Paeds · fetal-neonatal-and-perinatal
Bronchopulmonary dysplasia and chronic neonatal lung disease
Also known as Bronchopulmonary dysplasia and chronic neonatal lung disease
Fellowship guide to bronchopulmonary dysplasia and chronic neonatal lung disease.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Bronchopulmonary dysplasia (BPD) is the most common serious complication of extreme prematurity, affecting up to 40 percent of infants born before 28 weeks' gestation. The condition was first described by Northway in 1967 in oxygen-exposed, mechanically ventilated preterm infants, but the modern "new BPD" reflects arrested lung development rather than adult-style fibrotic injury [1].
The modern definition requires supplemental oxygen or respiratory support at 36 weeks' postmenstrual age (PMA), validated by the NIH consensus definition in a landmark multicentre study [2]. This standardised classification replaced older criteria that relied on oxygen dependency at 28 days of life and has become the universal benchmark for severity grading.
BPD sits at the intersection of neonatology, respiratory medicine, and developmental biology. The preterm lung is still in the canalicular-to-saccular stage when the infant is born, making it exquisitely vulnerable to the very interventions that sustain life — oxygen, positive pressure ventilation, and caloric restriction [10].
Epidemiology & Risk Factors
BPD incidence is inversely related to gestational age and birth weight. Among extremely preterm infants (under 28 weeks), approximately 40 to 68 percent develop BPD, compared with less than 5 percent of infants born at 32 weeks or later [4]. Data from the Neonatal Research Network show that even with modern care, BPD rates have plateaued rather than declined because more extremely preterm infants now survive [5].
The principal risk factors cluster into antenatal, perinatal, and postnatal domains. Antenatal chorioamnionitis and intrauterine growth restriction prime the lung for postnatal injury. Perinatal factors include male sex, white race, and perinatal asphyxia. Postnatal exposures — particularly mechanical ventilation, oxygen toxicity, postnatal sepsis, and patent ductus arteriosus — are the most modifiable targets for prevention [9].
