Paeds · fetal-neonatal-and-perinatal
Congenital heart disease presenting in the newborn
Also known as Congenital heart disease presenting in the newborn · Critical congenital heart disease · Duct-dependent congenital heart disease · Neonatal cyanotic heart disease · CCHD
Fellowship guide to the newborn with congenital heart disease: the cyanotic versus duct-dependent-obstructive bedside split, pulse-oximetry screening, prostaglandin-first resuscitation, definitive transfer and intervention, and family counselling.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The single decision that changes everything in a newborn with suspected heart disease is whether the lesion is duct-dependent. If it is, the open ductus arteriosus is the only route keeping blood reaching the lungs or the body, and the baby will collapse when it closes. Recognising that fact in the first hour — and starting prostaglandin to hold the duct open — is the difference between a planned transfer to a cardiac centre and a cardiorespiratory arrest. Most newborns with critical CHD look well at first; the trap is being reassured by that early wellbeing. [1] [6]
This page covers the newborn presentation of CHD: the bedside split, the physiology of duct closure, pulse-oximetry screening, the prostaglandin-first resuscitation, definitive transfer and intervention, and family counselling. It links out to the dedicated leaves for neonatal cyanosis and the collapsed neonate, neonatal respiratory distress, and prenatal diagnosis rather than repeating them. [1]
Overview & Definition
Congenital heart disease presenting in the newborn period demands rapid recognition because duct-dependent lesions can collapse within hours of birth. The key clinical question is always: does this infant need prostaglandin E1 right now? [1]
The reason CCHD behaves as it does in the newborn is the ductus arteriosus. In fetal life it shunts blood from the pulmonary artery to the aorta, bypassing the lungs. After birth it narrows functionally over 24 to 48 hours and is permanently closed by 2 to 3 weeks. A normal heart does not need the duct. A duct-dependent lesion does — and when the duct closes, that lesion declares itself. So the practical question at the bedside is always the same: is this baby dependent on the duct? [6]
Antenatal detection picks up roughly half to two-thirds of critical lesions overall, but it is imperfect for the lesions that most often collapse: transposition of the great arteries and the left-heart obstructions. A baby with a normal antenatal cardiac scan can still present in shock from coarctation on day three. [10]
Classification
The fastest way to classify CHD in the newborn is by what you see at the bedside, because that drives the first action. There are three buckets, shown below. [1]
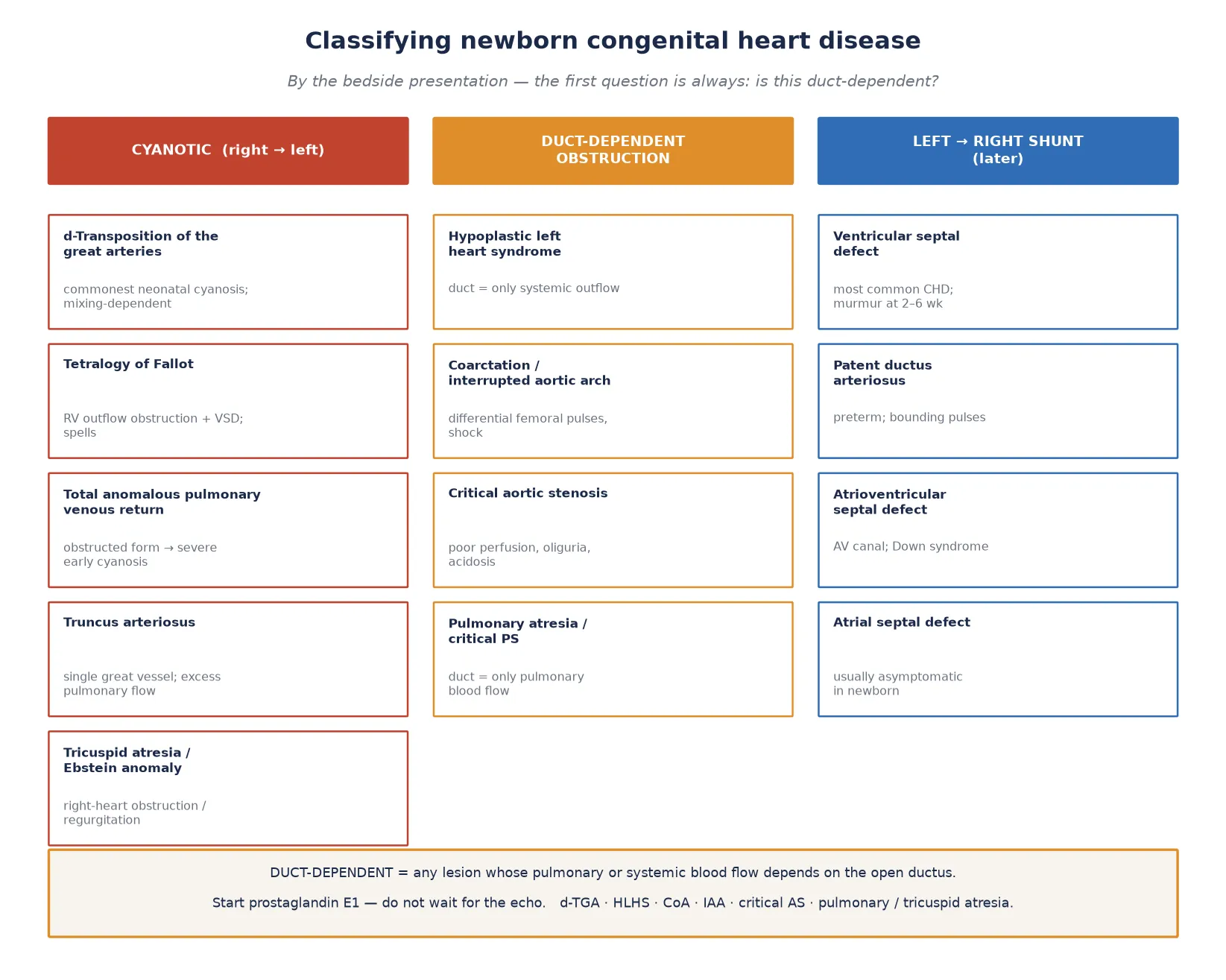
Cyanotic (right to left shunt)
- Stays blue even on oxygen
- Lesion mixes deoxygenated blood into the aorta
- d-TGA, tetralogy of Fallot, TAPVR, truncus, Ebstein, tricuspid atresia
- First action: oxygen, hyperoxia test, prostaglandin if duct-dependent mixing
Duct-dependent obstruction
- Pinks up, then collapses as the duct closes
- Perfusion fails — shock, acidosis, oliguria
- Left: HLHS, coarctation/IAA, critical AS; Right: pulmonary atresia/critical PS
- First action: prostaglandin E1 before the echo
Large left to right shunt (later)
- Presents at weeks, not hours
- Tachypnoea, poor feeding, failure to thrive, murmur
