Paeds · fetal-neonatal-and-perinatal
Hypoxic-ischaemic encephalopathy and therapeutic hypothermia
Also known as Hypoxic-ischaemic encephalopathy and therapeutic hypothermia · Perinatal asphyxia and neonatal brain injury · Birth asphyxia encephalopathy · Neonatal hypothermia neuroprotection (cooling) · HIE
Fellowship guide to hypoxic-ischaemic encephalopathy and therapeutic hypothermia: the excitotoxic cascade and latent phase, Sarnat staging and cooling eligibility, the 6-hour window, the 72-hour cooling protocol, supportive neurocare, MRI prognostication and the adjuvant-therapy controversies.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A term newborn who is limp, silent, and not breathing at birth, and who does not recover to a normal neurological state within hours, has sustained a hypoxic-ischaemic insult to the brain. When that insult produces a clinical syndrome of disturbed neurological function in the first days of life, the diagnosis is neonatal encephalopathy; when the cause is hypoxia and ischaemia around the time of birth, it is hypoxic-ischaemic encephalopathy (HIE). [10]
Hypoxic-ischaemic encephalopathy is not simply "birth asphyxia." It is a distinct clinicopathological syndrome: a recognisable constellation of altered consciousness, abnormal tone, depressed or absent primitive reflexes, autonomic disturbance, feeding difficulty, and (often) seizures, set against a history and biochemical evidence of perinatal asphyxia. The decisive clinical task is to grade its severity quickly, because moderate and severe HIE are eligible for the one intervention proven to change outcome — therapeutic hypothermia. [1] [4]
Classification
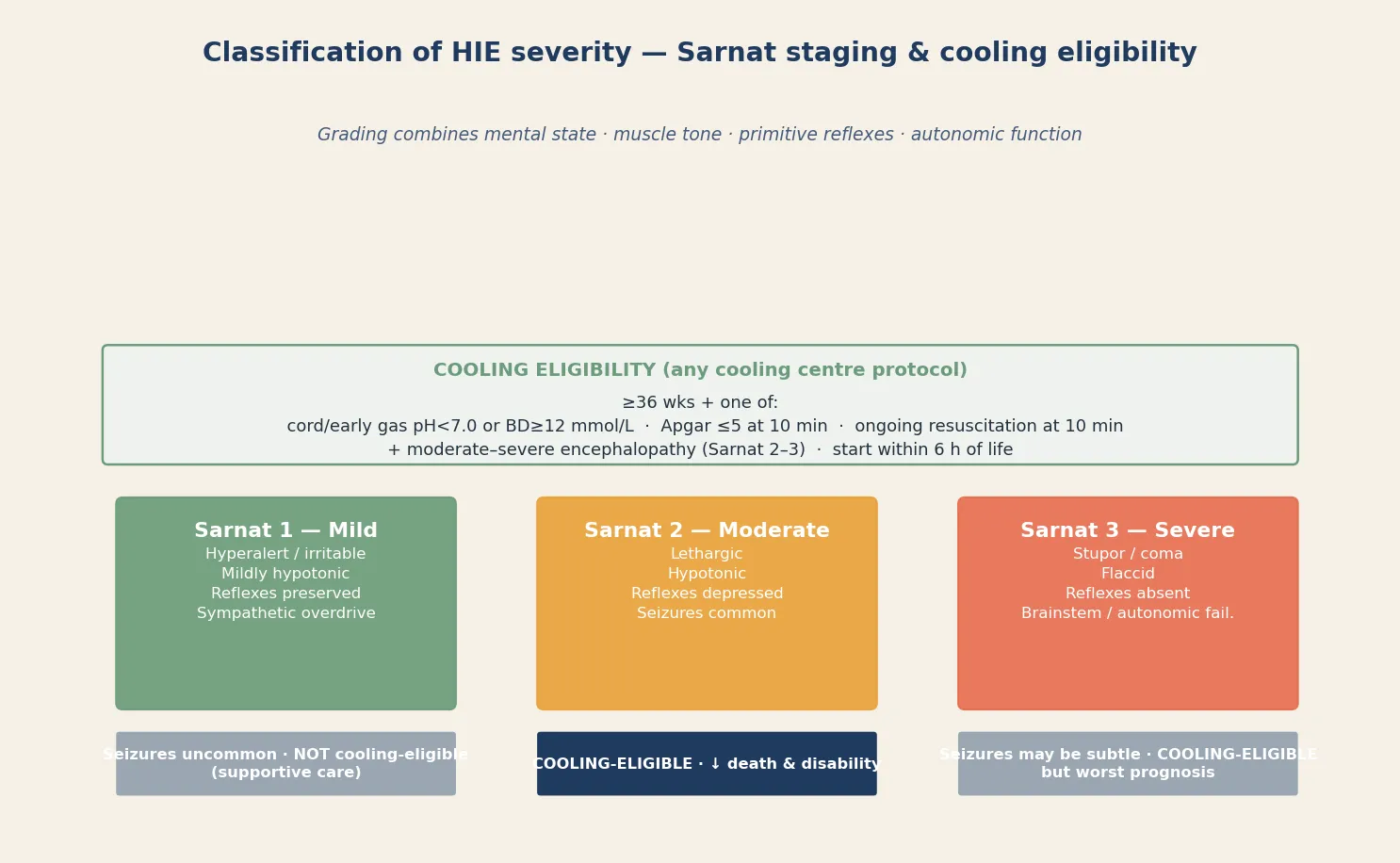
Hypoxic-ischaemic encephalopathy is classified by severity, and severity is the gateway to treatment. The Sarnat staging system, described by Sarnat and Sarnat in 1976, combines four clinical domains — mental state, muscle tone, primitive reflexes, and autonomic function — into three stages that map directly onto the cooling decision. [1]
Sarnat stage 1 (mild) shows hyperalertness and irritability with mildly increased or normal tone, preserved reflexes, and sympathetic overdrive; seizures are uncommon and the infant usually recovers fully. Sarnat stage 2 (moderate) shows lethargy, hypotonia, depressed primitive reflexes, and seizures; this stage is cooling-eligible. Sarnat stage 3 (severe) shows stupor or coma, flaccid tone, absent reflexes, and brainstem or autonomic failure, with a worse prognosis — and it is also cooling-eligible. The staging is dynamic, so a stage-2 infant can evolve to stage 3, and the most severe stage reached guides both the cooling decision and prognosis. [1] [10]
Epidemiology & Risk Factors
Hypoxic-ischaemic encephalopathy affects roughly 1 to 3 per 1000 live term births in high-income settings, and it remains a leading cause of neonatal death and long-term neurological disability worldwide. The incidence is several-fold higher in low- and middle-income settings, where perinatal asphyxia is still a dominant cause of under-five mortality. [10]