Indigenous and socioeconomically disadvantaged populations carry disproportionate risk due to higher rates of preterm birth and reduced access to antenatal care. In Australia and New Zealand, Aboriginal and Torres Strait Islander and Māori infants have significantly elevated BPD burden compared with non-Indigenous infants [5].
Pathophysiology
The preterm lung is structurally immature at birth, with lungs still in the late canalicular or early saccular stage. Alveoli are large and few in number, capillaries are primitive, and antioxidant enzyme systems (superoxide dismutase, catalase) are underdeveloped. This immaturity makes the lung uniquely vulnerable to injury from oxygen free radicals and mechanical stretch [1].
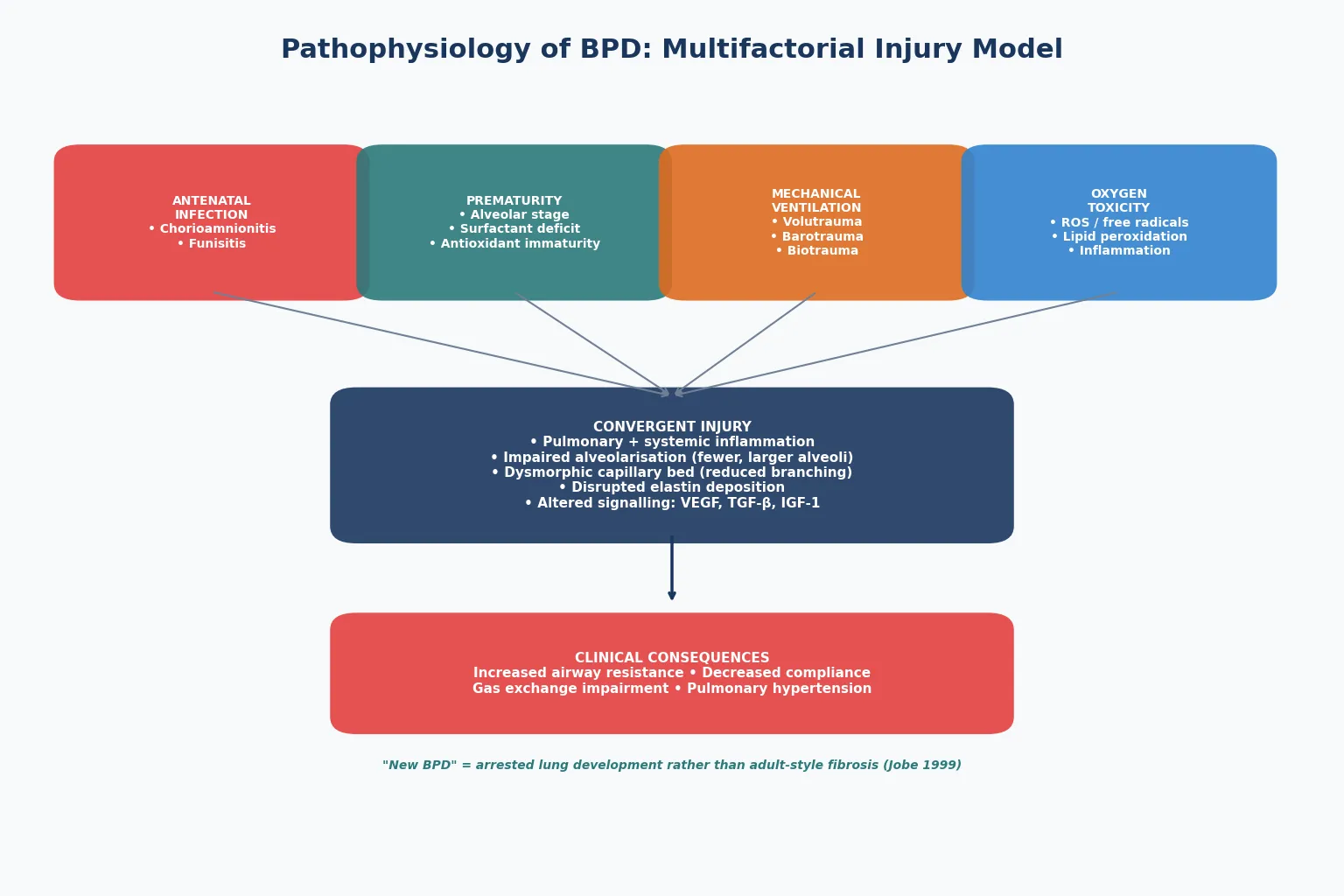
BPD develops through a convergent injury model. Antenatal chorioamnionitis triggers fetal lung inflammation before birth. Postnatally, mechanical ventilation causes volutrauma and biotrauma — the release of pro-inflammatory cytokines from over-stretched alveoli. Hyperoxia generates reactive oxygen species that overwhelm immature antioxidant defences. Together these insults disrupt critical signalling pathways including vascular endothelial growth factor (VEGF), transforming growth factor beta, and insulin-like growth factor-1 [10].
The hallmark of "new BPD" is arrested alveolar development rather than the cystic fibrosis-like fibrosis seen in the original Northway description. Alveoli are fewer and larger, the capillary bed is dysmorphic with reduced branching, and elastin is deposited abnormally. This structural simplification leads to chronically impaired gas exchange, reduced lung compliance, and increased airway resistance [1].
Classification
The NIH consensus definition classifies BPD severity at 36 weeks' PMA based on the level of respiratory support required. This grading system has been validated against neurodevelopmental and respiratory outcomes at 18 to 22 months [2].
