Paeds · fetal-neonatal-and-perinatal
Fetal growth restriction and small-for-gestational-age infant
Also known as Intrauterine growth restriction (IUGR) · Small for gestational age · Fetal growth restriction · SGA infant · Placental insufficiency
Fellowship guide to distinguishing fetal growth restriction from the constitutionally small infant, antenatal surveillance and Doppler interpretation, and the early neonatal management of hypothermia, hypoglycaemia, polycythaemia and feeding difficulty.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Meet a common scenario. A baby is born at term weighing 2350 g — below the 10th centile. The midwife calls the baby "small for dates". Before you reach for tests or admit to NICU, ask one question that changes everything: is this baby small because they are meant to be small, or because something went wrong in utero? [3]
That single distinction — between the constitutionally small infant and the growth-restricted infant — is the whole of this topic. [1]
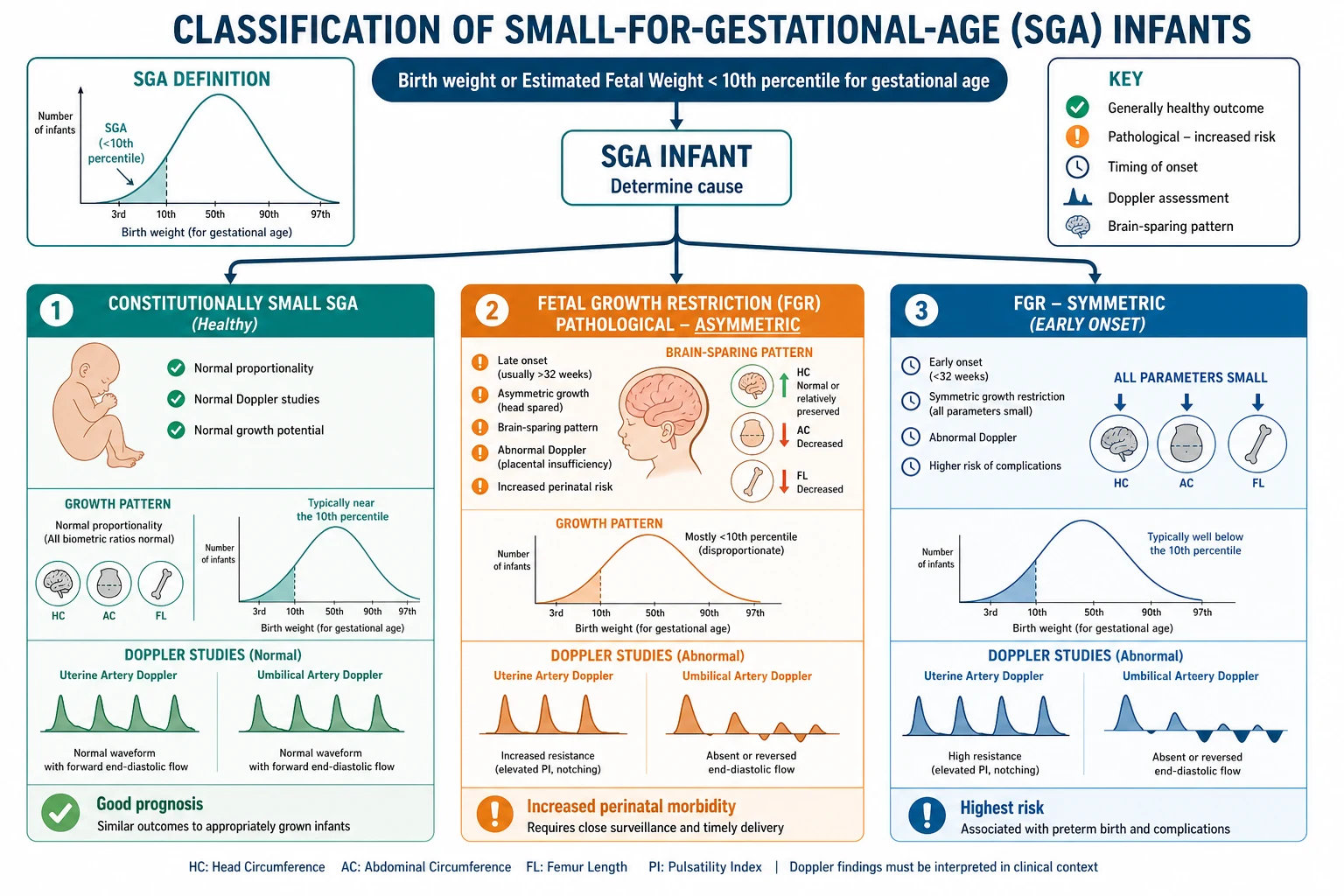
Small for gestational age (SGA) is a size label. It means the birthweight (or the antenatal estimated fetal weight) is below the 10th centile for gestational age and sex on a standard chart. [3] About one baby in ten carries the label by definition. Severe SGA is below the 3rd centile. None of this tells you why the baby is small.