- VSD, PDA, AVSD
- First action: medical heart-failure therapy, planned repair
A lesion can belong to more than one bucket. Pulmonary atresia is both cyanotic and duct-dependent for pulmonary flow, and d-TGA is cyanotic and often needs a prostaglandin-maintained duct for mixing. The buckets are a decision aid, not a final diagnosis. The final diagnosis is echocardiographic. [2]
Epidemiology & Risk Factors
Congenital heart disease is the most common birth defect, with a birth prevalence of about 9 per 1000 live births worldwide; roughly a quarter of these infants have a critical lesion. [5] CCHD is a leading cause of infant mortality from birth defects, and infants who present in shock after duct closure have substantially higher mortality and morbidity than those diagnosed before collapse. [6]
The strongest risk factor is a parent affected by CHD, which raises the recurrence risk to about 3 to 5 percent. Other recognised contributors are maternal diabetes, congenital infection such as rubella, teratogens (alcohol, lithium, retinoic acid, some anticonvulsants), assisted reproduction, and chromosomal or syndromic associations. Several syndromes carry a high CHD yield and should prompt a cardiac review. [5]
CHD
Down (AVSD, VSD), Turner (coarctation), Noonan, 22q11 / DiGeorge (conotruncal: TOF, truncus, IAA)
Maternal diabetes: transposition, VSD, hypertrophic cardiomyopathy
Lithium (Ebstein), retinoic acid, alcohol, valproate, rubella (PDA, peripheral PS)
Antenatal detection has improved over two decades, but it remains uneven. Overall, half to two-thirds of critical lesions are suspected before birth, yet detection of transposition of the great arteries — the commonest cause of neonatal cyanosis — and of the left-heart obstructions is still incomplete. A reassuring antenatal scan never lowers your threshold to investigate a cyanotic or shocked newborn. [10] [6]
Pathophysiology
To understand why these babies collapse, picture the ductus arteriosus as a pipe that the fetus used to bypass the lungs. When that pipe closes, a normal heart barely notices — pulmonary venous return now fills the left heart, and systemic flow is independent of the duct. A duct-dependent heart, however, was using that pipe as its only route to the lungs or the body. When the pipe closes, the flow stops. [6]
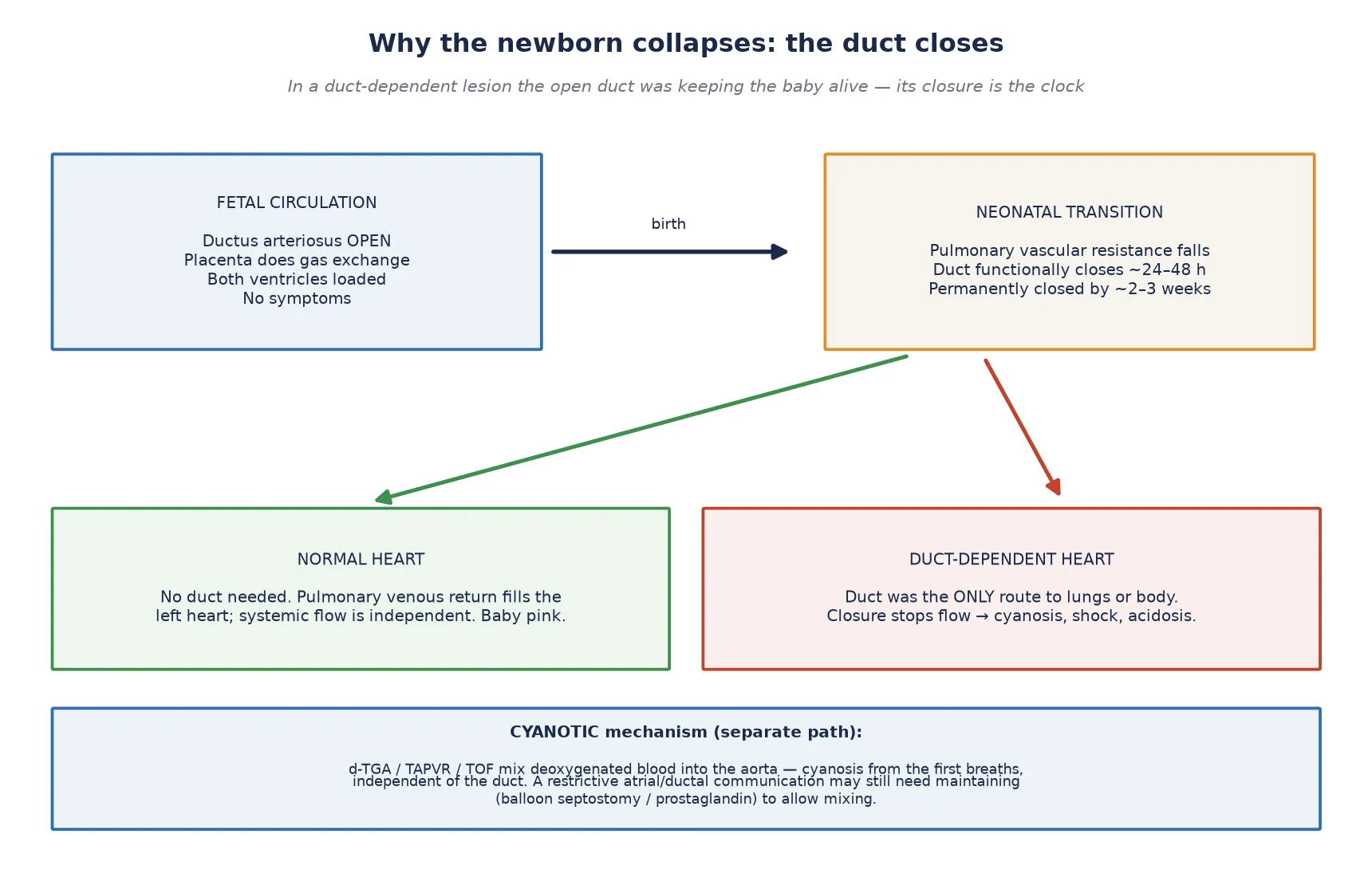
There are two distinct mechanisms, and they behave differently. [1]
Duct-dependent obstruction (collapse)
- Left obstruction (coarctation, HLHS, critical AS): systemic flow falls — shock, weak pulses, oliguria, acidosis
- Right obstruction (pulmonary atresia, critical PS): pulmonary flow falls — severe cyanosis
- Onset tracks duct closure: day 2 to 3
- Treat by reopening the duct with prostaglandin
Cyanotic mixing (blue from birth)
- d-TGA: parallel circulations — survival needs mixing at atrial or ductal level
- TAPVR: pulmonary venous blood returns to the right heart
- TOF: right to left shunt across a VSD driven by right outflow obstruction
- Cyanosis does not depend on the duct, though mixing may
The cyanotic lesions explain why some babies are blue from the first breath rather than collapsing later. In d-transposition, the aorta arises from the right ventricle and the pulmonary artery from the left, so the two circulations run in parallel and only mixed blood — through the atrial septum or the duct — reaches the aorta. In total anomalous pulmonary venous return, pulmonary venous blood is mis-routed back to the right heart. In tetralogy of Fallot, a right outflow obstruction drives deoxygenated blood across a ventricular septal defect into the aorta. None of these waits for the duct to close; they declare themselves immediately. [2]
