Paeds · fetal-neonatal-and-perinatal
Maternal disease, medication and substance effects on the fetus
Also known as Teratogenesis · Fetal teratogenic effects · Maternal medication in pregnancy · Substance use in pregnancy · Fetal alcohol spectrum disorder · Infant of a diabetic mother
Fellowship guide to how maternal medical conditions, therapeutic medications and non-medical substances affect the developing fetus and newborn: principles of teratogenesis and critical windows, the high-yield agents (diabetes, thyroid, antiepileptics, SSRIs, lithium, warfarin, ACE inhibitors, isotretinoin, maternal PKU, alcohol, tobacco, cannabis, stimulants, opioids), folic acid and magnesium sulfate prophylaxis, neonatal adaptation and withdrawal syndromes, and regional guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A teratogen is any agent — a maternal disease, a drug, a substance, a nutrient imbalance or an infection — that disturbs fetal development and produces a structural, growth, functional or behavioural abnormality. The word hides a subtlety examiners probe: teratogenesis is not one event. It is a timing-dependent process in which the same agent does different harm depending on the gestational window, the dose, and the genetic susceptibility of the fetus. [1]
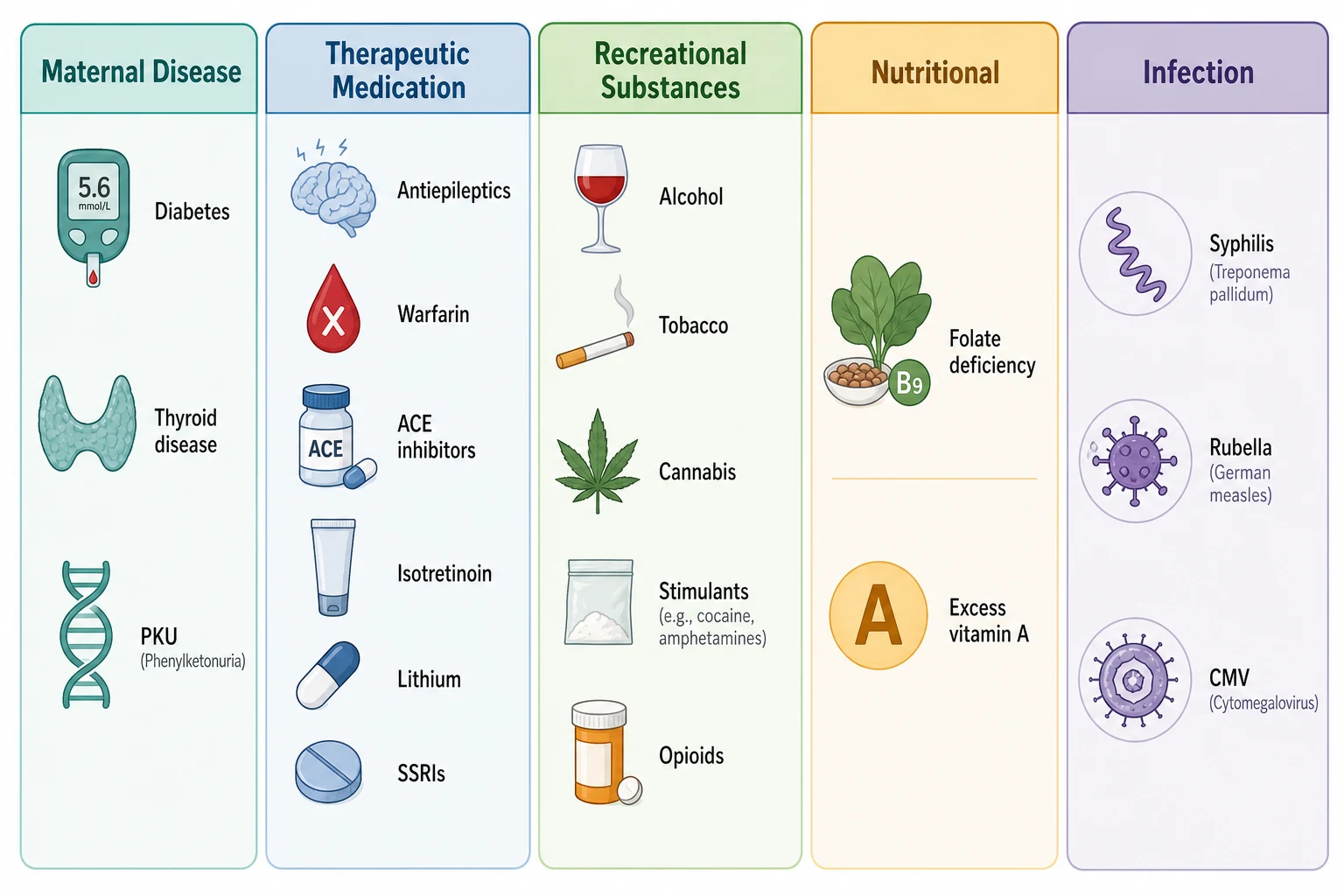
This topic covers the whole map of maternal-to-fetal harm: how maternal medical conditions injure the fetus (diabetes, thyroid disease, PKU, autoimmune disease), how therapeutic drugs do so (antiepileptics, SSRIs, lithium, warfarin, ACE inhibitors, isotretinoin, antithyroid drugs), and how recreational substances do so (alcohol, tobacco, cannabis, stimulants, opioids). It does not cover the neonatal management of abstinence syndrome in procedural detail, the management of neonatal hypoglycaemia, or perinatal infection screening — those have their own dedicated topics. What it does cover is how each exposure produces its effect, what to look for, what to prevent, and how to counsel a family without stigma. [27] [4]
The framework that organises everything here is the three critical windows of pregnancy: the pre-implantation all-or-none period, the organogenesis window when major structural defects arise, and the fetal period when growth and brain development are the targets. Once that framework is in place, every agent slots into a window, and every named syndrome becomes explicable. [1]
Classification
Start by separating the kinds of harm an exposure can cause, because a structural defect, a growth problem, a functional brain effect and a neonatal withdrawal syndrome are different things that need different surveillance. [1]
The first distinction is between a teratogenic structural effect (a major malformation from exposure in organogenesis, such as a cardiac defect from isotretinoin), a fetal growth effect (restriction from tobacco or alcohol in the fetal period), a functional or neurodevelopmental effect (cognitive impairment from valproate or maternal PKU, sometimes not evident until school age), and a neonatal adaptation or withdrawal syndrome (opioid or SSRI effects presenting after birth). One agent can span more than one category — alcohol harms structure, growth, function and behaviour all at once. [1] [21]
Maternal disease
Endocrine, metabolic
- Diabetes — cardiac, neural tube, caudal regression, macrosomia
- Thyroid disease — neurodevelopment
- Maternal PKU — microcephaly, cardiac, intellectual disability
- Systemic lupus — congenital heart block
Therapeutic medication
By drug class
- Antiepileptics — valproate highest risk
- SSRIs/SNRIs — PPHN, adaptation
- Lithium — cardiac (Ebstein)
- Warfarin — skeletal, CNS
- ACE inhibitors — renal fetopathy
- Isotretinoin — cardiac, craniofacial
- Antithyroid drugs — fetal goitre
Recreational substance
Non-medical
- Alcohol — FASD across all windows
- Tobacco — growth, stillbirth, neurodevelopment
- Cannabis — growth, neurodevelopment
- Stimulants — growth, placental
- Opioids — NAS, growth
Nutritional
Deficiency or excess
- Folate deficiency — neural tube defects
- Excess vitamin A or retinoids — teratogenic
- Iodine deficiency — cretinism
Infection
Congenital
- Syphilis, rubella, CMV, toxoplasma
- See perinatal infection screening topic
Epidemiology & Risk Factors
Roughly half of pregnancies in high-income countries are unplanned, so many teratogenic exposures happen before the woman knows she is pregnant. That single fact explains why pre-conception counselling matters more than first-trimester counselling for a planned pregnancy, and why so much harm is unintentional. [1]
Maternal diabetes is the most common endocrine condition to affect the fetus. The risk of a major congenital malformation in a pregnancy complicated by pre-existing diabetes is two to five times that of the background population, and the risk tracks directly with periconception glycaemic control. A woman with a normal HbA1c at conception approaches background risk; a woman with a high HbA1c carries the full excess. This is why pre-conception care for diabetes is one of the most evidence-based interventions in all of obstetrics. [4] [5]
The global prevalence of fetal alcohol spectrum disorder is estimated at close to 8 per 1000 in the general population by the JAMA Pediatrics meta-analysis — far higher than most clinicians realise, and higher still in some high-risk communities. Alcohol is the leading preventable, non-genetic cause of intellectual disability and neurodevelopmental disability in many settings. [21]
