Paeds · fetal-neonatal-and-perinatal
Bilious vomiting and neonatal intestinal obstruction
Also known as Neonatal bowel obstruction · Duodenal atresia · Malrotation with midgut volvulus · Jejunoileal atresia · Meconium ileus · Hirschsprung disease presenting in the newborn
Fellowship guide to bilious vomiting and neonatal intestinal obstruction: why green vomit demands an obstructive and surgical explanation, the proximal-versus-distal causes (duodenal atresia, malrotation with volvulus, jejunoileal atresia, meconium ileus, Hirschsprung disease, anorectal malformation), the resuscitation-first and decompression pathway, the contrast-study decision tree, definitive condition-specific surgery, and the time-critical volvulus trap.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A newborn brings up a green-stained vomit on the postnatal ward. Within minutes the question becomes narrow and urgent: is the bowel obstructed, and if so where? Neonatal intestinal obstruction presenting with bilious vomiting is the clinical syndrome caused by a mechanical blockage of the gut distal to the ampulla of Vater, where bile enters the duodenum. Because bile cannot travel backward past a distal obstruction, its appearance in the vomit is the single most reliable bedside marker that the gut is blocked somewhere downstream. [1] [10]
The obstruction may be intrinsic (atresia, stenosis, web, meconium plug), extrinsic (Ladd bands, annular pancreas), or functional (aganglionosis in Hirschsprung disease). What unifies them is the consequence: proximal bowel distends, peristalsis reverses, and bile-stained gastric and intestinal content is expelled. The clinical challenge is not whether to investigate — every bilious vomit is investigated — but to triage the causes that can kill within hours (midgut volvulus, ischaemia) from those that allow a measured workup (duodenal atresia, Hirschsprung). [5] [10]
The fellowship candidate should hold three frames simultaneously. First, beyond the ampulla — the anatomical reason bile means obstruction. Second, proximal versus distal — proximal obstruction vomits early with little distension, distal obstruction distends and fails to pass meconium. Third, time-critical versus elective — volvulus is a same-hour emergency, duodenal atresia can wait for a planned operation the next day. The management pathway, the imaging choice, and the counselling of parents all flow from holding these three frames. [1] [5]
Epidemiology & Risk Factors
Congenital intestinal obstruction is among the commonest neonatal surgical emergencies, occurring in roughly 1 in 2000 to 1 in 5000 live births, though the exact figure varies by which lesions are counted. Duodenal atresia is the most frequent intrinsic obstruction, jejunoileal atresia is the commonest cause of distal obstruction, and malrotation is the diagnosis that can convert a stable infant into a surgical catastrophe at any time in the first weeks of life. [3] [10]
Risk factors map onto the underlying cause. Duodenal atresia is strongly associated with Down syndrome — roughly a third of infants with duodenal atresia have trisomy 21, and any antenatal finding of polyhydramnios with a double-bubble in a fetus raises the question. Jejunoileal atresia is the legacy of an in-utero mesenteric vascular accident, so it is typically sporadic and isolated. Meconium ileus is the presenting feature of cystic fibrosis in roughly 10–20% of affected neonates, so a distal obstruction with inspissated meconium demands a sweat test or genetic CFTR testing. Hirschsprung disease is more common in males and in Down syndrome, and presents with delayed passage of meconium. Malrotation is a sporadic developmental anomaly that can coexist with gastroschisis, omphalocele, and congenital diaphragmatic hernia. [3] [7] [9]
Antenatal detection increasingly shapes the presentation. Polyhydramnios, a dilated echogenic bowel, or a clearly visible double-bubble on the 20-week anatomy scan or third-trimester growth scan allows planned delivery at a surgical centre, with the paediatric surgical team counselled and present. Infants detected antenatally are typically stable, fasted from birth, and have a decompressing NG tube placed before any feed — a far safer pathway than the infant who obstructs and vomits bile on the postnatal ward at 24 hours. [4] [10]
Pathophysiology
Every cause of neonatal obstruction produces bile-stained vomiting by the same mechanism: the bowel proximal to the blockage distends, peristalsis cannot advance content past the obstruction, and reverse peristalsis delivers bile-stained intestinal content back up through the pylorus and out as vomit. Because bile enters the duodenum at the ampulla of Vater, only an obstruction beyond the ampulla allows bile into the vomit — this is why a bilious vomit is anatomically specific for a distal-duodenal or more distal problem. [1] [10]