Clinical Presentation
Most newborns with critical CHD look well at first. The danger is that the well-looking phase is exactly when the duct is still open, so a normal early examination can be falsely reassuring. The presentation then splits along the same lines as the classification: cyanosis, or collapse. [1]
The cyanotic newborn is blue centrally, tachypnoeic but without the marked recessions and grunting of lung disease, and has saturations that do not rise with oxygen. The work of breathing is often less than you would expect for the degree of hypoxia — a key clue that the problem is the heart, not the lungs. Differential cyanosis, with a pink right hand and blue feet, points to coarctation or interrupted aortic arch, or to d-TGA with a patent duct. [2]
The duct-dependent obstructive newborn tells a more deceptive story. The baby looks pink and well for the first day or two, then, as the duct narrows, slides into shock: mottled, cool peripheries, prolonged capillary refill, tachypnoea from acidosis, oliguria, and weak or absent femoral pulses in coarctation. Hepatomegaly appears as the failing heart congests. This is the infant most often mislabelled as sepsis and treated with fluids while the duct closes irreversibly. [6]
The hyperoxia test helps separate cyanotic CHD from lung disease. Place the infant in 100 percent oxygen for about 10 minutes: in pulmonary disease the arterial oxygen tension rises substantially, whereas in cyanotic CHD it stays low. A PaO2 that fails to rise above about 100 mmHg, or saturations that remain depressed, is suggestive of CHD or a right-to-left shunt. A low result is not perfectly specific — persistent pulmonary hypertension of the newborn behaves similarly — so interpret it with the rest of the picture. [2]
Differential Diagnosis
Neonatal cyanosis and neonatal shock each have a broad differential, and CHD sits inside both. The skill is reaching for CHD at the same time as the more obvious explanations, not after them. [1]
For the cyanotic newborn, the competing diagnoses are respiratory distress syndrome, transient tachypnoea of the newborn, meconium aspiration, congenital pneumonia or sepsis, persistent pulmonary hypertension of the newborn, and methaemoglobinaemia. The discriminating features are the work of breathing (low in cyanotic CHD relative to the hypoxia), the response to oxygen (poor in CHD), and the chest radiograph. [2]
For the shocked newborn, sepsis is the universal mimic and must always be covered with cultures and empiric antibiotics. Also consider inborn errors of metabolism, adrenal insufficiency, hypovolaemia, and perinatal asphyxia. The features that reweight toward CHD are differential or absent femoral pulses, a murmur, an abnormal chest radiograph or pre/post-ductal saturation difference, and a history of being well before abrupt collapse at the age when the duct closes. [6]
Points to CHD
- Cyanosis disproportionate to work of breathing
- Saturations fail to rise in high inspired oxygen
- Weak or absent femoral pulses; differential four-limb BP
- Murmur; abnormal heart shape on X-ray; pre/post-ductal difference
- Well, then collapse at 24 to 72 h
Points to lung or sepsis