Prenatal tobacco use remains one of the most common harmful exposures, with rates of 10 to 20 percent in many high-income settings and higher in groups with socioeconomic disadvantage. Cannabis use in pregnancy has risen in jurisdictions that have legalised recreational use, and the meta-analysis evidence shows an association with lower birthweight and small-for-gestational-age infants. Opioid exposure and neonatal abstinence syndrome have risen steeply in North America over the last two decades and are increasingly recognised elsewhere. [23] [25] [27]
Risk amplifies when exposures combine. A woman smoking and drinking, or on polytherapy antiepileptics, carries a higher teratogenic load than the sum of the parts suggests. Social context — mental illness, intimate partner violence, poverty, substance-use disorder — both drives exposure and predicts outcomes, because the same adversity that drives use also impairs follow-up and developmental support. [10] [22]
Pathophysiology
Teratogenesis runs on a clock. The same agent does different harm at different gestational ages, so the mechanism is best understood window by window. [1]
During the pre-implantation period (the first two weeks after conception), the embryo is a small cluster of undifferentiated cells. Damage here follows the all-or-none rule: either the embryo is destroyed and lost as an early miscarriage, or it recovers completely because surviving cells can still form a whole organism. Teratogenic structural defects are generally not produced in this window. [1]
During organogenesis (weeks 3 to 8 post-conception, the embryonic period), the organs are forming. This is the critical window for major structural malformations. The heart is septating, the neural tube is closing, the face is fusing, the limbs are budding. An agent that disrupts cell migration, proliferation or programmed cell death in this window produces a structural defect — isotretinoin disrupting cranial neural crest cell migration to produce cardiac and craniofacial anomalies, valproate disrupting neural tube closure, warfarin disrupting vitamin-K-dependent osteocalcin to produce nasal and limb hypoplasia. [1] [19]
During the fetal period (from week 9 to term), the organs are growing and the brain is wiring. This is the window for growth restriction, functional impairment and neurodevelopmental effects. Tobacco, alcohol, cannabis and poorly controlled maternal diabetes act here. The harm is often invisible at birth and only emerges as a learning, attention or behavioural problem in childhood. [4] [21] [24]
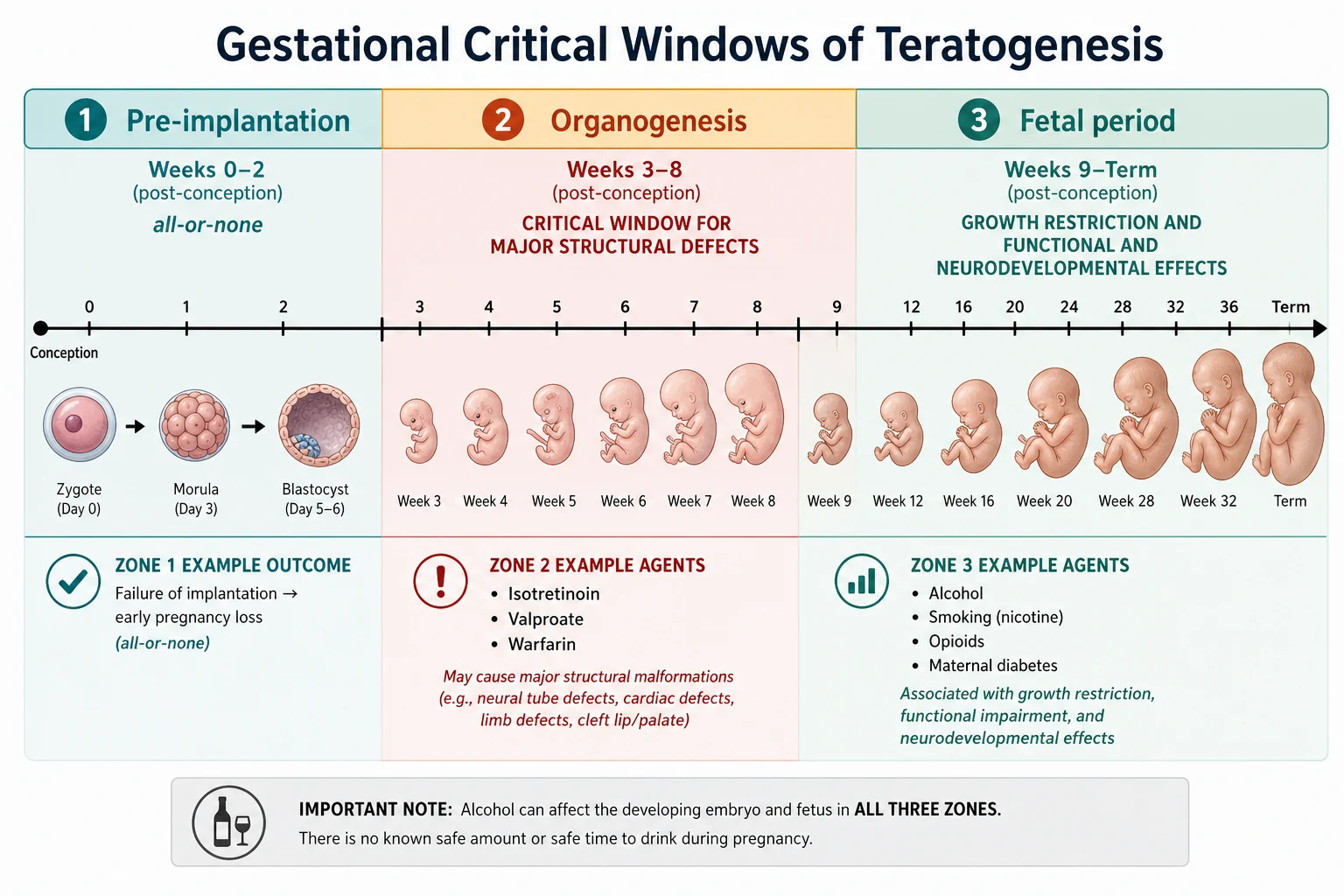
Alcohol is the agent that breaks the window rule, because it damages across all three periods. In organogenesis it produces the characteristic facial features and structural anomalies. In the fetal period it restricts growth and disrupts neuronal migration and synaptogenesis. Its mechanism is multifactorial: apoptotic neurodegeneration from altered NMDA and GABA signalling, disrupted neural crest cell migration, impaired astrocyte function and oxidative stress. The FASD phenotype is the integrated result. [21] [22]
Maternal diabetes harms through hyperglycaemia and its downstream messengers. Glucose crosses the placenta, the fetus responds with hyperinsulinaemia, and the result is macrosomia, neonatal hypoglycaemia and the metabolic cluster. Oxidative stress and disrupted gene expression in organogenesis produce the structural defects — cardiac (conotruncal and septal), neural tube, caudal regression and renal anomalies. The fetal heart is especially vulnerable because cardiac organogenesis is complete by week 7, before many women realise they are pregnant. [4] [5] [6]
Valproate's mechanism is among the best studied. It inhibits histone deacetylase, disrupts folate metabolism, increases oxidative stress and alters gene transcription during neural tube closure — hence its high rate of neural tube defects and its disproportionate neurodevelopmental signature, including an elevated risk of autism spectrum disorder. [11] [12]
Warfarin crosses the placenta and inhibits vitamin-K-dependent proteins, including osteocalcin, which is required for normal bone mineralisation in the fetal skeleton. The result is nasal hypoplasia, stippled epiphyses and limb hypoplasia when exposure occurs in organogenesis, and central nervous system abnormalities including intracranial calcification and haemorrhage when exposure continues later. Heparin and low-molecular-weight heparin do not cross the placenta and are the safer anticoagulant choice in pregnancy. [16]
ACE inhibitors block the fetal renin-angiotensin system. In the second and third trimester this causes fetal renal hypoperfusion, reduced urine output and oligohydramnios, which in turn causes limb contractures, craniofacial deformity and the characteristic hypocalvaria (deficient skull calcification) described in the kidney-skull connection. Neonatal renal failure and hypotension may follow. First-trimester ACE inhibitor exposure carries a smaller but measurable risk. [17] [18]
Clinical Presentation
The presentation depends entirely on which kind of harm occurred. A structural defect presents in the newborn period or on antenatal ultrasound; a growth effect presents as a small infant at birth; a neurodevelopmental effect may not present until school age; and an adaptation or withdrawal syndrome presents in the first hours to days of life. [21] [27]
