Paeds · fetal-neonatal-and-perinatal
Human milk, fortification and preterm nutrition
Also known as Human milk, fortification and preterm nutrition · Preterm enteral nutrition · Human milk fortifier · Breast milk fortification
Fellowship guide to human milk fortification and preterm nutrition, covering growth targets, fortification strategy, and evidence for mother's own and donor milk.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Preterm nutrition is the clinical discipline of delivering energy, protein, minerals, and micronutrients at rates that reproduce the rapid intrauterine accretion the third trimester would have provided. The preterm infant is born with minimal glycogen and fat stores at exactly the moment the brain is growing fastest, so undernutrition during the NICU stay is not a cosmetic problem — it measurably lowers IQ and raises cerebral palsy risk [2].
The central operational challenge is that unfortified mother's own milk, while biologically ideal for the term infant, simply cannot deliver the protein and mineral load a foetus receives in the third trimester. A landmark cohort demonstrated that infants under 1500 g accumulate a cumulative protein and energy deficit within the first two weeks of life that is rarely recovered, producing growth that falls below the tenth centile at discharge in roughly half of very low birth weight (VLBW) infants [1].
Human milk fortification — adding protein, calcium, phosphate, energy, and micronutrients to expressed breast milk — is the intervention that bridges this gap. The ESPGHAN Committee on Nutrition sets the framework: preterm infants require 110 to 135 kcal/kg per day and 3.5 to 4.5 g/kg per day of protein to achieve the intrauterine growth rate of 15 to 20 g/kg per day [6].
Epidemiology & Risk Factors
The population at risk is the entire VLBW cohort — infants under 1500 g or born before 32 weeks. The degree of nutritional vulnerability is directly proportional to the degree of prematurity, because the most rapid phase of brain growth and nutrient accretion occurs between 28 and 40 weeks' gestation. An infant born at 26 weeks misses fourteen weeks of intrauterine nutrient delivery that must be replaced ex utero [2].
Extrauterine growth restriction (EUGR) — defined as weight below the tenth centile at 36 weeks' postmenstrual age or discharge — is the most common adverse outcome of inadequate nutrition. The seminal study of longitudinal growth in VLBW infants found that a substantial proportion were below the tenth centile for weight at discharge, and that the magnitude of growth faltering correlated with illness severity and the delay in establishing full enteral feeds [2].
Risk factors for nutritional failure include extreme prematurity, intrauterine growth restriction at birth, delayed initiation of parenteral nutrition, slow enteral feed advancement, and interruptions to feeding for procedures or suspected sepsis. The risk is compounded by the common but incorrect practice of withholding feeds for prolonged periods out of fear of necrotising enterocolitis (NEC), which paradoxically increases rather than decreases NEC risk [1].
Socioeconomically disadvantaged populations and Indigenous families in Australia and New Zealand face compounded risk through higher rates of preterm birth, reduced access to lactation support, and lower rates of mother's own milk availability at discharge — making equitable nutritional care a health-equity priority. [1]
Pathophysiology
The preterm infant is born mid-way through the most metabolically demanding phase of human development. During the third trimester, the foetus accrues protein, fat, calcium, and iron at rates that are physiologically impossible to achieve with unfortified human milk after birth. The foetal brain triples in volume and accumulates docosahexaenoic acid and iron at a pace that demands an ex utero equivalent [2].
Three converging deficits drive extrauterine growth restriction. First, limited nutrient stores: the preterm infant has negligible glycogen and fat reserves and low hepatic and skeletal mineral stores. Second, high metabolic demand: the work of breathing, thermoregulation, and ongoing organogenesis consume energy that the stable foetus never had to expend. Third, an immature gut with limited digestive and absorptive capacity constrains the volume and concentration of feeds that can be tolerated [1].