- Marked recession, grunting, nasal flaring
- Saturations improve in oxygen
- Risk factors for sepsis; positive cultures
- Diffuse lung disease on X-ray
- Persistent pulmonary hypertension — variable response
Clinical & Bedside Assessment
The cardiovascular examination of the newborn takes two minutes and changes the differential. Do it the same way every time so nothing is missed. [1]
Begin with colour — central cyanosis, and any difference between the hands and the feet. Then palpate the right brachial and femoral pulses simultaneously: a brachio-femoral delay, or weak or absent femorals, is coarctation or interrupted aortic arch until proven otherwise. Feel the precordium for a right ventricular heave or a thrill, and listen to the heart sounds — a single or narrowly-split second sound suggests pulmonary hypertension or a great-vessel malformation, while a loud pulmonary component points to pulmonary hypertension. Murmurs are graded by location and radiation, but remember that serious CHD can present with no murmur, and a loud murmur can be benign. [4]
Check the liver edge — hepatomegaly is a sign of right-heart congestion. Measure perfusion by capillary refill and skin temperature. Where possible, take four-limb blood pressure: a lower-limb pressure more than 10 to 20 mmHg below the upper limb is suspicious for coarctation. [1]
Bedside, run pre-ductal (right hand) and post-ductal (foot) pulse oximetry. A difference of 3 percent or more suggests a right-to-left ductal shunt and should prompt cardiology review. Combined with the hyperoxia test, this pair of bedside manoeuvres does most of the work of deciding who needs an urgent echo. [4]
Investigations
The bedside tests come first because they change management within minutes, and because the definitive test — echocardiography — may take time to organise or require transfer. [1]
First-hour investigation bundle
Pre-ductal and post-ductal pulse oximetry — look for cyanosis and a 3% difference
Four-limb blood pressure — look for a gradient suggesting coarctation
Capillary gas with lactate — metabolic acidosis marks a sick, duct-closing baby
Glucose and ionised calcium — correct hypoglycaemia and hypocalcaemia
Cultures and CRP — cover sepsis, the universal mimic
Chest radiograph — heart shape and pulmonary vascularity
ECG — axis, chamber hypertrophy
Urgent echocardiography — the definitive test, but do NOT delay prostaglandin for it
The chest radiograph carries named patterns worth knowing. An "egg on a string" with a narrow mediastinum and increased pulmonary flow suggests d-TGA. A boot-shaped heart with pulmonary oligaemia suggests tetralogy of Fallot. The "snowman" sign appears in some unobstructed supracardiac TAPVR. Cardiomegaly with pulmonary venous congestion suggests an obstructed TAPVR or a large shunt. Rib notching and a figure-of-3 are classical for coarctation but are usually seen later, not in the newborn. [5]
Echocardiography is the definitive diagnostic test. It defines the anatomy, the direction and size of shunts, the ductal dependence, and the ventricular function. The crucial operational point is that an echo confirms the diagnosis but does not treat the patient: in a suspected duct-dependent lesion, start prostaglandin and stabilise first, and obtain the echo as soon as feasible. [9]
Management — Resuscitation
Resuscitation of the newborn with suspected CHD runs on two tracks at once: stabilise the ABCs, and — the single most important decision — open or keep open the ductus arteriosus if the lesion could be duct-dependent. [1]