The infant of a diabetic mother is the prototype neonatal presentation. The baby is macrosomic, plump and plethoric. Within hours, hypoglycaemia from fetal hyperinsulinaemia is the dominant risk. Respiratory distress from delayed surfactant maturation, polycythaemia with hyperbilirubinemia, and hypocalcaemia all occur at higher rates. Congenital anomalies — cardiac, caudal regression, neural tube, renal — may be present and demand targeted examination. [5] [6]
Fetal alcohol spectrum disorder presents with a characteristic facial phenotype in early childhood: short palpebral fissures, a thin vermilion border of the upper lip, and a smooth philtrum. Growth restriction (often postnatal onset) and a pattern of neurodevelopmental impairment — attention deficit, executive dysfunction, poor impulse control, language delay — become more apparent with age. The facial features may fade in adolescence and adulthood, but the cognitive and behavioural difficulties persist and often worsen without support. [21] [22]
Neonatal abstinence syndrome after opioid exposure presents with a constellation of central nervous system and gastrointestinal hyperexcitability: tremors, irritability, high-pitched cry, poor sleep, hypertonia, yawning, sneezing, nasal stuffiness, loose stools and feeding dysregulation. The timing of onset reflects the drug half-life — usually within 24 to 72 hours for short-acting opioids, and later for methadone or buprenorphine. The Finnegan score and the Eat-Sleep-Console functional approach are the two common assessment frameworks. [27] [28]
SSRI adaptation or discontinuation syndrome presents in the first days of life with irritability, tremor, feeding difficulty, mild respiratory distress and sometimes seizures. It is usually mild and self-limiting. The rarer but more serious association is persistent pulmonary hypertension of the newborn, which presents with severe hypoxaemia in a term or late-preterm infant. [14]
A fetal goitre from maternal antithyroid drugs is an antenatal or perinatal emergency. The enlarged thyroid can compromise the fetal airway and oesophagus, producing polyhydramnios antenatally and airway obstruction at birth. Affected neonates are hypothyroid at birth. Delivery must be planned with a team capable of securing a difficult airway, including consideration of an EXIT (ex-utero intrapartum treatment) procedure. [8]
Differential Diagnosis
When a neonate presents with dysmorphism, growth restriction, congenital anomalies, or neonatal irritability, the differential spans teratogenic, chromosomal, genetic, infectious and metabolic causes. The job is to assemble the exposure history and let it narrow the field, while never assuming teratogenic exposure is the whole story. [1]
For a dysmorphic neonate with congenital anomalies, the differential includes a chromosomal syndrome (trisomy 21, 18, 13; microdeletions), a single-gene syndrome (Noonan, Cornelia de Lange), a teratogenic syndrome (fetal valproate, fetal warfarin, fetal alcohol, isotretinoin embryopathy) and congenital infection (rubella, CMV, syphilis, toxoplasma). The discriminating questions are: what was the mother exposed to and when, what is the anomaly pattern, and what does the targeted genetic and infectious workup show. [11] [16]
For neonatal irritability and tremor, the dangerous mimics of withdrawal are sepsis, hypoglycaemia, hypocalcaemia, intracranial haemorrhage, metabolic disease and hypoxic-ischaemic encephalopathy. The exposure history helps — but if there is fever, temperature instability, abnormal tone, a metabolic acidosis, or a CSF pleocytosis, the diagnosis is not simple withdrawal. [27] [28]
For a fetal goitre, the differential is antithyroid drug effect, transient maternal TSH receptor antibody transfer (in a mother with Graves' disease), congenital hypothyroidism from dyshormonogenesis, and a fetal thyroid cyst or tumour. Maternal history and fetal thyroid function testing (often by cordocentesis) clarify the cause. [8]
For small-for-gestational-age, the differential weighs maternal smoking, alcohol, placental insufficiency (including preeclampsia), congenital infection, a genetic syndrome and chromosomal abnormality. Each has associated features; isolated growth restriction in a smoker is common, but combined with structural anomalies it broadens the workup. [23]
Clinical & Bedside Assessment
Start with the exposure history, because it is the single most powerful tool you have. Ask about every medication by name, dose, trimester and duration — including over-the-counter, herbal and complementary products. Ask about recreational substances specifically and without judgement, including alcohol in units per week (or more usefully, on any occasion), tobacco, vaping, cannabis, stimulants and opioids. Ask about the partner's substance use and the home environment. Then ask about maternal medical conditions — diabetes, thyroid disease, epilepsy, autoimmune disease, psychiatric illness, PKU — and their control around conception. [1] [27]
The dysmorphology examination should be systematic and targeted. Measure the palpebral fissure length and inspect the philtrum and upper lip vermilion with the standardised FASD lip-philtrum guide if available. Examine the nasal bridge, the limbs and the nails (hypoplasia suggests fetal warfarin or phenytoin). Auscultate the heart for a murmur or a rate suggesting congenital heart block. Examine the abdomen for organomegaly and the head circumference for microcephaly. [21] [16]
