Paeds · fetal-neonatal-and-perinatal
Intraventricular haemorrhage and periventricular leukomalacia
Also known as Intraventricular haemorrhage and periventricular leukomalacia · Germinal matrix haemorrhage · Periventricular leukomalacia · Preterm brain injury · White-matter injury of prematurity
Fellowship guide to the two great injuries of the preterm brain: germinal-matrix intraventricular haemorrhage and periventricular leukomalacia — the vascular vulnerability, Papile grading, the white-matter cascade, cranial-ultrasound surveillance, prevention, and family-centred prognostic counselling.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Intraventricular haemorrhage (IVH) and periventricular leukomalacia (PVL) are the two signature brain injuries of the preterm infant, and they share a single anatomical stage: the periventricular region, where the fragile germinal matrix vasculature and the vulnerable premyelinating oligodendrocytes of the white matter lie in close apposition to the lateral ventricles. A haemorrhage from the germinal matrix that breaches the ependyma and enters the ventricular system is an IVH; injury to the periventricular white matter itself — whether from ischaemia, inflammation, or the downstream effect of a large haemorrhage — is PVL. [1] [5]
The two are clinically and prognostically intertwined. A large IVH can infarct the adjacent parenchyma (the grade IV lesion), obstruct cerebrospinal fluid pathways to cause post-haemorrhagic hydrocephalus, and trigger the inflammatory cascade that injures white matter. Conversely, the same haemodynamic instability and infection that cause PVL can also rupture the germinal matrix. For the clinician the practical point is that an IVH and a PVL are often found together on the same cranial ultrasound, and the severity of each independently shapes the prognosis a family must be helped to understand. [5] [10]
Classification
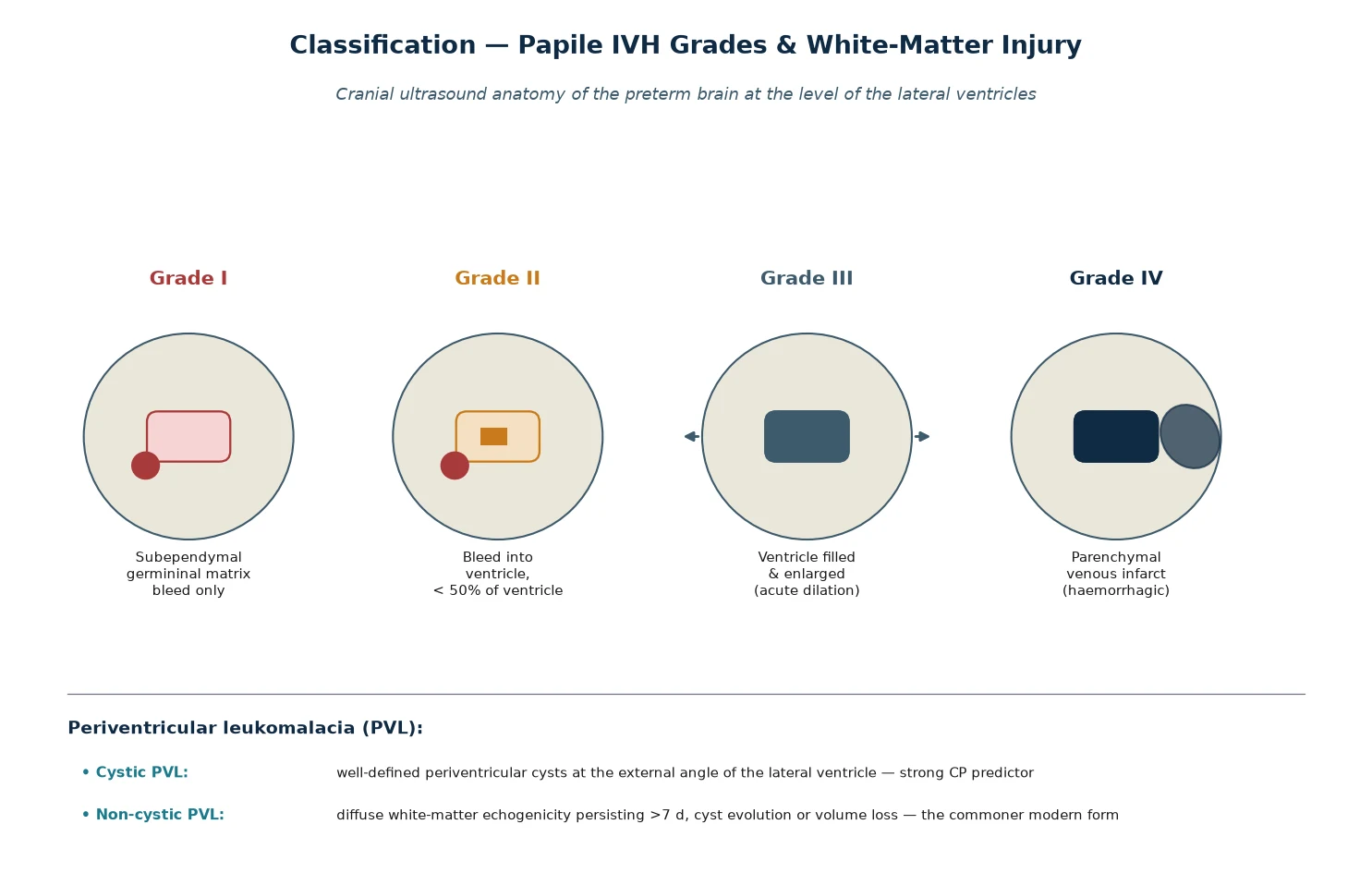
IVH is classified by the Papile system, originally described in 1978 on computed tomography and still the universal cranial-ultrasound grading language. Grade I is a subependymal germinal-matrix haemorrhage confined to the region beneath the ependyma. Grade II is an intraventricular haemorrhage that fills less than half of the ventricular area, without ventriculomegaly. Grade III is an intraventricular haemorrhage that distends and acutely dilates the ventricles. The grade IV lesion is an intraparenchymal haemorrhage — a haemorrhagic infarction of the periventricular white matter adjacent to the ventricle, now understood to be a venous infarction caused by compression of the terminal veins by the distended ventricle rather than simple extension of the bleed. [1]
PVL is classified separately, and the single most important distinction is cystic versus non-cystic. Cystic PVL appears as well-defined cystic lesions in the periventricular white matter, typically at the external angle of the lateral ventricle, evolving over two to three weeks after the insult; it is the strongest ultrasound predictor of subsequent cerebral palsy. Non-cystic (diffuse) white-matter injury — persisting periventricular echogenicity, ventricular enlargement from white-matter volume loss, or thinning of the corpus callosum — is now the commoner pattern detected on modern imaging, and it carries a more variable but still significant neurodevelopmental burden. [5] [9]
Epidemiology & Risk Factors
IVH is overwhelmingly a disease of prematurity. Severe (grade III–IV) IVH occurs in roughly 10 to 15 percent of extremely preterm infants born under 28 weeks or under 1000 g, and the incidence falls steeply with advancing gestational age — it is uncommon after 32 weeks and rare in term infants, in whom an intracranial haemorrhage more often reflects trauma, coagulopathy or a vascular malformation. The single strongest epidemiological predictor is gestational age, followed by birthweight, because both track the maturity of the germinal matrix vasculature and the robustness of cerebral autoregulation. [1] [10]
