Paeds · fetal-neonatal-and-perinatal
Birth trauma and brachial plexus injury
Also known as Birth trauma and brachial plexus injury · Obstetric brachial plexus injury · Neonatal brachial plexus palsy · Erb's palsy and Klumpke's palsy · Birth injury
Fellowship guide to birth trauma and brachial plexus injury: the full spectrum from soft-tissue and skeletal injuries to the Narakas-graded nerve lesion, the mechanism of traction injury, the 3-month biceps-recovery threshold for microsurgical referral, and the secondary musculoskeletal procedures for residual deficits.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Birth trauma is the physical injury a newborn sustains during the mechanical forces of labour and delivery. It spans the gamut from trivial soft-tissue bruising and clavicular fracture to the devastating neurological injuries that shape a child's lifetime function — and the most important of these, because of its frequency and its treatability, is brachial plexus birth injury (BPBI). A newborn who holds one arm adducted, internally rotated, and pronate at the side with the wrist flexed — the so-called waiter's-tip posture — has an upper-trunk (Erb-Duchenne) palsy until proven otherwise. [1] [2]
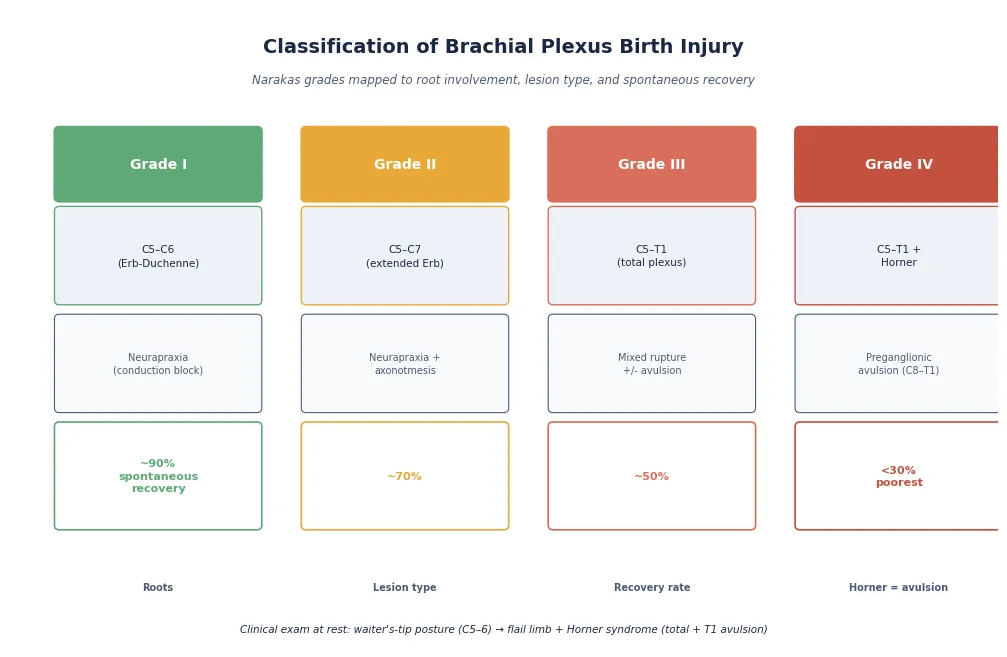
Brachial plexus birth injury is the traction injury of the C5–T1 nerve roots sustained when the head and neck are forced laterally away from the shoulder during delivery. It is not a single disease but a spectrum, graded by the Narakas system from a mild conduction-block neurapraxia (grade I, near-complete recovery) to a total-plexus injury with preganglionic root avulsion and Horner syndrome (grade IV, the poorest outcome). The decisive clinical task is not the diagnosis at birth — the posture makes it obvious — but the disciplined monthly tracking of recovery, because the absence of biceps recovery by three months is the threshold that separates the infants who will recover spontaneously from those who need microsurgical nerve reconstruction. [2] [3]
Classification
Birth trauma is classified first by the tissue system injured, then — for brachial plexus injuries specifically — by the Narakas grade, which integrates root involvement, lesion severity, and expected recovery into a single prognostic framework. The tissue-system classification matters because it directs the immediate newborn assessment: skeletal injuries (clavicle fracture is the most common), soft-tissue injuries (cephalohaematoma, subgaleal haemorrhage, bruising), neurological injuries (brachial plexus, facial nerve, phrenic nerve, spinal cord), and visceral injuries (adrenal, liver, or splenic haemorrhage). [6]
The Narakas classification, the workhorse for BPBI, grades the injury from I to IV. Grade I (C5–6, Erb-Duchenne) is a neurapraxia with near-complete spontaneous recovery. Grade II (C5–7, extended Erb) combines neurapraxia and axonotmesis with good but incomplete recovery. Grade III (C5–T1, total plexus) involves mixed rupture and avulsion with moderate recovery. Grade IV (C5–T1 with Horner syndrome) is dominated by preganglionic avulsion, carries the poorest prognosis, and is distinguished at the bedside by ptosis, miosis, and anhidrosis on the affected side — a finding that signals T1 root avulsion the moment the newborn is examined. [2] [9]
Epidemiology & Risk Factors
Brachial plexus birth injury affects roughly 1.5 per 1000 live births in high-income settings, making it the most common focal neurological birth injury. The incidence has declined modestly over recent decades, attributed to improved obstetric practice, but it remains a persistent and clinically significant problem — and in many cases, no risk factor is identifiable, which means the absence of a risk factor never excludes the diagnosis. [1]