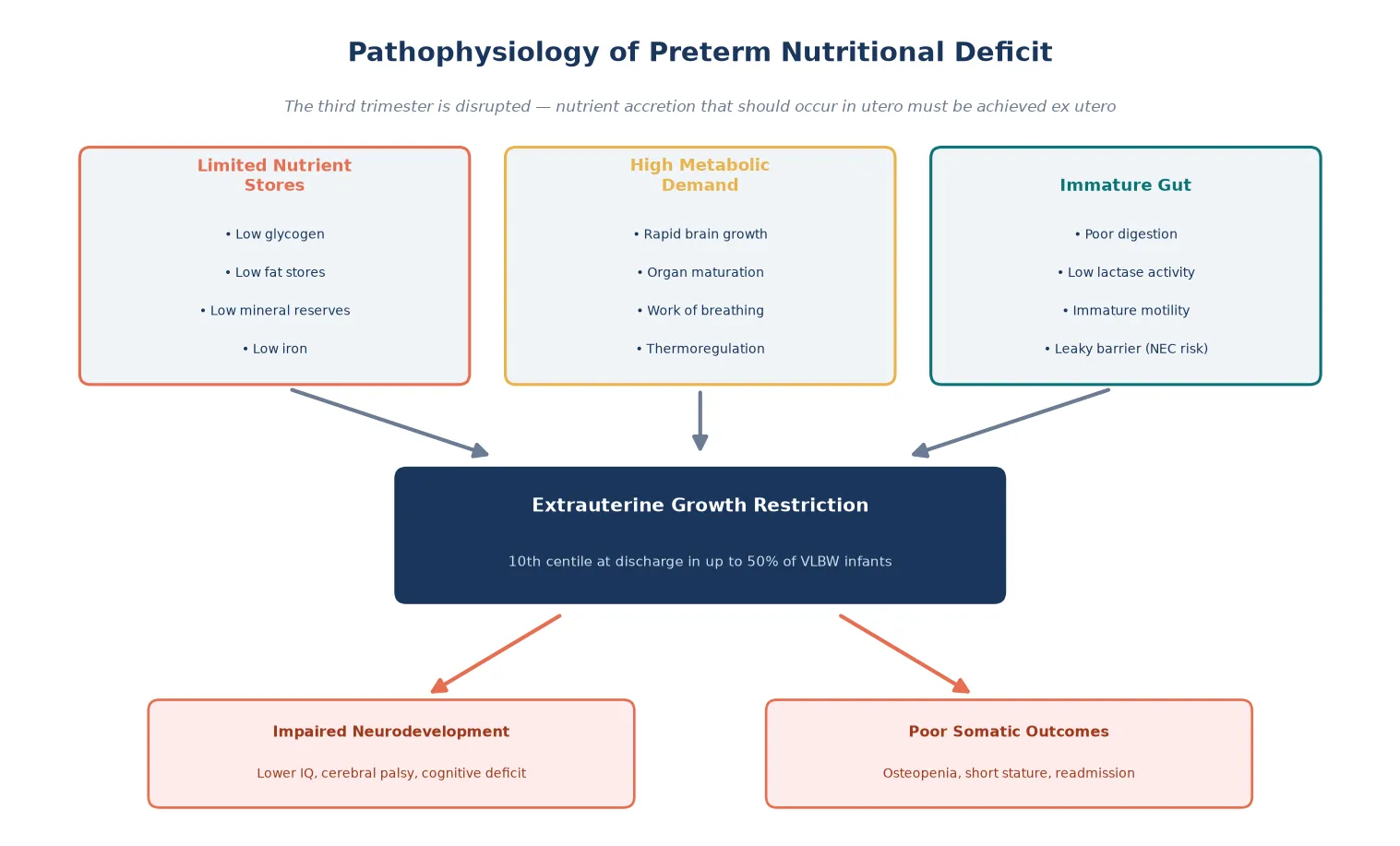
Unfortified human milk provides approximately 20 kcal per ounce (67 kcal per 100 mL) and about 1.0 g of protein per 100 mL — roughly half the protein and mineral concentration that the foetus receives transplacentally in the third trimester. Without fortification, even full enteral feeds at 150 mL/kg per day deliver only 100 kcal/kg per day and 1.5 g/kg per day of protein, a deficit that accumulates into measurable growth failure within two weeks [9].
The biological case for human milk despite this deficit rests on its non-nutritive properties. Human milk contains immunoglobulins, lactoferrin, oligosaccharides, stem cells, and growth factors that protect the preterm gut and actively promote intestinal maturation. The original epidemiological evidence that human milk feeding halves the incidence of NEC compared with formula established human milk as the preferred substrate, with fortification layered on top rather than replacing it [4].
[9]Classification
Preterm feeding strategy is classified by phase — parenteral, transition, full enteral, and growth optimisation — with the fortifier type overlaid once the infant reaches sufficient enteral volume. This phased approach prevents the abrupt nutritional transitions that destabilise the preterm gut [6].
