Paeds · fetal-neonatal-and-perinatal
Extremely preterm infant: viability and periviable counselling
Also known as Extremely preterm infant: viability and periviable counselling
Fellowship guide to extremely preterm infant: viability and periviable counselling.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Periviable birth refers to delivery occurring at the borderline of extrauterine viability, typically defined as birth between 20+0 and 25+6 weeks of gestation. [8] This is a critical clinical and ethical threshold because each additional week of gestation within this narrow window dramatically alters the probability of survival and the risk of long-term neurodevelopmental impairment. [1] The period encompasses the "grey zone" of shared decision-making, generally framed as 22+0 to 24+6 weeks, during which active treatment may or may not be offered depending on parental values, institutional policy, and individualised prognostic factors. [8]
Counselling at the threshold of viability is among the most demanding conversations in perinatal medicine. It requires synthesising gestational age estimates, antenatal and intrapartum risk modifiers, institutional outcome data, and the family's values into a shared decision about whether to pursue active resuscitation and intensive care or to provide comfort-focused palliative care. [9] The paediatrician's role is to provide honest, balanced, probabilistic information that avoids both false reassurance and undue pessimism, while creating space for genuine parental autonomy. [9]
Epidemiology & Risk Factors
Approximately 0.4 to 0.5 per cent of all births in high-income countries occur before 28 weeks of gestation, yet these infants account for a disproportionate share of neonatal mortality, long-term disability, and healthcare expenditure. [3] In the United States, infants born at less than 28 weeks represent fewer than 2 per cent of live births but over one-third of all infant deaths. [5] In England, the EPICure 2 study demonstrated improved survival for infants born at 22 to 25 weeks between 1995 and 2006, reflecting advances in antenatal and neonatal care. [3]
Key risk factors for extremely preterm delivery include spontaneous preterm labour (often associated with intrauterine infection or chorioamnionitis), preterm prelabour rupture of membranes, preeclampsia and other hypertensive disorders, placental abruption, multiple gestation, maternal smoking, short interpregnancy interval, low maternal body mass index, prior preterm birth, and certain cervical and uterine anomalies. [8] Socioeconomic disadvantage and ethnic minority status are also associated with increased risk, reflecting both biological and structural determinants. [3]
