Paeds · fetal-neonatal-and-perinatal
Cephalhaematoma and subgaleal haemorrhage
Also known as Cephalohematoma · Subgaleal haemorrhage · Subaponeurotic haemorrhage · Birth scalp swelling · Caput succedaneum differential
Fellowship guide to the three birth-related scalp swellings: the anatomical planes that separate caput succedaneum, cephalohaematoma and subgaleal (subaponeurotic) haemorrhage, the shearing of emissary veins in instrumental delivery, recognition of the deteriorating infant, resuscitation with volume and blood, and the complications of anaemia, hyperbilirubinaemia and skull fracture.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A newborn delivered by vacuum or forceps, or after a long obstructed labour, is noted to have a swelling of the scalp. The question that decides everything is simple: which plane is the blood in? The answer separates a harmless caput from a benign cephalhaematoma from a potentially lethal subgaleal haemorrhage, and it is answered by examining the swelling against the suture lines. [3] [8]
Caput succedaneum is oedema of the soft tissue of the scalp — subcutaneous, present at birth from the pressure of the presenting part against the cervix, crossing the suture lines, pitting on pressure, and resolving over the first days. It is harmless. Cephalhaematoma is a collection of blood between a skull bone and its periosteum — subperiosteal — confined by the attachments of the periosteum to the suture of that bone, so it does not cross the suture line, is firm and non-pitting, and enlarges over the first hours to days. Subgaleal haemorrhage is blood in the loose areolar tissue beneath the galea aponeurotica — the subaponeurotic space — which is a large potential space extending across the whole vault and down to the nape of the neck, so the swelling is diffuse, crosses the sutures and fontanelles, and can hold a volume of blood large enough to exsanguinate a newborn. [3] [6] [8]
The clinical importance of each is set by its plane. The subperiosteal space of a single bone is small and tight — a cephalhaematoma is self-limiting and its blood stays localised, the main late consequences being anaemia and hyperbilirubinaemia as the clot is reabsorbed. The subaponeurotic space is enormous by comparison — it has been estimated to hold a substantial fraction of a newborn's blood volume, which is why a subgaleal haemorrhage is the one scalp bleed that can kill. Recognising which plane you are dealing with, and reacting to the systemic signs of blood loss, is the heart of this topic. [3] [4]
The modern story of these conditions is one of prevention and vigilance. Safer operative vaginal delivery — limits on the number of cup detachments and pulls, abandoning the instrument for a caesarean when delivery does not progress, and alerting the neonatal team whenever a vacuum or forceps has been used — has not abolished subgaleal haemorrhage but has made early recognition the difference between a stable infant and a death. The fellowship candidate is expected to carry both the anatomical reasoning and the disciplined post-instrumental observation protocol. [3] [9] [10]
Epidemiology & Risk Factors
Cephalhaematoma is common: it occurs in roughly 1 to 2 per 100 live births, and the rate rises several-fold after instrumental delivery, affecting up to a tenth or more of vacuum or forceps deliveries in some series. Subgaleal haemorrhage is rarer but more dangerous, reported at around 1 to 3 per 1000 vacuum deliveries, with case fatality in severe or under-recognised cases of up to about a quarter. The two conditions share a risk profile but differ in consequence. [3] [7] [10]
The dominant risk factor for both is operative vaginal delivery, particularly vacuum (ventouse) extraction. Vacuum traction shears the scalp and aponeurosis against the underlying periosteum and skull, tearing the emissary veins that cross the subaponeurotic space; the risk rises with the number of cup detachments, the number of pulls, and the total duration of vacuum application. Forceps carry their own birth-injury profile, and a failed instrumental delivery that is then converted to caesarean section is a particularly high-risk sequence, because the infant has sustained both the traction of the instrument and the delay. [5] [9] [10]
Beyond the instrument itself, the risk factors cluster around difficult or obstructed delivery: prolonged first or second stage, nulliparity, cephalopelvic disproportion, macrosomia, malposition (especially occipitoposterior), and asynclitism. An underlying bleeding tendency — haemophilia, severe vitamin K deficiency (including parental refusal of vitamin K), maternal thrombocytopenia or anticoagulant therapy, or a consumptive coagulopathy — both increases the risk of a scalp bleed and worsens its course once begun. [3] [4]