PVL shares this prematurity gradient but adds an independent infectious dimension. Chorioamnionitis, prolonged rupture of membranes, neonatal sepsis, and a fetal inflammatory response are all associated with white-matter injury, because cytokine-mediated injury to premyelinating oligodendrocytes amplifies the ischaemic damage. The Logan 2013 study of very preterm newborns showed that the antecedents of white-matter damage differ depending on whether an IVH coexists — haemodynamic instability dominates the combined picture, while infection and inflammation dominate isolated PVL. [10]
The modifiable risk factors are the ones prevention targets. Rapid fluctuations in cerebral blood flow — from a pneumothorax, aggressive ventilation, rapid carbon dioxide change, seizures, or a patent ductus arteriosus — stress the pressure-passive cerebral circulation of the preterm infant. Coagulopathy, acidosis, and hypoglycaemia lower the threshold for rupture. Antenatal corticosteroids and delayed cord clamping are the two interventions with the strongest evidence for reducing IVH incidence, because both stabilise the transitional circulation and improve the infant's haemodynamic reserve. [3] [4]
Pathophysiology
The pathophysiology of IVH begins with the germinal matrix, a highly vascular, metabolically active region of proliferating neural and glial precursors that sits in the ganglionic eminence beneath the ependyma of the lateral ventricle. The germinal matrix is largest and most prominent between 24 and 32 weeks' gestation, and it involutes thereafter — which is exactly why IVH is a disease of the very preterm infant. Its vessels are large, thin-walled, immature capillaries with little supportive stroma, and they lie in a region whose autoregulation of cerebral blood flow is poorly developed. [1] [5]
The decisive event is the failure of cerebral autoregulation. In the healthy term brain, cerebral blood flow is held constant across a range of systemic blood pressures. In the very preterm infant this autoregulation is impaired, so the cerebral circulation becomes pressure-passive — systemic blood pressure swings are transmitted directly to the fragile germinal-matrix capillaries. Any event that raises intrathoracic or systemic pressure (a pneumothorax, a vigorous resuscitation, seizures, rapid ventilation), or that swings the partial pressure of carbon dioxide, transmits a surge to the matrix vessels, and a friable capillary ruptures. [5]
Once the matrix bleeds, the clinical course is set by the volume and direction of the haemorrhage. A small bleed confined to the subependymal region is a grade I lesion and usually stays contained. A larger breach carries blood into the ventricle (grade II), and if the volume is great enough the ventricle distends acutely (grade III). The grade IV lesion follows when the distended, clot-filled ventricle compresses the terminal veins: the periventricular white matter congests, infarcts, and becomes haemorrhagic. The clot and the protein-laden cerebrospinal fluid then obstruct the arachnoid villi and the aqueduct, seeding the post-haemorrhagic ventricular dilation that may progress to hydrocephalus over the following days to weeks. [1] [6]
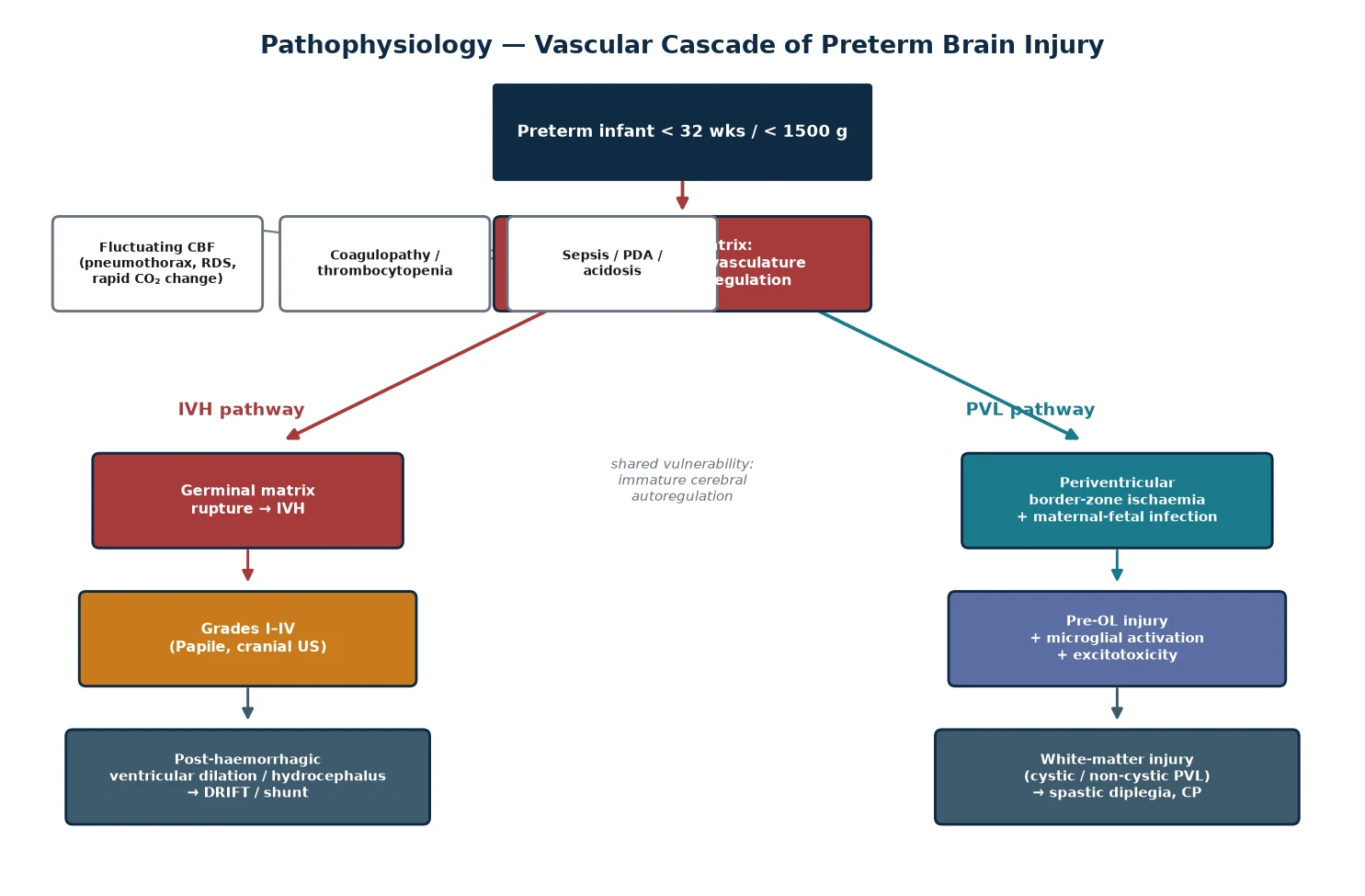
The pathophysiology of PVL runs in parallel and converges. The periventricular white matter lies at the arterial border zone between the long penetrators of the middle cerebral artery and the basifugal vessels, making it the watershed territory most vulnerable to a fall in cerebral perfusion. Its dominant cell during the vulnerable window is the late oligodendrocyte progenitor — the premyelinating oligodendrocyte — which is exquisitely susceptible to oxidative stress, excitotoxicity from glutamate, and cytokine-mediated injury. Hypoxia-ischaemia, maternal or neonatal infection, and the inflammatory spill from a large IVH each injure these cells, producing either focal necrosis (cystic PVL) or diffuse maturational arrest (non-cystic injury). The result is the dysmaturation of white matter that Volpe has framed as the unifying pathology of the preterm brain. [5] [10]
Clinical Presentation