Prognostic factors that modify survival and outcome at a given gestational age include estimated fetal weight, fetal sex (female infants have better outcomes), singleton versus multiple gestation, receipt of antenatal corticosteroids, and the presence or absence of chorioamnionitis. [2] The Tyson estimator, developed from the NICHD Neonatal Research Network, demonstrated that combining these variables substantially improves outcome prediction beyond gestational age alone. [2]
Pathophysiology
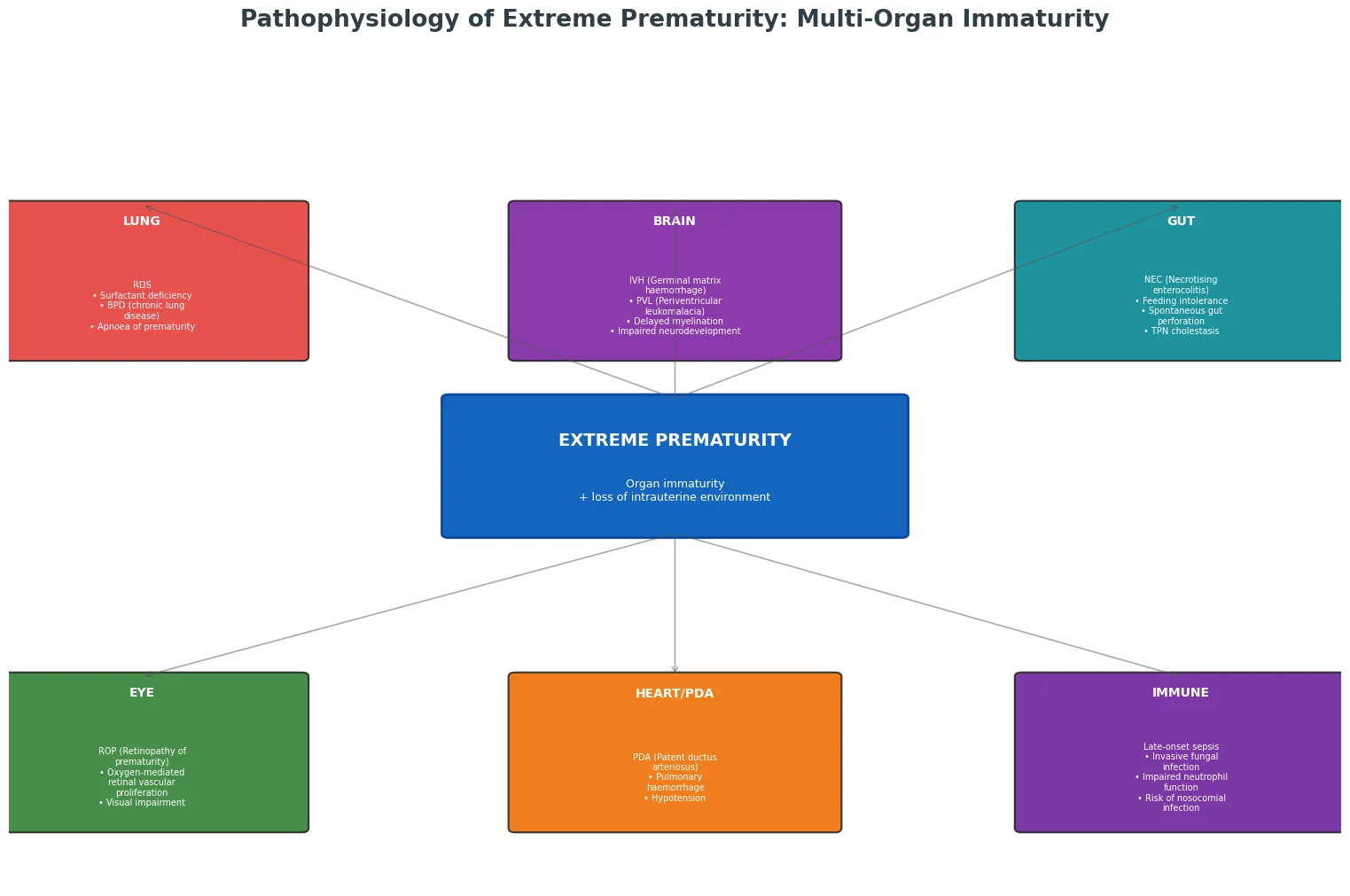
Extreme prematurity results from the birth of an infant whose organ systems are profoundly immature and unprepared for extrauterine life. The pathophysiology of complications in the periviable infant reflects the interaction between developmental immaturity and the stressors of the extrauterine environment, including mechanical ventilation, oxygen exposure, parenteral nutrition, and infection risk. [5]
The central nervous system is among the most vulnerable systems. The germinal matrix, a highly vascularised region of neuronal and glial precursor cells, is prominent between 24 and 32 weeks and is the principal site of germinal matrix haemorrhage and subsequent intraventricular haemorrhage. [5] The periventricular white matter is susceptible to ischaemic injury (periventricular leukomalacia) because of the immaturity of the vascular supply and the vulnerability of premyelinating oligodendrocytes to oxidative and inflammatory injury. [6]
The lungs are structurally and biochemically immature, with reduced surfactant production, underdeveloped alveoli, and a compliant chest wall, leading to respiratory distress syndrome and an increased risk of bronchopulmonary dysplasia. [5] The gastrointestinal tract has immature motility and barrier function, predisposing to feeding intolerance and necrotising enterocolitis. The immune system is functionally deficient, with low immunoglobulin levels and impaired neutrophil function, increasing susceptibility to nosocomial and late-onset sepsis. [5]
Classification
Periviable infants are classified by gestational age, and each week carries a distinct prognosis that frames the counselling and management conversation. [8] The classification below reflects the broad consensus from the joint NICHD, SMFM, AAP, and ACOG workshop on periviable birth. [8]
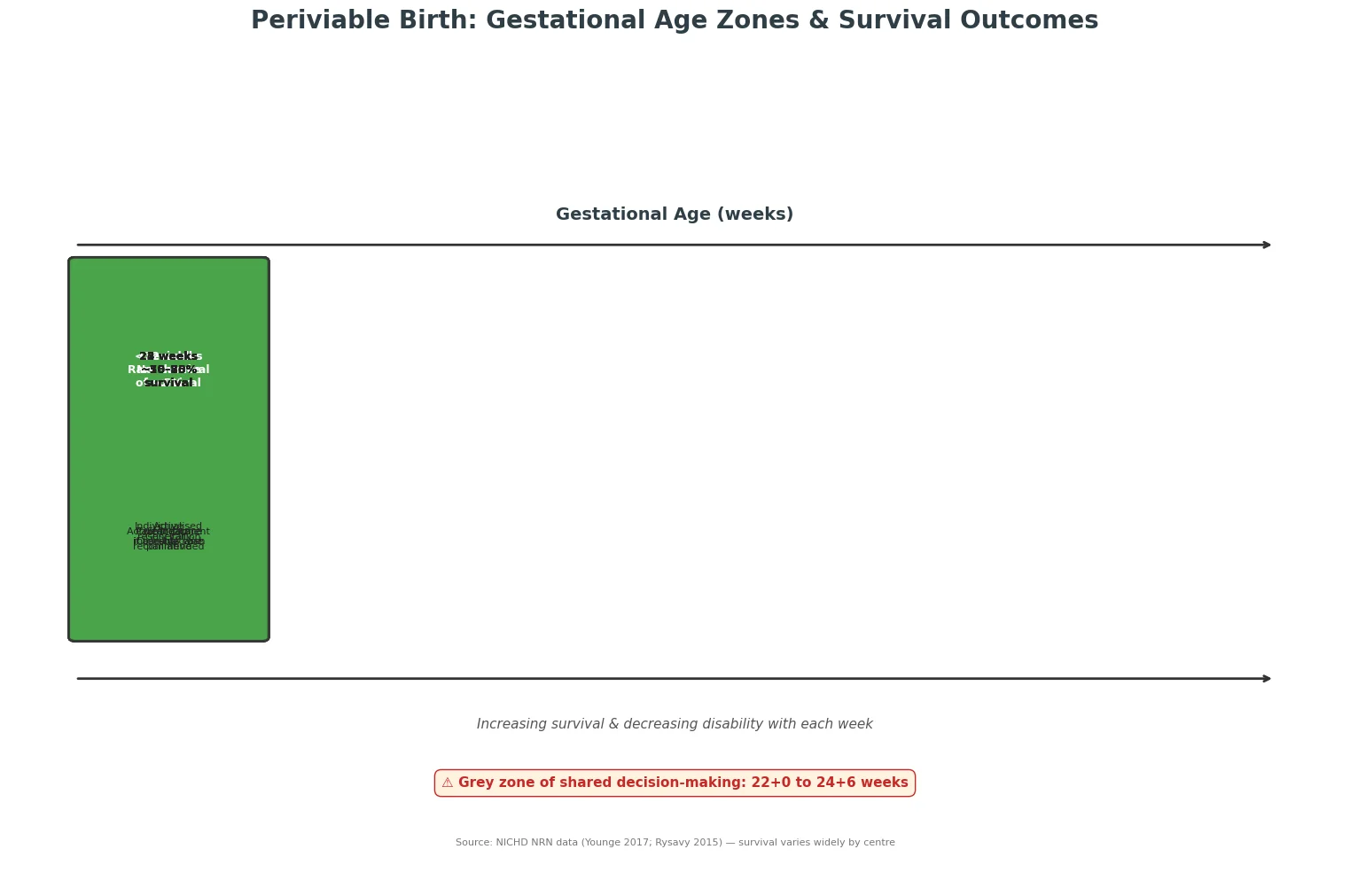
At 20+0 to 21+6 weeks, the fetus is considered previable. Survival with intensive care is negligible and universally, palliative comfort care is the appropriate management. [8] At 22+0 to 22+6 weeks, survival is possible but rare, estimated at 5 to 15 per cent with active treatment in select centres, with very high rates of severe neurodevelopmental impairment among survivors. This is a zone of individualised decision-making. [1] [8]
At 23+0 to 23+6 weeks, survival with active treatment ranges from approximately 25 to 50 per cent depending on centre aggressiveness and prognostic factors, and this represents the core of the grey zone where shared decision-making is paramount. [1] At 24+0 to 24+6 weeks, survival exceeds 50 to 65 per cent, and active resuscitation is generally recommended, though the counselling conversation remains essential because rates of moderate-to-severe impairment remain substantial. [4] At 25+0 weeks and above, survival is 70 per cent or higher, and active treatment is the standard of care. [4]