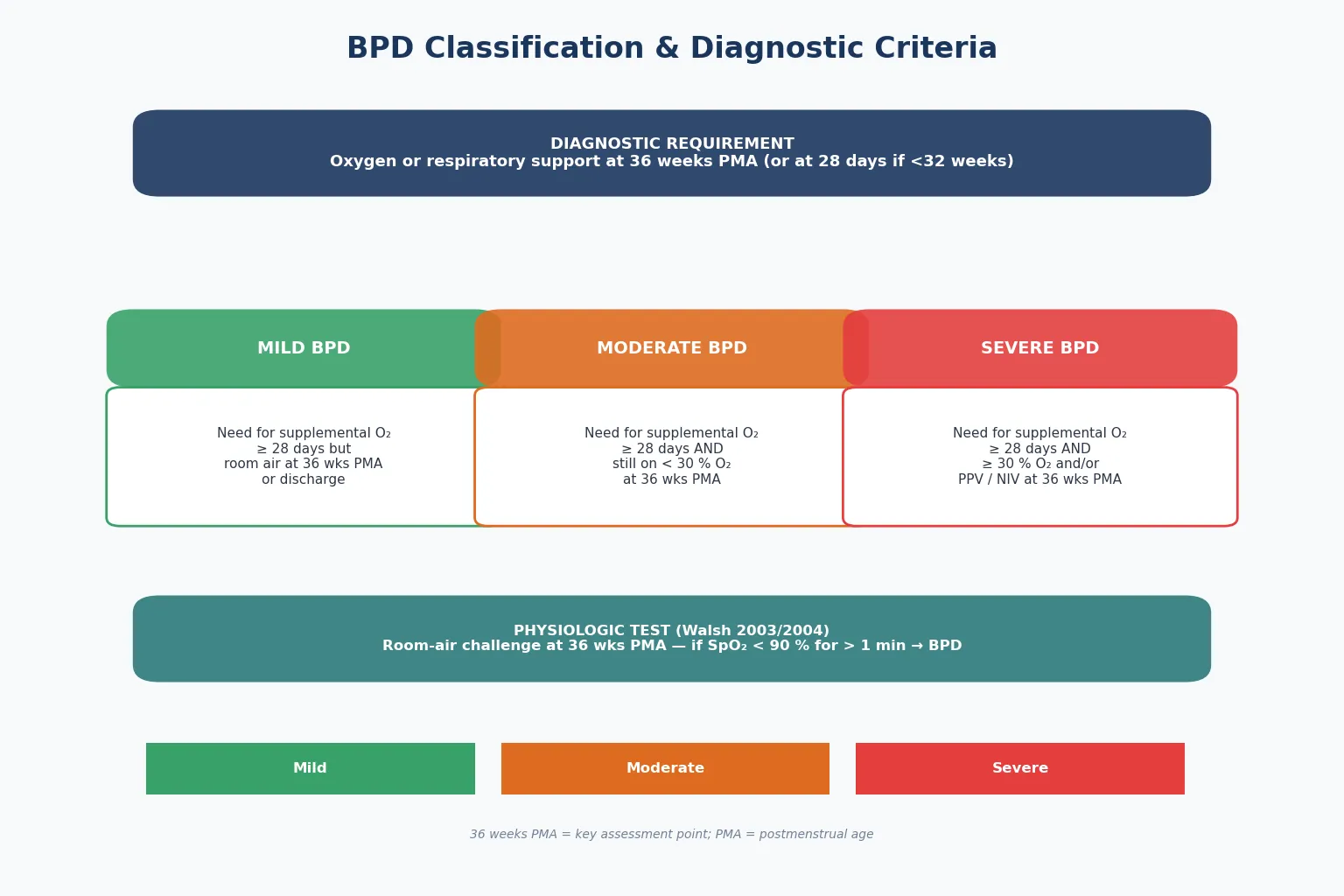
The physiologic definition (Walsh room-air challenge) provides an objective, severity-graded alternative. Infants undergo a timed room-air trial at 36 weeks PMA, and those whose SpO₂ drops below 90 percent for more than one minute are classified as having BPD. This reduces inter-centre variability introduced by different oxygen-weaning practices [2].
Clinical Presentation
Infants with evolving BPD typically show a trajectory of persistent or escalating respiratory support requirement beyond the first one to two weeks of life. The clinical picture includes increased work of breathing with retractions, tachypnoea, and nasal flaring. Auscultation reveals scattered crackles, wheeze, or a prolonged expiratory phase reflecting airway obstruction and hyperinflation [1].
Infants with established BPD often demonstrate oxygen desaturation during feeds and sleep. Growth faltering is common because the increased work of breathing raises caloric expenditure while feeding tolerance is limited. Recurrent apnoea or bradycardia may signal worsening respiratory compromise or intercurrent infection [9].
Severe BPD can present with signs of pulmonary hypertension — a loud pulmonary component of the second heart sound, right ventricular heave, or hepatomegaly from right heart failure. Any preterm infant with BPD who develops unexplained tachypnoea, failure to wean from oxygen, or episodic desaturation should be evaluated for pulmonary vascular disease [10].