Most intraventricular haemorrhages are clinically silent, and this is the central diagnostic problem. The haemorrhage occurs deep in the ventricle, away from the cortex, and the preterm infant lacks the neurological maturity to produce a focal sign. When symptoms do appear they are nonspecific and reflect the consequences of the bleed — a sudden drop in haemoglobin, a metabolic acidosis, new or worsening apnoea, hypotension, a fall in saturation, or seizures — rather than the bleed itself. [1]
The classic dramatic presentation of a large IVH is a catastrophic decline: a previously stable preterm infant develops a sudden fall in haemoglobin, a bulging anterior fontanelle, a fall in blood pressure, apnoea, metabolic acidosis, seizures, and a reduced level of consciousness over minutes to hours. A grade III–IV haemorrhage with acute ventricular distension can present this way, and it signals that the intracranial pressure has risen and the bleed is large. This presentation mandates an urgent cranial ultrasound and rapid stabilisation of the airway, breathing and circulation. [1]
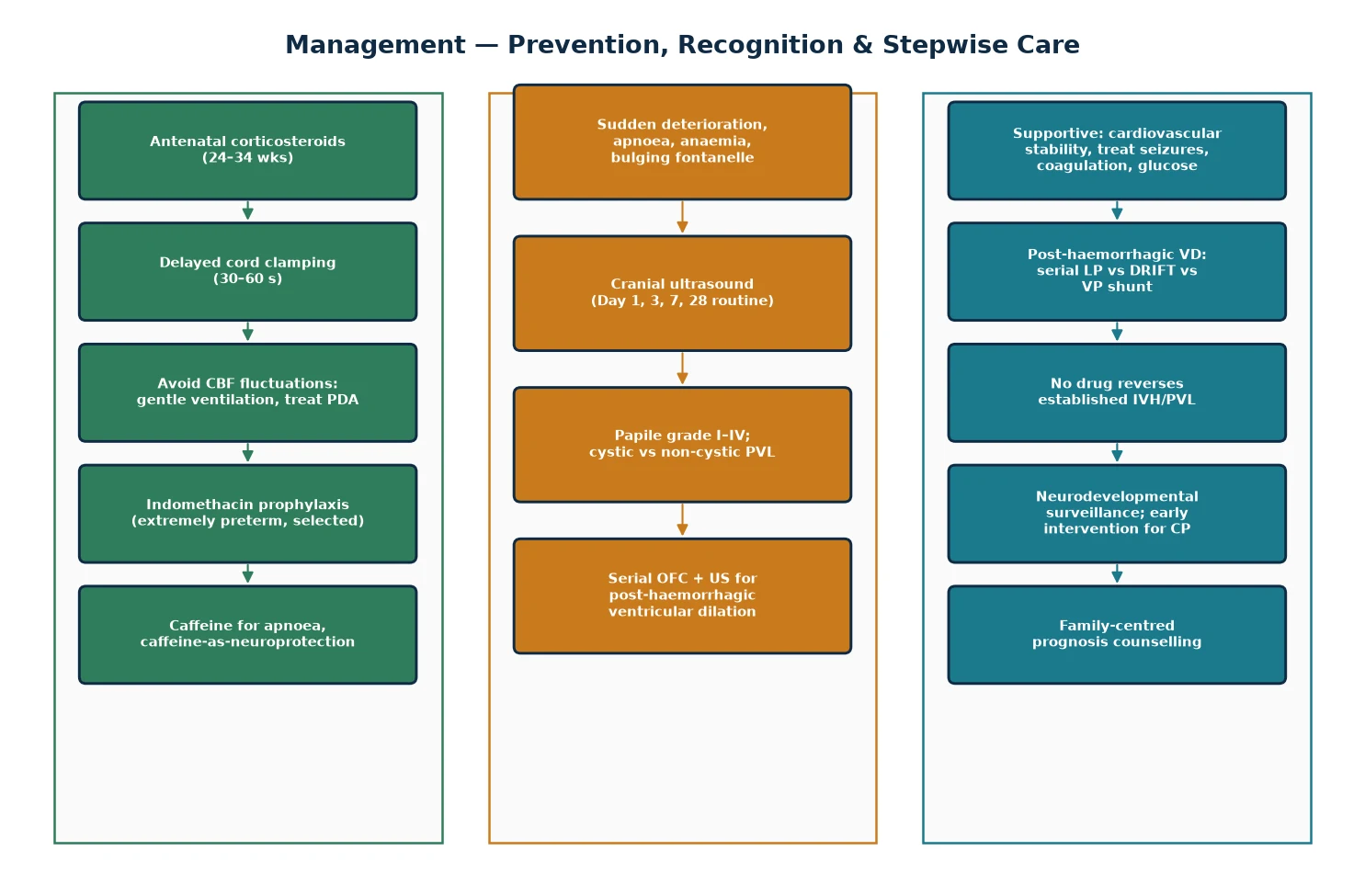
The subtler, commoner presentation is an unexplained drop in haematocrit or a new cluster of apnoeas in an infant in the first three days of life. Because the bleed is often clinically silent, the only reliable strategy is routine cranial-ultrasound surveillance of all very preterm and very-low-birthweight infants — typically on day 1, day 3, day 7, and around day 28 — so that bleeds are detected, graded, and followed regardless of symptoms. [9]
Cerebellar haemorrhage deserves separate mention. The preterm cerebellum is itself rapidly developing and vulnerable, and a cerebellar bleed — sometimes visible only on magnetic resonance imaging — can produce a non-cerebral-palsy phenotype of cognitive, behavioural and social difficulties disproportionate to a normal motor exam. The Volpe 2009 review established the cerebellum as a clinically important and previously under-recognised site of preterm injury. [8]
Differential Diagnosis
When a cranial ultrasound shows an intracranial haemorrhage in a preterm infant, the diagnosis is usually IVH — but the clinician must still consider whether the bleed reflects something other than classic germinal-matrix IVH, and whether the white-matter changes reflect PVL or another process. A choroid plexus bleed, a bleed from a residual area of matrix, or a traumatic subdural or subarachnoid haemorrhage can mimic IVH on ultrasound, and the location and morphology on sequential scans usually distinguish them. [1]
In a term infant, the differential of an intracranial haemorrhage shifts away from germinal-matrix IVH entirely. Birth trauma (subdural haematoma from instrumental delivery), sinovenous thrombosis, an arteriovenous malformation, a bleeding diathesis (vitamin K deficiency bleeding, severe thrombocytopenia, haemophilia), and a hypoxic-ischaemic injury with secondary haemorrhage all enter the differential. The age, the mode of delivery, the coagulation profile, and the magnetic-resonance-imaging pattern resolve most cases. [1]
For periventricular white-matter change, the distinction is between PVL and the artefactual or transient echogenicity that is common in the first week. Normal periventricular echogenicity ('flares') can be prominent in a healthy preterm infant and resolves within a week; persistence, evolution into cysts, or progression to ventricular enlargement and white-matter volume loss confirms true PVL. Magnetic resonance imaging at term-equivalent age is the most sensitive tool for the diffuse, non-cystic white-matter injury that ultrasound underestimates. [5] [9]
Clinical & Bedside Assessment
Bedside assessment combines the clinical suspicion triggered by a deterioration with the structured cranial-ultrasound programme that catches the silent bleeds. When a very preterm infant deteriorates in the first three days of life, the bedside assessment is a rapid ABC stabilisation paired with an urgent cranial ultrasound — the haemoglobin, the acid-base status, the coagulation profile, and the anterior fontanelle are checked at once, and the ultrasound is performed as soon as the infant is stable enough to tolerate the probe. [1]