It is important for the candidate to know that subgaleal and cephalohaematoma can occur without instruments. Subgaleal haemorrhage has been described after unassisted vaginal delivery and even after elective caesarean section, presumably from head compression and shearing forces in labour; these cases are rarer and easily missed because the clinician's index of suspicion is lower when no instrument was used. The lesson is that the swelling — not the mode of delivery — drives the diagnosis. [11]
Pathophysiology
The newborn scalp is built in layers, and the plane of bleeding is determined by which layer the shearing force disrupts. From outside in: skin and subcutaneous fat, the frontalis and occipitalis muscles joined across the vault by the galea aponeurotica, a layer of loose areolar tissue (the subaponeurotic space), the periosteum adherent to each skull bone, the skull bones themselves, and the dura. The blood vessels that matter are the emissary veins, which run from the scalp through the skull to the dural venous sinuses and cross the subaponeurotic space. [3] [8]
A cephalohaematoma forms when the periosteum is lifted off a skull bone — most often a parietal bone — by shearing of the diploic veins between the bone and its periosteum. Because the periosteum is anchored at the margins of the bone to the sutures, the blood cannot cross into the next bone's territory: the swelling stops sharply at the suture line. The space is small and the pressure self-limits, so the bleed is contained; the main problem is what happens to that sequestered blood over the following weeks. [8] [12]
A subgaleal haemorrhage forms when the galea aponeurotica is sheared off the underlying periosteum and skull by the traction of the vacuum cup or forceps, tearing the emissary veins that traverse the subaponeurotic space. Blood now enters the loose areolar tissue, a large potential plane with no firm boundary — it spreads forward over the forehead into the eyelids, backward over the occiput into the neck, and laterally around the ears, and it crosses every suture and the fontanelle. Because this space is so capacious, the bleed can continue until the infant is hypovolaemic, and the externally visible swelling may modestly understate how much blood has been lost. [3] [5] [6]
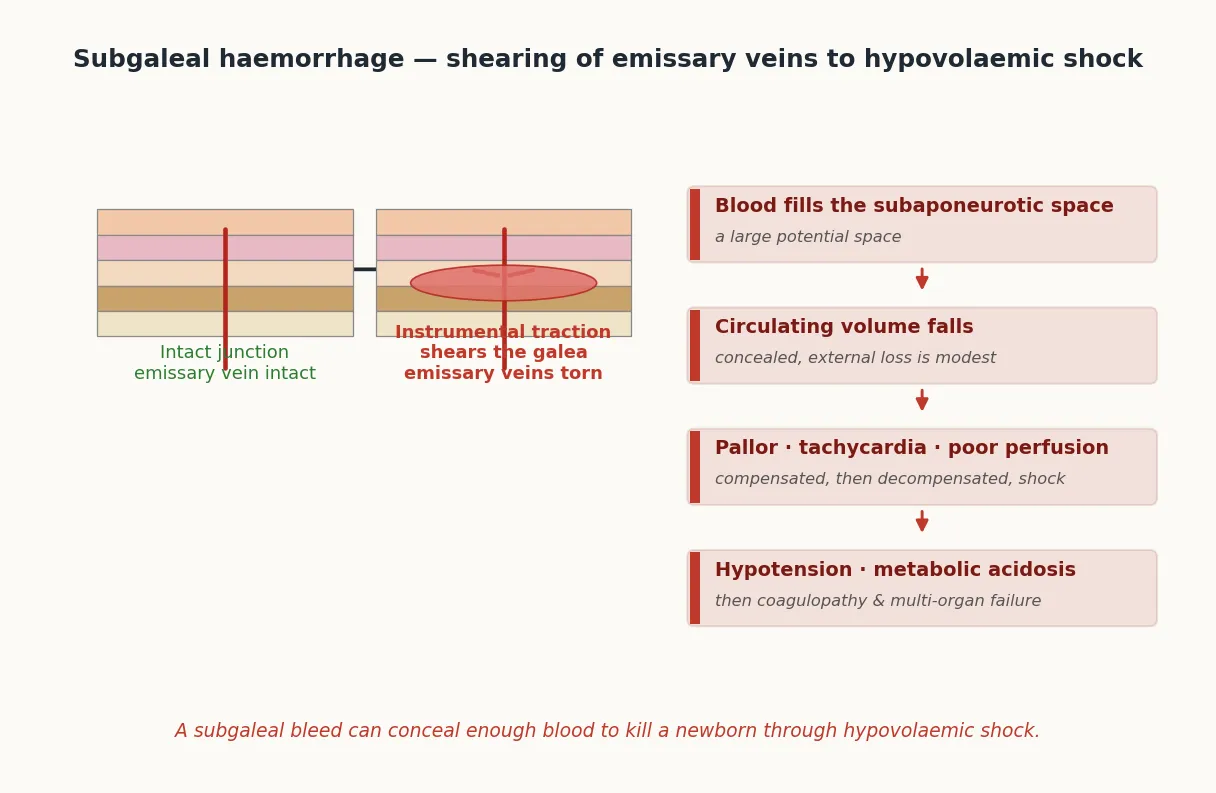
What makes the subgaleal bleed dangerous is the size of the space relative to the infant's blood volume. A term newborn's circulating volume is roughly 80 to 90 mL/kg — about 250 to 300 mL for a 3 kg infant. The subaponeurotic space can hold a substantial fraction of that before external swelling becomes dramatic, which is why an infant can be in haemorrhagic shock with a scalp swelling that looks only moderately large. The cephalohaematoma, by contrast, is in a small tight space and stops itself; its blood is contained and its danger is delayed and biochemical, not immediate and circulatory. [3] [4]
The late pathophysiology of a cephalohaematoma is about bilirubin and iron. As the clot breaks down over days to weeks, the haemoglobin releases bilirubin, driving an unconjugated hyperbilirubinaemia that can cross the phototherapy and even the exchange-transfusion threshold; this is why a large cephalohaematoma is a recognised risk factor for hazardous jaundice. The same reabsorption can leave the infant anaemic, sometimes enough to require transfusion, and over weeks the haematoma may calcify, producing a firm skull contour deformity that usually remodels over months. [12] [14]
Classification
The three birth-related scalp swellings are classified by the anatomical plane they occupy and their relationship to the suture lines, and these two facts together predict the clinical behaviour. Holding the three in your head, with the plane written on each, is the classification the examiner wants. [3] [8]
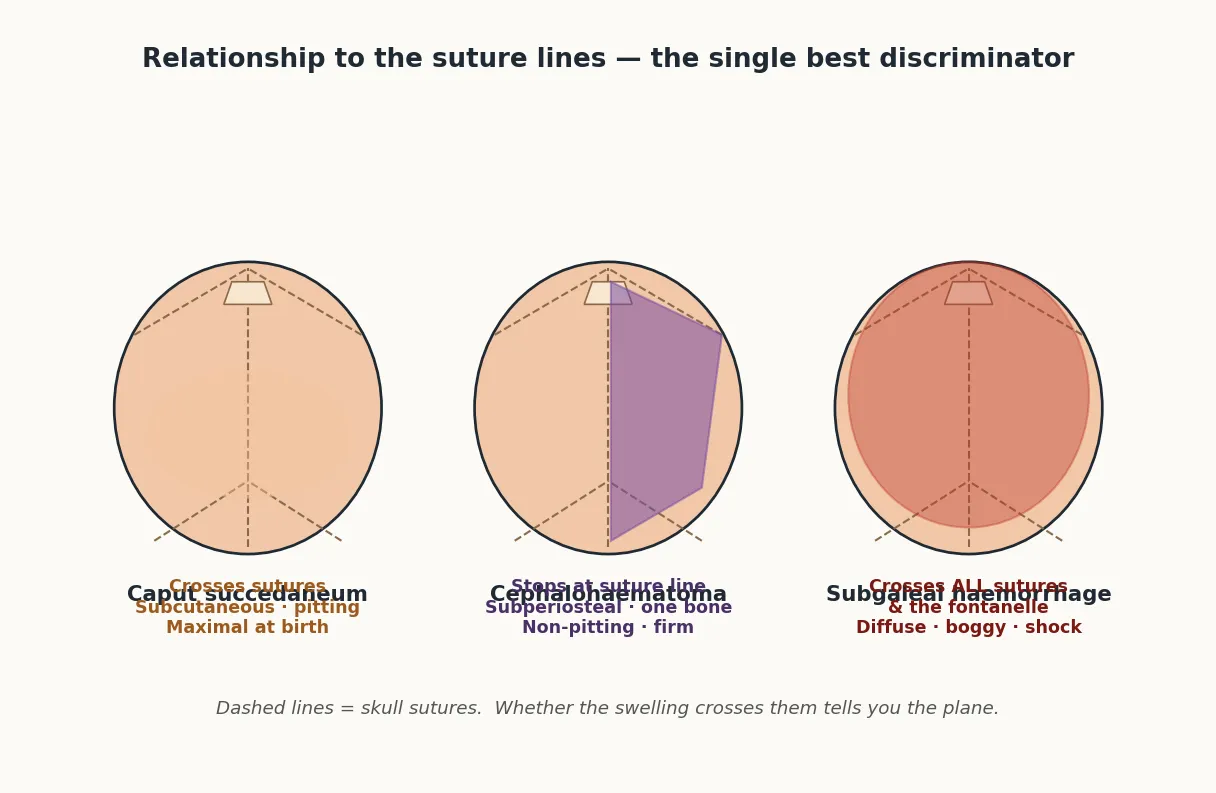
Caput succedaneum — subcutaneous oedema, in the skin and subcutaneous tissue plane. It is present at birth, crosses the suture lines, is soft and pitting, may extend beyond the limits of the vault onto the face and scalp, and resolves over the first two to three days. It is harmless and needs no treatment. [8]
Cephalhaematoma — a subperiosteal blood collection, between the skull bone and its periosteum. It appears over the first hours to days, is confined to a single bone and does not cross the suture line, is firm and non-pitting, and is most often over a parietal bone. It may be bilateral, in which case two separate collections are felt, each respecting its own suture boundary. [8] [12]
Subgaleal (subaponeurotic) haemorrhage — blood in the loose areolar tissue beneath the galea aponeurotica. It develops over the first hours, is diffuse, boggy and fluctuant, crosses the sutures and the fontanelles, tracks forward into the eyelids and forehead and backward into the neck, and is the dangerous one because of its capacity and its association with shock. [3] [6]
