Paeds · fetal-neonatal-and-perinatal
Meconium aspiration syndrome
Also known as Meconium aspiration · MAS · Meconium-stained amniotic fluid aspiration · Neonatal meconium pneumonitis
Fellowship guide to meconium aspiration syndrome: the pathophysiology of meconium-induced lung injury (airway obstruction, surfactant inactivation, chemical pneumonitis, infection risk), the vigour-based delivery-room algorithm that replaced routine suctioning, the severity-based escalation ladder (oxygen, CPAP, ventilation, surfactant, inhaled nitric oxide, ECMO), recognition and management of persistent pulmonary hypertension of the newborn, and regional guideline differences across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Meconium aspiration syndrome (MAS) is the clinical syndrome of respiratory distress that develops in a newborn infant born through meconium-stained amniotic fluid (MSAF), with characteristic radiographic findings, when other causes of neonatal respiratory distress have been excluded [7]. The meconium — the neonate's first stool, composed of desquamated intestinal cells, swallowed lanugo, mucus, bile pigments, pancreatic enzymes and water — is passed in utero in the setting of fetal stress or post-maturity and is then aspirated, typically through fetal gasping driven by hypoxia [7].
MAS remains one of the leading causes of term and near-term neonatal respiratory failure. Its hallmark is a triad of MSAF, respiratory distress within the first hours of life, and a chest radiograph showing coarse, patchy infiltrates with hyperinflation and, frequently, air leak. The clinical course ranges from transient tachypnoea requiring minimal oxygen to fulminant respiratory failure complicated by persistent pulmonary hypertension of the newborn (PPHN), pneumothorax and death [7].
Epidemiology & Risk Factors
Meconium staining of the amniotic fluid occurs in approximately 8 to 15 per cent of all live births and is strongly related to gestational age: it is rare before 34 weeks, rises steadily toward term, and is most frequent in post-term pregnancies of 42 weeks or more [4]. Of those infants exposed to MSAF, only about 2 to 5 per cent develop MAS, and a smaller subset — roughly 0.5 to 1 per cent of all MSAF-exposed infants — progress to severe disease requiring high ventilatory support or extracorporeal membrane oxygenation (ECMO) [4].
The incidence and mortality of MAS have fallen substantially over the past three decades, driven by changes in obstetric practice (proactive labour management, reduction in post-term deliveries, abandonment of routine perineal and intrapartum suctioning) and by improvements in neonatal respiratory support [4].
The principal risk factors cluster into fetal, placental and obstetric categories. Recognising them at the bedside allows anticipation of resuscitation needs and early escalation [7].