The anterior fontanelle is the single most useful bedside sign of raised intracranial pressure in a preterm infant. A full or bulging fontanelle, a widening of the cranial sutures, or a rapidly increasing head circumference (more than 1 cm per week beyond the first week, or a sudden acceleration) are the clinical hallmarks of post-haemorrhagic ventricular dilation. Serial head circumference measurement, plotted on a preterm-appropriate chart, is the simplest and most reliable bedside monitor after any IVH, and an accelerating head circumference is the trigger for a repeat ultrasound. [6]
The clinical history captures the modifiable risk factors and shapes the prognostic discussion. The gestational age and birthweight set the baseline risk; the antenatal corticosteroid exposure and the cord-clamping practice set the prevention context; the resuscitation, the occurrence of a pneumothorax, a PDA, sepsis, or rapid carbon-dioxide swings identify the precipitating haemodynamic insult; and the maternal history of chorioamnionitis or prolonged rupture of membranes adds the infectious dimension relevant to PVL. [3] [10]
Investigations
Cranial ultrasound is the primary investigation, and it is both diagnostic and prognostic. It is portable, radiation-free, and repeatable at the bedside through the anterior fontanelle, which makes it ideal for the unstable preterm infant. A haemorrhage appears as an area of increased echogenicity, and the location, the extent of ventricular filling, the presence of ventricular dilation, and any parenchymal extension allow the Papile grade to be assigned. Sequential scans track the evolution of the clot, the development of ventricular dilation, and the appearance or resolution of cystic PVL. [1] [9]
The ventricular index — the distance from the midline to the lateral wall of the anterior horn — is the standard quantitative measure of ventricular size, and serial measurements detect post-haemorrhagic ventricular dilation before it becomes clinically obvious. An increasing ventricular index, an enlarging head circumference, and progressive ventricular asymmetry on sequential scans are the triad that prompts escalation from observation to intervention for hydrocephalus. [6]
Magnetic resonance imaging at term-equivalent age (around 36 to 40 weeks' postmenstrual age) is the most sensitive tool for the diffuse, non-cystic white-matter injury that ultrasound underestimates. It detects reduced white-matter volume, thinning of the corpus callosum, delayed myelination, and cerebellar injury, and it is the strongest single predictor of long-term neurodevelopmental outcome after preterm brain injury. Where available, it is now part of the standard follow-up of extremely preterm infants. [5] [8]
The supporting laboratory work-up is directed at the precipitants and the consequences. A full blood count identifies the anaemia and the thrombocytopenia; a coagulation profile identifies a bleeding diathesis; blood gas and lactate quantify the acidosis and the perfusion; blood cultures exclude sepsis; and the serum glucose and electrolytes are checked because metabolic derangement coexists and worsens prognosis. None of these reverse an established bleed, but each identifies a factor that can be corrected to prevent extension and to stabilise the infant. [1] [3]
Management — Resuscitation
Resuscitation of the preterm infant with a suspected or confirmed large IVH follows the ABCDE framework with two neonatal-specific priorities: gentle, gradual support of the cardiorespiratory transition, and the avoidance of the very fluctuations in cerebral blood flow that caused the bleed. Maintain the airway in a neutral position, oxygenate to the target saturations, ventilate with the gentlest effective settings, and correct hypotension with cautious volume or inotrope rather than aggressive boluses that swing the blood pressure. [1]