Fetal growth restriction (FGR) is a process. The fetus has failed to reach the size it was genetically programmed to achieve, because it was deprived of nutrients or oxygen — most often by a failing placenta. [1] Many FGR fetuses are also SGA, but not all. A fetus whose growth falls from the 60th to the 15th centile is growth-restricted even though it never crosses the 10th, and a perfectly healthy small baby can sit comfortably below the 10th all pregnancy.
So the terms overlap like two circles that do not sit perfectly on top of each other. Most SGA babies are healthy and constitutionally small. Some are pathologically growth-restricted. And a few growth-restricted babies are not (yet) below the 10th centile. Your job at the bedside and in the long case is to work out which circle each baby sits in. [2]
Classification
Start with the size descriptor, then add the pathology. [3]
By size, plot weight, length and head circumference on an international (INTERGROWTH-21st) chart. SGA is below the 10th centile; severe SGA is below the 3rd. [3] [4]
By proportion, separate symmetric from asymmetric. In symmetric restriction the head, length and weight are all reduced together, suggesting an early insult that hit the fetus before it could redirect its blood supply — think chromosomal anomaly or congenital infection. In asymmetric restriction the head is relatively preserved while the body and limbs are wasted, the classic "brain-sparing" pattern of late placental insufficiency. [11] In real life the two blend together, so use the pattern as a clue, not a verdict. [11]
By onset, separate early-onset FGR (before 32 weeks) from late-onset FGR (32 weeks and beyond). This matters because they are different diseases. Early FGR is rare and severe, driven by serious placental failure, and the TRUFFLE trial has taught us how to monitor and time its delivery. [6] Late FGR is far more common, carries a lower absolute mortality but a real risk of late stillbirth, and is monitored chiefly with growth and the cerebroplacental ratio. [2]
Epidemiology & Risk Factors
About 10% of all live births are SGA by definition. FGR is harder to count because definitions vary, but it underlies a large share of unexplained stillbirths and perinatal deaths, which is why the obstetric team watches growth so closely. [1]
