Paeds · fetal-neonatal-and-perinatal
Congenital and perinatally acquired infections
Also known as TORCH infections · Congenital infections · Perinatally acquired infection · Mother-to-child transmitted infection · Vertical transmission of infection
Fellowship guide to congenital and perinatally acquired infections: the expanding TORCH differential, mechanisms of mother-to-child transmission, the pattern-recognition signs of congenital infection, serology and PCR interpretation, organism-specific therapy with doses (CMV, toxoplasmosis, syphilis, HSV, parvovirus, HIV, hepatitis B, rubella, Zika), and the lifelong surveillance that follows.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Congenital and perinatally acquired infections are infections transmitted from mother to child during pregnancy, labour, delivery, or the early postnatal period. They range from clinically silent to lethal, and the damage they cause is determined less by the identity of the organism alone than by the timing of infection, the inoculum, and the maturity of the fetal immune response. The classical mnemonic TORCH - Toxoplasmosis, Other (syphilis, varicella, parvovirus), Rubella, Cytomegalovirus, and Herpes simplex - is a useful entry point, but it understates the modern list, which now firmly includes Zika virus and Chagas disease alongside the preventable perinatally transmitted hepatitis B, hepatitis C, and human immunodeficiency virus. [10]
A congenital infection is acquired in utero, almost always before birth, via transplacental haematogenous spread or ascending infection through ruptured or intact membranes. A perinatally acquired infection is contracted during passage through the birth canal or in the immediate postnatal period, while postnatally acquired infection is transmitted after birth through breastfeeding, blood exposure, or close contact. The distinction matters: congenital infection produces the structural and neurodevelopmental malformations of the TORCH phenotype, whereas perinatal acquisition more often causes acute neonatal disease such as disseminated herpes simplex or early-onset bacterial sepsis. [10]
Cytomegalovirus is the commonest congenital infection in developed countries, affecting around 0.5 to 1 per cent of all live births, and it is the leading non-genetic cause of sensorineural hearing loss and neurodevelopmental disability in children. By contrast, rubella - once the archetypal teratogen - has been driven to near-elimination by universal vaccination, and congenital rubella syndrome is now a disease of unvaccinated populations and migrant communities. Congenital syphilis, however, is resurgent globally and demands vigilance. [7]
Epidemiology & Risk Factors
Cytomegalovirus infects approximately 0.5 to 1 per cent of live births in high-income settings. Around 10 per cent of infected newborns are symptomatic at birth with the classic cytomegalic inclusion disease phenotype, and a further 10 to 15 per cent of apparently asymptomatic infants go on to develop late-onset sequelae - most importantly progressive sensorineural hearing loss. Seroprevalence is higher in lower socioeconomic groups and in communities with early childbearing-age contact, and primary maternal infection carries a roughly 30 to 40 per cent risk of fetal transmission, far exceeding the 1 to 2 per cent risk of transmission after non-primary (reactivation or reinfection) infection. [1]
Toxoplasma gondii seroprevalence varies widely by region and dietary customs, and maternal seroconversion carries an overall vertical transmission risk that rises steeply with gestational age at infection - from less than 15 per cent in the first trimester to over 60 per cent near term - while the severity of fetal disease falls as gestation advances. Congenital syphilis incidence has risen sharply in many high-income countries over the last decade, driven by gaps in antenatal screening, late or inadequate maternal treatment, and socioeconomic deprivation; it remains entirely preventable with a single dose of benzathine penicillin at least 30 days before delivery. [7]