The dominant risk factor, by an overwhelming margin, is shoulder dystocia — the impaction of the anterior shoulder behind the pubic symphysis after the head has delivered — which multiplies the risk of BPBI roughly a hundredfold. Macrosomia (birthweight above 4.5 kg) increases the risk fourteenfold, and instrumental delivery with forceps ninefold. Other contributors include prolonged second stage of labour, malposition (occiput-posterior), maternal diabetes (which drives fetal macrosomia), and a history of shoulder dystocia in a previous pregnancy. Breech presentation produces a different mechanism — direct traction on the arm rather than head–neck distraction — and is associated with lower-trunk and total-plexus injuries. [1] [7]
A crucial and often underappreciated epidemiological fact: over half of infants with BPBI have no identifiable risk factor. This means the injury is not exclusively a consequence of excessive traction or poor obstetric technique — it reflects the interaction of fetal positioning, tissue vulnerability, and intrapartum mechanics that cannot always be predicted or prevented. Elective caesarean delivery is protective but does not eliminate the risk entirely. [1] [7]
Pathophysiology
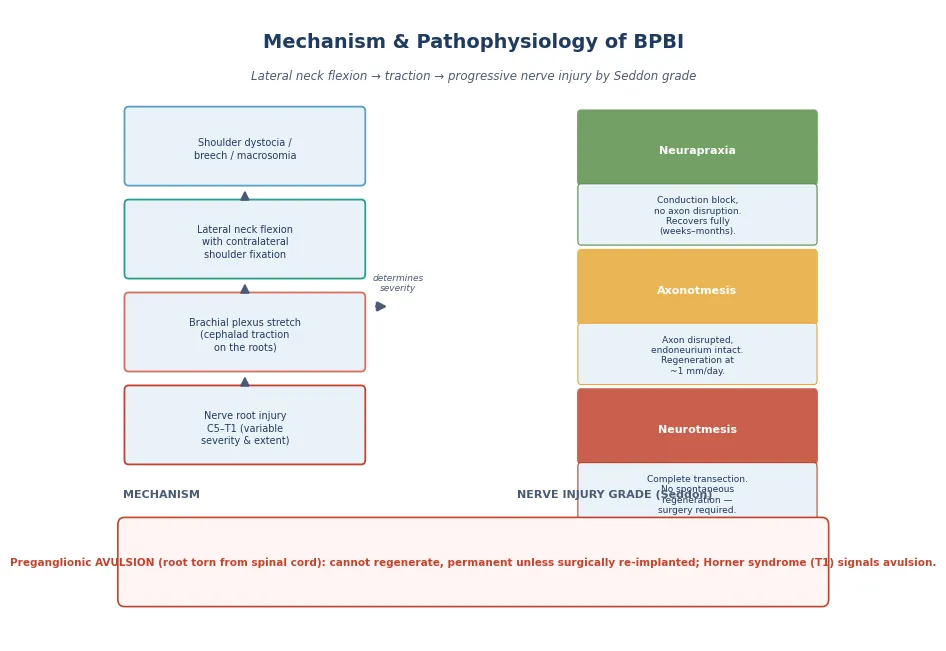
The brachial plexus is formed by the ventral rami of C5 through T1. During a vertex delivery complicated by shoulder dystocia, the head delivers but the anterior shoulder impacts behind the pubic symphysis; the subsequent downward traction on the head creates lateral flexion of the neck away from the impacted shoulder, stretching the contralateral brachial plexus — most often the upper trunk (C5–6). In a breech delivery, the mechanism is reversed: the arms are elevated above the head, and traction on the body stretches the lower trunk and the posterior cord. The severity of the stretch determines the lesion grade. [2]
The nerve injury follows the Seddon classification of nerve damage. Neurapraxia — a conduction block without axonal disruption — is the mildest grade and recovers fully within weeks to months as the myelin sheath remyelinates. Axonotmesis — disruption of the axon with preservation of the endoneurial tube — allows axonal regeneration at approximately one millimetre per day, but recovery is slow and incomplete because regeneration may be misdirected. Neurotmesis — complete transection of the nerve including its connective tissue sheath — precludes spontaneous regeneration entirely and requires surgical intervention. When the injury is preganglionic, meaning the nerve root is avulsed from the spinal cord, no regeneration is possible at all: the motor neurons in the anterior horn are disconnected from the peripheral nerve, and only surgical re-implantation or nerve transfer can restore any function. [2] [9]
Axonal regeneration follows a strict timeline: the regenerating axon advances at roughly one millimetre per day (approximately one inch per month), and the further the target muscle from the injury site, the longer the regeneration takes and the more likely the motor endplate will have degenerated beyond the point of reinnervation. This is the physiological basis of the 3-month surgical threshold: the muscles nearest to the plexus — particularly the biceps (elbow flexion, C5–6) — are the first to receive regenerating axons. If they have not recovered by three months, the more distant muscles (hand intrinsics) will almost certainly not recover, and surgical reconstruction is needed to bypass the damaged segment. [4] [9]
Clinical Presentation
The newborn with a brachial plexus injury is identified on the routine newborn examination by an abnormal arm posture. The classic upper-trunk (Erb-Duchenne) posture is unmistakable: the affected arm lies adducted and internally rotated at the shoulder, extended at the elbow, pronated at the forearm, and flexed at the wrist and fingers — the waiter's-tip or port-wine posture. The Moro reflex is asymmetric (absent on the affected side), and spontaneous movement of the shoulder and elbow is reduced or absent. The hand and wrist may move normally if the lower trunk is spared. [2] [6]