The infant of a diabetic mother needs a glucose-focused early assessment: baseline glucose within the first hours, feeding observation, and a low threshold for escalation if glucose is below the operational threshold. Examine for the macrosomia, respiratory distress, birth injury (brachial plexus, clavicle) and congenital anomalies that cluster in this group. [5]
For opioid withdrawal assessment, a validated tool must be used consistently. The Finnegan Neonatal Abstinence Scoring Tool scores signs across multiple systems at intervals. The Eat-Sleep-Console functional approach assesses whether the infant can eat, sleep and be consoled, and uses non-pharmacological care as the first-line intervention, with pharmacological treatment reserved for infants who fail these functional assessments. Rooming-in with the mother reduces the need for pharmacological treatment. [27] [28]
The antenatal assessment of a fetal goitre requires ultrasound to measure the thyroid, to assess for polyhydramnios, and to plan delivery. Cordocentesis for fetal thyroid function is considered when the diagnosis is uncertain. A multidisciplinary plan with neonatology, otolaryngology and obstetric anaesthesia is essential. [8]
Investigations
Investigations are driven by the exposure and the suspected effect. There is no blanket workup for "a maternal exposure" — each agent has its own targeted assessment. [1]
A detailed fetal anatomy ultrasound at 18 to 20 weeks is the cornerstone after any significant first-trimester teratogenic exposure. It detects structural defects — cardiac, craniofacial, neural tube, skeletal, renal. The timing matters: too early and the structures have not formed; the standard 18 to 20 week scan is the optimal window. [19]
A fetal echocardiogram is indicated after first-trimester exposure to lithium, valproate, isotretinoin or poorly controlled maternal diabetes, because the fetal heart is a common target. It is usually performed at 18 to 22 weeks by a specialist in fetal cardiology. [5] [15]
For maternal PKU, serial serum phenylalanine levels guide dietary restriction. The target is a phenylalanine level within the recommended therapeutic range (commonly 120 to 360 micromol/L), maintained from before conception through pregnancy. Tight control before conception and in the first trimester is what prevents the congenital anomalies and intellectual disability. [20]
For the neonate with suspected withdrawal, drug screens (meconium, umbilical cord tissue and urine) can confirm exposure and identify unsuspected substances, but they do not by themselves diagnose or score withdrawal — clinical assessment does. Useful neonatal investigations to exclude mimics include blood glucose, calcium, full blood count, blood gas, and cultures if sepsis is possible. [27] [28]
For the infant of a diabetic mother, early and serial blood glucose monitoring, bilirubin, and a targeted examination for congenital anomalies. An echocardiogram is indicated if a murmur or distress is present, or if antenatal cardiac findings were abnormal. [5]
For suspected ACE inhibitor fetopathy, a renal ultrasound and serial renal function and electrolytes are indicated, because the renal injury may evolve over the first days. Skull radiographs or imaging for hypocalvaria is rarely required clinically but is part of the named syndrome. [17] [18]
Management — Resuscitation
The immediate neonatal management of a teratogenic exposure depends on which effect has presented. Three scenarios dominate. [1]
Hypoglycaemia in the infant of a diabetic mother. Early feeding is the first step. Glucose is monitored by local protocol, typically within the first one to two hours and then before feeds. If glucose is below the operational threshold despite feeding, escalation is buccal 40 percent dextrose gel combined with a feed and recheck, then intravenous 10 percent dextrose. The exact concentration and rate follow the local neonatal guideline — state that you would use the current protocol rather than a memorised number. [5]
Persistent pulmonary hypertension of the newborn after SSRI exposure is a respiratory and haemodynamic emergency. Support oxygenation, consider surfactant if there is parenchymal disease, use inhaled nitric oxide for refractory hypoxaemia, and escalate to specialised neonatal intensive care. Early involvement of the neonatal retrieval or intensive care team is essential. [14]
Neonatal abstinence syndrome that is moderate or severe despite non-pharmacological care requires pharmacological treatment. The first-line agent in most protocols is an opioid — oral morphine or methadone — started when withdrawal scores reach the treatment threshold, and weaned gradually. Adjuncts (phenobarbital, clonidine) are used in specific protocols, especially for polysubstance exposure. The goal is a comfortable, feeding, sleeping infant who can be weaned safely. [27] [28]
Fetal goitre with airway risk is a planned-delivery problem. An EXIT procedure, in which uteroplacental circulation is maintained while the neonatal airway is secured, may be needed. This requires a full multidisciplinary team and a tertiary obstetric and neonatal centre. [8]
Management — Definitive & Stepwise
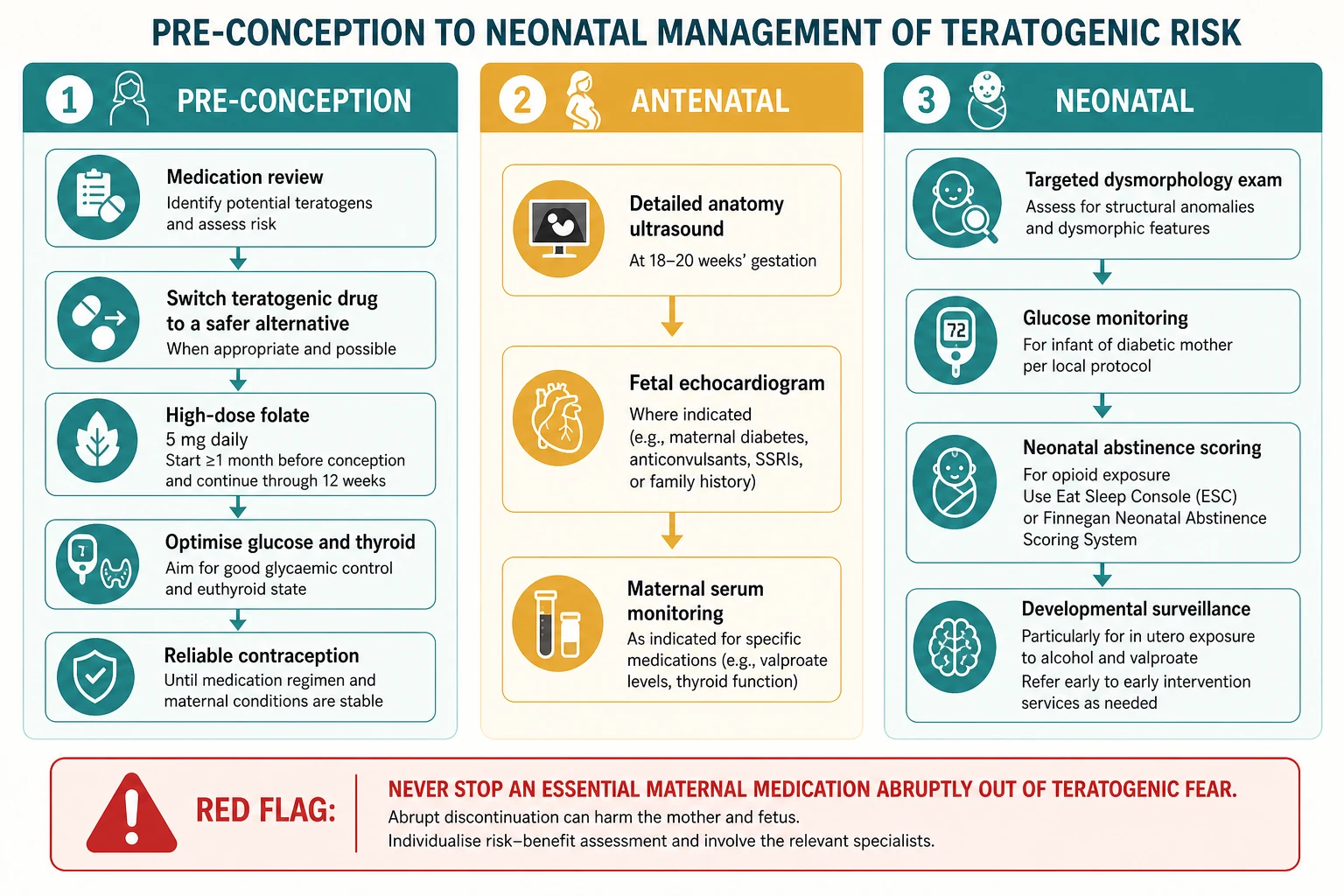
The definitive management of teratogenic risk begins before conception and runs through the neonatal period and into long-term surveillance. It is best organised in three phases. [1]