The major risk factors across the group are primary maternal infection in pregnancy (highest transmission risk), absent or incomplete antenatal screening, late or inadequate maternal treatment, immunosuppression, intravenous drug use, multiple sexual partners, and exposure to animal reservoirs (cats and undercooked meat for toxoplasmosis, mosquitoes for Zika). For perinatally acquired HIV and hepatitis B, the dominant risk factor is a mother who is positive for the virus but has not received antenatal care, antiretroviral therapy, or - in the case of hepatitis B - timely birth-dose active-passive immunoprophylaxis. [4]
Pathophysiology
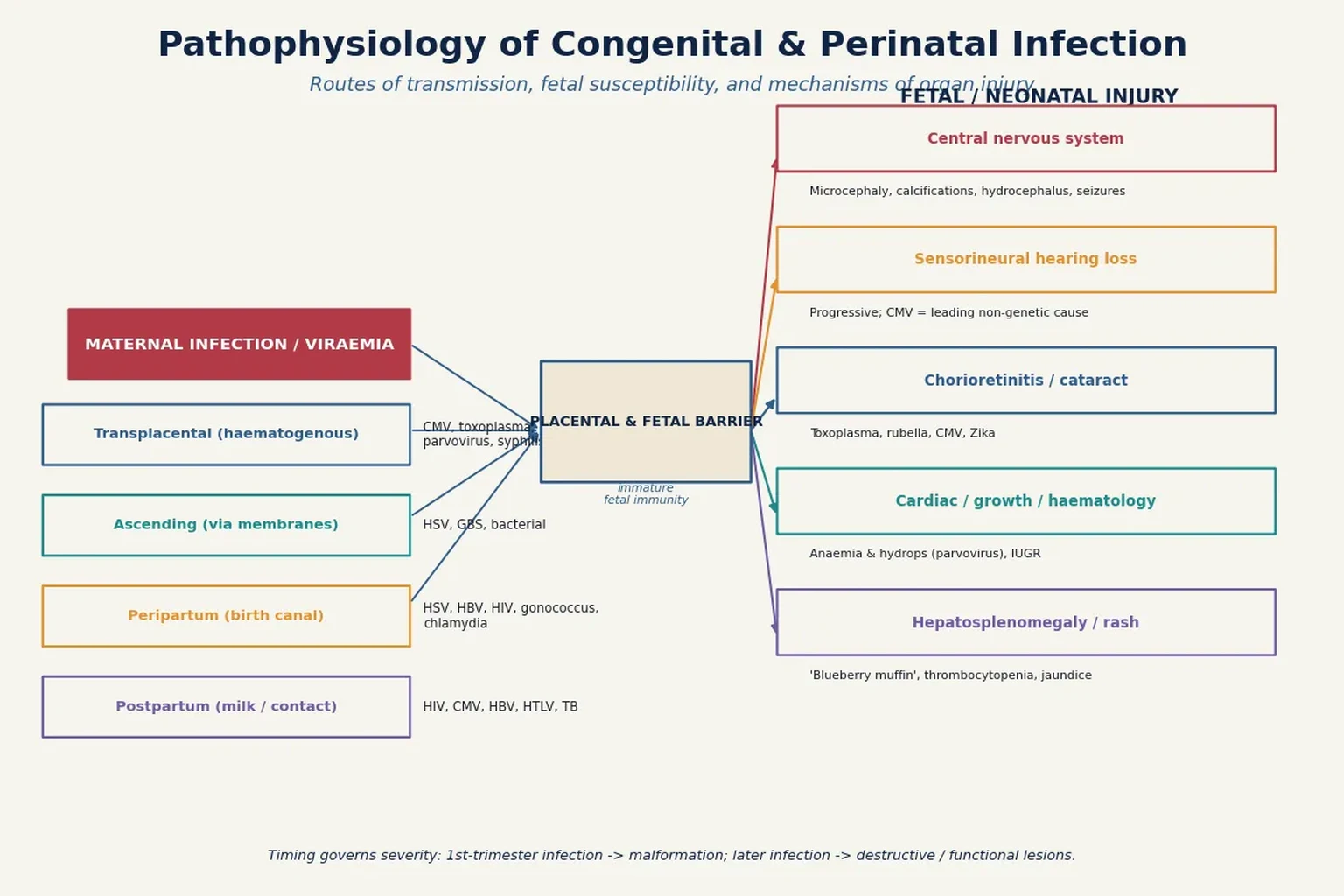
The route of transmission defines the clinical syndrome. Transplacental haematogenous spread delivers organisms directly into the fetal circulation and underlies the congenital infections - CMV, toxoplasma, rubella, parvovirus B19, syphilis, Zika and varicella. Ascending infection through the membranes, most often after rupture, seeds the amniotic fluid and is aspirated or swallowed. Peripartum acquisition occurs as the infant traverses a colonised birth canal, accounting for neonatal herpes simplex, gonococcal ophthalmia, chlamydial conjunctivitis, hepatitis B, HIV, and group B streptococcal disease. Postnatal transmission is predominantly via breast milk (HIV, HTLV-I, CMV) or household contact. [10]
The timing of infection relative to organogenesis is the single most important determinant of the type of damage. First-trimester infection, during maximal cellular differentiation and organ formation, produces structural malformations - exemplified by congenital rubella syndrome with its cardiac defects, cataracts, and sensorineural deafness. Later infection, after organogenesis is largely complete, produces destructive or functional lesions such as tissue necrosis, inflammation, and progressive hearing loss. This principle explains why cytomegalovirus, which can infect at any gestation, produces a wider and more varied phenotype than rubella. [10]
Fetal vulnerability is amplified by an immature immune system. The fetus mounts a limited IgM response and relies almost entirely on transplacentally acquired maternal IgG, which is transferred predominantly in the third trimester; consequently the very preterm infant is particularly defenceless. Parvovirus B19 exploits this by binding the P antigen on fetal erythroid precursors, causing a pure red-cell aplasia that, in a fetus unable to mount an effective response, leads to high-output cardiac failure, severe anaemia, and hydrops fetalis. [5]
Once infection is established, the mechanisms of injury are a combination of direct cytopathic damage, immune-mediated inflammation, vascular injury, and impaired cellular proliferation. The 'blueberry muffin' rash reflects dermal extramedullary haematopoiesis in response to severe congenital infection and haemolysis, while intracranial calcifications (periventricular in CMV, diffuse in toxoplasmosis) mark the sites of tissue necrosis and mineralisation. [10]
Classification
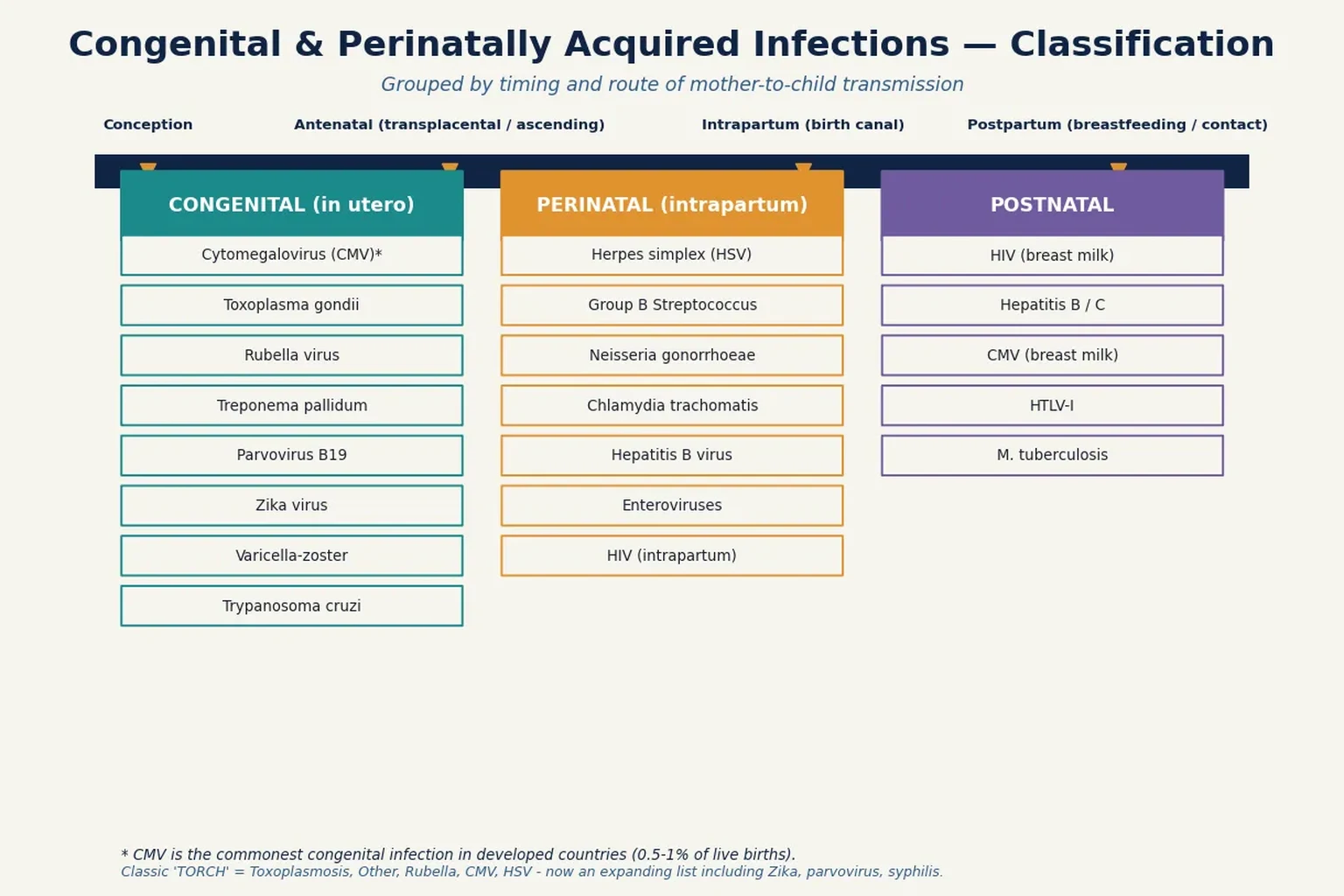
The classical TORCH framework remains a memorable anchor - Toxoplasmosis, Other, Rubella, CMV, and Herpes simplex - but clinicians must think beyond it. The 'Other' category has expanded to include syphilis, varicella-zoster, parvovirus B19, Zika virus, and Trypanosoma cruzi (Chagas disease), and the preventable bloodborne viruses (hepatitis B and C, HIV) are properly considered alongside the TORCH group because they share the vertical-transmission pathway and demand a structured prevention strategy. [10]
Within each organism it is useful to separate the four clinical phenotypes: the asymptomatic infected newborn (the majority for CMV), the neonate with the classic multi-system congenital infection syndrome, the infant with isolated or late-onset sequelae such as progressive hearing loss, and the stillbirth or fetal hydrops presentation. This stratification guides the depth of investigation and the intensity of surveillance. [1]
Clinical Presentation
The clinical presentation spans a spectrum from the entirely asymptomatic newborn to the severely ill multi-organ-infected infant. The hallmark of the symptomatic congenital infection syndrome is the combination of growth restriction, hepatosplenomegaly, jaundice, a petechial or purpuric rash, thrombocytopenia, and neurological abnormalities. This 'cytomegalic inclusion disease' phenotype is the prototype, but elements of it appear in symptomatic toxoplasmosis, rubella, syphilis, and enteroviral infection. [10]