The haematological consequences of a large bleed are managed directly. A significant fall in haemoglobin is treated with a packed-red-cell transfusion; thrombocytopenia is corrected with platelets; and a coagulopathy is reversed with fresh frozen plasma or vitamin K as indicated. Seizures are treated with phenobarbital as first-line, because an untreated seizure both raises intracranial pressure and consumes energy in an already-injured brain. The principle is that the resuscitation must itself be haemodynamically gentle — a rough resuscitation can extend the bleed. [1]
Immediate management of suspected large IVH
Assess and stabilise ABC: airway, gentle ventilation, avoid blood-pressure swings
Check haemoglobin, coagulation, platelets, blood gas, glucose, cultures
Transfuse packed red cells for anaemia; correct coagulopathy and thrombocytopenia
Treat seizures with phenobarbital 20 mg/kg IV if present
Urgent cranial ultrasound to confirm and grade the bleed
Begin serial head circumference and ventricular-index monitoring for post-haemorrhagic ventricular dilation
Start the family-centred prognostic conversation, calibrated to the grade
Management — Definitive & Stepwise
Definitive management is layered into prevention, supportive care of the established bleed, and the management of post-haemorrhagic hydrocephalus — because no drug or procedure reverses an established IVH or PVL. The most effective intervention is prevention, and the evidence base for prevention is the strongest part of the whole topic. Antenatal corticosteroids given to the mother before a preterm birth at 24 to 34 weeks reduce IVH incidence by accelerating fetal lung and vascular maturation. Delayed cord clamping, at 30 to 60 seconds, allows a placental transfusion that stabilises the transitional circulation; the Rabe 2019 Cochrane review confirmed that it reduces IVH in preterm infants. [3] [4]
Caffeine citrate, given for apnoea of prematurity, has emerged as an intervention with a neurodevelopmental benefit beyond apnoea control. The Caffeine for Apnea of Prematurity (CAP) trial (Schmidt 2006) showed that caffeine improved survival without neurodevelopmental disability at 18 to 21 months, and long-term follow-up showed lasting cognitive benefit — a finding interpreted as both better ventilation weaning and a possible direct neuroprotective effect relevant to white-matter injury. [3]
Prophylactic indomethacin — a low dose given to extremely preterm infants in the first hours of life — reduces the incidence of severe IVH and of patent ductus arteriosus, by promoting germinal-matrix vessel maturation and ductal closure. The Ment 1994 multicentre trial established this benefit, though long-term follow-up has shown no clear improvement in neurodevelopmental outcome at school age, so practice varies and indomethacin prophylaxis is generally reserved for the most immature infants under local protocol. [2]
[2] [3] [4]The management of post-haemorrhagic ventricular dilation is the main therapeutic challenge after a grade III–IV bleed, because no intervention reliably prevents progression to hydrocephalus. Serial lumbar punctures, ventricular reservoirs, and the drainage-irrigation-fibrinolytic-therapy (DRIFT) technique each have a role, but the evidence is mixed. The original Whitelaw 2007 randomised trial of DRIFT showed a reduction in shunt placement but a higher rate of secondary intracranial bleeding, and the Luyt 2020 ten-year follow-up confirmed a cognitive benefit in survivors but a continued mortality signal. Most infants who progress are managed with a ventriculoperitoneal shunt once the cerebrospinal fluid is clear of heavy blood and protein. [6] [7]
Caffeine citrate
Loading dose
20 mg/kg IV/PO (caffeine citrate)
Maintenance dose
5–10 mg/kg/day
Indomethacin (prophylaxis)
Loading dose
0.1 mg/kg IV once, then 0.1 mg/kg/day for 2 more days
Maintenance dose
— (3-day course)
Specific Subtypes & Scenarios
The grade I–II IVH is the common, lower-risk scenario. A grade I subependymal bleed or a grade II intraventricular bleed usually resolves without sequelae, and the prognosis is close to that of a preterm infant without a bleed, with a small added risk of developmental delay. Management is surveillance — repeat ultrasound to confirm no extension, serial head circumference, and standard preterm follow-up. The family is counselled with cautious reassurance and a clear follow-up plan. [9]