Clinical Presentation
Periviable delivery typically presents as a pregnant woman at 20 to 26 weeks gestation with threatened preterm labour, preterm prelabour rupture of membranes, or a planned iatrogenic delivery for maternal or fetal indications such as severe preeclampsia or placental abruption. [8] The clinical scenario demands simultaneous obstetric and neonatal assessment: confirming gestational age accurately, estimating fetal weight, administering antenatal corticosteroids and magnesium sulfate for neuroprotection where appropriate, assessing for chorioamnionitis, and arranging in-utero transfer to a tertiary perinatal centre. [8]
At birth, the extremely preterm infant has translucent, gelatinous skin, fused eyelids, minimal subcutaneous fat, and extreme low birthweight (typically 400 to 800 g at 22 to 25 weeks). The infant is immediately dependent on a coordinated resuscitation team for thermoregulation, respiratory support, and vascular access. The clinical presentation is one of total physiological dependency on intensive care technology. [5]
Differential Diagnosis
The primary differential in the periviable counselling context is not a diagnostic one but rather a decision-making differential: active intensive care versus palliative comfort care. [10] However, several clinical conditions can confound the assessment and must be considered:
Intrauterine growth restriction can coexist with prematurity and independently worsens prognosis beyond gestational age alone; distinguishing a growth-restricted 24-week infant from an appropriate-for-gestational-age 22-week infant with similar weight is essential. [2] Congenital anomalies and chromosomal disorders may be identified antenatally and fundamentally alter the prognosis and counselling approach. [8] Intrauterine infection and fetal inflammatory response syndrome worsen outcomes and may be evidenced by maternal fever, tachycardia, or raised inflammatory markers. [8]
Uncertain gestational dating is the most important confounder. If first-trimester dating is unavailable or uncertain, the gestational age estimate may be off by one to two weeks, which at the threshold of viability can shift the infant from one management category to another. [8] Always clarify the dating method and its reliability during counselling.
Clinical & Bedside Assessment
The clinical assessment of the periviable scenario begins antenatally with accurate gestational age determination. First-trimester crown-rump length is the gold standard, with an accuracy of plus or minus 5 to 7 days. Second-trimester biometry is less precise at plus or minus 10 to 14 days. [8] Estimated fetal weight from ultrasound adds prognostic information, and the combination of gestational age and estimated fetal weight substantially improves outcome prediction. [2]