Neurological involvement is the most consequential feature and the main driver of long-term disability. Microcephaly, intracranial calcifications, ventriculomegaly, hydrocephalus, cerebral atrophy, seizures, and abnormal tone may all be present or evolve over the first months. Cytomegalovirus characteristically produces periventricular calcifications, whereas toxoplasmosis tends to produce scattered, diffuse cerebral calcifications and chorioretinitis. Congenital Zika syndrome produces a distinctive severe microcephaly with overlapping suture lines, scalp rugae, and subcortical calcifications. [8]
Sensory organ involvement is common and may be the only manifestation. Sensorineural hearing loss is the most frequent sequela of congenital CMV and may be absent at birth but emerge and progress over the first years. Chorioretinitis occurs in toxoplasmosis, rubella, and CMV, while congenital cataracts - classically a 'salt-and-pepper' retinopathy with cataract and congenital heart disease - point to rubella. The 'blueberry muffin' rash of dermal haematopoiesis, purpura, and thrombocytopenia rounds out the haematological phenotype. [9]
Pattern-recognition clues by organism
Microcephaly + periventricular calcifications + SNHL -> CMV
Diffuse intracranial calcifications + chorioretinitis + hydrocephalus -> toxoplasmosis
Cataracts + PDA / pulmonary stenosis + SNHL -> rubella
Hydrops fetalis / severe anaemia -> parvovirus B19
Maculopapular rash + snuffles + hepatosplenomegaly + long-bone changes -> syphilis
Severe microcephaly + arthrogryposis + subcortical calcifications -> Zika
Vesicles + hepatitis + encephalitis (day 2-3 wk) -> herpes simplex
Differential Diagnosis
The differential diagnosis of suspected congenital infection is deliberately broad because the non-specific multi-system phenotype overlaps with metabolic, genetic, and haematological disease. Inborn errors of metabolism - particularly peroxisomal disorders, congenital disorders of glycosylation, and lysosomal storage diseases - can present with hepatosplenomegaly, growth restriction, cataracts, and neurological deterioration. Chromosomal anomalies and syndromic microcephalies (such as Seckel, Meier-Gorlin, or primary microcephaly genes) must be considered when microcephaly is the dominant finding. [10]
Rhesus and ABO haemolytic disease can mimic the jaundice, anaemia, and hepatosplenomegaly of congenital infection, and severe early-onset sepsis with group B streptococcus or Escherichia coli produces an indistinguishable picture of multi-organ failure. Neonatal alloimmune thrombocytopenia causes petechiae and purpura identical to those of congenital infection, and congenital leukaemia (transient myeloproliferative disorder in Down syndrome) can mimic the 'blueberry muffin' rash. Structural causes of hydrops fetalis - anaemias, cardiac arrhythmia, twin-twin transfusion, and lymphatic malformations - must be excluded when parvovirus is being considered. [5]
A targeted infection screen is therefore best interpreted alongside a metabolic workup (plasma amino acids, urine organic acids, acylcarnitines), a karyotype or chromosomal microarray when dysmorphism is present, a direct antiglobulin test and bilirubin fractionation for haemolysis, and a careful family history. The diagnosis of congenital infection is one of pattern recognition and exclusion, supported by specific microbiology. [10]
Clinical & Bedside Assessment
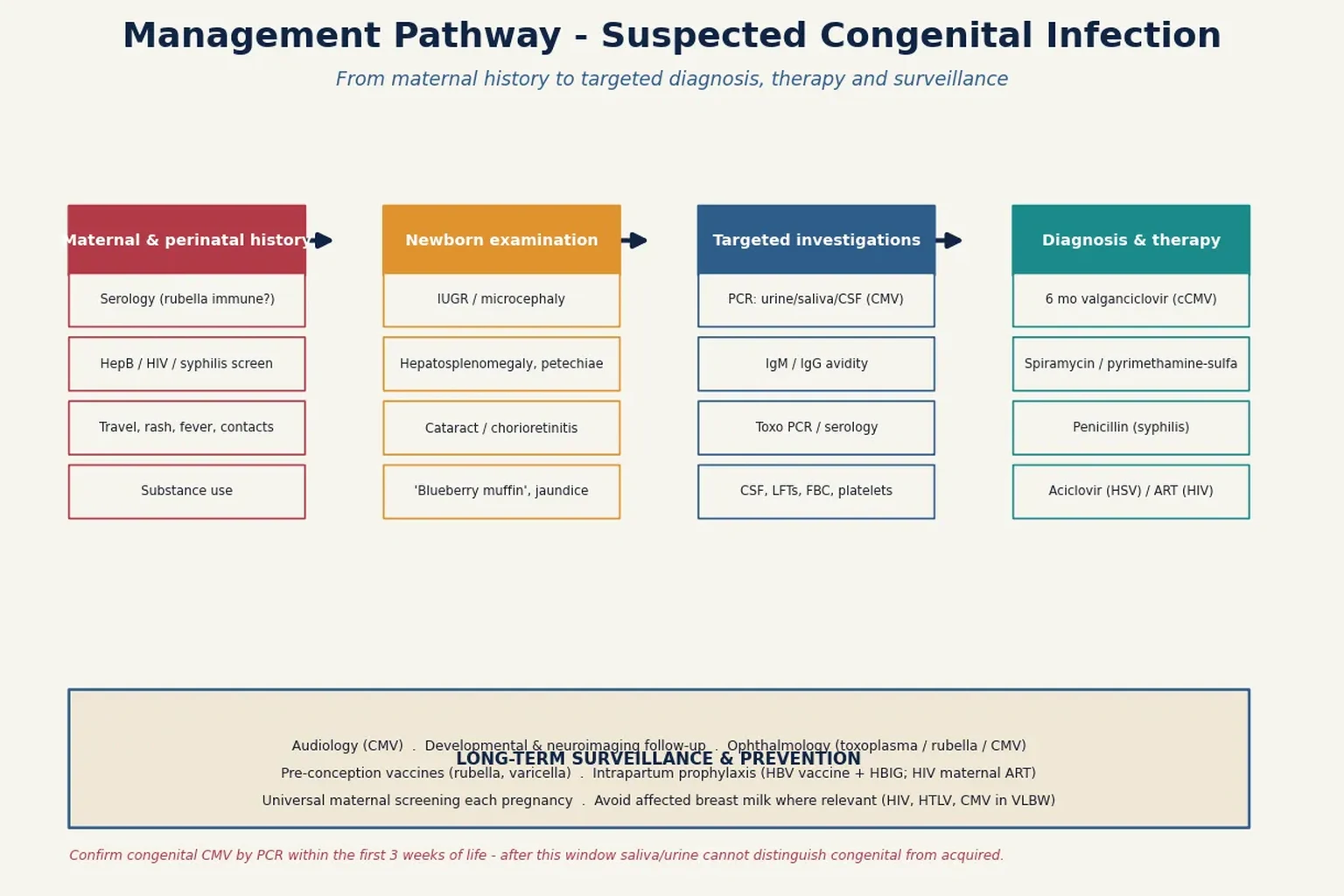
Begin with the maternal and perinatal history, because the single most useful piece of information is usually there. Establish the maternal serological status for rubella, hepatitis B, HIV, and syphilis; document any antenatal illness, rash, fever, lymphadenopathy, or contact with cats, undercooked meat, or mosquitoes; and record the results of any antenatal imaging that showed growth restriction, calcifications, echogenic bowel, ventriculomegaly, or hydrops. Note intravenous drug use, sexual history, and the adequacy of any antenatal treatment. [10]