Stabilise the airway and breathing, establish vascular access, and correct hypoglycaemia, hypocalcaemia and acidosis. Give empiric antibiotics if sepsis is possible, because sepsis and CHD are indistinguishable early and the cost of covering both is low. Avoid both hyperoxia and over-ventilation: excess oxygen can worsen pulmonary vascular dynamics and does not help a cyanotic mixing lesion. [2]
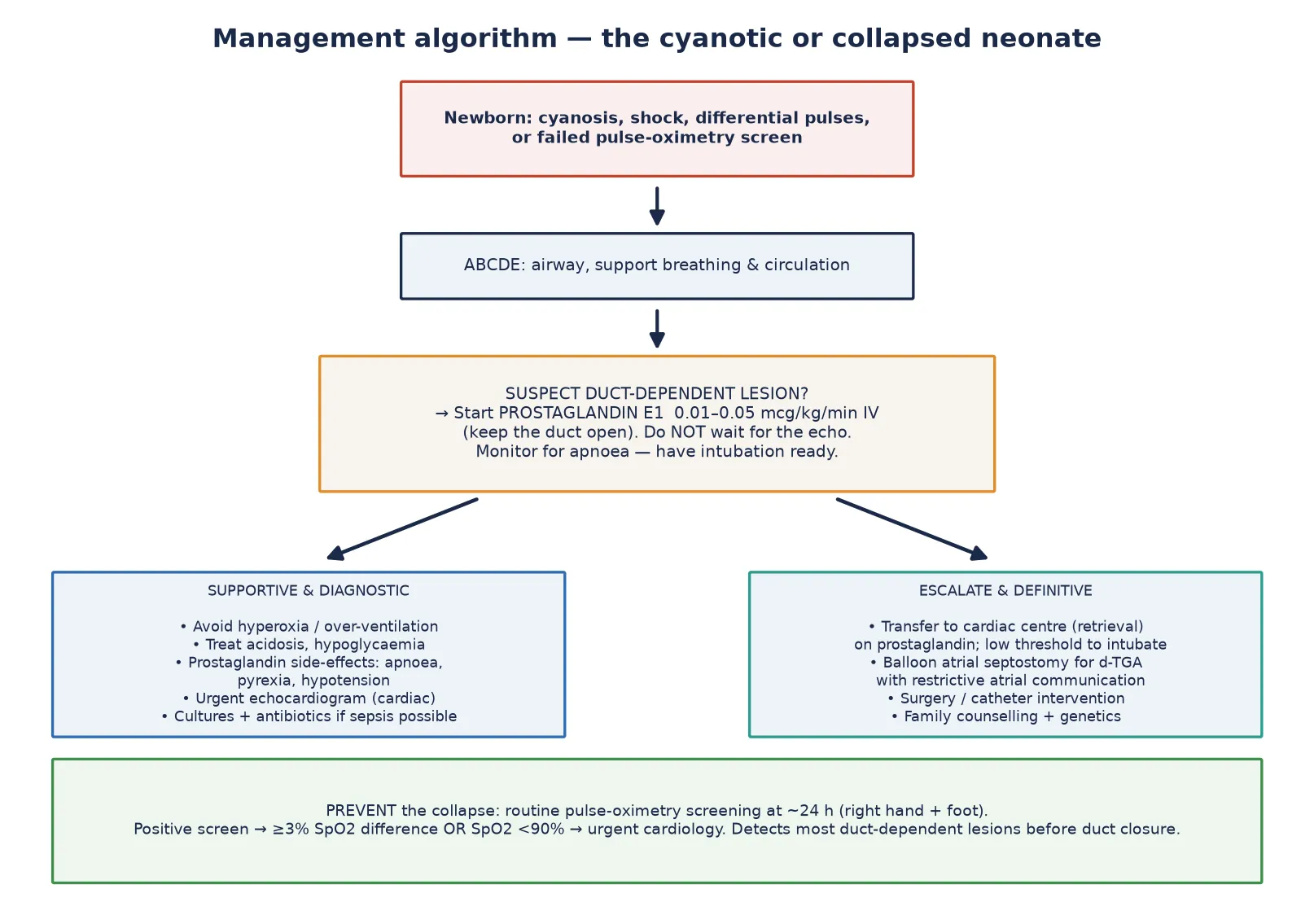
The decisive drug is prostaglandin E1 (alprostadil) 0.01 to 0.05 mcg/kg/min intravenously, started when a duct-dependent lesion is suspected. The aim is to keep the duct open, restore pulmonary or systemic flow, and buy time for echocardiography, transfer and definitive repair. Published retrieval practice confirms that low-dose prostaglandin can safely maintain the duct for transport, often without routine intubation. [9]
Prostaglandin has predictable side-effects that you must anticipate: apnoea, pyrexia, hypotension and, with longer use, gastric-outlet effects and cortical proliferation. Because apnoea is common, have intubation equipment ready, and use a low threshold for elective intubation before a long retrieval. Then arrange transfer to a cardiac centre on prostaglandin, with a team ready to manage the airway. [9]
Across AHA/AAP, ESC and ANZ guidance, prostaglandin E1 is started before echocardiography when a duct-dependent lesion is suspected, with retrieval to a cardiac surgical centre. Local retrieval protocols vary on whether to intubate electively before transport; the threshold is lower for long transfers and for higher prostaglandin doses. Name your local protocol when you act. [9]
Management — Definitive & Stepwise
Once the duct is open and the baby is stable, definitive management is echocardiographic diagnosis followed by lesion-specific surgery or catheter intervention. The pathway runs in stages. [1]
Definitive pathway for suspected critical CHD
Prostaglandin E1 to maintain ductal patency and stabilise perfusion
Urgent transthoracic echocardiography to define anatomy and duct dependence
Balloon atrial septostomy for d-TGA with a restrictive atrial communication (to improve mixing)
Lesion-specific surgery or catheter intervention (e.g. coarctation repair; balloon valvuloplasty for critical pulmonary or aortic stenosis; staged single-ventricle palliation for HLHS)
Syndrome and genetics evaluation (22q11 microdeletion in conotruncal lesions)
Family counselling and structured long-term cardiology follow-up
Specific lesion management follows the anatomy. d-Transposition is treated with an arterial switch operation, often after balloon atrial septostomy if atrial mixing is poor and the duct is maintained on prostaglandin. Coarctation is repaired surgically; interrupted aortic arch needs early surgery. Critical aortic stenosis and critical pulmonary stenosis are often amenable to balloon valvuloplasty in the catheter laboratory. Hypoplastic left heart syndrome follows a staged single-ventricle pathway — Norwood or hybrid, then Glenn, then Fontan. Tetralogy of Fallot is repaired, but in the newborn a spell is treated first with knee-chest positioning, oxygen, morphine and a beta-blocker. [10]
The large left-to-right shunts (VSD, PDA, AVSD) present later with heart failure rather than collapse. Their management is medical first — diuretics such as frusemide and caloric supplementation — with timely surgical or catheter repair to protect the pulmonary vascular bed and allow growth. [5]