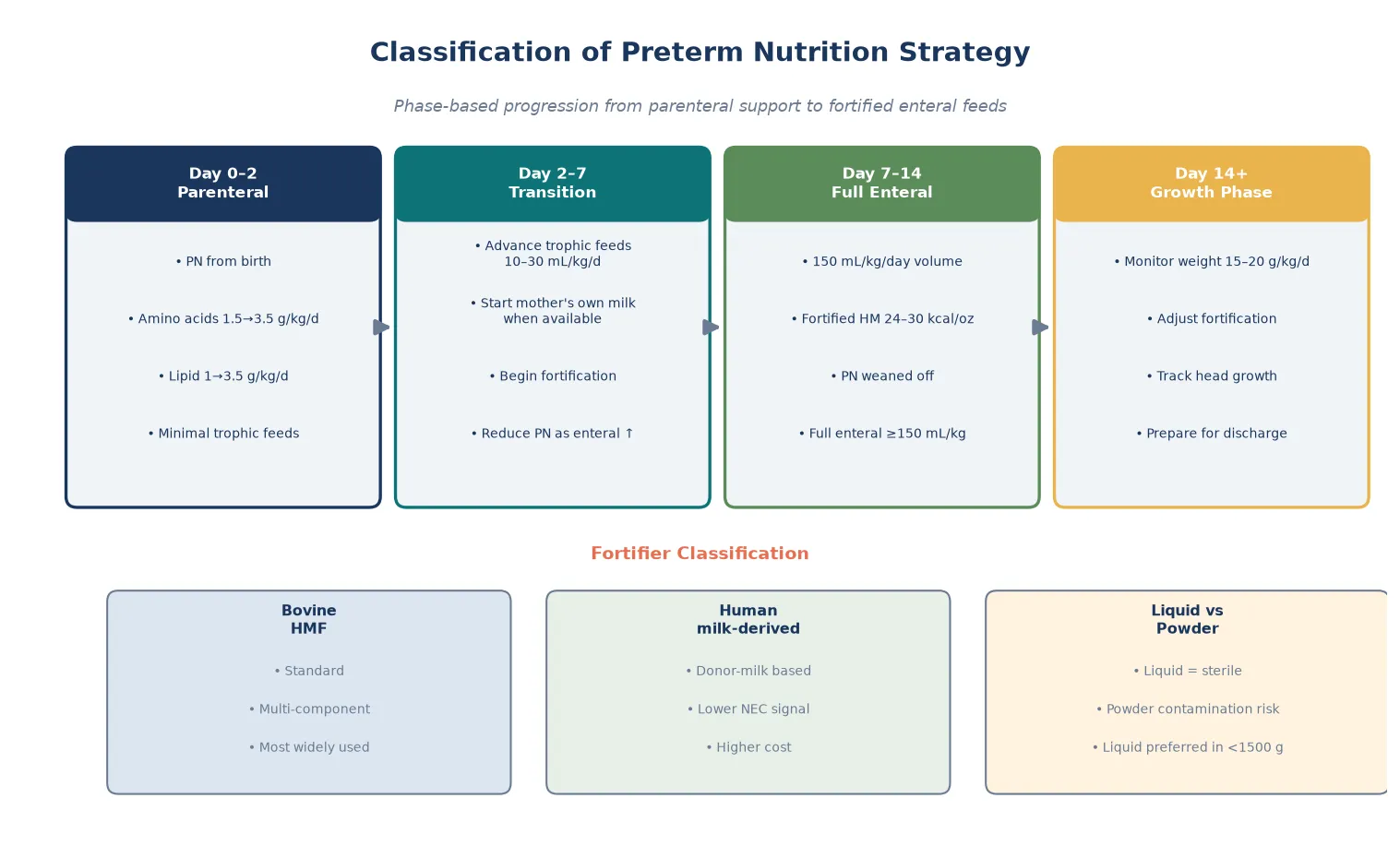
Fortifier itself is classified by source and formulation. Bovine-derived multicomponent fortifiers are the global standard, adding protein, carbohydrate, calcium, phosphate, and micronutrients to raise the milk to 24 to 30 kcal per ounce. Human milk-derived fortifiers, produced from donor milk, have emerged to create a fully human-milk diet and carry a signal toward lower NEC rates in extremely preterm infants. Liquid fortifiers are preferred over powder in infants under 1500 g because powder carries a risk of bacterial contamination [5].