Risk factors for meconium passage and for progression to MAS
| Category | Risk factors |
|---|---|
| Fetal | Post-term gestation (42 wk or more), intrauterine growth restriction, fetal distress / acidosis, chronic intrauterine hypoxia, poor biophysical profile |
| Placental / umbilical | Placental insufficiency, oligohydramnios, nuchal cord, abruptio placentae |
| Maternal / obstetric | Pre-eclampsia, hypertension, diabetes, chorioamnionitis, prolonged labour, emergency caesarean for fetal distress |
| Iatrogenic (historical) | Routine perineal/intratracheal suctioning (now abandoned — no longer recommended) [1] |
Pathophysiology
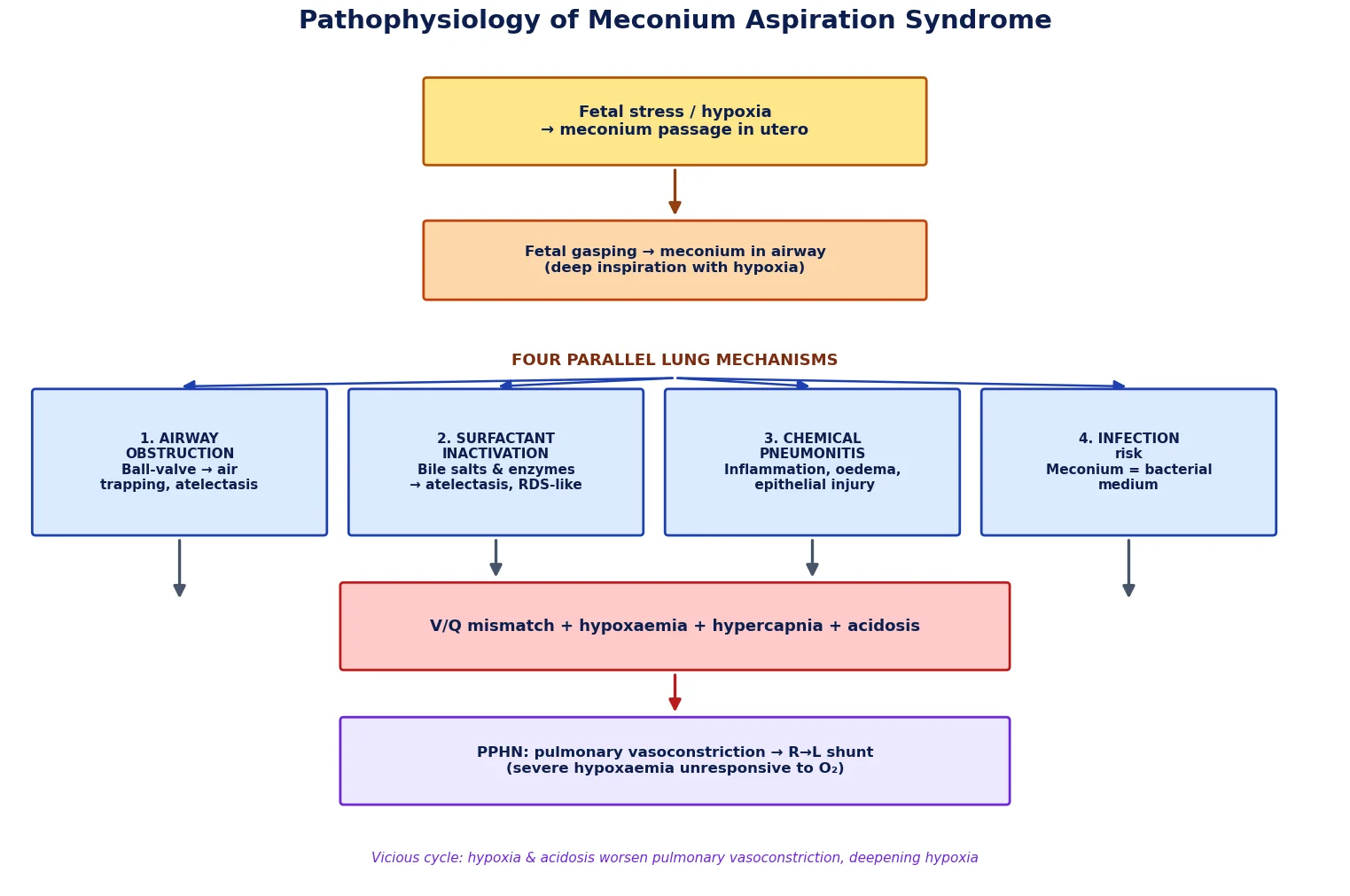
The pathophysiology of MAS is a self-amplifying cascade in which four parallel lung injury mechanisms converge to produce severe gas-exchange failure and, in the most severe cases, PPHN. The initiating event is fetal stress — usually hypoxia — which both triggers meconium passage and induces fetal gasping that draws meconium into the large and small airways in utero [7].
The first mechanism is airway obstruction. Particulate meconium and mucus plugs produce a ball-valve effect: gas can enter during inspiration but is trapped on expiration, producing hyperinflation, air trapping and a high risk of pneumothorax and pulmonary interstitial emphysema. Complete plugging of bronchioles produces distal atelectasis and right-to-left intrapulmonary shunting [7].
The second mechanism is surfactant inactivation. The bile salts, free fatty acids and enzymes in meconium are potent surfactant inhibitors; they displace surfactant from the alveolar surface, reduce surface tension-lowering capacity, and produce a clinical and radiographic picture that closely resembles surfactant-deficiency respiratory distress syndrome. This is the rationale for exogenous surfactant therapy in moderate-to-severe MAS [2].
The third mechanism is chemical pneumonitis. Meconium is intensely irritant to the alveolar epithelium, triggering an inflammatory cascade with neutrophil influx, release of cytokines and proteases, pulmonary oedema, and epithelial necrosis within hours. This inflammation independently worsens surfactant dysfunction and predisposes to secondary bacterial infection [7].
The fourth mechanism — and the one that defines severe MAS — is persistent pulmonary hypertension of the newborn (PPHN). Hypoxaemia, acidosis and hypercapnia drive intense pulmonary vasoconstriction and prevent the fall in pulmonary vascular resistance that should normally occur at birth. Right ventricular pressure exceeds systemic pressure, and the ductus arteriosus and foramen ovale shunt right-to-left, producing profound, oxygen-refractory hypoxaemia [6].