Pre-conception
Pre-conception care is where most teratogenic harm is actually prevented. The principles are to review every medication, to switch a teratogen to a safer alternative where possible, to optimise any maternal disease, and to use reliable contraception until the woman is stable. For a woman on valproate, lamotrigine or levetiracetam are preferred alternatives where the epilepsy allows. For a woman on isotretinoin, contraception must be reliable and pregnancy excluded before, during and after treatment (the iPLEDGE programme and its regional equivalents). For a woman on an ACE inhibitor, switching to a pregnancy-compatible antihypertensive (labetalol, nifedipine, methyldopa) before conception removes the risk. For a woman on warfarin, switching to low-molecular-weight heparin before conception removes the embryopathy risk. [9] [11]
Pre-conception medication review
List every agent
Prescribed, over-the-counter, herbal, recreational, by trimester
Rank teratogenic risk
High (isotretinoin, warfarin, valproate) versus low or none
Switch where possible
Lamotrigine or levetiracetam for valproate, LMWH for warfarin, labetalol for ACE inhibitor
Optimise the disease
Diabetes glycaemic control, thyroid euthyroid, epilepsy seizure-free
Start high-dose folate
5 mg daily for high-risk women, 400 microgram standard for all
Contraception until stable
Then aim conception on the safest possible regimen
Folic acid is the single most evidence-based preventive intervention. A daily supplement of 400 microgram from before conception through the first trimester reduces the risk of a first neural tube defect. For women at higher risk — previous affected pregnancy, on valproate or carbamazepine, maternal diabetes, obesity — the recommended dose is 4 to 5 mg daily. Mandatory folic acid fortification of staple foods, adopted in the United States, Canada, Australia and New Zealand, has reduced the population prevalence of neural tube defects. [2]
Magnesium sulfate given to the mother before a preterm birth under 30 weeks gestation reduces the risk of cerebral palsy in the surviving infant. This is a fetal neuroprotective intervention delivered by the obstetric team, and the updated Cochrane review confirms the benefit. Know the gestational cut-off and the indication: it is for anticipated preterm birth under 30 weeks, not for all preterm labour. [3]
Antenatal
During pregnancy, surveillance is tailored to the exposure. Detailed anatomy ultrasound at 18 to 20 weeks for any significant first-trimester teratogen. Fetal echocardiography for cardiac-targeting agents. Serial serum phenylalanine for maternal PKU. Serial antiepileptic drug levels for women on lamotrigine (whose clearance rises sharply in pregnancy) and other agents. Ongoing obstetric management of maternal diabetes and thyroid disease. [7] [9] [20]
Maternal thyroid disease in pregnancy is managed in partnership with endocrinology. The levothyroxine dose typically increases by 25 to 30 percent in early pregnancy because of the rise in thyroxine-binding globulin and placental deiodinase, and the target TSH is trimester-specific (commonly below 2.5 mIU/L in the first trimester). For a woman with Graves' disease, propylthiouracil is preferred in the first trimester (lower teratogenicity than carbimazole or methimazole), with a switch to carbimazole or methimazole in the second trimester (lower hepatotoxicity than PTU). Both drugs cross the placenta and can cause fetal goitre and hypothyroidism, so fetal thyroid surveillance is part of care. [7] [8]
Maternal PKU requires strict dietary phenylalanine restriction, ideally begun before conception, maintained through pregnancy, and supervised by a metabolic team. Even modestly elevated phenylalanine in the first trimester predicts congenital anomalies and microcephaly; the later the control is achieved, the worse the neurodevelopmental outcome. [20]
Neonatal and beyond
The neonatal plan is exposure-specific. Glucose monitoring for the infant of a diabetic mother. Withdrawal scoring for opioid exposure. Targeted dysmorphology examination and cardiac evaluation for isotretinoin or warfarin exposure. Thyroid function for antithyroid drug exposure. Renal function for ACE inhibitor exposure. And, for every exposure with a neurodevelopmental signature — alcohol, valproate, maternal PKU, tobacco — a planned schedule of developmental surveillance into early childhood. [4] [11] [27]
Specific Subtypes & Scenarios
Maternal pre-existing versus gestational diabetes. The fetal structural anomaly risk is driven by periconception glycaemic control, which is why pre-existing diabetes carries a higher malformation risk than gestational diabetes (which begins after organogenesis is complete). Gestational diabetes still produces macrosomia and neonatal hypoglycaemia. Pre-conception care for pre-existing diabetes is one of the most cost-effective interventions in all of obstetrics. [4] [5]
Antiepileptic drug ranking. Valproate carries the highest teratogenic risk (major malformation rate around 6 to 10 percent, with neurodevelopmental harm on top). Topiramate and phenobarbital carry intermediate risk. Carbamazepine and phenytoin carry lower but real risk and produce their own named syndromes (fetal hydantoin syndrome — hypoplastic nails and digits, cleft lip and palate, characteristic facies). Lamotrigine and levetiracetam carry the lowest risk and are the preferred agents in pregnancy where the epilepsy allows. Polytherapy multiplies the risk. [9] [10] [12] [13]