Examine the newborn systematically. Measure head circumference, length, and weight and plot them against gestational age, because symmetric intrauterine growth restriction with a small head is a strong clue. Inspect the skin for petechiae, purpura, vesicles, and the purplish papules of a 'blueberry muffin' rash. Palpate for hepatosplenomegaly. Examine the eyes for cataracts (using the red reflex), chorioretinitis, and microphthalmia. Auscultate the heart for murmurs of structural disease. Examine the long bones for signs of syphilitic periostitis, palpate the abdomen for masses, and perform a full neurological assessment for tone, seizures, and abnormal movements. [10]
Hearing assessment is mandatory in any infant with suspected congenital infection. The automated newborn hearing screen may be passed despite early or fluctuating CMV-related loss, so a failed screen or any risk factor warrants referral for diagnostic auditory brainstem response testing. Given the high prevalence of CMV-related progressive hearing loss, targeted CMV screening of infants who fail the newborn hearing screen is an increasingly advocated strategy. [1]
Investigations
The diagnostic strategy is targeted, not blanket. For suspected congenital cytomegalovirus, the gold standard is detection of the virus by polymerase chain reaction in urine or saliva collected within the first three weeks of life; after this window, postnatally acquired CMV (including from breast milk) cannot be distinguished from congenital infection. Blood, cerebrospinal fluid, and dried blood spot (Guthrie card) PCR are useful adjuncts, with retrospective testing of the neonatal blood spot valuable when the diagnosis is considered late. [1]
Serology has a defined but limited role. Maternal IgG avidity testing distinguishes recent from remote infection - low avidity indicates primary infection within the preceding three to four months and is most useful in the first trimester. Fetal or neonatal IgM indicates de novo immune response, but its sensitivity and specificity vary by organism and assay. For toxoplasmosis, PCR of amniotic fluid (performed after 18 weeks and at least four weeks after maternal seroconversion) is the prenatal diagnostic test of choice. For syphilis, a non-treponemal test (RPR or VDRL) quantifies disease activity while a treponemal-specific test (TPPA) confirms past or present infection; both are needed in the neonate and interpreted against maternal titres. [7]
Supportive investigations include a complete blood count (anaemia, thrombocytopenia, eosinophilia, neutropenia), liver function tests (raised transaminases, conjugated hyperbilirubinaemia), and cerebrospinal fluid analysis if neurological involvement is suspected. Neuroimaging is essential: cranial ultrasound identifies periventricular calcifications and ventriculomegaly, while MRI better delineates cortical malformations, migrational abnormalities, and cerebellar involvement. An ophthalmology assessment, audiology referral, and - where indicated - echocardiography and long-bone radiographs complete the workup. For hepatitis B, test the infant's hepatitis B surface antigen and antibody status after the prophylaxis series is complete, not at birth. [6]
Management - Resuscitation
Most neonates with congenital infection are haemodynamically stable and require no resuscitation beyond routine delivery-room care. The exceptions are the infant with overwhelming sepsis from perinatally acquired HSV, the hydropic or anaemic fetus with parvovirus B19 infection, and the infant with congenital infection complicated by severe thrombocytopenia, coagulopathy, or cardiogenic shock. In these situations, standard neonatal resuscitation applies: secure the airway, support breathing, establish intravenous access, and treat shock with judicious fluid boluses and inotropes. [10]
A profoundly anaemic hydropic neonate with parvovirus B19 infection may require a partial exchange transfusion or simple transfusion with cytomegalovirus-negative, irradiated packed red cells. In the antenatal setting, severe fetal anaemia from parvovirus is treated with intrauterine transfusion, which dramatically improves survival: in one large prospective series, 84.6 per cent of severely hydropic transfused fetuses survived, whereas all non-transfused severely hydropic fetuses died. [5]