The antecedents of HIE are the events that deprive the fetus of oxygenated blood. Sentinel perinatal events — placental abruption, uterine rupture, cord prolapse, severe placental insufficiency, or a tight nuchal cord — interrupt fetoplacental gas exchange acutely. Intrapartum factors include prolonged or obstructed labour, chorioamnionitis, and non-reassuring cardiotocography. Maternal conditions such as severe pre-eclampsia and placental insufficiency produce chronic hypoxia that depletes fetal reserve, so the fetus tolerates an acute intrapartum event poorly. [10]
The strongest predictors that an encephalopathic infant has suffered perinatal asphyxia, rather than another cause of neonatal encephalopathy, are the biochemical markers of acute hypoxia. A cord or early postnatal blood gas pH under 7.0, a base deficit of at least 12 mmol/L, an Apgar score of 5 or less at 10 minutes, or the need for ongoing resuscitation including ventilation at 10 minutes each support the diagnosis. These are not academic thresholds — they are the entry criteria that most cooling protocols use to establish cooling eligibility. [3] [4]
Pathophysiology
The injury in HIE unfolds in phases, and understanding the phases is the whole basis of cooling. The initial hypoxic-ischaemic event causes a primary energy failure: the brain is deprived of oxygen and glucose, ATP production collapses, and the sodium-potassium pump and membrane ion channels fail. Neurons depolarise, glutamate floods the synapse, and over-activation of NMDA and AMPA receptors drives a massive influx of calcium and sodium into the cell. This is the excitotoxic cascade, and it generates both seizures and cell death by necrosis. [10]
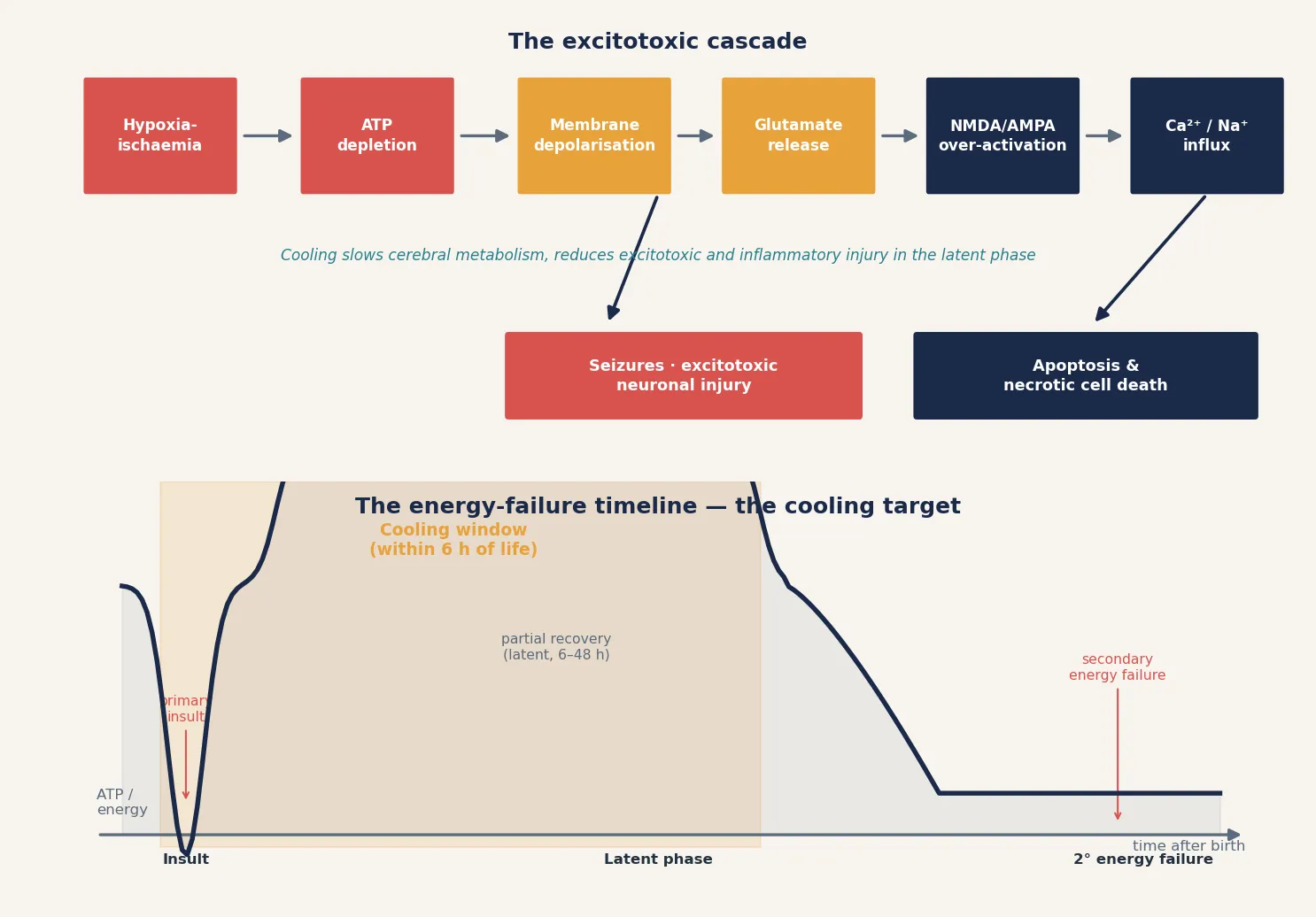
The crucial feature is what happens next. After resuscitation, cerebral metabolism partially recovers — this is the latent phase, lasting roughly 6 to 48 hours. The infant may even look better. But a secondary energy failure then follows, driven by mitochondrial dysfunction, ongoing excitotoxicity, oxidative stress, and inflammation, producing a second wave of neuronal apoptosis and necrosis. This is why an infant can look deceptively well in the first hours and deteriorate over the following day. [10]
The latent phase is the therapeutic target. Cooling the brain to 33.5 to 34.5 °C slows cerebral metabolism by roughly 5 to 8 percent per degree, reduces excitotoxic and inflammatory injury, and interrupts the secondary cascade — but only if it is established before the secondary energy failure takes hold, which is the entire reason for the 6-hour window. [4] [5]
The pattern of brain injury depends on the maturity of the brain and the nature of the insult. In the term brain, a profound acute insult (as in sentinel events like abruption) injures the deep grey matter — the basal ganglia, thalamus, and posterior limb of the internal capsule — producing the severe pattern associated with motor disability and a poor outcome. A milder, more prolonged insult injures the parasagittal watershed zones, producing a cognitive-predominant pattern with a relatively better prognosis. These patterns are visible on MRI and carry prognostic weight. [7]
Clinical Presentation