Differential Diagnosis
The differential diagnosis for persistent respiratory distress in a preterm infant is broad. The key task is distinguishing evolving BPD from other causes of ongoing oxygen or ventilator dependency [1].
| Condition | Key Features | Diagnostic Clue |
|---|---|---|
| Respiratory distress syndrome | Day 1 to 3 onset, responds to surfactant | Improves within days |
| Neonatal pneumonia | Positive cultures, focal infiltrate | Blood or tracheal culture |
| Congenital heart disease | Murmur, differential cyanosis | Echocardiography |
| Aspiration syndrome | Meconium in amniotic fluid | Perinatal history |
| Pulmonary interstitial emphysema | CXR lucencies | Complication of PPV |
| Patent ductus arteriosus | Bounding pulses, widened pulse pressure | Echocardiography |
The distinction between late RDS and early BPD can be difficult in the first two weeks, as both involve oxygen and ventilator dependency. BPD is generally a diagnosis of evolution — the infant who does not improve as expected from RDS and remains oxygen-dependent beyond the first month of life [1].
Patent ductus arteriosus often coexists with and worsens BPD. A significant left-to-right shunt causes pulmonary over-circulation, worsening respiratory status and delaying weaning. Clinicians should assess for a PDA murmur, bounding pulses, and widened pulse pressure in any infant failing to wean from respiratory support [9].
Clinical & Bedside Assessment
Bedside assessment of the infant with BPD focuses on respiratory effort, growth, and developmental trajectory. The respiratory examination documents the type and level of support, oxygen requirement at rest and during feeds, and signs of increased work of breathing. Serial weight, length, and head circumference plotted on growth charts reveal growth faltering that may require nutritional intervention [9].
Cardiovascular examination is essential. A loud P2, right ventricular heave, or hepatomegaly suggests pulmonary hypertension, a feared complication of moderate-to-severe BPD. Preterm infants on diuretics require monitoring for electrolyte disturbances, and those on corticosteroids need blood pressure and glucose surveillance [10].
Developmental assessment documents muscle tone, movement quality, and visual tracking. Infants with BPD are at increased risk of cerebral palsy, cognitive impairment, and sensorineural hearing loss — early identification allows timely intervention [5].
Investigations
Chest radiography in BPD typically shows hyperinflated lungs with diffuse fine reticulogranular opacities, areas of atelectasis or emphysema, and bronchial wall thickening. CXR findings correlate poorly with disease severity and are most useful for detecting complications such as focal overdistension, consolidation, or pneumothorax [1].
Echocardiography is critical in moderate-to-severe BPD to evaluate for pulmonary hypertension. Key findings include elevated estimated pulmonary artery pressure, right ventricular hypertrophy, septal flattening, and tricuspid regurgitation. An echocardiogram should be performed in any infant who fails to wean from oxygen or has unexplained tachypnoea [10].
Routine blood gas analysis monitors oxygenation, ventilation, and acid-base status. Serial electrolytes and bone profile are needed for infants on diuretics. A complete blood count and inflammatory markers help distinguish BPD exacerbation from intercurrent infection [9].
Investigation pathway
CXR: confirm chronic changes and exclude complications
Echocardiography: screen for pulmonary hypertension
Blood gas: assess oxygenation and ventilation
Electrolytes: monitor diuretic effects
Microbiology: exclude infection
Overnight oximetry: evaluate desaturation
Management — Resuscitation
Acute respiratory decompensation in an infant with BPD requires rapid assessment of airway, breathing, and circulation. The infant is transitioned to an appropriate level of respiratory support — escalating from low-flow cannula to high-flow nasal cannula, then CPAP or NIV, and ultimately invasive ventilation if non-invasive strategies fail [3].
Lung-protective ventilation principles apply to BPD. Use the lowest tidal volume and inspiratory pressure compatible with adequate gas exchange, accepting permissive hypercapnia to minimise volutrauma. Positive end-expiratory pressure is titrated to maintain alveolar recruitment, typically 5 to 7 cmH₂O in BPD [1].
Oxygen therapy targets a SpO₂ of 91 to 95 percent, balancing oxidative lung injury from hyperoxia against hypoxic pulmonary vasoconstriction. Lower saturation targets increase mortality, while higher targets do not improve outcomes [11].
Caffeine citrate
Loading dose
20 mg/kg caffeine citrate PO or IV
Maintenance dose
5 to 10 mg/kg daily
Caffeine citrate should be initiated early in preterm infants under 1250 g to reduce the incidence of BPD. The CAP trial demonstrated that caffeine therapy started in the first ten days reduced the rate of BPD from 47 to 36 percent [6]. Long-term follow-up at five years showed no adverse effects on growth or behaviour [7].
