Paeds · fetal-neonatal-and-perinatal
Large-for-gestational-age infant and infants of diabetic mothers
Also known as Large for gestational age (LGA) · Macrosomia · Infant of a diabetic mother (IDM) · Fetal hyperinsulinaemia · Neonatal hypoglycaemia of the IDM
Fellowship guide to the large-for-gestational-age infant and the infant of a diabetic mother: the Pedersen hypothesis, macrosomia, and the stepwise neonatal management of hypoglycaemia, polycythaemia, respiratory distress, cardiomyopathy, metabolic disturbance and birth injury.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a term baby weighing 4350 g — well above the 90th centile — born to a mother whose gestational diabetes was picked up late. The midwife calls the baby "macrosomic". Before you reach for a glucometer or a cot in special care, hold two ideas separate in your mind: how big the baby is, and why it is that big. [9]
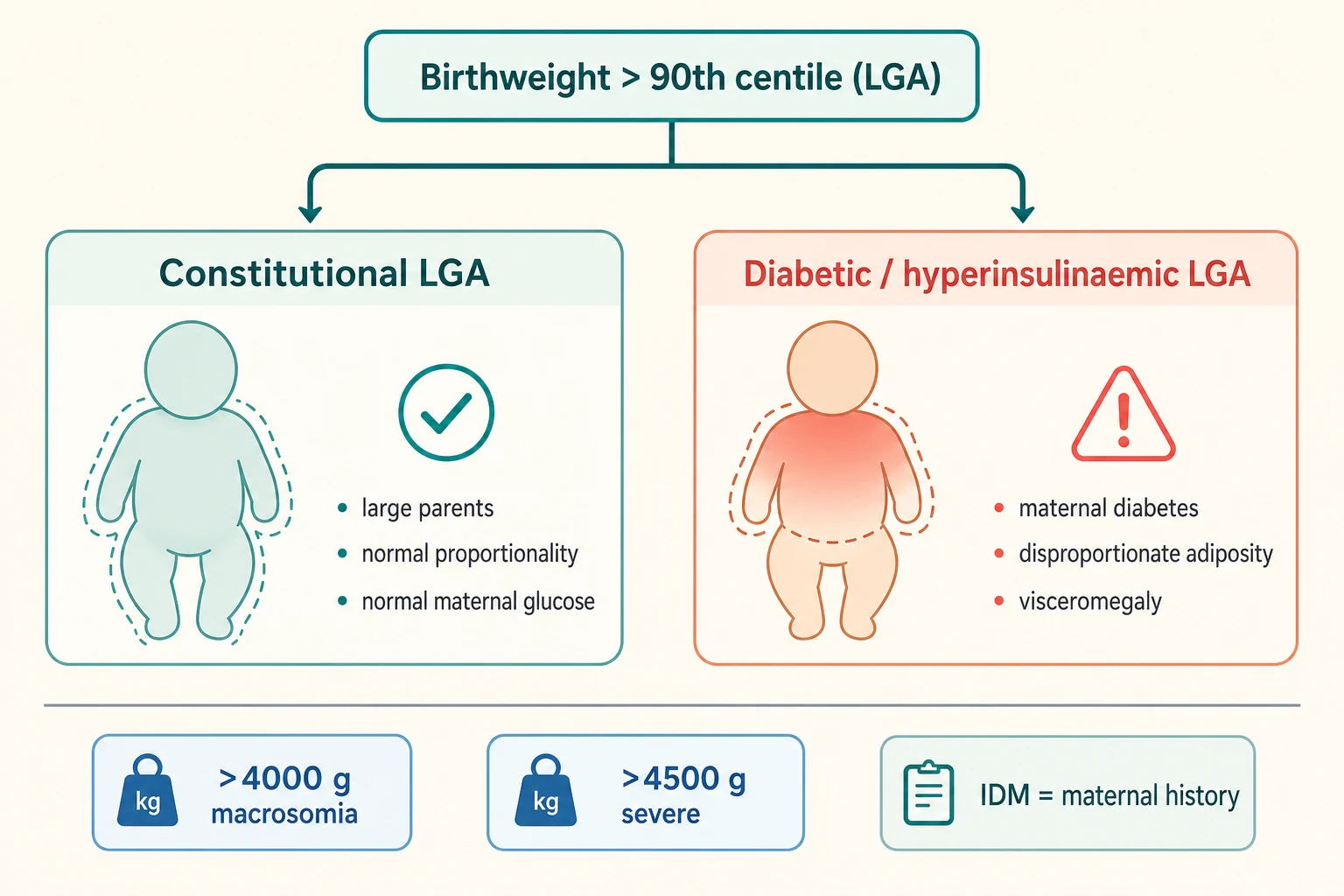
Large for gestational age (LGA) is a size label. It means the birthweight is above the 90th centile for gestational age and sex on a standard chart. [9] Macrosomia is an absolute-weight label — most commonly above 4000 g, with many guidelines treating above 4500 g as severe or probable macrosomia. [9] Neither word tells you why the baby is large. Most LGA babies are simply constitutionally big — large parents, a post-term pregnancy, or a boy. Diabetes accounts for only a minority of all macrosomic births. [10]
Infant of a diabetic mother (IDM) is a history label. It describes any newborn whose mother had pregestational (type 1 or type 2) or gestational diabetes mellitus, whether or not the baby is large. [8] The two labels overlap heavily when diabetes is poorly controlled, because maternal hyperglycaemia drives the fetus to grow — but a well-controlled diabetic pregnancy can produce a normally grown infant, and a non-diabetic pregnancy can produce a large one.
