis when the bedside examination is equivocal and documents the degree and the side of the vestibular loss. Videonystagmography or electronystagmography records the spontaneous and the induced nystagmus. The caloric test assesses each horizontal canal through the warm and the cool irrigation, and the video head impulse test quantifies the gain of each canal. The vestibular-evoked myogenic potentials assess the otolith organs. Together these tests localise the lesion to the canal, the nerve, or the central pathway. The audiological assessment, the pure-tone audiogram, the tympanometry, and where indicated the otoacoustic emissions, complete the workup. They are performed in any child with a hearing loss or troublesome tinnitus. [3] [10]
The child with troublesome tinnitus has a directed workup that begins with a full audiological assessment to document and to characterise any hearing loss. Unilateral or pulsatile tinnitus, or tinnitus with an asymmetric hearing loss, is investigated with magnetic resonance imaging of the temporal bone and the internal auditory meati. This excludes a vestibular schwannoma, a glomus tumour, or a vascular lesion. The majority of children with tinnitus have a benign cause, such as cerumen, otitis media with effusion, or noise. The imaging is reserved for the red-flag patterns, while the management of the common case addresses the underlying cause and the symptom. [9]
Management — Resuscitation
The resuscitation priority in the child with an acute vestibular syndrome is to control the violent vertigo and the vomiting, to ensure hydration, and to recognise the central cause that changes the plan. A child who is vomiting continuously is at risk of dehydration. The first steps are antiemesis, fluid replacement, and a safe place to lie still while the acute vertigo settles. The acute vestibular suppressants, such as prochlorperazine or ondansetron at standard paediatric doses, are used for a short course of one to three days to control the acute vertigo and vomiting. Their prolonged use impairs the central compensation that is the route to recovery, so they are stopped early. [7] [3]
The recognition of a central cause is the resuscitation act that saves the child from a missed stroke or tumour. The head impulse, nystagmus, test of skew rule is applied at the bedside in the acute vestibular syndrome. A child with a normal head impulse test, a direction-changing nystagmus, or a skew deviation in the acute vestibular syndrome is managed as a posterior circulation stroke until proven otherwise, with urgent imaging and the involvement of the neurology and the stroke teams. A child with a posterior fossa tumour and obstructive hydrocephalus who is deteriorating needs urgent neurosurgical decompression. The early recognition of raised intracranial pressure and the involvement of the neurosurgical and retrieval teams is the resuscitation priority. [7]
[7]Management — Definitive & Stepwise
The definitive management of benign paroxysmal vertigo of childhood is reassurance, because the condition is self-limiting and the episodes resolve before the child starts school in most cases. The family is counselled on the benign nature of the episodes, the absence of a seizure, the association with migraine, and the expected resolution. The child is reviewed only if the pattern changes. No medication alters the course, and the role of the clinician is to confirm the diagnosis, to exclude the red flags, and to reassure. The same principle applies to vestibular migraine in its mild form, where lifestyle measures on sleep, hydration, screen time, and the migraine triggers are the first step. [2] [1]
The definitive management of benign paroxysmal positional vertigo is the Epley canalith repositioning manoeuvre, which is curative in a single session in most children. The manoeuvre moves the displaced otoconia out of the posterior canal and back toward the utricle through a sequence of head positions. It follows directly from the Dix-Hallpike that localises the affected canal. The studies of positional vertigo in children confirmed that the repositioning is effective. They showed that the paediatric condition differs from the adult one mainly in the lower intensity of the nystagmus and the higher rate of a post-traumatic or post-concussion cause. Post-concussion positional vertigo is treated with the same Epley manoeuvre and is a treatable cause of persistent dizziness after a head injury. [5] [6]