FOUR LUNG MECHANISMS of MAS — OBIS
Classification
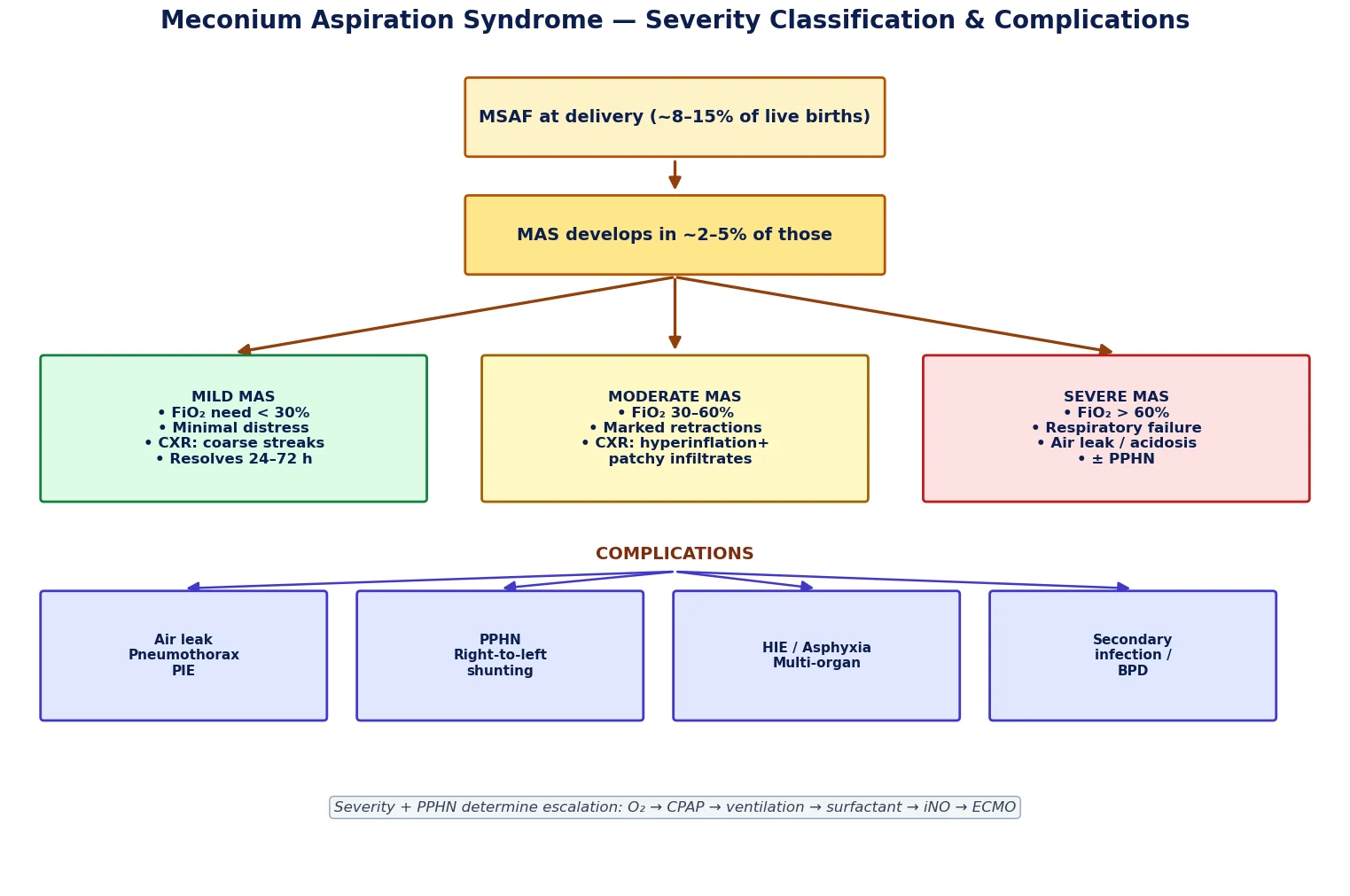
MAS is most usefully classified by clinical severity, because severity directly determines the escalation pathway and predicts the risk of complications such as air leak and PPHN. Severity is defined by the inspired oxygen concentration required to maintain acceptable saturation, the degree of respiratory distress, and the presence of respiratory failure [7].
A second, orthogonal classification distinguishes MAS with PPHN from MAS without PPHN, because the two carry different management (need for echo, inhaled nitric oxide, and consideration of ECMO) and different prognoses. PPHN is suspected clinically when hypoxaemia is profound and labile, out of proportion to the radiographic infiltrates, and is confirmed by echocardiographic demonstration of right-to-left ductal or foramen-ovale shunting with elevated pulmonary pressures [6].
Mild vs moderate vs severe MAS
| Feature | Mild | Moderate | Severe |
|---|---|---|---|
| FiO₂ to keep SpO₂ 90–95% | below 30% (room air +/- low-flow) | 30–60% | above 60%, or ventilated |
| Respiratory distress | Minimal, mild tachypnoea | Marked retractions, grunt | Failure, apnoea, fatigue |
| Chest radiograph | Coarse streaky infiltrates | Hyperinflation + patchy infiltrates | Diffuse opacification +/- air leak |
| Air leak | Uncommon | Possible | Frequent |
| PPHN | Absent | Possible | Frequent |
| Typical course | Resolves 24–72 h | Days of support | ECMO / iNO, prolonged [7] |
Clinical Presentation
Infants with MAS typically present with respiratory distress within the first minutes to hours of life, born through visibly meconium-stained liquor. The severity of distress is variable but classically includes tachypnoea (respiratory rate above 60/min), grunting, nasal flaring, intercostal and subcostal retractions, and a hyperinflated (barrel-shaped) chest due to air trapping [7].
Auscultation may reveal coarse crackles and rhonchi from retained meconium and mucus in the airways. Cyanosis in room air reflects the underlying right-to-left shunting and V/Q mismatch. Yellow-green staining of the umbilical cord, nails, skin and vernix provides supportive evidence of meconium exposure and an estimate of duration, since skin staining develops over hours [7].