So the examiner's first question is always: is this large baby large because of diabetes, or for some other reason? That distinction sets the whole neonatal plan, because only the hyperinsulinaemic IDM carries the predictable cascade of metabolic, haematological, respiratory and cardiac complications. [8]
Classification
Begin with the size, then probe the cause. [9]
By size, plot weight, length and head circumference on a gestation- and sex-specific international chart (INTERGROWTH-21st). LGA is above the 90th centile. Macrosomia is conventionally above 4000 g, with above 4500 g marking the range where birth-injury and operative-delivery risk rise sharply. [9] A unisex or adult chart misclassifies large babies just as it misclassifies small ones — always use the gestation-specific standard.
By proportion, separate constitutional from hyperinsulinaemic overgrowth. The constitutionally large infant is simply a scaled-up version of a well-grown baby — proportionate, muscular, not particularly plethoric. The diabetic LGA infant carries its excess weight as disproportionate truncal and shoulder adiposity with visceromegaly (a palpable liver), because insulin lays down fat and glycogen preferentially. [8] That body habitus is the physical clue that you are dealing with hyperinsulinaemia, not genes.
By maternal diabetes type, separate pregestational from gestational diabetes. Pregestational disease (type 1 or type 2) adds first-trimester malformation risk and, with vascular disease, a paradoxical risk of growth restriction or preterm birth. Gestational diabetes — by far the commonest — carries lower malformation risk but the full late-pregnancy macrosomia and neonatal-complication profile when poorly controlled. [11]
Epidemiology & Risk Factors
Roughly 9–10% of live births are LGA by definition; absolute macrosomia above 4000 g affects around 5–10%, with wide regional variation driven by maternal obesity and diabetes prevalence. [10] Maternal diabetes is the strongest modifiable driver of pathological overgrowth, but it explains only a minority of all macrosomic births — most large babies are constitutionally big. [10]
Non-diabetic risk factors cluster around constitutional growth: large parents, multiparity, advanced maternal age, high body mass index, excessive gestational weight gain, a post-term pregnancy, male sex, and a prior macrosomic infant. [9] Among diabetic pregnancies, the risk modifiers are the ones that matter most for the neonatal team: poor third-trimester glycaemic control, a high glycated haemoglobin (HbA1c), untreated gestational diabetes, and pregestational disease with vascular involvement. [8]
The foundational evidence here is the HAPO study, which followed more than 25,000 pregnancies and showed a smooth, continuous dose-response between maternal glucose (even below the traditional diabetes threshold) and the risk of birthweight above the 90th centile, neonatal hypoglycaemia and other adverse outcomes. [1] There was no obvious threshold where risk began — risk rose steadily with glucose — which is exactly why the IADPSG committee derived the current diagnostic cut-offs from outcome data rather than from an arbitrary sugar level. [2]