The bedside assessment after birth includes Apgar scores (which are less informative and not used to guide resuscitation decisions in this population), temperature, respiratory effort, heart rate, and oxygen saturation targets appropriate for gestational age. [5] Continuous monitoring of oxygen saturation, heart rate, and temperature is essential from the first minute of life. Target preductal oxygen saturations in the first minutes after birth for infants under 28 weeks are lower than term targets, typically 60 to 70 per cent at 5 minutes rising gradually thereafter. [5]
Investigations
Antenatal investigations relevant to the periviable infant include ultrasound confirmation of gestational age and estimated fetal weight, assessment of fetal wellbeing (biophysical profile, Doppler studies if growth restriction is suspected), and maternal screening for infection, Group B Streptococcus, and other relevant conditions. [8]
Postnatal investigations in the surviving extremely preterm infant include serial cranial ultrasound to detect intraventricular haemorrhage and periventricular leukomalacia, blood gas analysis for acid-base status, bedside glucose monitoring, complete blood count and inflammatory markers, and blood cultures if sepsis is suspected. [5] Echocardiography assesses ductal patency and haemodynamic significance. Serial ophthalmological examinations for retinopathy of prematurity begin at 31 to 34 weeks postmenstrual age or 4 to 6 weeks of age, whichever is later. [5]
Japan has the most proactive approach, with active resuscitation commonly offered from 22 weeks, reflecting cultural norms and national guidelines that emphasise maximum effort. Sweden, through the EXPRESS study, demonstrated excellent outcomes with active management from 22 to 23 weeks. The United Kingdom (EPICure data, Nuffield Council guidelines, and BAPM framework) traditionally adopted a more conservative stance, though the 2019 BAPM framework moved toward offering active treatment at 22 weeks with parental agreement. Australia and New Zealand generally offer active treatment from 23 weeks, with a shared decision-making approach at 22 to 23 weeks. The United States (AAP, ACOG guidance) recommends individualised counselling with active treatment generally offered from 23 to 24 weeks and strongly recommended from 25 weeks. [3] [7] [8]
Management — Resuscitation
The management of periviable birth begins with antenatal interventions that optimise outcomes regardless of the ultimate resuscitation decision. [8]
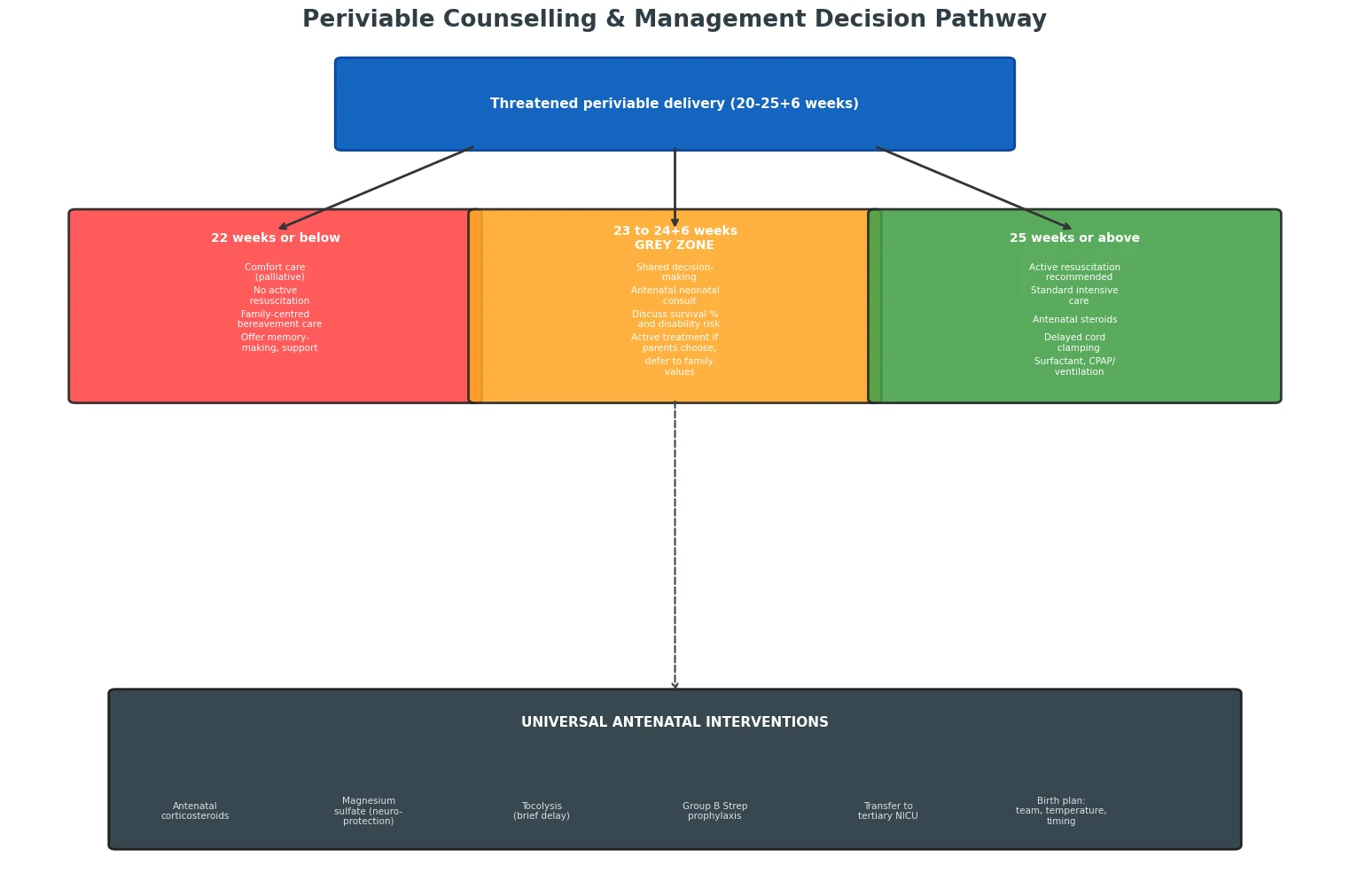