The clinical presentation of HIE is the encephalopathic newborn, and the signs map directly onto the Sarnat domains. The infant is lethargic rather than alert, with generalised hypotonia and depressed or absent primitive reflexes. Autonomic disturbance shows as poor perfusion, abnormal respiratory pattern, and disturbed heart-rate variability. Seizures are common in moderate and severe HIE and are often the first sign that brings the infant to attention. [1] [10]
A striking and examiner-favoured feature is the deceptively well appearance during the latent phase. After resuscitation the infant may transiently look better as cerebral metabolism partially recovers, only to deteriorate over the following day when secondary energy failure takes hold. This waxing course is why a single bedside assessment is not enough — the infant is observed and re-examined, and the most severe Sarnat stage reached drives the cooling decision and prognosis. [10]
Severe HIE (Sarnat stage 3) presents with stupor or coma, flaccid tone, absent primitive reflexes, and brainstem or autonomic failure. This is the worst presentation and the worst prognosis, yet it is still cooling-eligible — severity is never a reason to withhold cooling. Mild HIE (Sarnat stage 1) presents with hyperalertness, irritability, and preserved reflexes; it is not cooling-eligible and the infant usually recovers fully. [1] [4]
Differential Diagnosis
The diagnosis of HIE requires evidence of perinatal asphyxia as the cause of the encephalopathy. Several other conditions produce neonatal encephalopathy and can mimic HIE, and they must be actively excluded, because cooling is not the treatment for sepsis, a metabolic disorder, or a stroke. The distinction is made on the history, the biochemistry, and the time course. [10]
Sepsis and meningitis can produce an encephalopathic picture indistinguishable from HIE at the bedside, and the two can coexist after prolonged rupture of membranes or chorioamnionitis. A septic screen and early antibiotics are part of the first-hour work-up of any encephalopathic infant. Metabolic encephalopathies — hypoglycaemia, inborn errors of metabolism, urea cycle disorders — present with encephalopathy and sometimes seizures; checking the blood glucose, ammonia, lactate, and a metabolic screen is essential. Vascular causes include arterial stroke and sinovenous thrombosis, which present with focal seizures and asymmetry. [10]
[10]Clinical & Bedside Assessment
Bedside assessment has one purpose: to grade the encephalopathy and decide on cooling, fast. The assessment begins the moment an infant is identified as depressed at birth or encephalopathic on the postnatal ward. Airway, breathing, and circulation are stabilised first; the capillary glucose is checked immediately; and a focused neurological examination is performed to assign a Sarnat stage. [1] [4]
The Sarnat examination assesses four domains. Mental state ranges from hyperalert (stage 1) through lethargy (stage 2) to stupor or coma (stage 3). Muscle tone moves from normal or mildly increased through hypotonia to flaccidity. The primitive reflexes — Moro, grasp, suck, and the deep tendon reflexes — are preserved in stage 1, depressed in stage 2, and absent in stage 3. Autonomic function moves from sympathetic overdrive through mixed to brainstem failure, reflected in pupillary response, heart rate variability, and respiratory pattern. [1]