Social determinants amplify the whole picture. Obesity, food insecurity and reduced antenatal access raise the incidence of gestational diabetes and worsen glycaemic control, so the large IDM is over-represented among socioeconomically disadvantaged families and in communities with high diabetes prevalence. [7]
Pathophysiology
To understand the big, hypoglycaemic baby, follow the glucose. The story is the Pedersen hypothesis, and it explains almost every IDM complication in one causal chain. [7]
Glucose crosses the placenta freely, but maternal insulin does not. So when the mother runs high blood sugars, the fetus is bathed in glucose and responds the only way it can: its pancreas pours out insulin. In fetal life, insulin is not just a glucose regulator — it is the dominant growth hormone. The hyperinsulinaemic fetus lays down fat, glycogen and muscle at an accelerated rate, storing the excess energy as the disproportionate truncal and shoulder adiposity and visceromegaly you see at birth. [7] [8]
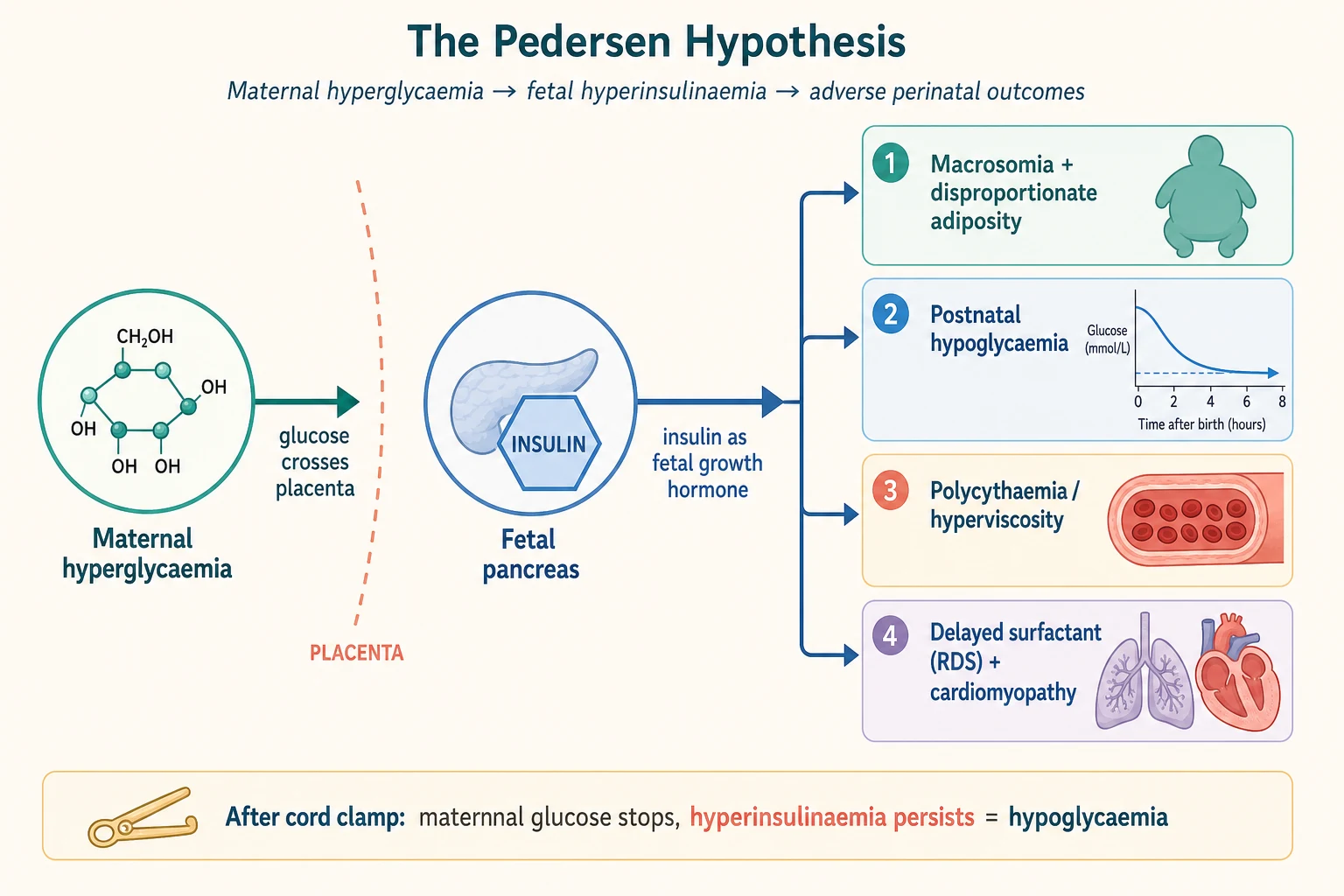
The same chain sets up the neonatal complications, and each is worth tracing. When the cord is clamped, the maternal glucose supply stops abruptly — but fetal insulin secretion does not. The hyperinsulinaemic newborn continues to drive glucose into cells, so blood sugar falls: this is neonatal hypoglycaemia, the commonest and most important IDM complication, peaking in the first hours of life. [3] Chronic fetal hyperinsulinaemia and a relatively hypoxic intrauterine environment stimulate erythropoietin release, so the IDM arrives polycythaemic; a high haematocrit then causes hyperviscosity, sluggish flow and the organ dysfunction that follows. [12]
Fetal hyperinsulinaemia also antagonises surfactant maturation, so the lungs of the IDM lag behind their gestational age. Even at term, an IDM can develop respiratory distress syndrome — a fact that surprises candidates who assume RDS is a disease of prematurity alone. [8] The heart is affected too: insulin drives myocardial hyperplasia and hypertrophy, producing an asymmetric septal hypertrophic cardiomyopathy that may cause outflow obstruction or heart failure in the first days. [8] Finally, disordered parathyroid and magnesium handling lower serum calcium and magnesium in the first 48 hours, producing hypocalcaemia and hypomagnesaemia that can contribute to jitteriness and, rarely, seizures. [8]
In pregestational diabetes there is one more, earlier chapter. First-trimester hyperglycaemia and oxidative stress, before the pancreas and placenta take over, disrupt organogenesis — raising the rate of neural tube defects, cardiac defects and the rare but classic caudal regression sequence. [11] This is why pregestational diabetes carries a malformation risk that good later-pregnancy control cannot undo, and why preconception optimisation matters so much.