The two dominant embryological mechanisms that produce the surgical lesions deserve separate understanding. Intestinal atresia (duodenal, jejunal, ileal) arises from an in-utero event — most often a mesenteric vascular accident such as a volvulus, intussusception, or segmental ischaemia — that causes a segment of bowel to resorb, leaving either a fibrous cord connecting blind-ending proximal and distal segments or, in the most severe forms, a complete gap with a mesenteric defect (the "apple-peel" or "Christmas-tree" variant). The proximal segment dilates chronically against the obstruction in utero and is poorly functional at birth; the distal segment is unused and collapses into the microcolon of distal atresia. [3] [12]
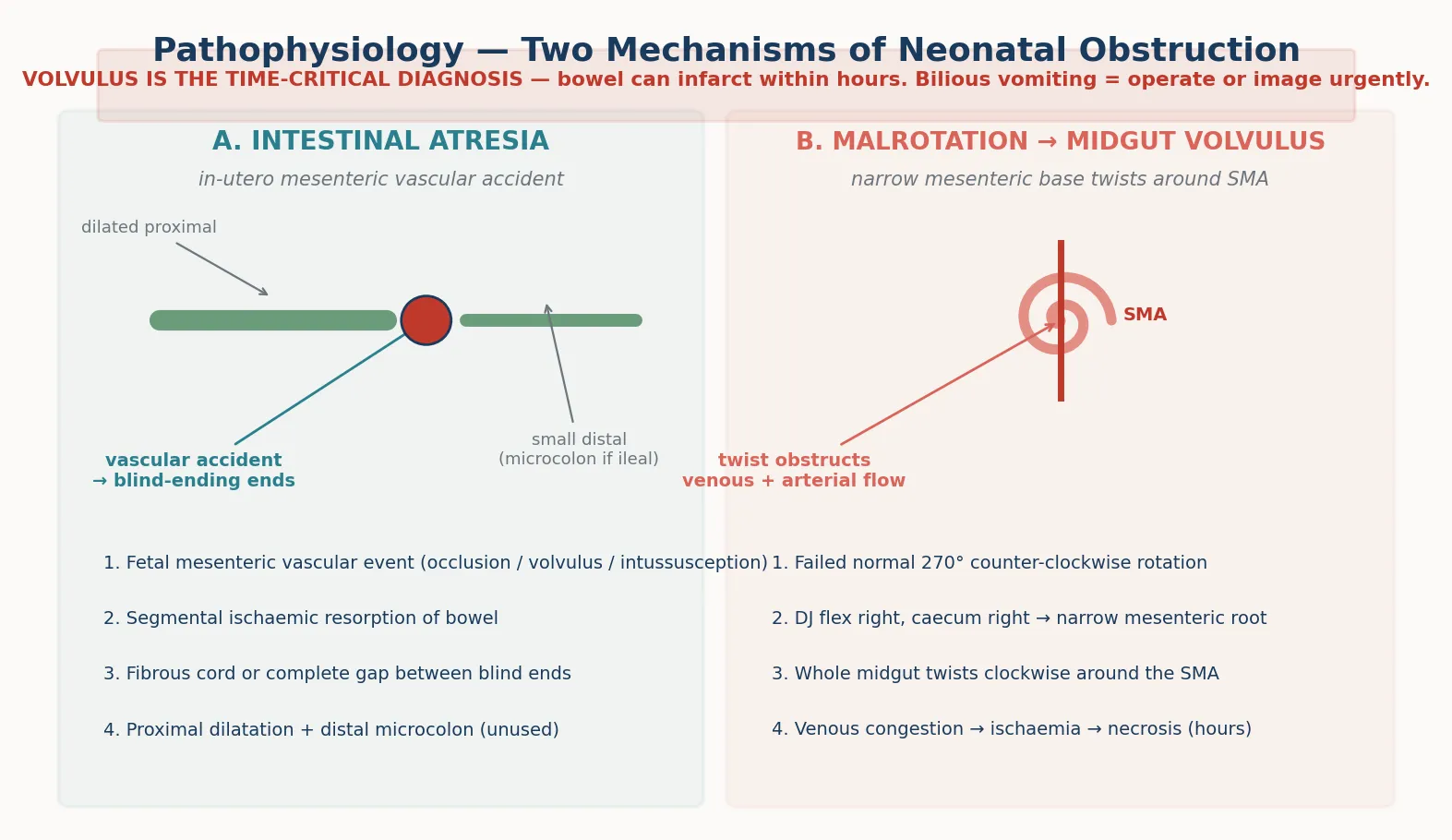
Malrotation with midgut volvulus is the pathophysiology that makes bilious vomiting a same-hour emergency. Normal gut development involves a 270-degree counter-clockwise rotation of the midgut around the superior mesenteric artery during the sixth to tenth weeks of gestation, returning to the abdomen and fixing the duodenojejunal flexure to the left of the spine (ligament of Treitz) and the caecum to the right lower quadrant. When rotation fails, the DJ flexure and caecum both lie on the right, leaving only a narrow mesenteric pedicle carrying the superior mesenteric vessels. The entire midgut can then twist clockwise around this narrow pedicle, kinking first the veins (venous congestion, dark bile) and then the arteries (ischaemia and necrosis). The twist is why a previously well infant suddenly vomits green and can lose the entire midgut within hours. [5] [6]
Hirschsprung disease is a functional obstruction — the aganglionic segment lacks enteric ganglion cells, so it cannot relax and remains tonically contracted, producing a functional blockage at the transition zone with massive proximal dilatation. Meconium ileus is a mechanical-obstructive consequence of abnormally viscous, protein-rich meconium adhering to the ileal mucosa in cystic fibrosis, obstructing the terminal ileum. Each mechanism produces the same downstream effect — proximal distension and bilious vomiting — but the tempo, the imaging, and the surgery differ. [7] [9]
Classification
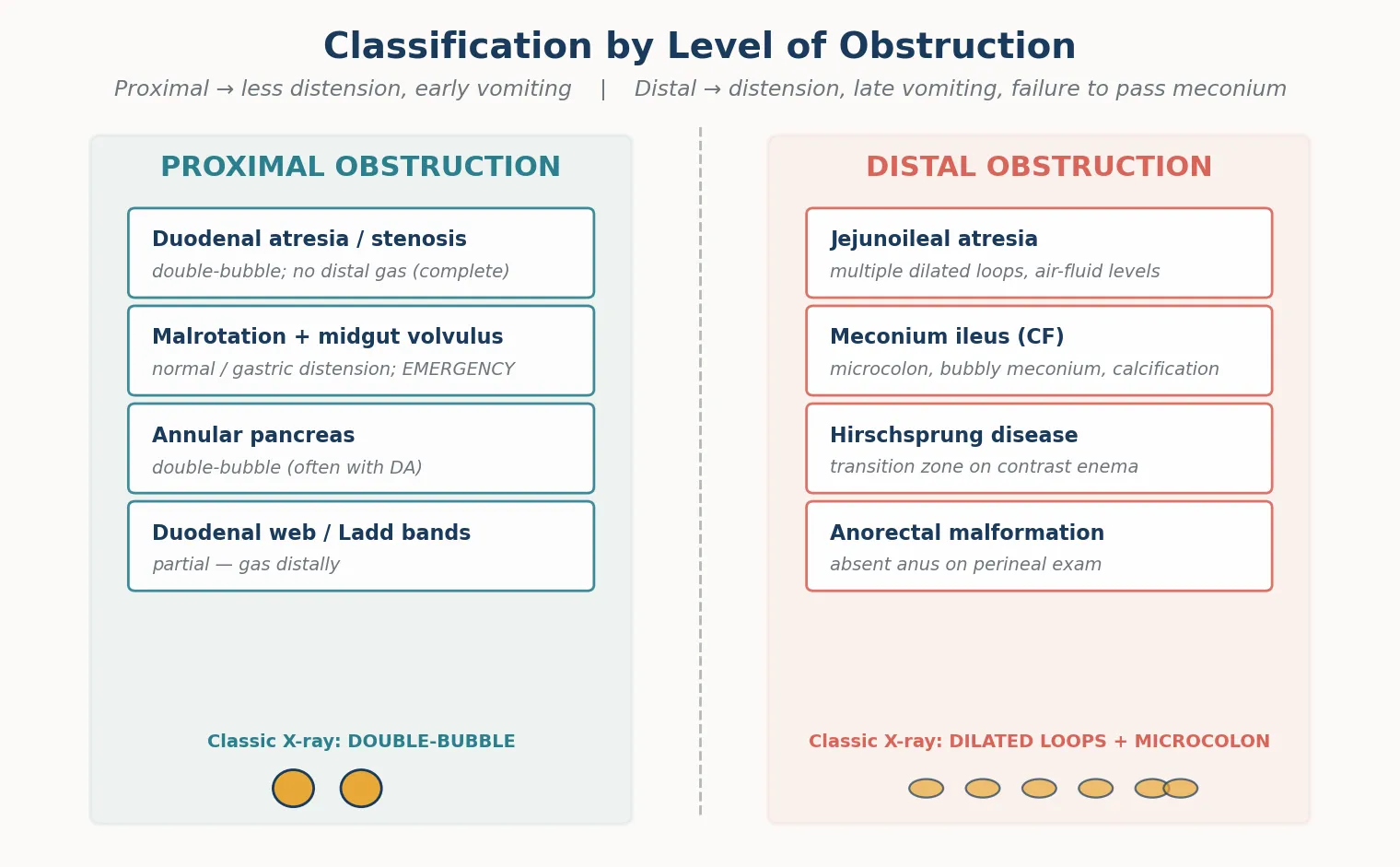
Classifying neonatal obstruction by level (proximal versus distal) is the single most useful scheme, because it predicts the clinical picture, the radiograph pattern, and the choice of contrast study. A proximal obstruction (duodenum or proximal jejunum) presents with early, frequent bilious vomiting and minimal abdominal distension, because only a short segment of bowel lies above the block. A distal obstruction (distal jejunum, ileum, or colon) presents with progressive abdominal distension, later and less frequent vomiting, and characteristically a failure to pass meconium. [10] [11]
Proximal versus distal obstruction
- Early, frequent bilious vomiting
- Minimal or no abdominal distension
- Radiograph: double-bubble (duodenal atresia)
- Upper GI contrast study is the key investigation
- Causes: duodenal atresia, annular pancreas, malrotation with volvulus, duodenal web
- Progressive abdominal distension
- Later, less frequent vomiting
- Failure to pass meconium
- Radiograph: multiple dilated loops, air-fluid levels
- Contrast enema is the key investigation — microcolon, transition zone
- Causes: jejunoileal atresia, meconium ileus, Hirschsprung, anorectal malformation
Within each level, the individual conditions carry their own signatures. Duodenal atresia gives the classic double-bubble — the dilated stomach and proximal duodenum — with no distal gas if the atresia is complete. Malrotation with volvulus may show a relatively normal plain film or only gastric distension, which is precisely why it is dangerous: the radiograph underestimates the emergency. Jejunuoileal atresia shows multiple dilated loops with air-fluid levels. Meconium ileus shows distal obstruction with a characteristic bubbly mass of inspissated meconium in the right lower quadrant, sometimes with intraperitoneal calcification from in-utero perforation. Hirschsprung disease shows a transition zone on contrast enema — a contracted aganglionic segment opening into a dilated ganglionic colon. Anorectal malformation is visible on perineal inspection — no anal opening, or a fistula. [3] [7] [9]