Neonatal herpes simplex is the perinatal infection most likely to present as acute collapse. The three presentations - skin-eye-mouth disease, encephalitis, and disseminated disease with hepatitis - may overlap, and disseminated disease carries the highest mortality. When HSV is suspected, obtain surface swabs and CSF for PCR, check liver function, and start intravenous aciclovir 60 mg per kg per day in three divided doses without waiting for confirmation, because early treatment is the single biggest determinant of survival and neurological outcome. [3]
Resuscitation priorities in acutely unwell perinatal infection
Assess ABC: airway, breathing, circulation - oxygen or PPV as needed
Establish IV access; draw bloods including glucose, FBC, LFTs, coagulation
Severe parvovirus anaemia/hydrops: CMV-negative irradiated packed cell transfusion
Suspected disseminated HSV: swabs + CSF PCR, start aciclovir 60 mg/kg/day immediately
Shock: 10 mL/kg isotonic crystalloid, reassess, inotropes if refractory
Correct hypoglycaemia, thrombocytopenia and coagulopathy
Management - Definitive & Stepwise
Treatment is organism-specific, and for the major congenital pathogens it is now evidence-based. For symptomatic congenital CMV with central nervous system involvement, six months of oral valganciclovir (16 mg per kg per dose, twice daily) improves both long-term hearing and neurodevelopmental outcomes compared with six weeks of therapy, as shown in the landmark randomised trial by Kimberlin and colleagues. Treatment is generally reserved for infants with symptomatic central nervous system or sensorineural disease; the role of antiviral therapy for moderately symptomatic or isolated hearing-loss presentations is the subject of ongoing trials. Neutropenia is the principal adverse effect and requires monitoring of the full blood count during therapy. [1]
Congenital toxoplasmosis is treated with pyrimethamine and sulfadiazine plus folinic acid, typically for one year; spiramycin is used in maternal infection before fetal infection is confirmed, to reduce transplacental transmission, but it does not treat established fetal disease. The evidence base for prenatal treatment is weak - the SYROCOT individual-patient-data meta-analysis found only modest evidence that early treatment reduces transmission and no clear evidence that prenatal therapy reduces clinical manifestations in infected infants, a finding that has challenged long-standing European practice. Congenital syphilis is treated with intravenous or intramuscular aqueous crystalline penicillin G (50,000 units per kg per dose, 12-hourly in the first week then 8-hourly) for 10 days, with the whole strategy underpinned by maternal screening and treatment with benzathine penicillin at least 30 days before delivery. [2]
For the preventable bloodborne viruses, treatment is primarily prevention. Hepatitis B is prevented by hepatitis B immunoglobulin plus the first dose of hepatitis B vaccine within 12 hours of birth for infants of HBsAg-positive mothers, completing the vaccine series, and - for mothers with high viral loads - maternal antiviral prophylaxis (tenofovir) in the third trimester; this combination reduces perinatal transmission to below 5 per cent and is cost-effective. Perinatal HIV is prevented by maternal combination antiretroviral therapy, choice of mode of delivery, avoidance of breastfeeding where safe alternatives exist, and neonatal prophylaxis. When a mother has not received antenatal antiretrovirals, a two-drug (zidovudine plus three doses of nevirapine) or three-drug infant regimen is superior to zidovudine alone for preventing intrapartum HIV transmission, with the two-drug regimen carrying less toxicity. [4]
TREAT the organism
Supportive and preventive care runs in parallel: nutritional support, correction of anaemia and thrombocytopenia, treatment of seizures, and - critically - the assurance that every case is notified to public health, contacts are traced, and partner and family screening is arranged, because the index case of congenital syphilis or HIV often reveals an unrecognised maternal infection with implications for siblings and future pregnancies. [7]
Specific Subtypes & Scenarios