In the most severely affected infants the picture is one of rapidly progressive respiratory failure: increasing oxygen requirement, labile saturations, a widened pre-/post-ductal gradient, signs of right heart strain (hepatomegaly, tricuspid regurgitant murmur), and hypotension. Hypoxic-ischaemic encephalopathy (HIE) may coexist because the same fetal hypoxia that caused the meconium passage and gasping also injures the brain [7].
Differential Diagnosis
The differential diagnosis of neonatal respiratory distress with MSAF is broad, and several conditions can coexist with or masquerade as MAS. A key principle is that the presence of MSAF does not prove that the respiratory distress is MAS — sepsis, transient tachypnoea of the newborn (TTN), respiratory distress syndrome (RDS) and congenital malformations must all be actively considered [7].
The most important mimics are neonatal pneumonia and sepsis, which produce an identical radiographic picture of patchy infiltrates and may be precipitated or worsened by meconium acting as a bacterial growth medium; TTN, which is milder and self-limited; RDS (rare at term, but surfactant inactivation by meconium produces an identical physiology); and congenital diaphragmatic hernia, cystic adenomatoid malformation and other structural lesions seen on radiograph. PPHN may occur secondary to MAS or as a primary entity, and an echocardiogram is required to distinguish its contribution [6].
MAS vs key mimics in the neonate with MSAF
| Condition | Distinguishing features |
|---|---|
| MAS | MSAF + early distress + coarse hyperinflated CXR; meconium staining |
| Neonatal pneumonia / sepsis | Maternal risk factors, positive cultures, CRP raised; CXR overlap — always cover empirically |
| TTN | Mild, resolves within 72 h; CXR shows perihilar streaking, fluid in fissures |
| RDS | Preterm; ground-glass CXR, low lung volumes; (surfactant inactivation mimics this in MAS) |
| PPHN | Hypoxaemia disproportionate to CXR; pre-/post-ductal gradient; echo confirms |
| Congenital diaphragmatic hernia | Scaphoid abdomen, bowel in chest on CXR; antenatal diagnosis |
| Cyanotic congenital heart disease | No significant distress, fails hyperoxia test; echo diagnostic [6] |
Clinical & Bedside Assessment
Bedside assessment of the infant with suspected MAS is rapid and systematic, focusing on the adequacy of gas exchange, the work of breathing, and the search for complications (air leak, PPHN, HIE). The first priority is a structured Neonatal Resuscitation Programme assessment — tone, breathing or crying, heart rate, colour — because the initial management diverges sharply on the basis of whether the infant is vigorous or not [1].
Ongoing assessment quantifies the respiratory status: respiratory rate, work of breathing (retractions, grunting, nasal flaring), chest hyperinflation, auscultatory findings, and the inspired oxygen concentration required to maintain the target SpO₂ of 90 to 95 per cent in term infants. Continuous pre- and post-ductal oximetry is essential to detect PPHN, since a gradient above 10 to 15 per cent warrants echocardiography [6].
Cardiovascular assessment looks for signs of right heart strain (hepatomegaly, tricuspid regurgitant murmur, hypotension, prolonged capillary refill) and for coexisting HIE (altered tone, seizures, poor feeding). The general examination documents the extent of meconium staining, excludes dysmorphic features and structural anomalies, and assesses temperature and glucose stability [7].
Bedside assessment sequence in suspected MAS
ABC / resuscitation assessment — tone, breathing/crying, HR, colour; decide vigorous vs non-vigorous
Continuous pre- + post-ductal SpO₂; titrate O₂ to 90–95%; record FiO₂
Assess work of breathing (RR, retractions, grunt) and chest hyperinflation
Auscultate for crackles/rhonchi and asymmetry suggesting air leak
Cardiovascular exam: HR, BP, perfusion, murmur, hepatomegaly — look for PPHN signs
Neurological exam for coexisting HIE (tone, seizures, reflexes)
Inspect cord/nails/skin for meconium staining; document extent
Investigations
The investigation of MAS is designed to confirm the diagnosis, grade severity, detect complications, and exclude the principal mimics. The chest radiograph is the cornerstone; arterial blood gases, echocardiography and septic work-up complete the core panel [7].
Chest radiograph typically shows coarse, fluffy or streaky infiltrates with areas of hyperinflation and patchy atelectasis — the classic "fluffy" pattern. Complications seen on film include pneumothorax, pulmonary interstitial emphysema, pleural effusion and cardiomegaly. The radiographic severity correlates only modestly with clinical severity, which is one reason PPHN may be missed without an echocardiogram [7].
Arterial blood gases (pre- and post-ductal) quantify the degree of hypoxaemia, hypercapnia and acidosis and are essential for calculating the oxygenation index (OI), the principal threshold for escalation to inhaled nitric oxide and ECMO. Echocardiography confirms or excludes PPHN, estimates pulmonary pressures, demonstrates right-to-left ductal or foramen-ovale shunting, and excludes structural congenital heart disease [6]. Septic work-up (blood culture, CRP, +/- CSF) and glucose, electrolytes and full blood count complete the panel [7].