Cephalohaematoma versus subgaleal haemorrhage
- Subperiosteal plane
- Confined to ONE bone — does NOT cross the suture
- Firm, non-pitting, well-circumscribed
- Usually benign; risk is late anaemia and jaundice
- Managed by observation; do not aspirate
- Subaponeurotic plane
- Crosses ALL sutures and the fontanelle
- Diffuse, boggy, fluctuant; tracks into eyelids/neck
- Can cause hypovolaemic shock and coagulopathy
- Managed by resuscitation — volume, blood, correct coagulopathy
The clinical urgency runs on a spectrum. Life-threatening within hours: a significant subgaleal haemorrhage with evolving shock. Important but not immediately dangerous: a large cephalohaematoma, which demands surveillance for anaemia and hyperbilirubinaemia. Reassuring and self-limiting: caput succedaneum, and a small uncomplicated cephalohaematoma in a well infant. This urgency spectrum drives the management ladder and the observation protocol. [3] [4]
Clinical Presentation
The classical cephalohaematoma is found at the routine newborn check on day one or two: a firm, well-circumscribed swelling over a parietal or occipital bone that does not transilluminate, does not pit, and — the key sign — stops sharply at the suture line of that bone. The infant is systemically well; there is no pallor, the perfusion is normal, and the mother may not even have noticed the swelling. Bilateral parietal cephalohaematomas are common after a difficult delivery. [8] [12]
The classical subgaleal haemorrhage presents differently and dangerously. Over the first hours after an instrumental delivery the scalp becomes diffusely boggy and fluctuant, the swelling crosses the suture lines and the fontanelle, and there is ecchymosis that tracks forward into the eyelids and forehead and backward into the nape of the neck. The anterior fontanelle may be obscured by the overlying swelling. As the bleed progresses the infant becomes pale and tachycardic, then tachypnoeic, then hypotensive — the textbook march of hypovolaemic shock, except that the blood is hidden under the scalp. [3] [4] [6]
The early systemic signs of a significant subgaleal bleed are exactly those of blood loss in a newborn who is trying to compensate: tachycardia, a widening pulse pressure then narrowing, prolonged capillary refill, pallor, and increasing work of breathing. Hypotension is a late sign — by the time the blood pressure has fallen the infant has decompensated. A dropping haematocrit drawn serially is the most sensitive confirmatory finding, but the clinician should not wait for the second value if the swelling and the perfusion tell the story. [3] [6]
There are important atypical presentations. A cephalohaematoma may overlie an intracranial bleed, and an infant who has seizures, apnoea, a bulging fontanelle, or an altered conscious state alongside a scalp swelling needs cranial imaging — the scalp bleed may be the visible part of a deeper injury. A calcified cephalohaematoma may present weeks to months later as a hard skull asymmetry that alarms the parents. And a subgaleal bleed can present primarily as eyelid ecchymosis, the scalp swelling being subtle, which is why any periorbital bruising after an instrumental delivery warrants a careful scalp and perfusion assessment. [12] [13]
SWELL — the post-instrumental newborn check
Differential Diagnosis
The first differential is between the three scalp swellings themselves, and it is solved by the suture line and the consistency. Caput crosses sutures, pits, and is present at birth; cephalohaematoma stops at the suture of one bone and is firm and non-pitting; subgaleal crosses the sutures and fontanelle and is diffuse and boggy. Misreading a subgaleal bleed as "just a big caput" is the classic and dangerous error, because caput does not cause shock and a subgaleal bleed does. [3] [6]
The next question is whether the scalp bleed is the whole story or the visible part of an intracranial injury. An epidural haematoma may coexist with a cephalohaematoma and an underlying skull fracture, especially after a vacuum extraction, and may require neurosurgical evacuation; the clues are neurological signs, a falling haematocrit out of proportion to the scalp bleed, or a seizure. A subdural or subarachnoid haemorrhage from the shearing of bridging veins presents with seizures, apnoea, irritability, a bulging fontanelle, or a depressed conscious state. [12] [13]
Three scalp swellings — the discriminator table
Beyond the birth-trauma family, several non-traumatic causes of scalp swelling must be considered. An infected cephalohaematoma or a subgaleal abscess may present weeks after birth as a fluctuant, erythematous, tender, febrile swelling, and needs antibiotics and surgical drainage rather than observation. A coagulopathy-driven spontaneous bleed — haemophilia, severe vitamin K deficiency, or alloimmune thrombocytopenia — can produce a scalp bleed with little or no trauma and demands a haematology workup. Rarely, a vascular malformation or tumour of the scalp presents as a swelling in the newborn period and is distinguished by its imaging appearance. [15]