Antenatal corticosteroids (betamethasone 12 mg intramuscularly, two doses 24 hours apart, or dexamethasone 6 mg intramuscularly, four doses 12 hours apart) accelerate fetal lung maturation and reduce neonatal mortality, respiratory distress syndrome, and intraventricular haemorrhage. [8] Current guidelines support their use from 22+0 weeks if active treatment is planned after birth. [8]
Magnesium sulfate for fetal neuroprotection (4 g intravenous loading dose over 20 to 30 minutes, with or without a 1 g per hour maintenance infusion) reduces the risk of cerebral palsy when administered to women at risk of delivery before 32 weeks. [8] Tocolysis may be used to delay delivery sufficiently to complete a corticosteroid course and arrange in-utero transfer to a tertiary centre. [8]
At birth, the resuscitation of the extremely preterm infant follows the principles of gentle stabilisation: delayed cord clamping for 30 to 60 seconds when feasible, thermal protection using plastic wraps and an exothermic mattress to maintain admission temperature of 36.5 to 37.5 degrees Celsius, and early respiratory support with positive end-expiratory pressure and judicious use of surfactant. [5] Oxygen should be initiated at 21 to 30 per cent and titrated based on saturation targets, avoiding hyperoxia. [5]
Antenatal resuscitation checklist for periviable delivery
Confirm gestational age from first-trimester dating and estimate fetal weight
Administer antenatal corticosteroids (betamethasone 12 mg IM x2, 24 h apart) if active treatment considered
Administer magnesium sulfate 4 g IV loading for neuroprotection if below 32 weeks
Offer tocolysis to complete steroid course and enable transfer
Transfer in-utero to tertiary perinatal centre with NICU
Conduct antenatal neonatal consultation with both parents
Document a clear, agreed birth plan: resuscitation or comfort care
Mobilise the neonatal team: senior neonatologist, nurse, respiratory therapist present at delivery
Management — Definitive & Stepwise
For infants receiving active intensive care, definitive management is a longitudinal, multi-system effort spanning the neonatal intensive care unit stay and extending into long-term follow-up. [5]
Respiratory management focuses on minimising ventilator-associated lung injury through non-invasive ventilation (continuous positive airway pressure or nasal intermittent positive pressure ventilation), early surfactant administration via a minimally invasive technique where feasible, and caffeine citrate (loading dose 20 mg per kg, maintenance 5 to 10 mg per kg daily) [5] to reduce apnoea of prematurity and facilitate extubation. [5]
Nutritional management prioritises early enteral feeding with expressed breast milk, supplemented with human milk fortifier as tolerated, with parenteral nutrition supporting growth until full enteral feeds are established. [5] Haemodynamic management addresses hypotension and patent ductus arteriosus with fluid boluses, inotropes, and, where necessary, pharmacological or surgical ductal closure. [5]