Risk factors cluster into three buckets. Maternal factors are the commonest: pre-eclampsia and chronic hypertension, diabetes with vascular disease, chronic renal disease, malnutrition and low body mass index, smoking and alcohol, substance use, extremes of maternal age, short interpregnancy interval, and assisted reproduction. Fetal factors include multiple pregnancy, chromosomal anomalies (trisomy 13, 18, Turner), structural syndromes, and congenital infection (cytomegalovirus, toxoplasmosis, rubella, malaria). Placental factors are the engine of most FGR: failed spiral artery remodelling, placental infarction, velamentous cord insertion, single umbilical artery, and the praevia/accreta spectrum. [1]
The strongest single predictor of FGR in a current pregnancy is a previous affected pregnancy. Social determinants amplify all of this: smoking, food insecurity, poor antenatal access and socioeconomic disadvantage both raise the incidence and worsen the outcome. [14]
Pathophysiology
To understand the small baby, follow the oxygen. Normal placentation remodels the spiral arteries so they pour blood freely into the intervillous space. When that remodelling fails — the same failure that drives pre-eclampsia — the placenta becomes a high-resistance, low-flow organ. Nutrients and oxygen cross poorly. The fetus is, in effect, being starved and choked at once. [1]
The fetus fights back. It redirects its limited cardiac output to the organs it cannot live without — brain, heart and adrenal glands — and lets the liver, kidneys and body wall go short. That redistribution is brain sparing, and it is why the head is relatively spared while the body wastes: asymmetry is a survival strategy, not a coincidence. [10] [11]
The same deprivation explains the four classic neonatal complications. Low glycogen stores and low substrate make hypoglycaemia almost expected. Almost no body fat makes hypothermia likely. Chronic hypoxia drives the kidneys to pour out erythropoietin, so the baby arrives polycythaemic. And a starved, encephalopathic gut feeds poorly and is prone to intolerance. [12]
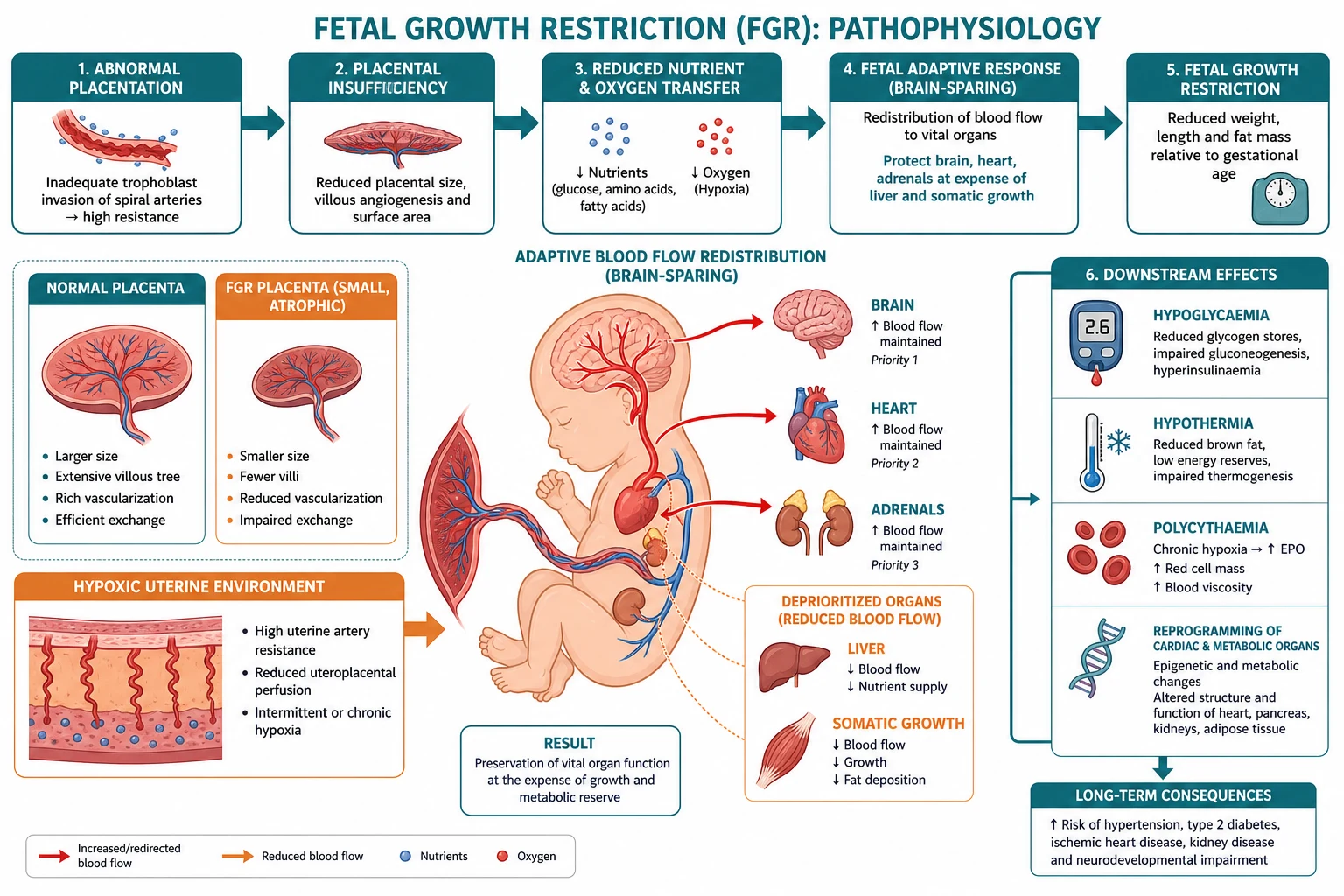
There is a longer story too. The growth-restricted fetus does not just "catch up and forget". Its heart is remodelled — thicker, stiffer walls — and its metabolism is reprogrammed, so that FGR is now recognised as an origin of adult cardiovascular and metabolic disease. [10] You will not see this in the neonatal unit, but it is the reason long-term follow-up and a frank family conversation matter.