The total-plexus injury presents with a flail limb — no movement from shoulder to fingers — and may include Horner syndrome (ptosis, miosis, anhidrosis) on the affected side when T1 is avulsed. The lower-trunk (Klumpke) injury in isolation is uncommon but presents with a flaccid hand and wrist while the shoulder and elbow retain some function — the grasping reflex may be absent. Bilateral injuries, though rare, raise the possibility of a breech mechanism or a cervical spinal cord injury. [2]
Other birth injuries present alongside BPBI or independently. Clavicular fracture — the most common skeletal birth injury — presents with asymmetrical Moro, localised crepitus, and reduced arm movement, and it frequently coexists with BPBI. Facial nerve palsy presents with asymmetrical crying and a flattened nasolabial fold, typically on the side of forceps application. Phrenic nerve palsy (C3–5) presents with respiratory distress and an elevated hemidiaphragm on chest radiograph. Cephalohaematoma and subgaleal haemorrhage present with scalp swellings of distinct boundaries and different risks. [6]
Differential Diagnosis
The differential diagnosis of a newborn with a weak or immobile arm extends beyond brachial plexus injury to several conditions that mimic or coexist with it. The clinical task is to distinguish the treatable focal nerve injury from the conditions that require a different pathway — particularly the cervical spinal cord injury, which is devastating and easily missed when attention fixates on the arm. [6]
Clavicular fracture is the most common mimic and the most common coexisting injury. It presents with the same reduced arm movement and asymmetric Moro as BPBI, but the lesion is bony: palpation reveals crepitus, angulation, or a palpable callus after a week. Because the two injuries coexist in a significant minority of cases, a newborn with a suspected BPBI should have the clavicle palpated and, if doubt remains, a radiograph obtained. [6]
Cervical spinal cord injury is the critical differential that must not be missed. It presents with a flaccid arm (or arms), but unlike BPBI it is accompanied by signs beyond the brachial plexus distribution: hypotonia of the legs, apnoea or respiratory distress, bulbar weakness, and absent reflexes below the lesion. A newborn with an injured arm who is also floppy, apnoeic, or has poor suck and swallow does not have an isolated BPBI — and urgent MRI of the cervical spine is mandatory. Other mimics include humeral fracture (painful, swollen upper arm), osteomyelitis or septic arthritis (fever, systemic signs), and congenital limb anomalies. [6]
[6]Clinical & Bedside Assessment
Bedside assessment has two purposes: to confirm the diagnosis and grade the injury at birth, and to track recovery monthly so the 3-month threshold decision is made on objective data. The initial examination is part of the routine newborn check. The clinician observes the resting posture (the waiter's-tip or flail-limb pattern), elicits the Moro reflex to demonstrate the asymmetry, palpates the clavicle to exclude fracture, auscultates the chest for asymmetrical breath sounds (phrenic nerve), and examines the face (facial nerve) and the eyes (Horner syndrome). The affected limb is examined for tone, spontaneous movement, and the presence of any antigravity movement in each joint. [2] [6]
The Active Movement Scale (AMS) is the standard tool for serial assessment. It grades each joint movement (shoulder flexion, abduction, external and internal rotation; elbow flexion and extension; forearm pronation and supination; wrist and finger extension and flexion; thumb extension) on a scale from 0 (no contraction) to 7 (full movement against gravity and resistance). The AMS is performed monthly from the first outpatient visit, and the biceps (elbow flexion) score is the single most important item — because antigravity elbow flexion (AMS 5 or above) by three months is the predictor of spontaneous recovery. [2]