For infants for whom comfort care is chosen, management focuses on dignity, family-centred care, and symptom relief. The infant is wrapped in a warm blanket and held by the parents; analgesia is provided as needed (morphine or similar); the team supports memory-making activities such as photographs, handprints, and footprints, and bereavement follow-up is arranged. [10]
Specific Subtypes & Scenarios
22-week gestation with parental desire for active treatment: At 22 weeks, survival with intensive care is 5 to 15 per cent in the most aggressive centres, and severe impairment affects 60 to 80 per cent of survivors. [1] If parents strongly desire active treatment after comprehensive counselling, some centres will proceed, but many institutional policies default to comfort care. The decision must be documented carefully, and a plan for re-evaluation is essential. [1]
23-week gestation, the paradigmatic grey-zone scenario: At 23 weeks, survival is 25 to 50 per cent with active treatment. [1] The Rysavy study demonstrated enormous between-hospital variation, with some centres treating 100 per cent of 23-week infants actively and others treating fewer than half, even after adjusting for case mix. [1] The counselling must present local outcome data where available and clearly explain that the family's values are the decisive factor. [9]
Multiple gestation at the threshold of viability: Multiple gestation independently worsens prognosis at a given gestational age. The Tyson model showed that singleton status confers a significant survival advantage. [2] Counselling should present outcomes specific to multiple gestation rather than extrapolating from singleton data. [2]
Severe fetal growth restriction at 24 weeks: A growth-restricted 24-week infant may have outcomes more consistent with a 22-week infant. The combination of prematurity and placental insufficiency compounds the risk. Estimated fetal weight below the 3rd centile at 24 weeks should prompt a modified, more cautious prognosis. [2]
Complications & Pitfalls
The major complications of extreme prematurity span every organ system. Intraventricular haemorrhage and periventricular leukomalacia are the dominant neurological complications, leading to cerebral palsy, cognitive impairment, sensory deficits, and epilepsy. [6] Bronchopulmonary dysplasia affects 40 to 60 per cent of surviving infants born at less than 28 weeks and is associated with prolonged oxygen dependence, recurrent hospitalisations, and impaired lung function into adulthood. [5]
Retinopathy of prematurity can lead to blindness in severe cases and requires ongoing ophthalmological surveillance. Necrotising enterocolitis carries a mortality of 20 to 30 per cent and may require surgical resection with long-term gastrointestinal consequences. [5] Late-onset sepsis and invasive fungal infections are leading causes of morbidity and mortality. Patent ductus arteriosus is nearly universal at this gestational age and contributes to haemodynamic instability, pulmonary haemorrhage, and chronic lung disease. [5]