Doppler changes track the pathology in a recognisable order. As placental resistance climbs, the umbilical artery waveform loses its diastolic flow — first rising resistance, then absent, then reversed end-diastolic flow, the gravest sign. The cerebral vessels dilate in response (brain sparing), dropping the middle cerebral artery pulsatility index and the cerebroplacental ratio. Only later does the cardiotocograph deteriorate. [6] [8]
Clinical Presentation
Antenatally the picture is often quiet. The mother reports reduced fetal movements, the symphysis-fundal height measures small, or a routine growth scan finds the fetus has fallen behind. The dangerous late sign is a stillbirth that surveillance was meant to prevent. [2]
At birth, the growth-restricted neonate looks wasted rather than simply small. Subcutaneous fat and muscle are stripped away, the skin is loose and dry, the abdomen is scaphoid, and the head looks disproportionately large. The Ponderal Index (a weight-for-length measure) is low, capturing that wasting. [11] The constitutionally small infant, by contrast, is simply a smaller version of a well-nourished baby — proportionate, plump and alert.
Four early complications define the first hours: hypoglycaemia, hypothermia, polycythaemia with hyperviscosity, and feeding difficulty. [12] A growth-restricted infant may also show respiratory distress, polycythaemia-driven lethargy or, in the worst cases, perinatal depression and hypoxic-ischaemic encephalopathy.
Look deliberately for clues to a cause. Dysmorphic features, a structural anomaly, hepatosplenomegaly, petechiae or a "blueberry muffin" rash point to a chromosomal or congenital infection explanation rather than simple placental insufficiency — and they change the workup entirely. [11]
Differential Diagnosis
The differential turns on one question: is the growth restriction pathological, or is the baby constitutionally small? [2]
The constitutionally small infant has small parents, a normal antenatal growth velocity, normal Doppler studies, normal amniotic fluid, a normal Ponderal Index, and is alert and feeding at birth. This baby needs no investigation and no admission — only reassurance and routine care. [2]
The pathologically restricted infant has fallen across centiles, shows wasting or abnormal Doppler, or has features of an underlying cause. Within pathology, separate the causes: [1]
- Placental insufficiency (commonest) — asymmetric, late-onset, brain-sparing, abnormal umbilical artery Doppler.
- Chromosomal / syndromic — symmetric, early-onset, often with dysmorphism or structural anomaly (trisomy 13, 18, Turner, Russell-Silver, Noonan).
- Congenital infection — symmetric with stigmata such as hepatosplenomegaly, petechiae, chorioretinitis, sensorineural hearing loss (CMV, toxoplasmosis, rubella).
- Multiple pregnancy — selective, discordant growth with its own management framework.
- Structural / skeletal — a single small dimension (e.g. limb shortening) rather than global restriction. [2]
Do not conflate FGR with prematurity. A preterm baby may be both early and small; classify the two axes separately so you do not attribute complications of prematurity to growth restriction or vice versa. [1]
Clinical & Bedside Assessment
Begin with a focused antenatal history that frames the whole neonatal plan: which risk factors were present, what the serial growth scans and Doppler studies showed, whether steroids and magnesium were given, and why and when delivery was induced or performed. A baby delivered early for reversed end-diastolic flow is a different patient from one born at term with a low-normal cerebroplacental ratio. [8]
Accurate anthropometry is the single most important bedside act. Weigh the baby, measure length and head circumference with a tape, calculate the Ponderal Index (weight in grams × 100 divided by length in centimetres cubed), and plot everything on a gestation- and sex-specific INTERGROWTH-21st chart. [3] A unisex or adult chart misclassifies small babies — never use one.