The grade III–IV IVH is the high-risk scenario that dominates the prognostic conversation. A grade III bleed carries a moderate risk of cerebral palsy, cognitive impairment, and post-haemorrhagic hydrocephalus; a grade IV bleed — the parenchymal venous infarct — carries the heaviest burden, with roughly half to two-thirds of affected infants developing cerebral palsy (typically a spastic hemiplegia contralateral to the lesion) and a high rate of cognitive and behavioural difficulties. The O'Shea 2008 study quantified the developmental delay at two years associated with cranial-ultrasound lesions in extremely preterm children. [1] [9]
Post-haemorrhagic ventricular dilation is the scenario where active intervention is weighed against observation. A rising ventricular index and head circumference after a grade III–IV bleed are monitored with twice-weekly ultrasound; intervention is considered when the ventricular index crosses the 97th centile plus 2 to 4 mm, or when there are clinical signs of raised intracranial pressure. The options — serial lumbar puncture, ventricular access device, DRIFT, and ventriculoperitoneal shunt — are chosen on the basis of the rate of progression, the cerebrospinal-fluid protein, and the infant's size and stability. [6] [7]
In Australia, New Zealand and the United Kingdom, post-haemorrhagic ventricular dilation is initially observed with serial ultrasound and head circumference. Intervention thresholds and the choice between serial lumbar puncture, a ventricular access device, and DRIFT vary by centre; DRIFT is used in a small number of specialist centres after the Whitelaw 2007 and Luyt 2020 trials, weighing the cognitive benefit against the bleeding risk. Most infants who progress receive a ventriculoperitoneal shunt once the cerebrospinal fluid clears. Local neurosurgical protocol should guide the sequence. [6] [7]
The scenario of the cerebellar haemorrhage is increasingly recognised with magnetic resonance imaging. A cerebellar bleed in a very preterm infant may produce a non-cerebral-palsy phenotype — cognitive, behavioural, autistic-spectrum and attentional difficulties — disproportionate to a normal early motor exam, and Volpe has emphasised the cerebellum as a clinically important site of preterm injury. These infants require developmental rather than purely motor follow-up. [8]
Complications & Pitfalls
The complications of IVH and PVL are neurological, haematological, and neurosurgical. The neurological complications are the ones that shape prognosis: cerebral palsy (typically a spastic hemiplegia from a grade IV lesion, or a spastic diplegia from cystic PVL), cognitive impairment, sensory impairment (hearing and visual), and post-haemorrhagic hydrocephalus. The haematological complications are the acute anaemia and coagulopathy of the large bleed. The neurosurgical complication is the post-haemorrhagic ventricular dilation that progresses to hydrocephalus and may require a shunt, with the lifelong risks of shunt infection, blockage and revision. [1] [9]
The pitfalls are both diagnostic and prognostic. The diagnostic pitfall is to assume an IVH will declare itself clinically — about half of severe bleeds are silent, so waiting for symptoms misses them. The prognostic pitfall is to over-call or under-call the future from a single early scan: a grade III–IV bleed carries a high risk of cerebral palsy but not certainty, and cystic PVL is a strong predictor but the extent of the cysts and the whole clinical picture modulate the individual prognosis. The counselling pitfall is to deliver a prognosis as a fixed verdict rather than as a calibrated probability that the family can revisit as the infant develops. [6] [9]
Prognosis & Disposition
Prognosis is driven by the grade of the IVH, the presence and extent of cystic PVL, and the occurrence of post-haemorrhagic hydrocephalus. A grade I–II IVH carries a prognosis close to that of an unaffected preterm infant, with a small added risk of developmental delay. A grade III IVH carries a moderate risk of cerebral palsy and cognitive impairment. A grade IV IVH — the parenchymal venous infarct — carries the heaviest burden: roughly half to two-thirds of affected infants develop a spastic hemiplegia contralateral to the lesion, and a high proportion have cognitive and behavioural difficulties. [1] [9]