Investigation panel in MAS and what each shows
| Test | Purpose / typical finding |
|---|---|
| Chest radiograph | Coarse infiltrates, hyperinflation +/- air leak; grades severity; excludes CDH |
| Arterial blood gas (pre-/post-ductal) | Hypoxaemia, hypercapnia, acidosis; basis for oxygenation index |
| Oxygenation index | OI above 15–25 points to iNO; OI above 40 points to ECMO referral |
| Echocardiogram | Confirms PPHN, R-to-L shunt, RV pressure; excludes CHD |
| Blood culture + CRP + FBC | Exclude sepsis / pneumonia (mandatory) |
| Glucose, calcium, electrolytes | Detect hypoglycaemia, hypocalcaemia (exacerbate distress) |
| +/- Lumbar puncture | If sepsis suspected / before stopping antibiotics [7] |
Management — Resuscitation
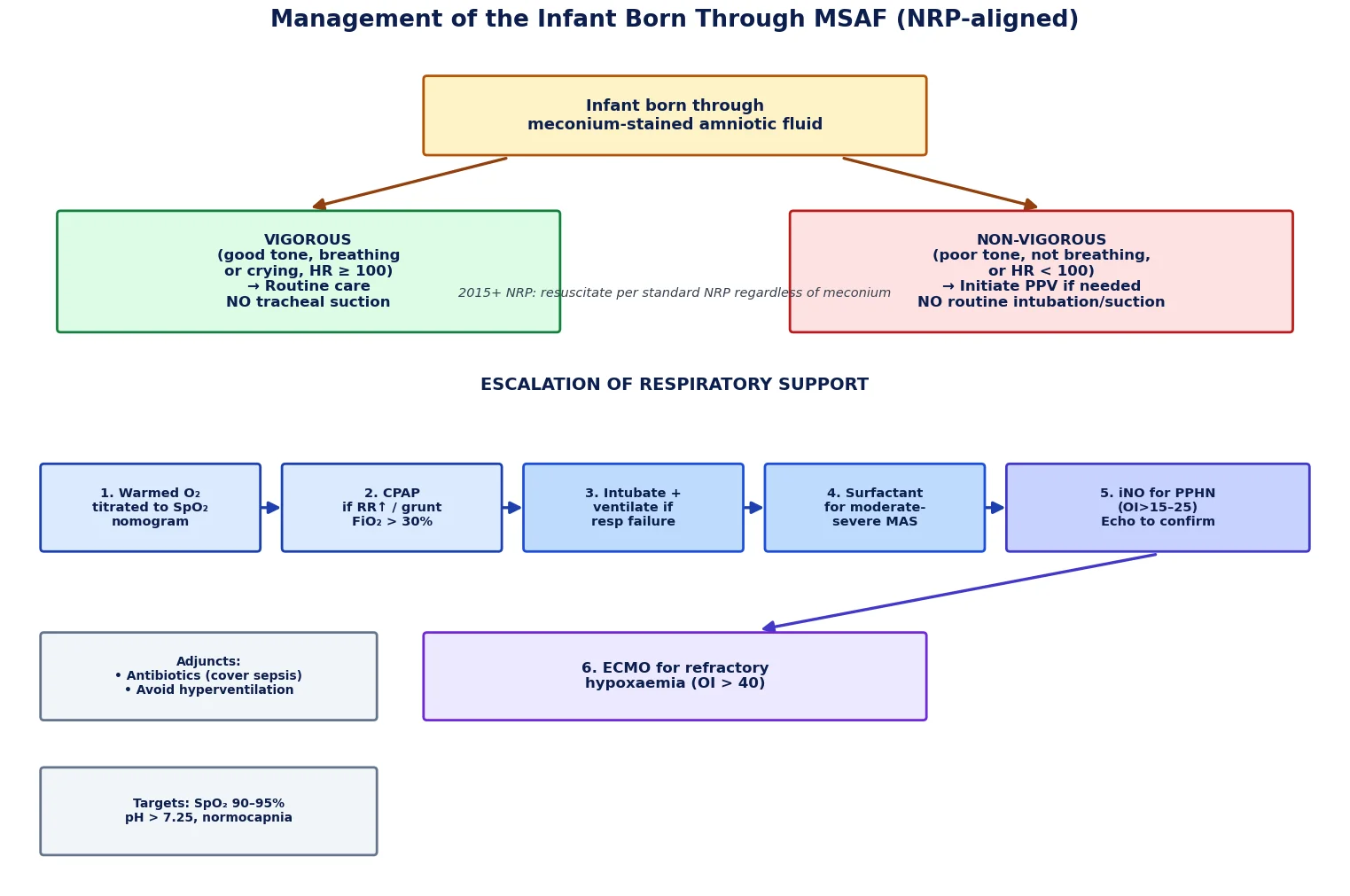
The management of MAS begins at the moment of birth with a delivery-room strategy driven entirely by the infant's clinical state, not by the presence of meconium. This is the single most important conceptual change in neonatal resuscitation of the last two decades, and it is heavily examined [1].