The trickiest differential is the well-looking infant with a large cephalohaematoma: is it an uncomplicated cephalohaematoma to be observed, or is there an underlying skull fracture or a small intracranial bleed? The answer comes from the neurological examination and the skull radiograph or cranial ultrasound: a well infant with a normal examination and no fracture is observed, while any neurological sign, a depressed fracture, or an unexplained fall in haematocrit prompts imaging. [12] [13]
Clinical & Bedside Assessment
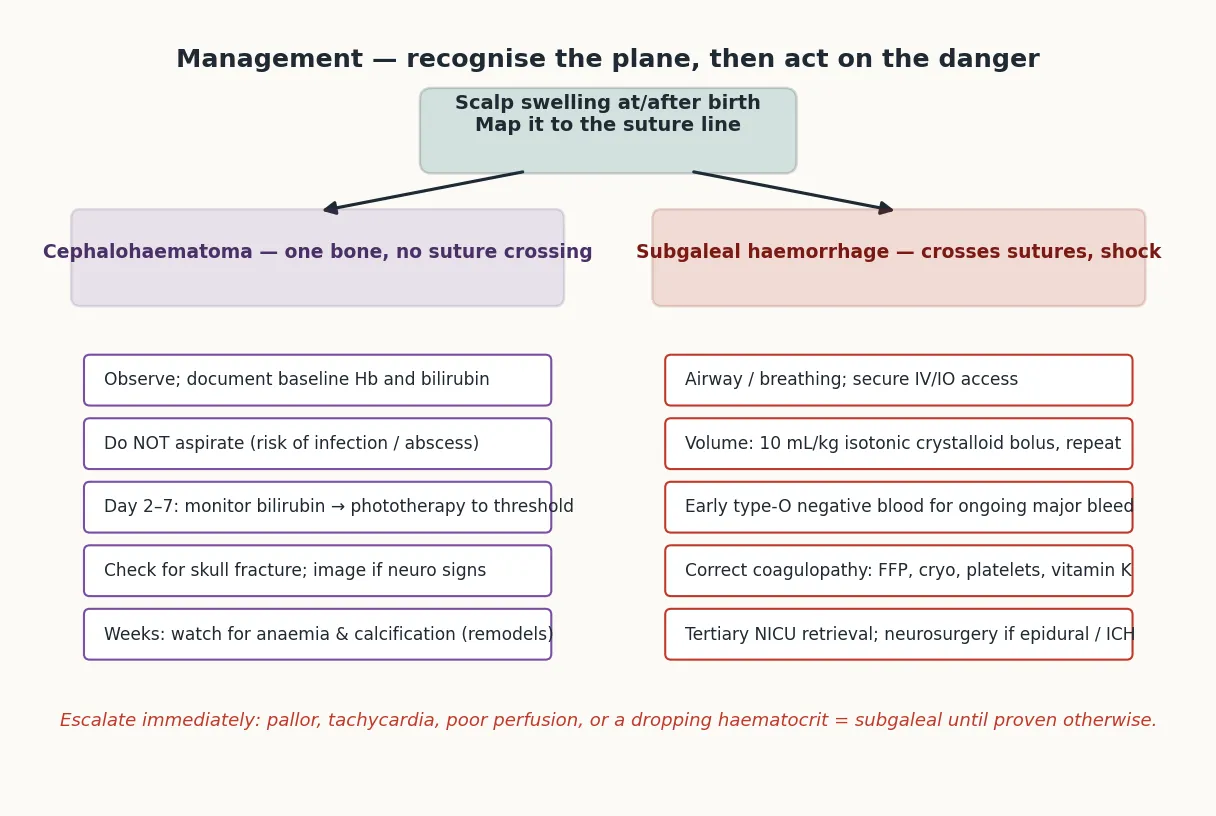
The focused assessment of a newborn with a scalp swelling is performed in a fixed order so that the dangerous subgaleal bleed is not missed behind a reassuring-looking swelling. First inspect and palpate the swelling: map it against the suture lines — does it stop at the suture of one bone, or does it cross the sagittal and lambdoid sutures and the anterior fontanelle? Is it firm and well-circumscribed, or diffuse, boggy and fluctuant? Does it pit? Is there ecchymosis tracking into the eyelids, forehead or neck? [3] [8]
Then assess the systemic perfusion, because the scalp tells you the plane and the perfusion tells you the danger. Look at the colour (pallor is the key sign of blood loss), the capillary refill (central, more than 2 to 3 seconds is abnormal), the heart rate (tachycardia is the earliest sign of hypovolaemia), and the blood pressure and pulse pressure. A boggy diffuse swelling with pallor and tachycardia is a subgaleal haemorrhage in trouble; a firm localised swelling in a pink, well-perfused infant is almost certainly a cephalohaematoma. [3] [4]
For any infant delivered by vacuum or forceps — and especially after a difficult delivery, multiple cup detachments, or a failed instrumental delivery — a structured observation protocol is mandatory for the first hours. This means serial heart rate, respiratory rate, colour, capillary refill, blood pressure, scalp and head circumference, and anterior fontanelle checked at set intervals, with a low threshold to act if any of them deteriorates. The protocol exists precisely because a subgaleal bleed can declare itself hours after a delivery that seemed straightforward. [3] [9]
Assess also for a coexisting intracranial injury. Examine the tone and the conscious state, look for seizures or apnoea, and palpate the anterior fontanelle — though remember it may be obscured by an overlying subgaleal bleed. Any neurological abnormality in an infant with a scalp swelling is an indication for cranial imaging. Finally, take a precise birth history: which instrument, how many pulls and cup detachments, the total application time, whether the instrumental delivery failed and was converted to caesarean, and whether vitamin K was given. This history sets the pre-test probability and is a direct question at viva. [9] [10]
Investigations
The investigations are chosen to quantify the blood loss, exclude a coagulopathy, detect the evolving hyperbilirubinaemia, and look for an underlying fracture or intracranial injury. The core blood set is a serial haemoglobin or haematocrit (the trend matters more than the first value), a coagulation screen (prothrombin time or INR, activated partial thromboplastin time, and fibrinogen), a blood group and direct antiglobulin test, and — over the following days — a serial serum bilirubin. [3] [4]
A coagulation screen is essential in any significant scalp bleed, for two reasons. First, an unrecognised coagulopathy — haemophilia, severe vitamin K deficiency, maternal antiplatelet antibodies, or a consumptive disseminated intravascular coagulation driven by the bleed itself — may be both the cause and the consequence of the haemorrhage, and it must be corrected before the bleed will stop. Second, the products needed (fresh frozen plasma, cryoprecipitate, platelets, vitamin K) are chosen from the abnormal values, so the screen guides treatment. [3]
A serum bilirubin is measured because a cephalohaematoma is a recognised risk factor for hazardous hyperbilirubinaemia: as the sequestered blood breaks down over days, the released bilirubin can push the infant across the phototherapy and even the exchange-transfusion threshold. A large subgaleal bleed does the same, faster, because more blood is reabsorbed. The bilirubin is trended against the gestation- and hour-specific threshold over the first days and weeks. [12] [14]