Fortification strategy is further classified as standard (fixed-dose addition), adjustable (titrated by blood urea nitrogen and weight gain), and targeted or individualised (analysis of milk composition with addition of individual macronutrient modules to hit exact targets). Targeted fortification most closely replicates foetal accretion but requires laboratory infrastructure [10].
Clinical Presentation
The preterm infant with nutritional inadequacy does not present with acute symptoms in the way a septic or hypoxic infant does. The presentation is a trajectory — a weight curve that flattens, a head circumference that lags, and a cumulative deficit that becomes visible only on growth charts over weeks. The clinician must plot weight daily, length weekly, and head circumference weekly on Fenton (preterm) or Intergrowth-21st charts from birth [2].
Early signs that fortification is inadequate include weight gain consistently below 15 g/kg per day despite full enteral feeds at 150 mL/kg per day, a head circumference velocity below 0.9 cm per week, and a rising alkaline phosphatase with declining phosphate suggestive of metabolic bone disease. The blood urea nitrogen falls below 1.5 mmol/L, indicating protein inadequacy [6].
Conversely, the infant who is over-fortified or fed too rapidly presents with feed intolerance — increasing gastric aspirates, abdominal distension, and vomiting. These signs overlap with early NEC and demand immediate evaluation rather than simple feed reduction. The clinician must distinguish benign intolerance from surgical pathology at every feed [7].
Differential Diagnosis
Feed intolerance and growth failure in the preterm infant have a broad differential. The task is to distinguish benign, modifiable nutritional problems from surgical or infectious emergencies that mandate feed cessation [4].
| Condition | Key Features | Action |
|---|---|---|
| Feed intolerance | Mild distension, residual aspirates | Reduce rate, reassess in 12 h |
| Necrotising enterocolitis | Bilious aspirates, bloody stools, abdominal wall change | NPO, antibiotics, surgical review |
| Sepsis with ileus | Temperature instability, lethargy, raised CRP | Sepsis screen, cultures, antibiotics |
| Lactase deficiency | Loose acidic stools, perianal excoriation | Reduce lactose, consider lactose-free formula |
| Metabolic bone disease | Raised alk phos, low phosphate, fractures | Increase Ca and P fortification |
| Gastro-oesophageal reflux | Vomiting, desaturations, arching | Position, thicken feeds, anti-reflux |
The most critical distinction is between early NEC and simple feed intolerance. NEC is suggested by systemic signs (lethargy, apnoea, temperature instability), abdominal wall changes (erythema, induration, discolouration), and radiographic pneumatosis intestinalis. Any preterm infant with bilious aspirates or abdominal wall changes must be made nil by mouth immediately and evaluated for NEC [4].
Growth failure may also reflect non-nutritional causes — congenital heart disease with increased work of breathing, chronic lung disease, recurrent sepsis, or undiagnosed metabolic disease. These must be excluded before attributing poor growth solely to inadequate fortification [2].
Clinical & Bedside Assessment
Bedside assessment of the preterm infant's nutritional status is a daily, longitudinal exercise. The weight is measured daily and plotted on a Fenton chart from birth to 50 weeks' postmenstrual age, targeting a weight velocity of 15 to 20 g/kg per day to mirror intrauterine growth. Length and head circumference are measured weekly, with head growth the most sensitive marker of adequate nutrition and a proxy for brain growth [2].
The abdominal examination precedes every feed advancement. The clinician assesses for distension, tenderness, abdominal wall discolouration, and bowel sounds, and records gastric residual volumes. A benign residual is non-bilious and less than 50 percent of the previous feed volume; bilious or bloody residuals demand immediate investigation for NEC [7].
Biochemical monitoring tracks the adequacy of specific nutrients. Blood urea nitrogen reflects protein intake. Alkaline phosphatase, calcium, and phosphate screen for metabolic bone disease, which affects up to 30 percent of very preterm infants. Haemoglobin and ferritin guide iron supplementation, typically started at 2 to 4 mg/kg per day from four weeks of age [6].
Investigations
Growth chart plotting is the single most important investigation. Serial weight on Fenton or Intergrowth-21st charts reveals the trajectory that single measurements cannot. An infant tracking parallel to the centile lines is growing well; one whose trajectory flattens or crosses centile lines downward needs nutritional intervention [2].
Biochemistry panels guide fortification. The baseline panel includes blood urea nitrogen, creatinine, electrolytes, alkaline phosphatase, calcium, phosphate, and full blood count. These are repeated weekly during the acute growth phase and adjusted to the fortification strategy. A rising alkaline phosphatase above 800 IU/L with phosphate below 1.5 mmol/L indicates metabolic bone disease requiring intensified mineral fortification [6].