A second classification axis, useful for prognosis and counselling, separates simple obstruction (atresia, web) from ischaemic obstruction (volvulus, necrotising enterocolitis). A simple obstruction can usually be repaired with a single anastomosis and a good outcome; an ischaemic obstruction may leave the infant with short-bowel syndrome, lifelong parenteral nutrition, and intestinal failure. This distinction drives the urgency: the surgeon and the family are not just managing a blockage, they are racing to prevent bowel loss. [5] [10]
Clinical Presentation
The presentation of neonatal obstruction clusters around three findings — bilious vomiting, abdominal distension, and failure to pass meconium — and the combination points to the level. A proximal obstruction presents chiefly with vomiting; a distal obstruction presents chiefly with distension and a meconium delay. The fellowship candidate should elicit all three deliberately, because the pattern is diagnostic before any radiograph. [1] [10]
Bilious vomiting is the cardinal sign. The first vomit may be clear or milky, then turns green or yellow-green as bile accumulates and reverses. The timing matters: duodenal atresia often vomits within the first day of life, while distal obstruction may not vomit bile until 24 to 48 hours as the distal bowel fills. The volume can be large, and the infant dehydrates quickly if the NG tube is not in place. Document the colour explicitly in the notes — "green, bile-stained" — because the surgical referral rests on that word. [1] [2]
Abdominal distension signals a distal obstruction. A proximal obstruction keeps the abdomen flat or scaphoid, because the distal bowel is empty; a distal obstruction fills the loops with gas and meconium, producing a tense, distended abdomen with visible loops and sometimes visible peristalsis. In midgut volvulus with ischaemia the abdomen may be scaphoid early (the bowel is obstructed but empty) then becomes tender and discoloured as infarction develops — a tender, discoloured abdomen with bilious vomiting is a peritonitic volvulus until proven otherwise and is an immediate laparotomy. [5] [10]
Failure to pass meconium is the sign of distal obstruction. Over 90% of term infants pass meconium in the first 24 hours and virtually all by 48 hours. A delayed first stool beyond 48 hours, especially with vomiting and distension, raises Hirschsprung disease, meconium ileus, or a distal atresia. Inspect the perineum for an anorectal malformation at every newborn examination — it is the obstruction you can diagnose without a radiograph. [7] [10]
Differential Diagnosis
The differential diagnosis of bilious vomiting divides into surgical-obstructive causes (the majority), medical causes that mimic obstruction, and non-bilious entities to exclude by the colour test. The surgical-obstructive causes are the six the candidate must hold in ranked order of urgency, because the rank determines the imaging and the operating room. [1] [10]
The ranked surgical differential, from most time-critical to most elective, is: malrotation with midgut volvulus (minutes to hours), necrotising enterocolitis with obstruction (hours to days), duodenal atresia or annular pancreas (day one, stable), jejunoileal atresia (day one to two), meconium ileus (day one to two, with CF), and Hirschsprung disease presenting in the newborn (days). This ranking is the spine of the viva answer: when asked "what could this be?", lead with volvulus because it is the one that kills bowel, then enumerate the rest. [5] [10]
The ranked differential — lead with the time-critical
1. Malrotation with midgut volvulus — the bowel-losing diagnosis; image or operate now
2. Necrotising enterocolitis — obstructive picture with systemic illness, preterm infant
3. Duodenal atresia / annular pancreas — double-bubble, stable, often Down syndrome
4. Jejunoileal atresia — multiple dilated loops, microcolon
5. Meconium ileus — distal obstruction, inspissated meconium, cystic fibrosis
6. Hirschsprung disease — delayed meconium, transition zone, enterocolitis risk
7. Anorectal malformation — absent anus on perineal exam
Medical mimics are fewer but important. Sepsis with ileus can vomit bile and distend, but the infant is systemically unwell with an inflammatory picture and no clear level of obstruction on imaging — though sepsis and NEC can coexist with true obstruction, so do not dismiss a surgical cause in a septic infant. Necrotising enterocolitis produces bilious vomiting, distension, and bloody stools, usually in a preterm infant, and may require surgery for perforation or strictures. Swallowed maternal blood or meconium-stained liquor can colour a vomit brown or dark but not truly green — if there is genuine doubt about the colour, treat it as bilious and image. [10]