Clinical Presentation
The large or hyperinsulinaemic neonate looks the part. The IDM is plump, heavy and often plethoric (ruddy), carrying excess weight as soft truncal and shoulder fat with a palpable liver from glycogen storage. The constitutionally large infant, by contrast, is a proportionate, muscular, well-grown version of a normal baby without the diabetic body habitus. [8]
What you will see in the first hours are the complications, not the cause. Hypoglycaemia is the headline: the baby may be asymptomatic, or may show the classic neuroglycopenic and adrenergic signs — jitteriness and tremors, irritability, hypotonia, poor feeding, an abnormal or high-pitched cry, apnoea, cyanosis, and in the worst case seizures. [3] Because these signs are non-specific, a glucose check is mandatory in any IDM or unexplained large infant with any of them.
Polycythaemia and hyperviscosity declare themselves as plethoric skin, lethargy, poor feeding, tachypnoea, and — in the severest cases — thrombosis (renal vein thrombosis presenting with haematuria, or a NEC-like picture of feeding intolerance). [12] Respiratory distress in the term IDM has a broad differential that includes RDS, transient tachypnoea of the newborn, and cardiomyopathy-related heart failure — grunting, recessions and an oxygen requirement in a term baby should make you think of all three. [8]
Look deliberately for birth injury, because a macrosomic delivery is a difficult delivery. Palpate the clavicles for a fracture, assess the brachial plexus (an asymmetric Moro reflex, a limp arm held internally rotated — Erb's palsy), check facial nerve function, and distinguish a cephalhaematoma from a caput or a dangerous subgaleal haemorrhage. [9] Finally, in pregestational diabetes, examine for congenital malformation: a cardiac murmur, absent or weak femoral pulses, or a structural anomaly. [11]
The well constitutional LGA infant is simply a big, alert, feeding baby with none of these — and recognising that distinction at the bedside spares the family unnecessary monitoring and separation. [9]
Differential Diagnosis
The differential turns on one question: is the overgrowth constitutional, hyperinsulinaemic (diabetic), or syndromic? [8]
The constitutionally large infant has large parents, a normal antenatal growth trajectory, normal maternal glucose tolerance, normal proportionality, and is well at birth. This baby needs only routine care with a single confirming glucose check if there is any doubt. [9]
The infant of a diabetic mother has the disproportionate adiposity and visceromegaly of hyperinsulinaemia, a known diabetic pregnancy, and the predictable complication profile. Within the IDM group, separate gestational from pregestational diabetes: the latter adds malformation and vascular-placental risk. [11]
A short list of overgrowth syndromes can masquerade as an IDM and must not be missed. Beckwith-Wiedemann syndrome is the classic mimic — macrosomia with macroglossia, an omphalocele or umbilical hernia, hemihypertrophy, ear creases and neonatal hypoglycaemia from hyperinsulinaemia; it needs a genetics referral, hypoglycaemia workup and lifelong tumour surveillance. [8] Sotos syndrome (cerebral gigantism) and congenital hyperinsulinism (persistent, severe, genetically driven hypoglycaemia unrelated to maternal diabetes) are the other two to name.
When the presenting problem is hypoglycaemia rather than size, broaden the differential to inborn errors of metabolism, neonatal sepsis and perinatal asphyxia — but in an IDM the cause is obvious, and the question is severity and persistence rather than identity. [3]
Clinical & Bedside Assessment
Begin with a focused antenatal history that frames the whole neonatal plan. Establish the maternal diabetes type (gestational, type 1, type 2), the glycaemic control through pregnancy (HbA1c trend, insulin or metformin use), the third-trimester growth scans and estimated fetal weight, whether there was polyhydramnios (a marker of fetal polyuria from hyperglycaemia), whether antenatal steroids were given, the intrapartum glucose control, and the mode and indication for delivery. [8] A baby delivered by caesarean for suspected macrosomia of a poorly controlled diabetic is a very different patient from a spontaneous vaginal delivery of a constitutionally large infant.