Isotretinoin: oral versus topical. Oral isotretinoin is a potent teratogen with effects on cranial neural crest cells — cardiac outflow tract anomalies, craniofacial defects, thymic aplasia and CNS malformations. The critical window is weeks 2 to 5 post-conception, often before the pregnancy is known. Topical retinoids have substantially lower systemic absorption and the evidence does not support a comparable teratogenic risk, though avoidance in pregnancy is still advised. Prevention programmes (iPLEDGE) aim to eliminate pregnancy exposure through contraception and pregnancy testing. [19]
Warfarin versus heparin. Warfarin crosses the placenta and causes fetal warfarin syndrome; unfractionated and low-molecular-weight heparin do not cross the placenta and are safe for the fetus. Women requiring anticoagulation in pregnancy should be switched to LMWH before conception or as soon as pregnancy is diagnosed. [16]
Lithium and the heart. The historical association of first-trimester lithium exposure with Ebstein anomaly (a downward displacement of the tricuspid valve septal leaflet) is real but the absolute risk is small and was historically overstated. The NEJM cohort showed a dose-dependent increase in cardiac malformations overall. Lithium may be the safest option for some women with severe bipolar disorder; the decision is individualised with psychiatry. [15]
Type of opioid and NAS. Methadone is associated with a longer and sometimes more severe withdrawal than buprenorphine. The choice of maintenance therapy in pregnancy is made by addiction medicine, with buprenorphine increasingly favoured for a milder neonatal course. [27] [28]
Combined exposures. Alcohol and tobacco together, antiepileptic polytherapy, or substance use plus a prescribed teratogen — combinations multiply risk and complicate the counselling. Always ask about the full picture, not just the index exposure. [10] [22]
Complications & Pitfalls
The most dangerous pitfall in this whole topic is stopping an essential medication abruptly out of teratogenic fear. A woman who stops her antiepileptic in pregnancy can seize — and a generalised tonic-clonic seizure carries a risk to both mother and fetus that may exceed the teratogenic risk of a carefully chosen drug. A woman who stops her psychiatric medication can relapse, with devastating consequences. A woman who stops her anticoagulation can thrombose. The correct action is always to consult early, individualise the risk-benefit balance, and switch to the safest effective regimen — never to stop in a panic. [1] [9]
The unrecognised FASD is a major complication with lifelong consequences. Children with FASD are over-represented in foster care, youth justice and mental health populations. Early diagnosis, a stable home, and appropriate educational and behavioural support substantially improve outcomes — but they require the clinician to recognise the phenotype and to ask about alcohol non-judgementally. [21] [22]
The neonatal mimic trap — attributing irritability to opioid or SSRI withdrawal while missing sepsis, hypoglycaemia or metabolic disease — has been emphasised already but deserves repetition. Always exclude the dangerous mimics before settling on withdrawal as the sole diagnosis. [27]
Communication pitfalls are everywhere in this topic. Stigmatising a woman for substance use drives her away from care. Frightening a woman who has already been exposed, when the exposure is past and the harm if any is done, adds anxiety without benefit. The skill is to be honest about risk, supportive of change, and practical about surveillance. [28]
Medicolegal and ethical pitfalls include mandatory reporting done badly, coerced treatment, and punitive approaches to substance use in pregnancy. The evidence does not support punitive approaches; they deter care and worsen outcomes. Supportive, harm-reduction approaches work better. [27]
Prognosis & Disposition
Prognosis depends on the exposure, the timing, the dose, and the developmental support the child receives afterwards. [1]
For fetal alcohol spectrum disorder, the long-term outlook is determined by early diagnosis, a stable and supportive home, absence of further adversity (including ongoing exposure), and access to appropriate educational and mental health support. With the right support, many individuals with FASD live independent and productive lives; without it, they are at high risk of school failure, mental illness, substance use and justice involvement. [21] [22]
For fetal valproate exposure, the structural anomalies are managed in their own right, but the neurodevelopmental effect — lower IQ, elevated autism risk, attentional difficulties — often becomes apparent in early childhood and requires longitudinal developmental surveillance and educational support. [11] [12]
For ACE inhibitor fetopathy, the renal outcome depends on the severity and duration of the renal injury. Some neonates recover renal function; others are left with chronic kidney disease and require long-term nephrology follow-up. [17] [18]
For neonatal abstinence syndrome, the acute prognosis is good with appropriate care, and opioid exposure in isolation does not appear to cause lasting cognitive harm. The longer-term outcomes are more strongly predicted by the social and environmental context — stability of the home, ongoing parental substance use, poverty and adversity — than by the opioid exposure itself. Supporting the mother-infant dyad is central. [27] [28]