Abdominal radiography is reserved for suspected complications. A flat and decubitus film is obtained when NEC is suspected to look for pneumatosis intestinalis, portal venous gas, or free air. Routine radiography is not part of nutritional monitoring [4].
Nutritional monitoring pathway
Daily weight on Fenton chart — target 15 to 20 g/kg/day
Weekly length and head circumference — head growth above 0.9 cm/week
Weekly BUN above 1.5 mmol/L for protein adequacy
Weekly alk phos, Ca, PO4 for metabolic bone disease
Abdominal exam before each feed advance
Adjust fortifier by trajectory — standard, adjustable, or targeted
Management — Resuscitation
The nutritional "resuscitation" of the preterm infant begins in the first hours of life with parenteral nutrition. Because the preterm gut cannot tolerate full enteral feeds immediately, the infant will accumulate a deficit unless amino acids and energy are provided intravenously from birth. ESPGHAN recommends starting parenteral amino acids at 1.5 to 2 g/kg per day within hours of birth, advancing to 3.5 g/kg per day [6].
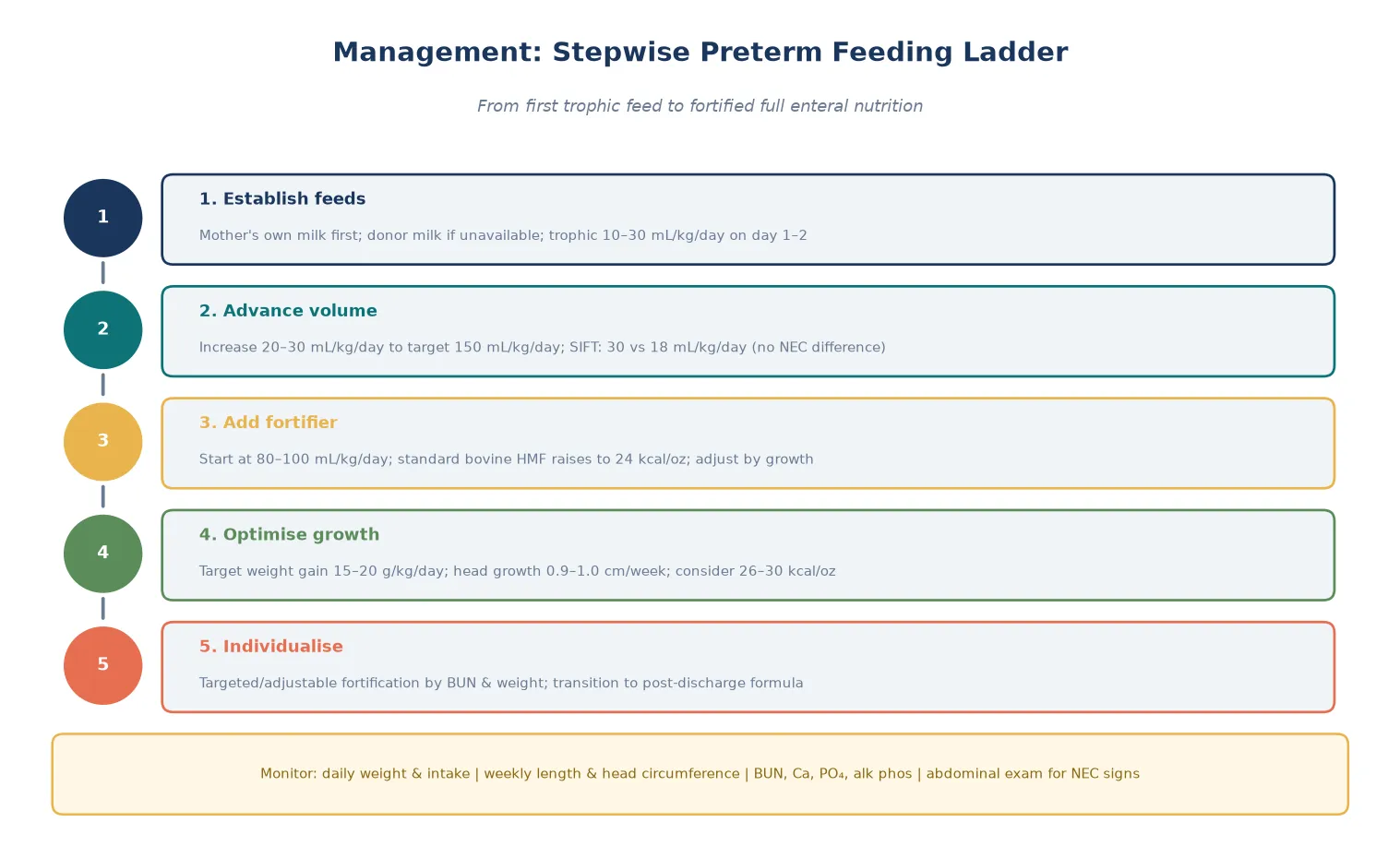
Enteral feeds are initiated as soon as the infant is haemodynamically stable, typically on day one or two, using trophic volumes of 10 to 30 mL/kg per day of mother's own milk or donor milk. Trophic feeds stimulate gut maturation through hormonal and trophic effects rather than contributing meaningfully to nutrition, which remains parenteral during this phase [7].