Examine the baby for wasting versus proportionality to judge symmetry. Look for subcutaneous fat and muscle loss, loose skin folds, a scaphoid abdomen and a relatively large head. Then screen for a cause: dysmorphism, congenital anomalies, organomegaly, rash or petechiae. [11]
Assess function in the first hours: tone, colour, perfusion, temperature, feeding and respiratory effort. The tiring, cold or hypoglycaemic baby declares itself early if you look — and those are the findings that move a baby from mother's room to NICU. [12]
Finally, synthesise. A good one-line summary sounds like: "A 37-week male, birthweight 2200 g (3rd centile), asymmetric, with antenatal reversed end-diastolic flow, now cold and hypoglycaemic — severe late-onset FGR with early neonatal metabolic compromise." That sentence tells the team the category, the severity and the first moves. [2]
Investigations
SGA is a diagnosis you make with a tape measure and a chart, not a battery of tests. Over-investigating the well constitutionally small infant causes harm, anxiety and wasted resources. [2]
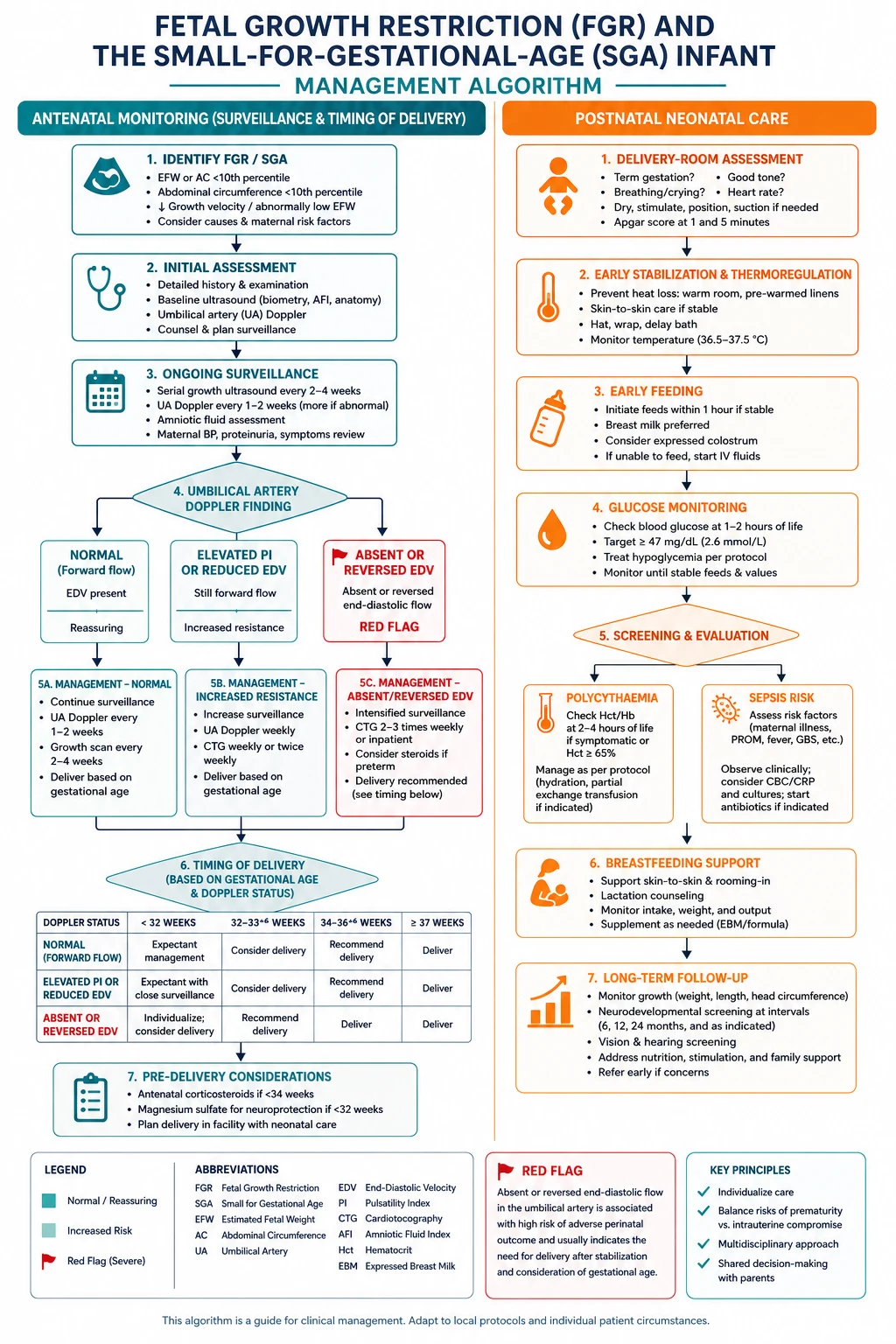
Antenatally, surveillance is the obstetric team's domain but you must understand it to read the handover. The toolkit is serial estimated fetal weight and abdominal circumference, umbilical artery Doppler (the cornerstone), middle cerebral artery Doppler and the cerebroplacental ratio, computerised cardiotocography, and the biophysical profile. [6] [8]
Postnatally, tailor tests to the baby in front of you. For the at-risk FGR infant, monitor pre-feed bedside glucose on a schedule and treat per the hypoglycaemia protocol. [12] Check a venous haematocrit for polycythaemia if the baby is plethoric, lethargic or feeding poorly; a serum bilirubin if jaundiced; a blood gas if in respiratory distress; and a septic screen if there is maternal or neonatal risk. If the baby is dysmorphic, severely and symmetrically restricted, or there is another clinical pointer, send a karyotype or chromosomal microarray and a congenital infection screen. [2]
Know what to avoid. Do not take routine arterial samples when capillary or venous sampling answers the question. Do not image or culture a well, proportionate, feeding baby just because of a centile. And do not let a panel of normal results reassure you about a baby who looks wasted and is not feeding. [2]
The four Hs to expect in FGR
Management — Resuscitation