Accurate anthropometry is the single most important bedside act. Weigh the baby, measure length and head circumference, and plot everything on a gestation- and sex-specific INTERGROWTH-21st chart to confirm LGA and assess proportionality. The pattern of overgrowth — proportionate versus the disproportionate truncal adiposity and hepatomegaly of hyperinsulinaemia — is the physical evidence that distinguishes constitutional from diabetic causes. [9]
Then examine systematically for the complications. Look at the skin colour (plethora of polycythaemia), palpate the clavicles and assess the brachial plexus and facial nerve for birth injury, listen to the heart and lungs (a murmur, gallop or tachypnoea pointing to cardiomyopathy or RDS), feel the abdomen for hepatomegaly, and screen for congenital malformation — especially cardiac, with attention to femoral pulses. [8]
Assess function in the first hours: tone, colour, perfusion, temperature, respiratory effort and feeding. The jittery, tachypnoeic or poorly feeding IDM declares itself early if you look, and those are the findings that move a baby from mother's room to a higher level of care. [3]
Finally, synthesise a one-line summary. A good example: "A 39-week male, birthweight 4400 g (>97th centile), disproportionate truncal adiposity and hepatomegaly, born to a mother with poorly controlled gestational diabetes, now jittery with a low pre-feed glucose — IDM with early symptomatic hypoglycaemia." That sentence carries the category, the severity and the first move. [8]
Investigations
LGA is a diagnosis you make with a tape measure and a chart, not a battery of tests. Over-investigating the well constitutional LGA infant causes harm, anxiety and unnecessary admission. [9]
The cornerstone neonatal investigation for the IDM is scheduled pre-feed bedside glucose monitoring. Begin within the first one to two hours of life and repeat before feeds through the first 24 hours, because the IDM's insulin peaks over that window and a single normal reading does not clear the baby. [3] The treatment threshold commonly cited is a blood glucose below 2.6 mmol/L in the first 48 hours (with clinical correlation), though local policies vary and some use 2.0 mmol/L; treat the infant and the trend, not the number alone. [3]
Tailor the remaining tests to the baby in front of you. Check a venous haematocrit for polycythaemia in any plethoric, lethargic or poorly feeding IDM (capillary samples overestimate haematocrit). Send a serum calcium and magnesium if the baby is jittery with a normal or treated glucose. Check a bilirubin as jaundice develops (polycythaemia raises the haemoglobin load and the IDM is at increased hyperbilirubinaemia risk). If there is respiratory distress, a blood gas, chest X-ray and pre- and post-ductal saturations distinguish RDS, transient tachypnoea and cyanotic congenital heart disease. [8] When cardiomyopathy is suspected, an echocardiogram confirms the asymmetric septal hypertrophy and outflow obstruction.
Know what to avoid. Do not take routine arterial samples when capillary or venous sampling answers the question. Do not admit and panel-investigate a well, proportionate, feeding large baby of a non-diabetic mother just because of a centile. And do not let one reassuring glucose reading close the surveillance window on an IDM. [3]
The IDM complications to expect and pre-empt
Management — Resuscitation
Most LGA and IDM infants do not need resuscitation beyond routine newborn care — the danger is assuming that is always true. A macrosomic infant delivered after shoulder dystocia, or an IDM with perinatal depression, can present with a low Apgar and need the full neonatal resuscitation algorithm (covered in the dedicated resuscitation topic). [8]
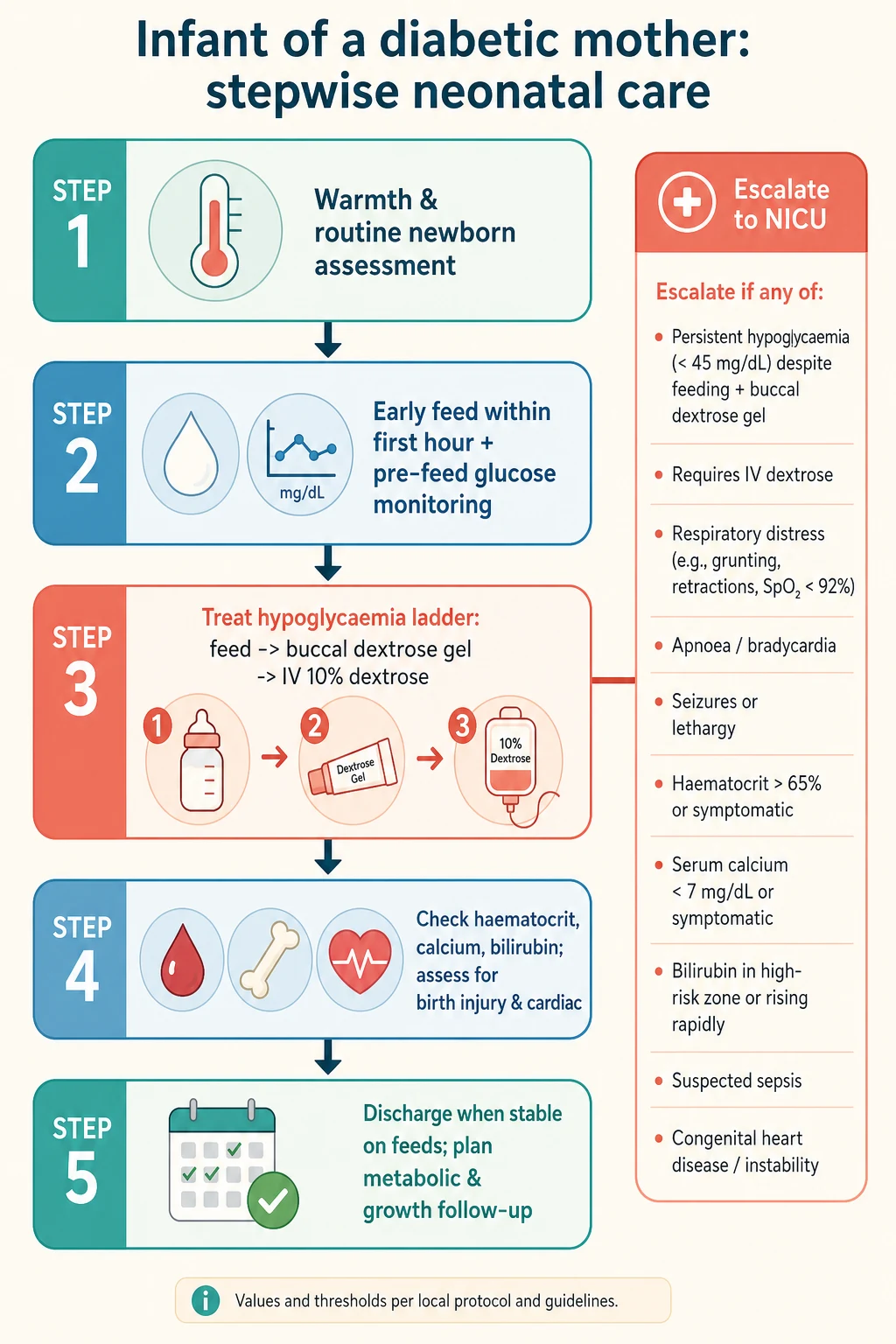
The two resuscitation priorities specific to the IDM are warmth and glucose. Dry and warm the baby, aim for normothermia and early skin-to-skin when stable, and — critically — feed within the first hour to protect against the post-cord-clamp glucose fall. Check a pre-feed glucose and treat hypoglycaemia promptly. [3]
Escalate to a higher level of care when any of these is present: symptomatic or persistent hypoglycaemia despite feeding and buccal dextrose gel, respiratory distress, polycythaemia needing intervention, suspected cardiomyopathy, significant birth injury, or the need for intravenous fluids. A well, term, constitutionally large infant feeding well and thermally stable stays with mother with a single confirming glucose check. [3]