For an infant born through MSAF who is vigorous (good tone, breathing or crying, heart rate at least 100), no tracheal suctioning is performed and routine newborn care is delivered. For an infant who is non-vigorous (poor tone, apnoea or gasping, or heart rate below 100), the current Neonatal Resuscitation Programme and ILCOR guidance is to initiate positive-pressure ventilation if needed and to resuscitate according to the standard NRP algorithm — routine direct laryngoscopy and endotracheal intubation with suctioning is no longer recommended, because evidence showed no benefit and potential harm from delay [1].
This represents a decisive move away from earlier practice. Randomised trials showed that routine oropharyngeal and nasopharyngeal suctioning before delivery of the shoulders (intrapartum suction) confers no benefit in preventing MAS, and it too has been abandoned [1]. The key exception where intubation may still be considered in a non-vigorous meconium-stained infant is when there is suspected physical airway obstruction by particulate meconium that prevents effective ventilation [1].
Delivery-room approach by vigour (current NRP)
| Infant state | Action |
|---|---|
| Vigorous (good tone, breathing/crying, HR at least 100) | Routine care; no tracheal suction; observe |
| Non-vigorous (poor tone, not breathing, HR below 100) | Initiate PPV per NRP; no routine intubation/suction; intubate only if ventilation ineffective due to suspected obstruction [1] |
Management — Definitive & Stepwise
Beyond the delivery room, the management of established MAS follows an escalation ladder of respiratory support, calibrated to severity and to the presence of complications, in parallel with supportive care and sepsis cover [7].
The first step is supplemental oxygen warmed and humidified, titrated to the age-specific SpO₂ nomogram (target 90 to 95 per cent in term infants). If the work of breathing increases or FiO₂ exceeds about 30 per cent, continuous positive airway pressure (CPAP) is commenced, which splints alveoli, reduces work of breathing, and counters the surfactant-inactivation atelectasis. Endotracheal intubation and mechanical ventilation are indicated for respiratory failure (rising PaCO₂, worsening acidosis, fatigue, apnoea), and lung-protective settings aim to avoid air leak [7].
For moderate-to-severe MAS, exogenous surfactant improves oxygenation and reduces the need for ECMO, because meconium potently inactivates endogenous surfactant [2]. Cochrane evidence supports surfactant in this group, with bolus or dilute lavage strategies both described [2][3]. When PPHN is confirmed by echocardiography (or strongly suspected from a wide pre-/post-ductal gradient and disproportionate hypoxaemia), inhaled nitric oxide (iNO) at 20 ppm is the selective pulmonary vasodilator of choice, improving oxygenation and reducing the combined endpoint of death or need for ECMO [6]. ECMO is reserved for refractory hypoxaemia (oxygenation index above 40) failing maximal conventional therapy [6].
Adjunctive care is critical: empiric broad-spectrum antibiotics until cultures are negative (meconium promotes bacterial growth and sepsis is clinically indistinguishable); meticulous temperature, glucose and fluid management; avoidance of hyperventilation (which can worsen cerebral perfusion) while targeting a normal to slightly high pH; and sedation and analgesia to minimise agitation-induced pulmonary hypertension crises [7].
Escalation ladder for established MAS
Warmed humidified O₂ titrated to SpO₂ 90–95% (pre- + post-ductal)
CPAP if FiO₂ above ~30% or rising work of breathing
Intubate + ventilate for respiratory failure (lung-protective: low tidal volume, permissive hypercapnia)
Surfactant for moderate-to-severe MAS (inactivation of endogenous surfactant) — Cochrane-supported
Inhaled nitric oxide 20 ppm if PPHN / OI above 15–25 (echo-confirmed)
ECMO referral if OI above 40 and refractory to iNO
Throughout: empiric antibiotics, normoglycaemia/normothermia, correct acidosis, avoid hyperventilation
Rescue therapies and their triggers
| Therapy | Trigger | Mechanism |
|---|---|---|
| Surfactant | Moderate-to-severe MAS, high FiO₂ | Replaces surfactant inactivated by bile salts/enzymes [2] |
| Dilute surfactant lavage | Severe MAS with thick particulate meconium | Physically clears particulate matter + surfactant [3] |
| Inhaled nitric oxide | PPHN, OI above 15–25, wide pre-/post-ductal gradient | Selective pulmonary vasodilation via cGMP [6] |
| ECMO | OI above 40, refractory hypoxaemia on iNO | Bypasses lung; rests pulmonary circulation [6] |
Specific Subtypes & Scenarios
MAS complicated by persistent pulmonary hypertension of the newborn
PPHN is the defining complication of severe MAS and the principal driver of mortality. It presents with hypoxaemia disproportionate to the radiographic infiltrates, a wide pre-/post-ductal saturation gradient, labile saturations, and signs of right heart strain. Echocardiography is diagnostic, demonstrating elevated pulmonary pressures with right-to-left ductal or foramen-ovale shunting. Management centres on iNO (selective pulmonary vasodilation), correction of acidosis, and avoidance of triggers that worsen pulmonary vasoconstriction (hypoxia, acidosis, pain and agitation) [6].