Specific Subtypes & Scenarios
The four scenarios below cover the highest-yield lesions for exams and for the bedside, because they are the ones that present, collapse, and kill if missed. [1]
d-Transposition of the great arteries is the commonest cause of neonatal cyanosis. The circulations run in parallel, so survival depends on mixing at the atrial or ductal level. Cyanosis is present from birth and may deepen as the duct closes; a restrictive atrial septum is dangerous and may need a balloon atrial septostomy. Antenatal detection, though improved, is still imperfect. [10]
Coarctation of the aorta and interrupted aortic arch are the archetypal pinks-up-then-collapses lesions. The baby is well while the duct supplies the lower body, then develops shock, metabolic acidosis and differential cyanosis as the duct closes. Weak or absent femoral pulses and a four-limb blood-pressure gradient are the bedside clues. [6]
Hypoplastic left heart syndrome is duct-dependent for systemic flow: the single right ventricle pumps to both circuits through the duct. Presentation is shock as the duct closes, and survival depends on a staged single-ventricle pathway. These infants are among the sickest in paediatric cardiology and need prostaglandin, transfer and a cardiac surgical centre without delay. [5]
Tetralogy of Fallot presents with cyanosis driven by right-to-left shunting across a ventricular septal defect, set against right outflow obstruction. Hypercyanotic spells are treated as an emergency with knee-chest positioning, oxygen, morphine and a beta-blocker such as propranolol, which relaxes the infundibulum. The chest radiograph shows a boot-shaped heart with pulmonary oligaemia. [5]
Complications & Pitfalls
These lesions collapse when the ductus closes, so the first question is always whether to start prostaglandin. [1]
Delayed diagnosis of a duct-dependent lesion leads to cardiogenic shock, end-organ injury — renal, hepatic, and gut, raising the risk of necrotising enterocolitis — neurological injury, and death. Prostaglandin itself causes apnoea, hypotension, pyrexia and, with prolonged use, gastric-outlet obstruction and cortical proliferation. Both risks are real, and both are manageable if anticipated. [6]
Diagnostic pitfalls
- Attributing cyanosis to lung disease when it is d-TGA
- Treating day-3 shock as sepsis and missing coarctation
- Being reassured by an early normal saturation (duct still open)
- Waiting for the echo before starting prostaglandin
- Accepting a passed pulse-oximetry screen as excluding CHD
Treatment pitfalls
- Intubating without preparing for prostaglandin-induced apnoea
- Over-oxygenating a cyanotic mixing lesion
- Missing the deterioration hidden behind a deceptively well early course
- Fluid-loading a duct-closing obstructive lesion (worsens perfusion)
- Delaying transfer for non-essential tests
The most insidious trap is the well baby. A normal examination and a passed screen on day one do not exclude a lesion that will collapse on day three. Counsel parents on safety-net warning signs — poor feeding, colour change, breathlessness, lethargy — and ensure a clear pathway back to care. [7]
Prognosis & Disposition