Most SGA infants do not need resuscitation beyond routine newborn care — the danger is assuming that is always true. Severe FGR, especially with abnormal Doppler or late prematurity, can present with perinatal depression. Warm the room, dry and stimulate, and assess tone, breathing and heart rate through the standard neonatal resuscitation algorithm (covered in the dedicated resuscitation topic). [1]
The two resuscitation priorities specific to the small infant are warmth and glucose. Use plastic wrap and a hat for the vulnerable late-preterm or wasted baby, aim for skin-to-skin contact when stable, and feed within the first hour to protect the depleted glycogen stores. Check a pre-feed glucose and treat hypoglycaemia promptly. [12]
Escalate to NICU when any of these is present: severe FGR (below the 3rd centile or abnormal Doppler), gestation below about 34–37 weeks (locally defined), symptomatic or persistent hypoglycaemia, respiratory distress, polycythaemia needing intervention, or the need for intravenous fluids. A well, term, mildly SGA infant feeding well and thermally stable stays with mother with monitoring. [12]
Management — Definitive & Stepwise
Once stable, definitive care is a sequence you can rehearse: warm, feed, monitor, support, follow up. [12]
- Thermoregulation. Maintain normothermia from birth — warm room, drying, plastic wrap for the vulnerable, hat, and skin-to-skin when stable. Hypothermia worsens hypoglycaemia and acidosis.
- Early and frequent feeding. Establish the first feed within an hour, then feed every 2–3 hours. Breast milk is first choice; supplement only if intake is inadequate. [12]
- Glucose monitoring. Check pre-feed glucose on a schedule for at-risk infants. Treat in a stepwise ladder: feed, then buccal 40% dextrose gel (200 mg/kg, repeated as needed) with feeding, then intravenous 10% dextrose bolus and an escalating infusion for persistent hypoglycaemia. [12] [13]
- Watch for polycythaemia and jaundice. A symptomatic baby with a venous haematocrit above the local threshold may need a partial exchange transfusion; manage jaundice by standard thresholds for gestation.
- Nutrition and catch-up growth. Aim for controlled catch-up — adequate but not excessive. Fortify expressed breast milk or supplement if growth lags, and watch for feeding intolerance.
- Discharge. Send the baby home only when thermally stable, glucose-stable on full enteral feeds, gaining weight, feeding competently, and with confident, supported parents.