Cystic PVL is the strongest single predictor of cerebral palsy, with extensive cysts conferring a 50 to 70 percent risk, typically of a spastic diplegia. Non-cystic, diffuse white-matter injury carries a more variable but still significant burden of cognitive and milder motor difficulties, and it is best quantified by magnetic resonance imaging at term-equivalent age. Post-haemorrhagic hydrocephalus, especially if it requires a shunt, adds an independent risk of cognitive impairment on top of the bleed's own prognosis. [5] [9]
Disposition follows the severity. Any preterm infant with a confirmed IVH is managed in a neonatal intensive care unit with cranial-ultrasound capability, and a grade III–IV bleed or post-haemorrhagic ventricular dilation is managed in, or retrieved to, a tertiary centre with neonatal neurology, neurosurgery and magnetic-resonance-imaging support. After discharge, all infants with a grade III–IV IVH, cystic PVL, post-haemorrhagic hydrocephalus, or a concerning term-equivalent-age MRI enter a structured neurodevelopmental surveillance programme — because the early detection of cerebral palsy and cognitive impairment enables early intervention that improves function and quality of life. [9] [10]
Special Populations
The extremely preterm infant (under 28 weeks, under 1000 g) is the highest-risk group, and the one in whom IVH and PVL concentrate. The germinal matrix is at its most prominent, cerebral autoregulation is at its most immature, the premyelinating oligodendrocytes populate the periventricular white matter, and the infant is the most haemodynamically fragile. The prevention bundle — antenatal corticosteroids, delayed cord clamping, gentle ventilation, caffeine, and selected indomethacin prophylaxis — is most decisively applied to this group. [1] [2]
The growth-restricted preterm infant combines the vascular vulnerability of prematurity with the chronic hypoxia and altered placental supply of fetal growth restriction, which independently injures the white matter and lowers the threshold for a haemorrhage. The antenatally diagnosed fetal condition pathway and the maternal disease context — pre-eclampsia, chorioamnionitis, substance exposure — each add layers of risk that the clinician weaves into the prognostic discussion. [10]
The rural or remote preterm infant raises the retrieval dimension. A preterm infant who bleeds in a non-tertiary centre must be retrieved to a tertiary neonatal intensive care unit with ultrasound capability, and the retrieval itself must be haemodynamically gentle — the cerebral blood-flow fluctuations of a rough transport can extend a bleed just as a rough resuscitation can. The regional network should have a protocol for the timing of cranial ultrasound at the receiving centre and for the maintenance of stable perfusion throughout the journey. [4]
Evidence, Guidelines & Regional Differences
The evidence base for IVH and PVL is strongest on prevention and prognosis, and weakest on the treatment of established injury. The prevention evidence rests on three pillars: the established benefit of antenatal corticosteroids for fetal maturation; the Rabe 2019 Cochrane meta-analysis confirming that delayed cord clamping reduces IVH in preterm infants; and the Schmidt 2006 Caffeine for Apnea of Prematurity (CAP) trial, which showed improved survival without neurodevelopmental disability and a lasting cognitive benefit, supporting caffeine as both an apnoea treatment and a probable neuroprotective agent. [3] [4]
The indomethacin evidence is more equivocal. The Ment 1994 multicentre randomised trial established that low-dose indomethacin prophylaxis reduces severe IVH and patent ductus arteriosus in extremely preterm infants, but long-term follow-up showed no clear improvement in neurodevelopmental outcome at school age, so it is reserved for the most immature infants under local protocol rather than applied universally. [2]