The most important counselling pitfall is presenting outcomes as binary (survival versus death) rather than as a spectrum that includes the quality of survival. [9] Parents need to understand that survival does not equate to intact survival, and that approximately 30 to 50 per cent of surviving periviable infants will have moderate-to-severe neurodevelopmental impairment, including cerebral palsy, cognitive disability, blindness, or deafness. [4] [6] Another pitfall is over-reliance on national or international averages when local institutional outcomes may differ substantially. [1]
Prognosis & Disposition
Survival and neurodevelopmental outcomes have improved substantially over the past two decades. The EPICure studies demonstrated improved survival at every gestational age between 1995 and 2006 in England. [3] The NICHD Neonatal Research Network data from 1993 to 2013 showed steady improvements in survival without major morbidity. [5] The Swedish EXPRESS cohort reported some of the best outcomes globally, with 6.5-year follow-up showing that among infants born before 27 weeks, approximately 60 per cent had no or mild disability, 30 per cent had moderate disability, and 10 per cent had severe disability. [7]
The long-term prognosis for surviving periviable infants includes a spectrum from normal development to severe, multi-domain impairment. At 6 to 6.5 years of age, the EPICure and EXPRESS cohorts showed that 40 to 50 per cent of survivors born before 26 weeks have cognitive impairment (IQ below 70), 10 to 15 per cent have cerebral palsy, and 5 to 10 per cent have severe visual or hearing impairment. [6] [7] Behavioural and educational difficulties are common and often persist into adolescence and adulthood. [6]
Disposition planning for surviving periviable infants involves coordination with early intervention services, developmental follow-up clinics (typically through corrected age 2 to 3 years), audiology and ophthalmology surveillance, and community-based support services. [5] Growth is plotted on Fenton charts to 50 weeks postmenstrual age, then transitioned to WHO or INTERGROWTH-21st standards, with milestones corrected for prematurity until approximately 2 years. [5]
Special Populations
Indigenous and remote-dwelling populations in Australia and New Zealand: Aboriginal, Torres Strait Islander, and Maori populations have higher rates of preterm birth, and geographic distance from tertiary perinatal centres introduces additional challenges in timely access to antenatal corticosteroids, magnesium sulfate, and specialist neonatal teams. [8] Culturally safe counselling, including the involvement of Aboriginal health workers or cultural liaison officers, is essential. Transfer decisions must account for both clinical need and the importance of keeping families connected to country and community.