Congenital cytomegalovirus is the single most important congenital infection in developed countries because of its frequency and its burden of sensorineural hearing loss and neurodevelopmental disability. Around 90 per cent of infected infants are asymptomatic at birth, yet 10 to 15 per cent of these develop late sequelae - principally progressive hearing loss - making CMV the leading non-genetic cause of childhood deafness. Symptomatic infants show the cytomegalic inclusion disease triad of petechiae, hepatosplenomegaly, and thrombocytopenia, often with microcephaly, periventricular calcifications, chorioretinitis, and sensorineural hearing loss. [1]
Congenital toxoplasmosis classically presents with the triad of hydrocephalus, intracranial calcifications, and chorioretinitis, but the spectrum is wide and many infants are asymptomatic at birth, with chorioretinitis emerging years later. The classic 'Sabin's tetrad' (hydrocephalus, chorioretinitis, convulsions, intracranial calcifications) is now uncommon because of antenatal screening and treatment in endemic regions. Transmission risk rises with gestational age at seroconversion while severity falls, so late third-trimester infection is common but usually mild. [2]
Congenital rubella syndrome is now rare in vaccinated populations but devastating where it occurs, comprising the classic triad of cataracts, cardiac defects (patent ductus arteriosus, pulmonary stenosis), and sensorineural deafness, with additional features of microcephaly, intellectual disability, thrombocytopenic purpura, hepatitis, and a 'salt-and-pepper' retinopathy. First-trimester infection causes the most severe disease; the risk falls sharply after 18 weeks. The lesson of rubella is that universal childhood and pre-conception vaccination, with high coverage, can virtually eliminate the condition. [9]
Parvovirus B19 infection in pregnancy is the classic cause of non-immune hydrops fetalis. By binding the P antigen on fetal erythroid precursors it causes a pure red-cell aplasia; in the second trimester, when fetal haematopoiesis is maximal and the placenta is least able to compensate, severe anaemia, high-output cardiac failure, and hydrops follow. Intrauterine transfusion is life-saving for the severely hydropic fetus. Congenital anomalies are not a feature, and survivors who receive timely transfusion generally have normal neurodevelopment. [5]
Congenital and perinatal syphilis is resurgent. Early congenital syphilis presents in the first two years with snuffles (blood-tinged nasal discharge), a maculopapular rash involving the palms and soles, hepatosplenomegaly, lymphadenopathy, and skeletal changes (periostitis, osteochondritis, Wimberger sign). Late stigmata - interstitial keratitis, Hutchinson teeth, saddle-nose deformity, and saber shins - reflect persistent untreated infection. The condition is entirely preventable with adequate maternal treatment, making every case a system failure. [7]
Congenital Zika syndrome, recognised after the 2015-2016 epidemic, produces a distinctive phenotype of severe microcephaly with partially collapsed skull, scalp rugae, subcortical calcifications, arthrogryposis, hypertonia, seizures, and ocular abnormalities. The syndrome highlights how rapidly a new pathogen can join the congenital infection differential and how dependent recognition is on epidemiological context. [8]
Perinatal hepatitis B, hepatitis C, and HIV are the preventable bloodborne viruses. Hepatitis B is reliably prevented with birth-dose active-passive immunoprophylaxis. Hepatitis C has no vaccine or immunoglobulin; vertical transmission is approximately 5 per cent, higher with HIV co-infection, and infected infants are identified by HCV RNA PCR after 2 months and confirmed by anti-HCV after 18 months. Perinatal HIV prevention rests on maternal antiretroviral therapy, planned delivery, and infant prophylaxis; where the mother has had no antenatal care, a two-drug infant regimen outperforms zidovudine alone. [4]
[7]Complications & Pitfalls
The dominant long-term complications of congenital infection are neurological and sensory. Sensorineural hearing loss is the most common sequela of congenital CMV: it may be absent at birth, unilateral at onset, and progressive, and it is the leading non-genetic cause of childhood deafness. Cerebral palsy, epilepsy, intellectual disability, and developmental delay complicate symptomatic CMV and toxoplasmosis. Visual impairment from chorioretinitis, cataract, and glaucoma affects infants with toxoplasmosis, rubella, and CMV. Congenital syphilis left untreated causes bony deformity, interstitial keratitis, and eighth-nerve deafness. [1]