A skull radiograph detects an underlying linear or depressed skull fracture associated with a cephalohaematoma. Most are linear and need no treatment, but a depressed fracture may need neurosurgical evaluation, and a fracture overlying a venous sinus is a marker of greater force. Cranial ultrasound or computed tomography is indicated when there are neurological signs, a large or rapidly expanding cephalohaematoma, a suspected epidural or intracranial bleed, or an unexplained fall in haematocrit — the scalp bleed may be the visible part of a deeper injury that needs surgery. [12] [13]
The crucial investigation principle is one of tempo: in the unstable infant with a boggy diffuse swelling and poor perfusion, resuscitation precedes investigation. The first bloods are drawn as access is secured and the first fluid bolus is running, but the team does not wait for the haematocrit to return before starting volume. The confirmatory bloods and imaging follow resuscitation, not the other way around. [1] [3]
Management — Resuscitation
The immediate priority in a newborn with a significant subgaleal haemorrhage is airway, breathing, and circulatory access with volume resuscitation. Secure intravenous or intraosseous access early — peripheral access may be difficult in a shocked, oedematous infant — and send the baseline haematocrit, coagulation screen, blood group and crossmatch as the first bolus is running. [1] [3]
The fluid resuscitation begins with an isotonic crystalloid bolus of 10 mL/kg of normal saline, repeated as guided by the perfusion and the haematocrit. For ongoing major haemorrhage — a bleed that has not stopped, or shock that does not respond to crystalloid — early type-O negative blood is given rather than further clear fluid, because the problem is red-cell loss and giving more crystalloid dilutes the remaining blood and worsens coagulopathy. A falling haematocrit with haemodynamic instability, or a haematocrit below the transfusion threshold for the infant's gestation and postnatal age, is the trigger for a red-cell transfusion. [3] [4]
Normal saline (0.9%) — first-line volume
Dose
10 mL/kg
Any coagulopathy is corrected in parallel with the volume, because the bleed will not stop while the clotting is deranged. Fresh frozen plasma at 10 to 15 mL/kg corrects the prothrombin time and provides clotting factors; cryoprecipitate is given for a low fibrinogen; platelets are transfused for thrombocytopenia with active bleeding; and vitamin K (1 mg intramuscular, or intravenous if there is a bleeding disorder concern) is given if it has not been administered or if there is any possibility of vitamin K deficiency bleeding. These products are chosen from the coagulation screen, not given blindly. [3]
The disposition decision follows the resuscitation. An infant with a significant subgaleal haemorrhage — any shock, any coagulopathy, any ongoing bleed — is retrieved to a tertiary NICU with full monitoring and access to blood products and paediatric surgery. An infant with a small, uncomplicated cephalohaematoma in a well newborn may stay with the mother on the postnatal ward under a monitoring protocol. The threshold to retrieve is deliberately low for subgaleal bleeds, because deterioration can be rapid. [3] [4]
Management — Definitive & Stepwise
The definitive management follows two distinct ladders, one for the uncomplicated cephalohaematoma and one for the significant subgaleal haemorrhage, because the two conditions have almost nothing in common beyond their origin in birth trauma. [3] [8]
For an uncomplicated cephalohaematoma, the management is expectant observation. Document the baseline haematocrit and bilirubin, examine for an underlying skull fracture, reassure the parents, and arrange surveillance. Do not aspirate or incise the haematoma — the routine aspiration of an uncomplicated cephalohaematoma is avoided because of the risk of introducing infection and converting a sterile collection into an abscess. Over the first days and weeks, monitor the bilirubin and give phototherapy to the threshold, monitor the haemoglobin for evolving anaemia, and watch for the rare complications — a calcifying haematoma, an infected haematoma, or an underlying intracranial injury that declares itself late. [8] [12]
For a significant subgaleal haemorrhage, the management is the resuscitation described above, followed by ongoing intensive care: serial haematocrit and coagulation, titrated blood and product support, correction of any acidosis, and surveillance for the secondary hyperbilirubinaemia as the blood is reabsorbed. The escalation triggers are explicit: persistent haemodynamic instability despite volume and blood, an expanding lesion, a suspected epidural or intracranial bleed needing neurosurgery, or a severe refractory coagulopathy requiring haematology. [3] [4]
Management ladder for birth scalp swelling
Map the swelling to the suture line — does it cross the sutures and fontanelle?