The Toronto Test Score provides a structured threshold for surgical referral. It scores elbow flexion, elbow extension, wrist extension, finger extension, and thumb extension on a 0-to-2 scale (0 absent, 1 diminished, 2 normal) for a maximum of 10 points. A score below 3.5 at three months predicts poor spontaneous recovery and triggers microsurgical referral. The score is combined with the clinical picture — the presence of Horner syndrome or a total-plexus pattern from the outset lowers the threshold for early referral, because these infants have a high probability of avulsion that will not recover. [2] [4]
Investigations
Investigations in birth trauma serve three purposes: to confirm or exclude the coexisting injuries (clavicle fracture, phrenic nerve palsy), to identify the mimics (cervical spinal cord injury), and — in selected cases — to define the nerve lesion anatomy for surgical planning. Most investigations are reserved for the atypical or non-recovering case; the straightforward upper-trunk injury recovering on schedule needs no imaging at all. [2] [6]
The immediate investigations, when the clinical picture is not straightforward, include a chest radiograph (for clavicular fracture, rib fractures, and elevated hemidiaphragm), and — when cervical spinal cord injury is suspected — an urgent MRI of the cervical spine. Ultrasound of the shoulder, increasingly used in follow-up, assesses glenohumeral joint congruity and detects the posterior glenoid dysplasia and humeral head flattening that develop in non-recovering injuries. For surgical planning, MRI of the brachial plexus (with MR neurography) and, in some centres, CT myelography define the pseudomeningocoeles that signal root avulsion, and electrodiagnostic studies (nerve conduction and electromyography) help distinguish preganglionic avulsion from postganglionic rupture. [2] [5]
The shoulder ultrasound and MRI become important in the longer-term follow-up of non-recovering or partially recovering injuries. The Waters classification of glenohumeral dysplasia — from a normal glenoid (grade I) through posterior subluxation (grade II–III) to a severely deformed pseudoglenoid (grade IV–V) — guides the decision for secondary musculoskeletal procedures such as arthroscopic reduction or external rotation osteotomy. These imaging modalities are not part of the newborn work-up; they belong to the specialist surveillance of the child whose recovery is incomplete. [5]
Management — Resuscitation
The immediate management of a newborn with a birth injury is protection. The affected arm is immobilised gently across the chest for the first one to two weeks — not rigidly splinted, which risks contracture, but rested in a position that avoids further traction on the injured plexus. The newborn is assessed for the coexisting injuries that alter the immediate plan: a chest radiograph excludes phrenic nerve palsy and clavicular fracture; the face and eyes are examined for facial nerve palsy and Horner syndrome; and any signs beyond the arm (apnoea, leg hypotonia, bulbar weakness) trigger urgent cervical spine imaging. [6]
The principle of the first weeks is to avoid harm while awaiting the recovery trajectory. Passive range-of-motion exercises of the shoulder, elbow, and wrist — gentle and within pain limits — begin after the first week to prevent contracture, particularly internal rotation and adduction contractures of the shoulder. The parents are taught these exercises by a physiotherapist, because daily maintenance of joint mobility is the foundation of the conservative phase and the prerequisite for good surgical outcomes if surgery is later needed. [2]