Plan long-term follow-up from discharge. Monitor growth, offer neurodevelopmental surveillance (especially after early-onset or severe FGR), arrange vision and hearing checks if very preterm, and use the ongoing relationship to counsel the family about the cardiovascular and metabolic implications of FGR without alarming them at the bedside. [10]
Specific Subtypes & Scenarios
Early-onset FGR (before 32 weeks). Rare but severe. These are the babies TRUFFLE taught us about: surveillance is Doppler-driven, delivery timing turns on late computerised CTG deterioration and ductus venosus changes, and perinatal and 2-year outcomes are guarded but improvable with the right timing. [6] [7] [8]
Late-onset FGR (32 weeks and beyond). Far commoner. Lower absolute mortality, but a genuine risk of late stillbirth, which is why surveillance does not stop. A falling growth centile or a cerebroplacinal ratio below the 5th centile is the trigger to intensify surveillance and consider delivery. [2] [14]
Severe SGA (below the 3rd centile). Higher risk of an underlying cause and of neonatal complications. Lower your threshold for workup, NICU admission and glucose monitoring. [1]
Symmetric FGR. Think early intrinsic cause — chromosome, syndrome, infection — and broaden the workup accordingly. [11]
Asymmetric FGR. Think late placental insufficiency, brain sparing and the metabolic neonatal complications. [10]
Selective FGR in twins. Discordant growth carries its own staging and surveillance framework; manage with the fetal-medicine team. [6]
Late-preterm FGR (34–36+6 weeks). Balances the risks of prematurity against the risks of continuing a compromised pregnancy; the late-preterm infant needs both neonatal-metabolic and prematurity care. [6]
Complications & Pitfalls
Short-term, expect hypoglycaemia, hypothermia, polycythaemia and hyperviscosity, respiratory distress, feeding intolerance, necrotising enterocolitis risk, jaundice and perinatal depression. [12] [13] Long-term, expect (in a minority) impaired cognition and lower IQ, cerebral palsy in the most severe cases, persistent short stature, and adult cardiovascular and metabolic disease. [10]
The common pitfalls are predictable, and worth naming so you avoid them. Reassuring on a centile while ignoring a fall in growth velocity — the baby who has dropped three centiles but is still "above the 10th" is still growth-restricted. Over-investigating the well constitutionally small baby, generating harm and anxiety. Missing hypoglycaemia because the infant looked well at one moment — small babies can look well and still be hypoglycaemic an hour later. Attributing everything to placental insufficiency and missing a syndromic or infective cause hiding in plain sight. And forgetting the family — rapid catch-up growth looks like success, but it carries its own metabolic programming risk that the parents deserve to understand. [1]
Prognosis & Disposition
Outcome is driven by cause, severity, gestation and Doppler abnormality — not by size alone. A healthy constitutionally small infant has a normal outlook. A severely growth-restricted preterm infant with reversed end-diastolic flow carries a real risk of mortality, neurodevelopmental impairment and cerebral palsy. [6] [7]
TRUFFLE gave us the evidence: in early-onset FGR delivered before 32 weeks, perinatal mortality is significant but not uniform, and 2-year neurodevelopmental outcomes are best when delivery is timed to computerised CTG and ductus venosus change rather than to umbilical artery Doppler alone. The GRIT–TRUFFLE comparison confirmed that watchful, surveillance-driven delivery does not worsen long-term outcomes compared with earlier delivery. [7] [9]
Disposition follows the risk. A well term SGA infant feeding and thermally stable stays with mother with monitoring. A moderate-risk baby goes to a transitional or NICU environment for glucose and temperature support. A severe, preterm or symptomatic baby goes to NICU, often with the neonatal team present at delivery. Most growth-restricted infants catch up physically by two years; a minority carry lasting cognitive, growth or cardiovascular sequelae, which is why follow-up is part of treatment, not an optional extra. [10]
Special Populations
Preterm FGR compounds two risks — prematurity and growth restriction. Expect a neonatal team at delivery and plan for surfactant, thermal and glucose needs together. [6]
Selective FGR in multiple pregnancy is discordant and fetal-medicine-led; the paediatrician's job is to be briefed on the larger, smaller and shared risks. [6]
Indigenous and socioeconomically disadvantaged families carry higher smoking, nutrition and access burdens. Provide culturally safe antenatal and postnatal care, address smoking and nutrition directly, and ensure the growth-monitoring and follow-up loop does not drop. [14]
Rural and remote settings must plan antenatal transfer to a service with neonatal capability before delivery wherever possible; a growth-restricted baby born away from support is an avoidable crisis. [6]
Syndromic or chromosomal causes need a parallel genetic and dysmorphology pathway, with honest, staged communication with the family. [2]
Out-of-home-care and migrant-refugee infants need deliberate continuity — confirm growth monitoring, immunisation and follow-up are transferred, not lost, across moves. [14]
Evidence, Guidelines & Regional Differences
The foundational papers are the Gordijn 2016 Delphi consensus, which standardised the FGR definition to stop overdiagnosis; [1] the Figueras-Gratacos 2014 stage-based management framework; [2] and the INTERGROWTH-21st international standards, which showed that fetal and newborn growth is near-identical across healthy populations and so replaced population-specific charts. [3] [4] [5]
The TRUFFLE trial and its follow-ups define early-onset FGR care: perinatal outcomes (Lees 2013), [6] 2-year neurodevelopment (Lees 2015), [7] monitoring before 32 weeks (Ganzevoort 2017), [8] and the GRIT–TRUFFLE comparison (Ganzevoort 2020). [9] Neonatal glycaemia thresholds and their neurodevelopmental meaning come from the McKinlay studies at 2 and 4.5 years. [12] [13] The fetal-programming story is summarised by Crispi. [10]
Two live controversies: whether to offer universal third-trimester growth scanning (improves detection of late FGR but increases intervention), and whether customised charts outperform international standards for identifying pathological FGR. [2] [5] Neither is resolved; know your local policy and the reasoning behind it.