The history reweights the differential. The clinician captures the perinatal course, any sentinel event (abruption, cord prolapse, uterine rupture), the cardiotocograph, the Apgar scores, the cord blood gases, the resuscitation required, the maternal temperature and infection risk, and the gestation. A preterm infant under 36 weeks, an infant with a major congenital anomaly, or an infant whose encephalopathy is better explained by sepsis or metabolic disease is not a candidate for standard cooling — these exclusions are applied during the bedside assessment. [4] [10]
Investigations
Investigations in suspected HIE serve three purposes: to confirm perinatal asphyxia, to exclude the mimics, and to prognosticate. The immediate tests run in parallel with the cooling decision. A cord or early postnatal blood gas confirms the acidosis. Blood glucose, full blood count, coagulation profile, electrolytes, liver function, and a septic screen (blood culture, CRP, and lumbar puncture once stable) exclude metabolic and infective contributors. [4] [10]
Continuous amplitude-integrated EEG (aEEG) or, where available, full conventional video-EEG, is started early. The background pattern carries prognostic weight: a suppressed or flat background that fails to recover predicts an adverse outcome, and ongoing seizure activity is detected and treated to an electrographic endpoint. The EEG is also part of some cooling eligibility protocols, where an abnormal aEEG background combined with encephalopathy confirms the diagnosis even when the blood gas is borderline. [4]
Magnetic resonance imaging is the gold standard for prognostication, performed between days 4 and 7, after rewarming. The injury pattern on MRI maps onto outcome: a basal ganglia–thalamus–posterior limb pattern (the severe, profound-insult pattern) predicts a high risk of cerebral palsy; a watershed-zone pattern predicts a cognitive-predominant outcome with a relatively better motor prognosis. MR spectroscopy adds biochemical information (lactate elevation, N-acetylaspartate reduction) that refines prognosis. [7]
Management — Resuscitation
Resuscitation of the infant who will develop HIE follows the standard neonatal resuscitation algorithm, with the addition of post-resuscitation neuroprotection. The airway is secured, breathing supported with positive pressure ventilation or intubation as needed, and circulation maintained. Delayed cord clamping and cord milking are avoided in the asphyxiated infant requiring immediate resuscitation. Once the infant is stable, the focus shifts to the brain. [4]
The post-resuscitation principle is to avoid the secondary insults that extend the primary injury. Hyperthermia worsens outcome — even a modestly elevated temperature is harmful — so the asphyxiated infant is kept normothermic while cooling is being assessed, never actively warmed. Hypoglycaemia, hypotension, hypocapnia, and hypercapnia each independently worsen brain injury, so glucose, blood pressure, and carbon dioxide are monitored and maintained in the normal range from the outset. [10]
Immediate resuscitation and the cooling trigger
Stabilise airway, breathing, circulation per neonatal resuscitation algorithm
Check blood glucose immediately; treat hypoglycaemia with 10% dextrose 2 mL/kg IV
Keep normothermic — avoid active warming; never allow hyperthermia