Feed advancement follows a graduated protocol. Volume is increased by 20 to 30 mL/kg per day toward a target of 150 mL/kg per day. The SIFT trial, the definitive randomised evidence on feed advancement, compared rapid (30 mL/kg/day) with slow (18 mL/kg/day) advancement in very preterm infants and found no significant difference in survival without disability, giving clinicians licence to advance feeds at the faster rate in haemodynamically stable infants without fear of increasing NEC [7].
Human milk fortifier (bovine multicomponent)
Loading dose
Standard addition: 1 sachet per 50 or 100 mL per manufacturer
Maintenance dose
Raises milk from 20 to 24 kcal/oz; may increase to 26 to 30 kcal/oz
Management — Definitive & Stepwise
Definitive nutritional management is a longitudinal, phase-based strategy that transitions the infant from total parenteral nutrition to fortified full enteral feeds while protecting the gut and optimising growth. There is no single dose — the plan adapts daily to the growth trajectory, feed tolerance, and biochemical markers [6].
Phase 1 — Parenteral nutrition and trophic feeds
Parenteral nutrition with amino acids at 1.5 to 3.5 g/kg per day, glucose, and lipid is established from the first hours of life and maintained until enteral feeds reach 120 to 150 mL/kg per day. Trophic feeds of 10 to 30 mL/kg per day of mother's own milk begin on day one or two [6].
Phase 2 — Feed advancement and fortification
Feeds are advanced by 20 to 30 mL/kg per day to a target of 150 mL/kg per day. When enteral volume reaches 80 to 100 mL/kg per day, multicomponent fortifier is added to raise the caloric density from 20 to 24 kcal per ounce, with protein content increasing toward the 3.5 to 4.5 g/kg per day target [9].
The Cochrane review of multicomponent fortification confirms that fortification produces modest but statistically significant short-term improvements in weight gain, length, and head circumference without increasing NEC risk — the evidence base that justifies routine fortification in VLBW infants [9].
Phase 3 — Optimising and individualising
For infants who fail to achieve target growth on standard fortification, the strategy intensifies. Caloric density may be increased to 26 or 30 kcal per ounce. Adjustable fortification titrates the protein dose by blood urea nitrogen, adding more protein when BUN falls below 1.5 mmol/L. Targeted fortification analyses the actual macronutrient content of each mother's milk batch and adds individualised protein, carbohydrate, and fat modules to hit exact targets, most closely replicating foetal accretion [10].
FORTIFY
Human milk versus formula — the evidence
The choice of base substrate is settled by evidence. The original case-control study demonstrated that human milk halves the incidence of NEC compared with formula, a finding replicated across decades and populations [4]. The randomised trial by Sullivan and colleagues extended this to fortifier choice, showing that an exclusively human milk-based diet (mother's milk plus human milk-derived fortifier) was associated with a lower NEC rate than a diet combining human milk with bovine-based products [5].
The Cristofalo trial confirmed that extremely premature infants randomised to an exclusive human milk diet had similar growth but significantly lower NEC and mortality than those fed preterm formula [8]. The Cochrane review of formula versus donor breast milk found that donor milk, while associated with slower short-term growth, reduces NEC compared with formula — justifying donor milk as the substitute when mother's own milk is unavailable [3].