The definitive management of an acute vestibular neuritis or labyrinthitis is early vestibular rehabilitation, supported by a short course of a vestibular suppressant for the acute vertigo alone. The acute suppressants are stopped after one to three days. Their prolonged use delays the central compensation that restores balance. The child is encouraged to move the head and to perform the gaze-stabilisation and the habituation exercises that drive the recovery. The vestibular rehabilitation review by Rine framed rehabilitation as the cornerstone of the management of vestibular hypofunction in children. It emphasised its role in restoring the motor milestones and the balance that a chronic vestibular loss impairs. [10]
VORTEX: the management of the dizzy child
The definitive management of vestibular migraine that is frequent or disabling adds a migraine prophylaxis to the lifestyle measures, using the same agents and the same principles as migraine headache. The paediatric migraine prophylaxis is built on lifestyle first and then on a prophylactic agent when the episodes remain disabling. The choice among propranolol, amitriptyline, and topiramate follows the paediatric migraine guidance and the individual child's comorbidity. The family is counselled that the vertigo of vestibular migraine shares the triggers and the prognosis of migraine headache, and that the response to the prophylaxis is judged over weeks to months. [1] [11]
Specific Subtypes & Scenarios
Vestibular neuritis and labyrinthitis are the acute vestibular syndromes of childhood, and the clinical task is to confirm the peripheral cause and to exclude the central mimic through the head impulse, nystagmus, test of skew rule. The child presents with the acute onset of severe continuous vertigo, nausea, and vomiting. The peripheral signs of an abnormal head impulse, a unidirectional nystagmus, and no skew establish vestibular neuritis when the hearing is preserved. The addition of a sensorineural hearing loss or tinnitus defines labyrinthitis. It prompts the audiological assessment and, when atypical, the imaging to exclude a vascular, an inflammatory, or a structural cause of the sudden hearing loss. The management is a short course of a suppressant and early vestibular rehabilitation, and the prognosis of the peripheral cause is good. [7]
Benign paroxysmal positional vertigo deserves its own scenario in the child and the adolescent because it is under-recognised and because it is the one vestibular cause with a curative bedside manoeuvre. The child describes brief vertigo, under a minute, triggered by rolling over in bed, looking up, or bending down. The Dix-Hallpike manoeuvre elicits the characteristic latent torsional upbeating nystagmus that fatigues on repetition. The posterior canal is most often affected, and the Epley repositioning cures the vertigo in a single session in most children. The recognition of positional vertigo after a sports-related concussion is the scenario that the examinations most often test, because it explains persistent dizziness after a head injury and because it is treatable. [5] [6]
Vestibular neuritis
the safe acute one
- Acute prolonged vertigo, nausea, vomiting
- Abnormal head impulse, unidirectional nystagmus, no skew
- Hearing preserved
- Short-course suppressant and early vestibular rehabilitation
- Good prognosis with central compensation
Labyrinthitis
with hearing loss
- Acute prolonged vertigo with sensorineural hearing loss
- Localises the lesion to the labyrinth
- Audiology and imaging if atypical
- Treat the cause, such as infection or vascular
- Early vestibular rehabilitation
BPPV
the curable one
- Brief positional vertigo under one minute
- Positive Dix-Hallpike with torsional upbeating nystagmus
- Posterior canal, often post-concussion in adolescents
- Epley canalith repositioning is curative
- Recognise and treat after head injury
Meniere disease
rare in children
- Episodic vertigo with fluctuating hearing loss
- Tinnitus and aural fullness complete the tetrad
- Low-frequency sensorineural hearing loss
- Exclude secondary causes in children
- Rare before adolescence
Meniere disease is rare in children and combines recurrent episodic vertigo with a fluctuating low-frequency sensorineural hearing loss, tinnitus, and aural fullness. The paediatric series by Wang and Young documented the clinical features. They emphasised that Meniere disease in children is far less common than in adults and that secondary causes, such as congenital, traumatic, or post-infectious injury to the inner ear, must be excluded. The management of the acute attack and the prevention of the progression follow the adult principles, adapted to the child. The long-term surveillance monitors the hearing that the disease threatens. The principle is that a child with the Meniere pattern is referred to otolaryngology for the full vestibular and audiological assessment. [8]