Immediate management of the newborn with a birth injury
Confirm diagnosis and grade: observe posture, elicit Moro, palpate clavicle, examine face and eyes
Immobilise the affected arm gently across the chest for 1–2 weeks — no rigid splinting
Chest radiograph: exclude clavicle fracture, rib fracture, elevated hemidiaphragm (phrenic)
Examine for Horner syndrome (ptosis, miosis, anhidrosis) — signals T1 avulsion, grade IV
If any sign beyond the arm (apnoea, leg hypotonia, bulbar) — urgent cervical spine MRI
Begin gentle passive range-of-motion exercises after week 1, taught by physiotherapist
Schedule first outpatient review at 2–4 weeks with Active Movement Scale assessment
Management — Definitive & Stepwise
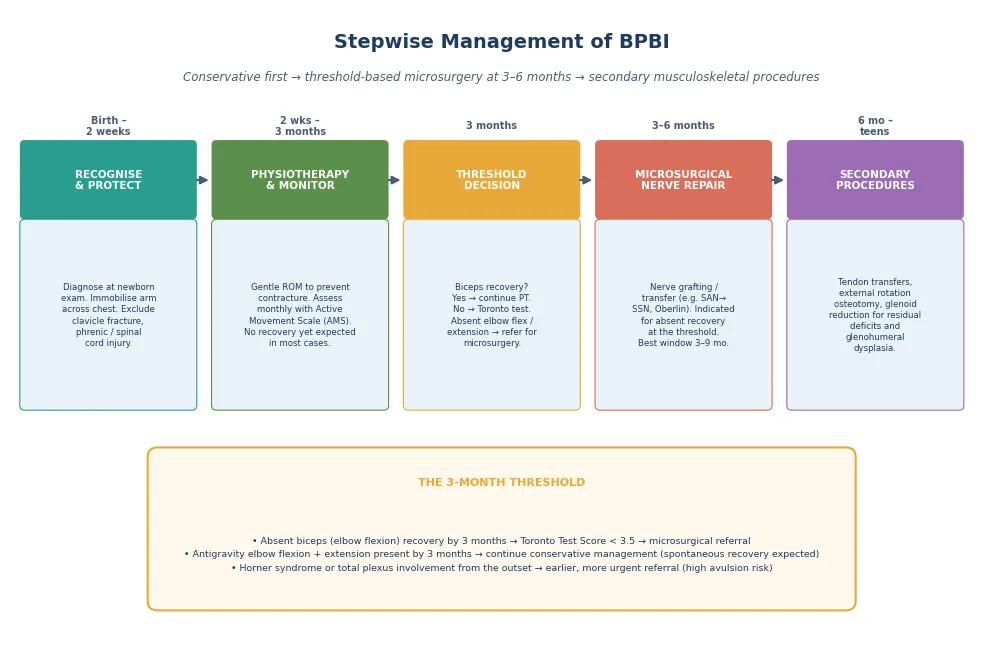
The definitive management of BPBI is a staged pathway from conservative physiotherapy through threshold-based microsurgical nerve reconstruction to secondary musculoskeletal procedures for residual deficits. The pathway is driven by the monthly Active Movement Scale and the Toronto Test Score, and the linchpin is the 3-month biceps-recovery threshold. [2]
In the conservative phase (birth to three months), the infant receives daily physiotherapy for joint mobility, and the AMS is assessed monthly. The majority of upper-trunk (grade I) injuries recover spontaneously — antigravity biceps function returns within the first three months, and the infant continues on a conservative pathway with progressive functional recovery over the first year. Infants who recover biceps by one month have near-complete recovery; those who recover by three months have a good but incomplete outcome. [3] [4]
The surgical threshold is reached at three months. An infant with absent antigravity biceps recovery (AMS below 5) and a Toronto Test Score below 3.5 is referred for microsurgical nerve reconstruction. The surgery — performed optimally between three and nine months of age — involves nerve grafting (using the sural nerve as a cable graft to bridge a postganglionic rupture) and nerve transfer (re-routing a functioning donor nerve, such as the spinal accessory nerve to the suprascapular nerve for shoulder abduction and external rotation, or the Oberlin transfer of a fascicle of the ulnar nerve to the musculocutaneous nerve for elbow flexion). Preganglionic avulsions cannot be grafted and require nerve transfers from extra-plexal donors. [2] [9]
In Australia, New Zealand and the United Kingdom, the standard of care for BPBI is conservative management with monthly Active Movement Scale assessment, with microsurgical referral when antigravity biceps recovery has not occurred by three months (Toronto Test Score below 3.5). Microsurgical nerve reconstruction, performed at a specialist brachial plexus centre, is optimally undertaken between three and nine months. Infants with Horner syndrome or total-plexus involvement from birth are referred earlier because of the high probability of avulsion. Regional networks exist for referral from peripheral centres to the specialist surgical service. [2] [4]
Secondary musculoskeletal procedures — tendon transfers (to restore external rotation, abduction, or elbow flexion), derotational humeral osteotomy, and arthroscopic or open glenohumeral reduction for posterior dysplasia — address the residual deficits and joint deformities that persist after nerve recovery or nerve surgery. These procedures belong to the long-term follow-up under the specialist service, typically from late infancy through adolescence, and are guided by the Waters classification of glenohumeral dysplasia on imaging. [5]
Specific Subtypes & Scenarios