The non-bilious entities are excluded by the colour. Pyloric stenosis classically produces projectile non-bilious vomiting at three to six weeks, with a hypochloraemic hypokalaemic metabolic alkalosis — it is not a cause of bilious neonatal vomiting. Gastro-oesophageal reflux and overfeeding produce milky, non-bilient vomits. The discipline of the colour test keeps the candidate anchored: if it is green, it is obstruction until proven otherwise, and the differential is surgical. [1]
Clinical & Bedside Assessment
The bedside assessment of a vomiting newborn is rapid, structured, and oriented toward answering two questions: is this obstruction, and is this infant stable enough to image or do they need the operating room? Begin with the airway, breathing, and circulation, because a dehydrated or shocked obstructed infant can deteriorate while you examine the abdomen. Look for signs of volume depletion — sunken fontanelle, dry mucous membranes, reduced capillary refill, tachycardia, hypotension — and resuscitate in parallel with the assessment, not after it. [10]
Expose the abdomen fully. Inspect for distension, visible loops, surgical scars (or their absence — a gastroschisis or omphalocele is obvious), and abdominal wall discolouration that suggests ischaemia or perforation. Palpate for tenderness, guarding, a palpable mass (a distended loop in atresia, or rarely a pyloric tumour in pyloric stenosis, which is non-bilious), and hernial orifices for an incarcerated inguinal hernia. Auscultate bowel sounds — they may be hyperactive early in obstruction and absent in ileus or peritonitis. A peritonitic, silent, tender abdomen with bilious vomiting mandates immediate surgical review and likely laparotomy. [10]
Inspect the perineum — this is the step candidates forget. Confirm a patent anus in the correct position; an absent, anteriorly placed, or fistulous opening diagnoses an anorectal malformation at the bedside and changes the workup entirely. Examine for the stigmata of associated syndromes: the flat facies and single palmar crease of Down syndrome (duodenal atresia), the features of VACTERL association, and any dysmorphism suggesting a chromosomal anomaly. A complete examination also checks for the cardiac murmurs that may accompany syndromic obstruction. [4] [10]
Establish the feeding and meconium history from the midwife and the chart. When was the first feed, when did vomiting start, what colour, how much? Has meconium been passed, and when? Was there polyhydramnios or an abnormal antenatal scan? The answers sharpen the differential in minutes — a term infant with polyhydramnios, a double-bubble antenatally, and Down syndrome has duodenal atresia on history alone, while a previously well term infant with sudden green vomiting at five days has volvulus until excluded. [1] [5]
Investigations
The investigation sequence is stabilisation first, then imaging, then condition-specific confirmatory tests. The first investigation on every bilious newborn is a plain abdominal radiograph (supine and erect or a lateral decubitus), which is cheap, fast, and immediately informative. The candidate should read it for three features: the gas pattern, the presence of a double-bubble, and signs of perforation (free intraperitoneal air, Rigler's sign). [10] [11]
A double-bubble — two large gas-filled structures in the upper abdomen (the stomach and the dilated proximal duodenum) with no distal bowel gas — is diagnostic of complete duodenal obstruction, most often duodenal atresia, and in a stable infant may be sufficient to proceed to surgery. Multiple dilated loops with air-fluid levels indicate a distal obstruction and prompt a contrast enema. A gasless or near-normal abdomen in a vomiting infant does not exclude obstruction — it is the hallmark of early volvulus, and is the radiograph that must not reassure. [4] [11]
For suspected proximal obstruction or malrotation, the definitive study is the upper gastrointestinal contrast series. It locates the duodenojejunal flexure (the ligament of Treitz): if it lies to the right of the spine or low, malrotation is present, and a corkscrew or "Z-shaped" duodenum suggests volvulus. The study also defines a duodenal web or stenosis. In experienced hands the upper GI series is highly sensitive for malrotation, but interpretation in the neonate requires expertise, and an equivocal study in a sick infant should not delay laparotomy. [6] [5]