Specific Subtypes & Scenarios
| Scenario | Strategy | Evidence |
|---|---|---|
| Mother's own milk available | First-line substrate; fortify to 24 kcal/oz | Lucas 1990 — NEC halving |
| Mother's own milk unavailable | Donor human milk; fortify similarly | Quigley 2019 — donor milk < NEC |
| VLBW with EUGR | Intensify to 26–30 kcal/oz; adjustable fortification | Embleton 2001 |
| Extreme prematurity (<1000 g) | Exclusive human-milk diet if available | Sullivan 2010, Cristofalo 2013 |
| Feed intolerance on bovine HMF | Switch to human-milk-derived HMF | Sullivan 2010 |
| Post-discharge preterm | Post-discharge formula or continued fortification | ESPGHAN 2010 |
The extremely low birth weight (ELBW) infant under 1000 g represents the highest-stakes subgroup. These infants have the greatest nutrient deficit, the most immature gut, and the highest NEC risk. An exclusively human milk-based diet — mother's own milk plus human milk-derived fortifier, with donor milk as a bridge — is the evidence-based standard where available, supported by the Sullivan and Cristofalo trials [5].
The late preterm infant (34 to 36 weeks) is often presumed to be nutritionally robust but in fact commonly fails to establish adequate oral feeding and may develop significant dehydration and jaundice. Fortification is less aggressive than in the ELBW group, but growth monitoring and feeding support remain essential [2].
[6]Complications & Pitfalls
The most feared complication of enteral feeding is necrotising enterocolitis, a fulminant inflammatory bowel necrosis with mortality of 20 to 30 percent. NEC is more common with formula feeding, rapid feed advancement in unstable infants, and in the presence of patent ductus arteriosus or sepsis. The protective effect of human milk is the strongest modifiable evidence-based intervention [4].
Metabolic bone disease of prematurity affects up to 30 percent of very preterm infants and results from inadequate calcium and phosphate delivery. It presents with a rising alkaline phosphatase above 800 IU/L, declining phosphate, and in severe cases rib and long-bone fractures. Prevention requires adequate mineral fortification from the onset of feeds [6].
The most common pitfall is under-fortification driven by fear of feed intolerance. Clinicians who routinely hold or dilute feeds, or who fail to introduce fortifier at the recommended volume, guarantee extrauterine growth restriction and its neurodevelopmental consequences. The counter-pitfall is over-fortification — concentrating feeds above 30 kcal per ounce or pushing protein above 4.5 g/kg per day causes osmotic diarrhoea and metabolic acidosis [9].
Prognosis & Disposition
The prognosis of preterm nutrition is directly measurable: an infant who grows at the intrauterine rate through to discharge has the best available neurodevelopmental outcome. Cohort data show that the rate of weight gain in the NICU is an independent predictor of cognitive and motor outcomes at 18 to 22 months, with each additional 10 g/kg per day of weight gain associated with measurably higher developmental scores [2].
Conversely, extrauterine growth restriction at discharge predicts worse outcomes. The seminal cohort study established that infants whose weight fell below the tenth centile during their hospital stay had higher rates of cerebral palsy, subnormal mental development index, and neurodevelopmental impairment at follow-up — establishing growth failure as a preventable cause of disability, not merely a cosmetic concern [1].
Discharge planning for the preterm infant requires sustained nutritional support beyond the NICU. The infant should be on stable full enteral feeds with documented growth at the target rate, and a post-discharge plan — either continued fortification, post-discharge preterm formula, or breastfeeding support with monitoring — must be in place to prevent late growth failure in the community [6].
Special Populations
Indigenous infants in Australia and New Zealand carry a disproportionate burden of preterm birth and its nutritional consequences. Aboriginal and Torres Strait Islander and Māori infants have higher rates of prematurity and lower rates of sustained mother's own milk feeding at discharge, compounding the risk of extrauterine growth restriction. Culturally safe lactation support, peer counselling, and kangaroo mother care are essential to equitable nutritional outcomes [2].
Infants from socioeconomically disadvantaged backgrounds face additional barriers including limited access to donor milk, lactation support, and post-discharge follow-up. These families need proactive nutritional planning and community health integration to prevent the post-discharge growth faltering that widens developmental inequity [1].
Technology-dependent infants with complex chronic conditions — those with short bowel syndrome, bronchopulmonary dysplasia, or congenital anomalies requiring prolonged hospitalisation — need individualised, multidisciplinary nutritional plans. These infants frequently require extended fortification, specialised formulas, or long-term enteral feeding devices and warrant coordinated discharge planning [6].