Disposition from the neonatal period is home with a targeted follow-up plan — developmental surveillance for the neurodevelopmental signatures, nephrology for renal injury, cardiology for structural heart disease, and a medical home that coordinates the whole package. [4]
Special Populations
Indigenous, rural and remote families carry a disproportionate burden of fetal alcohol spectrum disorder and substance-related harm in some settings, driven by the upstream determinants of health — colonisation, intergenerational trauma, poverty, access to care. Screening, diagnosis and support must be culturally safe, family-inclusive, and delivered in partnership with community. A diagnosis made without a support plan, or delivered in a stigmatising way, causes harm. [21] [22]
Women with severe mental illness on polypharmacy who become pregnant need joint management with perinatal psychiatry. Lithium, valproate (often still used in psychiatry for bipolar disorder), some antipsychotics and benzodiazepines all carry risks, and the risk of untreated maternal psychiatric illness is also substantial. The decision is individualised, never made by stopping everything. [15]
Pregnant adolescents with substance use need care that respects confidentiality and developmental stage, with attention to consent, safeguarding, and the often-hidden coercion or trauma that drives use. [27]
Migrant and refugee families may have incomplete medical records, unknown medication and exposure histories, and may need interpreter-supported counselling. Hepatitis B, syphilis and other infectious exposures may be untested. [7]
Women with epilepsy and intellectual disability or complex psychosocial circumstances need extra support to adhere to the safest regimen, to attend surveillance, and to manage the infant — a pre-conception plan is essential. [9]
Evidence, Guidelines & Regional Differences
The evidence base for teratogenic risk comes from a combination of prospective pregnancy registries, large cohort studies and systematic reviews. For antiepileptics, the EURAP registry and the Neurodevelopmental Effects of Antiepileptic Drugs (NEAD) study have defined the relative risks and the neurodevelopmental signature of valproate. The 2019 European consensus statement on fetal valproate spectrum disorder codified the diagnosis. [9] [11] [12]
The 2024 Cochrane review of magnesium sulfate for fetal neuroprotection confirms the benefit before preterm birth under 30 weeks. The evidence for folic acid is decades old but reaffirmed in recent reviews; the debate now is about fortification policy and optimal dose. [2] [3]
Australia and Aotearoa New Zealand mandate folic acid fortification of bread-making flour and follow NHMRC and RANZCOG guidance on medication in pregnancy. The Australian Guide to the Diagnosis of FASD and the New Zealand FASD action plan provide diagnostic and support frameworks. Culturally safe care for Aboriginal, Torres Strait Islander, Maori and Pacific families is a priority. NAS care emphasises rooming-in and non-pharmacological approaches. [2] [21]
United Kingdom has agreed to mandatory folic acid fortification (rollout in progress) after decades of voluntary policy. NICE and RCOG guidance governs medication in pregnancy, and the BUMPS and UKTIS services support clinicians. NAS guidance emphasises non-pharmacological care first. [2]
United States has had mandatory folic acid fortification of enriched grain since 1998. ACOG, AAP and CDC guidance applies. The iPLEDGE programme governs isotretinoin. The opioid-exposed newborn is managed with Finnegan or Eat-Sleep-Console approaches, and the shift is toward functional assessment and rooming-in. [2] [19] [27]
Canada has mandatory folic acid fortification and follows SOGC and CPS guidance, with provincial NAS and rooming-in policies. [2]
WHO and low-resource settings emphasise folate supplementation where fortification is absent, the prevention of alcohol and tobacco use in pregnancy, and harm-reduction approaches to substance use. Access to prenatal diagnosis and to safe medication switching may be limited. [2] [21]
Exam Pearls
- The all-or-none period is the first two weeks post-conception. Structural defects come in weeks 3 to 8. [1]
- Fetal valproate syndrome: neural tube defects, cardiac anomalies, characteristic facies, developmental delay, autism risk. [11] [12]
- Fetal warfarin syndrome: nasal hypoplasia, stippled epiphyses, limb hypoplasia, CNS calcification. Switch to LMWH. [16]
- ACE inhibitor fetopathy: oligohydramnios, renal failure, hypocalvaria. Second and third trimester is the danger zone. [17] [18]
- Isotretinoin: cardiac and craniofacial, critical window weeks 2 to 5, often before pregnancy is known. iPLEDGE prevents exposure. [19]
- Lithium and Ebstein: real but historically overstated; absolute risk small; individualise with psychiatry. [15]
- Lamotrigine and levetiracetam are the preferred antiepileptics in pregnancy. Lamotrigine levels fall in pregnancy — monitor and dose-adjust. [9]
- High-dose folic acid is 5 mg for women on valproate or carbamazepine, previous NTD, maternal diabetes, obesity. [2]
- Maternal PKU target phenylalanine is commonly 120 to 360 micromol/L, from before conception. [20]
- NAS: exclude sepsis, hypoglycaemia and metabolic disease before settling on withdrawal. Use Finnegan or Eat-Sleep-Console. [27] [28]