Send cord / early blood gas; obtain Apgar and resuscitation history
Perform Sarnat staging at the bedside
If Sarnat 2 or 3 with asphyxia evidence — activate cooling within 6 h of life
Send septic screen; start antibiotics; start continuous EEG / aEEG
Management — Definitive & Stepwise
Therapeutic hypothermia is the standard of care for moderate-to-severe HIE in term infants, established by three landmark randomised trials — the CoolCap selective head cooling trial (Gluckman 2005), the NICHD whole-body hypothermia trial (Shankaran 2005), and the TOBY trial (Azzopardi 2009) — and confirmed by the Jacobs 2013 Cochrane meta-analysis. Cooling reduces death and major disability by roughly a quarter, and it is now the global standard of care in tertiary centres. [2] [3] [4] [5]
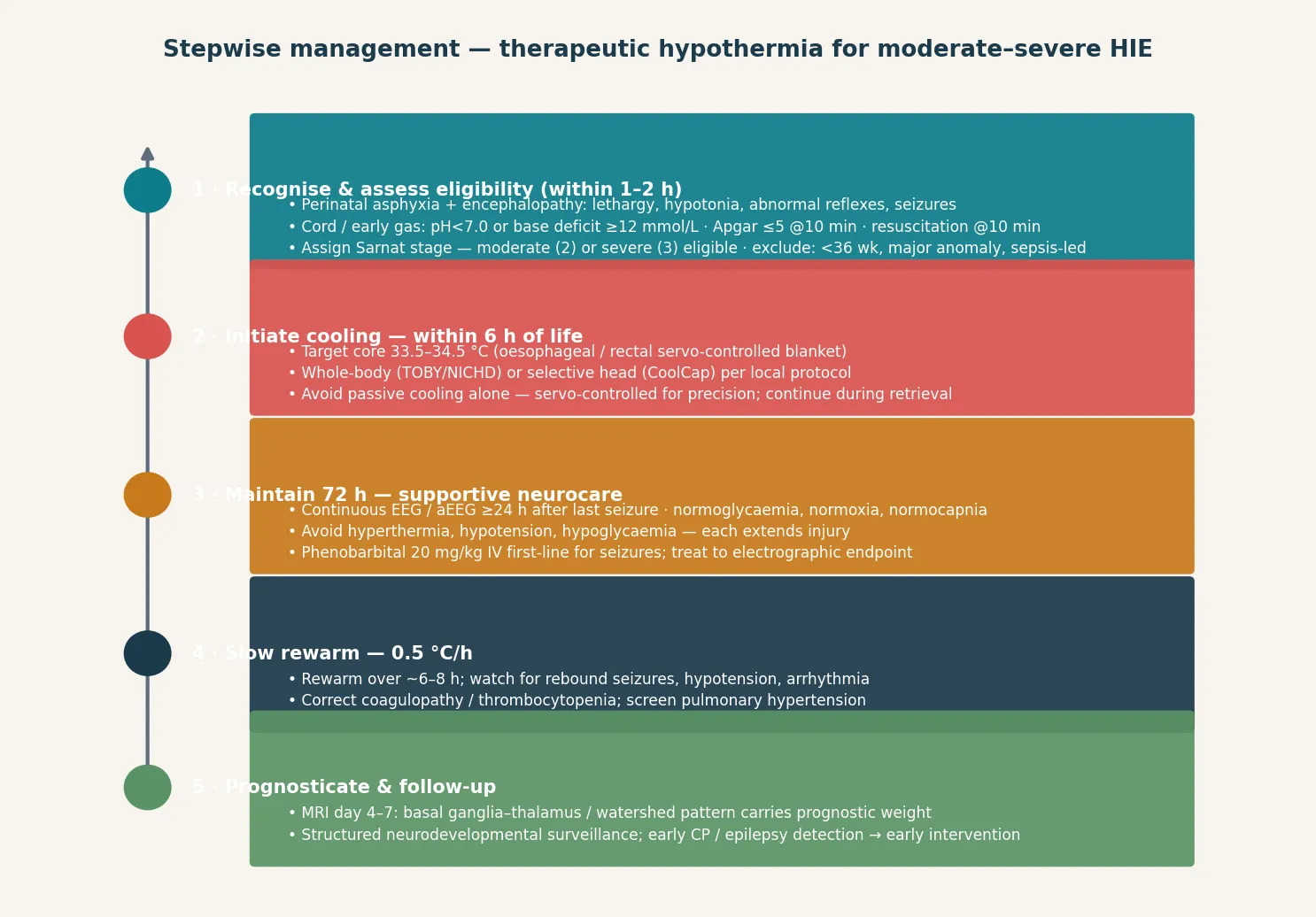
The cooling protocol is standardised. A term infant (at least 36 weeks) with moderate or severe HIE (Sarnat 2 or 3) and biochemical evidence of perinatal asphyxia is cooled to a core temperature of 33.5 to 34.5 °C, maintained for 72 hours, then rewarmed slowly at 0.5 °C per hour. Cooling is initiated within 6 hours of life, ideally with a servo-controlled whole-body or selective-head device; passive cooling alone is imprecise and reserved for transport when no servo device is available, with close temperature monitoring. [4] [5]
During the 72 hours of cooling, supportive neurocare is as important as the hypothermia itself. The metabolic targets are normoglycaemia, normoxia, normocapnia, and normotension — each secondary insult extends the brain injury cooling is trying to prevent. Seizures are detected on continuous EEG or aEEG and treated to an electrographic endpoint, with phenobarbital 20 mg/kg intravenously as the first-line antiseizure medication. Coagulopathy and thrombocytopenia are monitored and corrected, because hypothermia impairs the coagulation cascade. [4] [10]
In Australia, New Zealand and the United Kingdom, therapeutic hypothermia is the standard of care for term infants (at least 36 weeks) with moderate (Sarnat 2) or severe (Sarnat 3) HIE. Eligibility typically requires a cord or early blood gas pH under 7.0 or a base deficit of at least 12 mmol/L (or an Apgar of 5 or less at 10 minutes, or ongoing resuscitation at 10 minutes), combined with moderate-to-severe encephalopathy. Cooling is initiated within 6 hours of life, maintained at 33.5 to 34.5 °C for 72 hours, and rewarmed at 0.5 °C per hour. Cooling is maintained during neonatal retrieval to a tertiary NICU. [2] [4] [5]
Rewarming is the final stage and a trap for the unwary. The core temperature is raised slowly at 0.5 °C per hour, because rapid rewarming provokes rebound seizures, hypotension, and arrhythmia. The infant is monitored throughout rewarming for these complications. After rewarming, the focus shifts to prognostication (MRI between days 4 and 7) and to planning the structured neurodevelopmental surveillance that every cooled infant enters. [4]
Specific Subtypes & Scenarios
The eligible infant with moderate-to-severe HIE is the central scenario. Once the Sarnat stage and the blood gas meet the criteria, cooling is initiated without delay and maintained for 72 hours with supportive neurocare. The question in this scenario is never whether to cool an eligible infant, but how fast — the 6-hour window closes regardless of seizure control or investigation results. [4]