Management — Definitive & Stepwise
Definitive management of BPD is a multidisciplinary, longitudinal process spanning the NICU stay, discharge preparation, and community follow-up. There is no single cure; the strategy is to minimise further lung injury while supporting somatic growth and alveolar development [9].
Prevention and lung-protective care
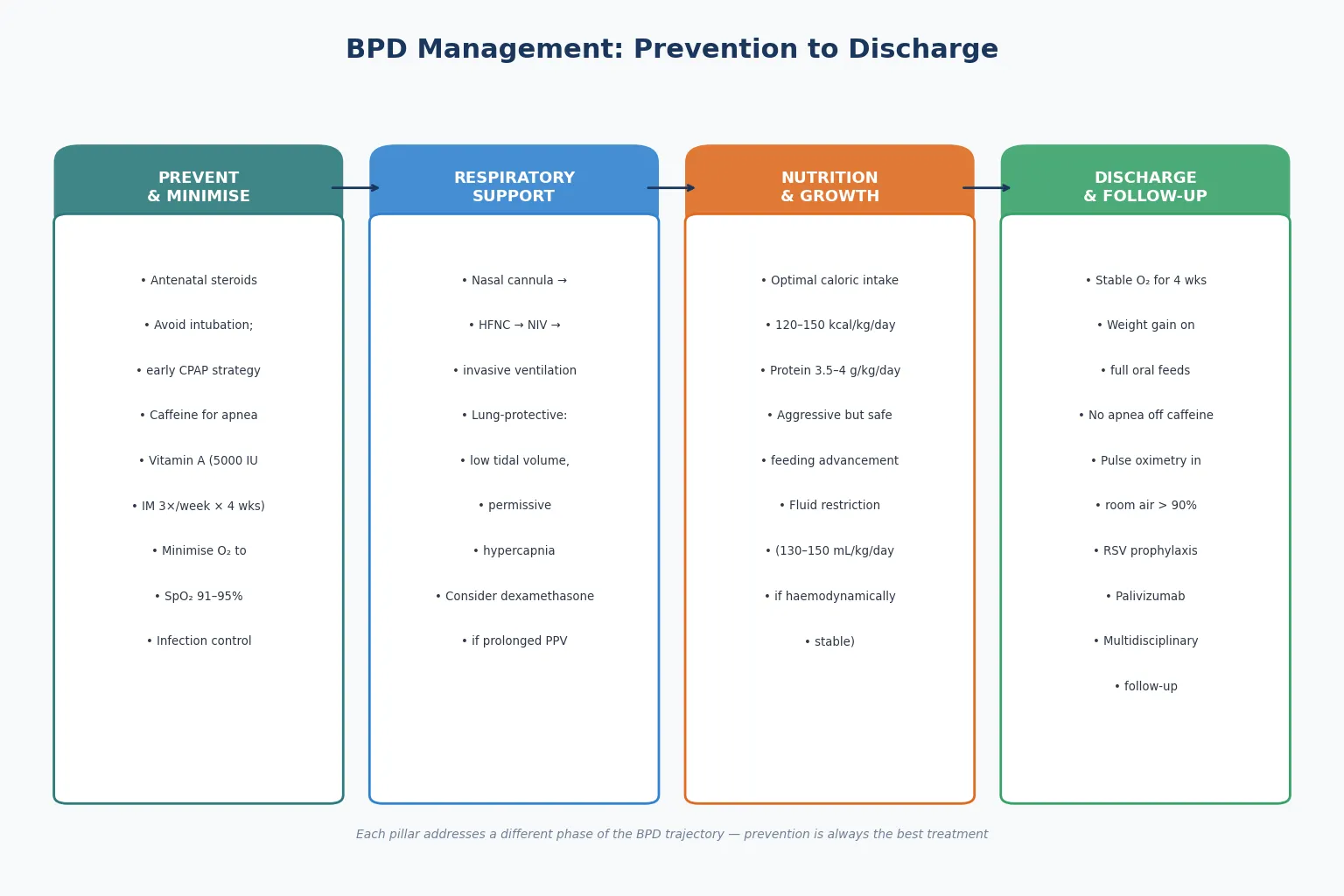
The best treatment for BPD is prevention. Antenatal corticosteroids accelerate lung maturation and reduce RDS severity. A non-intubated, early CPAP strategy avoids the volutrauma associated with intubation, as demonstrated by the SUPPORT trial [3].