The treatment evidence for post-haemorrhagic hydrocephalus is genuinely uncertain. The Whitelaw 2007 randomised trial of DRIFT showed a reduction in shunt placement and a later cognitive benefit, but at the cost of a higher rate of secondary intracranial bleeding and a mortality signal, and the Luyt 2020 ten-year follow-up confirmed the cognitive benefit in survivors. No drug — acetazolamide, furosemide, or any other — reliably prevents the progression of post-haemorrhagic ventricular dilation to hydrocephalus. [6] [7]
The prognostic evidence is mature. The Papile 1978 grading system remains the universal language, and the O'Shea 2008 study quantified the developmental delay at two years associated with cranial-ultrasound lesions in extremely preterm children. The Logan 2013 study refined the understanding of the antecedents of white-matter damage with and without IVH, and Volpe's dysmaturation framework unified the cystic and non-cystic patterns as expressions of a single maturational disturbance. [1] [5] [9] [10]
Across ANZ, the UK, Europe and North America, the standard of care is routine cranial-ultrasound surveillance of all very preterm and very-low-birthweight infants, with the timing (commonly day 1, day 3, day 7, and around day 28) calibrated to the local network and to any clinical deterioration. Magnetic resonance imaging at term-equivalent age is increasingly standard where available, as the most sensitive tool for the diffuse non-cystic white-matter injury that ultrasound underestimates. Prevention bundles — antenatal corticosteroids, delayed cord clamping, gentle ventilation, caffeine, and selected indomethacin — are broadly uniform across high-resource settings, with local variation in the threshold for indomethacin prophylaxis and in the DRIFT-versus-shunt pathway for post-haemorrhagic hydrocephalus. [3] [4] [6]
Exam Pearls
IVH risk and prevention — 'SAFE hands'
References
- [1]Papile LA; Burstein J; Burstein R; Koffler H Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr, 1978.PMID 305471
- [2]Ment LR; Oh W; Ehrenkranz RA; Philip AG; Duncan CC; Makuch RW Low-dose indomethacin and prevention of intraventricular hemorrhage: a multicenter randomized trial. Pediatrics, 1994.PMID 8134206
- [3]Schmidt B; Roberts RS; Davis P; Doyle LW; Barrington KJ; Ohlsson A; Solimano A; Tin W Caffeine therapy for apnea of prematurity. N Engl J Med, 2006.PMID 16707748
- [4]Rabe H; Gyte GM; Díaz-Rossello JL; Duley L Effect of timing of umbilical cord clamping and other strategies to influence placental transfusion at preterm birth on maternal and infant outcomes. Cochrane Database Syst Rev, 2019.PMID 31529790
- [5]Volpe JJ Dysmaturation of Premature Brain: Importance, Cellular Mechanisms, and Potential Interventions. Pediatr Neurol, 2019.PMID 30975474
- [6]Whitelaw A; Evans D; Carter M; Thoresen M; Wrobel C; Odd DE; Cohen N; Brownsdon S; Puntis J; James SR; et al Randomized clinical trial of prevention of hydrocephalus after intraventricular hemorrhage in preterm infants: brain-washing versus tapping fluid. Pediatrics, 2007.PMID 17403819
- [7]Luyt K; Jary SL; Lea CL; Young GR; Hurrion E; Garnett E; Smallman LA; Steventon V; Hollands L; Cowan FM; et al Drainage, irrigation and fibrinolytic therapy (DRIFT) for posthaemorrhagic ventricular dilatation: 10-year follow-up of a randomised controlled trial. Arch Dis Child Fetal Neonatal Ed, 2020.PMID 32623370
- [8]Volpe JJ Cerebellum of the premature infant: rapidly developing, vulnerable, clinically important. J Child Neurol, 2009.PMID 19745085
- [9]O'Shea TM; Kuban KC; Allred EN; Paneth N; Hirtz D; Fichorova RN; Heeren T; Leviton A Neonatal cranial ultrasound lesions and developmental delays at 2 years of age among extremely low gestational age children. Pediatrics, 2008.PMID 18762501
- [10]Logan JW; Westra SJ; Allred EN; Bose C; Leviton A; Kuban KC; O'Shea TM; Paneth N; ELGAN Study Group Antecedents of perinatal cerebral white matter damage with and without intraventricular hemorrhage in very preterm newborns. Pediatr Neurol, 2013.PMID 23859853