The infant presenting outside the 6-hour window is a recognised problem. The Laptook 2017 trial (the late-hypothermia study) tested cooling initiated between 6 and 24 hours of life and found no significant reduction in death or moderate-to-severe disability. Cooling beyond 6 hours is therefore not standard, but some clinicians still consider it for individual infants, weighing the equipoise against the lack of an alternative neuroprotective option. This is a scenario examiners probe to test whether candidates know the boundary of the evidence. [8]
[4] [8]The preterm infant (under 36 weeks) is excluded from standard cooling protocols, because the trials enrolled only term and late-preterm infants. The preterm brain's vulnerability is different (the germinal matrix and periventricular white matter rather than the cortex and basal ganglia), and the safety and efficacy of hypothermia in this group are unproven. The late-preterm infant (34 to 36 weeks) is a grey zone managed case by case at tertiary centres, following specialist consultation. [3] [4]
Complications & Pitfalls
The complications of therapeutic hypothermia are predictable and managed proactively. Sinus bradycardia is common and expected at the cooled target temperature, reflecting the direct effect of hypothermia on cardiac conduction; it is benign and is not an indication to rewarm. Thrombocytopenia and coagulopathy occur because hypothermia impairs platelet function and the coagulation cascade, so platelets and clotting factors are monitored and corrected as needed. [4]
Pulmonary hypertension is a recognised complication, screened with pre- and post-ductal oxygen saturations. Subcutaneous fat necrosis, a self-limiting calcinosis, can cause late hypercalcaemia in the weeks after cooling, so serum calcium is checked at follow-up. Skin integrity is monitored throughout cooling because the cold blanket injures cooled skin. Each of these is anticipated, not discovered late. [4] [10]
The neurological complications of HIE itself — cerebral palsy, cognitive impairment, epilepsy, and sensorineural hearing or visual impairment — are concentrated in infants with severe HIE and an abnormal MRI pattern. These are the outcomes cooling reduces, and they are the targets of the structured neurodevelopmental surveillance every cooled infant enters after discharge. [6] [7]
Prognosis & Disposition
Prognosis is determined by the severity of the initial injury, the pattern on MRI, the background recovery on EEG, and whether cooling was given in time. Cooling reduces death and major disability by roughly a quarter; the long-term follow-up of the NICHD trial (Shankaran 2012) confirmed that this benefit persists into childhood, with no increase in disability among survivors. Roughly a quarter to a third of cooled infants with moderate-to-severe HIE still develop cerebral palsy, cognitive impairment, or epilepsy, concentrated in those with a severe (Sarnat 3) presentation and a basal-ganglia–thalamic MRI pattern. [4] [6] [7]