Evidence, Guidelines & Regional Differences
The Lucas and Cole study from 1990 remains the foundational evidence that human milk protects against NEC. In a cohort of nearly 1000 preterm infants, exclusive formula feeding increased the risk of NEC six-fold compared with exclusive human milk feeding, establishing the principle that human milk is not merely nutrition but active gastrointestinal protection [4].
The Sullivan trial in 2010 was the first randomised controlled trial to show that an exclusively human milk-based diet was associated with a lower rate of NEC and surgical NEC compared with a diet incorporating bovine milk-based products. This extended the "human milk first" principle from the base milk to the fortifier itself [5].
SIFT (2020)
RCT: rapid (30 mL/kg/day) vs slow (18 mL/kg/day) feed advancement
Population: 2804 very preterm or VLBW infants
Key finding
No significant difference in primary outcome or NEC
Practice change
Gives clinicians licence to advance feeds at the faster rate in stable infants
The Cochrane review of multicomponent fortification remains the evidence base for routine fortification, confirming improved short-term growth without increased NEC [9]. The Cochrane review of formula versus donor breast milk confirms that donor milk reduces NEC at the cost of slower short-term growth — justifying donor milk as the second-line substrate [3].
Regional differences centre on fortifier availability and cost. ANZ and European units predominantly use bovine liquid HMF as standard, with human milk-derived fortifier reserved for tertiary centres and high-risk infants. North American practice varies widely, with some networks adopting exclusive human-milk diets for ELBW infants. Low-resource settings rely on mother's own milk with locally produced or improvised fortification, recognising that the protective effect of any human milk outweighs the risk of no fortification [6].
Exam Pearls
The single most testable fact is the ESPGHAN target: 110 to 135 kcal/kg per day energy and 3.5 to 4.5 g/kg per day protein, achieved with fortified feeds at 24 to 30 kcal per ounce. Know these numbers precisely — they appear in every neonatal nutrition question [6].
The protective effect of human milk against NEC is the second key concept. The Lucas cohort showed a six-fold NEC increase with formula, and the Sullivan trial extended this to fortifier choice — an exclusively human milk diet reduces NEC. Donor milk is the substitute when mother's milk is unavailable [4].
The SIFT trial is the modern evidence on feed advancement: rapid (30 mL/kg/day) versus slow (18 mL/kg/day) showed no difference in survival without disability or NEC, so clinicians need not fear faster advancement in stable infants. This directly contradicts older dogma that slow advancement is safer [7].
NUTRITION TARGETS
References
- [1]Embleton NE, Pang N, Cooke RJ Postnatal malnutrition and growth retardation: an inevitable consequence of current recommendations in preterm infants? Pediatrics, 2001.PMID 11158457
- [2]Ehrenkranz RA, Younes N, Lemons JA, et al Longitudinal growth of hospitalized very low birth weight infants Pediatrics, 1999.PMID 10429008
- [3]Quigley M, Embleton ND, McGuire W Formula versus donor breast milk for feeding preterm or low birth weight infants Cochrane Database Syst Rev, 2019.PMID 31322731
- [4]Lucas A, Cole TJ Breast milk and neonatal necrotising enterocolitis Lancet, 1990.PMID 1979363
- [5]Sullivan S, Schanler RJ, Kim JH, et al An exclusively human milk-based diet is associated with a lower rate of necrotizing enterocolitis than a diet of human milk and bovine milk-based products J Pediatr, 2010.PMID 20036378
- [6]Agostoni C, Buonocore G, Carnielli VP, et al Enteral nutrient supply for preterm infants: commentary from the European Society of Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition J Pediatr Gastroenterol Nutr, 2010.PMID 19881390
- [7]Dorling J, Hewer O, Hurd M, et al Two speeds of increasing milk feeds for very preterm or very low-birthweight infants: the SIFT RCT Health Technol Assess, 2020.PMID 32342857
- [8]Cristofalo EA, Schanler RJ, Blanco CL, et al Randomized trial of exclusive human milk versus preterm formula diets in extremely premature infants J Pediatr, 2013.PMID 23968744
- [9]Kuschel CA, Harding JE Multicomponent fortified human milk for promoting growth in preterm infants Cochrane Database Syst Rev, 2004.PMID 14973953
- [10]Fusch S, Fusch G, Yousuf EI, et al Individualized Target Fortification of Breast Milk: Optimizing Macronutrient Content Using Different Fortifiers and Approaches Front Nutr, 2021.PMID 34621769