Management — Definitive & Stepwise
Once stable, definitive care is a sequence you can rehearse: warm, feed, monitor, treat the complications, support feeding, and follow up. [3]
- Thermoregulation. Maintain normothermia from birth — dry, warm, hat, and skin-to-skin when stable. Hypothermia worsens hypoglycaemia and acidosis. [8]
- Early and frequent feeding. Establish breastfeeding within the first hour, then feed at least every 2–3 hours. Breast milk is first-line; the aim is a steady exogenous glucose supply to counter the persistent hyperinsulinaemia. [3]
- Scheduled glucose monitoring and the hypoglycaemia ladder. Check pre-feed glucose on a schedule through the first day. If it is low, step up the ladder: first feed, then buccal 40% dextrose gel at 200 mg/kg with a feed and a recheck, then an intravenous 10% dextrose bolus (2 mL/kg) and an escalating dextrose infusion for persistent hypoglycaemia, with glucagon or hydrocortisone reserved for refractory cases. [5] [6] The Sugar Babies trial established buccal dextrose gel as an effective first-line treatment that reduces separation and intravenous therapy, and the Cochrane review confirmed its prophylactic and treatment role. [5] [6]
- Polycythaemia and hyperviscosity. A symptomatic IDM with a venous haematocrit above the local threshold may warrant a partial exchange transfusion; asymptomatic infants are managed with hydration and monitoring. Treat the infant, not the number. [12]
- Hypocalcaemia and hypomagnesaemia. Supplement when symptomatic or below threshold, correcting magnesium first if both are low (calcium will not correct until magnesium does). [8]
- Respiratory and cardiac support. Give oxygen and CPAP for RDS or transient tachypnoea, and surfactant for established RDS. For hypertrophic cardiomyopathy, seek cardiology input and treat supportively — avoid inotropes that increase contractility and worsen dynamic outflow obstruction; fluid restriction and time usually allow the hypertrophy to regress. [8]
- Birth injury. Document and follow up clavicular fracture, brachial plexus and facial nerve injury; most recover, but a persistent palsy needs physiotherapy and specialist review. [9]
Plan discharge once the baby is thermally stable, glucose-stable on full enteral feeds without treatment, feeding competently, gaining weight, free of respiratory compromise, with birth injuries documented and confident parents. [3]
Plan long-term follow-up from discharge. Monitor growth, offer neurodevelopmental surveillance after severe or recurrent hypoglycaemia, and — uniquely for the IDM — educate the family about the increased childhood obesity, impaired glucose tolerance and type 2 diabetes risk, framing it as a reason for healthy lifestyle and ongoing primary-care surveillance rather than a foregone conclusion. [11]
Specific Subtypes & Scenarios
Well constitutional LGA (non-diabetic). The healthy large infant of large parents. Confirm feeding and normoglycaemia with a single check if any doubt, provide breastfeeding support, and reassure — this baby needs no admission. [9]
IDM with good antepartum glycaemic control. Lower complication rates because the hyperinsulinaemic drive was blunted, but still warrants scheduled glucose monitoring and a low threshold for the IDM complication set. [8]
IDM with poor glycaemic control. The highest-risk profile — macrosomia, early hypoglycaemia, RDS, polycythaemia, cardiomyopathy, and (if pregestational) malformation. Plan NICU proximity and a full surveillance and treatment plan from birth. [8]
Pregestational diabetes (type 1 or type 2). Added malformation and vascular-placental risk. A paradox to hold in mind: pregestational diabetes with vascular disease can produce a growth-restricted or preterm infant rather than a macrosomic one, because placental insufficiency overrides the insulin-driven growth signal. [11]
Macrosomia with shoulder dystocia. Assess the brachial plexus and clavicles, document thoroughly, and arrange early physiotherapy follow-up for any palsy. [9]
Hypertrophic cardiomyopathy in the IDM. May present with a murmur, gallop, tachypnoea or heart failure in the first days. Confirm with echocardiography, restrict fluids, avoid inotropes, and allow time for regression — most resolve over weeks to months. [8]