The MRI injury pattern is the strongest imaging prognosticator. A basal ganglia–thalamus–posterior limb pattern, reflecting a profound acute insult, predicts a high risk of cerebral palsy and severe disability. A watershed-zone pattern, reflecting a more prolonged partial insult, predicts a cognitive-predominant outcome with relatively preserved motor function. A normal MRI predicts a favourable outcome. An EEG background that recovers over the first days predicts a better outcome than one that remains suppressed. [7]
Disposition follows severity and the cooling pathway. Any infant undergoing cooling is managed in (or retrieved to) a tertiary NICU with continuous EEG, neurology, and MRI support. After discharge, every cooled infant enters a structured neurodevelopmental surveillance programme, because early detection of cerebral palsy and epilepsy enables early intervention — and because some cognitive sequelae only declare themselves at school age. [6]
Special Populations
The preterm infant (under 36 weeks) is excluded from standard cooling because the trials did not enrol them, the preterm brain's vulnerability is anatomically different, and the safety of hypothermia in this group is unproven. The late-preterm infant (34 to 36 weeks) is managed case by case at tertiary centres. Management of the preterm asphyxiated infant is supportive — normoglycaemia, normoxia, normocapnia, normotension — with seizures treated to an EEG endpoint. [3] [4]
The infant with an HIE mimic — sepsis, metabolic encephalopathy, stroke — is not a candidate for standard cooling, and the priority is to find and treat the cause. Cooling is reserved for infants who meet the HIE criteria; an encephalopathic infant with a normal cord gas and no perinatal asphyxia event warrants a septic and metabolic work-up rather than cooling. [10]
The rural or remote infant raises retrieval considerations. The 6-hour window does not pause for geography, so cooling is initiated at the referring hospital and maintained during neonatal retrieval to a tertiary NICU. Passive cooling with close temperature monitoring, or a transport servo-controlled device, keeps the infant in the target range throughout transfer; the receiving centre continues the protocol. Regional retrieval networks exist specifically to support this. [4] [5]
Evidence, Guidelines & Regional Differences
The evidence base for cooling in HIE is one of the strongest in neonatology. Three landmark randomised trials established the benefit. The CoolCap trial (Gluckman 2005) tested selective head cooling with mild systemic hypothermia and showed a benefit in the moderate-severity subgroup. The NICHD whole-body hypothermia trial (Shankaran 2005) showed a reduction in death and moderate-to-severe disability. The TOBY trial (Azzopardi 2009) confirmed the benefit of whole-body cooling at 33.5 to 34.5 °C for 72 hours. The Jacobs 2013 Cochrane meta-analysis pooled these and confirmed that cooling reduces death and major disability, with no increase in severe disability among survivors. [2] [3] [4] [5]
The boundary of the evidence is the 6-hour window. The Laptook 2017 trial tested cooling initiated between 6 and 24 hours of life and found no significant benefit, so late cooling is not standard. The search for adjuvant neuroprotective therapies has so far been disappointing: the Wu 2022 trial of high-dose erythropoietin added to cooling found it did not improve outcomes and may have harmed, tempering enthusiasm for adjuvant drug therapy. Other candidates (xenon, melatonin, stem cells) remain investigational. Cooling remains the only proven neuroprotective intervention. [8] [9]