MAS with pneumothorax or air leak
The ball-valve obstruction in MAS produces air trapping and a high incidence of pneumothorax and pulmonary interstitial emphysema. Sudden clinical deterioration with asymmetrical breath sounds, rising oxygen requirement, or cardiovascular collapse demands urgent chest radiograph and, if tension pneumothorax, immediate needle aspiration followed by chest drain placement [7].
MAS with coexisting hypoxic-ischaemic encephalopathy
Because the same fetal hypoxia that triggers meconium passage and gasping also injures the brain, HIE frequently coexists with severe MAS. Affected infants require assessment for therapeutic hypothermia (within the 6-hour window) according to local criteria; neurological follow-up is essential because long-term outcome is largely driven by the severity of the hypoxic-ischaemic insult rather than the lung disease itself [7].
MAS in resource-limited settings
In low-resource settings the epidemiology of MAS is shifted: higher rates of post-term delivery, less access to antenatal monitoring and obstetric intervention, and limited access to iNO and ECMO. Prevention through avoidance of post-term pregnancy and appropriate obstetric management assumes greater relative importance [4].
Complications & Pitfalls
The acute complications of MAS are dominated by air leak (pneumothorax, pulmonary interstitial emphysema, pneumomediastinum) arising from the ball-valve obstruction, and by PPHN with its attendant profound, oxygen-refractory hypoxaemia. Coexisting HIE, acute kidney injury, hypoglycaemia and disseminated intravascular coagulation may all occur as part of multi-organ hypoxic-ischaemic injury. Secondary bacterial infection of the inflamed, meconium-exposed lung is a constant risk, justifying empiric antibiotics [7].
The principal pitfall is conceptual: continuing to intubate and suction the trachea of a non-vigorous meconium-stained infant, or to perform intrapartum suctioning. These practices were abandoned after randomised trials showed no benefit and the potential for harmful delay in initiating ventilation [1]. A second pitfall is overlooking PPHN — treating only the lung disease without recognising the contribution of right-to-left shunting, leading to inadequate use of iNO and late referral for ECMO. A third is hyperventilation to force down PaCO₂, which can impair cerebral perfusion and is no longer recommended; targets are normocapnia or mild permissive hypercapnia with a pH above 7.25 [6].
Acute complications of MAS
| Complication | Recognition | Action |
|---|---|---|
| Pneumothorax | Sudden deterioration, asymmetrical breath sounds | Urgent CXR; needle aspiration then chest drain |
| PPHN | Disproportionate hypoxaemia, wide sat gradient | Echocardiogram; iNO 20 ppm; correct acidosis |
| HIE | Altered tone, seizures, poor feeding | Assess for therapeutic hypothermia within 6 h |
| Secondary infection | Worsening after initial improvement, CRP raised | Culture + broaden antibiotics |
| Acute kidney injury / DIC | Oliguria, rising creatinine, coagulopathy | Multi-organ supportive care [7] |
Prognosis & Disposition
The prognosis of MAS has improved markedly over the past three decades and now depends predominantly on severity at presentation, the presence and severity of PPHN and coexisting HIE, and the timeliness of escalation [4]. Most infants with mild-to-moderate MAS recover within 24 to 72 hours, and uncomplicated MAS without HIE carries an excellent long-term outlook. Mortality in developed settings is approximately 3 to 5 per cent, almost entirely confined to the severe subset complicated by PPHN or requiring ECMO [4].
Long-term neurodevelopmental outcome is driven by the associated hypoxic-ischaemic brain injury, not by the lung disease itself: infants with MAS who did not sustain significant HIE generally have normal neurodevelopment, whereas those with HIE follow the prognosis of that condition [7]. Chronic lung disease (BPD) is uncommon because most affected infants are term, but it can occur in the most severe cases.
Disposition reflects severity: mild MAS may be managed in a special-care nursery with monitoring; moderate MAS requires a level that can deliver CPAP and escalating FiO₂; and any infant with severe MAS, suspected or confirmed PPHN, or an oxygenation index trending upward warrants transfer to a tertiary neonatal intensive care unit capable of iNO and ECMO [6].
Special Populations
Post-term and growth-restricted infants
Infants born post-term (42 weeks or more) and those with intrauterine growth restriction are at markedly increased risk of both meconium passage and progression to MAS, because chronic intrauterine stress and placental insufficiency predispose to fetal hypoxia, gasping and aspiration. They are also at higher risk of coexisting HIE, hypoglycaemia and hypothermia, and warrant heightened surveillance from the outset [4].
Preterm infants with "meconium-stained" liquor
True meconium passage is rare before 34 weeks. A preterm infant with green-stained liquor should raise suspicion of intra-amniotic infection, particularly Listeria, rather than physiological meconium; investigation and management should be directed accordingly, with a low threshold for septic work-up and antibiotics [7].