Complications & Pitfalls
The complications of dizziness and vertigo in children fall into the complications of the underlying disease and the complications of a missed or a delayed diagnosis. A child with a chronic vestibular hypofunction develops delayed motor milestones, impaired balance, and a reduced participation in play and sport, which the vestibular rehabilitation addresses. A child with vestibular migraine develops the disability of the frequent attacks and the school absence that the prophylaxis prevents. A child with an untreated positional vertigo after a concussion has persistent dizziness that a single Epley manoeuvre cures, and the missed diagnosis is a preventable burden. [10] [6]
The avoidable pitfalls recur in every examination. The first is the catastrophic error of dismissing a central cause as a benign periodic syndrome of childhood. A posterior circulation stroke, a posterior fossa tumour, and a demyelinating lesion each present with vertigo. The omission of the head impulse, nystagmus, test of skew rule or of the red-flag screen is the error that misses them. The second is the prolonged use of a vestibular suppressant beyond the acute attack, which delays the central compensation and converts a recoverable vestibular neuritis into a chronic imbalance. The third is the failure to perform the Epley manoeuvre in a child with positional vertigo, which leaves a curable condition untreated. The fourth is the dismissal of a unilateral or progressive hearing loss with tinnitus without imaging for a retrocochlear lesion. [7] [9]
Missed stroke
- Discharging a posterior circulation stroke as neuritis
- Omitting the head impulse, nystagmus, test of skew rule
- A normal head impulse with direction-changing nystagmus is central
- Urgent magnetic resonance imaging
- The cardinal error in the acute vestibular syndrome
Prolonged suppressant
- Vestibular suppressants beyond the acute attack
- Delays the central compensation
- Converts a recoverable neuritis into a chronic imbalance
- Limit to one to three days
- Rehabilitation is the treatment
Missed BPPV
- Positional vertigo attributed to concussion or migraine
- Dix-Hallpike not performed
- Epley manoeuvre not given
- A curable condition left untreated
- Common after head injury in adolescents
Missed retrocochlear lesion
- Unilateral hearing loss or tinnitus dismissed
- No audiological assessment
- No gadolinium magnetic resonance imaging
- Vestibular schwannoma or NF2 missed
- Imaging for any asymmetric or progressive loss
The complications of troublesome tinnitus in children are the impact on concentration, sleep, and mood, and the risk that a serious underlying cause is missed. The child with persistent tinnitus may have anxiety, sleep disturbance, and difficulty concentrating at school. The management addresses the symptom and its impact as well as the cause. The missed retrocochlear lesion or vascular malformation is the high-stakes error, and the red-flag patterns of unilateral, pulsatile, or progressive tinnitus are the safeguard against it. The principle is that troublesome tinnitus in a child is assessed with a full audiological workup and, when a red flag is present, with imaging. [9]
Prognosis & Disposition
The prognosis of benign paroxysmal vertigo of childhood is excellent and is the foundation of the family consultation, because the episodes resolve before the child starts school in most cases. The child is discharged with the reassurance that the episodes are benign, that they are not seizures, and that they reflect the migraine predisposition of the child and the family. The family is advised to return if the pattern changes. A proportion of the children go on to develop migraine or vestibular migraine later in childhood. This is explained to the family as the natural evolution of the migraine spectrum rather than a recurrence of the original condition. The disposition is community management with review only if the pattern changes. [2]
The prognosis of vestibular migraine is that of migraine across childhood, with a substantial proportion of children improving with lifestyle measures and a minority requiring a prophylactic agent. The episodes persist into adolescence and adulthood in a proportion, and the management is built on the lifestyle measures, the prophylaxis when the episodes are disabling, and the reassurance that the vertigo of vestibular migraine shares the prognosis of migraine headache. The disposition is outpatient management with the generalist or the neurologist. The long-term plan addresses the migraine triggers, the school attendance, and the quality of life. [1] [11]