The major clinical pitfalls are several. The first is relying on a blanket 'TORCH screen' rather than targeted testing, leading to misinterpretation of past-immunity IgG. The second is missing the three-week window for CMV PCR confirmation, after which congenital and postnatal acquisition cannot be distinguished. The third is failing to investigate the mother and contacts, so that a single case of congenital syphilis or HIV does not lead to identification and treatment of the source and at-risk siblings. The fourth is delaying aciclovir in suspected neonatal HSV while awaiting PCR, a decision that measurably worsens survival. [3]
A further pitfall is over-interpreting a positive neonatal IgG, which almost always reflects passively transferred maternal antibody rather than fetal infection; IgM, by contrast, does not cross the placenta and indicates fetal/neonatal immune response, although its sensitivity varies. Finally, clinicians must not reassure parents of an 'asymptomatic' infected infant: the late emergence of hearing loss and developmental delay in asymptomatic congenital CMV mandates long-term surveillance regardless of the neonatal appearance. [1]
Prognosis & Disposition
Prognosis depends on the organism, the gestational timing of infection, the presence and severity of central nervous system involvement at birth, and the adequacy and timing of treatment. Infants with symptomatic congenital CMV and central nervous system signs have the worst prognosis, with high rates of cerebral palsy, epilepsy, cognitive impairment, and progressive sensorineural hearing loss; the six-month valganciclovir course modestly but significantly improves both hearing and developmental outcomes. Infants with asymptomatic congenital CMV have a much better but not benign prognosis, with a 10 to 15 per cent risk of late-onset hearing loss that demands surveillance. [1]
Congenital toxoplasmosis treated early has a substantially better outcome than untreated disease, in which chorioretinitis and neurodevelopmental impairment are common. Parvovirus B19 hydrops treated with intrauterine transfusion has a generally good neurodevelopmental prognosis. Congenital syphilis treated adequately in the neonatal period has an excellent prognosis; untreated or late-treated disease carries the burden of the late stigmata. Congenital rubella and Zika syndromes carry severe, lifelong disability proportional to the structural brain and sensory injury. [8]
Disposition requires a clear, written surveillance plan for every diagnosed infant. This includes serial audiology (baseline and at least every six months through early childhood for CMV), developmental surveillance and early intervention, neuroimaging and ophthalmology follow-up, and structured multidisciplinary review. For hepatitis B and HIV, the post-vaccination and post-prophylaxis serological follow-up schedule must be explicit and communicated to the family and primary care team. [6]
Special Populations
Preterm and very low birth weight infants are uniquely vulnerable to the consequences of congenital and perinatal infection. They have less transplacentally acquired maternal IgG, an immature immune response, and - in the case of postnatal CMV - are at risk of symptomatic disease from cytomegalovirus transmitted through transfused blood products or, in very low birth weight infants, breast milk from a seropositive mother. For this reason, some units restrict fresh breast milk from CMV-seropositive mothers to extremely preterm infants, or use frozen or pasteurised milk to reduce viral load. [1]
Immunocompromised mothers and their infants require special attention. Women living with HIV who are viraemic at delivery transmit infection at higher rates, and infants of these mothers need an enhanced prophylaxis regimen and early diagnostic PCR rather than antibody testing. In migrant, refugee, and asylum-seeking populations, gaps in antenatal screening and vaccination mean that congenital syphilis, congenital rubella (in unvaccinated women), and Chagas disease are over-represented; a catch-up screening approach at the first presentation in pregnancy or postpartum is essential. [7]