- There is no known safe level of alcohol in pregnancy. [21]
- Antithyroid drugs: PTU in first trimester, switch to carbimazole or methimazole in second trimester. Both can cause fetal goitre. [7] [8]
- Magnesium sulfate for fetal neuroprotection: before preterm birth under 30 weeks. [3]
TERATOGEN
References
- [1]Frias JL, Thomas IT Teratogens and teratogenesis: general principles of clinical teratology. Annals of Clinical and Laboratory Science, 1988.PMID 3289471
- [2]van Gool JD, Hirche H, Lax H, De Schaepdrijver L Folic acid and primary prevention of neural tube defects: A review. Reproductive Toxicology, 2018.PMID 29777755
- [3]Shepherd ES, Goldsmith S, Doyle LW, Middleton P, et al. Magnesium Sulfate Before Preterm Birth for Neuroprotection: An Updated Cochrane Systematic Review. Obstetrics and Gynecology, 2024.PMID 38830233
- [4]Ye W, Luo C, Zhou J, Liang X, et al. Association between maternal diabetes and neurodevelopmental outcomes in children: a systematic review and meta-analysis of 202 observational studies comprising 56.1 million pregnancies. Lancet Diabetes and Endocrinology, 2025.PMID 40209722
- [5]Hornberger LK Maternal diabetes and the fetal heart. Heart, 2006.PMID 16698822
- [6]Rodolaki K, Pergialiotis V, Iakovidou N, Boutsikou T, et al. The impact of maternal diabetes on the future health and neurodevelopment of the offspring: a review of the evidence. Frontiers in Endocrinology, 2023.PMID 37469977
- [7]Huget-Penner S, Feig DS Maternal thyroid disease and its effects on the fetus and perinatal outcomes. Prenatal Diagnosis, 2020.PMID 32181913
- [8]Bliddal S, Rasmussen AK, Sundberg K, Brocks V, et al. Antithyroid drug-induced fetal goitrous hypothyroidism. Nature Reviews Endocrinology, 2011.PMID 21403664
- [9]Tomson T, Landmark CJ, Battino D Antiepileptic drug treatment in pregnancy: changes in drug disposition and their clinical implications. Epilepsia, 2013.PMID 23360413
- [10]Vajda FJ, Hitchcock AA, Graham J, O'Brien TJ, et al. The teratogenic risk of antiepileptic drug polytherapy. Epilepsia, 2010.PMID 19817810
- [11]Clayton-Smith J, Bromley R, Dean J, Journel H, et al. Diagnosis and management of individuals with Fetal Valproate Spectrum Disorder; a consensus statement from the European Reference Network for Congenital Malformations and Intellectual Disability. Orphanet Journal of Rare Diseases, 2019.PMID 31324220
- [12]Cummings C, Stewart M, Stevenson M, Morrow J, et al. Neurodevelopment of children exposed in utero to lamotrigine, sodium valproate and carbamazepine. Archives of Disease in Childhood, 2011.PMID 21415043
- [13]Hegde A, Kaur A, Sood A, Dhanorkar M, et al. Fetal Hydantoin Syndrome. Journal of Pediatrics, 2017.PMID 28578158
- [14]Berard A, Sheehy O, Zhao JP, Vinet E, et al. SSRI and SNRI use during pregnancy and the risk of persistent pulmonary hypertension of the newborn. British Journal of Clinical Pharmacology, 2017.PMID 27874994
- [15]Patorno E, Huybrechts KF, Bateman BT, Cohen JM, et al. Lithium Use in Pregnancy and the Risk of Cardiac Malformations. New England Journal of Medicine, 2017.PMID 28591541
- [16]Chan KY, Gilbert-Barness E, Tiller G Warfarin embryopathy. Pediatric and Developmental Pathology, 2003.PMID 14692224
- [17]Barr M Jr, Cohen MM Jr ACE inhibitor fetopathy and hypocalvaria: the kidney-skull connection. Teratology, 1991.PMID 1771591
- [18]Deva M, Kara T ACE inhibitor fetopathy: a case series and survey of opinion amongst New Zealand paediatricians, obstetricians, neonatologists, and nephrologists. New Zealand Medical Journal, 2012.PMID 22960716
- [19]Cha EH, Kim N, Kwak HS, Han HJ, et al. Pregnancy and neonatal outcomes after periconceptional exposure to isotretinoin in Koreans. Obstetrics and Gynecology Science, 2022.PMID 35193174
- [20]Verduci E, Tosi M, Zuvadelli J, Giorda S, et al. The First 1000 Days of PKU: A Narrative Review of Maternal PKU and Early Life Management After Positive Newborn Screening. Nutrients, 2026.PMID 41599812
- [21]Lange S, Probst C, Gmel G, Rehm J, et al. Global Prevalence of Fetal Alcohol Spectrum Disorder Among Children and Youth: A Systematic Review and Meta-analysis. JAMA Pediatrics, 2017.PMID 28828483
- [22]Popova S, Lange S, Shield K, Mihic A, et al. Comorbidity of fetal alcohol spectrum disorder: a systematic review and meta-analysis. Lancet, 2016.PMID 26777270
- [23]Abraham M, Alramadhan S, Iniguez C, Duijts L, et al. A systematic review of maternal smoking during pregnancy and fetal measurements with meta-analysis. PLoS One, 2017.PMID 28231292
- [24]Correa ML, Soares PSM, da Silva BGC, Wehrmeister F, et al. Maternal smoking during pregnancy and intelligence quotient in offspring: A systematic review and meta-analysis. Neurotoxicology, 2021.PMID 34004235
- [25]Lo JO, Shaw B, Robalino S, Ayers CK, et al. Cannabis Use in Pregnancy and Neonatal Outcomes: A Systematic Review and Meta-Analysis. Cannabis and Cannabinoid Research, 2024.PMID 36730710
- [26]Kalaitzopoulos DR, Chatzistergiou K, Amylidi AL, Kokkinidis DG, et al. Effect of Methamphetamine Hydrochloride on Pregnancy Outcome: A Systematic Review and Meta-analysis. Journal of Addiction Medicine, 2018.PMID 29509557
- [27]Coyle MG, Brogly SB, Ahmed MS, Patrick SW, et al. Neonatal abstinence syndrome. Nature Reviews Disease Primers, 2018.PMID 30467370
- [28]Jansson LM, Patrick SW Neonatal Abstinence Syndrome. Pediatric Clinics of North America, 2019.PMID 30819342