The recovering upper-trunk injury (grade I–II, C5–6 or C5–7) is the central scenario and the one most infants follow. Antigravity biceps recovery occurs within the first three months, the AMS improves progressively, and the infant is managed conservatively with physiotherapy and periodic specialist review. Full or near-full functional recovery is expected, though mild residual weakness of shoulder external rotation and supination is common. The key is confirming recovery at the 3-month assessment and not over-treating with surgery. [3]
The non-recovering upper-trunk injury is the scenario that demands surgery. The infant who has not achieved antigravity biceps by three months, with a Toronto Test Score below 3.5, is referred for microsurgical reconstruction. The earlier the referral and surgery (within the 3-to-9-month window), the better the regenerative outcome — because the motor endplates of the target muscles degenerate irreversibly after roughly eighteen months, and a delay forfeits the window. [4] [9]
[2] [4]The total-plexus injury with Horner syndrome (grade IV) is the scenario that breaks the watchful-waiting rule. Horner syndrome (ptosis, miosis, anhidrosis) at birth signals T1 preganglionic avulsion — a lesion that cannot regenerate and will not recover spontaneously. These infants are referred for early specialist assessment, often before the 3-month threshold, because the probability of useful spontaneous recovery is very low and the surgical pathway (extra-plexal nerve transfers) is different from the standard grafting approach. The presence of Horner syndrome is the bedside finding that distinguishes grade IV from the other grades and demands a different, more urgent pathway. [2] [9]
Complications & Pitfalls
A child whose shoulder external rotation and abduction fail to recover after a brachial plexus injury develops a progressive internal rotation deformity at the shoulder — the humeral head is driven posteriorly by the unopposed pull of the pectoralis major and latissimus dorsi, remodelling the glenoid into a retroverted, dysplastic surface known as the pseudoglenoid. This glenohumeral dysplasia is the most important secondary deformity of BPBI, because it produces a visible and functional loss of external rotation and abduction that worsens with growth and becomes the primary target of the secondary reconstructive procedures. It arises from the muscle imbalance that persists when the primary nerve recovery is incomplete. [5]
Shoulder and elbow contractures — particularly internal rotation and adduction contractures of the shoulder, and flexion or extension contractures of the elbow — develop when daily range-of-motion exercises are inadequate or when the muscle imbalance persists. Limb-length discrepancy and forearm pronation or supination contractures occur in the more severe injuries. These complications are mitigated by consistent physiotherapy in the conservative phase and by timely surgical intervention when the recovery threshold is not met. [5]
Beyond BPBI, the complications of birth trauma as a whole include the subgaleal haemorrhage (a rapidly expanding scalp bleed that can cause hypovolaemic shock and coagulopathy), the cephalohaematoma (which calcifies and may cause anaemia or hyperbilirubinaemia), and the adrenal haemorrhage (which presents as a flank mass, anaemia, and — in bilateral cases — adrenal insufficiency). Each is managed on its own merits, but the principle is the same: recognise early, investigate appropriately, and do not let the obvious injury distract from the dangerous one. [6]
Prognosis & Disposition
The prognosis of BPBI is determined by the Narakas grade, the recovery trajectory on the monthly AMS, and the timeliness of surgical intervention when the threshold is met. The overall spontaneous recovery rate is high — roughly 80 to 90 percent of all infants recover useful function, concentrated in the grade I–II upper-trunk injuries that recover biceps within three months. However, the grade III–IV total-plexus and avulsion injuries have substantially poorer outcomes, and even among recovered infants, mild residual deficits of shoulder external rotation and supination are common. [1] [3]