For suspected distal obstruction, the contrast enema is the key study. A microcolon (a tiny unused colon) indicates a distal ileal atresia or meconium ileus; a transition zone from a narrow distal segment to a dilated proximal colon indicates Hirschsprung disease; intraluminal filling defects in the terminal ileum suggest meconium ileus, and the water-soluble contrast itself can be therapeutic, dislodging the inspissated meconium. The contrast enema thus serves both diagnostic and, in meconium ileus, therapeutic roles. [11] [9]
Laboratory tests support resuscitation and screen for associated disease. Check capillary or venous blood gas for acid-base status (a metabolic acidosis suggests ischaemia or sepsis), electrolytes and glucose for the dehydration and the refeeding plan, a full blood count and CRP for infection or NEC, and blood group and crossmatch in anticipation of surgery. Send a CFTR genetic test or arrange a sweat test for any infant with meconium ileus. A rectal biopsy confirms Hirschsprung disease by demonstrating absent ganglion cells in the submucosal plexus. [7] [9]
Management — Resuscitation
The resuscitation of a bilious newborn follows the same non-negotiable sequence regardless of the eventual diagnosis: decompress, resuscitate, antibiotics, and refer. The first action is to keep the infant nil by mouth and pass a large-bore (10–12 French) nasogastric tube on free drainage, aspirating and measuring the aspirate regularly. The NG tube relieves the vomiting, reduces the risk of aspiration, decompresses the proximal bowel to make surgery safer, and gives an objective measure of ongoing losses to replace. A small or fine-bore tube will block with intestinal content — use a large-bore tube. [10]
Establish intravenous access — ideally umbilical venous access in a neonate, or peripheral cannulae — and resuscitate with isotonic crystalloid (normal saline or Hartmann's) in 10 mL/kg boluses, reassessing after each, until perfusion is restored. Correct hypoglycaemia with a dextrose infusion, and check and correct electrolytes, because vomiting and NG losses deplete sodium, potassium, and chloride rapidly. Replace ongoing NG aspirate volume millilitre-for-millilitre with an appropriate replacement fluid, and chart inputs and outputs meticulously. [10]
Start broad-spectrum antibiotics — for example a combination covering gram-negative and anaerobic organisms, such as ampicillin, gentamicin, and metronidazole, per local neonatal protocol — because ischaemia, NEC, and perforation are differential possibilities and because surgery is imminent. Give analgesia, maintain normothermia, and monitor the infant in a neonatal unit or retrieval environment. If the infant is being transferred to a surgical centre, stabilise fully before retrieval and send the images and the history with the team. [10]
Management — Definitive & Stepwise
Once stabilised and imaged, definitive management is condition-specific and surgical, because the obstruction is anatomical and requires operative correction in almost every case. The surgeon's choice of operation depends on the cause, the state of the bowel, and associated anomalies, and the paediatric team's role is to support the operation with optimal resuscitation, monitoring, and family communication. [3] [10]
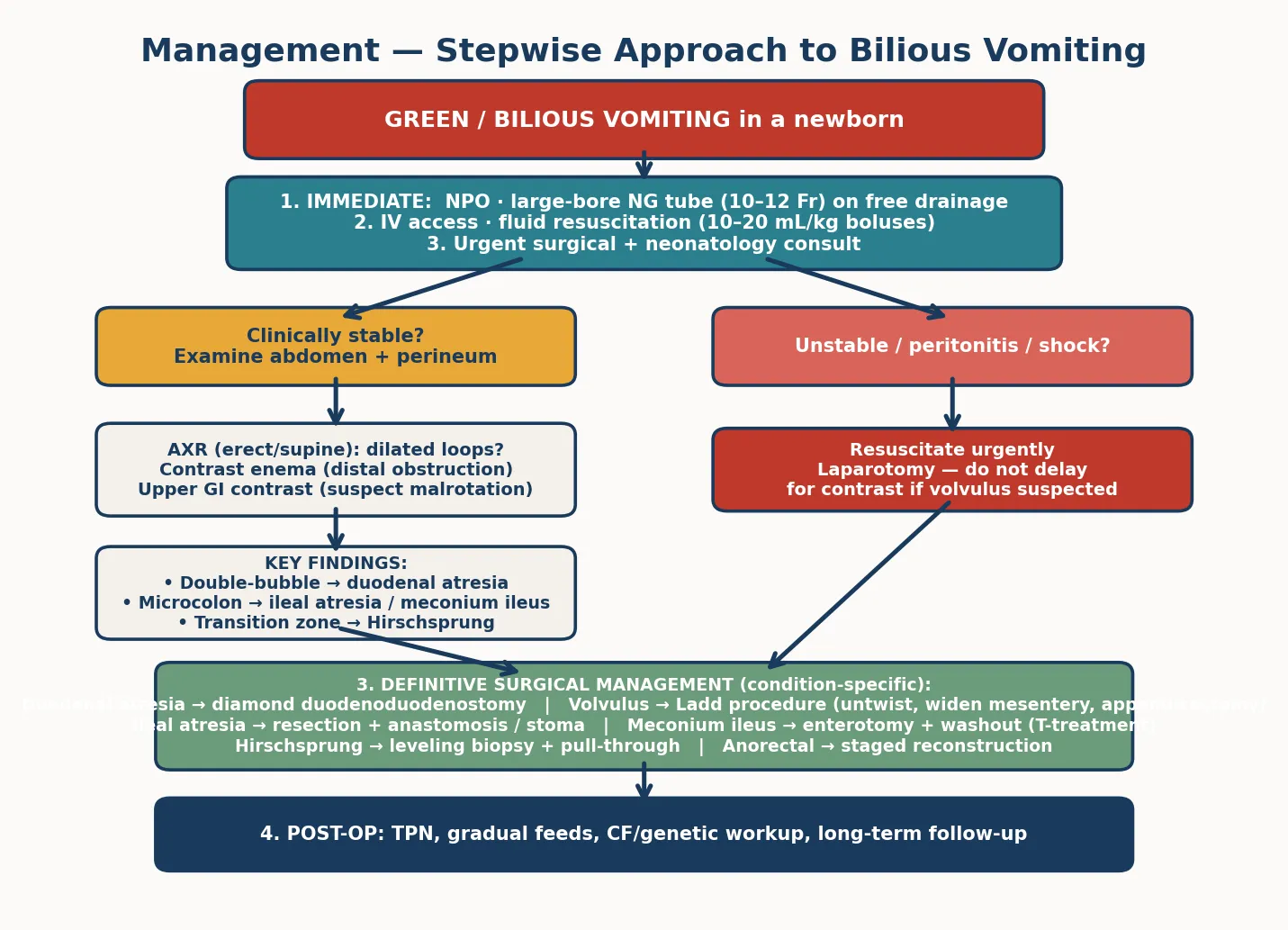
Duodenal atresia and annular pancreas are repaired with a diamond-shaped duodenoduodenostomy (the Kimura procedure), bypassing the obstruction with an anastomosis between the proximal and distal duodenum; an annular pancreas is never divided but bypassed. The operation is typically performed on day two or three once stabilised, and outcomes are excellent in the absence of major cardiac anomalies. [4] [13]
Malrotation with volvulus requires an emergency Ladd procedure: untwist the volvulus (counter-clockwise), divide the Ladd bands, widen the mesenteric base by laying the bowel out in non-rotation, resect any non-viable bowel, and perform an appendicectomy (because the caecum will now lie on the left, making future appendicitis a diagnostic trap). The aim is both to save bowel and to prevent recurrence. The amount of bowel lost dictates the long-term outlook — the difference between a normal life and short-bowel syndrome. [5]
Jejunoileal atresia is repaired by resecting the dilated, poorly functional proximal segment to a calibre-matched point, and performing a primary end-to-end anastomosis, or fashioning a stoma if the bowel is compromised or the infant unstable. The "apple-peel" variant with a large mesenteric defect and limited distal bowel carries a higher risk of short gut. Meconium ileus is managed initially with a therapeutic water-soluble contrast enema to dislodge the inspissated meconium; if that fails, or if there is perforation or complex obstruction, the surgeon performs an enterotomy with washout or a stoma (the Bishop-Koop technique). [3] [9]