Multiple gestations: Twins and higher-order multiples born at periviable gestational ages face compounded risks. The second-born twin is at higher risk of adverse outcomes. Counselling should address the potential for discordant outcomes (one twin survives, one dies or is disabled), which creates unique ethical and emotional complexities. [2]
Religious and cultural considerations: Some families hold beliefs that mandate maximum effort regardless of prognosis. The clinician's role is to provide honest information and respect autonomy, while ensuring that decisions are informed and aligned with the child's best interests. Involvement of hospital chaplaincy, cultural liaison, or ethics committees may be valuable. [9]
Evidence, Guidelines & Regional Differences
The evidence base for periviable outcomes draws on several landmark population cohorts and network datasets. The NICHD Neonatal Research Network (United States) provides the largest contemporary dataset, including the Tyson estimator and the Younge outcome data. [2] [4] The EPICure studies (England, 1995 and 2006) provide longitudinal follow-up data demonstrating temporal improvement and long-term neurodevelopmental outcomes. [3] [6] The Swedish EXPRESS cohort (born 2004 to 2007) demonstrated outcomes achieved with a proactive approach to perinatal care at extremely low gestational ages. [7]
Guideline frameworks differ by region but share common principles. The 2014 joint NICHD, SMFM, AAP, and ACOG workshop on periviable birth provided a framework recommending individualised counselling, antenatal consultation, and a graduated approach: comfort care below 22 weeks, shared decision-making from 22 to 24 weeks, and active treatment from 25 weeks. [8] The British Association of Perinatal Medicine (BAPM) framework, updated in 2019, moved the UK toward offering active treatment at 22 weeks with parental consent, reflecting improving outcomes. The Nuffield Council on Bioethics guidelines provided the foundational ethical framework for UK practice. [10]
The Rysavy study revealed that institutional variation in treatment rates at 22 to 24 weeks is extreme, ranging from 0 to 100 per cent, and that this variation drives outcome differences as much as biology. [1] This finding underscores that the decision to treat or not treat is shaped by institutional culture and policy as much as by patient factors, and has led to calls for greater transparency and standardisation. [1]
PREEMIE — prognostic factors for periviable outcome
Exam Pearls
-
Know the weekly survival numbers: 22 weeks (5 to 15 per cent), 23 weeks (25 to 50 per cent), 24 weeks (55 to 70 per cent), 25 weeks (70 per cent plus). These are commonly tested in the DWE and MRCPCH. [1] [4]
-
The grey zone is 22+0 to 24+6 weeks. Shared decision-making is the standard framework within this zone. Active resuscitation is recommended from 25 weeks. Below 22 weeks, comfort care is the default. [8]
-
Antenatal corticosteroids should be offered from 22+0 weeks if active treatment is planned. Magnesium sulfate for neuroprotection is indicated before 32 weeks. Both improve outcomes and should be part of the antenatal bundle. [8]
-
The five prognostic factors are gestational age, birthweight, sex, antenatal corticosteroids, and singleton status (the Tyson model). [2] Chorioamnionitis worsens prognosis. Know how each modifies the baseline estimate.
-
Between-hospital variation is enormous. The Rysavy study is a landmark finding: at 22 to 24 weeks, treatment rates vary from 0 to 100 per cent between hospitals. [1] This is a high-yield exam point.
-
Long-term outcomes: Approximately 30 to 50 per cent of surviving periviable infants have moderate-to-severe neurodevelopmental impairment at school age. [4] [6] Cerebral palsy affects 10 to 15 per cent. IQ below 70 affects 40 to 50 per cent. [6]
-
Regional differences are testable. Japan and Sweden are proactive from 22 weeks. Australia and New Zealand offer active treatment from 23 weeks. The UK has become less conservative with the 2019 BAPM update. [3] [7]
-
Counselling principles: honest, balanced, probabilistic; avoid both false reassurance and undue pessimism; use plain language; create space for genuine parental autonomy; document the conversation. [9] [10]
References
- [1]Rysavy MA Between-hospital variation in treatment and outcomes in extremely preterm infants. N Engl J Med, 2015.PMID 25946279
- [2]Tyson JE Intensive care for extreme prematurity — moving beyond gestational age. N Engl J Med, 2008.PMID 18420500
- [3]Costeloe KL Short term outcomes after extreme preterm birth in England: comparison of two birth cohorts in 1995 and 2006 (the EPICure studies). BMJ, 2012.PMID 23212881
- [4]Younge N Survival and Neurodevelopment of Periviable Infants. N Engl J Med, 2017.PMID 28490002
- [5]Stoll BJ Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993-2013. JAMA, 2015.PMID 26348753
- [6]Marlow N Neurologic and developmental disability at six years of age after extremely preterm birth. N Engl J Med, 2005.PMID 15635108
- [7]Serenius F Neurodevelopmental Outcomes Among Extremely Preterm Infants 6.5 Years After Active Perinatal Care in Sweden. JAMA Pediatr, 2016.PMID 27479919
- [8]Raju TNK Periviable birth: executive summary of a joint workshop by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal-Fetal Medicine, American Academy of Pediatrics, and American College of Obstetricians and Gynecologists. Obstet Gynecol, 2014.PMID 24785861
- [9]Kaempf JW Counseling pregnant women who may deliver extremely premature infants: medical care guidelines, family choices, and neonatal outcomes. Pediatrics, 2009.PMID 19482761
- [10]Kaempf JW Extremely premature birth and the choice of neonatal intensive care versus palliative comfort care. J Perinatol, 2016.PMID 26583942