Assess perfusion — colour, capillary refill, heart rate, blood pressure
If diffuse/boggy + poor perfusion: subgaleal haemorrhage — secure access, start 10 mL/kg isotonic crystalloid
Send haematocrit, coagulation, group and crossmatch; give early type-O negative blood for ongoing major bleed
Correct coagulopathy: FFP 10 to 15 mL/kg, cryoprecipitate, platelets, vitamin K as indicated
Retrieve to tertiary NICU; neurosurgery if epidural or intracranial bleed
If firm/localised + well infant: cephalohaematoma — observe, do NOT aspirate
Monitor bilirubin (phototherapy to threshold) and haemoglobin over days to weeks
The management of an infected cephalohaematoma is the exception to the no-aspiration rule. An infant presenting days to weeks later with a fluctuant, erythematous, tender, febrile swelling over the original haematoma site has an infected collection or abscess, and needs antibiotics covering skin organisms (such as a antistaphylococcal agent) plus surgical drainage and cultures. This is a different disease from the sterile birth cephalohaematoma and is managed as a soft-tissue infection. [15]
The prevention and counselling answer closes the management section. The risk of subgaleal haemorrhage is reduced by disciplined operative vaginal delivery — limits on the number of cup detachments and pulls, abandoning the instrument for a caesarean when delivery does not progress, and a neonatal alert whenever a vacuum or forceps has been used so that the observation protocol is triggered. After the event, the family is counselled honestly: the mechanism (shearing of small veins by the instrument), the management (resuscitation and support), and the prognosis (good with early recognition and resuscitation, worse with delay or coagulopathy). [3] [9] [10]
Specific Subtypes & Scenarios
Subgaleal haemorrhage after vacuum delivery is the prototype and the danger scenario. Recognise it early from the diffuse boggy swelling and the systemic signs, resuscitate aggressively with volume and blood, correct any coagulopathy, retrieve to tertiary NICU, and counsel the family on the mechanism and the prognosis. The mortality in severe or under-recognised cases is up to about a quarter, which is why early recognition is the single most important determinant of outcome. [3] [5]
Large or bilateral cephalohaematoma with severe hyperbilirubinaemia is the scenario where the cephalohaematoma stops being benign. As the sequestered blood breaks down over the first days, the bilirubin climbs and the infant crosses the phototherapy and sometimes the exchange-transfusion threshold. Management is bilirubin-trended phototherapy to the gestation- and hour-specific threshold, with exchange transfusion if the threshold is exceeded, alongside monitoring for the concurrent anaemia. [12] [14]
Cephalohaematoma with an underlying skull fracture needs the fracture documented and characterised. A linear fracture is managed conservatively and observed; a depressed fracture may need neurosurgical evaluation, though many "ping-pong" depressions elevate spontaneously; and a fracture over a venous sinus or with an overlying intracranial bleed is the scenario that links to neurosurgery. [13]
Infected cephalohaematoma presenting weeks after birth is a soft-tissue infection rather than a birth injury. The infant has a fluctuant, erythematous, tender, febrile swelling, and management is antibiotics and surgical drainage. The lesson is that a cephalohaematoma that becomes hot, red, or tender is no longer being observed — it is being treated for infection. [15]
The infant with a calcifying cephalohaematoma and skull asymmetry at months of age is usually a cosmetic concern. As the haematoma organises it may calcify, producing a firm contour deformity that alarms the parents; in most infants this remodels over months to a year without surgery, and reassurance is the management. Cosmetic surgery is reserved for the rare persistent deformity. [8]
The newborn with a cephalohaematoma and a coexisting intracranial bleed is the scenario that links this topic to neurosurgery. An epidural haematoma may develop beneath a cephalohaematoma, especially with an underlying skull fracture after a vacuum extraction, and may need surgical evacuation. The clues are neurological signs, a haematocrit that falls out of proportion to the scalp bleed, or a seizure — any of which prompts cranial imaging and neurosurgical involvement. [12] [13]
Complications & Pitfalls
The life-threatening complications are those of subgaleal haemorrhage: hypovolaemic and haemorrhagic shock, a secondary consumptive coagulopathy or disseminated intravascular coagulation, multi-organ failure from prolonged hypoperfusion, and death. These are the reason subgaleal haemorrhage is treated as an emergency and retrieved to a tertiary centre; the mortality in severe cases is real and the morbidity in survivors includes neurodevelopmental impairment from the hypoperfusion. [3] [4]
The common complications of cephalohaematoma are biochemical and delayed rather than circulatory and immediate. The reabsorption of the sequestered blood drives an unconjugated hyperbilirubinaemia that can cross the phototherapy and exchange-transfusion thresholds, with the attendant risk of kernicterus if it is not detected and treated; the same reabsorption can leave the infant anaemic, sometimes enough to need a transfusion. These complications are why a cephalohaematoma is observed, not ignored. [12] [14]
The late complications of cephalohaematoma are a skull contour deformity and calcification — usually remodelling over months — and, rarely, an infected cephalohaematoma or abscess weeks later, which may complicate a calcifying haematoma or follow a (avoided) aspiration. A cephalohaematoma overlying a skull fracture carries the additional risk of a meningitis if the fracture communicates with the meninges, which is a rare but documented scenario. [8] [15]
The classic errors each have a name and a consequence. Dismissing a boggy diffuse swelling as caput succedaneum and missing an evolving subgaleal haemorrhage until shock develops is the cardinal error — caput does not cause shock, and a subgaleal bleed does. Failing to measure a serial haematocrit and bilirubin in an infant with a large cephalohaematoma misses the evolving anaemia and hyperbilirubinaemia. Aspirating an uncomplicated cephalohaematoma risks infection and abscess. And missing a coexisting intracranial bleed because the scalp swelling was attributed to a cephalohaematoma and the neurological signs were not acted on, delays a neurosurgical evacuation. [3] [12]