Hirschsprung disease is managed in stages: a levelling suction rectal biopsy confirms the diagnosis and the transition zone, an initial diverting colostomy or a primary pull-through is performed depending on the centre and the infant, and definitive pull-through surgery brings the ganglionic bowel down to the anus. The major danger is Hirschsprung-associated enterocolitis, which can be life-threatening and requires prompt recognition with rectal washouts and antibiotics. Anorectal malformation is managed with a staged reconstruction — a colostomy in the neonatal period, then a definitive posterior sagittal anorectoplasty — though some centres perform a primary procedure in selected low lesions. [7] [8]
Specific Subtypes & Scenarios
Each major cause has a specific scenario the fellowship candidate must be able to walk through, because the long case and the OSCE will test depth on at least one. The high-yield subtypes are duodenal atresia (the double-bubble), malrotation with volvulus (the emergency), meconium ileus (the CF link), and Hirschsprung disease (the delayed meconium). [10]
Duodenal atresia is the antenatal-to-postnatal scenario. Polyhydramnios and a double-bubble on antenatal ultrasound prompt counselling about the association with Down syndrome and planned delivery at a surgical centre. At birth the infant is kept nil by mouth with an NG tube; a plain film showing the double-bubble confirms the diagnosis, and a diamond duodenoduodenostomy is performed on day two or three. Cardiac anomalies (most often an endocardial cushion defect) and the trisomy 21 itself shape the perioperative risk, and the long-term outcome is good in the absence of major cardiac disease. [4]
Malrotation with volvulus is the scenario where minutes matter. A previously well term infant, often days old, suddenly vomits green and becomes listless; the abdomen may be scaphoid early, then tender. A normal or near-normal plain film does not exclude it. The upper GI series shows the malpositioned ligament of Treitz or the corkscrew duodenum, but a sick infant goes straight to theatre for the Ladd procedure. The family must be counselled that the amount of bowel salvaged determines whether the child will have a normal gut or require lifelong parenteral nutrition. [5] [6]
Hirschsprung disease presents with delayed passage of meconium beyond 48 hours, abdominal distension, and bilious vomiting, and carries the specific danger of Hirschsprung-associated enterocolitis — acute colitis with fever, distension, and bloody diarrhoea that can progress to toxic megacolon, perforation, and death. Enterocolitis is prevented and treated by rectal washouts and decompression, and the diagnosis is confirmed by rectal biopsy showing aganglionosis. The pull-through brings ganglionic bowel to the anus, and long-term outcomes are good, though soiling and enterocolitis can persist. [7] [8]
The annular pancreas scenario usually presents as duodenal obstruction with a double-bubble and is discovered at surgery; the pancreatic ring is never divided (division risks fistula and pancreatitis) but bypassed with a duodenoduodenostomy. Jejunoileal atresia presents with distal obstruction and multiple dilated loops, and the surgeon resects the dilated proximal bulb to improve function — leaving a dilated, poorly peristaltic segment causes persistent dysmotility. [3] [13]
Complications & Pitfalls
The complications of neonatal obstruction divide into those of the disease (bowel loss, perforation, sepsis) and those of the management (fluid and electrolyte disturbance, line and NG complications, anaesthetic and surgical morbidity). The single gravest complication is midgut ischaemia and short-bowel syndrome from delayed diagnosis of volvulus, which converts a curable obstruction into lifelong intestinal failure requiring parenteral nutrition and often small-bowel transplantation. This is the complication every minute of delay risks. [5] [10]
The pitfalls that lose bowel — delay, reassurance, and the wrong study
Fluid and electrolyte disturbance is common and dangerous. Vigorous NG losses deplete sodium, potassium, and chloride, producing a hypochloraemic, hypokalaemic metabolic alkalosis (the mirror image of pyloric stenosis, though the obstruction is distal), while resuscitation can over-shoot. Chart NG aspirate and replace it millilitre-for-millilitre, check electrolytes every six to twelve hours, and avoid hypoglycaemia with a dextrose-containing maintenance regimen. [10]