Prognosis is driven by the specific lesion, the timing of diagnosis and intervention, and any syndromic or chromosomal comorbidity — not by how cyanotic the baby looks at presentation. The single biggest modifiable factor is whether the diagnosis was made before collapse. Antenatal detection and pulse-oximetry screening both shift diagnosis earlier, and earlier diagnosis reduces preoperative mortality and morbidity for duct-dependent lesions. [1] [6]
For most operated CHD, survival into adulthood is now good, with lesion-specific needs for re-intervention, arrhythmia surveillance, exercise advice, endocarditis prophylaxis, and neurodevelopmental follow-up. Single-ventricle physiology and the most complex arch and outflow lesions carry a harder course and lifelong surveillance. [5]
Disposition follows the lesion. Stabilise and transfer to a cardiac centre for definitive diagnosis and intervention; arrange structured paediatric cardiology follow-up; and plan transition to adult congenital heart disease services for the long-term survivors. Every infant should leave hospital with a named safety-net and a clear review plan. [8]
Special Populations
Antenatally diagnosed infants are the planned pathway: delivery at or near a cardiac-capable centre, early postnatal echocardiography, and prostaglandin if the lesion is duct-dependent. Yet prenatal diagnosis is imperfect — transposition and the left-heart obstructions are the lesions most often missed — so even a booked delivery needs a structured postnatal assessment. [10]
Preterm and remote or rural infants face retrieval logistics. A duct-dependent baby on prostaglandin may need long-distance transfer, and low-dose prostaglandin protocols can maintain the duct safely for transport, often without routine intubation when the dose is low and the baby is stable. [9]
Syndromic infants need the genetics evaluation alongside the cardiac one: Down syndrome with an atrioventricular septal defect, 22q11 microdeletion (DiGeorge) with conotruncal lesions, and Turner syndrome with coarctation are high-yield associations that change counselling and recurrence-risk discussion. [5]
Socioeconomic and ethnic variation affects incidence, access to prenatal diagnosis, and surgical outcomes. Equity of access to screening, to antenatal diagnosis, and to timely surgery is a determinant of outcome and a legitimate subject for advocacy, not just an epidemiological observation. [7]
Evidence, Guidelines & Regional Differences
The case for routine pulse-oximetry screening rests on a coherent evidence base. The Swedish prospective study of nearly 40,000 newborns showed that adding pulse oximetry reduced the diagnostic gap — fewer duct-dependent lesions were first discovered after collapse. [1] The Lancet meta-analysis pooled the screening studies and reported a sensitivity of about 76 percent and a specificity of about 99 percent for critical congenital heart defects, with a low false-positive rate when screening was done after 24 hours of age. [2]
Pulse-oximetry screening meta-analysis
Lancet
Systematic review and meta-analysis of pulse oximetry screening for critical congenital heart defects in asymptomatic newborns (Thangaratinam 2012)
Key finding
Sensitivity about 76% and specificity about 99% for critical congenital heart defects; the false-positive rate was low when screening was performed after 24 hours of age.
Practice change
Pulse oximetry is an effective, acceptable adjunct to the routine newborn examination, but it misses about a quarter of critical lesions — so it supplements rather than replaces clinical assessment.