Vitamin A supplementation at 5000 IU intramuscularly three times weekly for four weeks reduces the incidence of BPD in extremely-low-birth-weight infants. The number needed to treat is approximately 14 to 20 infants [8].
Pharmacotherapy
Postnatal corticosteroids reduce inflammation and facilitate extubation but carry significant risks. Low-dose dexamethasone starting at 0.15 mg/kg per day and tapering over 7 to 10 days is reserved for ventilator-dependent infants after one to two weeks [9].
Diuretics provide short-term improvement in lung compliance by reducing interstitial fluid, but chronic use is limited by electrolyte disturbances and nephrocalcinosis. They are used as intermittent courses rather than continuous therapy [10].
Inhaled bronchodilators may help selected infants with significant wheeze, but routine use is not supported by strong evidence. Azithromycin is emerging as a potential anti-inflammatory agent [9].
Nutrition and growth
Optimal nutrition is fundamental to BPD management because alveolar development requires energy. Target caloric intake is 120 to 150 kcal/kg/day with protein at 3.5 to 4 g/kg/day [10].
CAN'T BREATHE
Fluid management requires balance between adequate nutrition and avoidance of pulmonary oedema. Fluid restriction to 130 to 150 mL/kg/day is standard when haemodynamically stable [10].
Pulmonary hypertension management
Pulmonary hypertension complicates moderate-to-severe BPD in 8 to 25 percent of cases and is the leading cause of late mortality. Management includes optimisation of oxygenation, treatment of contributing factors, and pulmonary vasodilator therapy including inhaled nitric oxide, sildenafil, and bosentan [10].
Specific Subtypes & Scenarios
| Scenario | Key Features | Management Focus |
|---|---|---|
| Mild BPD | Room air at 36 wks PMA | Monitoring and immunisation |
| Moderate BPD | Oxygen under 30% at 36 wks | Gradual wean, nutrition |
| Severe BPD | Oxygen 30% or PPV at 36 wks | Multidisciplinary care |
| BPD with pulmonary HTN | Echo evidence of elevated PAP | Pulmonary vasodilators |
| BPD with tracheomalacia | Stridor, airway collapse | CPAP, possible surgery |
Infants with severe BPD represent the most challenging subgroup, often technology-dependent at discharge with home oxygen and complex medication regimens. Their care demands coordinated input from neonatology, pulmonology, cardiology, and developmental therapy [5].
The late preterm or term infant with prolonged oxygen requirement warrants careful reassessment for alternative diagnoses including congenital heart disease, airway malacia, or neuromuscular disease [1].
[6]Complications & Pitfalls
The complications of BPD extend far beyond the respiratory system. Infants face increased risks of recurrent respiratory infections, hospital readmissions in the first two years, asthma-like symptoms, and persistent reductions in exercise capacity. Neurodevelopmental sequelae include cerebral palsy, cognitive impairment, and sensorineural hearing loss [5].
Pulmonary hypertension is the most feared respiratory complication, occurring in 8 to 25 percent of infants with moderate-to-severe BPD. It significantly increases mortality — up to 40 percent of infants with BPD-associated pulmonary hypertension may die in the first two years [10].
Common management pitfalls include over-reliance on CXR findings, neglecting growth while focusing on respiratory parameters, and using diuretics or corticosteroids indiscriminately [9].
Prognosis & Disposition
The prognosis for BPD depends on severity. Most infants with mild BPD achieve complete recovery by two to three years of age as alveolarisation continues. However, even mild BPD is associated with reduced lung function in adolescence and early adulthood [1].
Infants with moderate-to-severe BPD have higher rates of hospital readmission (30 to 50 percent in the first year), persistent respiratory symptoms, and developmental delays [5].
Discharge criteria require clinical stability demonstrated over time. The infant should be on stable support for at least four weeks, achieving adequate weight gain on full feeds, free from apnoea for five to seven days off caffeine, and maintaining SpO₂ above 90 percent [9].
Discharge readiness
Stable support for over 4 weeks
Adequate weight gain on full feeds
No apnoea for 5 to 7 days off caffeine
SpO₂ over 90% in room air or prescribed O₂
Parents trained in home care
Follow-up and RSV prophylaxis arranged
Special Populations
Indigenous infants in Australia and New Zealand carry a disproportionate burden of prematurity and BPD due to higher preterm birth rates and geographic barriers to antenatal care. Culturally safe, family-centred care is essential for equitable outcomes [5].