The specific surgical pitfalls include anastomotic leak and stricture after atresia repair, recurrent volvulus or internal hernia after an incomplete Ladd procedure, and enterocolitis after Hirschsprung pull-through. A missed second atresia (the "string of beads" with multiple sequential atresias) causes persistent postoperative obstruction, so the surgeon inspects the entire bowel at laparotomy. Postoperatively, prolonged ileus, adhesions, and the risk of future small-bowel obstruction persist throughout childhood. [3] [8]
Prognosis & Disposition
Prognosis is driven by the cause, the amount of bowel lost, and the associated anomalies. Duodenal atresia repaired electively has an excellent prognosis, with near-normal long-term gastrointestinal function, and outcome is governed chiefly by the cardiac and chromosomal associations. Jejunoileal atresia has a good outcome when a primary anastomosis is possible, though the apple-peel variant and short remaining bowel carry a short-gut risk. [3] [4]
Malrotation corrected by a complete Ladd procedure before ischaemia has an excellent prognosis; once bowel is lost, the prognosis tracks the length of residual bowel and the adequacy of absorption. Infants with short-bowel syndrome require long-term parenteral nutrition, gradual intestinal adaptation, and centres with intestinal-failure expertise. The disposition for any surgically corrected obstruction is a tertiary neonatal surgical centre with access to paediatric surgery, neonatology, nutrition, and long-term follow-up. [5]
Hirschsprung disease has a good functional outcome after pull-through, though soiling, enterocolitis, and constipation can persist into childhood and require ongoing surgical and continence input. Meconium ileus links directly to the cystic-fibrosis trajectory, so long-term prognosis is shaped by the pulmonary and pancreatic disease of CF as much as by the bowel. Every infant with meconium ileus enters the CF pathway with a multidisciplinary team. [7] [9]
Special Populations
Several populations require a modified approach to neonatal obstruction. The antenatally diagnosed infant is the model of best practice — delivery at a surgical centre, the team forewarned, an NG tube placed before the first feed, and planned surgery — and the candidate should contrast this with the higher-risk postnatal presentation. Antenatal counselling of parents about a double-bubble or echogenic bowel is a communication-skill station in its own right. [4]
Down syndrome infants are over-represented in duodenal atresia and Hirschsprung disease, and the cardiac anomalies that accompany trisomy 21 shape both the anaesthetic risk and the long-term outcome. The workup of a Down syndrome infant with bilious vomiting must include an echocardiogram and a karyotype confirmation, and the surgery is planned around the cardiac status. [4]
The preterm infant with obstruction raises necrotising enterocolitis as a leading differential, and the management blends medical NEC treatment with surgical decision-making for perforation or stricture. Preterm infants tolerate fluid shifts and surgery less well, and the threshold for involving the surgical team is lower. Rural and remote infants who obstruct far from a surgical centre depend on a retrieval service and pre-transfer stabilisation, and the candidate should be able to articulate the retrieval principles — NG decompression, IV access, fluids, antibiotics, and a stable infant handed to the retrieval team with the images. [10]
The family facing short-bowel syndrome after volvulus enters a long trajectory of parenteral nutrition, intestinal rehabilitation, and possibly transplantation, and the paediatric team's role extends well beyond the neonatal period into nutritional, developmental, and psychosocial support. This is the population for whom a delay of an hour at the outset changes a lifetime. [5]
Evidence, Guidelines & Regional Differences
The evidence base for neonatal obstruction is largely surgical series and expert consensus rather than randomised trials, because the conditions are individually uncommon and the surgical management is well established. The seminal series of 277 intestinal atresias defined the classification, the surgical principles, and the outcomes that still guide practice, and modern single-centre and multicentre series have refined survival to over 90% for most atresias in developed settings. [3] [10]