Exam Pearls
- SGA is a size word (<10th centile); FGR is a pathology word. The distinction is the single most testable idea. [1]
- Asymmetric + brain sparing → late placental insufficiency. Symmetric → early intrinsic cause (chromosome, infection). [11]
- Absent or reversed end-diastolic flow on the umbilical artery is high-risk and changes delivery timing. [6]
- Expect and pre-empt the four neonatal complications: hypothermia, hypoglycaemia, polycythaemia, feeding difficulty. [12]
- Plot every small infant on a gestation- and sex-specific INTERGROWTH-21st chart — never a unisex or adult chart. [3]
- In TRUFFLE, late computerised CTG and ductus venosus change drove delivery timing in early FGR before 32 weeks. [7] [8]
- FGR carries lifelong cardiovascular and metabolic risk — counsel the family, but do not alarm at the bedside. [10]
- A fall in growth velocity matters even if the baby is still above the 10th centile.
References
- [1]Gordijn SJ Consensus definition of fetal growth restriction: a Delphi procedure. Ultrasound in Obstetrics & Gynecology, 2016.PMID 26909664
- [2]Figueras F Update on the diagnosis and classification of fetal growth restriction and proposal of a stage-based management protocol. Fetal Diagnosis and Therapy, 2014.PMID 24457811
- [3]Villar J International standards for newborn weight, length, and head circumference by gestational age and sex: the Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet, 2014.PMID 25209487
- [4]Papageorghiou AT International standards for fetal growth based on serial ultrasound measurements: the Fetal Growth Longitudinal Study of the INTERGROWTH-21st Project. Lancet, 2014.PMID 25209488
- [5]Villar J The likeness of fetal growth and newborn size across non-isolated populations in the INTERGROWTH-21st Project: the Fetal Growth Longitudinal Study and Newborn Cross-Sectional Study. The Lancet Diabetes & Endocrinology, 2014.PMID 25009082
- [6]Lees CC Perinatal morbidity and mortality in early-onset fetal growth restriction: cohort outcomes of the trial of randomized umbilical and fetal flow in Europe (TRUFFLE). Ultrasound in Obstetrics & Gynecology, 2013.PMID 24078432
- [7]Lees CC 2 year neurodevelopmental and intermediate perinatal outcomes in infants with very preterm fetal growth restriction (TRUFFLE): a randomised trial. Lancet, 2015.PMID 25747582
- [8]Ganzevoort W How to monitor pregnancies complicated by fetal growth restriction and delivery before 32 weeks: post-hoc analysis of TRUFFLE study. Ultrasound in Obstetrics & Gynecology, 2017.PMID 28182335
- [9]Ganzevoort W Comparative analysis of 2-year outcomes in GRIT and TRUFFLE trials. Ultrasound in Obstetrics & Gynecology, 2020.PMID 31125465
- [10]Crispi F Long-term cardiovascular consequences of fetal growth restriction: biology, clinical implications, and opportunities for prevention from birth. American Journal of Obstetrics and Gynecology, 2018.PMID 29422215
- [11]Romo A Anthropometric characterization of impaired fetal growth: risk factors for and prognosis of newborns with stunting or wasting. JAMA Pediatrics, 2015.PMID 26147058
- [12]McKinlay CJ Neonatal glycemia and neurodevelopmental outcomes at 2 years. New England Journal of Medicine, 2015.PMID 26465984
- [13]McKinlay CJD Association of neonatal glycemia with neurodevelopmental outcomes at 4.5 years. JAMA Pediatrics, 2017.PMID 28783802
- [14]Paules C Premature placental aging in term small-for-gestational-age and growth-restricted fetuses. Ultrasound in Obstetrics & Gynecology, 2019.PMID 30125412