Beckwith-Wiedemann syndrome masquerading as IDM. Macrosomia with macroglossia, omphalocele, hemihypertrophy and neonatal hypoglycaemia. This is not an IDM — it needs a genetics referral, a persistent-hypoglycaemia workup, and lifelong tumour surveillance. [8]
Complications & Pitfalls
Short-term, expect hypoglycaemia, polycythaemia and hyperviscosity, respiratory distress (RDS and transient tachypnoea), hypocalcaemia and hypomagnesaemia, hyperbilirubinaemia, hypertrophic cardiomyopathy, birth injury, feeding difficulty and NEC risk. [8] Long-term, expect (in a subset) childhood obesity, impaired glucose tolerance and increased type 2 diabetes risk, and potential neurodevelopmental sequelae from severe or recurrent neonatal hypoglycaemia. [11]
The pitfalls are predictable, and worth naming so you avoid them. A single normal glucose reading falsely reassuring you — the IDM's insulin peaks over the first day, so a normal early reading can be followed by a low one; schedule repeated pre-feed checks. [3] Missing symptomatic hypoglycaemia because jitteriness and poor feeding are non-specific — in an IDM, check the glucose. Treating the number rather than the infant — an asymptomatic IDM just below threshold who feeds and rechecks upward is different from a seizing one. [3] Forgetting to examine for birth injury after a difficult macrosomic delivery — a clavicle or brachial plexus injury is easily missed if you do not look. [9] Giving an inotrope to an IDM in heart failure — in hypertrophic cardiomyopathy that worsens the outflow obstruction; treat supportively instead. [8] And missing an overgrowth syndrome by assuming every large, hypoglycaemic baby is an IDM, when Beckwith-Wiedemann carries its own hypoglycaemia and tumour-surveillance implications. [8]
Prognosis & Disposition
Outcome is driven by maternal glycaemic control, gestation, the severity of complications and the promptness of neonatal management — not by size alone. A well constitutional LGA infant has a normal outlook. An IDM of a well-controlled diabetic pregnancy has near-normal short-term outcomes. The risk concentrates in the poorly controlled IDM and the preterm or growth-restricted pregestational infant. [8]
The evidence that makes surveillance worthwhile is the McKinlay work on neonatal glycaemia: severe or recurrent hypoglycaemia is associated with adverse neurodevelopment at 2 and 4.5 years, which is exactly why pre-empting hypoglycaemia from the first feed is not over-cautious but evidence-based. [3] [4] The longer view is metabolic programming: offspring of diabetic pregnancies carry an increased risk of childhood obesity, impaired glucose tolerance and type 2 diabetes — a risk the family should know about and that primary care should monitor. [11]
Disposition follows the risk. A well term LGA or IDM feeding and normoglycaemic stays with mother with scheduled glucose checks. A moderate-risk IDM needing glucose support or respiratory observation goes to transitional care. A severe, symptomatic or preterm IDM — persistent hypoglycaemia, RDS, polycythaemia needing exchange, cardiomyopathy, or significant birth injury — goes to NICU, often with the neonatal team present at delivery. [3]
Special Populations
Pregestational diabetes with vascular disease is the paradox every candidate must hold: the same disease that drives macrosomia can, through placental insufficiency, produce a growth-restricted or preterm infant. Adjust expectations and plan for both possibilities. [11]
Late-preterm IDM (34–36+6 weeks) compounds prematurity and diabetes — RDS, hypoglycaemia and feeding difficulty all stack, lowering the threshold for NICU admission. [8]
Indigenous and socioeconomically disadvantaged families carry a higher burden of gestational diabetes, obesity and access barriers. Provide culturally safe antenatal and postnatal care, address nutrition and lifestyle directly, and ensure the metabolic-surveillance and follow-up loop does not drop. [7]
Rural and remote settings must plan antenatal transfer to a service with neonatal capability before the delivery of a known macrosomic or IDM pregnancy; a hypoglycaemic macrosomic infant born away from support is an avoidable crisis. [8]
Beckwith-Wiedemann and overgrowth syndromes need a parallel genetics, hypoglycaemia-workup and tumour-surveillance pathway — they are not managed as routine IDM. [8]
Out-of-home-care and migrant-refugee infants need deliberate continuity — confirm growth monitoring, glycaemic follow-up and metabolic surveillance are transferred, not lost, across moves. [7]