In Indigenous and remote communities, higher rates of untreated maternal syphilis, reduced access to timely antenatal care, and the logistical challenges of follow-up surveillance all contribute to a disproportionate burden of congenital infection and its sequelae. Culturally safe, family-centred care, interpreter access, and clear discharge communication are as important as the medical management. In low- and middle-income countries, the burden is greatest of all: congenital syphilis alone causes hundreds of thousands of stillbirths and neonatal deaths annually, almost all preventable with a single dose of penicillin. [7]
[7]Evidence, Guidelines & Regional Differences
The evidence base for congenital infection management is uneven, and a few landmark trials dominate practice. The 2015 randomised controlled trial by Kimberlin and the Collaborative Antiviral Study Group established six months of valganciclovir as the standard for symptomatic congenital CMV with central nervous system involvement, demonstrating improved total-ear hearing at 12 and 24 months and better neurodevelopmental scores at 24 months compared with six weeks of therapy. By contrast, the SYROCOT individual-patient-data meta-analysis of over 1400 mother-child pairs found only weak evidence that prenatal treatment of toxoplasmosis reduces transmission and no clear evidence it reduces clinical manifestations - a finding that has shaken the long-standing European spiral/spiramycin tradition and driven calls for a definitive randomised trial. [2]
For parvovirus B19, the prospective cohort of 1018 women by Enders and colleagues remains the definitive epidemiological study, defining fetal death and hydrops risks by gestational age and establishing intrauterine transfusion as life-saving for severe hydrops. For perinatal HIV, the HPTN 040 trial by Nielsen-Saines and colleagues showed that two-drug and three-drug infant regimens are superior to zidovudine alone when the mother has not received antenatal antiretrovirals, with the two-drug regimen preferred for its lower toxicity. [4]
[7]Controversies and active research areas include whether to adopt universal (rather than targeted) CMV screening of newborns, the role of antiviral therapy for moderately symptomatic or asymptomatic congenital CMV, the true benefit of prenatal toxoplasmosis treatment, maternal tenofovir for hepatitis B prevention in high-viraemic mothers, the optimal infant HIV prophylaxis regimen, and the long-term neurodevelopmental trajectory of congenital Zika syndrome. The resurgence of congenital syphilis in many high-income countries is a stark reminder that even fully preventable congenital infections depend on functioning public-health systems, antenatal access, and maternal treatment. [8]
Exam Pearls
TORCH (expanded)
References
- [1]Kimberlin DW Valganciclovir for symptomatic congenital cytomegalovirus disease. N Engl J Med, 2015.PMID 25738669
- [2]Thiebaut R Effectiveness of prenatal treatment for congenital toxoplasmosis: a meta-analysis of individual patients' data. Lancet, 2007.PMID 17223474
- [3]Corey L Once-daily valacyclovir to reduce the risk of transmission of genital herpes. N Engl J Med, 2004.PMID 14702423
- [4]Nielsen-Saines K Three postpartum antiretroviral regimens to prevent intrapartum HIV infection. N Engl J Med, 2012.PMID 22716975
- [5]Enders M Fetal morbidity and mortality after acute human parvovirus B19 infection in pregnancy: prospective evaluation of 1018 cases. Prenat Diagn, 2004.PMID 15300741
- [6]Fan L Cost-effectiveness of active-passive prophylaxis and antiviral prophylaxis during pregnancy to prevent perinatal hepatitis B virus infection. Hepatology, 2016.PMID 26509655
- [7]Gilmour LS Congenital syphilis: a review of global epidemiology. Clin Microbiol Rev, 2023.PMID 36920205
- [8]Freitas DA Congenital Zika syndrome: a systematic review. PLoS One, 2020.PMID 33320867
- [9]Gudeloglu E Congenital rubella syndrome: a short report and literature review. Trop Doct, 2023.PMID 36321169
- [10]Moodley A The term newborn: congenital infections. Clin Perinatol, 2021.PMID 34353577