The medicolegal and safety pitfall is failing to observe and document. After every instrumental delivery, the serial observations, the scalp findings, the decision to escalate, and the personnel involved must be recorded. In a subgaleal haemorrhage that later comes to review, the documentation that the observation protocol was followed and the deterioration was acted on is the defence — and its absence is the liability. [3] [9]
Prognosis & Disposition
Outcome is determined by four factors: the size of the bleed, the speed of recognition and resuscitation, the presence of a coagulopathy or intracranial injury, and the gestational age and comorbidity of the infant. A subgaleal haemorrhage recognised and resuscitated early has a good prognosis; one missed until shock and coagulopathy are established carries the up-to-a-quarter mortality and the neurodevelopmental morbidity of prolonged hypoperfusion. [3] [4]
The prognosis of an uncomplicated cephalohaematoma is excellent. The swelling resolves over weeks to months, the bilirubin and haemoglobin normalise as the blood is reabsorbed, the calcification remodels, and there is no long-term sequel in the great majority. The exceptions are the rare infected cephalohaematoma, the rare persistent skull deformity needing cosmetic surgery, and the cephalohaematoma that was the visible part of an intracranial injury. [8] [12]
The retrieval decision is guided by the level of care needed. Infants retrieved to a tertiary NICU are those with a significant subgaleal bleed (any shock, any coagulopathy, any ongoing bleed), a suspected intracranial injury, or a severe refractory coagulopathy. A stable term infant with a small uncomplicated cephalohaematoma may stay on the postnatal ward under a monitoring protocol with a bilirubin and haemoglobin follow-up plan. During transport, the subgaleal infant is monitored continuously for re-bleeding and shock. [3]
After a significant subgaleal haemorrhage, neurodevelopmental follow-up is essential. Survivors of a severe bleed with hypoperfusion are at elevated risk of neurodevelopmental impairment, and they enter a high-risk follow-up programme with hearing and vision assessment and developmental surveillance. The family is counselled honestly about the mechanism, the acute course, and the prognosis at each stage. [3] [4]
Special Populations
The preterm infant differs in two ways. The scalp tissues are thinner and more fragile, so a given shearing force may do more damage; and the circulating blood volume is smaller, so a subgaleal bleed of a given size reaches shock sooner and the reserve for anaemia is less. Preterm infants also carry a higher baseline risk of hyperbilirubinaemia, so a cephalohaematoma pushes an already-vulnerable infant closer to the threshold. The threshold to investigate and transfuse is lower. [3]
The infant with an underlying bleeding disorder — haemophilia, severe von Willebrand disease, alloimmune thrombocytopenia, or severe vitamin K deficiency (including the infant whose parents declined vitamin K) — may present with a scalp bleed disproportionate to the birth trauma, or with bleeding at other sites. The workup is broader: a full coagulation and platelet screen, factor assays where indicated, and haematology involvement. Correcting the underlying disorder is part of stopping the bleed. [3] [4]
The infant of a mother on anticoagulants (warfarin, or less commonly heparin that crosses influences) or with thrombocytopenia (autoimmune or alloimmune) presents a dual problem: the bleed may be driven by the maternal condition, and the workup must include the maternal drug and platelet history. Vitamin K is given; specific reversal (for warfarin) or platelet support (for thrombocytopenia) is guided by the screen. [3]
In a low-resource setting where point-of-care haematocrit, coagulation testing, and blood products may be limited, the approach relies on clinical recognition — the diffuse boggy swelling, the pallor, the tachycardia — and on early oral or intravenous fluids and urgent referral. The principles are universal: recognise the plane, recognise the shock, resuscitate, and escalate. A subgaleal haemorrhage is a sentinel event in any setting and warrants the highest level of monitoring available. [3]
Counselling differs by the context of the delivery. After an indicated instrumental delivery — one performed for a clear fetal or maternal indication and within safe parameters — the family is counselled that the birth injury was a recognised complication of a necessary intervention. After a delivery where the instrumental attempt was clinically marginal or prolonged, the counselling is more difficult and the medicolegal context sharper; honest disclosure of the mechanism, the acute management, and the prognosis is the standard in both. [9] [10]
Evidence, Guidelines & Regional Differences
The evidence base for the risk of subgaleal haemorrhage is stronger than the evidence base for its treatment, a distinction the viva candidate should hold. On risk, the dose-response with vacuum parameters is well established: the number of cup detachments, the number of pulls, and the total application time each raise the risk of neonatal injury including subgaleal haemorrhage, and these are the parameters the obstetric guidelines limit. The landmark Towner study in the New England Journal of Medicine established that spontaneous vaginal delivery, vacuum, and forceps each carry intracranial-injury risks that differ by mode, reframing birth injury as a problem of instrumental delivery rather than of one device. [7] [9] [10]
On treatment, the evidence is largely observational and consensus-based: early recognition, volume resuscitation, blood and product support, correction of coagulopathy, and tertiary retrieval are endorsed by every review, but specific transfusion thresholds for neonatal subgaleal haemorrhage and the role of agents such as recombinant factor VIIa in refractory bleeding remain weakly supported. The 2025 comprehensive review and earlier calls for early diagnosis and aggressive management set the current standard. [3] [4]
Towner et al., NEJM 1999 — mode of delivery and neonatal intracranial injury
Population-based retrospective cohort of singleton term nulliparous deliveries
Key finding
Operative vaginal delivery (vacuum, forceps, or both) was associated with a higher rate of neonatal intracranial injury than spontaneous or caesarean delivery; the absolute risk remained low but the relative increase framed birth injury as an instrumental-delivery problem.