Evidence, Guidelines & Regional Differences
The foundational evidence is the HAPO study (Metzger 2008), which established the continuous dose-response between maternal glucose and adverse outcomes including birthweight above the 90th centile and neonatal hypoglycaemia — with no clear threshold, justifying the modern outcome-derived diagnostic approach. [1] The IADPSG consensus (Metzger 2010) translated that dose-response into the diagnostic cut-offs for gestational diabetes adopted by the WHO, ADIPS and many national bodies. [2]
For neonatal hypoglycaemia, the Sugar Babies trial (Harris 2013) established buccal 40% dextrose gel as effective first-line treatment, [5] and the Cochrane review (Edwards 2021) confirmed its role in prophylaxis and treatment of at-risk neonates. [6] The glycaemic thresholds and their neurodevelopmental meaning come from the McKinlay studies at 2 years and 4.5 years. [3] [4] The IDM complication profile and Pedersen pathophysiology are summarised in the gestational diabetes primer (McIntyre 2019) and the IDM review (Kallem 2020). [7] [8]
Two live controversies: the threshold for prophylactic caesarean by estimated fetal weight (ACOG discusses a cut-off around 4500 g in diabetic pregnancies, with regional variation), and the balance between elective early delivery and expectant management for suspected macrosomia — neither is resolved, and both trade operative and birth-injury risk against prematurity risk. [9]
Exam Pearls
- LGA is a centile word (>90th); macrosomia is a weight word (>4000 g); IDM is a maternal-history word. Answer the question the stem asks. [9]
- The Pedersen hypothesis in one chain: maternal glucose → fetal insulin → insulin is the fetal growth hormone → macrosomia, and after cord clamp → hypoglycaemia. [7]
- The five IDM complications to expect and pre-empt: hypoglycaemia, polycythaemia/hyperviscosity, respiratory distress, hypocalcaemia/hypomagnesaemia, and (in pregestational) malformation. [8]
- Respiratory distress in the term IDM is often RDS — hyperinsulinaemia delays surfactant maturation independent of gestation. [8]
- For hypertrophic cardiomyopathy in the IDM, do NOT give inotropes — they worsen dynamic outflow obstruction. Treat supportively. [8]
- Caudal regression is the classic but rare diabetic embryopathy; neural tube and cardiac defects are commoner. [11]
- A single normal glucose does not clear the IDM — schedule repeated pre-feed checks over the first day. [3]
- Plot every large infant on a gestation- and sex-specific chart; adult or unisex charts misclassify. [9]
- Beckwith-Wiedemann mimics IDM — macrosomia with macroglossia, omphalocele, hemihypertrophy and hypoglycaemia — and needs genetics and tumour surveillance. [8]
References
- [1]Metzger BE Hyperglycemia and adverse pregnancy outcomes. New England Journal of Medicine, 2008.PMID 18463375
- [2]Metzger BE International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care, 2010.PMID 20190296
- [3]McKinlay CJ Neonatal glycemia and neurodevelopmental outcomes at 2 years. New England Journal of Medicine, 2015.PMID 26465984
- [4]McKinlay CJD Association of neonatal glycemia with neurodevelopmental outcomes at 4.5 years. JAMA Pediatrics, 2017.PMID 28783802
- [5]Harris DL Dextrose gel for neonatal hypoglycaemia (the Sugar Babies Study): a randomised, double-blind, placebo-controlled trial. Lancet, 2013.PMID 24075361
- [6]Edwards T Oral dextrose gel to prevent hypoglycaemia in at-risk neonates. Cochrane Database of Systematic Reviews, 2021.PMID 33998668
- [7]McIntyre HD Gestational diabetes mellitus. Nature Reviews Disease Primers, 2019.PMID 31296866
- [8]Kallem VR Infant of diabetic mother: what one needs to know? Journal of Maternal-Fetal & Neonatal Medicine, 2020.PMID 29947269
- [9]ACOG Macrosomia: ACOG Practice Bulletin, Number 216. Obstetrics and Gynecology, 2020.PMID 31856124
- [10]Kc K Gestational diabetes mellitus and macrosomia: a literature review. Annals of Nutrition and Metabolism, 2015.PMID 26045324
- [11]Ornoy A Diabetes during pregnancy: a maternal disease complicating the course of pregnancy with long-term deleterious effects on the offspring. A clinical review. International Journal of Molecular Sciences, 2021.PMID 33803995
- [12]Sarkar S Neonatal polycythemia and hyperviscosity. Seminars in Fetal and Neonatal Medicine, 2008.PMID 18424246