The prognosis of an acute vestibular neuritis is good with the early vestibular rehabilitation that drives the central compensation, and most children recover their balance over weeks. The prognosis of labyrinthitis depends on the hearing, which may recover partially or persist, and the child is referred to audiology and otolaryngology for the hearing surveillance. The prognosis of a central cause depends on the underlying lesion. The role of the generalist is to recognise the red flags, to image, and to refer, because the early recognition shortens the interval to the treatment that changes the outcome. [7] [10]
Special Populations
The child with disability and neurodiversity may struggle to articulate the quality of the dizziness or to cooperate with the head impulse and the Dix-Hallpike manoeuvres. The behavioural signs of vertigo therefore take greater diagnostic weight. These signs are a refusal to move, a clinging to a parent, or a loss of a previously acquired motor skill. The developmental history, the trajectory of the motor milestones, and the carer's report of a change from the baseline are the high-yield elements. The vestibular assessment is adapted to the developmental level of the child. The threshold for audiological assessment and for imaging is lower when the history is unreliable or when the examination cannot localise the lesion. [10] [3]
Aboriginal and Torres Strait Indigenous children and those in rural and remote settings may have reduced access to magnetic resonance imaging, paediatric otolaryngology, and audiology. The emphasis therefore falls on the high-yield bedside screen and on the treatable and the preventable causes. The delayed diagnosis of a retrocochlear lesion and of a chronic vestibular hypofunction is a recurring problem where access is limited. This is why a unilateral hearing loss or a persistent imbalance is treated as an indication for transfer and imaging regardless of the distance. The culturally safe consultation involves the family and the local health service in the decision to manage locally or to transfer. [9]
The adolescent with vestibular migraine or with post-concussion positional vertigo faces the compounded burden of the episodes, the school absence, and the restriction from sport. The management addresses the return to learning and to play alongside the symptom control. The post-concussion dizziness is a particular scenario in the adolescent athlete. The recognition and the treatment of the positional vertigo that follows a head injury, together with the gradual return-to-play protocol, restores the participation. The psychosocial impact of a chronic dizziness on a teenager is addressed as part of the multidisciplinary plan. [6] [1]
Evidence, Guidelines & Regional Differences
The international evidence base for dizziness and vertigo in children has converged on clear principles, though it rests more on cohort studies and consensus than on randomised trials for most causes. The consensus diagnostic criteria for vestibular migraine of childhood and recurrent vertigo of childhood, produced jointly by the Bárány Society and the International Headache Society, standardised the diagnosis and are the anchor of the topic. The clinical framework for the paediatric vestibular assessment and the evaluation and the management of paediatric vertigo framed the bedside and the laboratory approach. The review of vertigo and dizziness in children brought the breadth of the causes together. [1] [3]
The evidence for the head impulse, nystagmus, test of skew rule rests on the studies that established its sensitivity for the posterior circulation stroke in the acute vestibular syndrome. The acute vestibular syndrome review by Kerber framed its application. The evidence for vestibular rehabilitation in children rests on the review by Rine and on the clinical experience that early rehabilitation restores the motor milestones and the balance that a vestibular loss impairs. The evidence for positional vertigo in children rests on the series that documented the lower intensity of the paediatric nystagmus and the high rate of a post-traumatic or a post-concussion cause. They confirmed that the Epley manoeuvre is as effective in children as in adults. [7] [5]