Practice change
Established the modern scrutiny of operative vaginal delivery and the drive to limit pulls and detachments; the bedrock citation for birth-trauma risk.
Regional guidance converges on the principles and differs in the obstetric detail. ANZ guidance (RANZCOG on operative vaginal delivery, with neonatal alert protocols for any vacuum or forceps birth) and the UK (RCOG green-top guidance on operative vaginal delivery, recommending a maximum number of cup detachments and pulls and a structured neonatal observation) and the US (ACOG and the Neonatal Resuscitation Program's emphasis on recognising birth injury and shock) all share the recognition-and-resuscitation philosophy. They differ in the specific obstetric limits and the retrieval infrastructure. [1] [9] [10]
All three regions converge on the early recognition of subgaleal haemorrhage, the structured post-instrumental observation protocol, and the volume-and-blood resuscitation principle. The differences are practical: ANZ has a strong neonatal retrieval network (NETS and equivalents) and a RANZCOG-led operative vaginal delivery framework with neonatal alert; the UK (RCOG green-top) sets explicit maximum numbers of cup detachments and pulls; the US (ACOG and NRP) provides the most widely taught neonatal resuscitation algorithm globally. For exams, cite the shared recognition-and-resuscitation principle and the regional obstetric guideline (RANZCOG, RCOG, ACOG). [1] [10]
The evidence is still moving in three areas. Specific transfusion thresholds for neonatal subgaleal haemorrhage remain borrowed from the general neonatal transfusion literature rather than trial-derived for this condition. Recombinant factor VIIa and other pro-haemostatic agents have been reported in refractory cases but are not standard. And conservative management of small subgaleal bleeds in haemodynamically stable infants is increasingly described, but the threshold for observation versus active resuscitation is clinical and protocol-driven rather than evidence-defined. [3] [4]
Exam Pearls
The one-liner anatomical distinction: cephalohaematoma is subperiosteal and cannot cross the suture line; subgaleal haemorrhage is subaponeurotic and crosses all sutures and the fontanelle; caput is subcutaneous and also crosses sutures. The suture line is the single best bedside discriminator. [3] [8]
The lethal one-liner: a subgaleal haemorrhage can conceal enough blood to kill a newborn through hypovolaemic shock, because the subaponeurotic space is large. [3] [4]
The delayed one-liner for cephalohaematoma: it drives anaemia and hyperbilirubinaemia over the first days and weeks as the blood is reabsorbed — a large cephalohaematoma is a recognised risk factor for hazardous jaundice and for late anaemia. [12] [14]
The vacuum dose-response one-liner: subgaleal haemorrhage risk rises with the number of cup detachments, the number of pulls, and the total application time — the parameters the obstetric guidelines limit. [9]
The management one-liner: an uncomplicated cephalohaematoma is observed and must not be aspirated (risk of infection), while a subgaleal haemorrhage is resuscitated with volume, blood, and coagulation correction, and retrieved to a tertiary NICU. [3] [8]
The classic viva trap: dismissing a boggy diffuse swelling as caput succedaneum and missing an evolving subgaleal haemorrhage until shock develops. The counter-trap is failing to measure a serial haematocrit and bilirubin in a large cephalohaematoma and missing the delayed anaemia or kernicterus. [3] [12]
References
- [1]Aziz K Part 5: Neonatal Resuscitation 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Pediatrics, 2021.PMID 33087555
- [2]Madar J European Resuscitation Council Guidelines 2021: Newborn resuscitation and support of transition of infants at birth. Resuscitation, 2021.PMID 33773829
- [3]Babata K Subgaleal hemorrhage in neonates: a comprehensive review and summary recommendations. J Perinatol, 2025.PMID 39284927
- [4]Colditz MJ Subgaleal haemorrhage in the newborn: A call for early diagnosis and aggressive management. J Paediatr Child Health, 2015.PMID 25109786
- [5]Florentino-Pineda I Subgaleal hemorrhage in the newborn infant associated with silicone elastomer vacuum extractor. J Perinatol, 1994.PMID 8014708
- [6]Reid J Neonatal subgaleal hemorrhage. Neonatal Netw, 2007.PMID 17710955
- [7]Towner D Effect of mode of delivery in nulliparous women on neonatal intracranial injury. N Engl J Med, 1999.PMID 10580069
- [8]Pollina J Cranial birth injuries in term newborn infants. Pediatr Neurosurg, 2001.PMID 11641618
- [9]Ghidini A Neonatal complications in vacuum-assisted vaginal delivery: are they associated with number of pulls, cup detachments, and duration of vacuum application? Arch Gynecol Obstet, 2017.PMID 27677283
- [10]Muraca GM Maternal and neonatal trauma following operative vaginal delivery. CMAJ, 2022.PMID 35012946
- [11]Liu LY Neonatal Subgaleal Hematoma from Trauma During Vaginal Delivery without Instrument Use. Pediatr Dermatol, 2017.PMID 27981624
- [12]Kim HM Intracranial hemorrhage in infants with cephalohematoma. Pediatr Int, 2014.PMID 24274929
- [13]Park SH Surgical treatment of subacute epidural hematoma caused by a vacuum extraction with skull fracture and cephalohematoma in a neonate. Pediatr Neurosurg, 2006.PMID 16714873
- [14]Watchko JF Identification of neonates at risk for hazardous hyperbilirubinemia: emerging clinical insights. Pediatr Clin North Am, 2009.PMID 19501698
- [15]Karagol BS A linear fracture and meningitis associated with non-infected cephalohematoma in a neonate. Neuropediatrics, 2010.PMID 21445821