Across ANZ, the UK, Europe and North America, therapeutic hypothermia is the standard of care for moderate-to-severe HIE in term infants. The two cooling methods — selective head cooling (CoolCap) and whole-body cooling (TOBY/NICHD) — are both in use; the meta-analysis shows no clear superiority of one over the other, and local protocol governs the choice. The eligibility window (within 6 hours), the target temperature (33.5–34.5 °C), the duration (72 hours), and the rewarming rate (0.5 °C/h) are consistent across regions. [2] [4] [5]
The long-term outcomes were confirmed by the NICHD childhood follow-up (Shankaran 2012), which showed the cooling benefit persists into school age without an increase in disability among survivors. MRI prognostication, based on the injury patterns described by Barkovich and others, is the imaging foundation for counselling families about outcome. [6] [7]
Exam Pearls
Sarnat stages — 'Mild, Moderate, Mortal'
References
- [1]Sarnat HB; Sarnat MS Neonatal encephalopathy following fetal distress. A clinical and electroencephalographic study. Arch Neurol, 1976.PMID 987769
- [2]Gluckman PD; Wyatt JS; Azzopardi D; Ballard R; Edwards AD; Ferriero DM; Polin RA; Robertson CM; Thoresen M; Whitelaw A; Gunn AJ Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: multicentre randomised trial. Lancet, 2005.PMID 15721471
- [3]Shankaran S; Laptook AR; Ehrenkranz RA; Tyson JE; McDonald SA; Donovan EF; Fanaroff AA; Poole WK; Wright LL; Higgins RD; et al Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy. N Engl J Med, 2005.PMID 16221780
- [4]Azzopardi DV; Strohm B; Edwards AD; Dyet L; Halliday HL; Juszczak E; Kapellou O; Levene M; Marlow N; Porter E; et al Moderate hypothermia to treat perinatal asphyxial encephalopathy. N Engl J Med, 2009.PMID 19797281
- [5]Jacobs SE; Berg M; Hunt R; Tarnow-Mordi WO; Inder TE; Davis PG Cooling for newborns with hypoxic ischaemic encephalopathy. Cochrane Database Syst Rev, 2013.PMID 23440789
- [6]Shankaran S; Pappas A; McDonald SA; Vohr BR; Hintz SR; Ehrenkranz RA; Tyson JE; Das A; Hammond J; Perritt R; et al Childhood outcomes after hypothermia for neonatal encephalopathy. N Engl J Med, 2012.PMID 22646631
- [7]Barkovich AJ; Westmark KD; Partridge C; Sola A; Ferriero DM Perinatal asphyxia: MR findings in the first 10 days. AJNR Am J Neuroradiol, 1995.PMID 7793360
- [8]Laptook AR; Shankaran S; Tyson JE; Munoz B; Bell EF; Goldberg RN; Das A; Pappas A; Pedroza C; Heyne RJ; et al Effect of Therapeutic Hypothermia Initiated After 6 Hours of Age on Death or Disability Among Newborns With Hypoxic-Ischemic Encephalopathy: A Randomized Clinical Trial. JAMA, 2017.PMID 29067428
- [9]Wu YW; Mathur AM; Chang T; McKinstry RC; Mulkey SB; Shellhaas RA; Blossom S; Cunningham F; Reber C; Young A; et al Trial of Erythropoietin for Hypoxic-Ischemic Encephalopathy in Newborns. N Engl J Med, 2022.PMID 35830641
- [10]Douglas-Escobar M; Weiss MD Hypoxic-ischemic encephalopathy: a review for the clinician. JAMA Pediatr, 2015.PMID 25685948