Infants of diabetic mothers and large-for-gestational-age infants
These infants are at elevated risk of fetal distress and operative delivery but, more importantly, often have coexisting respiratory distress, hypoglycaemia and polycythaemia that complicate the assessment and management of MAS. Glucose monitoring and early feeding are essential adjuncts [7].
ANZ / RACP: Follows NRP-aligned Australasian Resuscitation Council guidance; iNO and ECMO available in tertiary NICUs; emphasis on avoidance of post-term pregnancy through proactive obstetric management. UK / MRCPCH: NLS (Newborn Life Support) algorithms from the Resus Council UK — same vigour-driven, no-routine-suction approach. US / ABP: NRP 8th edition (AAP/AHA) — identical vigour-based algorithm; ECMO via accredited centres. Canada / RCPSC: NRP-aligned approach with equivalent vigour-based delivery-room management [1].
Evidence, Guidelines & Regional Differences
The evidence base underpinning modern MAS management has reshaped practice profoundly. The Vain et al. multicentre randomised trial (Lancet 2004) of intrapartum oropharyngeal and nasopharyngeal suctioning before delivery of the shoulders showed no reduction in MAS and ended the practice of routine intrapartum suctioning [1]. Subsequent evidence and the 2015 ILCOR and NRP update removed routine intubation-with-suction of non-vigorous infants, after trials showed no benefit and concern for delay in ventilation [1].
Surfactant therapy in moderate-to-severe MAS is supported by Cochrane systematic reviews showing improved oxygenation and reduced need for ECMO [2]; dilute surfactant lung lavage has been investigated in severe particulate MAS, with Cochrane evidence suggesting possible short-term oxygenation benefit but insufficient data for routine recommendation [3]. The changing epidemiology of MAS — falling incidence and mortality — is attributed to obstetric practice change, particularly avoidance of post-term delivery [4]. Amnioinfusion for meconium-stained liquor in labour, while shown in some settings to reduce MAS in the presence of standard intrapartum monitoring, is no longer routinely recommended where adequate fetal monitoring exists, as reflected in current Cochrane analysis [5].
The management of PPHN — including the use of inhaled nitric oxide, gentle ventilation, and ECMO — is built on a body of evidence summarised in classic and contemporary reviews of neonatal pulmonary hypertension [6].
Practice changes over time in MAS
| Era | Practice | Evidence / change |
|---|---|---|
| Pre-2000s | Routine intrapartum suction; routine intubation-suction of non-vigorous | Standard of care |
| 2004 | Intrapartum suction abandoned | Vain et al. RCT — no benefit [1] |
| 2015 (NRP) | Routine intubation-suction of non-vigorous abandoned | ILCOR/NRP — no benefit, harm from delay |
| Current | Surfactant for moderate-to-severe; iNO for PPHN; ECMO for refractory | Cochrane-supported [2][6] |
Exam Pearls
The meconium aspiration syndrome is a high-yield topic that examiners use to test three things: the vigour-based delivery-room algorithm (the single most examined point), the pathophysiological rationale for therapies (why surfactant, why iNO), and the recognition and management of PPHN [1].
Be ready to state clearly that the presence of meconium never mandates tracheal suctioning; vigour dictates action; a non-vigorous infant receives standard NRP resuscitation with PPV. Know the four parallel mechanisms (obstruction, surfactant inactivation, chemical pneumonitis, infection risk), the indication and mechanism of surfactant (inactivation by bile), and the role and threshold for iNO (OI above 15 to 25) and ECMO (OI above 40). Always state that sepsis is covered empirically and that PPHN is screened with pre-/post-ductal oximetry and confirmed with echo [7][6].
Escalation ladder — O-C-V-S-N-E
References
- [1]Vain NE; Szyld EG; Prudent LM; Wiswell TE; Aguilar AM; Vivas NI Oropharyngeal and nasopharyngeal suctioning of meconium-stained neonates before delivery of their shoulders: multicentre, randomised controlled trial. Lancet, 2004.PMID 15313360
- [2]El Shahed AI; Dargaville PA; Ohlsson A; Soll RF Surfactant for meconium aspiration syndrome in term and late preterm infants. Cochrane Database Syst Rev, 2014.PMID 25504256
- [3]Dargaville PA; Copnell B; Mills JF; Harigopal S; Loughnan PM Lung lavage for meconium aspiration syndrome in newborn infants. Cochrane Database Syst Rev, 2013.PMID 23633311
- [4]Gordon MC; Narula K; O'Shaughnessy R; Barth WH Jr Changing obstetric practices associated with decreasing incidence of meconium aspiration syndrome. Obstet Gynecol, 2002.PMID 11978280
- [5]Eke AC; Okoye JA; Eze BI; Okechukwu ZN Amnioinfusion for meconium-stained liquor in labour. Cochrane Database Syst Rev, 2014.PMID 24453049
- [6]Walsh-Sukys MC Persistent pulmonary hypertension of the newborn. The black box revisited. Clin Perinatol, 1993.PMID 8458161
- [7]Fuloria M; Wiswell TE The meconium aspiration syndrome: the saga continues. Indian Pediatr, 1998.PMID 10216539