The historical cohort study by Hoeksma and colleagues provided the recovery benchmarks: infants who recovered biceps within the first month had near-complete recovery; those who recovered by three months had a good but incomplete outcome; and those who had not recovered by three months had a high probability of persistent deficit without surgery. The Waters comparison of natural history, microsurgical repair, and operative reconstruction established that microsurgical nerve reconstruction improves the outcome of non-recovering injuries compared with the natural history, validating the 3-month threshold. [3] [4]
Disposition follows the recovery pathway. The infant recovering on schedule is managed as an outpatient with physiotherapy and periodic specialist review. The infant meeting the surgical threshold is referred to a specialist brachial plexus centre for microsurgical reconstruction, then enters long-term surveillance for residual deficits and secondary procedures. The infant with Horner syndrome or total-plexus involvement from birth is referred early. Every infant with BPBI receives structured neurodevelopmental follow-up, because the injury is a marker of perinatal adversity and because comorbidities — including torticollis, developmental delay, and sensory deficits — occur in a significant minority and benefit from early detection. [8]
Special Populations
The infant with a grade IV (Horner-positive) injury is the population that breaks the watchful-waiting rule. The presence of ptosis, miosis, and anhidrosis signals T1 preganglionic avulsion, and these infants are referred for early specialist assessment before the 3-month threshold. The surgical pathway is different from the standard grafting approach — extra-plexal nerve transfers (such as intercostal nerves to the musculocutaneous nerve for elbow flexion) are often needed — because avulsed roots cannot be grafted. The prognosis is guarded, and families are counselled honestly about the expected residual deficits. [2] [9]
The infant with an associated coexisting injury — clavicle fracture, phrenic nerve palsy, facial nerve palsy — is managed for both. Clavicle fractures heal spontaneously with analgesia and gentle handling. Phrenic nerve palsy may require respiratory support until the diaphragm recovers or, in persistent cases, surgical plication. Facial nerve palsy usually recovers spontaneously within weeks to months; failure to recover by two months warrants specialist assessment. The scoping review by Lewis and Sweeney documented the multisystem comorbidities that accompany NBPP — including torticollis, developmental concerns, and sensory deficits — and recommended structured multisystem screening rather than an arm-only focus. [6] [8]
The rural or remote infant raises referral considerations. The 3-month threshold does not pause for geography, and the monthly AMS requires a clinician trained in the technique. Regional networks in ANZ and the UK support peripheral centres with telehealth consultation, AMS training, and structured referral pathways to the specialist brachial plexus service. The principle is that no infant should miss the 3-month decision because of distance — the monitoring and the threshold decision are feasible in any setting with the right support. [2]
Evidence, Guidelines & Regional Differences
The evidence base for BPBI management combines observational natural-history data with comparative surgical outcome studies. The epidemiological foundation was established by Foad and colleagues, who used the Kids' Inpatient Database to determine the US incidence (1.5 per 1000 live births), the dominant risk factors (shoulder dystocia, macrosomia, instrumental delivery), and the notable finding that over half of affected infants had no identifiable risk factor. This work reframed BPBI as a multifactorial injury rather than a pure marker of obstetric trauma. [1]