Regional differences centre on antenatal detection, place of delivery, and access to paediatric surgical expertise. In Australia and New Zealand, a tiered network of surgical centres with retrieval services ensures that most infants are transferred safely, and antenatal detection allows planned delivery at a tertiary centre. The RACP and RCPCH curricula emphasise the recognition and stabilisation of the surgical newborn as a core competency, and the surgical society guidelines (for example, those of the Australian and New Zealand Association of Paediatric Surgeons) guide practice. [1] [10]
Controversies include the timing of primary anastomosis versus stoma in jejunoileal atresia, the role of laparoscopic versus open Ladd procedure, the choice of primary pull-through versus staged repair in Hirschsprung disease, and the utility of the upper GI series in asymptomatic malrotation picked up incidentally. These are decisions for the surgical team, but the paediatric candidate should know the principles and the evidence on both sides. The role of therapeutic contrast enema in meconium ileus is well supported by the CF foundation consensus guidelines. [4] [9]
Exam Pearls
The single highest-yield fact for this topic is the rule itself: bilious vomiting in a newborn is obstruction until proven otherwise, and it is a surgical problem. Lead every answer with this statement, then build the differential from the time-critical (volvulus) to the elective (duodenal atresia, Hirschsprung). The colour test, the proximal-versus-distal split, and the imaging choice (upper GI series for proximal, contrast enema for distal) are the three frameworks that structure any viva or short case. [1] [10]
For the written exam, the high-yield associations are duodenal atresia with Down syndrome and the double-bubble, meconium ileus with cystic fibrosis, Hirschsprung with delayed meconium and a transition zone, and malrotation with the Ladd procedure and appendicectomy. Know the embryology of midgut rotation — the 270-degree counter-clockwise turn and the narrow mesenteric pedicle that predisposes to volvulus — because it is a favourite mechanism question. [5] [4]
For the clinical and communication stations, the discriminating behaviours are: recognising the colour and acting on it, placing the NG tube before requesting imaging, resuscitating in parallel, and knowing when to send the unstable infant to theatre without waiting for contrast. In the communication station around volvulus, the candidate must be honest about the bowel-loss risk without abandoning hope, and must keep the family informed as the situation evolves. The candidate who waits for a radiograph in a peritonitic infant fails the station; the candidate who decompresses, resuscitates, and calls surgery immediately passes with distinction. [5] [2]
References
- [1]Godbole P, Stringer MD Bilious vomiting in the newborn: How often is it pathologic? J Pediatr Surg, 2002.PMID 12037761
- [2]Lee RA, Dassios T, Bhat R Bilious Vomiting in the Newborn: A Three-Year Experience in a Tertiary Medical and Surgical Centre. Case Rep Pediatr, 2020.PMID 33110665
- [3]Dalla Vecchia LK, Grosfeld JL, West KW Intestinal atresia and stenosis: a 25-year experience with 277 cases. Arch Surg, 1998.PMID 9605910
- [4]Patterson KN, Cruz S, Nwomeh BC Congenital duodenal obstruction - Advances in diagnosis, surgical management, and associated controversies. Semin Pediatr Surg, 2022.PMID 35305801
- [5]Svetanoff WJ, Srivatsa S, Diefenbach K Diagnosis and management of intestinal rotational abnormalities with or without volvulus in the pediatric population. Semin Pediatr Surg, 2022.PMID 35305800
- [6]Birajdar S, Rao SC, Bettenay F Role of upper gastrointestinal contrast studies for suspected malrotation in neonatal population. J Paediatr Child Health, 2017.PMID 28425590
- [7]Haricharan RN, Georgeson KE Hirschsprung disease. Semin Pediatr Surg, 2008.PMID 19019295
- [8]Short SS, Durham MM, Rollins MD Hirschsprung disease outcomes. Semin Pediatr Surg, 2022.PMID 35690462
- [9]Sathe M, Houwen R Meconium ileus in Cystic Fibrosis. J Cyst Fibros, 2017.PMID 28986020
- [10]Hajivassiliou CA Intestinal obstruction in neonatal/pediatric surgery. Semin Pediatr Surg, 2003.PMID 14655163
- [11]Baad M, Delgado J, Dayneka JS Diagnostic performance and role of the contrast enema for low intestinal obstruction in neonates. Pediatr Surg Int, 2020.PMID 32572600
- [12]Ziegler MM Meconium ileus. Curr Probl Surg, 1994.PMID 8062591
- [13]Ali Almoamin HH, Kadhem SH, Saleh AM Annular pancreas in neonates; Case series and review of literatures. Afr J Paediatr Surg, 2022.PMID 35017379
- [14]Tobias J, Tillotson M, Maloney L Meconium Ileus, Distal Intestinal Obstruction Syndrome, and Other Gastrointestinal Pathology in the Cystic Fibrosis Patient. Surg Clin North Am, 2022.PMID 36209752