The evidence for paediatric Meniere disease rests on the series by Wang and Young. They documented the clinical features and the rarity of the condition in children and emphasised the exclusion of the secondary causes. The evidence for tinnitus in children rests on the review that framed the epidemiology and the management and emphasised the under-recognition and the red-flag patterns. The epidemiology review by Neuhauser framed dizziness and vertigo across the life course and emphasised that the causes shift with age. The regional difference that matters is the selective versus the reflex use of neuroimaging. The consensus across the regions is to observe a benign pattern without routine imaging and to reserve the magnetic resonance imaging for the red flag and the central sign. [8] [9]
Exam Pearls
Diagnose benign paroxysmal vertigo of childhood from the clinical picture. It is a preschool child with sudden, brief, stereotyped episodes of fright and unsteadiness that resolve completely and leave a normal examination, a strong family history of migraine, and an expected resolution before school. Manage it with reassurance and no routine imaging. Diagnose vestibular migraine from the consensus criteria, which are recurrent vertigo lasting five minutes to seventy-two hours with a personal or family history of migraine and migraine features in at least half of the attacks. The single high-yield skill is the head impulse, nystagmus, test of skew rule. It separates a peripheral vestibular neuritis from a posterior circulation stroke through an abnormal head impulse, a unidirectional nystagmus, and no skew for the peripheral cause. [2] [1]
Recognise benign paroxysmal positional vertigo from the brief positional vertigo and the positive Dix-Hallpike with the latent torsional upbeating nystagmus. Treat it with the curative Epley canalith repositioning manoeuvre, particularly after a sports-related concussion. The red-flag screen is the safeguard against the central cause. A focal sign, ataxia between attacks, papilloedema, a new or progressive headache, gaze-evoked or direction-changing nystagmus, a vertical nystagmus, a skew deviation, a normal head impulse in the acute vestibular syndrome, and a unilateral or progressive hearing loss each demand urgent magnetic resonance imaging. Localise the lesion at the bedside. A peripheral lesion gives a unidirectional nystagmus and an abnormal head impulse, while a central lesion gives a direction-changing or gaze-evoked nystagmus and a normal head impulse. [5] [7]
The cardinal pitfalls recur in every examination. The first is the dismissal of a posterior circulation stroke as a benign periodic syndrome through the omission of the head impulse, nystagmus, test of skew rule. The second is the prolonged use of a vestibular suppressant beyond the acute attack, which delays the central compensation. The third is the failure to perform the Epley manoeuvre in a child with positional vertigo. The fourth is the dismissal of a unilateral or progressive hearing loss with tinnitus without imaging for a retrocochlear lesion. The cardinal safeguard is the red-flag screen and the peripheral-versus-central assessment applied to every dizzy child. The management that follows is reassurance for the benign recurrent vertigos, the Epley manoeuvre for positional vertigo, and early vestibular rehabilitation for the acute and the chronic peripheral vestibular loss. [3] [9]
References
- [1]van de Berg R, et al Vestibular Migraine of Childhood and Recurrent Vertigo of Childhood: Diagnostic criteria Consensus document of the Committee for the Classification of Vestibular Disorders of the Bárány Society and the International Headache Society. J Vestib Res, 2021.PMID 33386837
- [2]Gurberg J, et al Benign paroxysmal vertigo of childhood. Handb Clin Neurol, 2023.PMID 38043965
- [3]Peterson JD, Brodsky JR Evaluation and management of paediatric vertigo. Curr Opin Otolaryngol Head Neck Surg, 2022.PMID 36165009
- [4]Jahn K, et al Vertigo and dizziness in children. Curr Opin Neurol, 2015.PMID 25502049
- [5]An JB, et al Pediatric Benign Paroxysmal Positional Vertigo: Degree of Nystagmus and Concurrent Dizziness Differs from Adult BPPV. J Clin Med, 2024.PMID 38610761
- [6]Wang A, et al Benign Paroxysmal Positional Vertigo in Children and Adolescents With Concussion. Sports Health, 2021.PMID 33528343
- [7]Kerber KA Acute Vestibular Syndrome. Semin Neurol, 2020.PMID 31994145
- [8]Wang C, et al Pediatric Meniere's disease. Int J Pediatr Otorhinolaryngol, 2018.PMID 29447806
- [9]Hoare DJ, et al Tinnitus in Children. J Assoc Res Otolaryngol, 2024.PMID 38709437
- [10]Rine RM Vestibular Rehabilitation for Children. Semin Hear, 2018.PMID 30038459
- [11]Beh SC Vestibular Migraine. Curr Neurol Neurosci Rep, 2022.PMID 36044103
- [12]Neuhauser HK The epidemiology of dizziness and vertigo. Handb Clin Neurol, 2016.PMID 27638063