Infants from socioeconomically disadvantaged backgrounds face additional challenges including reduced access to specialist follow-up, higher exposure to household smoking, and overcrowded housing increasing infection risk [10].
Technology-dependent infants with severe BPD require home ventilation, tracheostomy, and complex feeding support. These families need coordinated discharge planning, community nursing, and clear emergency plans [9].
Evidence, Guidelines & Regional Differences
The SUPPORT trial compared early CPAP with prophylactic intubation and surfactant in extremely preterm infants. It showed that early CPAP was non-inferior to the surfactant strategy for the composite outcome of death or BPD [3].
The CAP trial established caffeine citrate as a key BPD prevention strategy, reducing BPD from 47 to 36 percent and improving survival without neurodevelopmental disability at 18 to 21 months [6].
The Cochrane review of oxygen saturation targeting compared lower (85 to 89 percent) with higher (91 to 95 percent) targets and found that lower targets increased mortality without reducing severe retinopathy [11].
SUPPORT (2010)
RCT: early CPAP vs prophylactic surfactant in infants 24 to 27 weeks
Population: 1316 extremely preterm infants
Key finding
CPAP non-inferior
Practice change
Changed practice toward non-intubated management
Regional differences exist in oxygen saturation targets and corticosteroid protocols. ANZ guidelines have converged on 91 to 95 percent SpO₂ targets and universal caffeine for infants under 1250 g [11].
Exam Pearls
The single most testable concept is the NIH consensus definition: BPD is classified at 36 weeks PMA based on oxygen requirements. Know the mild, moderate, and severe thresholds precisely [2].
Caffeine and vitamin A are the two interventions with strong RCT evidence for BPD prevention. Know the doses: caffeine citrate 20 mg/kg loading then 5 to 10 mg/kg per day; vitamin A 5000 IU IM three times weekly for four weeks [6].
The "new BPD" concept is frequently examined. New BPD differs from the original Northway description: it affects more immature infants, shows arrested alveolarisation rather than fibrosis, and reflects multifactorial injury [1].
BPD RISK FACTORS
References
- [1]Jobe AH, Bancalari E Bronchopulmonary dysplasia Am J Respir Crit Care Med, 2001.PMID 11401896
- [2]Ehrenkranz RA, Walsh MC, Vohr BR, et al Validation of the National Institutes of Health consensus definition of bronchopulmonary dysplasia Pediatrics, 2005.PMID 16322158
- [3]SUPPORT Study Group of the Eunice Kennedy Shriver NICHD Neonatal Research Network Early CPAP versus surfactant in extremely preterm infants N Engl J Med, 2010.PMID 20472939
- [4]Stoll BJ, Hansen NI, Bell EF, et al Neonatal outcomes of extremely preterm infants from the NICHD Neonatal Research Network Pediatrics, 2010.PMID 20732945
- [5]Bell EF, Gould JB, Walden RJ, et al Mortality, in-hospital morbidity, care practices, and 2-year outcomes for extremely preterm infants in the US, 2013-2018 JAMA, 2022.PMID 35040888
- [6]Schmidt B, Roberts RS, Davis P, et al Caffeine therapy for apnea of prematurity N Engl J Med, 2006.PMID 16707748
- [7]Schmidt B, Anderson PJ, Davis PG, et al Long-term effects of caffeine therapy for apnea of prematurity N Engl J Med, 2007.PMID 17989382
- [8]Tyson JE, Wright LL, Oh W, et al Vitamin A supplementation for extremely-low-birth-weight infants N Engl J Med, 1999.PMID 10379020
- [9]Aschner JL, Bancalari EH, McEvoy CT, et al Can we prevent bronchopulmonary dysplasia? J Pediatr, 2017.PMID 28947055
- [10]McEvoy CT, Jain L, Schmidt B, et al Bronchopulmonary dysplasia: NHLBI Workshop on the Primary Prevention of Chronic Lung Disease Ann Am Thorac Soc, 2014.PMID 24754823
- [11]Askie LM, Darlow BA, Finer N, et al Effects of targeting lower versus higher arterial oxygen saturations on death or disability in preterm infants Cochrane Database Syst Rev, 2017.PMID 28398697