The test-accuracy study from the United Kingdom confirmed both effectiveness and acceptability and added cost-effectiveness modelling. [3] Policy followed: the United States Secretary of Health recommended screening in 2011, the AAP and AHA endorsed it, and implementation data showed it could be scaled. [4] [8] A modelling study estimated the number of infants detected and missed across the United States, reinforcing that screening is additive, not absolute. [7]
Two longitudinal observations frame the trend. Over twenty years in one region, the diagnosis of life-threatening neonatal cardiovascular malformations shifted earlier, though duct-dependent lesions still presented after discharge. [6] And over a 20-year period, prenatal detection of transposition of the great arteries improved but remained imperfect. [10]
Australia and Aotearoa New Zealand adopt universal pulse-oximetry screening as part of the newborn examination, with referral thresholds for saturations below 90 percent (immediate cardiology), below 95 percent in both limbs or a pre/post-ductal difference of 3 percent or more (repeat and refer). Prostaglandin E1 is the standard duct-opening infusion, started before echocardiography when a duct-dependent lesion is suspected, with retrieval to a cardiac surgical centre. [9]
The remaining controversies are practical: the optimal timing and the value of repeat or home screening; how to manage the residual missed cases, especially left-heart obstruction; equity of access to prenatal diagnosis and to cardiac surgery; and the best prostaglandin dose and the threshold for elective intubation during retrieval. [7]
Exam Pearls
One-sentence answer: the approach to suspected CHD in the newborn
Split the presentation at the bedside into cyanotic versus duct-dependent, start prostaglandin E1 the moment a duct-dependent lesion is suspected — before the echo — feel the femoral pulses in every baby, and organise echocardiography and transfer to a cardiac centre in parallel.
Epidemiology and screening
- Birth prevalence of CHD about 9 per 1000 live births; about 25% critical
- Antenatal detection about 50 to 60% overall, lower for d-TGA and left-heart obstruction
- Duct functionally closes about 24 to 48 h (permanent by 2 to 3 weeks)
- A passed pulse-oximetry screen does NOT exclude CHD
Pulse-oximetry screen (at 24 h)
- SpO2 below 90% any limb — immediate cardiology referral
- SpO2 below 95% in both limbs, or pre/post-ductal difference of 3% or more — repeat then refer
- Measure right hand (pre-ductal) and either foot (post-ductal)
Lesion to sign pairings
- d-TGA — cyanosis and 'egg on a string'; commonest neonatal cyanosis
- Coarctation / IAA — differential or absent femoral pulses; day-2/3 collapse
- TOF — boot-shaped heart and oligaemia; TET spells treated with knee-chest, oxygen, morphine, beta-blocker
- HLHS — duct-dependent systemic flow; staged single-ventricle pathway
- TAPVR (obstructed) — severe cyanosis; 'snowman' sign when unobstructed supracardiac
Frequently misremembered facts, stated correctly: a passed pulse-oximetry screen does not exclude CHD, because left-heart obstruction and some d-TGA are missed. Not all cyanosis is respiratory — the work of breathing is disproportionately low in cyanotic CHD. The femoral pulses must be felt in every newborn, including on day three. And prostaglandin is started before the echocardiogram in a suspected duct-dependent lesion, because the echo confirms the diagnosis but does not treat the patient. [7]
The lesion-to-sign pairings are the fastest route to a diagnosis at the bedside and the highest-yield material for a short case: d-TGA with an egg-on-a-string heart; coarctation with absent femoral pulses and a four-limb gradient; tetralogy with a boot-shaped heart and pulmonary oligaemia; TAPVR with the snowman sign and, when obstructed, severe early cyanosis. [5]
References
- [1]de-Wahl Granelli A; Wennergren M; Sandberg K; et al Impact of pulse oximetry screening on the detection of duct dependent congenital heart disease: a Swedish prospective screening study in 39,821 newborns. BMJ, 2009.PMID 19131383
- [2]Thangaratinam S; Brown K; Zamora J; et al Pulse oximetry screening for critical congenital heart defects in asymptomatic newborn babies: a systematic review and meta-analysis. Lancet, 2012.PMID 22554860
- [3]Ewer AK; Furmston AT; Middleton LJ; et al Pulse oximetry as a screening test for congenital heart defects in newborn infants: a test accuracy study with evaluation of acceptability and cost-effectiveness. Health Technol Assess, 2012.PMID 22284744
- [4]Mahle WT; Martin GR; Beekman RH 3rd; et al Endorsement of Health and Human Services recommendation for pulse oximetry screening for critical congenital heart disease. Pediatrics, 2012.PMID 22201143
- [5]van der Linde D; Konings EE; Slager MA; et al Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol, 2011.PMID 22078432
- [6]Wren C; Reinhardt Z; Khawaja K Twenty-year trends in diagnosis of life-threatening neonatal cardiovascular malformations. Arch Dis Child Fetal Neonatal Ed, 2008.PMID 17556383
- [7]Ailes EC; Gilboa SM; Honein MA; et al Estimated number of infants detected and missed by critical congenital heart defect screening. Pediatrics, 2015.PMID 25963011
- [8]Frank LH; Bradshaw E; Beckman R; et al Critical congenital heart disease screening using pulse oximetry. J Pediatr, 2013.PMID 23266220
- [9]Browning Carmo KA; Barr P; West M; et al Transporting newborn infants with suspected duct dependent congenital heart disease on low-dose prostaglandin E1 without routine mechanical ventilation. Arch Dis Child Fetal Neonatal Ed, 2007.PMID 16905574
- [10]Escobar-Diaz MC; Freud LR; Bueno A; et al Prenatal diagnosis of transposition of the great arteries over a 20-year period: improved but imperfect. Ultrasound Obstet Gynecol, 2015.PMID 25484180