The recovery benchmarks were established by the Hoeksma historical cohort study, which documented the relationship between the timing of biceps recovery and the overall functional outcome. The Waters comparison study — comparing the natural history, microsurgical repair outcomes, and operative reconstruction outcomes — validated that microsurgical nerve reconstruction improves the outcome of non-recovering injuries, providing the evidence base for the 3-month threshold. The Gilbert long-term results of primary repair confirmed that nerve grafting and transfer produce durable functional improvements into adolescence. [3] [4] [9]
Across ANZ, the UK, Europe and North America, the standard of care for BPBI is conservative management with monthly Active Movement Scale monitoring, with microsurgical referral when antigravity biceps recovery has not occurred by three months (Toronto Test Score below 3.5). The optimal surgical window is 3 to 9 months. The specific nerve transfer techniques (spinal accessory to suprascapular, Oberlin ulnar-to-musculocutaneous) and the approach to secondary musculoskeletal procedures vary by centre, but the threshold and the window are consistent across regions. [2] [9]
The prevention and obstetric-management dimension is informed by the shoulder dystocia guideline literature. Chauhan and colleagues compared the ACOG practice bulletin with other national guidelines, highlighting the manoeuvres (McRoberts, suprapubic pressure, rotational and posterior-arm manoeuvres) and the residual risk of BPBI despite best-practice management. Prophylactic caesarean for suspected macrosomia reduces but does not eliminate the risk. Current controversies include the optimal surgical technique (single versus double nerve transfers), the role of nerve transfers versus grafting for specific lesion patterns, and the timing of secondary musculoskeletal procedures for glenohumeral dysplasia. [7]
Exam Pearls
Narakas grades — 'Increasing severity, Decreasing recovery'
References
- [1]Foad SL; Mehlman CT; Ying J The epidemiology of neonatal brachial plexus palsy in the United States. J Bone Joint Surg Am, 2008.PMID 18519319
- [2]Hale HB; Bae DS; Waters PM Current concepts in the management of brachial plexus birth palsy. J Hand Surg Am, 2010.PMID 20141905
- [3]Hoeksma AF; ter Steeg AM; Nelissen RG; van Ouwerkerk WJ; de Jong BA; Lankhorst GJ Neurological recovery in obstetric brachial plexus injuries: an historical cohort study. Dev Med Child Neurol, 2004.PMID 14974631
- [4]Waters PM Comparison of the natural history, the outcome of microsurgical repair, and the outcome of operative reconstruction in brachial plexus birth palsy. J Bone Joint Surg Am, 1999.PMID 10360693
- [5]Hoeksma AF; Ter Steeg AM; Dijkstra P; Nelissen RG; van Ouwerkerk WJ; Lankhorst GJ; de Jong BA Shoulder contracture and osseous deformity in obstetrical brachial plexus injuries. J Bone Joint Surg Am, 2003.PMID 12571311
- [6]Parker LA Part 1: early recognition and treatment of birth trauma: injuries to the head and face. Adv Neonatal Care, 2005.PMID 16338668
- [7]Chauhan SP; Gherman R; Hendrix NW; Magann EF; Morrison JC Shoulder dystocia: comparison of the ACOG practice bulletin with another national guideline. Am J Perinatol, 2010.PMID 19565435
- [8]Lewis SP; Sweeney JK Comorbidities in infants and children with neonatal brachial plexus palsy: a scoping review to inform multisystem screening. Phys Occup Ther Pediatr, 2023.PMID 36659827
- [9]Gilbert A; Pivato G; Kheiralla T Long-term results of primary repair of brachial plexus lesions in children. Microsurgery, 2006.PMID 16634084
- [10]Malik S; Bhandekar HS; Korday CS Traumatic peripheral neuropraxias in neonates: a case series. J Clin Diagn Res, 2014.PMID 25478423